rx15 clinical tues_330_1_teater_2allespach
TRANSCRIPT

Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Disclosures
bull Don Teater MD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
bull Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
bull John J Dreyzehner MD MPH FACOEM has disclosed no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Disclosures
bull All plannersmanagers hereby state that they or their spouselife partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months
bull The following plannersmanagers have the following to disclosendash Kelly Clark ndash Employment Publicis Touchpoint Solutions
Consultant Grunenthal USndash Robert DuPont ndash Employment Bensinger DuPont amp
Associates-Prescription Drug Research Centerndash Carla Saunders ndash Speakerrsquos bureau Abbott Nutrition
Learning Objectives
1 Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Alternatives to opioids in pain management
Don Teater MD
National Safety Council
Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Disclosures
bull Don Teater MD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
bull Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
bull John J Dreyzehner MD MPH FACOEM has disclosed no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Disclosures
bull All plannersmanagers hereby state that they or their spouselife partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months
bull The following plannersmanagers have the following to disclosendash Kelly Clark ndash Employment Publicis Touchpoint Solutions
Consultant Grunenthal USndash Robert DuPont ndash Employment Bensinger DuPont amp
Associates-Prescription Drug Research Centerndash Carla Saunders ndash Speakerrsquos bureau Abbott Nutrition
Learning Objectives
1 Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Alternatives to opioids in pain management
Don Teater MD
National Safety Council
Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Disclosures
bull All plannersmanagers hereby state that they or their spouselife partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months
bull The following plannersmanagers have the following to disclosendash Kelly Clark ndash Employment Publicis Touchpoint Solutions
Consultant Grunenthal USndash Robert DuPont ndash Employment Bensinger DuPont amp
Associates-Prescription Drug Research Centerndash Carla Saunders ndash Speakerrsquos bureau Abbott Nutrition
Learning Objectives
1 Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Alternatives to opioids in pain management
Don Teater MD
National Safety Council
Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Learning Objectives
1 Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Alternatives to opioids in pain management
Don Teater MD
National Safety Council
Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Alternatives to opioids in pain management
Don Teater MD
National Safety Council
Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Disclosure
I Don Teater MD have no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Why this is important
bull 100 million people with pain in the US
bull Over 16000 die every year from opioid overdose
ndash Also consider
bull Addiction
bull Crime
bull Neonatal abstinence syndrome
bull Societal monetary costs
bull Workplace and traffic injuriesdeath
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
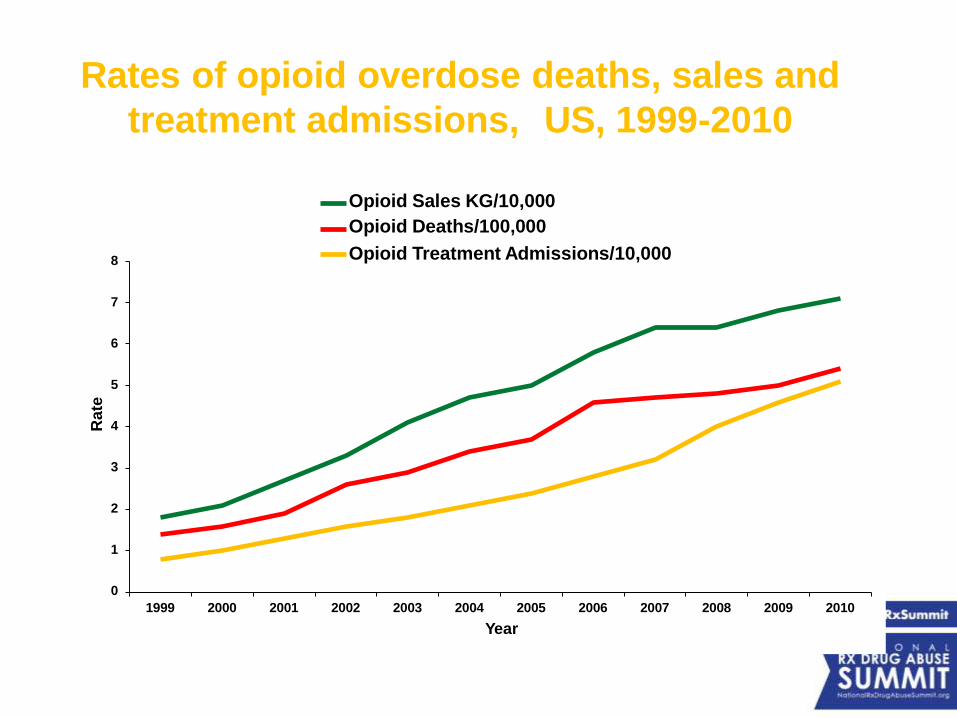
Rates of opioid overdose deaths sales and
treatment admissions US 1999-2010
Year
National Vital Statistics System DEArsquos Automation of Reports and ConsolidatedOrders System SAMHSArsquos TEDS
7
6
5
4
3
2
1
0
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rate
Opioid Sales KG10000
Opioid Deaths100000
Opioid Treatment Admissions10000
Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Opioid increase
Centers for Disease Control and Prevention CDC grand rounds Prescription drug overdoses ndash a US epidemic MMWR MorbMortal Wkly Rep 2012 6110-13
96
700
1997 2007
Mg per person
Mg per person
Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Is it possiblehellip
To reduce pain while at the same time reducing the use of opioids
Yes
20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

