safe surgery and interventional procedures policy
TRANSCRIPT

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 1 of 41
Safe Surgery and Interventional Procedures Policy
Post holder responsible for Procedural Document
Adrian Harris, Medical Director
Author of Policy Alex Grice, Governance and Patient Safety Lead Surgical Services Division
Division/Department responsible for Procedural Document
Cluster 4, Surgical Services Division (on behalf of the Medical Director)
Contact details x3919
Date of original document 01-07-11
Impact Assessment Performed
Yes/No
Ratifying body and date ratified Safety and Risk Committee: 19-07-18
Review date (and frequency of further reviews)
June 2022 (five yearly)
Expiry date
20 January 2023
Date document becomes live
07 August 2018
Please specify standard/criterion numbers and tick ✓ other boxes as appropriate
Monitoring Information Strategic Directions – Key Milestones
Patient Experience ✓
Maintain Operational Service Delivery
Assurance Framework ✓
Integrated Community Pathways
Monitor/Finance/Performance Develop Acute services
CQC Fundamental Standards – Regulation:
Infection Control
Other (please specify):
NPSA/2009/PSA002/U1 WHO Surgical Safety Checklists
NHS England: National Safety Standards for Invasive Procedures (NatSSIPs) 07-09-15
NHS/PSA/RE/2015/008 Supporting the introduction of the National
Safety Standards for Invasive Procedures 14-09-15
NHS/PSA/D/2017/006 Confirming removal or flushing of lines and
cannulae after procedures 09-11-17
Note: This policy has been assessed for any equality, diversity or human rights implications
Controlled document This document has been created following the Royal Devon and Exeter NHS Foundation Trust Development, Ratification & Management of Procedural Documents Policy. It should not be altered in any way without the
express permission of the author or their representative.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 2 of 41
Full History Status: Final
Version Date Author Reason
1.0 11-10-11 Medical Director New Policy launched on 11 October 2011
2.0 12-11-12 Chair, Critical Care Governance Group
3.0 06-03-13 Chair, Critical Care Governance Group
4.0 10-07-13 Chair, Critical Care Governance Group
5.0 23-10-14 Governance and
Patient Safety Lead, Surgical Services
6.0 10-06-15 Governance and Patient Safety Lead
Annual review of Policy–minor amendments, additional checklists to appendices
Minor amendments made to Policy and Checklists as a result of CQC Inspection Report in February 2013
Minor amendments made to Policy and Briefing checklist as a result of Internal Audit reports RDE27/13, June 2013 and RDE15/13, July 2013
Minor amendments – routine review
2 minor amendments resulting from incident investigations
7.0 13-12-16 Governance and Patient Safety Lead in conjunction with the Safe Surgery Review Group
Review of policy to incorporate changes made as a result of NHSE (Patient Safety Domain) guidance: National Safety Standards for Invasive Procedures (NatSSIPs) 07-09-15 together with feedback from stakeholders.
8.0 20-09-17 Medical Director (at Safety & Risk Committee 20-09- 17 – see action point 72.17)
9.0 20-06-18 Medical Director (at Safety & Risk Committee)
Removal of spinal surgery from the patient marking exceptions list (section 10.8) – given chair’s approval by Medical Director, 20-09- 17, Safety and Risk Committee.
Addition of information in relation to Patient Safety Alert NHS/PSA/D/2017/006 Confirming removal or flushing of lines and cannulae after procedures.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 3 of 41
Associated Trust Policies/Procedures:
Commercial Representatives Conduct Policy
Consent to Treatment and Examination Policy
Disciplinary and Appeals Policy
Identification of Patients Policy
Incident Reporting, Analysing, Investigating and Learning Policy and Procedures
Infection Control Prevention and Control Policy
Policy for Patients who Refuse Blood Components or Products
Exeter Clinical Laboratory’s Pathology Form and Specimen Labelling Procedure
Checking Pregnancy Status Before Treatment for under 18s Procedure
Privacy, Dignity and Compassion Policy
Supporting Staff Involved in Adverse Events
Theatre Guidelines
Specimen Handling Procedures in Theatre
Specimen Labelling Procedures in Theatre
Key Words:
Safe surgery, theatres, patient safety, pregnancy status, teamwork, human factors, NatSSIP, LocSSIP
In consultation with and date:
Five Steps to Safe Surgery Audit Group members, membership includes all theatres (including Community Theatres) / Surgery / Anaesthetics: 15-05-18
Anaesthetics/Theatres Specialty Governance Group: 22-05-18
Theatres staff and Anaesthetics staff: 15-05-18
Associate Medical Directors and Governance Managers, Medicine and Specialist Services Division: 30-05-18 (by email)
Medical Director/Chief Nurse/Divisional Directors/Assistant Directors of Nursing/ / Head of Governance/Acting Deputy Head of Governance/Acting Head of Safety, Risk and Patient Experience/Risk Manager: 30-05-18 (by email)
Governance Administration (Surgical Services): 06-07-18.
Quality Assurance Process: 07-08-18 (email)
Safety and Risk Committee: 19-07-18 (version 9)
Contact for Review:
Mark Daugherty, Associate Medical Director, Surgical Services Division
Executive Lead Signature:
Dr. Adrian Harris, Medical Director

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 4 of 41
CONTENTS
1. INTRODUCTION ......................................................................................................... 5
2. PURPOSE ................................................................................................................... 6
3. OBJECTIVES .............................................................................................................. 7
4. DEFINITIONS .............................................................................................................. 7
5. DUTIES AND RESPONSIBILITIES OF STAFF ........................................................... 8
6. WORKFORCE .......................................................................................................... 10
7. SCHEDULING AND LIST MANAGEMENT ............................................................... 11
8. PRE-OPERATIVE ASSESSMENT ............................................................................ 15
9. WARD PREPARATION ............................................................................................ 16
10. PATIENT MARKING ................................................................................................. 18
11. SIGN OUT FROM WARD – PROCESS ..................................................................... 20
12. FIVE STEPS TO SAFE SURGERY ........................................................................... 20
13. SIGN IN TO ANAESTHETIC/ PROCEDURE ROOM (STEP TWO) ........................... 22
14. REGIONAL ANAESTHESIA ..................................................................................... 23
15. TIME OUT (STEP THREE) ........................................................................................ 23
16. SIGN OUT FROM THEATRE (STEP FOUR) ............................................................. 24
17. THEATRE TEAM DEBRIEFING (STEP FIVE) .......................................................... 25
18. SURGICAL CHECKLIST FOR ORGAN DONATION FROM DEAD PATIENTS ........ 26
19. MANAGEMENT OF PATIENTS UNDERGOING SURGICAL PROCEDURES
REQUIRING LOCAL ANAESTHETIC ONLY ............................................................ 26
20. MANAGING PROCESS FAILURE ............................................................................ 26
21. THEATRE ENVIRONMENT ...................................................................................... 27
22. TRAINING REQUIREMENTS .................................................................................... 27
23. ARCHIVING ARRANGEMENTS ............................................................................... 28
24. AUDIT ARRANGEMENTS ........................................................................................ 28
25. MONITORING COMPLIANCE WITH AND EFFECTIVENESS OF THE POLICY ...... 29
25. ASSOCIATED TRUST POLICIES ............................................................................. 31
26. REFERENCES .......................................................................................................... 31
APPENDIX 1: SURGICAL SAFETY CHECKLISTS: LINKS TO BARCODED DOCUMENT
LIBRARY ........................................................................................................................... 32
APPENDIX 2: LOCAL GUIDELINES REQUIRING DEVELOPMENT (LOCSSIPS) ............ 33
APPENDIX 3: FLOWCHART FOR WARDS – SIGN OUT FROM WARDS ........................ 34
APPENDIX 4: FLOWCHART OF MANAGEMENT RESPONSIBILITIES ........................... 35
APPENDIX 5: PATIENTS WHO DECLINE A PREGNANCY TEST - DECISION TREE ..... 36
APPENDIX 6: SURGICAL NEVER EVENTS ...................................................................... 37
APPENDIX 7: COMMUNICATION PLAN ........................................................................... 39
APPENDIX 8: EQUALITY IMPACT ASSESSMENT TOOL ............................................... 40

