s7 ch33 occupational_toxicology
TRANSCRIPT
CHAPTER 33
OCCUPATIONAL TOXICOLOGY
Peter S. Thorne
ologically predictable latent interval between exposure and the ex-pression of disease. Third, diseases of occupational origin may bemultifactorial with personal or other environmental factors con-tributing to the disease process. Nevertheless, it has been shownrepeatedly that the dose of toxicant is a strong predictor of the like-lihood, severity, and type of effect.
WORKPLACES, EXPOSURES, ANDSTANDARDS
The Nature of the Work Force
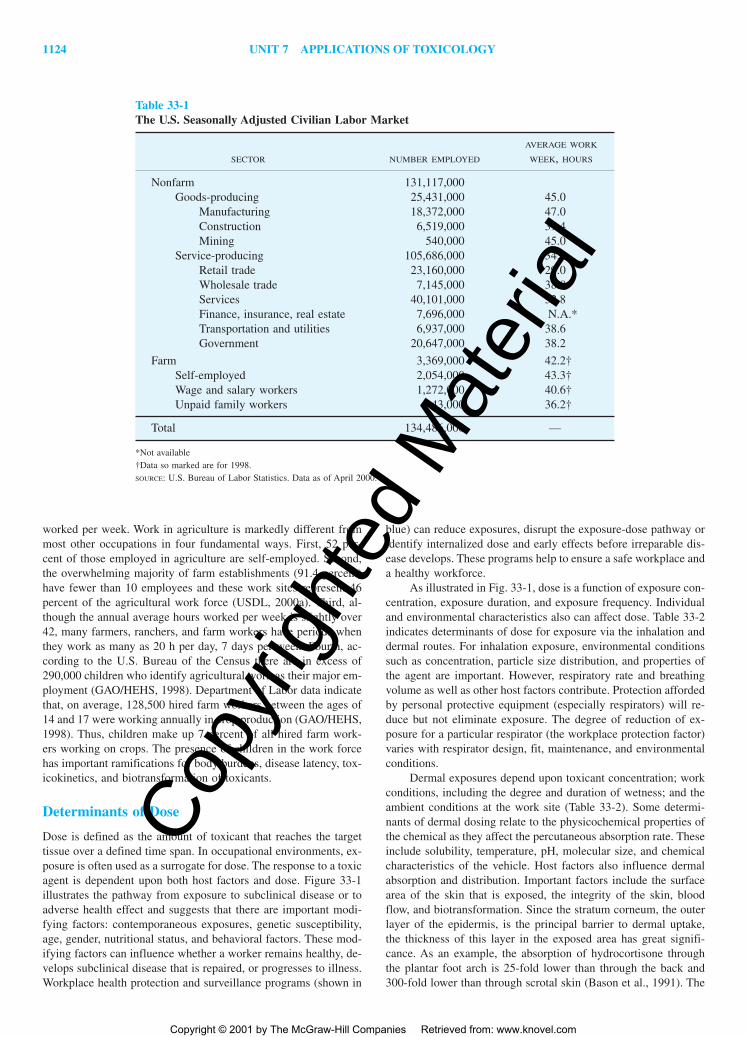
The demographics and distribution of the work force in industri-alized nations has undergone a progressive shift over the past threedecades away from jobs in heavy industry and toward jobs in theservice sector and high-technology industries. There are currently134.5 million people in the United States in the civilian, paid workforce (seasonally adjusted data). This represents 67.5 percent of allcitizens 16 years of age or older and is the highest proportion inhistory (USDL, 2000b). The 15 countries of the European Unionhave an estimated 155 million workers (European Union, 1998),and Japan has about 65 million. Table 33-1 shows the breakdownof employment in the United States. This illustrates that there areabout 25.4 million workers (18.9 percent) engaged in manufactur-ing, construction, and agriculture, occupations that have the po-tential for significant exposure to chemical and biological agents.Furthermore, there are occupations in the service sector, such asautomobile repair and employment in botanical gardens, that canalso include exposures to hazardous chemicals. Service-producingoccupations account for the majority (78.6 percent) of U.S. jobs.On average, weekly hours worked in service-sector jobs are lessthan in the goods-producing sector. Farm work employs an esti-mated 3.4 million workers 16 years of age and older and the U.S.Bureau of Labor Statistics has documented an average of 42.2 h
INTRODUCTION
WORKPLACES, EXPOSURES, AND STANDARDS
The Nature of the Work ForceDeterminants of DoseOccupational Exposure Limits
OCCUPATIONAL DISEASES
Routes of ExposureOccupational Respiratory DiseasesOther Occupational Diseases
TOXICOLOGIC EVALUATION OF OCCUPATIONALAGENTS
Evaluation of Occupational RisksEstablishing Causality
In Vitro AssaysAnimal Toxicology StudiesHuman Challenge StudiesCase ReportsEpidemiology Studies
Animal Toxicology Testing for EstablishingAcceptable Levels of Exposure
Worker Health SurveillanceLinkage of Animal Studies and Epidemiologic Studies
EXPOSURE MONITORING
Environmental Monitoring for Exposure AssessmentBiological Monitoring for Exposure Assessment
CONCLUSION
INTRODUCTION
For centuries the work environment has contributed significant riskof adverse health effects due to chemical and biological hazards.Early writings by Agricola (1494–1555) and Paracelsus (1492–1541) revealed the toxic nature of exposures in mining, smelting,and metallurgy. A systematic treatise by Ramazzini (1633–1714)described the hazards to miners, chemists, metal workers, tanners,pharmacists, grain sifters, stonecutters, sewage workers, and evencorpse bearers. Today we continue to be concerned with occupa-tional health and safety in these and other work environments. Al-though occupational settings are safer now than in the past, the lev-els of risk deemed acceptable have decreased and the recognitionof the causal link of exposures to chronic diseases or diseases withlong latencies has improved.
Occupational toxicology is the application of the principlesand methodology of toxicology toward chemical and biologicalhazards encountered at work. The objective of the occupationaltoxicologist is to prevent adverse health effects in workers arisingfrom their work environment. Since nonoccupational exposures canact as confounders or can increase the susceptibility of individualworkers, occupational toxicologists must evaluate the spectrum ofexposures of the work force under their consideration. Occupa-tional toxicology is a discipline that draws on occupational hy-giene, epidemiology, occupational medicine, and regulatory toxi-cology. The occupational toxicologist must have an intimateknowledge of the work environment and be able to recognize andprioritize exposure hazards. Since the work environment often pres-ents exposures to complex mixtures, the occupational toxicologistmust also recognize exposure combinations that are particularlyhazardous.
It is often difficult to establish a causal link between a worker’sillness and job. First, the clinical expressions of occupationally in-duced diseases are often indistinguishable from those arising fromnonoccupational causes. Second, there may be a protracted but bi-
1123
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1123
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
1124 UNIT 7 APPLICATIONS OF TOXICOLOGY
worked per week. Work in agriculture is markedly different frommost other occupations in four fundamental ways. First, 52 per-cent of those employed in agriculture are self-employed. Second,the overwhelming majority of farm establishments (91.4 percent)have fewer than 10 employees and these work sites represent 46percent of the agricultural work force (USDL, 2000a). Third, al-though the annual average hours worked per week is slightly over42, many farmers, ranchers, and farm workers have periods whenthey work as many as 20 h per day, 7 days per week. Fourth, ac-cording to the U.S. Bureau of the Census there are in excess of290,000 children who identify agricultural work as their major em-ployment (GAO/HEHS, 1998). Department of Labor data indicatethat, on average, 128,500 hired farm workers between the ages of14 and 17 were working annually in crop production (GAO/HEHS,1998). Thus, children make up 7 percent of all hired farm work-ers working on crops. The presence of children in the work forcehas important ramifications for body burdens, disease latency, tox-icokinetics, and biotransformation of toxicants.
Determinants of Dose
Dose is defined as the amount of toxicant that reaches the targettissue over a defined time span. In occupational environments, ex-posure is often used as a surrogate for dose. The response to a toxicagent is dependent upon both host factors and dose. Figure 33-1illustrates the pathway from exposure to subclinical disease or toadverse health effect and suggests that there are important modi-fying factors: contemporaneous exposures, genetic susceptibility,age, gender, nutritional status, and behavioral factors. These mod-ifying factors can influence whether a worker remains healthy, de-velops subclinical disease that is repaired, or progresses to illness.Workplace health protection and surveillance programs (shown in
blue) can reduce exposures, disrupt the exposure-dose pathway oridentify internalized dose and early effects before irreparable dis-ease develops. These programs help to ensure a safe workplace anda healthy workforce.
As illustrated in Fig. 33-1, dose is a function of exposure con-centration, exposure duration, and exposure frequency. Individualand environmental characteristics also can affect dose. Table 33-2indicates determinants of dose for exposure via the inhalation anddermal routes. For inhalation exposure, environmental conditionssuch as concentration, particle size distribution, and properties ofthe agent are important. However, respiratory rate and breathingvolume as well as other host factors contribute. Protection affordedby personal protective equipment (especially respirators) will re-duce but not eliminate exposure. The degree of reduction of ex-posure for a particular respirator (the workplace protection factor)varies with respirator design, fit, maintenance, and environmentalconditions.
Dermal exposures depend upon toxicant concentration; workconditions, including the degree and duration of wetness; and theambient conditions at the work site (Table 33-2). Some determi-nants of dermal dosing relate to the physicochemical properties ofthe chemical as they affect the percutaneous absorption rate. Theseinclude solubility, temperature, pH, molecular size, and chemicalcharacteristics of the vehicle. Host factors also influence dermalabsorption and distribution. Important factors include the surfacearea of the skin that is exposed, the integrity of the skin, bloodflow, and biotransformation. Since the stratum corneum, the outerlayer of the epidermis, is the principal barrier to dermal uptake,the thickness of this layer in the exposed area has great signifi-cance. As an example, the absorption of hydrocortisone throughthe plantar foot arch is 25-fold lower than through the back and300-fold lower than through scrotal skin (Bason et al., 1991). The
Table 33-1The U.S. Seasonally Adjusted Civilian Labor Market
AVERAGE WORK
SECTOR NUMBER EMPLOYED WEEK, HOURS
Nonfarm 131,117,000Goods-producing 25,431,000 45.0
Manufacturing 18,372,000 47.0Construction 6,519,000 39.4Mining 540,000 45.0
Service-producing 105,686,000 34.2Retail trade 23,160,000 29.0Wholesale trade 7,145,000 38.8Services 40,101,000 32.8Finance, insurance, real estate 7,696,000 N.A.*Transportation and utilities 6,937,000 38.6Government 20,647,000 38.2
Farm 3,369,000 42.2†Self-employed 2,054,000 43.3†Wage and salary workers 1,272,000 40.6†Unpaid family workers 43,000 36.2†
Total 134,486,000 —
*Not available†Data so marked are for 1998.SOURCE: U.S. Bureau of Labor Statistics. Data as of April 2000.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1124
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1125
use of protective gloves and clothing or aprons and the applicationof barrier creams can greatly reduce exposure. For maximal pro-tection, it is important that the material of construction of the glovebe tailored to the toxicant(s) of concern.
Occupational Exposure Limits
One of the roles of the occupational toxicologist is to contributedata to the process of establishing standards or determining the ap-propriateness of those standards. Workplace exposure limits existfor chemical, biological, and physical agents and are recommendedas guidelines or promulgated as standards in order to promoteworker health and safety. For chemical and biological agents, ex-posure limits are expressed as acceptable ambient concentrationlevels (occupational exposure limits) or as concentrations of a tox-icant, its metabolites, or a specific marker of its effects (biologicalexposure indices).
