routine immunization. immunisation process of artificially providing immunity active-vaccines...
TRANSCRIPT

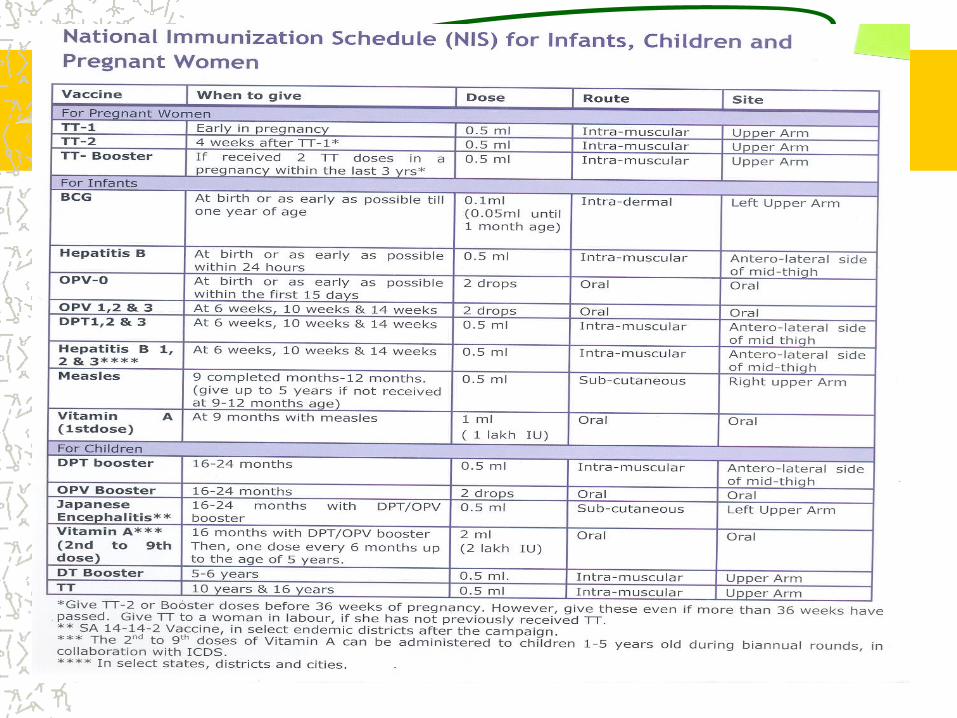
Routine Immunization

IMMUNISATION•PROCESS OF ARTIFICIALLY PROVIDING IMMUNITY
•ACTIVE-VACCINES
•LIVEATTENUATED,KILLED,TOXOID,SUBUNIT, RECOMBINANT
•PASSIVE-IMMUNOGLOBULIN
•MOST COST EFFECTIVE HEALTH CARE INTERVENTION AND BIRTH RIGHT OF EVERY CHILD


TYPES OF VACCINES
TYPE OF ANTIGEN EXAMPLE
LIVE BACTERIA,ATTENUATED BCG,TY21
LIVE VIRUS ATTENUATED OPV,MMR
KILLED BACTERIA PERTUSIS,S.TYPHII
KILLED VIRUS IPV,RABIES,HAV
TOXOID DT,TT
CAPSULAR POLYSACCHARIDE TYPHOID VI,HIB ,MENINGO
& PNEUMO
VIRAL SUBUNIT HBsAg
BACTERIA SUBUNIT ACELLULAR PERTUSIS

Vaccines and equity
Poorer / US community children at greater risk of illness and death from vaccine preventable diseases
Routine vaccination promotes equity in child health

Tuberculosis
Tuberculosis (TB) is caused by the bacterium Mycobacterium tuberculosis which usually attacks the lungs, but can also affect other parts of the body, including the bones, joints, and brain
TB is spread from one person to another through the air often when a person with the disease coughs or sneezes. TB spreads rapidly, especially in areas where people are living in crowded conditions, have poor access to health care, and are malnourished.