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 5 of 41
1. INTRODUCTION 1.1 General
1.1.1 The first job of all healthcare professionals is to keep patients safe. Patients undergoing surgical and other interventional procedures place their trust in all members of staff to follow the correct processes, policies and protocols required to ensure that we are properly prepared to perform the right procedure, on the right patient, every time.
1.1.2 In June 2008 the World Health Organisation (WHO) launched a safety challenge
“Safe Surgery Saves Lives” to reduce the number of surgical deaths across the world and strengthen the commitment of clinical staff to address safety issues within the surgical setting. This included improving anaesthetic safety practices, ensuring correct site surgery, avoiding surgical infections and improving communication and teamwork within the team.
1.1.3 The Royal Devon and Exeter NHS Foundation Trust (hereafter referred to as the Trust)
implemented a Correct Site Surgery Policy (2008) as a result of National Patient Safety Agency (NPSA) patient safety alerts (2005 and 2008) and introduced the use of a Surgical Safety Checklist modelled on the WHO Checklist and in line with the recommendations outlined in the NPSA Guidance Five Steps to Safer Surgery (2010).
1.1.4 On 7 September 2015, NHS England released guidance: National Safety Standards for Invasive Procedures (NatSSIPs) followed on 15 September by a Patient Safety Alert: NHS/PSA/RE/2015/008 Supporting the introduction of the National Safety Standards for Invasive Procedures. This Policy has been revised and updated in line with new information contained in this guidance. The Policy also takes account of guidance from the Association for Perioperative Practice (AfPP) Standards and Recommendations for Safe Perioperative Practice, fourth edition 2016; and from Patient Safety Alert NHS/PSA/D/2017/006 Confirming removal or flushing of lines and cannulae after procedures.
1.1.5 This policy sets out a detailed process to be rigorously followed by all staff involved in
providing surgical or interventional procedures in theatre settings, e.g. General, Princess Elizabeth Orthopaedic Centre (PEOC), Centre for Women’s Health (CWH), West of England Eye Unit (WEEU), Heavitree daycase, Community theatres and Procedure suites, such as Endoscopy, Cardiology and Radiology. See Appendix 1 for a detailed list of surgical safety checklists associated with this Policy.
1.1.6 The guidance noted in 1.1.4 recommends development of local standards (LocSSIPs)
for invasive procedures carried out in other settings, e.g. Outpatient Departments, treatment rooms, Emergency Department, on the wards, etc. Appendix 2 lists areas that have developed specialty-specific checklists and/or are developing local guidelines.
1.2 Does this policy apply to me? A Common Sense Approach
1.2.1 This Policy mandates some key processes and behaviours applicable to all procedures
within hospital, such as the requirements for team work; to robustly confirm patients’ identity and the key details of a procedure before commencing. Clearly, however, fundamental variations exist within the processes and languages used within different operating environments, which must be taken into consideration in order for this policy to be practical and meaningful.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 6 of 41
1.2.2 A key part of this Policy, for example, relates to anaesthetic check-in procedures yet we know that many daycase operations and procedures within Cardiology and Endoscopy do not require an anaesthetist. Similarly, some variations in terminology such as “theatre, surgeon, operator, operation, surgery, procedure, treatment, interventional procedure, diagnostic test” etc., might lead some specialities to feel that this policy may not be applicable to them.
1.2.3 In all cases where confusion might occur, a common sense approach should be used.
1.2.4 Procedures without an anaesthetist present may not require an anaesthetic check-in, for example; however, the team would still be expected to follow those elements of this policy which are clearly applicable. Equally, pre-operative assessment may not be appropriate for all patient groups and it is not the intention of this Policy to generate unnecessary patient episodes where there is limited or no added value.
1.2.5 It is appropriate for some specialties to include additional checks to address specific aspects of patient management, and this is actively supported by this Policy.
1.2.6 All specialties are therefore required to consider this Policy carefully and implement those elements which ‘fit’ with their processes in the interests of patient safety. Working as a team, Clinical Directors, Clinical Leads, Cluster Managers, Senior Nurses and other senior managers are required to review this policy and consider:
How to implement the processes which apply to the procedures within their specialty
How compliance will be monitored
Any special arrangements which might be required in order to meet policy requirements
Any areas which do not apply to their specialty, documenting controls in place to ensure patient safety is not compromised in their absence.
1.2.7 Failure to comply with this policy could result in disciplinary action.
2. PURPOSE
2.1 This Policy describes the steps that must be taken to ensure that any surgical or
invasive procedure is performed on the correct patient, the correct site and, if applicable, with the correct implant.
2.2 This Policy is applicable to all patients (adults and children) undergoing operative and
other invasive procedures performed under both local and/or general anaesthetic. This includes procedures performed in settings other than the operating theatre (e.g. interventional radiology, cardiology, endoscopy, dermatology, oral surgery, gynaecology, and procedures or operations performed in external services managed by the Trust (e.g. Community Theatres). Any future checklists developed within specialties should follow the principles of the original Surgical Safety Checklist (see Appendices 1 and 2) which includes safety critical checks only.
2.3 This Policy is applicable to all medical and clinical staff involved in the pre-operative
and perioperative care of patients undergoing surgery or interventional procedures in areas outlined in Section 1.1.15 and Appendix 1.
2.4 Failure to comply with, or act in accordance with, the terms laid down in this Policy may
result in disciplinary action.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 7 of 41
2.5 Falsification of any documentation, either paper or electronic, may be considered as gross misconduct. Staff should be aware that disciplinary action may be taken against them.
3. OBJECTIVES
No avoidable harm or death of patients undergoing surgery due to:
o Insufficient preparation before an operation
o Poor teamwork or communication
o Failure to robustly confirm key information relating to patient or the procedure being undertaken
Ensure patient safety is maintained throughout the perioperative journey
Assurance for Divisions and the Trust that by reliably using the Checklists listed in Appendix 1, the standards for ensuring correct site surgery/procedures are adhered to.
4. DEFINITIONS 4.1 Active Listening: a term used in Theatres to indicate the need for absolute silence
and attention required by all staff during key safety checks, e.g. Time Out and Sign Out.
4.2 Safety Pause: a mini briefing undertaken prior to any emergency case
4.3 EPRAT: Exeter Pressure Risk Assessment Tool, measurement for risk of skin damage
4.4 Five Steps to Safe Surgery:
Briefing (Step One): meeting where operating team share vital information about patients and potential/actual safety issues prior to commencement of the list.
Sign In (Step Two): safety checks undertaken in the Anaesthetic room on arrival of the patient.
Time Out (Step Three): safety check undertaken immediately prior to undertaking surgery.
Sign Out (Step Four): safety check undertaken immediately following surgery.
Debriefing (Step Five): post-list communication between theatre team and an opportunity to review any issues that arose throughout the day.
4.5 LocSSIP: Local Safety Standards for Invasive Procedures – local guidelines
developed according to the principles of the Safe Surgery Policy. 4.6 Critical Steps: Something out of the ordinary – a deviation from routine care.
A critical step is a point in the process at which there are key decisions to be made (e.g. converting to open, adding another specimen); key steps that must occur for a successful outcome (e.g. throat pack removal) or any point within the process that the pathway is not certain at the outset (the 'we might do this but if we find this then we will do that instead' type operation).

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 8 of 41
5. DUTIES AND RESPONSIBILITIES OF STAFF
5.1 Teamwork in Surgery
5.1.1 All aspects of healthcare rely on people working together safely and effectively and good teamwork is a vital defence available for a safer healthcare system. Recent research allows us to understand more about how errors happen in the operating theatre.
5.1.2 It is known that the way teams work together (leadership, communication, shared situational understanding and the opportunity to ‘speak up’) contributes significantly to the risk of errors (see ‘Just a Routine Operation’, (NHS Institute for Innovation and Improvement, 2008]).
5.1.3 The following are the responsibilities for key staff members who interact with patients during their perioperative journey. See Sections 8-17 for individual responsibilities in relation to completion of the Checklist.
5.2 All Staff
5.2.1 All staff are required to demonstrate some fundamental behaviours in order to keep patients safe. These are:
To work and communicate as a part of a team
To have the courage to protect patients and colleagues by speaking out if they have any concerns regarding patient safety
To receive challenge from a colleague in a positive and professional manner, giving the concerns others may have due consideration.
5.2.2 In addition, all staff are responsible for ensuring Datix incident reports are completed for any deviation from the Policy.
5.3 Registered Ward Nurse
5.3.1 On all surgical wards, including Creedy, Acute Medical Unit (AMU) and Endoscopy, the registered nurse is responsible for final pre-operative preparation of the patient and correct completion of the Ward Sign Out documentation (flow chart Appendix 2).
5.3.2 For all remaining medical wards, the ward registered nurse is responsible for completing the Sign Out in conjunction with a trained member of theatre staff.
5.4 HCA (Band 3 or 4)
5.4.1 If a theatres HCA staff member has competency training, he/she is able to retrieve the patient from Medical wards and complete the Ward Sign Out checks with the registered ward nurse handing over the patient.
5.5 Theatre Assistant (TA)
Responsible for collecting the patients from all surgical and medical wards when Ward Sign Out checks have been completed.
5.6 Surgeon / Radiologist / Endoscopist (Person Performing Procedure):
Responsible for ensuring correct patient identification, correct site surgery and correct examination or treatment is performed on the patient.
Responsible for ensuring Team Briefing, Time Out, Sign Out and Team Debriefing take place.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 9 of 41
5.7 Anaesthetist:
Responsible for ensuring Sign In to Anaesthetic Room has occurred prior to any anaesthetic intervention and ensuring correct site regional block, i.e. Stop Before You Block, is performed on the patient.
5.8 Anaesthetist Assistant (Operating Department Practitioner [ODP], Theatre Practitioner, Nurse or Physician’s Assistant):
Responsible for ensuring the Sign In to anaesthetic room is complete and correct.
5.9 Scrub Nurse:
Responsible for withholding skin preparation, instruments or equipment until Time Out has been completed.
Responsible for ensuring all equipment used during the procedure complies with appropriate sterility standards
Responsible for ensuring that all swabs and instruments are accounted for.
Responsible for ensuring all specimens undertaken during the case are documented on the specimen board and managed according to the requirements of the Specimen Handling in Theatres Policy and Procedure
Responsible for completing Sign Out (Step 4) of the Checklist.
Responsible for prompting the surgeon to instigate Team Debriefing (Step 5).
Responsible for handover of patient to recovery staff.
5.10 Operating Team (in Anaesthetic Room and Operating Theatre):
Responsible for ensuring checks are completed and confirmed on the Checklist.
Responsible for stopping and pausing while Time Out is undertaken before the treatment/surgery commences.
5.11 Theatre Team Leader / Theatre Coordinator:
Responsible for ensuring that the Briefing Checklist is completed and stored in the red binder in the theatre.
Responsible for ensuring the surgeon and anaesthetist are present in the building.
Responsible to ensure that all operating lists are appropriately staffed with competent personnel.
The following are responsibilities for management staff (see flow chart Appendix 3) 5.12 Safety and Risk Committee:
Responsibility for the ratification of this Policy and for receiving annual reports on its effectiveness.
5.13 Medical Director:
Overall Trust-wide responsibility for the development, review, implementation and monitoring of this Policy.
Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 10 of 41
Responsible for reporting compliance monitoring results to the Safety and Risk Committee.
5.14 Divisional Directors:
Responsible and accountable for ensuring that the standards of practice outlined in this Policy are maintained and assured.
Responsible for ensuring that monitoring systems are in place to enable robust assurance of compliance with this Policy to be provided to the Medical Director and the Safety and Risk Committee.
Responsible for identifying and resolving gaps in service provision which might adversely impact upon compliance with this Policy within their Division.
5.15 Associate Medical/Clinical Directors:
Responsible for ensuring medical staff receive guidance and training, understand the Policy and adopt the requirements within their practice.
5.16 Assistant Directors of Nursing:
Responsible to ensuring nursing staff and other non-medical healthcare professionals receive guidance and training, understand the Policy and adopt the requirements within their practice.
5.17 Line Managers/Supervisors
Responsible for ensuring all staff receive guidance and training, understand the Policy and adopt the requirements within their practice.
6. WORKFORCE
6.1 Effective organisation by all members of the perioperative team is essential for the
efficient management of elective and scheduled operating sessions. Managers responsible for calculating staff establishments comply with the recommendations set out in the Association for Perioperative Practice (AfPP) Standards and Recommendations for Safe Perioperative Practice, fourth edition, (Association for Perioperative Practice, 2016). The aim is to reduce or prevent the cancellation of elective surgery by ensuring that allocated theatre time is planned effectively and that perioperative personnel are deployed appropriately to identify service demand.
6.2 It is the responsibility of the Theatre Coordinator or designated team lead to ensure
that every elective and emergency operating list is staffed by a team of appropriately trained and competent personnel who are equipped with the knowledge, skills and abilities to administer high quality patient care, and who are able to identify and minimise any risks to the patient as they journey through the perioperative environment.
6.3 The workforce will reflect the complexity of the operating list, and a minimum level
below which a list will be cancelled (dependent on staff skill mix and list complexity) is as follows:
6.3.1 General, PEOC, WEEU, CWH AND Community Theatres (no fewer than 5 staff):
2 x Scrub practitioners (e.g. 1 x Band 5 + 1 x Band 3 with scrub competences)
1 x Circulator (Band 2 +)
1 x Operating Department Practitioner (ODP) / registered anaesthetic practitioner