Occupational exposure limits (OELs) are established as stan-dards by regulatory agencies or as guidelines by research groupsor trade organizations. In the United States, the Occupational Safetyand Health Administration (OSHA) under the Department of La-bor promulgates legally enforceable standards known as permissi-ble exposure limits (PELs). These are designed to apply the bestscientific evidence to assure “to the extent feasible . . . that no em-ployee will suffer material impairment of health or functional ca-pacity” with regular exposure “for the period of his working life.”However, there are relatively few PELs compared to the numberof compounds to which workers are exposed and some of the ex-isting PELs do not reflect current knowledge. The National Insti-tute for Occupational Safety and Health (NIOSH), under the Cen-ters for Disease Control and Prevention, publishes recommendedexposure limits (RELs) that are more frequently updated and aregenerally more stringent than PELs. NIOSH also performs researchand disseminates information on workplace hazards and their pre-
vention. Most developed countries have governmental inspectorateagencies analogous to OSHA that are responsible for establishingand enforcing OELs. In some countries the insurance system alsoplays a significant role.
The American Conference of Governmental Industrial Hy-gienists (ACGIH) is a trade organization that annually publishesoccupational exposure limits for chemicals and for physical agents.
Figure 33-1. Pathway from exposure to disease, showing modifying factors and opportunities for interven-tion.
Table 33-2Determinants of Toxicant Dose
Inhalation exposureAirborne concentrationParticle size distributionRespiratory rateTidal volumeOther host factorsDuration of exposureChemical, physical, or biological properties of the
hazardous agentEffectiveness of personal protective devices
Dermal exposureConcentration in air, droplets, or solutionsDegree and duration of wetnessIntegrity of skinPercutaneous absorption rateRegion of skin exposedSurface area exposedPreexisting skin diseaseTemperature in the workplaceVehicle for the toxicantPresence of other chemicals on skin
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1125
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1126 UNIT 7 APPLICATIONS OF TOXICOLOGY
These take the form of threshold limit values (TLVs) and biolog-ical exposure indices (BEIs). They are frequently revisited andgenerally reflect current knowledge in occupational toxicology andindustrial hygiene. They are developed as guidelines and are notenforceable standards; however, many industries adopt TLVs andBEIs as internal occupational exposure limits. As stated by theACGIH, TLVs “refer to airborne concentrations of substances andrepresent conditions under which it is believed that nearly all work-ers may be repeatedly exposed day after day without adverse healtheffects” (ACGIH, 2000).
Three types of TLVs are suggested, depending on the timescale of adverse effects inducible by the toxicants. The time-weighted average TLV (TLV-TWA) is an occupational exposurelimit for exposures averaged over an 8-h day, 5-day week workregimen. These are generally applied to toxicants that exert theireffects over long periods. The short-term exposure limit (TLV-STEL) is an occupational exposure limit for a 15-min measurementperiod. The TLV-STEL should not be exceeded in any 15-minsampling window and there should be 60 min or more between ex-posures in this range. The ceiling limit (TLV-C) represents a con-centration that should never be exceeded. These usually are appliedto toxicants that cause acute effects (such as potent sensory irrita-tion) and for which real-time monitoring devices are available.Biological exposure indices are guidelines for biological monitor-ing and represent levels “most likely to be observed in specimenscollected from healthy workers who have been exposed to chemi-cals to the same extent as workers with inhalation exposure at theThreshold Limit Value” (ACGIH, 2000). BEIs are recommendedfor analysis of urine, blood, and exhaled air. While hair and fin-gernails are used in forensic toxicology, there are no BEIs for thesespecimens. The appendix lists ACGIH TLVs and OSHA PELs forover 800 toxicants.
It is important to recognize that occupational exposure lim-its do not correspond to exposure conditions devoid of health risk.The concept of acceptable exposure level must be understood as the level of exposure below which the probability of impairingthe health of the exposed workers is acceptable. The process of de-ciding what is an acceptable risk to occupational or environmentalhazards blends the scientific disciplines of exposure assessment andtoxicology with often vexing policy issues. Historically, acceptablerisk in a society is related to the general health of the populationand to a host of factors that influence how risks are perceived. Todetermine that the risks from an occupational hazard are acceptable,it is necessary to characterize the hazard, identify the potential diseases or adverse outcomes, and establish the relationship betweenexposure intensity or dose and the adverse health effects. If bio-logical markers of exposure or early reversible effects are identi-fied, this can aid in the risk-assessment process.
OCCUPATIONAL DISEASES
Routes of Exposure
Diseases arising in occupational environments involve exposureprimarily through inhalation, ingestion, or dermal absorption. Inthe vast majority of work environments, inhalation of toxicants isa primary concern, with dermal exposure also of importance. In-halation exposures can occur with gases, vapors, liquid aerosols,particulate aerosols, fumes and mixtures of these. Dermal expo-sures can arise from airborne materials as well as liquids splashedonto the skin, immersion exposures, or from material handling.
Additional exposure hazards exist for infectious agents.Exposures leading to occupational infections may arise through in-halation or ingestion of microorganisms but can also arise fromneedlesticks in health care workers or through insect bites amongfarmers, natural resource workers, and others who work outdoors.Additionally, poisonings from toxic plants or venomous animalscan occur through skin inoculation (e.g. zookeepers, horticultur-ists, or commercial skin divers).
Occupational Respiratory Diseases
Because of the importance of the inhalation route of exposure,many of the major occupational diseases affect the lung and air-ways. Table 33-3 presents a list of the major occupational diseasesand examples of agents that cause them. This is not intended to beall-inclusive. Rather it is meant to highlight what are historicallythe most important occupational diseases plus those that continueto be prevalent in the workplace. The toxicants listed are those forwhich there is a strong association with the disease or the mostconclusive data to support causality. Examples are shown for can-cer and for diseases of the lung and airways, heart, liver, kidney,skin, nervous system, immune system, and reproductive system.Several examples of occupational infectious diseases are also listedto highlight the fact that, in many work settings, infectious agentsmay constitute the major hazard and may coexist with chemicalhazards. Most of the occupational diseases listed in Table 33-3 areassociated with industrial chemicals. These are discussed in otherchapters throughout this book. Presented below is the prevalenceof some very important occupational lung diseases and a discus-sion of several common diseases in occupational toxicology thatare not described elsewhere.
Occupational lung diseases have been studied extensively andare largely responsible for the creation of the occupational regula-tory framework. Deaths due to occupational lung diseases such ascoal workers’ pneumoconiosis, silicosis, asbestosis, byssinosis, andoccupational asthma led to important legislation such as the U.S.Occupational Safety and Health Act (1970). These occupationallung diseases continue to have significant morbidity associated withthem. Table 33-4 lists the crude U.S. death rate and annual deathsand illustrates that while the death rates are fairly low, there arestill about 3600 deaths per year attributable to asbestos, silica, coaldust, and other pneumoconiotic dusts and 343 from hypersensitiv-ity pneumonitis. However, fatalities are just the tip of the iceberg.Hypersensitivity pneumonitis is rarely fatal but is often debilitat-ing. Moreover, there are 11,000 yearly hospital discharges relatedto cases of asbestosis and 13,500 for coal workers’ pneumoconio-sis. OSHA has compiled data on inspector-collected samples in avariety of work environments and 3.9 to 24.9 percent of theseexceed the PEL for asbestos, coal dust, silica, or cotton dust(Table 33-4).
Many of the diseases listed in Table 33-3 are known by othernames that refer to a particular occupation or agent. One exampleis hypersensitivity pneumonitis, an allergic lung disease marked byinterstitial lymphocytic pneumonitis and granulomatous lesions.Hypersensitivity pneumonitis is also known as extrinsic allergicalveolitis, farmer’s lung disease, bagassosis (sugar cane), humidi-fier fever, Japanese summer house fever, pigeon breeder’s lung, andmaple bark stripper’s lung, depending upon the occupational set-ting in which it arises. Although we often think of these as thesame disease, it is important to recognize that the exposures and
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1126
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1127
Table 33-3Examples of Occupational Diseases and the Toxicants That Cause Them
ORGAN SYSTEM OR
DISEASE GROUP DISEASE CAUSATIVE AGENT
Lung and airways Acute pulmonary edema, bronchiolitis Nitrogen oxides, phosgeneobliterans
Allergic rhinitis Pollens, fungal sporesAsphyxiation Carbon monoxide, hydrogen cyanide, inert gas dilutionAsthma Toluene diisocyanate, �-amylase, animal urine proteinsAsthma-like syndrome Swine barn environments, cotton dust, bioaerosols Bronchitis, pneumonitis Arsenic, chlorineChronic bronchitis Cotton dust, grain dust, welding fumesEmphysema Coal dust, cigarette smokeFibrotic lung disease Silica, asbestosHypersensitivity pneumonitis Thermophilic Bacteria, avian proteins, pyrethrum,
Penicillium, AspergillusMetal fume fever Zinc, copper, magnesiumMucous membrane irritation Hydrogen chloride, swine barn environmentsOrganic dust toxic syndrome “Moldy” silage, endotoxinUpper respiratory tract inflammation Endotoxin, peptidoglycan, glucans, viruses
Cancer Acute myelogenous leukemia Benzene, ethylene oxideBladder cancer Benzidine, 2-naphthylamine, 4-biphenylamineGastrointestinal cancers AsbestosHepatic hemangiosarcoma Vinyl chlorideHepatocellular carcinoma Aflatoxin, hepatitis B virusMesothelioma, lung carcinoma Asbestos, arsenic, radon, bis-chloro methyl etherSkin cancer Polycyclic aromatic hydrocarbons, ultraviolet irradiation
Skin Allergic contact dermatitis Natural rubber latex, isothiazolins, poison ivy, nickelChemical burns Sodium hydroxide, hydrogen fluorideChloracne TCDD,† polychlorinated biphenylsIrritant dermatitis Sodium dodecyl sulfate
Nervous system Cholinesterase inhibition Organophosphate insecticidesNeuronopathy Methyl mercuryParkinsonism Carbon monoxide, carbon disulfidePeripheral neuropathy N-hexane, trichloroethylene, acrylamide
Immune system Autoimmune disease Vinyl chloride, silicaHypersensitivity See entries for allergic rhinitis, asthma,
Hypersensitivity pneumonitis, allergic contact dermatitisImmunosuppression TCDD,† lead, mercury, pesticides
Renal disease Indirect renal failure Arsine, phosphine, trinitrophenolNephropathy Paraquat, 1,4-dichlorobenzene, mercuric chloride
Cardiovascular disease Arrhythmias Acetone, toluene, methylene chloride, trichloroethyleneAtherosclerosis Dinitrotoluene, carbon monoxideCoronary artery disease Carbon disulfideCor pulmonale BerylliumSystemic hypotension Nitroglycerine, ethylene glycol dinitrate
Liver disease Fatty liver (steatosis) Carbon tetrachloride, tolueneCirrhosis Arsenic, trichloroethyleneHepatocellular death dimethylformamide, TCDD†
Reproductive system Male Chlordecone (Kepone), dibromochloropropane, hexaneFemale Aniline, styreneBoth sexes Carbon disulfide, lead, vinyl chloride
(continued)
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1127
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1128 UNIT 7 APPLICATIONS OF TOXICOLOGY
physiologic responses they induce are complex and may differ inthe manifestation of the disease.
The U.S. Bureau of Labor Statistics tracks data for respira-tory conditions arising from exposure to toxic agents. These con-ditions include pneumonitis, pharyngitis, rhinitis, and acute lungcongestion. Table 33-5 shows data for rates and cases for 1995 byindustry division. These data are representative of values over the1990s and indicate 24,000 cases per year of respiratory conditionsattributed to toxic agents. The manufacturing and services indus-tries contributed 72 percent of these cases. Eight specific indus-tries that consistently have case rates exceeding 4.5 per 10,000workers are listed in the footnote to Table 33-5.
