royal society of medicine
TRANSCRIPT
1162
but relaxation can just as easily be got by postureas it can by anaesthesia, and the obvious thing is tocombine the two to obtain the maximum effect.
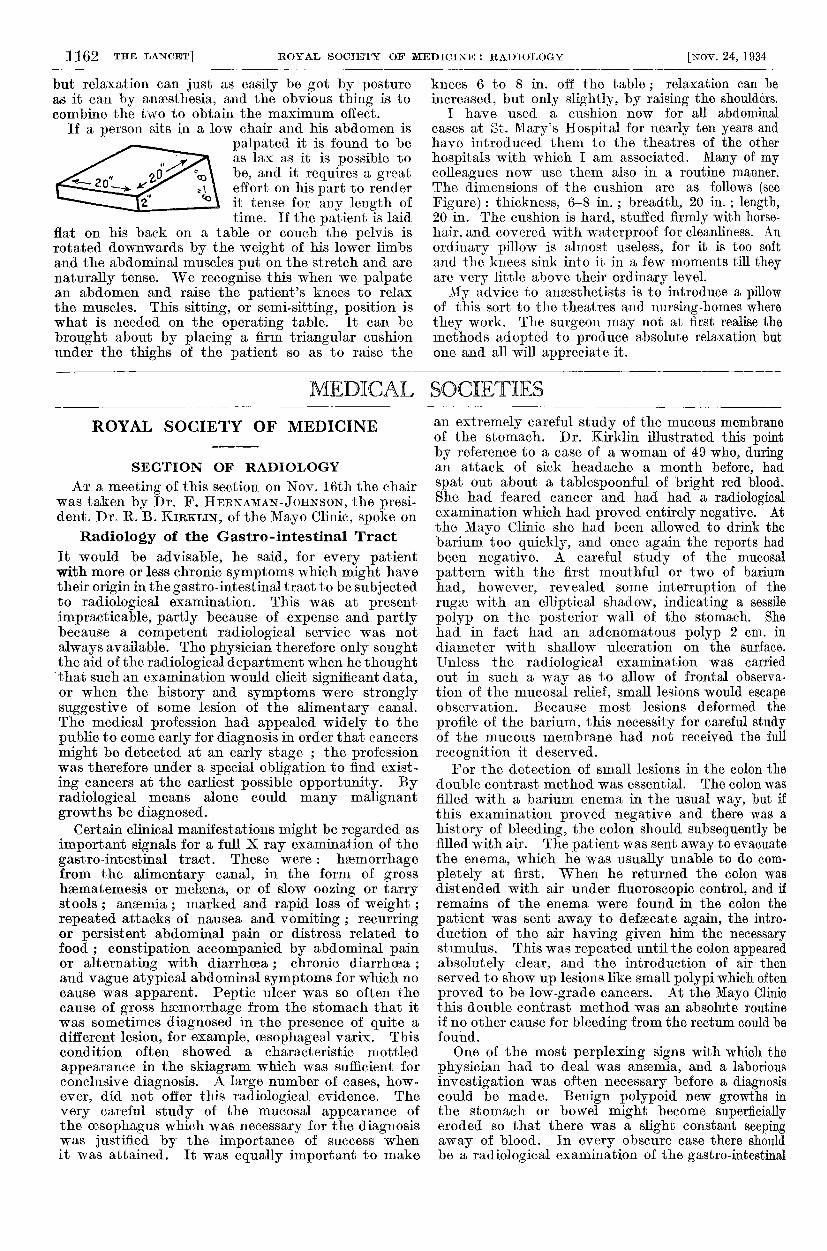
If a person sits in a low chair and his abdomen ispalpated it is found to beas lax as it is possible tobe, and it requires a greateffort on his part to renderit tense for any length oftime. If the patient is laid
flat on his back on a table or couch the pelvis isrotated downwards by the weight of his lower limbsand the abdominal muscles put on the stretch and arenaturally tense. We recognise this when we palpatean abdomen and raise the patient’s knees to relaxthe muscles. This sitting, or semi-sitting, position iswhat is needed on the operating table. It can be
brought about by placing a firm triangular cushionunder the thighs of the patient so as to raise the
knees 6 to 8 in. off the table ; relaxation can beincreased, but only slightly, by raising the shoulders.
I have used a cushion now for all abdominalcases at St. Mary’s Hospital for nearly ten years andhave introduced them to the theatres of the other
hospitals with which I am associated. Many of mycolleagues now use them also in a routine manner.The dimensions of the cushion are as follows (seeFigure) : thickness, 6-8 in. ; breadth, 20 in. ; length,20 in. The cushion is hard, stuffed firmly with horse-hair, and covered with waterproof for cleanliness. Anordinary pillow is almost useless, for it is too softand the knees sink into it in a few moments till theyare very little above their ordinary level.My advice to anaesthetists is to introduce a pillow
of this sort to the theatres and nursing-homes wherethey work. The surgeon may not at first realise themethods adopted to produce absolute relaxation butone and all will appreciate it.