20 year experiment
bull 20 years ago we made an honest effort to treat pain betterhellip
bull We have not succeeded
The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

The State of US HealthYears lived with disability (in thousands)
0
500
1000
1500
2000
2500
3000
3500
Low back pain Other MSdisease
Neck pain Osteoarthritis
1990
2010
Murray C (2013) The state of US health 1990-2010 burden of diseases injuries and risk factors JAMA The Journal of the American Medical Association 310(6) 591ndash608
Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Institute of MedicineRelieving Pain in America 2011
ldquoPain affects millions of Americans contributes greatly to national rates of morbidity mortality and disability and is rising in prevalencerdquo
IOM (Institute of Medicine) 2011 Relieving Pain in America A Blueprint for Transforming Prevention Care Education and Research Washington DC The National Academies Press
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage
International Association for the Treatment of Pain
Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Pain
bull Acute pain Pain lt 3 months
bull Chronic pain Pain gt 3 months
Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Efficacy of pain mediations
0
5
10
15
20
25
30
35
40
45
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Morphine 10 mgIM
Percent with 50 pain relief
Percent with 50 pain relief
Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Severity does not matter
A 2005 Cochran review of the treatment of renal colic concluded
NSAID medications and opioids have equal effectiveness in treatment of acute renal colichellipbut opioids have more side-effects
Holdgate A Pollock T Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute renal colic Cochrane Database of Systematic Reviews 2004 Issue 1 Art No CD004137 DOI 10100214651858CD004137pub3
Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Side effects
bull NSAIDs
ndash GI
ndash Renal
ndash Cardiac
bull Acetaminophen
ndash Liver
Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Opioid side effects
bull Mentally impairing
bull Delay recovery
bull Increase medical costs
bull Opioid hyperalgesia
bull Double the chance of disability
bull Increase falls (and fractures)
bull Cardiac GI
bull Addiction
Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Opioid side effects
bull Brain effects
ndash Impairing
ndash Calming
ndash Antidepressant effects
ndash Stimulate dopamine
ndash Cause neuroplastic changes
ndash Epigenetic changes
Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Chronic pain
bull No evidence that opioids are effective for long-term treatment of chronic pain
bull ldquoSafe and effectiverdquo use of opioids for chronic pain is an invalid concept
ndash No evidence that these can be used safely
ndash No evidence that they can be used effectively
bull Epidemiologic studies have shown that those on chronic opioid therapy have worse quality of life than those with chronic pain who are not1
(1) Eriksen J Sjoslashgren P Bruera E Ekholm O amp Rasmussen N K (2006) Critical issues on opioids in chronic non-cancer pain an epidemiological study Pain 125(1-2) 172ndash9 doi101016jpain200606009
Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Efficacy of pain mediations
0
10
20
30
40
50
60
70
Ibuprofen 200mg
Acetaminophen500 mg
Ibuprofen 400mg
Oxycodone 15mg
Oxy 10 + acet1000
Ibu 200 + acet500
Percent with 50 pain relief
Percent with 50 pain relief
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Takeaways
bull These are brain medications more than they are pain medications
ndash They do have a role but it is limited
bull Medical and dental providers We should be prescribing much less of these
bull Policymakers By making laws and rules to reduce prescribing we will improve the treatment of pain
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
ldquoTo write prescriptions is easy
but to come to an understanding with
people is hardrdquo
-- Franz Kafka ldquoA Country Doctorrdquo
Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Don Teater MDdonteaternscorg
White papers
Evidence on the efficacy of pain medications nscorgpainmedevidence
The Psychological and Physical Side Effects of Pain Medications
safetynscorgsideeffects
Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Helping Our Patients Helping Ourselves Physician-Administered Counseling Strategies to Decrease
Pain Perceptions amp Addictive Behaviors
Heidi H Allespach PhD
University of Miami Miller School of Medicine
Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Faculty Disclosure
Heidi H Allespach PhD has no relevant real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services
27
Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Learning Objectives
1Identify alternatives to opioids for pain management
2 Advocate that physicians avoid opioids when treating acute pain
3 Prepare physicians to use counseling strategies to decrease pain perceptions and addictive behaviors
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Since we are talking about addictive behaviorshelliphelliphellip
Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Questions
bull What types of thoughts do you have when you see an alcoholicaddicted pt What types of feelings do these thoughts create
bull How do these thoughtsfeelings differ depending on whether your pt is male or female Black or White Young or old
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Questions
bull Think about your own personal life experiences w an alcoholicaddict (family member friend self) How do you think these past experiences contribute to the ways you thinkfeel about your addicted pts
bull How might these reactions influence your Rx of these type of pts
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Brief Points Pain and Addiction
bull Not all patients who use and even misuse opioids are ldquoaddictsrdquo
bull Addiction is a chronic disease
bull Tolerance dependence pseudoaddiction
bull Pain affects every aspect of the individual
bull Cannot separate ldquoemotionalrdquo pain from ldquophysicalrdquo pain (mindbody)
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
Teaching Patients
Cognitive Restructuring to Decrease Pain amp Addictive Behaviors
Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Question
How confident are you in your ability to provide brief counseling to your patients with pain
A Extremely confidentB Very confidentC NeutralD Not very confident E Not at all confident
Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Cognitive Behavioral Therapy (CBT)
bull CBT is the most widely used amp studied psychotherapeutic modality in the medical setting
bull Aaron Beck MD
bull Time limited and focused
bull Helps you and your patients to feel more ldquoin controlrdquohellipand it works too
bull Wealth of literature on the efficacy of utilizing CBT to decrease pain
Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Cognitive Restructuring
bull Levy RL Langer SL Walker LS Romano JM Christie DL Youssef N DuPen MM Ballard SA Labus J Welsh E Feld LD Whitehead WE Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain JAMA Pediatr 2013 Feb167(2)178-84
bull Castro MM Daltro C Kraychete DC Lopes J Cognitive behavioral therapy causes an improvement in quality of life in patients with chronic musculoskeletal pain Arq Neuropsiquiatr 2012 Nov70(11)864-8
bull Friebe H Cognitive restructuring in chronic pain Help your patients understand their pain in a new light Pain Therapy Series 3 Active pain coping works Fortschr Med 1999 Feb 20117(5)53
Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Cognitive-Behavioral Model
ldquoWe feel what we thinkrdquo
--Albert Ellis
We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

