safer nursing care tool - shelford group · the safer nursing care tool has been developed to help...
TRANSCRIPT
Safer Nursing Care ToolImplementation Resource Pack2014

1 Settingthecontext............................................................................................ 2
2 IntroductiontotheTool.................................................................................... 4
3 AbriefoverviewoftheTool.............................................................................. 5
4 Howisacuityanddependencymeasured?...................................................... 7
5 ExampledatacollectionTools.......................................................................... 8
6 HowdoIensurethataccuratedataarecollected?........................................ 11
7 Whatnursesensitiveindicatorsarealliedtoacuityanddependency?.......... 12
8 Howtousethemultipliers............................................................................... 13
9 Occupancy....................................................................................................... 14
10 Toptipsfromthepilotandfieldtestsites...................................................... 14
11 Frequentlyaskedquestions............................................................................. 15
12 WhocanIcontactifIneedhelp?.................................................................... 16
13 References....................................................................................................... 17
Table of Contents
*TheShelfordGroupisanorganisationcomprisingtheChiefExecutivesoftenoftheleadingNHSmulti-specialtyacademichealthcareorganisationsinEngland.
TheChiefNursesofeachoftheseNHSTrustsbelongtoaSub-Groupoftheorganisationandtheymeeteverytwomonthstosharebest-practice,benchmarkandworktowardsimprovingstandardsinnursing.

Executive National LeadsProfessorKatherineFentonOBE,ChiefNurse,UniversityCollegeLondonHospitalsNHSFoundationTrustandProfessorHilaryChapmanCBE,ChiefNurse,SheffieldTeachingHospitalsNHSFoundationTrust
National Lead Nurses on behalf of Executive Leads:AnnCasey,SeniorNurseN&MEstablishments,UniversityCollegeLondonHospitalsNHSFoundationTrust,ChristineBryer,SeniorNurse,SheffieldTeachingHospitalsNHSFoundationTrustandSueSmith,DirectorofNursing,PatientSafety&Quality,NorthTeesandHartlepoolNHSFoundationTrust.
Validating the Tool and Developing the MultipliersDrKeithHurst,IndependentResearcher/Analyst;Editor,InternationalJournalofHealthCareQualityAssurance
DepartmentofHealthSupportfororiginalversionoftool:RosMoore,thenNursingOfficerDHEngland&Wales
Pilot sites• UniversityHospitalSouthampton
NHSFoundationTrust
• BartsHealthNHSTrust
• UniversityHospitalsCoventryandWarwickshireNHSTrust
• Guy’sandStThomas’HospitalNHSFoundationTrust
• HammersmithHospitalsNHSTrust
• King’sCollegeHospitalNHSFoundationTrust
• UniversityHospitalsofLeicesterNHSTrust
• OxfordUniversityHospitalsNHSTrust
• UniversityCollegeLondonHospitalsNHSFoundationTrust.
Field Test Sites original version• NHSScotland
• NewhamUniversityHospitalNHSTrust
• SheffieldTeachingHospitalsNHSFoundationTrust
• WhippsCrossUniversityHospitalNHSTrust
• Winchester&EastleighHealthcareNHSTrust.
Updating sitesTheShelfordgroupofHospitals*consistingofthefollowing:
• CambridgeUniversityHospitalsNHSFoundationTrust
• CentralManchesterUniversityHospitalsNHSFoundationTrust
• Guy’sandStThomas’HospitalNHSFoundationTrust
• ImperialCollegeHealthcareNHSTrust
• King’sCollegeHospitalNHSFoundationTrust
• TheNewcastle-upon-TyneHospitalsNHSFoundationTrust
• OxfordUniversityHospitalsNHSTrust
• SheffieldTeachingHospitalsNHSFoundationTrust
• UniversityCollegeLondonHospitalsNHSFoundationTrust
• UniversityHospitalsBirminghamNHSFoundationTrust
andAUKUHhospitals.
• AshfordandSt.Peter’sHospitalsNHSFoundationTrust
• UniversityHospitalsCoventryandWarwickshireNHSTrust
• WhippsCrossHospital,London,partofBartsHealthNHSTrust
Acknowledgements
1

Background and descriptionEnsuringwehavetherightstaff,withtherightskillsintherightplaceisActionArea5withinCompassioninPractice(NHSCB2012).Thisemphasisestheneedfordevelopingevidence-based,patientneed-drivenstaffinglevelsinallcaresettings.ThestrategyalsoadvocatesthatthereisatwiceyearlypublicBoardleveldiscussiontoratifyandagreenursestaffinglevelsinadultin-patientandacuteadmissionsunits.
TheSaferNursingCareTool(SNCT)isonemethodthatcanbeusedtoassistChiefNursestodetermineoptimalnursestaffinglevelsinadultin-patientandacuteadmissionsunits.