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 11 of 41
1 x Theatre Assistant (TA)
1 x Recovery registered practitioner. 6.3.2 Endoscopy Suites (no fewer than 4 staff):
1 x Decontaminator
1 x patient advocate (registered practitioner or Band 3 with Recovery competences)
1 x registered practitioner to admit, discharge, consent
1 x registered practitioner to assist the Endoscopist. 6.3.3 Emergency theatres
Monday to Friday from 1700-2000 hours = 5 staff
Monday to Friday from 2000-0800 hours = 4 staff and on calls Note: Any on call system must be adequate for the urgency and timeframe in which staff will be needed and the clinical skills required to manage emergency surgery.
Emergency surgery undertaken outside of core working hours must be a consideration when providing appropriate level of skill and competence and resource to support perioperative care and provision.
The number of staff required for an emergency session may be less than that required for an elective session, depending upon the specialty and normal pattern of emergency work and risk assessment.
7. SCHEDULING AND LIST MANAGEMENT
7.1 Booking Rules for Elective Theatre lists The purpose of these positive booking rules is to support the operating theatre teams to provide safer surgical care, boost productivity and take into account the Trust’s financial responsibilities.
The management will aim to work to the rules as documented below however there will be some circumstances that will require a flexible approach as with some cancer patients.
The aim of the 8-week positive booking process includes the following:
To deliver an effective process that meets the needs of the surgical teams, the anaesthetic department and theatre teams.
To simplify the configuration of Surgical and Anaesthetic staffing
To simplify the arrangement of required equipment
Will increase theatre utilisation
Will reduce unused resources and promote financial savings
Allow operational managers and clinical leads to backfill vacant theatre sessions
Forward planning of appropriate staffing for specific lists
Allow senior theatre staff, cluster managers and clinicians to review lists to prevent under and over runs
Allow surgical teams to book Critical Care beds
To provide a clear booking process over an 8 week period
Recognition that lists may change due to clinical urgency. 7.2 Booking Process:
At Week 8 & 7 - Confirm the specific surgeon for allotted specialty -backfill within own specialty
At weeks 6 & 5 – Any vacant theatre session offered to all specialities
At week 4 – Available session across all theatres will be reviewed by Divisional business manager or Divisional manager, decision to stand down a theatre to be made.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 12 of 41
At weeks 4 & 3 – PEOC, Community, WEEU and Heavitree Day case theatres list to be 75% completed
At week 2 - 100% of list for PEOC, Community, WEEU and Heavitree Day case theatres to be completed. Main theatres list to be 75% completed. Matrons/Team Leaders to review theatre lists for relevant specialty.
At week 1 – Main theatre list 100% booked. 7.3 Management review:
Week 8 & 7 Review leave notification provided
Week 6 & 5 Divisional escalation of available lists to cluster managers
Week 4 & 3 Critical Care Escalation and loaded to schedule
Week 2 PEOC, Community, WEEU and Heavitree Day case theatres locked down and loaded on to Plato
Week 1 Main theatres locked down and loaded on to Plato
7.4 Booking of the theatre list: Under or over assigned sessions will be challenged by theatre matrons and Cluster manager. For PEOC, Community, WEEU and Heavitree Day case theatres this process will take place week 2 prior to surgery. Main theatres lists will be reviewed and challenged 1 week before surgery.
Patients requiring specialist loan kit must be booked with enough time to allow the Hospital Sterilisation and Decontamination Unit (HSDU) to process the equipment. Patients requiring non-stock implants must be booked and theatres notified to allow the procurement process time to order and receive implants avoiding overnight orders
7.5 Booking of the Emergency Theatres
The Emergency theatres comprise three theatres:
The Emergency Theatre for emergency procedures of all specialties.
Heavitree Day case theatres for plastic trauma.
Trauma theatre (Theatre 8) for emergency orthopaedic procedures. 7.5.1 Booking of emergency cases for into the Emergency theatre:
The emergency theatre works 24 hours a day 7 days a week to facilitate all specialties with patients requiring emergency surgery. The theatre list runs by prioritising patients, considering clinical need, time sensitive case, and paediatric patients.
Cases can only be booked by completing the Emergency theatre booking form. All general surgery and upper Gastro Intestinal emergencies cases will be reviewed on Surgical Assessment Unit at 0800. A provisional list order will be agreed. Any additional cases added to the list will be discussed with the anaesthetist and Emergency theatre team leader.
7.5.2 Booking of Plastic trauma:
During the working week the decision to treat the patient as day case or in patient will be decided at the 0800 plastic trauma meeting. There will be designated theatre capacity for day case plastic trauma in the Heavitree day case theatres. In patients will be added to the emergency theatre list. Once the decision to treat is made the patient is added to the electronic plastics whiteboard highlighting suitability for surgery in Heavitree or in the emergency theatre. If it is agreed the patient needs to be treated in the emergency theatre the plastics team will book the patient onto the emergency list by completing the emergency theatre booking form.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 13 of 41
7.5.3 Booking of Trauma Emergencies: All cases potentially requiring trauma theatre 8 are uploaded to the trauma whiteboard. This is the responsibility of the admitting junior orthopaedic doctor or the trauma coordinator.
At 5pm the consultant orthopaedic surgeon covering fracture clinic reviews the whiteboard and makes a provisional plan for operating the next day.
At this point the default first patient (Golden Case) on the list is identified and this patient will automatically be called to theatre in time for a timely start the next day unless this instruction is countermanded following the admission of a higher priority case overnight. This decision will be made by the on call consultant surgeon.
All cases listed on the whiteboard as ‘ready for theatre’ are starved from midnight.
All patients waiting at home for surgery are told to ring Durbin Ward at 8.45 the following morning for an update on planned operation date.
The surgical team meet every morning to review the planned workload (trauma meeting) and confirm which cases are planned for that day. These cases are identified by sequential numbering on the trauma whiteboard.
The anaesthetic team will review all numbered patients on the list by midday.
The trauma theatre team brief at 8.30 and confirm with the operating surgeon which cases are to be undertaken during the day and the anticipated list order. Pre-operative patients being reviewed through fracture clinic will be listed on the whiteboard under the heading ‘not ready’. When the decision is made in clinic to operate the patients are assigned to the ‘ready for theatre’ group and managed as above.
At 1200 the Trauma theatre and anaesthetic and surgeon consultant will review the list confirming whether the list achievable, cancelling any cases that cannot be done and confirm patients for the evening list.
7.5.4 Booking considerations for Trauma surgery:
Specialty trauma should be avoided in Th8 unless this is the most appropriate place to perform the surgery. Firebreak lists should be in use by all teams to facilitate this.
Ten cases deemed as ‘ready’ on the trauma list should trigger a discussion between On-call consultant, Trauma Lead and Management about cancellation of elective cases to increase capacity.
Two or more patients with neck of femur fractures on the Th8 list who do not have a plan for surgery within their breach time should trigger a discussion between On- call consultant, Trauma Lead and Management about cancellation of elective cases to increase capacity.
7.6 Patient Cancellations: Patients will not be cancelled unless clinically appropriate, making cancellation the exception and reportable to Cluster Manager/Cluster Support Manager. On the day cancellations of individual patients will continue to be monitored. Where there is any plan to cancel due to non-medical reason, i.e. No Intensive Care Unit (ICU) bed will be escalated to Divisional Business Manager/Divisional Manager.
7.7 Cancellations:
When patients have been cancelled or cancel themselves in weeks 1 and 2 a replacement should be found to utilise the list where possible. All patients added at this late stage should be notified to the theatre schedulers.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 14 of 41
7.8 Intensive Care Unit (ICU) cases:
7.8.1 Provisionally booking ICU cases:
ICU cases can only be provisionally booked as we cannot guarantee the availability of the bed. To reduce the high risk of cancellations of patients who require an ICU bed on the day of surgery there is a booking limit of two elective patients per day. Staff booking these cases should review the ICU booking list before scheduling these patients. In situations where more than two cases are booked the following should take place:
Anaesthetic review
Cardiopulmonary Exercise Testing (CPEX) testing
Discussion between surgeons to prioritise case. Consideration should be given for having a reserve patient on hold if there are no ICU beds available.
7.9 Process of cancellations:
7.9.1 Bed pressures / Capacity problems
On call Cluster manager and Site Practitioners to liaise with the Cluster Manager of the specialty for the reason for cancellation
Specialty Cluster Managers to assess which patients could be cancelled based on clinical urgency, target times and number of previous cancellations, and discuss with Surgeon to come to an agreement that’s safe for the patient
Discuss with the Theatre Coordinator, Surgeon and Anaesthetist
Ensure the Theatre team have a list that reflects the case urgency and target times
Cluster Manager to ensure any patient cancelled is spoken to by the surgeon or the Cluster manager,
The admission wards are aware of the situation and revised list order
Cluster Manager to ensure the patient is re-booked at the earliest opportunity or within 28 days
Site Management to be updated with the names of the cancelled patients.
7.9.2 Availability of ICU beds
Theatre Coordinator, Surgeon and Anaesthetist to check availability of an ICU bed at 08:00 hours on the day of surgery
Consider changing the order of the list to meet the time when a bed will be available
ICU to liaise with Site Management to ensure patients who are fit enough to go to a ward are able to have a bed in the correct ward
ICU to negotiate the time frames with the planned admissions
If ICU Consultant and Site Management confirm NO beds are available, escalate to Cluster Manager, Divisional Business Manager and Executives
Site Manager to communicate to the Surgeon, Anaesthetist and the Theatre Coordinator the outcome
Surgeon and Cluster Manager to tell the patient if possible with another date for their procedure.
7.9.3 Cancellations for other reasons, i.e. previous operations taking longer than
expected overriding emergency, safety of the department due to other lists overrunning, Recovery full
Theatre Team Leader to liaise with the Theatre Coordinator, Surgeon, Anaesthetist and Recovery to discuss options
Consider utilising another theatre
Consider using the emergency theatre
Inform Cluster Manager if in hours
Liaise with the admission ward, Surgeon to speak to patient preferably with a new date for the procedure