Toxic gas injuries are often characterized by leakage of bothfluid and osmotically active proteins from the vascular tissue intothe interstitium and airways. Important determinants of the sever-ity and location of injury are the concentration and water solubil-ity of the toxic gas or vapor. Anhydrous ammonia, with its ex-tremely high solubility, primarily damages the eyes, sinuses, andupper airways. The vapors combine with water in the tissue andform ammonium hydroxide, quickly producing liquefaction necro-sis. Chemicals with lower solubility, such as nitrogen dioxide, actmore on the distal airways and alveoli and take longer to inducetissue damage.
Occupational asthma may be defined as a “disease character-ized by a variable air flow limitation and/or airway hyper-respon-
siveness due to causes and conditions attributable to a particularoccupational environment and not to stimuli encountered outsidethe workplace” (Bernstein et al., 1999). The Third National Healthand Nutrition Examination Survey (NHANES III) has provideddata on the prevalence of asthma based upon usual industry andsmoking status (Table 33-6). These data indicate that asthma preva-lence is highest in health services, hospitals, and agriculture andlowest in mining. Interestingly, in some industries current smok-ers demonstrate the highest prevalence (e.g., rubber, plastics, andleather products), while in other industries the highest prevalenceis seen among former smokers (e.g., textile mill products, healthservices).
There are a variety of industries in which there is increasedrisk of developing work-related asthma. In chemical-based indus-tries, plastic and rubber polymer precursors, diisocyanates, reac-tive dyes, and acid anhydrides are recognized low-molecular-weight sensitizing compounds. Biocides and fungicides used inmetal fabrication and machining, custodial services, lawn and turfgrowing, and agriculture are also chemicals associated with occu-pational asthma. A number of metals can induce sensitization andasthma, including chromium, cobalt, nickel, platinum, and zinc.Many enzymes can pose significant risks for occupational asthma.Examples include �-amylase among bakery workers (Houba et al.,1996) and subtilisin, a protease used in laundry detergents (Flindt,1969; Sarlo et al., 2000; Thorne et al., 1986). The enzyme pro-
Infectious diseases* Arboviral encephalidites Alphavirus, Bunyavirus, FlavivirusAspergillosis Aspergillus niger, A. fumigatus, A. flavusCryptosporidiosis Cryptosporidium parvumHepatitis B Hepatitis B virusHistoplasmosis Histoplasma capsulatumLegionellosis Legionella pneumophilaLyme disease Borrelia burgdorferiPsittacosis Chlamydia psittaciTuberculosis Mycobacterium tuberculosis hominis
*For more on occupational infectious diseases, see Douwes et al., 2001.†TCDD � 2,3,7,8-tetrachlorodibenzo-p-dioxin.
Table 33-3 (continued)
ORGAN SYSTEM OR
DISEASE GROUP DISEASE CAUSATIVE AGENT
Table 33-4Crude U.S. Death Rates (1987–1996) and Deaths in 1996 Attributed to Selected Occupational Lung Diseases
DEATH RATE PER DEATHS INSPECTOR SAMPLES
DISEASE MILLION (1996) EXCEEDING PEL
Asbestosis 4.83 1,176 3.9%Coal workers pneumoconiosis 9.16 1,417 7.4%Silicosis 1.40 212 13.6%Byssinosis 0.07 9 24.9%Other pneumoconioses* 1.60 316Neoplasms of the pleura 2.62 510Hypersensitivity pneumonitis 0.17 343
*This includes aluminosis, berylliosis, stannosis, siderosis, and fibrosis from bauxite, graphite fibers, wollastonite, cadmium, portland cement, emery, kaolin, antimony, and mica.SOURCE: U.S. Bureau of Labor Statistics.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1128
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1129
duction industry has had to adopt strict environmental and processcontrols to reduce the risk of occupational asthma in their pro-duction facilities.
Those working with animals or animal products are at in-creased risk of developing occupational asthma. Animal handlers,processors, and laboratory technicians who work with animals can
become immunologically sensitized to urine or salivary proteins inmany vertebrates; proteins in bat guano and bird droppings; ani-mal dander; serum proteins in blood products; dust from horns,antlers, and tusks; or shells of crustaceans. Very high rates of sen-sitization can occur in shellfish processors (Glass et al., 1998).Arthropods such as insect larvae, cockroaches, mites, or weevilsare recognized inducers of work-related asthma. Plants and plantproducts (e.g., soy flour, spices, and coffee beans) can also causeasthma among workers. In a variety of occupations, exposure tofungi—especially of the genera Aspergillus, Penicillium, Rhizopus,Mucor, and Paecilomyces are associated with allergic rhinitis andasthma. These are especially important in sawmills, wood-chiphandling, and composting facilities (Duchaine et al., 2000; Eduardet al., 1992; Halpin et al., 1994). Apart from the contaminating mi-croorganisms, certain woods themselves produce chemical sensi-tizing agents. Examples include western red cedar, redwood, andsome tropical hardwoods. Asthma has emerged as a major occu-pational health concern among health care workers. In order to re-duce the risk of hepatitis B and other infectious diseases, healthcare workers have increasingly adopted the use of natural rubberlatex gloves for barrier protection. Proteins from the latex of therubber tree, Hevea braziliensis, are the sensitizing agents. Sevenof these high-molecular-weight proteins have now been character-ized as allergens. Many other plants of less commercial value pro-duce a similar milky fluid when cut and have similar sensitizingproperties.
Studies of asthma prevalence in occupational settings with ex-posure to low-molecular-weight agents have suggested prevalencerates of 8.3 to 11.0 percent for toluene diisocyanate (Becklake etal., 1999; Pepys et al., 1972a; Weill et al., 1975), 3.2 to 18 percentfor anhydrides (Venables et al., 1985; Wernfors et al., 1986), 4 per-cent for plicatic acid from western red cedar (Chan-Yeung et al.,1984), and 54 percent in a platinum refinery (Pepys et al., 1972b;
Table 33-5Reported Respiratory Conditions* in Private Industry due toToxic Agents, 1995 Data
RATE PER
INDUSTRY DIVISION† 10,000 CASES
Manufacturing 5.1 9,400Services 3.4 7,900Transportation and public 3.2 1,800
utilitiesFinance 2.3 1,400Construction 1.7 800Mining 1.5 100Agriculture 1.4 200Wholesale and retail sales 1.3 2,900
Total 3.0 24,000
*These conditions are pneumonitis, pharyngitis, rhinitis, and acute congestions dueto chemicals, dusts, gases, or fumes.
†These occur at rates consistently above 4.5 per 10,000 full-time workers in the fol-lowing industries: transportation equipment, primary metals industry, electron-ics fabrication, health services, rubber and plastic products industry, chemical in-dustry, food production, career gardening.
SOURCE: U.S. Bureau of Labor Statistics, Annual Report of Occupational Injuries andIllnesses.
Table 33-6 U.S. Asthma Prevalence by Usual Industry and Smoking Status for Selected Industry Codes
Asthma Prevalence, %
NON- FORMER CURRENT
INDUSTRY SMOKERS SMOKERS SMOKERS
Health services 6.3 25.8 14.8Hospitals 14.4 12.9 8.9Agriculture services, forestry, and 0.3 11.8 19.8
fishingTrucking service 3.8 8.9 13.6Paper products, printing 9.7 7.3 8.4Lumber and wood products 2.8 8.0 12.8Textile mill products 3.6 15.9 2.8Repair services 2.0 4.0 15.5Rubber, plastics, and leather 1.8 3.5 16.1
productsChemicals, petroleum, and coal 8.4 5.7 4.9
productsAgriculture production 4.5 9.3 2.6Metal industries 1.6 5.1 5.9Mining 1.5 1.3 0
SOURCE: National Health and Nutrition Examination Survey, NHANES III, 1996 (NIOSH, 2000).
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1129
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1130 UNIT 7 APPLICATIONS OF TOXICOLOGY
Venables et al., 1989). For high-molecular-weight allergens, preva-lence among shellfish processors was estimated at 21 to 26 per-cent (Cartier et al., 1984; Desjardin et al., 1995; Glass et al., 1998),11 to 44 percent among lab animal workers (Cullinan et al., 1994;Fuortes et al., 1996, 1997; Hollander et al., 1997), and 26 percentamong bakers exposed to wheat and alpha-amylase (Houba et al.,1996). Surveillance through the NIOSH SENSOR program inCalifornia, Massachusetts, Michigan, and New Jersey indicates thatof 1100 cases reported in 1993–1995, 19 percent were for work-aggravated asthma and 81 percent for new-onset asthma (NIOSH,2000).
Agricultural workers exposed to grain dust, cotton dust, or at-mospheres in swine or poultry confinement barns are at risk forthe development of an asthma-like syndrome. This syndrome is anacute nonallergic airway response characterized by self-limited in-flammation with neutrophilic infiltrates and increased proinflam-matory cytokines (TNF-�, IL-6, and IL-8), but it does not includepersistent airway hyperreactivity, as in occupational asthma(Schenker et al., 1998). Asthma-like syndrome includes cough,mild dyspnea, fever, malaise, and cross-shift declines in lungfunction. Endotoxin in combination with other inflammatorybioaerosols are the likely etiologic agents (Douwes et al., 2001;Schwartz et al., 1994; Schwartz et al., 1995).
Other Occupational Diseases
Occupational toxicants may induce diseases in a variety of sitesdistant from the lung or skin. These include tumors arising in theliver, bladder, gastrointestinal tract, or hematopoietic systemattributable to a variety of chemical classes. For further discus-sion of other occupational diseases and the toxicants listed inTable 33-3, the reader is referred to the relevant chapters in Units4 and 5 of this text.
Nervous system damage can be central, peripheral, or both. Itmay be acute, as with some organophosphate exposures, or chronic,as with organomercury poisoning or acrylamide-induced neuropa-thy. Injury affecting the immune system may arise from the im-munosuppressive effects of chemicals such as dioxins or toxic met-als. Many occupational diseases of the immune system occur dueto hypersensitivity leading to respiratory or dermal allergy or sys-temic hypersensitivity reactions. Autoimmune syndromes havebeen associated with occupational exposures to crystalline silicaand vinyl chloride.
Occupational diseases of the cardiovascular system includeatherosclerosis, a variety of arrhythmias, problems with coronaryblood supply, systemic hypotension, and cor pulmonale (right ven-tricular hypertrophy usually due to pulmonary hypertension as withchronic obstructive pulmonary disease). Liver diseases such as car-bon tetrachloride–induced fatty liver and hepatocellular death dueto toxic concentrations of acetaminophen have classically beenused to illustrate chemical mechanisms of cellular injury leadingto organ failure. These are thoroughly discussed in Chap. 13. Oc-cupational diseases of the reproductive system can be gender- andorgan-specific; but several toxicants—including carbon disulfide,lead, and vinyl chloride—may affect both sexes.
Exposures to infectious agents are a part of a variety of oc-cupations. Veterinarians, health care workers, and biomedical re-searchers studying infectious agents have exposures that are largelyknown, and infection control strategies can limit their risks. Forothers, such as farmers and foresters, specific risks may be less ob-
vious. Zoonotic diseases such as Q-fever, rabies, leptospirosis, andbrucellosis may affect abattoir workers, zookeepers, animal han-dlers, and veterinarians. Foresters, field biologists, and naturalresource workers who spend time in wooded areas experience tick-and mosquito-borne illnesses with increased frequency over thegeneral population. These illnesses include the arboviral en-cephalitides, Rocky Mountain spotted fever, Lyme disease, andehrlichiosis. Occupational infections may arise as a result of worksettings bringing people into close proximity with other people oranimals, thus facilitating the transmission of microorganisms. Oc-cupational infectious diseases attributable to the clustering of peo-ple affect workers in day care centers, schools, health care settings,correctional facilities, dormitories, military barracks, shelters forthe homeless, and so on. Industrial settings can place large num-bers of workers in a shared space, leading to increased transmis-sion of diseases. This is especially true for diseases with annualoutbreaks, such as influenza and Norwalk-like viruses. Exposuresto chemicals may increase the susceptibility of workers to infec-tion through irritation of mucosa or the pulmonary epithelium orthrough immunosuppression leading to impaired host defense.