MEDICAL SOCIETIES
ROYAL SOCIETY OF MEDICINE
SECTION OF RADIOLOGY
AT a meeting of this section on Nov. 16th the chairwas taken by Dr. F. HERNAMAN-JOHNSON, the presi-dent. Dr. R. B. KIRKLIN, of the Mayo Clinic, spoke on
Radiology of the Gastro-intestinal TractIt would be advisable, he said, for every patientwith more or less chronic symptoms which might havetheir origin in the gastro-intestinal tract to be subjectedto radiological examination. This was at presentimpracticable, partly because of expense and partlybecause a competent radiological service was notalways available. The physician therefore only soughtthe aid of the radiological department when he thoughtthat such an examination would elicit significant data,or when the history and symptoms were stronglysuggestive of some lesion of the alimentary canal.The medical profession had appealed widely to thepublic to come early for diagnosis in order that cancersmight be detected at an early stage ; the professionwas therefore under a special obligation to find exist-ing cancers at the earliest possible opportunity. Byradiological means alone could many malignantgrowths be diagnosed.
Certain clinical manifestations might be regarded asimportant signals for a full X ray examination of thegastro-intestinal tract. These were: haemorrhagefrom the alimentary canal, in the form of grosshaematemesis or melaena, or of slow oozing or tarrystools ; anaemia ; marked and rapid loss of weight ;repeated attacks of nausea and vomiting ; recurringor persistent abdominal pain or distress related tofood ; constipation accompanied by abdominal painor alternating with diarrhoea ; chronic diarrhoea ;and vague atypical abdominal symptoms for which nocause was apparent. Peptic ulcer was so often thecause of gross haemorrhage from the stomach that itwas sometimes diagnosed in the presence of quite adifferent lesion, for example, oesophageal varix. Thiscondition often showed a characteristic mottled
appearance in the skiagram which was sufficient forconclusive diagnosis. A large number of cases, how-ever, did not offer this radiological evidence. The
very careful study of the mucosal appearance ofthe oesophagus which was necessary for the diagnosiswas justified by the importance of success whenit was attained. It was equally important to make
an extremely careful study of the mucous membraneof the stomach. Dr. Kirklin illustrated this pointby reference to a case of a woman of 49 who, duringan attack of sick headache a month before, hadspat out about a tablespoonful of bright red blood.She had feared cancer and had had a radiologicalexamination which had proved entirely negative. Atthe Mayo Clinic she had been allowed to drink thebarium too quickly, and once again the reports hadbeen negative. A careful study of the mucosalpattern with the first mouthful or two of bariumhad, however, revealed some interruption of the
rugae with an elliptical shadow, indicating a sessile
polyp on the posterior wall of the stomach. Shehad in fact had an adenomatous polyp 2 cm. indiameter with shallow ulceration on the surface.Unless the radiological examination was carriedout in such a way as to allow of frontal observa-tion of the mucosal relief, small lesions would escapeobservation. Because most lesions deformed the
profile of the barium, this necessity for careful studyof the mucous membrane had not received the full
recognition it deserved.For the detection of small lesions in the colon the
double contrast method was essential. The colon wasfilled with a barium enema in the usual way, but ifthis examination proved negative and there was ahistory of bleeding, the colon should subsequently befilled with air. The patient was sent away to evacuatethe enema, which he was usually unable to do com-pletely at first. When he returned the colon wasdistended with air under fluoroscopic control, and ifremains of the enema were found in the colon thepatient was sent away to defsecate again, the intro-duction of the air having given him the necessarystimulus. This was repeated until the colon appearedabsolutely clear, and the introduction of air thenserved to show up lesions like small polypi which oftenproved to be low-grade cancers. At the Mayo Clinicthis double contrast method was an absolute routineif no other cause for bleeding from the rectum could befound.One of the most perplexing signs with which the
physician had to deal was anaemia, and a laboriousinvestigation was often necessary before a diagnosiscould be made. Benign polypoid new growths inthe stomach or bowel might become superficiallyeroded so that there was a slight constant seepingaway of blood. In every obscure case there shouldbe a radiological examination of the gastro-intestinal

1163
tract. In one case a man of 65 had come to the clinicfor general examination as he felt he was " getting on."He had no particular symptoms but the routine
investigation revealed a low-grade anaemia. He hadhad haemorrhoids for eighteen months or two yearswith slight bleeding which he had ascribed to the piles.Barium enema had not revealed any lesion, but thedouble contrast method had shown up a small round
pedunculated polyp which had been successfullyremoved. It was very important to have stereoscopicfilms to distinguish these small growths from faecalcontents. To consider cancer in cases of loss of
weight might seem illogical in the absence of anysymptoms pointing to the gastro-intestinal tract.Nevertheless, cancer of the alimentary canal wasextremely insidious in onset and was often heraldedby loss of weight. A competent radiological examina-tion was often the only means of making an earlydiagnosis. In one case a man of 45 had complainedof nothing whatever but the loss of 25 lb. in threemonths and of an inability for three weeks to digestone of his favourite dishes. The radiographs showedextensive ulcerated carcinoma of the distal half ofthe lesser curvature of the stomach.