We also see what we EXPECT to see
Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Negative Self-Talk or ldquoThe Dis-Easerdquo
bull An automatic thought or ldquoself-talkrdquo statement that is distorted and creates distress
bull Fear-based critical
bull For those with addiction part of themselves that wants to drinkuse again
NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

NegativerdquoReactiverdquo Self-Talk
bull Only by becoming aware of their negative self-talk can our pt change the way she feels amp for addicted pts avoid relapse
bull Only by actively listening to our pts negative statements will we gain insight into what is going on with them
bull It is actually GOOD to tell your pts to ldquolose their mindsrdquo(good for you too)
ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

ldquoThe Monkeyrdquo
bull Future=Anxiety (The ldquoWhat Ifsrdquo)
bull Past=Depression Guilt Regrets (The ldquoWouldrsquoversquos Couldrsquoversquos amp Shouldrsquoversquos)
The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

The Relationship Between Thoughts and Feelings
Automatic Feeling
Negative
Self-Talk
(Thought)
Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Thoughts Feelings amp Behaviors
Automatic Feelings Physical
Thought Sensation
(Self-Talk)
Behaviors
Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Addictive (Reactive) Cognitions
Automatic Thought Feeling Physical
ldquoI have to get my anxiety INCREASED
meds-I CANrsquoT LIVE PAIN
WITHOUT THEM
ADDICTIVE BEHAVIORS
Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Cognitive-Restructuring
bull ldquoThe Wise Selfrdquo ldquoRational Non-Reactive Selfrdquo Higher Powerrdquo ldquoGodrdquomdashopposite of NegativerdquoMonkeyrdquoReactive Self-Talk
bull ldquoWhat can you tell yourself (or what would the ldquoWiseHigher Power Godrdquo part of you tell you---to make you feel less (anxious angry sad etc)rdquo
bull ldquoWhat would the WiseHigher Power God part of you say about your drug userdquo
Pomm (Allespach) HA Pomm RM Management of the
Addicted Patient in Primary Care 2007 Springer
Publishing
ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

ldquoNonreactiverdquo Cognitions
Balanced Thought Feeling Physical
I CAN live without taking less anxiety DECREASED
more medicationmdashfor PAIN
TODAY I have to ldquothink this
throughrdquoamp practice what
my doctor taught me
Tries non-narcotic strategy instead of opioid
WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