TheSNCTis:
• Anevidencebasedtoolthatenablesnursestoassesspatientacuityanddependency,incorporatingastaffingmultipliertoensurethatnursingestablishmentsreflectpatientneedsinacuity/dependencyterms.
• AppropriateforuseinanyacutehospitalwithintheUK(althoughfurtherworkisunderwaytorefinethetoolforuseinparticularclinicalenvironments,seesectiononongoingdevelopmentofthetool)
• UsedinconjunctionwithNurseSensitiveIndicators(NSI)suchaspatientfallsandpressureulcerincidence,whichcanbelinkedtostaffing
• AbletosupportbenchmarkingactivityinorganisationswhenusedacrossTrusts.Thiswillfacilitateconsistentnurse-to-patientratiosinlinewithagreedstandardsacrosssimilarcaresettingsinEngland.
Developing and validating the toolThetoolwasvalidatedbyDr.K.Hurst,(thenbasedattheUniversityofLeeds).ThisincludedrecalibratingthetoolusingtheUKNursingDatabase,whichatthattimeincluded1,000bestpracticewards(thoseachievingapre-determinedqualityrating)andsome119,000nursinginterventionsdeliveredtoalmost2,800patientsin14caregroupsovertwoyears.
TheSNCTtoolwastestedinTeachingandDistrictGeneralHospitalsinEnglandandacrossNHSScotland,toconfirmthatthetoolwaseasytouse.
1. Setting the context for using the Safer Nursing Care Tool
In2012theShelfordChiefNursesGroupcommissionedanexpertworkinggroupincludingDr.KeithHursttoreviewthetool,itsdefinitionsandmultiplierstoensuretheSNCTisstillcurrentandapplicable.Afullreviewwasundertakentakingintoconsiderationchangessuchas:
• Theageingpopulation’simpactoninpatientdependencyandacuity;
• Rapidthroughputandshorterpatient-stays;
• DecreasingRegisteredNursedirect-caretimeandthecorrespondingriseinsupportworkerdirectcaretime.
• Newrolesandsupportstaff;e.g.Band4NursingAssistants*andBand1-3housekeepers
Thisrequiredthatthedualscoringexercisewasrepeated.40,000dualassessmentswereundertakeninOctober2012usingtheUKNursingDatabaseandSaferNursingCareTooltoupdatethestaffingMultipliers.
Thestaffingmultipliers(nursingresource)werealsoupdatedforuseinAcuteAdmissionsUnits(AAU).Almost1,600AAUpatientsweredualassessedin2013usingtheUKNursingdatabaseandSNCT.Over1,100hourswerespentobservingnursingactivityandpatientcarein46AAUsrecordingalmost42,000nursingandsupportstaffinterventionsonwardsthatpassedapredeterminedqualityassessment.ThishasproducedtheAAUspecificstaffingmultipliers.
Using the tool in conjunction with other methods to increase assuranceNursingworkloadandtheabilitytoprovidegoodcareisinfluencedbymanyvariablesincludingpatientacuityanddependencyandotherissuesknowntoinfluencenursingworkloadmorelocally;e.g.:
• Theclinicalmodel
• Thelabourmarket
• Staffcapacityandcapability,seniorityandconfidence
• Organisationalfactors;i.e.supportroles,supportexternaltotheward,wardlayout
• SeniorSister/ChargeNursesupervisorytimeandleadershipcapability
2*includesHCAs/AssistantPractictioner
Nonationalworkforcetoolcanincorporateallfactorsandsocombiningmethods(triangulation)isrecommendedtoarriveatoptimalstaffinglevels.ThisshouldincludequantitativeassessmentssuchasthoseencapsulatedintheSNCTandothermorequalitativeandprofessionaljudgementmethodstoincreaseconfidenceinrecommendedstaffinglevelsandprovidebalancedassurance.
TheRoyalCollegeofNursingreport(RCN2010)alsoadvocatestriangulatingdifferentmethodsforcalculatingnursestaffinglevels.Appendix1summarisesothermethodsavailabletohelpdeterminenurseestablishments,whichcanbeusedfortriangulationpurposes.
Are we getting the results we want? Monitoring Nurse Sensitive IndicatorsLinksbetweenpatientacuityanddependency,workload,staffingandqualityhavebeenestablishedinrecentyears.Evidenceintheliteraturelinkslowstaffinglevelsandskillmixratiostoadversepatientoutcomes(Raffertyetal.2007;NPSA2009).
MonitoringNurseSensitiveIndicators(NSIs)suchasinfectionrates,complaints,pressureulcersandfallsisthereforerecommendedtoensurethatstaffinglevelsdeterminedinthewaysdescribedabove,deliverthepatientoutcomesthatweaimtoachieve.WithintheSNCTthesedataareconvertedintoarateper1,000occupiedbeddays,thusallowingconsistentcomparisonacrosswardsandTruststohelpensureoptimumstaffinglevels.