Tuberculosis…….
Immunization of infants with Bacille Calmette-Guérin vaccine (BCG) can protect against TB meningitis and other severe forms of TB in children less than five years old. BCG vaccine is not recommended after 24 months of age because the protection provided is variable and less certain.
BCG injections Protect the child against childhood tuberculosis
In institutional deliveries, immediately after birth
In home deliveries, at one and half month along with the DPT injection and OPV
Poliomyelitis
Disease of young children -80-90% <5 yrs, majority below 2 years
Clusters of susceptible needed to maintain circulation
Infectivity typically one week before paralysis and 4-6 weeks thereafter (peak first 2 weeks)Incubation period 7-21 days (range 3-35 days) Incubation period: Time from infection to appearance of symptoms Risk of paralysis increased by tonsillectomy, exercise, pregnancy, intramuscular injections

Clinical Features of Poliomyelitis
Acute onset, flaccid paralysisFever present at onsetNo progression after 2-3 daysAsymmetric Legs affected most oftenParalysis is permanent

How Polio Spreads?

How Polio Spreads? Transmitted person-to-person, primarily faecal-to-
oral route
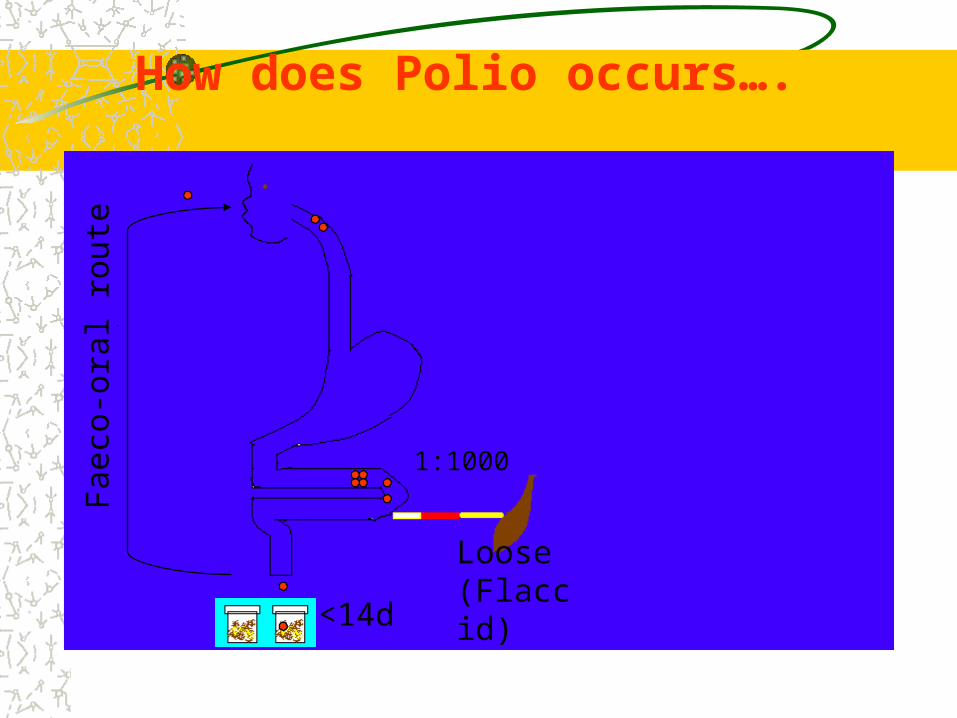
Faecal contamination of food & water enter through food pipe into intestineIt then multiply in thousandsFinally majority of virus excrete through stool
Fae
co-o
ral r
oute
1:1000
Loose(Flaccid)<14d
How does Polio occurs….
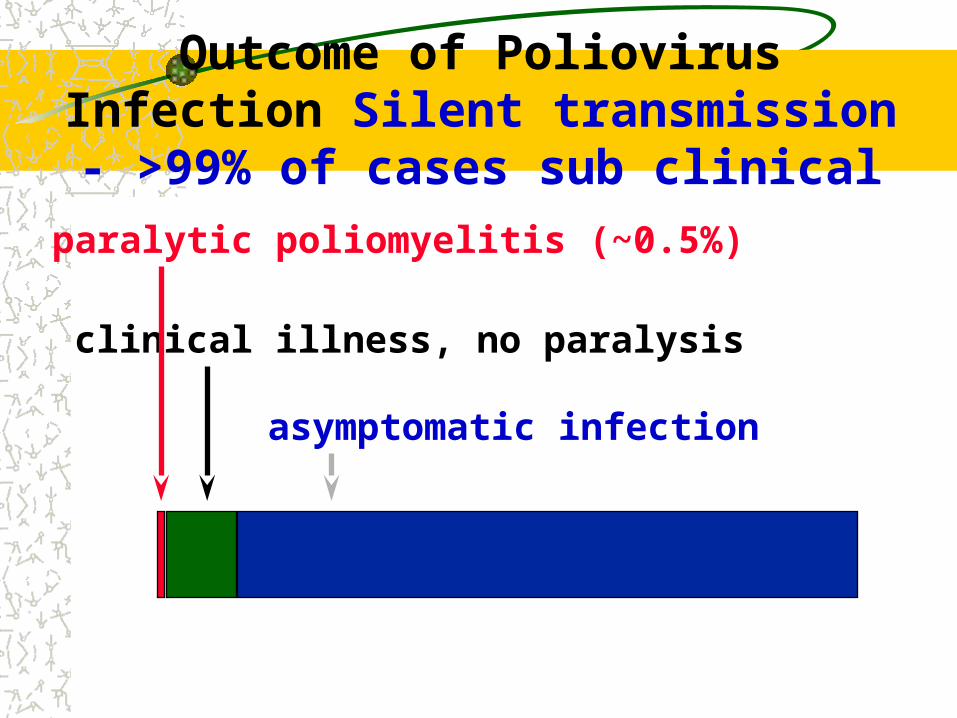
Outcome of Poliovirus Infection Silent transmission - >99% of cases sub clinical
asymptomatic infection
clinical illness, no paralysis
paralytic poliomyelitis (~0.5%)