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 15 of 41
Inform the theatre team and Recovery of out come
If out of hours ensure the Cluster Manager and the specialty secretary are aware the next day.
7.10 Trauma Theatre Scheduling
All cases potentially requiring trauma theatre are uploaded to the trauma whiteboard. This is the responsibility of the admitting junior orthopaedic doctor or the trauma coordinator.
At 5pm the consultant orthopaedic surgeon covering fracture clinic reviews the whiteboard and makes a provisional plan for operating the next day.
At this point the default first patient on the list is identified and this patient will automatically be called to theatre in time for a timely start the next day unless this instruction is countermanded following the admission of a higher priority case overnight.
All cases listed on the whiteboard as ‘ready for theatre’ are starved from midnight.
All patients waiting at home for surgery are told to ring Durbin Ward at 8.45 the following morning for an update on planned operation date.
The surgical team meet every morning to review the planned workload (trauma meeting) and confirm which cases are planned for that day. These cases are identified by sequential numbering on the trauma whiteboard.
The trauma theatre team brief at 8.30 and confirm with the operating surgeon which cases are to be undertaken during the day and the anticipated list order.
Pre-operative patients being reviewed through fracture clinic will be listed on the whiteboard under the heading ‘not ready’. When the decision is made in clinic to operate the patients are assigned to the ‘ready for theatre’ group and managed as above.
8. PRE-OPERATIVE ASSESSMENT
8.1 The pre-operative patient pathway should include a preparation for surgery
appointment. This may be as a one-stop following the decision to treat, a booked appointment or a telephone assessment.
8.2 Preparation for surgery should include:
An assessment of the patient’s fitness for surgery and anaesthesia with the aim of ensuring that the patient is as fit as possible on the day of surgery.
Social and psychological preparation, explanation of the likely course of their admission and the preparations the patient will need to make for their discharge home.
Advice about starvation times and cessation or continuation of medicines.
An opportunity for the patient to ask questions.
Completion of risk assessment paperwork and scoring, e.g. thromboembolism, nutrition, falls, EPRAT (Exeter Pressure Risk Assessment Tool).
Infection control screening.
8.3 All patients should have been pre-assessed. If a patient has not been pre-assessed, the anaesthetist and surgeon should determine whether there is adequate information available to proceed with the operation.
8.4 Patients who have not attended a preparation for surgery appointment must be assessed on the day of surgery. This may be done by the nurses on the admission ward, but requires input from the surgical team when patients have complex health problems or are planned inpatients.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 16 of 41
8.5 All patients wishing to refuse any blood product administration (including but not limited to Jehovah’s Witnesses) must be identified at the pre-operative assessment visit and the surgeon and anaesthetist notified. A consent form for refusal of blood should then be attached to the anaesthetic record in anticipation of its completion by patient, anaesthetist and surgeon on admission. It is then the responsibility of the surgeon and anaesthetist to ensure this consent form is completed and available for verification during Sign In and Time Out.
9. WARD PREPARATION 9.1 Privacy and Dignity
9.1.1 Patients for an elective procedure should be admitted to a designated area that affords them privacy and dignity in accordance with that outlined in the Trust’s Privacy, Dignity and Compassion Policy.
9.2 Preoperative screening and testing for pregnancy in adults
9.2.1 It is nationally recognised that incidents of patients undergoing a planned surgical procedure without having a documented pregnancy check in the preoperative period could result in a spontaneous abortion after the procedure.
9.2.2 Since 2012, the Trust has reported four incidents of undetected preoperative
pregnancy following surgical intervention. The common features with these incidents was the failure to systematically check for pregnancy; the failure to report to the surgeon a patient who had refused testing; and finally, a failure to robustly document the status in the patient’s operative record.
9.2.3 Robust assessment and informed consent to test for pregnancy in women of child bearing age will confirm unsuspected pregnancy, at which point the risks and benefits of the surgery can be discussed with the patient. Surgery may be postponed or anaesthetic and/or surgical approaches modified if necessary. In emergency situations, confirmation of pregnancy should not delay treatment.
9.3 Trust position on pregnancy testing
9.3.1 Women of child bearing age, between menarche and menopause (who have not had a
hysterectomy), should be assessed regarding pregnancy status. National Institute for Health and Care Excellence (NICE) guidance does not specify typical age ranges for women of child bearing age, but this is interpreted as being 12-55 years. This includes women who have had a sterilisation and women whose partners have had a vasectomy.
9.3.2 It may be useful to preface the conversation with the patient to include the following:
“We ask these questions of all females regardless of their personal circumstance; please accept my apologies in advance if you feel that this does not apply to you.”
9.3.3 We should then ask the patient:
“I need to ask you if you could possibly be pregnant. Are you agreeable that we exclude pregnancy by undertaking a urine test today?”
9.3.4 Informed consent to test the patient’s urine for pregnancy should include simple verbal
information explaining why the test is necessary and include the following:
Unrecognised pregnancy in female surgical patients is not uncommon and easily detected.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 17 of 41
There are risks of disruption to an undetected pregnancy following surgery and anaesthesia. The nature of this risk will depend on the surgery and gestation of the pregnancy.
That it is our policy that we ask patients for their informed consent to test.
The test result will be available to the female immediately.
9.4 Patients who decline to be tested 9.4.1 The Trust recognises the sensitivities of counselling patients about the likelihood of
pregnancy and it is the patient’s right to decline to be tested. In the event of this, the nurse should gain a gentle understanding of the reason for refusal and inform the patient’s surgeon. The surgeon must then make a decision as to whether to counsel the patient further, proceed with or cancel the surgical procedure. All decisions and outcomes should be fully documented in the patient’s medical records and Sign Out from the ward. The patient will be requested to sign the Sign Out documentation as a record of the informed consent to proceed with surgery in the absence of a definitive test. This is described using a decision tree in Appendix 4.
9.5 In the event of an unexpected positive test
9.5.1 In the event of an unexpected positive test result, the nurse should seek support from
the senior nurse in charge of the ward or admission unit. The preliminary result should be given to the patient in private with sensitivity towards the nature of the information given. The nurse must consider the appropriateness of other persons present when this information is provided.
9.5.2 The nurse should inform the patient’s surgeon immediately and request a senior
member of the surgical team attend the patient. The surgical team should consider a repeat test using a blood sample. The surgical team should consider contacting the gynae/obstetric team to counsel the patient regarding any decision to proceed and/or to provide advice following the detection of an unexpected pregnancy.
9.5.3 In recognition of the sensitivity of counseling young people; any menstrual history and
pregnancy testing of patients under the age of 18 should be in consultation with and at the discretion of the child’s clinician and the senior nurse in charge of the Paediatric Department (see Checking Pregnancy Status Before Treatment for under 18s Procedure).
9.5.4 If surgery proceeds it is the surgeon’s responsibility to inform the anaesthetist and
theatre team. The patient should receive the leaflet, “Having an operation whilst pregnant” (Appendix 5). All discussions with the patient should be fully documented and a new written informed consent to treatment, including any new risks completed.
9.5.5 If surgery is cancelled, the surgeon should explain the next steps regarding the surgical
pathway with the patient. This should be documented in a follow-up letter to the General Practitioner. This decision will depend on the patient’s individual circumstances and the nature of the surgery required.
9.5.6 The patient should be advised to contact their General Practice at the earliest opportunity to ensure that she receives the right support and maternal care.
9.5.7 The patient should be offered a meal and drink prior to leaving the hospital. 9.6 Patients who are known to be pregnant (not maternity) and listed for elective or
emergency surgery