IftheNSIsareadversethenstaffinglevelsrequirepromptreviewtotestiftheinitialrecommendationsremainappropriate.Itisimportanttoexcludefactorsthatmaycompromiseworkforcenumbers,suchashighturnover,sickness,leaveorunfilledvacancies.
Alternatively,theremaybeotherfactorsthatcompromiseworkforceefficacyincludingcompetence,inadequateleadership,poormoraleandpoorcompliancewithgoodpracticeallofwhichwillrequireredressthroughotheraction.
Ongoing development of the toolTheadult/AcuteAdmissionsUnittoolisnotvalidatedforuseinChildren’s/YoungPeople’swards.Thismodeliscurrentlybeingdevelopedfortheseareasandwillbereleasedwhenavailable.
Thetoolisalsobeingfurtherdevelopedtobetterreflectthecomplexitiesofcaringforolderpeopleinacutecarewards;thisversionisalmostreadyforuse.
Additionally,workhasbeencommissionedandisinprogresstodevelopasimilartoolforuseinAccidentandEmergencyDepartments.
DrRuthMay,RegionalChiefNurse,NHSEngland,(MidlandsandEast)leadstheimplementationofActionArea5andlearningfromtheexperienceinNHSScotland,workisunderwaytodevelopSNCTforuseinothercaresettings-Community,MentalHealthandLearningDisabilitiesinthefirstinstance.
Shelford Chief Nurse Group
May2014
3
Appendix 1: Methods available to calculate staffing requirements (Hurst, 2003)
The Professional Judgment model (Telford method)Simpletouseandtakesintoaccountclinicalstaffviewsbutisseentobesubjective,hasnoevidence-baseandisnotsensitivetoworkloadintensity.
Staff to Bed ratioSimpletouse,allowsbenchmarkingbutassumesthatbasestaffinglevelsareaccurateandreflectpatientneedandisinsensitivetochangesinworkload.
Activity Monitoring (GRASP )Usescareplans/carepathwaysandrelatednursingtimebutistaskoriented,canbetimeconsuming(togatherdata/undertakeworkloadstudies)andmayrequiresupportfromcommercialsystems
Nursing hours per patient day (NHPPD)ThismethodiswidelyusedintheUSAandAustralia.Itcalculatesthenumberofnursesandnursingassistantsrequiredinrelationtoactivitylevels.
Regression Methods (Teamwork)Commercialsystemsareavailableandhavebeenusefulwhereworkloadpredictionsarepossible,butisnoteasilyunderstoodbynursesandthereisanunderlyingassumptionthatallwardsareefficientandeffective.
Alloftheabove,usedincombination,provideevidencetoensurethatstaffinglevelsandpatientoutcomesarecorrelated.

TheSaferNursingCareToolhasbeendevelopedtohelpNHSHospitalstaffmeasurepatientacuityand/ordependencytoinformevidence-baseddecisionmakingonstaffingandworkforce.Thetool,whenalliedtoNSIs,willalsooffernursesareliablemethodagainstwhichtodeliverevidence-basedworkforceplanstosupportexistingservicesortodevelopnewservices.
Thisbookletoffersbriefguidanceforpeopleusingthetoolinpractice.
Itincludes:
• Abriefoverviewofthetool
• Howacuityand/ordependencyaremeasured
• Howtoensurethataccuratedataarecollected
• WhatNurseSensitiveIndicatorswillbealliedtoacuityand/ordependencymeasurement
• Howtousenursingmultiplierstosupportprofessionaljudgement
• WhatcanbelearnedfromthepilotsitesandFrequentlyAskedQuestions(FAQ)
• Howtogethelporsupportifneeded.
2. Introduction to the Tool

TheSaferNursingCareTool(SNCT)isbasedonthecriticalcarepatientclassification(Comprehensive Critical Care, DH 2000).Theseclassificationshavebeenadaptedtosupportmeasurementacrossarangeofwards/specialties.ThefullSNCTisoutlinedbelow.
Safer Nursing Care Tool (SNCT)
3. A brief overview of the Tool
Levels of Care Descriptor
Level 0 (Multiplier =0.99*, adult in-patient wards / 1.27* AAU)
Patientrequireshospitalisation
Needsmetbyprovisionofnormalwardcares.
Care requirements may include the following
• Electivemedicalorsurgicaladmission
• Mayhaveunderlyingmedicalconditionrequiringon-goingtreatment
• Patientsawaitingdischarge
• Post-operative/post-procedurecare-observationsrecordedhalfhourlyinitiallythen4-hourly
• Regularobservations2-4hourly
• Early Warning Scoreiswithinnormalthreshold.