MMR
• MULTIDOSE ,LIVE ATTENUATED VIRAL VACCINE
• 15 MONTHS TO 5 years
• DILUENT-DOUBLE DISTILLED WATER
• MEASLES-1000 TCID-50
• MUMPS-5000 TCID-50
• RUBELLA 1000 TCID50
• DOSE-0.5 ML S/C

HEPATITIS B
•RECOMBINANT
•DOSE-0.5 ML OR 10 MICROGRAM
•ROUTE INTRAMUSCULAR
•NOT TO BE GIVEN IN GLUTEAL REGION
•BIRTH DOSE-INSTITUTIONAL DELIVERIES
•3 DOSES WITH DPT STARTING FROM 6 WEEKS TO 14 WEEKS

Tetanus
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Immunization ProgramCenters for Disease Control and Prevention
Revised March 2002

Clostridium tetani
Spore-forming bacteria
Spores found in soil, dust, animal feces; may persist for months to years

Tetanus Pathogenesis
Toxin binds in central nervous system
Leads to muscle contraction and spasm

Tetanus Clinical Features
Incubation period 8 days (range, 3-21 days)Generalized tetanus: descending symptoms of trismus (lockjaw), difficulty swallowing, muscle rigidity, spasmsSpasms continue for 3-4 weeks; complete recovery may take months