Recurrent vomiting for no obvious reason was anemphatic indication for radiological examination, butnausea was not an impressive symptom and might beignored. Yet it might be the sole indication of seriousgastric disease. A physician suffering from anginapectoris and coronary sclerosis complained of ratherpersistent nausea, particularly noticeable with anempty stomach. Gastro-intestinal examination in the
radiological department had shown a very small lesionon the lesser curvature with a typical meniscus sign ;he had in fact an extensive perforating cancer of the
stomach, fixed to the pancreas. The clinical mani-festations of peptic ulcerweredefinite, but it wasnot easyto distinguish between gastric and duodenal ulcerationor between malignant and benign growths. In thesedifferential diagnoses radiology might often be ofthe greatest help. If the radiologist could definitelyvisualise a crater the duodenum should be opened upeven though the surgeon was unable to find a growthon superficial examination. A persistent fleck ofbarium remaining in the duodenum despite manipu-lation often revealed an ulcer which failed to causedeformity. Duodenitis might also be diagnosed by astudy of the duodenal mucous membrane in certaincases. This condition was not regarded at the
Mayo Clinic as necessarily a forerunner of duodenalulceration. The symptoms might extend for aboutthe same period of time and have the same degree
of severity as those of duodenal ulcer. Duodenitiswas therefore diagnosed when the radiologist foundtransient and varying deformity of the duodenumcombined with irritability and spasm, so that thebarium rushed through and an adequate picture wasvery difficult to obtain. The mucosa, when visualised,appeared as a fine reticular network.
It was possible in the preliminary fluoroscopicexamination to recognise the presence of air betweenthe diaphragm and the liver. This, in the absence ofrecent surgical intervention, indicated a perforatinglesion and further radiological examination was
contra-indicated.
DIFFERENTIAL DIAGNOSIS OF BENIGN AND MALIGNANT
CONDITIONS
Every gastric ulcer should be regarded as malignantuntil the contrary was proved. The following differentialpoints were, however, useful. The benign growth wasusually less than 2 cm. in diameter ; any ulcer morethan 2-5 em. across was probably malignant. The benign
ulcer showed a regular hemispherical outline with asharply defined dense barium shadow ; the malignantone was conical and irregular with a faint, poorlydefined outline. The benign growth usually appearedon the lesser curvature distant from the pylorus,while the malignant would be found on the greatercurvature or the posterior wall; 75 per cent. of ulcersnear the pylorus were malignant. Peristalsis was dimin-ished or absent and spastic manifestations were rare inmalignant growths, but the benign ulcer was usuallyaccompanied by active peristalsis and often bynarrowing or curling of the antrum and hour-glasscontraction. The pylorus also was spastic, whereas inmalignancy it would be found gaping. The rugseusually converged towards the niche of a benign ulcer,while in a malignant case they were faintly marked oreffaced. The best test, however, was the therapeutictest. It was very exceptional for a malignant ulcer todisappear under a fortnight’s medical treatment.The possibility of diaphragmatic hernia should
always be borne in mind by the radiologist. The
diagnosis of prepyloric hypertrophy from gastricsyphilis and prepyloric ulcer or cancer was difficult,but there were three distinguishing symptoms and iftwo of these were present a diagnosis of hypertrophymight be made. These were a slight invagination ormushrooming of the bulbar base, a marked cleft inthe inferior border of the canal and an elongationof the canal. Chronic or recurring diarrhoea calledurgently for full colon investigation. Patients whopresented peri-abdominal symptoms often enoughowed them to purely functional conditions, but in asmall minority there were diseases of the gastro-intestinal tract which could hardly be diagnosedwithout radiology. The stomach had been describedas the fire-alarm box of the abdomen, and manynegative reports must be expected. Nevertheless,radiology was capable of giving worthy assessments indiagnosis and in the elimination of malignant disease.
DISCUSSION
Dr. A. E. BARCLAY said that the double contrastmethod had originated in this country but had beenneglected. He asked what was the proof of malig-nancy ; the only real proof was the death of thepatient, and that was averted by surgical intervention.Dr. J.A. E. LYNHAM thought that duodenitis was lessa pathological entity than a reflex associated withsome lesion elsewhere.
Dr. G. E. VILVANDPP thought that duodenitis was abad diagnosis, the condition really being duodenalulcer. The failure to diagnose malignancy early wasnot the fault of the radiologist or even of the phy-sician, but of the patient, who went to the chemistwhen suffering from abdominal discomfort. In his
experience 99 per cent. of ulcers on the greatercurvature of the stomach were malignant.
MEDICAL SOCIETY OF INDIVIDUALPSYCHOLOGY
AT a meeting of this society held in London onNov. 8th, with Dr. J. C. YourrG, the president, inthe chair, a paper on
Post-menopausal Neuroseswas read by Dr. HiLDA WEBER. In consideringthe factors favouring the onset of post-menopausalneuroses, she pointed out that at this period of lifethe interest of sexual maturity has passed, and eventhe menopause as a matter of condolence is over,whilst the time when a woman’s years have become