• ECGmonitoring
• Fluidmanagement
• Oxygentherapylessthan35%
• Patientcontrolledanalgesia
• Nerveblock
• Singlechestdrain
• Confusedpatientsnotatrisk
• Patientsrequiringassistancewithsomeactivitiesofdailyliving,requiretheassistanceofonepersontomobilise,orexperiencesoccasionalincontinence
Level 1a (Multiplier =1.39*, adult in-patient ward/1.66* AAU)
AcutelyillpatientsrequiringinterventionorthosewhoareUNSTABLEwithaGREATERPOTENTIALtodeteriorate.
Care requirements may include the following
• Increasedlevelofobservationsandtherapeuticinterventions
• Early Warning Score-triggerpointreachedandrequiringescalation.
• Post-operativecarefollowingcomplexsurgery
• Emergencyadmissionsrequiringimmediatetherapeuticintervention.
• Instabilityrequiringcontinualobservation/invasivemonitoring
• Oxygentherapygreaterthan35%+/-chestphysiotherapy2-6hourly
• Arterialbloodgasanalysis-intermittent
• Post24hoursfollowinginsertionoftracheostomy,centrallines,epiduralormultiplechestorextraventriculardrains
• Severeinfectionorsepsis
5

Levels of Care Descriptor
Level 1b (Multiplier = 1.72*, adult in-patient ward/2.08* AAU)
PatientswhoareinaSTABLEconditionbutaredependantonnursingcaretomeetmostoralloftheactivitiesofdailyliving.
Care requirements may include the following
• Complexwoundmanagementrequiringmorethanonenurseortakesmorethanonehourtocomplete.
• VACtherapywhereward-basednursesundertakethetreatment
• PatientswithSpinalInstability/SpinalCordInjury
• Mobilityorrepositioningdifficultiesrequiringtheassistanceoftwopeople
• ComplexIntravenousDrugRegimes-(includingthoserequiringprolongedpreparatory/administration/post-administrationcare)
• Patientand/orcarersrequiringenhancedpsychologicalsupportowingtopoordiseaseprognosisorclinicaloutcome
• PatientsonEndofLifeCarePathway
• Confusedpatientswhoareatriskorrequiringconstantsupervision
• Requiresassistancewithmostorallactivitiesofdailyliving
• Potentialforself-harmandrequiresconstantobservation
• Facilitatingacomplexdischargewherethisistheresponsibilityoftheward-basednurse
Level 2 (Multiplier = 1.97* adult in-patient ward/2.26* AAU)
Maybemanagedwithinclearlyidentified,designatedbeds,resourceswiththerequiredexpertiseandstaffinglevelORmayrequiretransfertoadedicatedLevel2facility/unit
• Deteriorating/compromisedsingleorgansystem
• Postoperativeoptimisation(pre-opinvasivemonitoring)/extendedpost-opcare.
• Patientsrequiringnon-invasiveventilation/respiratorysupport;CPAP/BiPAPinacuterespiratoryfailure
• First24hoursfollowingtracheostomyinsertion
• Requiresarangeoftherapeuticinterventionsincluding:
• Greaterthan50%oxygencontinuously
• Continuouscardiacmonitoringandinvasivepressuremonitoring
• DrugInfusionsrequiringmoreintensivemonitoringe.g.vasoactivedrugs(amiodarone,inotropes,gtn)orpotassium,magnesium
• Painmanagement-intrathecalanalgesia
• CNSdepressionofairwayandprotectivereflexes
• Invasiveneurologicalmonitoring
Level 3 (Multiplier = 5.96*, adult in-patient ward/5.96* AAU)
Patientsneedingadvancedrespiratorysupportand/ortherapeuticsupportofmultipleorgans.
• Monitoringandsupportivetherapyforcompromised/collapseoftwoormoreorgan/systems
• RespiratoryorCNSdepression/compromiserequiresmechanical/invasiveventilation
• Invasivemonitoring,vasoactivedrugs,treatmentofhypovolaemia/haemorrhage/sepsisorneuroprotection
6
Truststaffcollectdataatthesametimetoenablebenchmarkingacrossparticipatingorganisations.Acuityanddependencymeasurementcurrentlytakesplaceatleasttwiceyearly(JanuaryandJune).Overtime,itisanticipatedthatthisacuityanddependencymeasurementwillidentifyseasonaltrendsinresponsetochangingdemographicsandhealthcareneeds.Ultimately,thisevidencebasewillsupportworkforceplansfornursingthatshouldaccuratelypredictandenableresourcestobeidentifiedtosupportnursingestablishmentsthatmeetpatientandserviceneeds.