Both industrial and nonindustrial indoor environments maypose occupational hazards due to the presence of chemical or bi-ological agents. With ineffective ventilation or decreased ventila-tion rates and increased utilization of synthetic building materials,there has been a rise in complaints associated with occupancy inbuildings. In some cases, workers in a problem building developspecific clinical conditions with recognized etiology. This is de-fined as building-related illness. In other cases, symptoms are non-specific and disappear when the worker leaves the problem build-ing. When this occurs with sufficient prevalence, it is termed sickbuilding syndrome. Volatile and semivolatile chemicals are releasedfrom manufacturing process materials, building materials, floorcoverings, furniture, cleaning products, biocides, and microorgan-isms. Office buildings and residences develop a complex ecologyconsisting of people, molds, mites, volatile organic compounds ofmicrobial and nonmicrobial origin, and sometimes plants, pets, andvermin (Thorne and Heederik, 1999b). An important example ofthis relationship involves skin cells, fungi, and house dust mites.People slough as much as 1 g of skin cells per person daily. Fungicolonize these skin cells in carpets, bedding, and upholstery, wherethey then serve as a food source for mites. The mites produce gas-tric enzymes to aid in the digestion of the fungi and skin cells, andthese enzymes are potent human allergens. Excrement from themites contains these allergenic molecules, which, when inhaled,complete the exposure pathway that can lead to allergy and asthma.Exposure to chemicals and biomolecules such as endotoxin mayenhance this process (Michel et al., 1996). In some cases the oc-cupied space of a building may be clean and dry, but local ampli-fication sites for molds may develop. These may arise in ventila-tion systems, utility closets, subfloors or basements that serve asreturn air plenums, or in local sites of water damage. Such sitescan become sources of microorganisms and aeroallergens ofsufficient volume to generate significant bioaerosol exposuresthroughout the environment. Airborne viruses, bacteria, and fungiare responsible for a variety of building-related illnesses arisingfrom organisms that are pathogenic to humans. Nonpathogenicmicroorganisms may induce symptoms or diseases through in-flammatory processes, by stimulating the immune response, or byreleasing noxious odors, allergenic compounds, or bioactive macro-molecules. These may combine with industrial chemicals released
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1130
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1131
into the air to create complex exposure environments. There aremany challenges to assessing exposures to microorganisms andchemicals in these environments (Thorne and Heederik, 1999a).
TOXICOLOGIC EVALUATION OFOCCUPATIONAL AGENTS
Evaluation of Occupational Risks
In most instances of prolonged exposure to chemicals, there is acontinuum between being healthy and being ill. The exposures mayimpart biochemical or functional changes that are without signs orsymptoms, subclinical changes, or more significant toxicity man-ifest as clinical disease. The health significance of the identifiedchanges resulting from exposure to a particular agent must be as-sessed in order to determine which are adverse. Following this as-sessment, one must consider the interindividual variability or sus-ceptibility factors that influence the risks. There is no one singledose-effect relationship but a distribution of responses. Therefore,to recommend an acceptable exposure level to an industrial chem-ical, one must attempt to define the risk associated with adverseeffects in the most sensitive populations exposed. It then remainsto decide what proportion of exposed subjects may still develop anadverse effect at the proposed acceptable exposure level. This ac-ceptable risk level will vary according to a value judgment of theseverity, permanence, and equality of the potential adverse effectsand the characteristics of the most susceptible population. Clearly,inhibition of an enzyme without functional consequences will beviewed as more acceptable than a more serious toxic effect, suchas teratogenicity leading to a congenital malformation.
Establishing Causality In complex occupational environmentsit may be difficult to establish a causal relationship between a toxicsubstance and a disease. For this reason a number of systematicapproaches have been devised to help define causation. In 1890Robert Koch proposed postulates for “proving” that a specific or-ganism caused a specific disease. T. M. Rivers extended this ap-proach to viruses in 1937. Sir Austin Bradford Hill suggested epi-demiologic criteria for assessing causality in 1965. These schemaand modern weight-of-evidence determination criteria were latercombined to suggest a set of postulates for the evaluation of evi-dence for disease agents in organic dust (Donham and Thorne,1994). A matrix was developed and is extended here to evaluatethe weight of evidence for a causal association between a toxicantand an occupational disease (Fig. 33-2). Evidence from well-conducted in vitro studies, animal studies, and human challengestudies, case reports, and epidemiologic investigations are evalu-ated with regard to data quality and clarity of evidence in supportof the establishment of causality. This evaluation is guided by sevencriteria (shown in blue). If a chemical were thoroughly studied inanimals, humans, and in vitro studies and produced clear and con-vincing evidence of an exposure-response relationship in controlledstudies that used appropriate models and relevant endpoints, thatwould constitute compelling evidence of a causal relationship be-tween that chemical and that disease. Figure 33-2 reminds us thata consortium of study types contributes data used for the evalua-tion of occupational hazards. These are discussed below.
To evaluate with some degree of confidence the level of ex-posure at which the risk of health impairment is acceptable, a bodyof toxicologic information is required. Five sources of data may beavailable to inform the occupational risk-assessment process.
Figure 33-2. Matrix for assessing the strength of an association between a toxicant and an occupational disease.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1131
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1132 UNIT 7 APPLICATIONS OF TOXICOLOGY
• In vitro assays • Animal toxicology studies• Human challenge studies • Case reports• Epidemiology studies
In Vitro Assays A number of useful in vitro assays have beendeveloped over the past several decades in order to provide screen-ing data and, in some cases, mechanistic insight without the needor expense of exposing animal or human subjects. While at thistime there are few validated methods to determine complex toxi-cologic responses such as immune hypersensitivity or peripheralneuropathy, there are validated and very useful screening assays.Notable examples are the Salmonella typhimurium reverse muta-tion assay, or Ames test, and the Corrositex assay for dermal cor-rosivity potential of chemicals (NIH-99-4495, 1999). In addition,quantitative structure-activity relationships can help suggest po-tential toxicologic effects for an unstudied compound if structurallysimilar compounds have been evaluated.
Animal Toxicology Studies Animal toxicology studies serve animportant function in terms of identifying adverse effects, provid-ing mechanistic data, establishing dose-response relationships, andaiding the process of establishing standards. Since animal studiescan be conducted before there is any human exposure, these stud-ies play an important role in hazard identification and preventionof human disease. There are numerous animal models for occupa-tional injury and illness; these are described throughout this text-book in the context of the affected organ system and the classes oftoxicants. Generation of animal toxicology data to predict healtheffects in workers is a central function of experimental toxicolo-gists. Toxicologic investigations using animals often serve to establish a tentative acceptable exposure level. Other important information that may also be derived from these investigations concerns the relationships between the metabolic handling of thechemical and its interactions with target molecules (mechanism ofaction), identification of methods for biological monitoring of ex-posure and early health effects, and of preexisting pathologic statesthat may increase susceptibility to the chemical. However, animaltesting can provide only an estimate of the toxicity of a chemicalfor humans. Animals do not always respond to chemical exposurethe same way humans do. For instance, there are very significantspecies and strain differences in responsiveness to aryl hydrocar-bon receptor agonists such as polychlorinated dibenzo-p-dioxins(Abnet et al., 1999; Whitlock et al., 1996; Wilson and Safe, 1998).In some instances, interspecies differences in metabolism or mech-anism of action cause certain chemicals to induce cancer in rodentsbut not in humans. One such example is kidney cancer, attributa-ble to the accumulation of a rat-specific protein (�2u-globulin) inproximal tubular cells, produced in male rats chronically exposedto unleaded gasoline (Hard et al., 1993). There are a few com-pounds for which animal models have not been found. As discussedfurther on, skin and internal cancers caused in humans by exces-sive oral exposure to inorganic arsenic have not been reproducedduring classic carcinogenicity studies in animals (ATSDR, 1993).
Human Challenge Studies Human challenge studies, or clinicalexposure studies, are a useful approach for verifying findings fromanimal toxicology studies in humans and for establishing whether
biotransformation pathways in the animal models represent thosein exposed humans. Human challenge studies help to establish bio-markers of exposure. For reversible conditions, they can be usefulfor testing therapeutic options. Extreme caution must be exercisedto ensure the safety of subjects. Idiosyncratic responses can causea subject to be exceptionally sensitive. For inhalation studies,equipment malfunction can result in overexposure. In the past 20years, there have been several serious injuries and fatalities asso-ciated with human challenge studies. These have been attributedto hypersensitivity reactions and generally used mock workplacesimulations without rigorous control and monitoring of exposures,as is the current standard of practice.
Case Reports When new toxicants or new combinations of tox-icants enter the workplace, a case or outbreak of cases can occur.These may be identified through workplace surveillance systemsor through workers associating their disease with workplace ex-posures. These may end up being reported as case reports or caseseries. NIOSH has a Health Hazard Evaluation (HHE) program inplace in which employees or their authorized representatives or em-ployers at a job site can request an investigation to evaluate a po-tentially hazardous situation. This program issues HHE Reports todisseminate information regarding the hazard. NIOSH also pub-lishes NIOSH Alerts, Criteria Documents, Special OccupationalHazard Reviews, Occupational Hazard Assessments, and CurrentIntelligence Bulletins. While useful for hazard identification, casereports and HHE Reports do not establish incidence or prevalenceof diseases associated with an occupational hazard.
Epidemiology Studies Epidemiology studies help to unravel theassociations between occupational diseases, exposures, and per-sonal risk factors. Several types of epidemiologic studies are usedto gather data on the association of workplace exposures withhuman disease. Cross-sectional studies compare disease prevalenceor health status between groups of workers classified according tojob title, work site, or exposure status. Cohort studies compare ex-posed workers versus unexposed workers either prospectively orretrospectively in order to associate the occurrence of disease withexposure. Since many occupational diseases have a long inductionperiod or occur only rarely, prospective cohort studies may requirea long time and need a large number of subjects to establish sig-nificant findings. Retrospective cohort studies can resolve the la-tency problem but require that relevant exposure data have beencollected over time. Exposure misclassification is frequently aproblem in retrospective studies. Case-control studies are usefulfor investigating rare diseases or diseases with long induction pe-riods. As the name suggests, case-control studies compare work-ers with disease to workers without disease with regard to their ex-posure intensity, frequency, and duration, plus other postulated riskfactors. In some instances where the exposure-disease relationshipis not understood, it may be difficult to identify an appropriate con-trol group
Animal Toxicology Testing forEstablishing Acceptable Levels ofExposure
It is evident that certainty as to the complete safety of a chemicalcan never be obtained whatever the extent of toxicologic investi-
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1132
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1133
gations performed on animals. Nevertheless, animal studies pro-vide valuable data from which to estimate the level of exposure atwhich the risk of health impairment is acceptable. Guidelines andprotocols for assessing experimentally the toxicologic hazards ofchemicals have been formulated by various national and interna-tional agencies. These tests include local and systemic acute toxi-city tests, tests of toxicity following repeated exposure, investiga-tions of metabolism and mechanism of action, short-term tests fordetecting potential mutagens and carcinogens, studies of effect onreproduction and of teratogenic activity, chronic studies to detectcarcinogenesis and other long-term effects, interaction studies, testsfor immunosuppression, and dermal and pulmonary hypersensitiv-ity tests. The need for performing these testing protocols shouldbe carefully evaluated for any occupational toxicant to which work-ers will be exposed. In selecting the studies most appropriate forsafety evaluation the toxicologist should be guided by an under-standing of the following:
• Physicochemical properties of the chemical• Potential for the generation of toxic derivatives when the chem-
ical is submitted to heat, pH changes, and UV light• Conditions of use• Type of exposure (continuous, intermittent, or incidental)• Degree of exposure
Toxicologic information already available on other chemicals withsimilar chemical structure and reactive chemical groups can sug-gest potential hazards and reactivity.