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 18 of 41
9.6.1 Occasionally, there are times when the benefits of surgery outweigh the risks, for example when emergency surgery is required or when a woman develops a condition that is considered to be a threat to her life if surgery is postponed until after delivery. In such circumstances, and if time permits, the patient should receive the leaflet “Having an operation whilst pregnant” which fully explains the risks to the mother and foetus in such circumstances.
9.7 Infection Control Status
9.7.1 The Ward Preparation section must document any patient alert in relation to infection control, e.g. infection control status, including Meticillin-Resistant Staphylococcus Aureus (MRSA). If yes, ward staff must telephone theatres to advise them of the alert.
9.8 Drug Charts and Medication
9.8.1 Patient alerts need to be documented, e.g. allergies. In addition, the Drug Chart must be checked to ensure that all regular medications have been given prior to leaving the ward. If a patient is noted to have taken any anticoagulant or antiplatelet drugs outside of the guideline the anaesthetist and surgeon are to be notified. Current antiplatelet drugs are aspirin, clopidogrel, dipyridamole, prasugrel, ticagrelor, and current anticoagulants are warfarin, phenindione, acenocoumarol, dabigatran, rivaroxaban, apixaban and fondaparinux. Further guidance is available on the Preparation for Surgery clinical guidelines pages on HUB.
9.8.2 Drug charts should have all regular preoperative medications prescribed prior to the
patient leaving the ward. It is not necessary to prescribe routine post-operative analgesia for elective admissions.
9.9 Radiological Procedures
9.9.1 Patients for interventional radiological procedures will require completion of the Radiology Interventional Procedures Checklist. Patient preparation for the procedure should begin on the inpatient ward with a handover to the Radiology ward after completion of the first section of the Checklist with the exception of patients undergoing EndoVascular Aneurysm Repair (EVAR) which follows the surgical pathway.
10. PATIENT MARKING
10.1 Pre-operative marking has a significant role in correct site surgery, including operating on the correct side of the patient and/or the correct anatomical location or level such as the correct finger on the correct hand.
10.2 Staff should be alert to the potential of children, and others, to self-mark.
10.3 Who is responsible for marking?
The site must be marked by the person performing the procedure or suitably trained deputy who will be present in the operating theatre/radiology/endoscopy suite at the time of the patient’s procedure. The intended site of incision or site of insertion should be unambiguous. Non-operative sites should not be marked.
10.4 When to mark
Marking must occur prior to the patient leaving the ward/daycase unit or other setting (i.e. before Sign Out from Ward).
Marking must take place before a sedative pre-medication.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 19 of 41
10.5 How to mark
Information from the medical notes and/or images should be used to confirm the intended surgical site and side.
An indelible marker pen must be used.
The mark should consist of an arrow that extends to, or near to, the incision site and remain visible after the application of skin preparation.
It is desirable that the mark should also remain visible after the application of theatre drapes.
10.6 Where/what to mark
For digits on the hand and foot the mark must extend to the correct specific digit. Similarly for lesions and levels of the spines.
For eyes, the mark must be sited above the correct eye.
For facial lesions a dot must be placed adjacent to those intended for excision.
Multiple skin lesions must be marked as per facial lesions, or marked with an arrow, where that form of marking is considered to be more appropriate.
The site of anaesthetic block must be confirmed in the anaesthetic room, but not marked as this could cause confusion.
10.7 Involvement of others in marking
Wherever possible, pre-operative marking must take place with the patient involved, awake and aware.
In the case of children, parents should be involved in the process of marking.
Family members/significant others should be involved wherever possible and especially in the case of incapacitated or vulnerable adults.
10.8 Exceptions to marking
Emergency surgery – where a delay in surgery to facilitate marking endangers a patient’s safety, a surgeon may choose to proceed at risk. This decision should be documented in the patient’s theatre notes.
Teeth and mucous membranes.
Cases of bilateral simultaneous surgery such as tonsillectomy, squint surgery, laparoscopic sterilisation (excluding bilateral grommets which should be marked on the ear, visible after draping).
Situations where laterality of surgery needs to be confirmed following examination under anaesthesia or exploration in theatre.
Certain cases performed via Endoscopy, such as cystoscopy and bronchoscopy.
Certain cases where laterality is not an issue as only single organ, e.g. caesarean section, hysterectomy, colon surgery or gastrectomy.
Interventional cases for which the catheter/instrument site is not pre-determined.
If the site is traumatic.
Where intra-procedural imaging for localisation will be used.
Patient’s refusal.
10.9 Patient refusal of marking
If a patient refuses pre-operative skin marking staff must:
Document the patient’s request in the nursing and medical notes.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 20 of 41
Complete the Surgical Safety Checklist, but clearly state patient refuses marking.
Verbally hand over the lack of marking during Sign In to the anaesthetic room and Time Out.
Side and site must be confirmed and verified using reliable documentation (e.g. imaging, notes, consent form) at Time Out.
The surgeon should consider the risks and benefits of proceeding.
10.10 Documentation
Upon Sign Out from ward section, the registered nurse should sign to confirm that the mark is present and visible or where the patient has declined marking, annotate the Checklist to indicate this.
11. SIGN OUT FROM WARD – PROCESS
Where anaesthetic input is required, the patient must be seen by an anaesthetist/ anaesthetic practitioner prior to leaving the ward.
Sign Out must be undertaken by a registered nurse (or practitioners with signed off competency – see Section 22) on all surgical wards, Creedy, AMU, Endoscopy and Bramble; for the remaining medical wards, Sign Out will be undertaken in conjunction with a trained member of theatre staff.
Patient identity should be confirmed by asking the patient and checking their identification against the (ID) bands in situ, and against the patient notes in line with the Trust’s Patient Identification Policy.
Consent form should be checked to ensure correct patient ID label.
The surgical site mark should be checked against the consent form and the notes to confirm it is correctly located.
If the site is not marked and the planned procedure does not preclude marking (see list of exceptions in Section 10.8, the patient must not leave the ward. The surgeon or nominated deputy should be contacted to attend and mark the site.
Where a patient has specific requirements (e.g. learning disabilities/dementia/ acquired brain injury) and are unable to advocate for themselves or do not have capacity, it may be appropriate for a family member or carer to accompany the patient to theatre.
Additional general patient information must be clearly documented, e.g. are there any alerts on the inside cover of the Buff notes such as prostatic stent, pacemaker, etc., implants, disabilities, communication issues, etc. and whether patient identified on ward as ‘at risk’ of pressure ulcer EPRAT (>one red box).
In extreme circumstances, where clinical need dictates, these checks may not be completed in order to facilitate urgent treatment of the patient (e.g. ruptured aortic aneurysm). All efforts must be made to confirm patient ID, allergies and blood type.
12. FIVE STEPS TO SAFE SURGERY
The five steps process includes Team Briefing, Sign In, Time Out, Sign Out and Debriefing. The minimum requirements for these processes are described in Sections 12 to 17. The policy recognises and supports specialty-specific additions to the minimum requirements as agreed through the specialty governance process.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 21 of 41
12.1 TEAM BRIEFING (STEP ONE) 12.1.1 Through root cause analysis of adverse events it has been identified that deficits in
‘non-technical’ skills such as poor communication, lack of situational awareness and ineffective teamwork were attributable to 60-80% of cases (Kohn et al, 2000).
The surgeon is responsible for ensuring that Team Briefing occurs prior to commencing the intervention on the first patient.
If new members of the team arrive, they need to be updated with information discussed at Team Briefing.
The team leader is responsible for leading the Team Briefing and should use the Briefing Checklist to ensure that the items listed below have been appropriately discussed. The completed Briefing Checklist must be stored in the red binder in the Anaesthetic Room and this will be used to provide assurance that all relevant items have been discussed between the team in preparation for carrying out the list.
All team members should be present with the exception of the patient escort who is to be acknowledged, but should remain in the anaesthetic room with the patient.
For patients with complex needs or specific requirements, consideration should be given to the patient escort attending Team Briefing so as to be able to communicate relevant issues.
All non-essential activity is to cease to enable staff to listen and concentrate.
Content (using the Briefing Checklist):
1. Have all team members introduced themselves by name and role?
2. Are there any changes to the published operating list?
3. How are specimens taken to be managed?
4. Is the theatre adequately staffed and are any changes expected?
5. Please confirm any equipment or implants that will be required.
6. Are the anaesthetic machines checked and ready for use?
7. Do we expect significant blood loss or any transfusion requirements?
8. Are there any patient allergies?
9. Are there any patient infection control issues?
10. Are there any specific anaesthetic concerns?
11. Are there any concerns about laterality / marking? (e.g. internal organs: it should be stated that laterality is unclear, but expecting “X” side.)
12. What is the plan for patient warming and glycaemic control?
Any patient who refuses blood or blood products should be highlighted during Team Briefing and completion of the Consent Form for Refusal of Blood confirmed. This consent form will then be checked as part of the safe surgery checks during Sign In and Time Out.
ICU/Recovery issues – to be identified and fed back as appropriate by the team leader.
All pertinent investigation results must be available prior to sending for patients.
12.2 List Order
12.2.1 Best practice is for the entire theatre team to know the operating list order at the beginning of the theatre session and that this list order is “fixed”. Local evidence tells us that changing the theatre list order has the potential for miscommunication. Therefore we should always minimise any potential for list changes in advance through careful planning and communications.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 22 of 41
12.2.2 However, it is also recognised that there are a number of very good, clinical reasons why a list order should change. Having the ability to do this ensures that patients are not cancelled, that they receive timely surgery and that they are operated on in the right order. Such examples include (but not exclusively):
When a patient’s international normalised ratio (INR) returns from the laboratory post briefing and is raised.
When blood or blood products are not ready.
When a patient has not followed starvation instruction.
When there is a clinical priority than should take precedence over another patient.
12.2.3 Having agreed exceptions to this “best practice” should not detract from our commitment to knowing everything possible about the patients and list order at Team Briefing. We must however ensure that the communication about any changes are deliberate, clear and understood by all. Should the order need to change, the theatre team leader MUST undertake a “mini briefing” so that all changes are agreed and understood.
12.3 Emergency Theatres
12.3.1 Comprehensive Team Briefing using the standard Briefing Checklist should occur at the following times:
Prior to the start of the morning theatre session
Following commencement of the night shift
If a case is scheduled involving a different surgical team, a “Safety Pause” should be undertaken prior to commencing the intervention on this patient.
A Safety Pause should also be utilised when any emergency case is added into an elective list.
13. SIGN IN TO ANAESTHETIC/ PROCEDURE ROOM (STEP TWO)
Content from Ward Sign Out should be reviewed prior to commencing Sign In.
Sign In should be a two-person check. Whilst the anaesthetist retains overall responsibility for ensuring this check is completed and may wish to lead the process, the check can be undertaken by the ODP/ PA(A) and theatre assistant.
There should be no interruptions during completion of the Sign In to the Anaesthetic/Procedure room.
If any aspect of the Checklist cannot be completed or if any member of staff has concerns regarding the safety to proceed then the patient should not be anaesthetised until all issues are resolved.
The practitioner checking in the patient must sign the bottom of the form to confirm that all checks have taken place and that all information has been verified and is correct.
13.1 Anaesthetic Equipment check
The practitioner leading the Sign In must confirm by ticking the box, and by signing the Sign In to Anaesthetic Room, to confirm that the anaesthetic equipment check has been completed.
13.2 Confirmation of Patient Identity
This should take place in the anaesthetic room, or if the patient goes straight to the operating or procedure room, must take place before they are anaesthetised.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 23 of 41
If the patient is incapable of personally participating in the verification process due to specific requirements and no authorised representative is present, the member from the preceding location (who carried out the Sign Out from ward) must act as the patient’s representative for verification.
The patient must be asked:
o Full name o Date of birth
o What procedure they are having
o Site of procedure
This information should be confirmed and be consistent with the patient’s ID band, medical records, consent form and theatre operating list.
Any patient identified at Briefing as refusing blood or blood products should have their Consent Form for Refusal of Blood checked with the patient during Sign In and confirmation sought that this refusal stands.
In addition to the above list, additional checks will be undertaken for obstetric, cataract and interventional radiology patients in accordance with their specialty- specific Surgical Safety Checklists.
13.3 Confirmation of Site Mark
The surgical site mark should be checked against reliable documentation to confirm it is correctly located and still legible.
If the site is not marked and the planned procedure does not preclude marking (see list of exceptions in Section 10.8) the surgeon must confirm the operation site using the consent form and the notes then mark the site as per Sections 10.3 to 10.7.
In the event of marking occurring in the anaesthetic room, an incident form must be completed and the event discussed with all staff involved in signing the patient out from the ward and into the anaesthetic room.
13.4 Presence of surgeon
Prior to induction of anaesthesia the Team Leader must confirm that the surgeon is present in the building.
14. REGIONAL ANAESTHESIA
The anaesthetist is responsible for confirming the correct site for any local anaesthetic nerve block
Immediately prior to commencing any unilateral regional/local technique the anaesthetist must undertake a verbal Stop Before you Block check (Royal College of Anaesthetists, 2016) with the ODP. This check includes:
o Consent form – confirming correct surgery site/side
o Patient mark – confirming correct surgery/limb/side
If the check cannot be completed, then the anaesthetist must confirm any discrepancy with the surgeon prior to placing the block.
15. TIME OUT (STEP THREE)
Time Out must occur as close to knife-to-skin as practicably possible.
After Time Out has taken place, the operating surgeon must not leave the theatre prior to the procedure taking place.
The surgeon has overall responsibility for ensuring Time Out is performed.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 24 of 41
Time Out must be performed by the whole team with a minimum of surgeon, scrub nurse, anaesthetist and ODP/practitioner (or whoever signed the patient into the anaesthetic room) using the consent form.
When Time Out is taking place, “Active Listening” must be observed and distractions must be avoided unless absolutely essential. All staff must stop all other activity and ‘pause’ to conduct a final verbal verification.
Any staff new to the theatre time since the Team Briefing must be introduced.
The team must agree the following:
o New team members have been introduced
o Presence of the correct patient
o Confirmation of correct procedure
o Correct site and side marked
o Imaging is present, correct and properly labelled
o What potential problems may arise and critical surgical steps
o Allergies
o The correct antibiotics have been given after giving consideration to IC status
o A final equipment/sterility check has been made
o Thrombo-embolic precautions
o Whether cross-matched blood is available.
The refusal of blood or blood products by any patient should be confirmed during Time Out and the completed Consent Form for Refusal of Blood should be included as part of the Time Out check.
For obstetric, cataract and interventional radiology patients, issues discussed in Time Out will vary from the above in accordance with the agreed specialty-specific checklists (see Appendix 1).
For laterality of surgery: a verbalised description of intended laterality for internal organs must be provided by the surgeon. If the surgeon’s expectations are in any way at odds with other documentation (e.g. consent form, theatre list and imaging) the team must stop and check that site, operation and side are verified and agreed by all to be correct.
If any aspect of the Checklist is non-compliant or there are any concerns raised about patient safety, the team must stop and verify that all information is correct before proceeding.
Compliance with the Time Out process must be documented on the Checklist whilst the check is undertaken by the delegated member of the operating team and recorded on PLATO.
If during the procedure subsequent interventions involving laterality are felt to be necessary, e.g. insertion of chest drain, a safety pause where side of insertion is confirmed by the surgical team should be undertaken prior to commencing the additional procedure.
In the event of a case involving two surgical teams, e.g. Head & Neck and Plastics, if one team is not present in theatre later in the case, a second Time Out must take place as close to the second knife to skin as possible.
16. SIGN OUT FROM THEATRE (STEP FOUR)
16.1 Sign Out is to be completed on all patients at the end of surgery and before the patient is woken from general anaesthesia. A verbal check should be recorded on the Sign Out section of the Checklist whilst the check is undertaken. Sign out includes:
Name and recording of the procedure with reference to the operating list.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 25 of 41
Confirmation of instrument counts (e.g. swabs, throatpacks, sharps).
Confirmation of how specimens should be processed in accordance with the Trust’s Specimen Labelling Procedure and the Theatres Specimen Handling in Theatre Suites Policy and Procedure.
Any clinically significant blood loss.
Key concerns for recovery and the ward for ongoing management of the patient including antimicrobials.
Verification of DVT prophylaxis prescription.
Confirmation that all cannulae have been identified and adequately flushed (as per NHS/PSA/D/2017/006 Confirming removal or flushing of lines and cannulae after procedures).
16.2 Previous patient notes/labels must be removed from theatre before the next patient arrives in theatre.
16.3 In the event of missing swabs or instrumentation, the actions taken to locate and resolve the situation must be clearly documented in the Care Plan and this occurrence must also be reported via Datix, the Trust’s incident reporting system. See Theatre Guidelines, Section 4.9.
16.4 If post-operative transfer to Intensive Care is required, Sign Out must also confirm that all necessary transfer equipment is available and minimum standards of monitoring can be maintained throughout the transfer.
16.5 If post-operative antimicrobials are indicated, the plan should be documented on the Operation Note under post-operative care (agents and duration; specific advice such as “Discuss with Microbiology” or “Chase (specified) cultures” and appropriate course prescribed onto the drug chart with an indication and duration. This is the responsibility of the operating surgeon who is a proxy for/is the consultant. It is the responsibility of the ward nursing staff and junior doctors to ensure the plan is implemented via the drug chart.
16.6 Before transfer, the anaesthetist should be satisfied that the Recovery area is adequately staffed and that staff are competent and able to take responsibility for the patient. If this cannot be assured, the anaesthetist should stay with the patient, either in the operating theatre or Recovery area, until the patient is fit to return to the ward. The anaesthetist must hand over the care of the patient to Recovery practitioners that are assessed as competent.
17. THEATRE TEAM DEBRIEFING (STEP FIVE)
The scrub nurse or team leader is to remind the surgeon to perform Team Debriefing.
Team debriefing can be led by any member of the team. It should occur at a suitable time towards the end of the theatre session and before the surgeon leaves theatre, or where there have been significant changes to theatre staffing during a theatre session (e.g. during a Confidential Enquiry into Patient Deaths [CEPOD] list).
In circumstances when there have been no issues, a simple recognition that there were no issues is sufficient.
In circumstances where there have been issues that caused a problem, disrupted the list or caused harm (or had the potential to) there should be a full discussion involving all members of the theatre team who should not be distracted by other duties.
In this event an incident form should be completed on Datix.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 26 of 41
Debriefing documentation must be completed to record that (1) Debriefing has occurred and (2) if any actions required including equipment issues, these are noted and assigned to the relevant staff to resolve. Significant issues should be discussed at the theatres Comm Cell and the Debriefing process should identify a team member to add the item to the Comm Cell discussion board.
18. SURGICAL CHECKLIST FOR ORGAN DONATION FROM DEAD PATIENTS
18.1 Please see full details of procedures to follow in the case of organ donation for DBD and DCD are available on the Safe Surgery pages of HUB (see links in Appendix 1.)
18.2 Patients undergoing organ donation after brain death confirmation (now known as Donation after Brain Death, DBD)
18.2.1 These patients are effectively elective cases, and require the presence of both anaesthetist and surgeon. Their management should proceed exactly as for any live patient elective case. When the patient is sent for, the anaesthetist, theatre orderly and ICU nurse should perform the usual Sign Out from Ward prior to transport to theatre.
18.3 Patients undergoing organ donation after cardiac death (now known as Donation after Cardiac Death, DCD)
18.3.1 This procedure is an emergency procedure that is performed as quickly as possible, after death has occurred. Further, there will be no anaesthetist/intensivist present through the whole procedure, so some surgeons will use their own local checklist prior to starting the surgery. This is quite acceptable, and should be supported by the local hospital staff.
19. MANAGEMENT OF PATIENTS UNDERGOING SURGICAL PROCEDURES
REQUIRING LOCAL ANAESTHETIC ONLY
19.1 The pre-operative/operative procedures for patients requiring local anaesthetic only should follow the same process as for all other operative procedures, that is:
Pre-operative assessment.
Ward Preparation.
Sign Out from ward.
Sign In to the anaesthetic room/procedure room.
Time Out in theatre.
Sign Out from theatre.
19.2 Patients who come straight to theatre for a local anaesthetic procedure, bypassing the Anaesthetic Room, must have both Sign In and Time Out checks undertaken together, but, where the checks are duplicated, e.g. checking the patient’s name and date of birth, they should be completed only once.
19.3 Additionally, it is imperative that patients who have undergone their surgical procedure requiring local anaesthetic only will have any medical history that impacts on patient care communicated to the recovery team post-operatively. Therefore, all patients who have undergone their surgical procedure with local anaesthetic only and who have not required an anaesthetist will have a detailed medical history handover by the surgeon to the recovery team. The scrub nurse/ practitioner will hand over the procedure that the patient has undergone and communicate information which currently is standard practice for all surgical patients.
20. MANAGING PROCESS FAILURE
20.1 In the event of a wrong patient, wrong procedure or wrong site/side incident, this must be reported immediately to the Theatre Coordinator. The Divisional Management Team and Risk Management Department must be notified immediately and an incident form