Acuityanddependencymeasurementmustbeconsistent.Itisessentialtoensurethatallrelevantdataarecollectedduringthesameperiod.Datashouldbecollectedoneverypatientonparticipatingwards/unitsat1500hrs,dailyMondaytoFridayfor20daysasaminimum.Qualitycontrolisfundamentaltoensuringarobustapproachtodatacollection.(Howtoensurethataccurate,qualitycontrolleddataarecollectedisoutlinedinsection6.)Thiswillallownursingstafftounderstandnotonlythelevelsofpatientsonwards,butalsoenablethisinformationtobealliedtootherkeydataincluding:
Nurse Sensitive Indicatorsarequalityindicatorslinkedtonursingcare.Theyinformnursesofgoodandpoorpatientoutcomes,enablinggoodpracticetobesharedandpoorpracticetoberectified.(Seesection7)
Patient Flow informationiscollectedtoenablenursesresponsiblefornursingworkforcereviewstoconsiderissuessuchasthroughput,includingnumbersofadmissions,discharges,transfers,wardattenders,deathsandtransfersawayfromtheward/department,occupancyandstaffinglevels.Themultipliersaccountfornormalpatient-flowlevels,howeverwhenthereisahighthroughputofpatients,anadditionalstaffingupliftmaybeconsideredappropriate-seeexampleinsection11.
NurseSensitiveIndicatorsandpatientflowalliedtoacuityanddependencysupportprofessionaljudgementandenableappropriatenursingestablishmentsformeetingthepatients’needstobeagreed.
ThedatacollectiontoolusedisincludedaspartofthisresourcepackforusebyTruststaff.Ascreenshotofasampledatabaseisalsoincluded.TruststaffmayprefertoworkwiththeirITdepartmentstafftodevelopanelectronicversionofthedatabase.
4. How is acuity anddependency measured?
7

5. Example data collection Tools
Ward .................................... Date
Bed No Level Comment Bed
No Level Comment
1 15
2 16
3 17
4 18
5 19
6 20
7 21
8 22
9 23
10 24
11 25
12 26
13 27
14 28
Patient Flow
Admissions Discharges
Transfer In Transfer out
Deaths Ward attender
Escorts on site Escorts off site
RMN specials:
Completed by
Name ........................................................................ Signature
Verified by ................................................................. Signature

Question 1: Ward Name
Question 3: Acuity Score
Question 5: Staffing
Question 6: Completed by
Question 4: Patient Flow
Question 2: Date
D D M M Y
Bay Bed 0 1a 1b 2 3
1 1
1 2
1 3
1 4
1 5
1 6
2 1
2 2
2 3
2 4
2 5
2 6
3 1
3 2
3 3
3 4
3 5
3 6
4 1
4 2
4 3
4 4
4 5
4 6
Room 1
Room 2
Room 3
Room 4
Please complete for the previous 24 hours 15.00 - 15.00
Please complete for the previous night, current morning and evening shift
RegisteredRegistered Bank / Agency
Unregistered Bank / Agency Unregistered
Admissions
Transfers in
Ward attenders
Escorts on site
Name Signature
Discharges
Transfers out
Deaths
Escorts off site
5 hour
6 hour
7.5 hour
10 hour
12 hour
Other
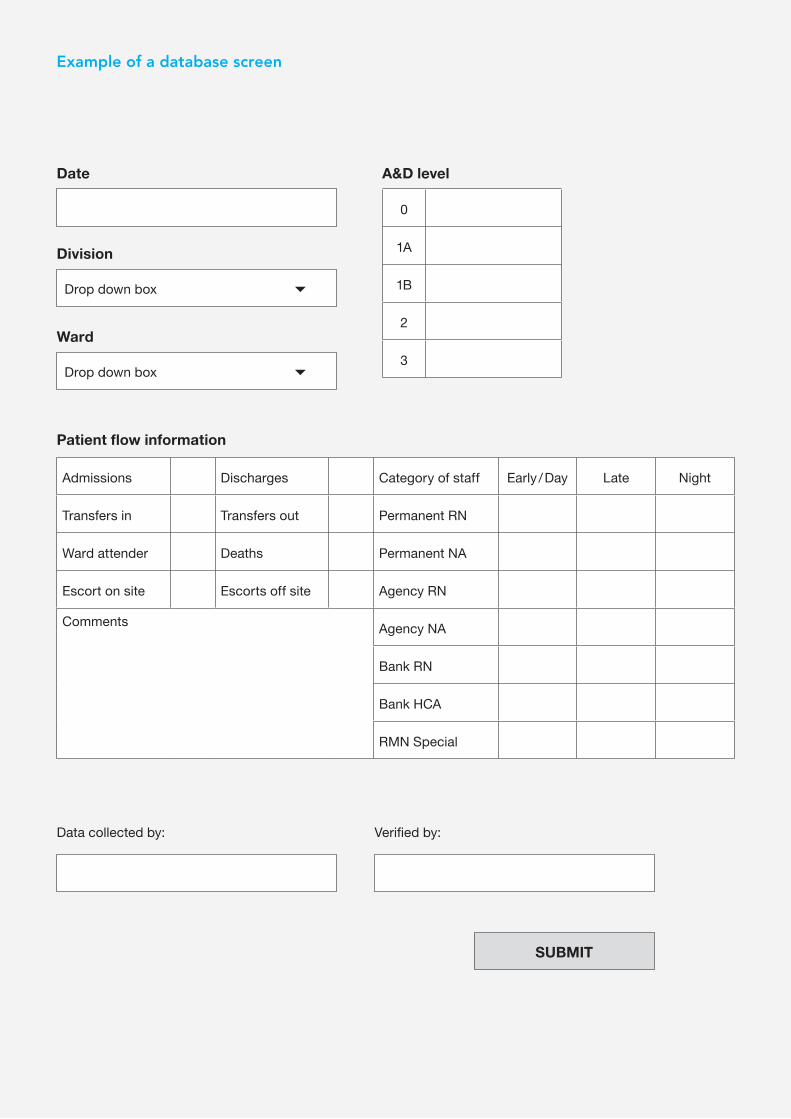
Date
Division
Ward
A&D level
Patient flow information
Drop down box
Drop down box
SUBMIT
0
1A
1B
2
3
Admissions Discharges Category of staff Early / Day Late Night
Transfers in Transfers out Permanent RN
Ward attender Deaths Permanent NA