Conclusions drawn from any toxicologic investigation are use-ful only if the composition and physical state of the tested prepa-ration is known. This would include the nature and concentrationof impurities or degradation products, speciation of inorganic com-pounds, characterization of physical properties for inhaled materi-als, and characterization of the vehicle (if any). Sensitive and spe-cific methods of analysis of the chemical in solution, air, andbiological material also should be available. The assessment of thetoxicity of malathion in the 1970s illustrates this point. Malathionis an organophosphate insecticide normally with relatively low hu-man toxicity. This pesticide was responsible for a 1976 episode ofmass poisoning among malaria workers in Pakistan because thespecific product contained impurities (mainly isomalathion) capa-ble of inhibiting tissue and plasma carboxyesterases (Baker et al.,1978; Aldridge et al., 1979). The toxicity evaluation for malathionhad not anticipated isomalathion coexposure.
The duration of tests necessary to establish an acceptable levelfor occupational exposure is primarily a function of the type oftoxic action suspected. It is generally recognized that for system-ically acting chemicals, subacute and short-term toxicity studiesare usually insufficient for proposing OELs. Subacute and short-term toxicity tests are usually performed to find out whether thecompound exhibits immunotoxic properties and cumulative char-acteristics. They also aid in selection of the doses for long-term-exposure studies and the kind of tests that may be most informa-tive when applied during long-term exposures. A number of studieshave drawn attention to the fact that the reproductive system mayalso be the target organ of industrial chemicals (e.g., glycol ethers,styrene, lead, dibromochloropropane). Thus, studies designed to evaluate reproductive effects and teratogenicity should also be considered during routine toxicologic testing of occupational toxicants.
Information derived from exposure routes similar to those sustained by workers is clearly most relevant. For airborne pollu-tants, inhalation exposure studies provide the basic data on whichprovisional OELs are based. Experimental methodology is cer-tainly much more complicated for inhalation studies than for oraladministration experiments and requires more specialized equip-ment and expertise (Thorne, 2000). For example, in the case of exposure to an aerosol, particle size distribution must be evalu-ated and the degree of retention in the respiratory tract of the animal species under study should be established. Ideally, par-ticle size should be selected according to the deposition pattern of dry or liquid aerosols in the particular animal species used in order to represent human lung deposition with occupational exposures. Particle deposition and retention curves have been published for human, monkey, dog, guinea pig, rat, and mouse(Hsieh et al., 1999; Schlesinger, 1985). It also should be kept inmind that the concentration of the material in the air and the du-ration of exposure do not give a direct estimate of the dose, sinceretained dose is also dependent on the minute volume and the pro-portion of inhaled particles retained. Measurement of pulmonarydust retention following exposure to a radiolabeled or fluorescentlytagged test aerosol should be performed prior to conducting acute,subchronic, or chronic studies. This allows one to assess deposi-tion and determine whether the selected levels of exposure mayoverwhelm pulmonary clearance mechanisms (Lewis et al., 1989;Morrow, 1992).
The choice of what studies to perform using which routes ofadministration must be evaluated scientifically for each toxicant.Important considerations include its target sites and mechanism ofaction, metabolism, the nature of its adverse effects, and how work-ers are exposed to the toxicant. The morphologic, physiologic, andbiological parameters that are usually evaluated, either at regularintervals in the course of the exposure period or at its termination,are described in Units 4 and 5 of this text. Knowledge of the ab-sorption, distribution, biotransformation, and excretion of the chem-ical and its mechanism of action are of major interest. Investigationsthat can make use of specific physiologic or biochemical tests,based on knowledge of the principal target organ or function, pro-duce highly valuable information and increase confidence in theOEL derived from them.
Worker Health Surveillance
The primary objective of occupational toxicology is to prevent the development of occupational diseases. The monitoring of exposures to toxicants in the workplace may play an important role in detecting excessive exposures before the occurrence of sig-nificant biological disturbances and health impairment. A schemefor biological monitoring of exposure and of early biological effects is possible only when sufficient toxicologic information has been gathered from animal studies on the mechanism of actionand the metabolism of xenobiotics to which workers are exposed.When a new chemical is being used on a large scale, the carefulclinical surveillance of workers and monitoring of workplacesshould be instituted in order to address three aims: (1) to identifyoverexposure or adverse effects on the health of the workers and quickly intervene, (2) to evaluate the validity of a proposedoccupational exposure limit derived from animal experiments, and(3) to test the validity of a proposed method for a biological monitoring.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1133
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1134 UNIT 7 APPLICATIONS OF TOXICOLOGY
Evaluation of the validity of the proposed OEL derived fromanimal experiments through workplace surveillance is the majoraim, since “studies and observations on [humans] will always be the final basis for deciding whether [an OEL] set originally on the basis of tests on animals is, in fact, truly acceptable as one that will not produce any signs of intoxication” (Barnes,1963). This means that sensitive clinical, biochemical, physio-logic, or behavioral tests for detecting an adverse effect of a toxi-cant should ideally be performed on the workers concurrent withexposure assessment. It is helpful if human challenge studies orstudies on workers can include the same biomarkers as used inprior animal studies. The occupational toxicologist cannot relysolely on the diagnostic tools used in clinical medicine, as theywere established primarily to reveal advanced pathologic states andnot to detect early adverse effects at a stage when they are still re-versible. For example, the measurement of serum creatinine is stilla widely used clinical test for assessing renal integrity; yet it is known that the glomerular filtration rate of the kidney must be reduced by more than 50 percent before serum creatinine risessignificantly.
The main limitation of current OELs or BEIs is that some arebased on limited experimental data or clinical studies in which onlylate effects have been investigated and correlated with past expo-sure. Furthermore, several BEIs are derived from the study ofexternal-internal exposure relationships and not from relationshipsbetween internal dose and early adverse effects. The validity of anOEL is much stronger if it is based on the study of dose-responserelationships in which the dose is expressed in terms of the cu-mulative target dose and the monitored effect reflects a critical bi-ological event. However, it should be noted that for some chemi-cals and some adverse effects (e.g., induction of hypersensitivityand possibly genotoxic effects), the frequency of peak exposuremay be more important for health risk assessment than the inte-grated dose. For example, long-term low-level exposures to com-mercial enzymes rarely induce sensitization. However, a single ex-posure to a high concentration can produce hypersensitivity andoccupational asthma.
Epidemiologic studies designed to assess exposure-responserelationships can be carried out by using a variety of variables forassessing the exposure and health changes. Exposure may be char-acterized using a surrogate measure such as job classification, sen-iority, or via questionnaire or more directly through ambient or per-sonal exposure monitoring or measurement of the internalizeddose. Adverse effects may be expressed in terms of mortality, in-cidence or prevalence of clinical disease, irreversible or reversiblefunctional changes, or critical biological changes. It is evident thatthe assessment of the health risk resulting from exposure will havemore validity if it results from exposure-response studies in whichboth the target dose and the critical biological changes are moni-tored. Of course, the use of such parameters requires knowledgeof the fate of the chemical in the organism and its mechanism ofaction. However, this approach is more expensive than simpler epi-demiologic study designs and may result in a trade-off between so-phistication and study sample size.
Because early biomarkers of effect are subtle and individualvariations exist in the response to a chemical insult, results gener-ally require a statistical comparison between a group of exposedworkers and a similar group of workers without the exposure ofinterest. The group of unexposed workers should be matched onvariables such as age, race, gender, socioeconomic status, and
smoking habits. The importance of selecting a control group thatis well matched with the exposed group and that undergoes thesame standardized clinical, biological, or physiologic evaluation atthe same time as the exposed group must be emphasized. Com-parison with the general population is not valid because an em-ployed population is a highly selected group and may have a higherdegree of physical fitness. Since occupational epidemiologic stud-ies often last for several years, all methods of investigation—suchas questionnaires, instrumentation, and analytic techniques—mustbe validated and standardized before the start of the study. Thenumber of subjects under study should be chosen based on a sam-ple size calculation to be able to detect a difference between ex-posed and unexposed subjects (should there be a difference) andshould take into account labor turnover and those declining par-ticipation in any aspects of the study. If exposures are high enoughto induce an adverse effect, it is expected that these studies maypermit establishment of the relationship between integrated expo-sure (intensity � time) and frequency of abnormal results and, con-sequently, a redefinition of the OEL.
In cases where a surveillance program was not instituted be-fore the introduction of a new chemical, it is more difficult to es-tablish the efficacy of the OEL. In this situation, evaluation de-pends on retrospective cohort studies or case-control studies or oncross-sectional studies on workers who have already sustained ex-posure. Evaluation of a “no observed adverse effect level”(NOAEL) is difficult because information on past exposures is of-ten incomplete and frank effects are generally the focus of retro-spective or case-control studies. Provided that a satisfactory as-sessment of past exposure is possible, cross-sectional studies thatrely on preclinical signs of toxicity may, to a certain extent, over-come these difficulties. Whether or not clinical investigations areplanned from the introduction of a new chemical or process, it isessential to keep standardized records of occupational histories andexposure. The need may arise for mortality or case history studiesin order to answer an urgent question on a suspected risk.
Case reports of isolated overexposures resulting from specificincidents such as containment breaches, chemical spills, vessel orpipe ruptures can provide useful information. Although suchobservations are usually not helpful for determining the NOAELin humans, they may indicate whether human symptomatology issimilar to that found in animals and may suggest functional or bi-ological tests that might prove useful for routine monitoring of ex-posed workers.
Human challenge studies with occupational toxicants are usu-ally designed to answer very specific questions regarding rates ofuptake, biotransformation pathways, the time course of metaboliteexcretion during and after exposure, evaluation of the thresholdconcentration for sensory responses (odor, irritation of the nasalmucosa, etc.), and acute effects of toxicant exposure on percep-tion, vigilance, and function. For ethical reasons, such studies canbe undertaken only when the same results cannot be obtainedthrough other means and under circumstances in which the risk forvolunteers can reasonably be estimated as negligible.
In most cases, studies on human subjects encompass the col-lection of samples from the subjects or data obtained through in-teraction with the subjects. Since this often includes identifiableprivate information, subjects are rightfully concerned about issuesof confidentiality. The guiding principle is that the value of thestudy does not outweigh the rights of the subjects. U.S. and inter-national law requires that subjects must always have the right to
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1134
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1135
refuse participation and investigators must have written consentfrom a duly informed volunteer obtained without coercion.
Linkage of Animal Studies andEpidemiologic Studies
In the field of occupational toxicology, perhaps more than in otherareas of toxicology, close cooperation between those conductinganimal studies and studies of workers is essential for examiningrisks associated with overexposure to chemicals and other toxi-cants. A few examples will serve to illustrate the complementarityof these disciplines.