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 27 of 41
completed, as per the Incident Reporting, Analysing, Investigating and Learning Policy and Procedures.
20.2 If the patient’s condition permits, an immediate plan to rectify the situation should be made by the consultant in charge of care. Wherever possible, the patient and the patient’s family should be involved in the management plan.
20.3 If performance failure is reported on Datix, this will be reviewed through Divisional governance structures. Persistent non-compliance will be escalated through the Trust’s disciplinary process (see Disciplinary and Appeals Policy).
21. THEATRE ENVIRONMENT
Staff should not enter the anaesthetic room or distract the anaesthetist whilst a patient is being anaesthetised; this is a high risk task-orientated process that requires complete concentration.
All staff in theatres have a duty of care to verbalise any concerns they may have about patient safety.
Wherever possible, changes to the theatre staff are to be kept to a minimum.
From the commencement of Sign In to Anaesthetic Room until the start of surgery, no non-essential team changes are to occur.
If any change of staff occurs during the day, the replacement personnel are to be introduced to the team by the nurse in charge of the theatre.
Theatres are restricted environments.
All staff entering theatre should wear scrubs (see Theatre Guidelines)
All mobile communications should only be used for essential/emergency communication.
Uncleanable equipment such as laptops should not be taken inside the patient zone in the operating theatre for infection control reasons (see Infection Control Prevention and Control Policy).
Only personnel involved with the procedure should be in theatre.
All staff to be mindful of potential damage to equipment, e.g. drink spillages.
Company representatives can attend theatre only at invitation of the surgeon or anaesthetist and following agreement from the theatre team leader (see Commercial Representatives Conduct Policy).
Tips on Theatre Etiquette sheet should be read by any visitor to theatres including students. These are available at Theatre reception.
22. TRAINING REQUIREMENTS
22.1 It is the responsibility of each Division to ensure that the appropriate staff are trained in, and adhere to, the standards of practice outlined in this Policy.
22.2 The following staff groups will be expected to read the training presentation available on the HUB (see Appendix 1 for links):
Operating surgeons, all grades including staff on honorary contracts
Anaesthetists, all grades.
All staff involved in interventional procedures: radiology, endoscopy, cardiology.
All relevant staff procedure rooms utilising a checklist identified in this Policy.
All theatre/recovery staff – registered and unregistered (nurses, ODPs, HCAs, TAs).

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 28 of 41
Senior nurses, ward matrons, preparation for surgery and all staff involved in completing the Ward Preparation and Ward Sign Out as designated by ward matrons.
22.3 These groups of staff will be expected to complete the learning available as a Powerpoint presentation on the HUB (see Appendix 1 for links), print off the final page and sign it as assurance that they have read and understood this Policy and their responsibilities within it. By completion of the training, staff verify that:
I understand my role with the Safe Surgery and Interventional Procedures Policy, and
I agree to work and communicate as part of a team and to speak out if I have any concerns about patient safety.
22.4 Band 3 and 4 practitioners undertaking Ward Sign Out must complete Ward Preparation and Ward Sign Out competency module prior to undertaking these duties.
23. ARCHIVING ARRANGEMENTS
The original of this policy will remain with the Governance and Patient Safety Lead, Surgical Services Division. An electronic copy will be maintained on the Trust Intranet, P – Policies (Trust wide) – S – Safe Surgery and Interventional Procedures Policy. Archived copies will be stored on the Trust's “archived policies” shared drive, and will be held indefinitely. A paper copy (where one exists) will be retained for 25 years.
24. AUDIT ARRANGEMENTS
24.1 A variety of quality audit tools have been developed (see audit tools listed in Appendix 1) for use in theatre settings and between 5 (minimum) and10 (maximum) audits will be carried out each month by trained auditors. The number of audits to be carried out will be agreed by the relevant specialty governance groups (e.g. Radiology, Endoscopy, Cardiology, etc). The number of audits for General, PEOC, CWH, WEEU and Community theatres will be kept under review by the Five Steps to Safe Surgery Audit Group and the Anaesthetics/Theatres Governance Group.
24.2 Objectives of the quality audit tool
1. To determine that the Five Steps are being performed
2. To ensure the quality of the safety checks performed and that sufficient time is allocated to each check with the full attention of the team
3. To ensure that any issues or concerns raised by the auditor or the theatre teams are actioned.
24.3 Required behaviours
1. Clear announcement of safety checks: A designated member of the team leads the team through the appropriate stage of the safety check (sign in, time out, sign out). The team member is observed to use the checklist and to clearly let the team know that the safety check is taking place.
2. Appropriate team responses: On announcement of the start of the safety check the team focus on the questions being asked. Any potential distractions such as music are eliminated. No disrespectful comments are made about the process.
3. Checklist read out accurately: The team utilise the appropriate checklist and follow its format accurately. There are no adaptations other than those agreed by the Trust for specialist areas.
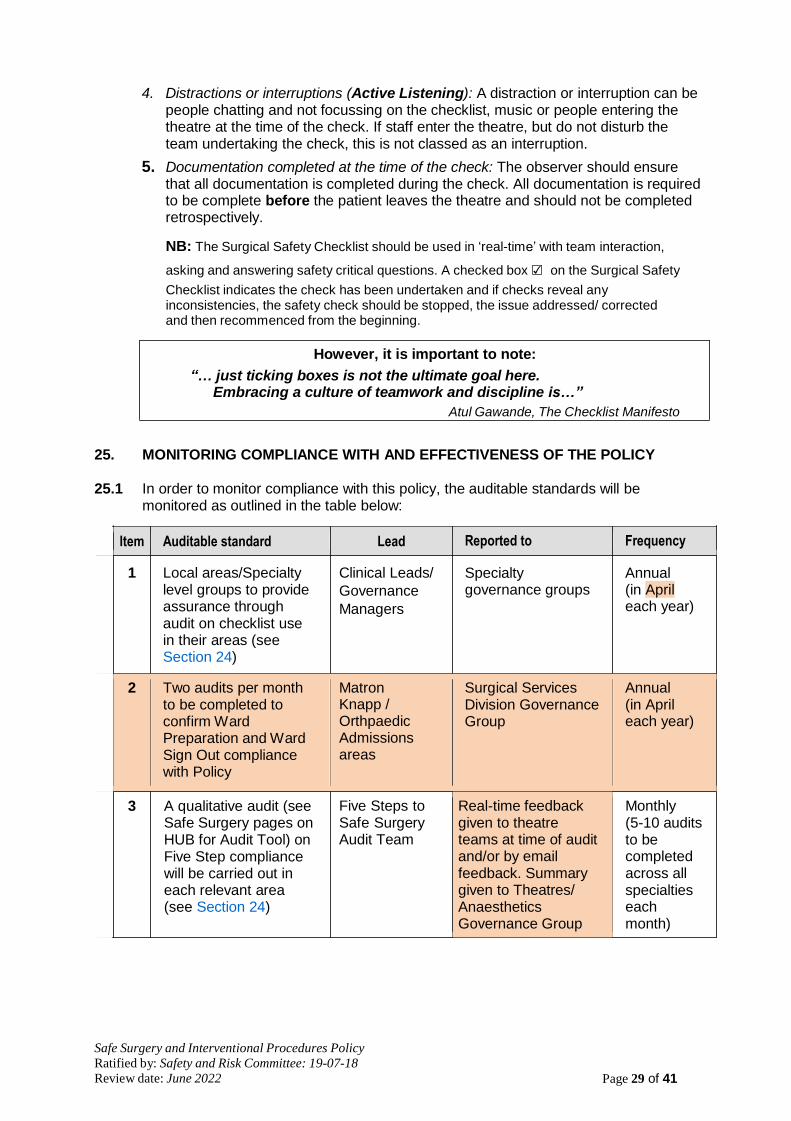
Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 29 of 41
4. Distractions or interruptions (Active Listening): A distraction or interruption can be people chatting and not focussing on the checklist, music or people entering the theatre at the time of the check. If staff enter the theatre, but do not disturb the team undertaking the check, this is not classed as an interruption.
5. Documentation completed at the time of the check: The observer should ensure that all documentation is completed during the check. All documentation is required to be complete before the patient leaves the theatre and should not be completed retrospectively.
NB: The Surgical Safety Checklist should be used in ‘real-time’ with team interaction,
asking and answering safety critical questions. A checked box ☑ on the Surgical Safety
Checklist indicates the check has been undertaken and if checks reveal any inconsistencies, the safety check should be stopped, the issue addressed/ corrected and then recommenced from the beginning.
However, it is important to note:
“… just ticking boxes is not the ultimate goal here. Embracing a culture of teamwork and discipline is…”
Atul Gawande, The Checklist Manifesto
25. MONITORING COMPLIANCE WITH AND EFFECTIVENESS OF THE POLICY 25.1 In order to monitor compliance with this policy, the auditable standards will be
monitored as outlined in the table below:
Item Auditable standard Lead Reported to Frequency
1 Local areas/Specialty level groups to provide assurance through audit on checklist use in their areas (see Section 24)
Clinical Leads/
Governance
Managers
Specialty governance groups
Annual (in April each year)
2 Two audits per month to be completed to confirm Ward Preparation and Ward Sign Out compliance with Policy
Matron Knapp / Orthpaedic Admissions areas
Surgical Services Division Governance Group
Annual (in April each year)
3 A qualitative audit (see Safe Surgery pages on HUB for Audit Tool) on Five Step compliance will be carried out in each relevant area (see Section 24)
Five Steps to Safe Surgery Audit Team
Real-time feedback given to theatre teams at time of audit and/or by email feedback. Summary given to Theatres/ Anaesthetics Governance Group
Monthly (5-10 audits to be completed across all specialties each month)