Escort on site Escorts off site Agency RN
Comments Agency NA
Bank RN
Bank HCA
RMN Special
Data collected by: Verified by:
Example of a database screen

Red RulesQualitycontrolisthekeytosuccessfuldatacollection.Thesesimplestepswillensureaconsistentapproachacrossparticipatingwards:
1 Nominatesomebodytoqualitycontrolthedatacollection.ThismaybeaPracticeFacilitator,amemberofyourCriticalCareOutreachTeamoraseniormemberofthecorporatenursingteam.
2 Identifynomorethanthreeleadersperwardtocompletethescoringdailyforthedurationofthedatacollectionperiod.
3 ThethreeleadersshouldincludetheSisters/ChargeNurses.IfnoSister/ChargeNurseisavailable,anominatedmemberofstaffshouldbeagreedwiththeSeniorNursefortheDirectorate.
4 ThedatacollectionshouldtakeplaceatleasttwiceperyearinJanuaryandJune
5 DatashouldberecordedoneverypatientfromMondayuntilFridayforatotalof20daysasaminimum.
6 Acuityanddependencydatashouldbecollectedforeachpatientineachbedat1500hrs,aspartofabedtobedwardroundreview.
7 Wherepaperbaseddatacollectionisutilised,datacollectionformsshouldbestoredinafolderontheward/unittoawaitcollection/inputtotheelectronicsystem.
8 Patientflowdatashouldbecollectedforthe24-hourperiodleadingtothedatacollectiontime;e.g.,alladmissions/dischargesbetween1500hrsthatdayand1500hrsthepreviousday.
9 NurseSensitiveIndicatordatacanbecollectedretrospectivelybyaseniornurseordirectlypulledfromtheelectronicincidentreportingsystem.
10 Datasheetsshouldbecollectedweeklyfromparticipatingwards/departmentswherecentraldataentrymanagementsystemsareinplace.
11 Datashouldbeenteredontothedatabaseasspeedilyaspossibleaftercollectionorwherethisiscompletedelectronicallyfollowyourlocalpolicybasedontheseprinciples.
12 FeedbackresultstoSistersandChargeNurses,Matrons,DirectorsofNursingandoperationalmanagementteamsassoonaspossible.
6. How do I ensure thataccurate data are collected?
11

NurseSensitiveIndicators(NSIs)refertoqualityindicatorsthatcanbelinkedtonursestaffingissues,includingleadership,establishmentlevels,skill-mixandtraininganddevelopmentofstaff.Thisinformationcanbeusedtofurthersupportwardstaffingrequirementsidentifiedthroughacuityanddependencymeasurement.TheNSIsusedwithinthisprojecthavebeenidentifiedasservicequalityindicatorswithspecificsensitivitytonursinginterventions.
Official ComplaintsOfficialcomplaintsaboutnursing/midwifery/carestaffreceived(per1,000occupiedbeddays)identifyingthethreeareasof:
• Communication
• ClinicalCare
• Attitude
Drug Errors• Actualdrugerrorswherenursingwastheprimarycause,notincludingnear
missesper1,000occupiedbeddays.
Infection• IncidenceratesofMRSAbacteraemiaper1,000occupiedbeddaysand
Clostridium Difficileper1,000occupiedbeddays.
Slips, Trips & Falls• Numberofslips,tripsorfallsper1,000occupiedbeddayscausedprimarily
bynursingerror.
Pressure Ulcers• Incidenceofhospitalacquiredpressureulcersper1,000occupiedbeddays.
Nutrition• Numberofpatientshavinghadnutritionalscreeningper1,000occupiedbed
days.
• PercentageofwardsthathaveimplementedprotectedmealtimespolicywithintheTrust.