Several occupational carcinogens have been identified clearlythrough combined epidemiologic and experimental approaches(IARC, 1987). For example, the carcinogenicity of vinyl chloridewas first demonstrated in rats (Viola et al., 1971), and a few yearslater, epidemiologic studies confirmed the same carcinogenic riskfor humans (Creech and Johnson, 1974; Monson et al., 1974). Thisobservation stimulated several investigations on the metabolism ofvinyl chloride in animals and on its mutagenic activity in in vitrosystems. Identification of vinyl chloride metabolites led to the con-clusion that there is microsomal oxidation leading to the formationof an epoxide derivative, which acts as a proximate carcinogen(ATSDR, 1997). This finding triggered further studies on the bio-transformation of structurally related halogenated ethylenes, suchas vinyl bromide, vinylidene chloride, 1,2-dichloroethene, tri-chloroethylene, perchloroethylene (Bonse et al., 1975; Uehleke etal., 1977; Dekant et al., 1987). Comparison of their oncogenic ac-tivity in relation to their metabolism suggested that an interplaybetween the stability and reactivity in reaching the DNA target andreacting with it after being formed would determine their geno-toxic risk (Bolt, 1984). It is now recognized that vinyl chloride pro-duces DNA adducts by inducing the formation of an additional ringin adenine and cytosine on DNA molecules (Birner et al., 1993;NTP, 2000).
1,3-Butadiene is a known human carcinogen that is used inthe manufacture of synthetic rubber products. Experimental stud-ies in rats and mice demonstrated carcinogenicity, with mice be-ing particularly sensitive (NTP, 2000). Subsequent to these find-ings 1,3-butadiene was shown to follow the same metabolicpathway in humans as in rats and mice forming mutagenic and car-cinogenic epoxides. That led to cohort and case-control studies es-tablishing 1,3-butadiene as a human carcinogen (NTP, 2000). Re-cent studies have considered the relative importance of themetabolic pathway leading to formation of the reactive metabolite1,2-epoxy-3-butene, which reacts with hemoglobin to form 1- and2-hydroxy-3-butenyl valine adducts (MHBVal) and with DNA toform guanine adducts. Under the assumption of a genotoxic mech-anism and cross-species comparisons of hemoglobin and DNAbinding, these data facilitate a more informed cancer risk assess-ment. This analysis suggests that for exposures to 1,3-butadiene,the cancer risk is lower for humans than rats or mice on an equiv-alent dose basis (Van Sittert et al., 2000). Furthermore, this workillustrates that the measurement of the MHBVal adducts is a sen-sitive method for monitoring 1,3-butadiene metabolism via theepoxide-forming pathway in workers.
In 1973, an outbreak of peripheral neuropathy occurred inworkers exposed to the solvent methyl butyl ketone (MBK)(McDonough, 1974; Allen et al., 1975). The same lesion was re-
produced in animals (Mendell et al., 1974; Spencer et al., 1975).Biotransformation studies were then undertaken in rats and guineapigs, and some MBK metabolites (2,5-hexanedione, 5-hydroxy-2-hexanone) were also found to possess neurotoxic activity (Spencerand Schaumburg, 1975; DiVincenzo et al., 1976; DiVincenzo etal., 1977). Similar oxidation products are formed from n-hexane,the neurotoxicity of which is probably due to the same activemetabolite as that produced from MBK. Since methyl isobutylketone and methyl ethyl ketone cannot give rise to 2,5-hexanedione,they were suggested as replacement solvents.
These examples demonstrate that studies of the metabolic han-dling of occupational toxicants in animals are instrumental in thecharacterization of reactive intermediates and may suggest unsus-pected risks or indicate new methods of biological monitoring.Conversely, clinical observations on workers may stimulate stud-ies of the metabolism or the mechanism of toxicity of a toxicantin animals, thereby revealing the health significance of a biologi-cal disturbance.
Arsenic is one of the very few compounds for which there arelimited data of predictive value from animal studies to humanhealth effects. Arsenic has been used as a medicine since the timeof Hippocrates. Initially used to treat ulcers, arsenicals achievednotoriety as medicinals for a wide variety of ailments, and then, inthe first half of the twentieth century, for the treatment of syphilisand parasites. Many foods and beverages contaminated with ar-senic have been associated with accidental and intentional poison-ings. Inorganic pentavalent arsenic (arsenate) is readily absorbedacross tissues and converted to the trivalent form (arsenite). Thisis then methylated to form monomethylarsenic acid and dimethy-larsenic acid (NRC, 1999). These are primarily transported in theblood bound to sulfhydryl groups in proteins. The half-life in hu-mans for arsenic compounds is 2 to 4 days and the major excre-tion is via the urine (Nriagu, 1994). These organic arsenicals havelower toxicity than the inorganic arsenic compounds.
Inorganic arsenic was first noted as a human carcinogen byHutchinson in 1887 (Hutchinson, 1887). Epidemiologic studies ledto classification of arsenic by the International Agency for Researchon Cancer (IARC) as a skin and lung carcinogen in 1980 (IARC,1980). Since then studies among occupationally exposed pop-ulations and populations with high arsenic in their drinking waterhave shown conclusively that arsenic causes human cancers of theskin, lung, bladder, kidney, liver, nasal tissue, and prostate. Thereis also evidence for arsenic-associated cutaneous effects, cardio-vascular and cerebrovascular disease, diabetes mellitus, and ad-verse reproductive outcomes (EPA, 2000).
A large number of carefully executed cancer bioassays inmice, rats, beagles, and monkeys have been performed usingsodium arsenate, sodium arsenite, lead arsenite, arsenic trioxide,and dimethylarsinic acid. These studies have been uniformly neg-ative. A number of subsequent studies that tested for tumor-promotion activity following dosing with recognized tumor initia-tors also yielded negative results. Negative results in animal studiesin the face of unquestionable oncogenic activity in humans sug-gest that inorganic arsenic may follow a nongenotoxic mode of ac-tion (NRC, 1999).
The examples above demonstrate that the occupational toxi-cologist cannot rely solely on animal or epidemiologic studies. Acombined approach is necessary in order to identify, elucidate, andprioritize risks and to develop interventions and techniques forworker health surveillance.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1135
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1136 UNIT 7 APPLICATIONS OF TOXICOLOGY
EXPOSURE MONITORING
Two important applications of occupational toxicologic investiga-tions are compared below: environmental monitoring and biologi-cal monitoring. As described above under “Occupational HealthStandards,” both are important in worker health surveillance andare essential elements of toxicology studies with dosing via the in-halation or dermal routes.
Environmental Monitoring forExposure Assessment
An important objective of experimental and clinical investigationsin occupational toxicology is the proposal of safe levels of expo-sure. It is evident that with the accumulation of new informationon the toxicity of industrial chemicals, OELs must be reevaluatedat regular intervals. It should also be made clear that these levelsmay not protect everyone and should not supplant close medicalsurveillance of workers. Various private and official institutions reg-ularly review the toxicologic information on chemicals in order topropose or update permissible levels of exposure. These includegovernmental organizations worldwide and trade organizationssuch as the ACGIH and the European Centre for Ecotoxicity andToxicology of Chemicals (ECETOC). A critical element of estab-lishing OELs is the accurate and uniform assessment of exposure.Methodology for exposure assessment must be specifically tailoredto the agent under study and the environment in which it appears.To assess airborne exposures for compliance purposes, personalsamples taken in the breathing zone are generally used. In a fewspecific environments, area samples form the basis of an exposurestandard (e.g. the standard for exposure to raw cotton dust speci-fies use of the vertical elutriator or an equivalent method). Occu-pational environmental surveys may use area sampling to deter-mine areas with higher or lower toxicant concentrations. However,concentrations determined from personal samples typically exceedarea concentrations, depending on the work practices and envi-ronmental controls. For example, geometric mean concentrationsof inhalable dust assessed from 159 personal samples in dairy barnswere 1.78 mg/m3, compared with 0.74 mg/m3 for 252 area sam-ples collected simultaneously in two locations in the same barns(Kullman et al., 1998). Thus, in this environment, area samplingalone would underestimate personal exposures by a factor of 2.4.
Repeated random sampling is theoretically the best approachto developing unbiased measures of exposure. However, this israrely the approach that is taken. Variability in exposure, especiallyvariability over time, is usually large; therefore a considerablenumber of repeated measurements are needed to obtain an accu-rate proxy of the true exposure. When the number of repeats is in-sufficient, the slope of the exposure-response relationship will bebiased, usually leading to considerable underestimation of the re-lationship (Heederik and Attfield, 2000). Recent studies havedemonstrated that group-based approaches are more efficient interms of measurement effort to obtain a desired level of accuracy.In a group-based approach, workers are grouped by job title or taskperformed and the group mean is used as the average exposure foreach worker (Kromhout et al., 1996). Further statistical modelingof the exposure data can reduce problems of bias and large tem-poral and spatial variability (Preller et al., 1995; Tielemans et al.,1998). While this approach is gaining acceptance among occupa-
tional epidemiologists for evaluating exposure-response data andassessing risks, it is not generally used for compliance monitoring.
Although one cannot assess dose directly through exposuremonitoring, it has distinct advantages over biomonitoring. Exposuremonitoring allows one to quantify exposure by route through se-lective air monitoring in the breathing zone of the worker and der-mal dosimetry using absorptive material affixed to the workers’ skinor clothing. Biomonitoring cannot provide route-specific exposuredata. Environmental monitoring techniques are generally less ex-pensive and less invasive than techniques involving the collectionand analysis of biological samples such as blood or urine. Thus, alarger population of workers can be studied for the same amount ofmoney. Workers are accustomed to wearing personal samplers forexposure assessment and generally quite willing to do so. However,they are often unwilling to give a blood or urine sample, fearingthat the sample will be surreptitiously used for drug testing, DNAtesting, or experimentation. Some express fear that they will con-tract a serious infectious disease during the process of giving a bloodsample. Another benefit of air sampling in the workplace is thatspatial, temporal, and work practice associations can be establishedand can suggest better interventions and engineering controls. Fi-nally, analytic interferences and variabilities are generally lowerwith environmental samples than with biological samples.
A fully validated sampling and analysis method requires spec-ification of the sampling methods, sample duration, sample han-dling, and storage procedures; the analytic method and measure-ment technique; the range, precision, accuracy, bias, and limits ofdetection; quality assurance issues; and known interferences. It isalso important to document intralaboratory and interlaboratoryvariability. Once a standard method is established, it must be fol-lowed in every detail in order to assure consistency of results.
The development of accurate and precise analytic methods forenvironmental assessment is an ongoing effort. NIOSH publishesthe extensive NIOSH Manual of Analytical Methods (Casinelli andO’Connor, 1994), and these are widely used. The American Soci-ety for Testing Materials (ASTM) has also established a rigoroussystem for the establishment of methods. It generally requires 5 ormore years to establish a new ASTM method for exposure assess-ment. The International Organization for Standardization (ISO) isa global federation of national standards bodies with over 125member countries. The subcommittee on workplace atmospheresis administered by the American National Standards Institute(ANSI). ISO has completed harmonization on a number of air sam-pling methods—for example, the determination of the number con-centration of airborne inorganic fibers by phase contrast optical mi-croscopy. The American Industrial Hygiene Association (AIHA)and the ACGIH publish compilations with descriptions of analyticdevices and methodology (Cohen and Hering, 1995; DiNardi,1997). Methods have also been developed for bioaerosol exposureassessment, and these have been recently reviewed (Eduard andHeederik, 1998; Heederik et al., 2001; Thorne and Heederik,1999a; Willeke and Macher, 1999).
Biological Monitoring for Exposure Assessment
Biological monitoring of exposure assesses health risk through theevaluation of the internal dose. Depending on the chemical and theanalyzed biological parameter, the term internal dose may have
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1136
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1137
different meanings. A biological parameter may reflect the amountof chemical absorbed shortly before sampling, as with the con-centration of a solvent in the alveolar air or in the blood during theworkshift. It may reflect exposure during the preceding day, as withthe measurement of a metabolite in blood or urine collected 16 hafter the end of exposure. For toxicants with a long biological half-life, the measured parameter may reflect exposure accumulatedover a period of weeks. Internal dose may refer to the amount ofchemical stored in one or in several body compartments or in thewhole body (the body burden).