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 30 of 41
Item Auditable standard Lead Reported to Frequency
Radiology to undertake quarterly audits of 30 Interventional Radiology Checklists (10 obser- vational audits and 20 retrospective docu- mentation audits.
4 Training for new staff
will be included in Local Induction handbooks.
5 Annual Report encompassing 1-4 above will be written
Susannah Fulthorpe Superintendent for Special Procedures
Divisional Governance Managers
Lead Clinician for Patient Safety and Governance, Surgical Services Division
Diagnostics Governance Group
Divisional Governance Groups:
Surgical Services
Specialist Services
Medical Services
Safety and Risk Committee
Quarterly
Ongoing activity. Compliance reported to DGGs annually in April
Annually (in May)
24.2 Frequency
An Annual Report outlining compliance with this policy will be presented by the Lead Clinician for Patient Safety and Governance, Surgical Services Division to the Trust’s Safety and Risk Committee.
24.3 Undertaken by
Lead Clinician for Patient Safety and Governance, Surgical Services Division. 24.4 Dissemination of Results
A copy of the Annual Report will be presented at the Safety and Risk Committee which meets monthly.
24.5 Recommendations/Action Plans
Implementation of any recommendations and action plans will be monitored by the Safety and Risk Committee, which meets monthly.
24.6 Any barriers to implementation will be risk-assessed and added to the Trust Risk
Register. 24.7 Any changes in practice needed will be highlighted to Trust staff via the Governance
Managers’ cascade system.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 31 of 41
25. ASSOCIATED TRUST POLICIES
Commercial Representatives Conduct Policy Consent to Treatment and Examination Policy Disciplinary and Appeals Policy Identification of Patients Policy Incident Reporting, Analysing, Investigating and Learning Policy and Procedures Infection Control Prevention and Control Policy Policy for Patients who Refuse Blood Components or Products Exeter Clinical Laboratory’s Pathology Form and Specimen Labelling Procedure Checking Pregnancy Status Before Treatment for under 16s Procedure Privacy, Dignity and Compassion Policy Supporting Staff Involved in Adverse Events Theatre Guidelines Specimen Handling Procedures in Theatre
26. REFERENCES
NHS England: National Safety Standards for Invasive Procedures (NatSSIPs) 07-09-15
NHS/PSA/RE/2015/008 Supporting the introduction of the National Safety Standards for Invasive Procedures 14-09-15The Association of Anaesthetists of Great Britain & Ireland; The Obstetric Anaesthetists' Association Regional Anaesthesia UK. (2013). Regional anaesthesia and patients with abnormalities of coagulation. Anaesthesia 2013, 68, 966–972. Available at: http://onlinelibrary.wiley.com/doi/10.1111/anae.12359/abstract
NHS/PSA/D/2017/006 Confirming removal or flushing of lines and cannulae after procedures
Association for Perioperative Practice (AfPP) Standards and Recommendations for Safe Perioperative Practice, fourth edition, 2016.
NHS England (2013). The Never Events List - 2013/14 update. [online]. Available at: http://www.england.nhs.uk/wp-content/uploads/2013/12/nev-ev-list-1314-clar.pdf
Kohn LT, Corrigan J, Donaldson MS (2000). To err is human: building a safer health system. Institute of Medicine (US).
NHS Institute for Innovation and Improvement (2008). Just a routine operation: human factors in patient safety. Available at: http://patientsafety.health.org.uk/resources/just- routine-operation-human-factors-patient-safety
National Patient Safety Agency (2010). "How to Guide": Five Steps to Safer Surgery. London: NPSA. Available at: http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=93286
National Patient Safety Agency (2009). Alert: NPSA/2009/PSA002/U1, WHO Surgical Safety Checklist 27 January 2009.
National Patient Safety Agency (2005). Patient Safety Alert 06: Correct Site Surgery 2 March 2005.
Royal College of Anaesthetists (2016) Standards of Clinical Practice: Wrong Site Block. [web only]. Available at: http://www.rcoa.ac.uk/standards-of-clinical- practice/wrong-site-block [15-06-17]
Safe Anaesthesia Liaison Group (SALG) and Regional Anaesthesia UK (RAUK) (2010). Stop Before You Block. Available at: http://www.ra-uk.org/index.php/stop- before-you-block
World Health Organisation (WHO) (2009). WHO guidelines for safe surgery: safe surgery saves lives. Available at: http://www.who.int/patientsafety/safesurgery/tools_resources/9789241598552/en/

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 32 of 41
APPENDIX 1: SURGICAL SAFETY CHECKLISTS: LINKS TO BARCODED DOCUMENT LIBRARY
1. There are links below to all surgical safety checklists / documentation available on the Barcoded Document Library on HUB. These documents can be ordered in the usual way via EROS:
Surgical Safety Checklist – General
Surgical Safety Checklist – Cataract Surgery (contained in the Cataract Management
Plan
Surgical Safety Checklist – Maternity Specific
Surgical Safety Checklist – Radiology Interventional Procedures
Endoscopy Interventional Procedures Safety Checklist
Cardiology checklist (included in Cardiology Day case Documentation)
Electroconvulsive Therapy (ECT) Safety Checklist
Daycase Pain Procedures Checklist
Termination of Pregnancy
2. Links to other key documents or items previously included within the Safe Surgery and Interventional Procedures Policy (2012) are now available on the Safe Surgery pages of HUB as follows:
Briefing Checklist
Consent Form 5 - Consent to Surgical Treatment by Patient who Refuses to have a Blood Transfusion
Five Steps Quality Audit Tool (December 2016 for Surgical Safety Checklist)
Five Steps Quality Audit Tool (June 2018 for new Surgical Safety Checklist)
Five Steps Quality Audit Tool for Cataract Checklist (July 2018)
Five Steps Quality Audit Tool for Maternity Specific Checklist (July 2018)
Patient information leaflet, Having an operation when pregnant: A guide for the pregnant woman who requires surgery for a condition unrelated to their pregnancy – available on the Trust’s PIL database
Safety Pause Checklist (for use in CEPOD theatres)
List of procedures that will need to be covered by the Radiology Interventional Procedures Safety Checklist (previously Appendix 4-1 in the 2012 policy)
Training presentation for Ward-based and Preparation for Surgery staff
Training presentation for theatre-based staff and surgical teams
Training Sign-off Sheet
Tips on Theatre Etiquette (for visitors to theatres)

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 33 of 41
APPENDIX 2: LOCAL GUIDELINES REQUIRING DEVELOPMENT (LOCSSIPS)
The following is a list of safety checklists – variations on the Trust standard Surgical Safety Checklist – in use in procedure rooms, outpatients etc. Development of local guidelines to ensure adherence with the principles of NatSSIPs guidance are underway within the relevant specialties.
Anaesthetics/ICU: Nerve block catheters, Seldinger arterial lines, chest drain, central line, intubation (in progress)
Botox injections (in progress)
Outpatients: covering all invasive procedures for Colorectal, Breast, Plastics, ENT, Vascular (currently being piloted)
Cystoscopy and related procedures (in use)
Dermatology Surgical Safety Checklist – Dermatology (currently being approved)
Lumbar Puncture
Neonates: chest drain, vascular access, exchange transfusion, ommaya/ventricle tap
Ophthalmology : Laser Eye Procedures, invitreal injections, eyelid surgery (minor ops)
Oral Surgery; Dental extraction under sedation. Currently being piloted.
Paediatrics: PICC lines, lumbar puncture, Chest drains (in progress)
PCRM: Fertility Service: Oocyte Retrieval and Tesa Procedure Checklist (in use)
Radiotherapy: Brachytherapy, treatment applicators, fiducial marker placement
Renal interventional procedures: kidney biopsy, externalise PD (currently being approved)
Respiratory: Pleural Aspiration, bronchoscopy, pleuradhesis,
Thoracic drain
TRUS Biopsy Checklist (in use)
Vascular access: central line, PVC, Midline, PICC, tunnelled catheter (policies in place)
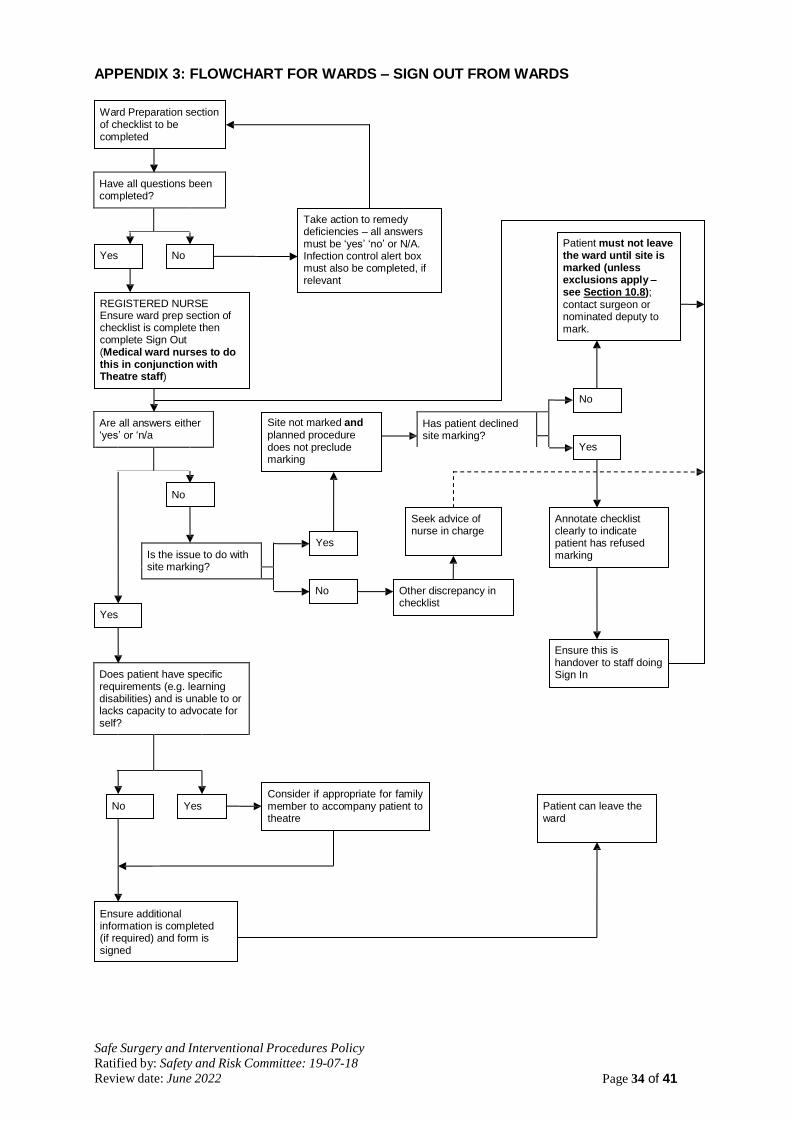
Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 34 of 41
Have all questions been completed?
Has patient declined site marking?
Are all answers either ‘yes’ or ‘n/a
Is the issue to do with site marking?
Does patient have specific requirements (e.g. learning disabilities) and is unable to or lacks capacity to advocate for self?
APPENDIX 3: FLOWCHART FOR WARDS – SIGN OUT FROM WARDS
Ward Preparation section of checklist to be completed
Yes No
Take action to remedy deficiencies – all answers must be ‘yes’ ‘no’ or N/A. Infection control alert box must also be completed, if relevant
Patient must not leave the ward until site is marked (unless exclusions apply – see Section 10.8);
REGISTERED NURSE Ensure ward prep section of checklist is complete then complete Sign Out (Medical ward nurses to do this in conjunction with Theatre staff)
contact surgeon or nominated deputy to mark.
No
Site not marked and planned procedure does not preclude marking
Yes
No
Yes
Seek advice of nurse in charge
Annotate checklist clearly to indicate patient has refused marking
Yes
No Other discrepancy in checklist
Ensure this is handover to staff doing Sign In
No Yes
Consider if appropriate for family member to accompany patient to theatre
Patient can leave the ward
Ensure additional information is completed (if required) and form is signed