7. What nurse sensitive indicators are allied to acuity and dependency?
12

Multiplierscanbeusedtosetnursingestablishmentsalliedtoacuityanddependencymeasurement.Themultipliersagreedforeachlevelofpatientsonin-patientwardsare:
8. How to use the multipliers
13
Level of Care Adult In-Patient wards Acute Admissions Units
Level0 0.99*WTEperbed 1.27*WTEperbed
Level1a 1.39*WTEperbed 1.66*WTEperbed
Level1b 1.72*WTEperbed 2.08*WTEperbed
Level2 1.97*WTEperbed 2.26*WTEperbed
Level3 5.96*WTEperbed 5.96*WTEperbed
Number of patients /level of care
Adult in-patient ward Acute Assessment Unit
12patientsatLevel0 0.99x12 = 11.88 1.27x12=15.24
7patientsatLevel1a 1.39x7 = 9.73 1.66x7 = 11.62
8patientsatLevel1b 1.72x8 =13.76 2.08x8 =16.64
1patientatLevel2 1.97x1 = 1.97 2.26x1 = 2.26
Total 37.34 WTE 45.76 WTE
*thisincludesa22%upliftforannualleave,studyleaveetc.
Forexample,ifa28-beddedwardhas12patientsatLevel0,7patientsatLevel1a,8patientsatLevel1b,and1patientatLevel2,atotalof37.34WTEnursingstaffwouldberequiredforanadultin-patientwardOR45.76WTEforanAcuteAdmissionsUnit.
Thisfigureisabaselineagainstwhichtosetnursestaffinglevels.Two28-beddedwardsmayhavedifferentactivity.Onemayhavefewadmissions,dischargesorwardattenderswhereasanothermayhavemany.Professionaljudgementisrequiredtoensurethatestablishmentsareadjustedappropriatelyunderthesecircumstances(Seeexampleinsection11).
Basedon130,000WardSister/ChargeNurseactivitiesobservedin1,414wards,20%oftheirshiftisspentonmanagerial/administration/coordinatingwork,andthistimeisincorporatedintothemultipliers.Intheorythisequatestoonedayperweek.However,somemanagersallowahigherpercentageandthereforeadjustmentmayberequiredtothetotalestablishmenttoensurethisreflectsthelocallyagreedallowanceforSeniorSister/ChargeNursesupervisorytime.
NurseSensitiveIndicatorscanalsobeusedatthisstagetoascertaintheimpactofacuity,dependencyandactivityonqualityoutcomes.

Occupancyiscalculatedbyobtainingthenumberofavailablebeddaysandthenumberofbeddaysused(thelatteriscalculatedbyaddingtogetherthetotalbedsassignedanacuity/dependencyscoreandarethereforeoccupied)asfollows:
Numberofbeddaysusedx100
Numberofbedsavailable
Forexampleifawardhas420beddaysavailableand400beddaysareused,theoccupancyratecalculationis:400x100=40,000dividedby420=95%occupancy
ThissectionaimstoprovideusefultipstosupportsuccessfulimplementationofSNCTscoringinyourTrust.
PreparationItisessentialthatstaffarepreparedandtrainedtoundertaketheacuityanddependencyscoring.
CommunicationMeetwithSisters/ChargeNursestoexplaintheprocessandreasonsformeasuringacuityanddependency.Iftheydonotunderstandthereasons,theymaybesuspiciousandreluctanttoparticipate.
EnsurethattheExecutiveBoard,GeneralManagersandClinicalDirectorsareengagedandunderstandthepotentialimplicationsofimplementingthistoolacrosstheorganisation.
Quality ControlQualitycontrolbytrainedindividual(s)atacorporatelevelwillensurethatthetoolisappliedconsistentlyacrossallwards/units.
Data InputDatainputcanbetimeconsuming.InputfromtheInformationTechnology(IT)departmentwithanominatedcontactpersonmaybeabletosupportthisaspectoftheproject.
FeedbackWardstaffwelcometimelyfeedbackonthelevelsofacuity/dependencywithintheirarea.
9. Occupancy
10. Top tips from the pilotand field test sites
14

Q If I have had a Level 1b patient in my bed for the last 18 hours and a Level 0 patient has just been admitted to that bed, do I score at Level 0 or Level 1b?
A Scoreforthepatientthathasoccupiedthebedforthelongesttimewithinthelast24hours;inthiscaseatLevel1b.
Q When looking at activity, do I include potential discharges?
A Noyoushouldincludeactualactivitynotpredictedorpotentialactivity.
Q I have just measured acuity for the second time and there is a big change in acuity. How can these data be used as evidence to show that we need more staff?
A Thismaybeananomaly.Itisnotadvisedthatthesedataareusedtoshowtrendsuntilithasbeencollectedanumberoftimes.Pilotsitestaffhavebeencollectingacuitydatasince2005andmaybewillingtosharetheirfindingswithyoutoenablecomparisonstobemade.Itisalsoimportantthatdataaretriangulatedwithotheroutcomes.
Q How do I score empty beds?