When biological measurements are available to assess the in-ternal dose, the approach offers important advantages over moni-toring the air of the workplace. Its greatest advantage is that thebiological parameter of exposure is more directly related to the ad-verse health effects than environmental measurements. Therefore,it may offer a better estimate of the risk than can be determinedfrom ambient monitoring. Biological monitoring accounts for up-take by all exposure routes. Many industrial chemicals can enterthe organism by absorption through the skin or the gastrointesti-nal tract as well as the lung. For example, some solvents (e.g., di-methylformamide) and many pesticide formulations exhibit sub-stantial exposure via the dermal route. In these situations, exposuresdetermined through monitoring airborne concentrations underesti-mate true exposure.
Several factors can influence uptake. Personal hygiene habitsvary from one person to another, and there is some degree of in-dividual variation in the absorption rate of a chemical through thelungs, skin, or gastrointestinal tract. Use of size-selective air sam-pling to determine the inhalable or respirable fraction canstrengthen the exposure estimate. However, biological factors suchas ventilatory parameters can affect the strength of such a correla-tion. For example, increased workload can markedly increase therespiratory uptake of an airborne toxicant. Because of its ability toencompass and evaluate the overall exposure (whatever the routeof entry), biological monitoring also can be used to test the over-all efficacy of personal protective equipment such as respirators,gloves, or barrier creams. Another consideration with biologicalmonitoring is the fact that the nonoccupational exposures (hobbies,residential exposures, dietary habits, smoking, second jobs) alsomay be expressed in the biological level. The organism integratesthe total external (environmental and occupational) exposure intoone internal load. While this is beneficial for worker health andsafety, it may be confounding in epidemiologic studies or compli-ance monitoring.
The value of biological monitoring is heightened when the re-lationships between external exposure, internal dose, and adverseeffects are established. Normally, biological monitoring of expo-sure cannot be used for assessing exposure to substances that ex-
hibit their toxic effects at the sites of first contact and are poorlyabsorbed. Examples include dermally corrosive compounds andprimary lung irritants. In this situation, the only useful relationshipis that between external exposure and the intensity of the localeffects.
Relationships between air monitoring and biological moni-toring may be modified by factors that influence the fate of an oc-cupational toxicant in vivo. Metabolic interactions can occur whenworkers are exposed simultaneously to chemicals that are bio-transformed through identical pathways. Exposure to chemicalsthat modify the activity of the biotransformation enzymes (e.g., mi-crosomal enzyme inducers or inhibitors) may also influence thefate of another compound. Furthermore, metabolic interferencesmay occur between occupational toxicants and alcohol, tobacco,food additives, prescription drugs, natural product remedies, orrecreational drugs. Changes in any of several biological variables(weight, body mass, pregnancy, diseases, immune status, etc.) alsomay modify the metabolism of an occupational chemical. Thesefactors have to be taken into consideration when the results of bi-ological exposure tests are interpreted. Whatever the parametermeasured, whether it is the substance itself, its metabolite, or anearly biomarker of effect, the test must be sufficiently sensitive andspecific to be of practical value.
Some chemicals have a long biological half-life in variousbody compartments (e.g., blood or urine), and the time of samplingmay not be critical. For other chemicals, the time of sampling iscritical because, following exposure, the compounds or theirmetabolites may be rapidly eliminated from the organism. In thesecases, the biological sample is usually collected during exposure,at the end of the exposure period, or sometimes just before the nextwork shift. When biological monitoring consists of the samplingand analysis of urine, it is usually performed in “spot” specimens,because routine collection of 24-h samples from workers is im-practical. It is standard practice to correct the results for the dilu-tion of the urine by expressing the results per gram of creatinine.Analyses performed on very dilute urine samples are not reliable.The World Health Organization has specified acceptable limits forurine specimens of between 0.3 and 3.0 g/L creatinine (or 1.010to 1.030 specific gravity) (ACGIH, 2000). When the large in-terindividual variability or high “background” level of the biolog-ical parameter selected makes the interpretation of a single meas-urement difficult, it is sometimes useful to analyze biologicalmaterial collected before and after the exposure period. The changein the biological parameter specifically due to exposure can some-times be better assessed by this method.
Environmental monitoring plays an important role for evalu-ating and preventing excessive exposure to toxicants in the work-place. However, the prevention of acute toxic effects on the respi-
Table 33-7Control Approaches for Occupational Inhalation Hazards
Change the process to use or produce less hazardous compounds.Automate and enclose the process to isolate the compounds.Incorporate administrative and work practice controls to reduce duration or intensity of
exposure.Install or upgrade local exhaust systems and dilution exhaust.Institute a comprehensive program for personal protective equipment use where necessary.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1137
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1138 UNIT 7 APPLICATIONS OF TOXICOLOGY
ratory tract, skin, or eye mucosa can only be achieved by keepingthe concentration of the irritant substance below a certain level oreliminating exposure. Local acute effects of chemicals do not lendthemselves to a biological surveillance program. Likewise, bio-logical monitoring is usually not indicated for detecting peak ex-posure to dangerous chemicals such as arsine (AsH3), carbonmonoxide, or prussic acid (HCN). Furthermore, identification ofemission sources and the evaluation of the efficiency of engineer-ing control measures are usually best performed by ambient airanalysis. Table 33-7 lists the approaches most useful for control-ling inhalation exposures in the workplace. It should be empha-sized that process changes and application of engineering controlsare preferable to reliance on personal protective equipment.
In summary, environmental and biological monitoring shouldnot be regarded as opposites but as complementary elements an
occupational health and safety program. They should be integratedas much as possible to ensure low levels of contaminants and op-timal health for workers.
CONCLUSION
The working environment will always present the risk of overex-posure of workers to various toxicants. Recognition of these risksshould not wait until epidemiologic studies have defined hazardouslevels. A combined experimental, clinical, and epidemiologic ap-proach is the most effective for evaluating the potential risks. Onecan then promulgate scientifically based occupational health stan-dards, apply effective workplace controls to ensure adherence tothose standards, and institute worker health surveillance programsto identify unexpected effects in susceptible individuals.
REFERENCES
Abnet CC, Tanguay RL, Heideman W, Peterson RE: Transactivation activ-ity of human, zebrafish, and rainbow trout aryl hydrocarbon receptorsexpressed in COS-7 cells: Greater insight into species differences intoxic potency of polychlorinated dibenzo-p-dioxin, dibenzofuran, andbiphenyl congeners. Toxicol Appl Pharmacol 159(1):41–51, 1999.
ACGIH: 2000 TLVs and BEIs: Threshold Limit Values for Chemical Sub-stances and Physical Agents and Biological Exposure Indices. Cincin-nati, OH: American Conference of Governmental Industrial Hygien-ists, 2000; pp 3–14 and 91–95.
Aldridge WN, Miles JM, Mount DL, Verschoyle RD: The toxicologicalproperties of impurities in malathion. Arch Toxicol 42:95–106, 1979.
Allen N, Mendell JR, Billmaier DJ, et al: Toxic polyneuropathy due tomethyl n-butylketone. Arch Neurol 32:209–218, 1975.
ATSDR (Agency for Toxic Substances and Disease Registry): Toxicologi-cal Profile for Arsenic. Atlanta: U.S. Department of Health and Hu-man Services, 1993.
ATSDR (Agency for Toxic Substances and Disease Registry): Toxicologi-cal Profile for Vinyl Chloride. Atlanta: U.S. Department of Health andHuman Services, 1997.
Baker EL, Zack M, Miles JV, et al: Epidemic malathion poisoning in Pak-istan malaria workers. Lancet 1:31–33, 1978.
Barnes JM: The basis for establishing and fixing maximum allowable con-centrations. Trans Assoc Ind Med Off 13:74–76, 1963.
Bason M, Lammintausta K, Maibach HI: Irritant dermatitis (irritation), inMarzulli FN and Maibach HI (eds): Dermatotoxicology, 4th ed. NewYork: Hemisphere, 1991, pp 223–252.
Becklake MR, Malo J-L, Chan-Yeung M: Epidemiological approaches inoccupational asthma, in Bernstein IL et al (eds) Asthma in the Work-place, 2d ed. New York:, Marcel Dekker, 1999, pp 27–66.
Bernstein IL, Bernstein DI, Chan-Yeung M, Malo J-L: Definition and clas-sification of asthma, in Bernstein IL et al (eds): Asthma in the Work-place, 2d ed. New York: Marcel Dekker, 1999, pp 1–3.
Birner G, Vamvakas S, Dekant W, Henschler D: Nephrotoxic and geno-toxic N-acetyl-S-dichlorovinyl-L-cysteine is a urinary metabolite afteroccupational 1,1,2-trichloroethylene exposure in humans: Implicationsfor the risk of trichloroethene exposure. Environ Health Perspect99:281–284, 1993.
Bolt HN: Metabolism of genotoxic agents: Halogenated hydrocarbons, inBerlin A, Draper M, Hemminki K, Vainio H (eds): Monitoring Hu-man Exposure to Carcinogenic and Mutagenic Agents. No. 59. Lyons,France: International Agency for Research on Cancer, 1984, pp 63–72.
Bonse G, Urban T, Reichert D, Henschler D: Chemical reactivity, meta-bolic oxirane formation and biological reactivity of chlorinated ethyl-
enes in the isolated perfused rat liver preparation. Biochem Pharma-col 24:1829–1834, 1975.
Cartier A, Malo J-L, Forest F, et al: Occupational asthma in snow crab-processing workers. J Allergy Clin Immunol 74:261–269, 1984.
Casinelli ME, O’Connor PF (eds): NIOSH Manual of Analytical Methods(NMAM), 4th ed. DHHS (NIOSH) Publication 94–113. Washington,DC: National Institute for Occupational Safety and Health, 1994.
Chan-Yeung M, Vedal S, Kus J, et al: Symptoms, pulmonary function andbronchial hyperactivity in western red cedar workers compared withthose in office workers. Am Rev Respir Dis 130:1038–1041, 1984.
Cohen BS, Hering SV (eds): Air Sampling Instruments for Evaluation ofAtmospheric Contaminants, 8th ed. Cincinnati, OH: American Con-ference of Governmental Industrial Hygienists, 1995.
Creech JL, Johnson HM: Angiosarcoma of the liver in the manufacture ofpolyvinylchloride. J Occup Med 16:150–151, 1974.
Cullinan P, Lowson D, Nieuwenhuijsen MJ, et al: Work related symptoms,sensitisation, and estimated exposure in workers not previously ex-posed to laboratory rats. Occup Environ Med 51:589–592, 1994.
Dekant W, Martens G, Vamvakas S, et al: Bioactivation of tetrachloroeth-ylene. Drug Metab Dispos 15:702–709, 1987.
Desjardins A, Malo JL, L’Archevêque J, et al: Occupational IgE-mediatedsensitization and asthma due to clam and shrimp. J Allergy Clin Im-munol 96:608–617, 1995.
DiNardi SR (ed.): The Occupational Environment—Its Evaluation andControl. Fairfax, VA: American Industrial Hygiene Association, 1997.
DiVincenzo GD, Hamilton ML, Kaplan CJ, Dedinas J: Metabolic fate anddisposition of 14C-labeled methyl n-butyl ketone in the rat. ToxicolAppl Pharmacol 41:547–560, 1977.
DiVincenzo GD, Kaplan CJ, Dedinas J: Characterization of the metabo-lites of methyl-n-butyl ketone, methyl iso-butyl ketone, and methylethyl ketone in guinea pig serum and their clearance. Toxicol ApplPharmacol 36:511–522, 1976.
Donham KJ, Thorne PS: Agents in organic dusts: Criteria for a causal re-lationship. Am J Ind Med 25:33–39, 1994.
Douwes J, Thorne PS, Pearce N, Heederik D: Biological agents—recogni-tion, in Perkins JL (ed): Modern Industrial Hygiene: Vol III. Biolog-ical Aspects. Cincinnati, OH: American Conference of GovernmentalIndustrial Hygienists, 2001. In press.