WITHOUT amp WITH CBT
Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Some Additional Strategieshellip
bull Diaphragmatic Breathing
bull ldquoThink It Throughrdquo
bull ldquoAct Donrsquot Reactrdquo
bull ldquoOne Day at a Timerdquo
bull ldquoProgress Not Perfectionrdquo
ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

ldquoMindfulnessrdquo
Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Mindfulness Literature
bull F Zeidan KT MartucciRA KraftNS Gordon JG McHaffie RC Coghill Brain Mechanisms Supporting Modulation of Pain by Mindfulness Meditation J Neurosci 2011 April 6 31(14) 5540ndash5548 J Psychosom Res 2010 Jan68(1)29-36
bull Rosenzweig S Greeson JM Reibel DK Green JS Jasser SA Beasley D Mindfulness-based stress reduction for chronic pain conditions variation in treatment outcomes and role of home meditation practice J Psychosom Res 2010 Jan68(1)29-36
bull Marchand WR Mindfulness-based stress reduction mindfulness-based cognitive therapy and Zen meditation for depression anxiety pain and psychological distress J Psychiatr Pract 2012 Jul18(4)233-52
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board
ldquoThe Awareness Exerciserdquo Demonstration
ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

ldquoThe Awareness Exerciserdquo
bull Present Orientation
bull Patients can use the Awareness Exercise to ldquodisconnectrdquo from The Monkey
bull In the beginning tell patients not to practice when they are feeling any ldquohotrdquo emotion amp also to do it out loud
bull DO NOT FOCUS ON PAIN OR OTHER INTERNAL SOMATIC SX
Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Pain Diary
bull To increase awareness that pain is never constant amp is influenced by thoughtsemotions
bull 3 times a Day
bull Write down Thoughts Feelings Situation Pain Level (1-10)
Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Resources for Learning More About CBT
bull The Beck Institute (training for you) httpwwwbeckinstituteorgcognitive-behavioral-therapy
bull WedMD (for patients) httpwwwwebmdcomdepressionguidecognitive-behavioral-therapy-for-depression
bull Judith Beck (Book-for you) httpwwwamazoncomCognitive-Behavior-Therapy-Second-Editiondp1609185048
bull The Relaxation amp Stress Management Workbook (for patients and for you)httpwwwamazoncomRelaxation-Reduction-Workbook-Harbinger-Self-Helpdp1572245492ref=sr_1_1s=booksampie=UTF8ampqid=1405023778ampsr=1-1ampkeywords=the+relaxation+and+stress+reduction+workbook+6th+edition
Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Great Resource for Patients
bull Workbook
ldquoManaging Pain Before It Manages Yourdquo
by Margaret A Caudill MD PhD MPHhttpwwwamazoncomManaging-Pain-Before-Manages-
ThirddpB001TKE4VGref=sr_1_2s=booksampie=UTF8ampqid
=1405023980ampsr=1-
2ampkeywords=managing+pain+before+it+manages+you
Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Practice Recommendations
Before initiating chronic opioid therapy clinicians should conduct a history physical examination and appropriate testing including an assessment of risk of substance abuse misuse or addiction
bull Primary health care professionals are well-positioned to provide interventions targeted to all substances irrespective of their legal status
3 Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain American Pain Society-American Academy of Pain Medicine Opioids Guidelines Panel Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain J Pain 2009 Feb10(2)113-30 AHRQ National Guidelines Clearinghouse httpwwwguidelinegovcontentaspxid=161654 WHO httpwwwwhointsubstance_abuseactivitiesassisten
Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Practice Recommendations
bull Psychosocial evaluation The psychosocial evaluation should include information about the presence of psychological symptoms (eg anxiety depression or anger) psychiatric disorders personality traits or states and coping mechanisms
bull Cognitive behavioral therapy biofeedback or relaxation training These interventions may be used as part of a multimodal strategy for patients with low back pain as
well as for other chronic pain conditionsNATIONAL GUIDELINES CLEARINGHOUSE Practice guidelines for chronic pain management An updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine httpwwwguidelinegovcontentaspxid=23845
Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Contact
bull Heidi Allespach PhD
hallespachmedmiamiedu
Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board

Clinical TrackAlternatives to Opioidsin Pain Management
Presentersbull Don Teater MD Medical Advisor National Safety
Councilbull Heidi H Allespach PhD Director of Behavioral
Medicine Family Medicine and Internal Medicine Residency and Subspecialty Fellowship Programs University of Miami Miller School of Medicine
Moderator John J Dreyzehner MD MPH FACOEM Commissioner Tennessee Department of Health and Member Rx Summit National Advisory Board