A Thesearenotgivenascoreunlessthepatienthasonlyjustgonehome.
Q How do I score a patient whose dependency has changed in the last 24 hours?
A Scoreapatientatthehighestleveltheyhavebeenintheprevious24hours.Donotscorethempredicatively.i.e.ifhe/sheisintheatrethenscorethemastheywerebeforetheywentforsurgery.
Q How do I score if there is a patient in the bed waiting to go home and another waiting to go into it?
A Scorethepatientstillinthebedasyoucannotpredictwhattheotherpatientwillbelike.
Q I have a lot of ward attenders who return for dressing changes - how should I capture this?
A Themultipliersallowforanormallevelofactivity.Wherethewardactivityexceedsthis,professionaljudgementneedstobeapplied.Asimplewayofcalculatingthiswouldbe-iftherewere12patientsattendingthewardeachdayandthedressingtakesonehourofnursingtimetocompletethiswouldrequirethefollowingequation(assumingthatthepatientisLevel0)
No.ofpatientsx1hour÷24(tocalculatethenumberperday)x0.99=
Therefore12x1÷24=0.5x0.99=0.49WTE
11. Frequently asked questions
15
TheShelfordGroupisanorganisationcomprisingtheChiefExecutivesoftenoftheleadingNHSmulti-specialtyacademichealthcareorganisationsinEngland(thesearelistedbelow).TheChiefNursesofeachoftheseNHSTrustsbelongtoaSub-Groupoftheorganisationandtheymeeteverytwomonthstosharebest-practice,benchmarkandworktowardsimprovingstandardsinnursing.
• CambridgeUniversityHospitalsNHSFoundationTrust
• CentralManchesterUniversityHospitalsNHSFoundationTrust
• Guy’sandStThomas’NHSFoundationTrust
• ImperialCollegeHealthcareNHSTrust
• King’sCollegeHospitalNHSFoundationTrust
• TheNewcastleuponTyneHospitalsNHSFoundationTrust
• OxfordUniversityHospitalsNHSTrust
• SheffieldTeachingHospitalsNHSFoundationTrust
• UniversityCollegeLondonHospitalsNHSFoundationTrust
• UniversityHospitalsBirminghamNHSFoundationTrust
12. Who can I contact if I need help?
16
London and the South of EnglandAnnCaseySeniorNurseN&MEstablishmentsUniversityCollegeLondonHospitalsNHSFoundationTrust
Tel:02034472412
Email:[email protected]
North of England and ScotlandChristineBryerSeniorNurseSheffieldTeachingHospitalsNHSFoundationTrust
Tel:01143052158
Email:[email protected]
DepartmentofHealth(2000)Comprehensive Critical Care:A Review of Adult Critical Care Services.London:DH
Hurst,K.(2003)Selecting and Applying Methods for Estimating the Size and Mix of Nursing Teams - A Systematic ReviewcommissionedbytheDepartmentofHealth.Leeds:NuffieldInstituteforHealth.
NationalPatientSafetyAgency(2009)Quarterly data summary. Issue 13: Learning from reporting - staffing. How do staffing issues impact on patient safety?London.NPSA
NHSCommissioningBoard(2012)Compassion in Practice, Nursing, Midwifery and Care Staff. Our Vision and Strategy.Leeds:NHSCB
Rafferty,A.M.ClarkeSP,ColesJ,BallJ,JamesP,McKeeM,AikenLH(2007)Outcomes of variation in hospital nurse staffing in English hospitals: a cross sectional analysis of survey data and discharge records.InternationalJournalofNursingStudies,44,(2),pp175-182
RCN(2010)Guidance on safe nurse staffing levels in the UK.London:RoyalCollegeofNursing
13. References
17
Bibliography
Ball,J.A&Washbrook,M.(1996)Birthrate Plus: A Framework for Workforce Planning and Decision-making for Midwifery Services.Cheshire.BookofMidwives
DepartmentofHealth(2013)The Cavendish Review : An Independent Review into Healthcare Assistants and Support Workers in the NHS and social care settings.London:DH
DepartmentofHealthandHumanServices(2011)Safe Staffing - User Manual Nursing Hours per patient day Model.Tasmania:DepartmentofHealthandHumanServices
DepartmentofHealth(2000)Comprehensive Critical Care: A Review of Adult Critical Care Services.London:DH
Hurst,K.(2005)Developing and Validating the AUKUH’s WP&D System.CommissionedbyAUKUHDirectorsofNursing.
Scott,C.(2003)Setting Safe Nurse Staffing Levels.London:RCN
Smith,S.Casey,A.Hurst,K.Fenton,K.Scholefield,H.A.(2009)Developing, testing and applying instruments for measuring rising dependency-acuity’s impact on ward staffing and quality.InternationalJournalofHealthCareQualityAssurance.22,(1),pp30-39

ProducedinconjunctionwiththeAssociationofUKUniversityHospitals