Duchaine C, Meriaux A, Thorne PS, Cormier Y: Assessment of particulatesand bioaerosols in Eastern Canadian sawmills. Am Ind Hyg Assoc J61:727–732, 2000.
Eduard W, Heederik D: Methods for quantitative assessment of airbornelevels of noninfectious microorganisms in highly contaminated workenvironments. Am Ind Hyg Assoc J 59:113–127, 1998.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1138
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 33 OCCUPATIONAL TOXICOLOGY 1139
Eduard W, Sandven P, Levy F: Relationships between exposure to sporesfrom Rhizopus microsporus and Paecilomyces variotii and serum IgGantibodies in wood trimmers. Int Arch Allergy Immunol 97:274–282,1992.
EPA. 40 CFR Parts 141 and 142, National primary drinking water regula-tions; arsenic and clarifications to compliance and new source con-taminants monitoring; proposed rule. Fed Reg 65(121):38888–38983,2000.
European Union: Employment rates report 1998 Employment perform-ance in the member states. http://europa.eu.int/comm/employmentsocial/empl&est/empL99/rates en.pd f, pp. 1–31, 1998.
Flindt, MHL: Pulmonary disease due to inhalation of derivatives of Bacil-lus subtilis containing proteolytic enzyme. Lancet 1:1177, 1969.
Fuortes LJ, Weih LA, Jones M, et al: Epidemiologic assessment of labo-ratory animal allergy among university employees. Am J Ind Med29:67–74, 1996.
Fuortes LJ, Weih L, Pomrehn P, et al: Prospective epidemiologic evalua-tion of laboratory animal allergy among university employees. Am JInd Med 32:665–669, 1997.
GAO/HEHS: Child Labor in Agriculture—Changes Needed to Better Pro-tect Health and Educational Opportunities. GAO/HEHS-98-193.Washington, DC: U.S. General Accounting Office, 1998, pp 1–90.
Glass, WI, Power P, Burt R, et al: Work-related respiratory symptoms andlung function in New Zealand mussel openers. Am J Ind Med 34:163–168, 1998.
Halpin DMG, Graneek BJ, Lacey J, et al: Respiratory symptoms, im-munological responses, and aeroallergen concentrations at sawmills.Occup Environ Med 51:165–172, 1994.
Hard GC, Rodgers IS, Baetcke KP, et al: Hazard evaluation of chemicalsthat cause accumulation of �2u-globulin, hyaline droplet nephropathy,and tubule neoplasia in the kidneys of male rats. Environ Health Per-spect 99:313–349, 1993.
Heederik D, Attfield M. Characterization of dust exposure for the study ofchronic occupational lung disease: A comparison of different expo-sure assessment strategies. Am J Epidemiol 151(10):982–990, 2000.
Heederik D, Thorne PS, Douwes J: Monitoring and evaluation of bioaerosolexposure, in Perkins JL (ed): Modern Industrial Hygiene: Vol III. Bi-ological Aspects. Cincinnati, OH: American Conference of Govern-mental Industrial Hygienists, 2001. In press.
Hollander A, Heederik D, Doekes G: Respiratory allergy to rats: exposure—response relationships in laboratory animal workers. Am J RespirCrit Care Med 155:562–567, 1997.
Houba R, Heederik DJ, Doekes G, van Run PE: Exposure-sensitization re-lationship for alpha-amylase in the baking industry. Am J Respir CritCare Med 154:130–136, 1996.
Hsieh TH, Yu CP, Oberdorster G: Deposition and clearance models of Nicompounds in the mouse lung and comparisons with the rat models.Aerosol Sci Technol 31:358–372, 1999.
Hutchinson J: Arsenic cancer. Br Med J 2:1280–1281, 1887.IARC (International Agency for Research on Cancer): IARC Monographs
on the Evaluation of Carcinogenic Risks to Humans. Suppl 7. Lyons,France: IARC, 1987.
IARC: Metals and metallic compounds. IARC Monographs on the Evalu-ation of Carcinogenic Risks to Humans, Vol 23. Lyon, France: Inter-national Agency for Research on Cancer, 1980.
Kromhout H, Tielemans E, Preller L, Heederik D: Estimates of individualdose from current measurements of exposure. Occup Hyg 3:23–39,1996.
Kullman GJ, Thorne PS, Waldron PF, et al: Organic dust exposures fromwork in dairy barns. Am Ind Hyg Assoc J 59:403–413, 1998.
Lewis TR, Morrow PE, McClellan RO, et al.: Establishing aerosol expo-sure concentrations for inhalation toxicity studies. Toxicol Appl Phar-macol 99:377–383, 1989.
McDonough JR: Possible neuropathy from methyl-n-butyl ketone. N EnglJ Med 290:695, 1974.
Mendell JR, Saida K, Ganasia MF, et al: Toxic polyneuropathy producedby methyl-n-butyl ketone. Science 185:787–789, 1974.
Michel O, Kips J, Duchateau J, et al: Severity of asthma is related to en-dotoxin in house dust. Am J Respir Crit Care Med 154:1641–1646,1996.
Monson RR, Peters JM, Johnson MN: Proportional mortality amongvinylchloride workers. Lancet 2(7877):397–398, 1974.
Morrow, PE: Contemporary issues in toxicology: Dust overloading of thelungs: Update and appraisal. Toxicol Appl Pharmacol 113:1–12, 1992.
NIH-99-4495: Corrositex: An in Vitro Test Method for Assessing DermalCorrosivity Potential of Chemicals. NIH-99-4495. Washington, DC:National Toxicology Program, 1999, pp 1–236.
NIOSH: Work-Related Lung Disease Surveillance Report. Number 2000-105. Washington, DC: Department of Health and Human Services(NIOSH), 2000.
NRC (National Research Council): Arsenic in Drinking Water. Washing-ton, DC: National Academy Press, 1999, pp 1–200.
Nriagu JO: Arsenic in the Environment: Part II: Human Health Effects andEcosystem Effects. New York: Wiley. 1994, pp 1–91.
NTP (National Toxicology Program): Ninth Report on Carcinogens. Re-search Triangle Park, NC: National Toxicology Program, U.S. De-partment of Health and Human Services, 2000.
Pepys J, Pickering CAC, Breslin ABX, Terry DJ: Asthma due to inhaledchemical agents — Toluene di-isocyanate. Clin Allergy 2:225–236,1972a.
Pepys J, Pickering CAC, Hughes EG: Asthma due to inhaled chemicalagents—complex salts of platinum. Clin Allergy 2:391–396, 1972b.
Preller L, Kromhout H, Heederik D, Tielen MJM: Modeling long-term av-erage exposure in occupational exposure-response analysis. Scand JWork Environ Health 21:504–512, 1995.
Sarlo K, Parris JS, Clark ED, et al: Influence of MHC background on theantibody response to detergent enzymes in the mouse intranasal test.Toxicol Sci 58:299–305, 2000.
Schenker MB, Christiani D, Cormier Y, et al: Respiratory health hazardsin agriculture. Am J Respir Crit Care Med Suppl 158(pt 2):S1–S76,1998.
Schlesinger RB: Comparative deposition of inhaled aerosols in experi-mental animals and humans: A review. J Toxicol Environ Health15:197–214, 1985.
Schwartz DA, Thorne PS, Jagielo PJ, et al: Endotoxin responsiveness andgrain dust–induced inflammation in the lower respiratory tract. Am JPhysiol 267:L609–L617, 1994.
Schwartz DA, Thorne PS, Yagla SJ, et al: The role of endotoxin in graindust–induced lung disease. Am J Respir Crit Care Med 152:603–608,1995.
Spencer PS, Schaumburg HH: Experimental neuropathy produced by 2,5-hexanedione A major metabolite of the neurotoxic industrial solventmethyl-n-butyl ketone. J Neurol Neurosurg Psychiatry 38:771–775,1975.
Spencer PS, Schaumburg HH, Raleigh RL, Terhaar CJ: Nervous system de-generation produced by the industrial solvent methyl-n-butyl ketone.Arch Neurol 32:219–222, 1975.
Thorne PS, Heederik D: Assessment methods for bioaerosols, in Saltham-mer T (ed): Organic Indoor Air Pollutants—Occurrence, Measure-ment, Evaluation. Weinheim, Germany: Wiley/VCH, 1999a; pp 85–103.
Thorne PS, Heederik D: Indoor bioaerosols—Sources and characteristics,in Salthammer T (ed): Organic Indoor Air Pollutants—Occurrence,Measurement, Evaluation. Weinheim, Germany: Wiley/VCH, 1999b;pp 275–288.
Thorne PS: Inhalation toxicology models of endotoxin- and bioaerosol-induced inflammation. Toxicology 152:13–23, 2000.
Thorne PS, Hillebrand J, Magreni C, et al: Experimental sensitization tosubtilisin: I. Production of immediate and late-onset pulmonary reac-tions. Toxicol Appl Pharmacol 86:112–123, 1986.
Tielemans E, Kupper LL, Kromhout H, et al: Individual-based and group-based occupational exposure assessment: Some equations to evaluatedifferent strategies. Ann Occup Hyg 42(2):115–119, 1998.
Uehleke H, Tabarelli-Poplawski S, Bonse G, Henschler D: Spectral evi-
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1139
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

1140 UNIT 7 APPLICATIONS OF TOXICOLOGY
dence for 2,2,3-trichloro-oxirane formation during microsomaltrichloroethylene oxidation. Arch Toxicol 37:95–105, 1977.
USDL (United States Department of Labor): Career Guide to Industries:Agricultural Production. 2000–01 ed. Washington, DC: U.S. Depart-ment of Labor, Bureau of Labor Statistics, http://www.bls.gov/oco/cg/cgs001.htm, 2000a.
USDL (United States Department of Labor): The Employment Situation:April 2000. USDL 00-126. U.S. Department of Labor, Bureau of La-bor Statistics 2000b, pp 1–20.
van Sittert NJ, Megens HJJJ, Watson WP, Boogaard PJ: Biomarkers of ex-posure to 1,3-butadiene as a basis for cancer risk assessment. ToxicolSci 56:189–202, 2000.
Venables KM, Dally MB, Nunn AJ, et al: Smoking and occupational al-lergy in workers in a platinum refinery. Br Med J 299:939–942, 1989.
Venables KM, Topping MD, Howe W, et al: Interaction of smoking andatopy in producing specific IgE antibody against a hapten protein con-jugate. Br Med J 290:201–204, 1985.
Viola PL, Bigotti A, Caputo A: Oncogenic response of rat skin, lungs, andbones to vinyl chloride. Cancer Res 31:516–522, 1971.
Weill H, Salvaggio JE, Neilson A, et al: Respiratory effects of toluene di-isocyanate manufacture: A multidisciplinary approach. Environ HealthPerspect 11:101–108, 1975.
Wernfors M, Nielsen J, Schültz A, Skerfving S: Phthalic anhydride-inducedoccupational asthma. Int Arch Allergy Appl Immunol 79:77–82,1986.
Whitlock JP Jr, Okino ST, Dong L, et al: Cytochromes P450 5: inductionof cytochrome P4501A1: A model for analyzing mammalian gene tran-scription. FASEB J 10(8):809–818, 1996.
Willeke K, Macher J: Air sampling, in Macher J (ed): Bioaerosols —Assessment and Control. Cincinnati, OH: American Conference ofGovernmental Industrial Hygienists, 1999, pp 11-1–11-25.
Wilson CL, Safe S: Mechanisms of ligand-induced aryl hydrocarbonreceptor-mediated biochemical and toxic responses. ToxicologicPathol 26(5):657–671, 1998.
2996R_ch33_1123-1140 4/25/01 1:04 PM Page 1140
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com