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 35 of 41
APPENDIX 4: FLOWCHART OF MANAGEMENT RESPONSIBILITIES
Safety and Risk Committee
Overall Trust-wide respons- ibility for the development, review, implementation and monitoring of Policy
Medical Director
Lead Clinician for
Governance and Patient Safety, Surgical
Services
Reporting compliance monitoring results to the Safety and Risk Committee on behalf of the Medical Director
1. Responsible and accountable for ensuring that the standards of practice outlined in this Policy are maintained
DD and assured 2. Responsible for ensuring that monitoring systems are in
place to enable robust assurance of compliance with this Policy to be provided to the Medical Director and the Safety and Risk Committee
3. Responsible for identifying and resolving gaps in service provision which might adversely impact upon compliance
with this Policy within their Division
AMD
Responsible for ensuring medical staff receive guidance and training, understand the Policy and adopt the requirements within their practice
ADN
Responsible to ensuring nursing staff and other non-medical healthcare professionals receive guidance and training, understand the Policy and adopt the requirements within their practice
Line Managers / Supervisors
1. Responsible for ensuring Datix incident reports are completed for any deviation from the Policy
2. Responsible for ensuring all staff receive guidance and training, understand the Policy and adopt the requirements within their practice
Theatre Team
Denotes reporting relationship
Denotes expectation of joint working to achieve responsibilities

Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 36 of 41
APPENDIX 5: PATIENTS WHO DECLINE A PREGNANCY TEST - DECISION TREE
The Evidence
Between October 2003 and November 2009, the National Patient Safety Agency (NPSA) received 42 reports of patients undergoing a planned surgical procedure without having a documented pregnancy check in the preoperative period. In three cases there was a spontaneous abortion after the procedure (NPSA 2010).
The national data reported through the NRLS is likely to underestimate the actual numbers of patients who have a surgical intervention during the early stages of an unrecognised pregnancy. The available evidence suggests that the incidence of unrecognised pregnancy in women presenting for surgery is somewhere between 0.15% and 2.2%. This difference in populations may be related to the variation in socio- economic status and the transferability of such research should be made with some caution.
However, the continuation of unrecognised pregnancy and its associated harm following surgical procedure is certain without robust procedures to counsel, assess and detect pregnancy in all women of child bearing age undergoing both elective and emergency surgery. This is mandated through the National Patient Safety Agency Rapid Response Alert (NPSA 2010) and this is Trust policy.
Robust assessment and informed consent to test for pregnancy in women of child bearing age will confirm unsuspected pregnancy, at which point the risks and benefits of the surgery can be discussed with the patient. Surgery may be postponed or anaesthetic and/or surgical approaches modified if necessary. In emergency situations, confirmation of pregnancy should not delay treatment.
Safe Surgery and Interventional Procedures Policy

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 37 of 41
APPENDIX 6: SURGICAL NEVER EVENTS
1. INTRODUCTION
1.1 In the UK, a list of 8 Never Events was published by the NPSA (2009), expanded in 2012 to 25 Never Events; reviewed and finalised as 15 Never Events on 1 February 2018 (see revised Never Events List 2018). Never Events are defined as serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented. Surgical Never Events include wrong site surgery, wrong implants and retained instruments/swabs post operation, described in the following paragraphs.
2. WRONG SITE SURGERY
2.1 A surgical intervention performed on the wrong site (for example wrong knee, wrong eye, wrong patient, wrong limb, or wrong organ); the incident is detected at any time after the start of the operation and the patient requires further surgery, on the correct site, and/or may have complications following the wrong surgery.
This includes interventions that are considered to be surgical but may be done outside a surgical environment, e.g. wrong site block (including blocks for pain relief), biopsy, interventional radiology procedure, cardiology procedure, drain insertion and line insertion (eg peripherally inserted central catheter (PICC)/ Hickman lines). This also includes teeth extracted in error that are immediately re-implanted.
3. RETAINED FOREIGN OBJECT POST-OPERATION
A ‘foreign object’ includes any items subject to a formal counting/checking process at the start of the procedure and before its completion (such as for swabs, needles, instruments and guidewires) except where items are:
not subject to the formal counting/checking process are inserted any time before the procedure, with the intention of removing them during the procedure but they are not removed
subject to the counting/checking process are inserted during the procedure and then intentionally retained after its completion, with removal planned for a later time or date as clearly recorded in the patient’s notes
known to be missing before completion of the procedure and may be inside the patient (e.g. screw fragments, drill bits) but action to locate and/or retrieve them is impossible or more damaging than retention.
4. WRONG IMPLANT/PROSTHESIS
Placement of an implant/prosthesis different from that specified in the procedural plan, either before or during the procedure. The incident is detected any time after the implant/prosthesis is placed in the patient.
Excludes:
placed implant/prosthesis is intentionally different from that specified in the surgical plan, based on clinical judgement at the time of the procedure • specified implant/prosthesis is placed as planned but later found to be suboptimal 6 | > Never Events list 2018
implant/prosthesis is different from the one specified due to incorrect preprocedural measurements or incorrect interpretation of the preprocedural data – for example, wrong intraocular lens placed due to wrong biometry or using wrong dataset from correct biometry.
Includes:
implantation of an intrauterine contraceptive device different from the one in the procedural plan.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 38 of 41
5. NEVER EVENTS REPORTING PROCESS
5.1 All Never Events must be reported to the Trust’s Commissioners and will be the subject of a formal investigation using Root Cause Analysis methodology
5.2 Never Events should be reported following the Trust’s red escalation process as described in the Incident Reporting, Analysing, Investigating and Learning Policy and Procedures.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 39 of 41
APPENDIX 7: COMMUNICATION PLAN
COMMUNICATION PLAN The following action plan will be enacted once the document has gone live.
Staff groups that need to have knowledge of the strategy/policy
All surgeons including trainees, SCPs All anaesthetists including trainees, PA(A)s All staff working in theatres – on Wonford site and all community sites ADNs, Senior Nurses, Matrons Clinical Leads: Cardiology, Radiology, Endoscopy (via relevant Governance Managers)
The key changes if a revised policy/strategy
Review of policy to incorporate changes made as a result of NHS/PSA/D/2017/006 Confirming removal or flushing of lines and cannulae after procedures 09-11-17 together with feedback from stakeholders.
The key objectives This Policy mandates some key processes and behaviours applicable to all procedures within the hospital, such as the requirements for team work; to robustly confirm patients’ identity and the key details of a procedure before commencing. The aim is to prevent avoidable harm or death for patients undergoing surgery due to:
Insufficient preparation before an operation
Poor teamwork or communication
Failure to robustly confirm key information relating to patient or the procedure being undertaken
How new staff will be made aware of the policy and manager action
The requirement to read and understand this Policy is included in induction handbooks for relevant areas and is the responsibility of relevant senior management to ensure staff sign-off their compliance and understanding. This information is entered onto the ESR training record.
Specific Issues to be raised with staff
A summary of minor changes made has been included in the
newsletter Better Safe Than Sorry, May 2018
Training available to staff A training presentation is available on the HUB for staff to read in conjunction with the policy prior to sign off:
Training presentation for Ward-based and Preparation for Surgery staff
Training presentation for theatre-based staff and surgical teams
Changes to the 2018 Policy
Training Sign-off Sheet
Any other requirements No
Issues following Equality Impact Assessment
No negative impacts
Location of hard / electronic copy of the document etc.
A copy of the policy will be retained in each theatre suite. An electronic copy of the Policy is available on the Trust Intranet, P – Policies (Trust wide) – S – Safe Surgery and Interventional Procedures Policy. Archived copies will be stored on the Trust's “archived policies” shared drive, and will be held indefinitely.

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 40 of 41
APPENDIX 8: EQUALITY IMPACT ASSESSMENT TOOL
Name of document Safe Surgery and Interventional Procedures Policy
Division/Directorate and service area Anaesthetics, Surgical Services Division
Name, job title and contact details of
person completing the assessment
Mark Daugherty, Associate Medical Director, Surgical Services Division
Date completed:
15-05-18
The purpose of this tool is to:
identify the equality issues related to a policy, procedure or strategy
summarise the work done during the development of the document to reduce negative impacts or to maximise benefit
highlight unresolved issues with the policy/procedure/strategy which cannot be
removed but which will be monitored, and set out how this will be done.
1. What is the main purpose of this document?
To ensure that staff involved in the perioperative patient journey follow correct processes and procedures to ensure that the right procedure is performed on the right patient safely every time.
2. Who does it mainly affect? (Please insert an “x” as appropriate:)
Carers ☒ Staff ☒ Patients ☒ Other (please specify)
3. Who might the policy have a ‘differential’ effect on, considering the “protected
characteristics” below? (By differential we mean, for example that a policy may have a noticeably more positive or negative impact on a particular group e.g. it may be more beneficial for women than for men)
Please insert an “x” in the appropriate box (x)
Protected characteristic Relevant Not relevant
Age ☒ ☐
Disability ☒ ☐
Sex including: Transgender, and Pregnancy / Maternity ☒ ☐
Race ☐ ☒
Religion / belief ☒ ☐
Sexual orientation including:Marriage / Civil Partnership ☐ ☒
4. Apart from those with protected characteristics, which other groups in society might this document be particularly relevant to… (e.g. those affected by homelessness, bariatric patients, end of life patients, those with carers etc.)?
N/A

Safe Surgery and Interventional Procedures Policy Ratified by: Safety and Risk Committee: 19-07-18 Review date: June 2022 Page 41 of 41
5. Do you think the document meets our human rights obligations? ☒
Feel free to expand on any human rights considerations in question 6 below.
A quick guide to human rights:
Fairness – how have you made sure it treat everyone justly?
Respect – how have you made sure it respects everyone as a person?
Equality – how does it give everyone an equal chance to get whatever it is offering?
Dignity – have you made sure it treats everyone with dignity?
Autonomy – Does it enable people to make decisions for themselves?
6. Looking back at questions 3, 4 and 5, can you summarise what has been done during the production of this document and your consultation process to support our equality / human rights / inclusion commitments?
The Policy recognises the following areas of good practice and the consultation has included experts in CWH (re paediatrics and pregnancy issues) and the Trust’s equality advisor.
Good practice on age in that the Policy recognises the risks of children self- marking.
Staff fully briefed and aware of this possibility and appropriate checks are in place, including the involvement of parents.
Minimises risk of self- marking by children
Good practice on pregnancy / maternity as the Policy includes tests for unrecognised pregnancy
Pregnancy testing will be carried out on all females according to Section 9 of the Policy
Minimises risk of females undergoing anaesthetic/ surgery whilst pregnant
Good practice as regards disability
Specific requirements, communication needs and disability issues are communicated on Ward Sign Out (Section 9) and carers involved as required
Minimises risk of poor communication between ward and theatre teams in relation to disability or communication issues
If you have noted any ‘missed opportunities’, or perhaps noted that there remains some concern about a potentially negative impact please note this below and how this will be monitored/addressed.
“Protected characteristic”:
Age and pregnancy / maternity
Issue:
Children could self-mark and females including young girls could undergo surgery without having declared a potential for pregnancy
How is this going to be monitored/addressed in the future:
All incidents of non-compliance with this Policy are reported on Datix. Continuous quality audits are carried out to ensure all aspects of the Policy are completed.
Group that will be responsible for ensuring this is carried out:
Five Steps to Safe Surgery Audit Group Anaesthetics / Theatres Governance Group Safety and Risk Committee via the Annual Report