Neonatal Tetanus
Generalized tetanus in newborn infant
Infant born without protective passive immunity: Mother not immunized with Tetanus Toxoid immunization
Almost all affected newborn die
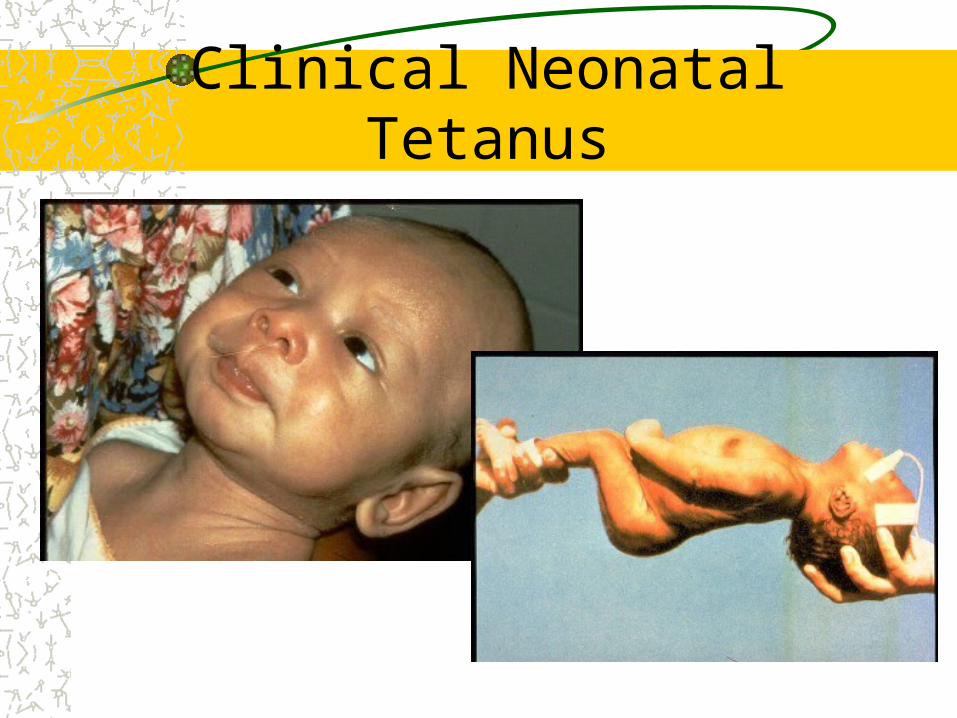
Clinical Neonatal Tetanus

Clinical Aspects of Neonatal Tetanus
C. tetani enters through unclean umbilical cord
Signs & Symptoms– Trismus (risus sardonicus)– Neck stiffness– Body rigidity– Opisthotonus– Convulsions– Respiratory muscle weakness resulting in
death
Neonatal Tetanus
Any newborn baby that - sucks and cries normally during the first 2 (two) days of life; - becomes ill between 3 and 28 days of life
with BOTH
1. Inability to suck - and - 2. Generalized muscle rigidity (stiffness)

How to Prevent Neonatal Tetanus
Two complimentary strategies
1. Clean delivery - “ 5 cleans”
•Clean delivery surface•Clean hands•Clean Thread•Clean and New Blade•Clean umbilical cord and stump care
2. Immunization of mother with TT

Tetanus EpidemiologyReservoir Soil and intestine of
animals and humans
Transmission Contaminated wounds Tissue injury
Communicability Not contagious

Diphtheria
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Immunization ProgramCenters for Disease Control and Prevention
Revised March 2002

Diphtheria Clinical Features
Incubation period 2-5 days (range, 1-10 days)
May involve any mucous membrane
Diphtheria Epidemiology
Reservoir Human carriers Usually asymptomatic
Transmission RespiratorySkin and fomites rarely
Communicability Up to several weeks without antibiotics

PertussisHighly contagious respiratory infection
caused by Bordetella pertussis
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Immunization ProgramCenters for Disease Control and Prevention
Revised August 2002

Pertussis Clinical Features
Incubation period 5-10 days (up to 21 days)
Slow onset, similar to minor upper respiratory infection with nonspecific cough
Fever usually minimal throughout course
Pertussis Clinical Features
Primary stage 1-2 weeks
Paroxysmalcough stage1-6 weeks
Convalescence Weeks to months

Pertussis Epidemiology
Reservoir HumanAdolescents and adults
Transmission Respiratory dropletsAirborne rare
Communicability Maximum in catarrhal stage
DPT
One dose gives very limited protection
Two doses give 80-% short term protection
Three doses lead to sustainable protection
Administered by intramuscular injection

Measles
Highly contagious viral illness caused by measles
virus {Paramyxovirus (RNA)}

Measles Pathogenesis
Respiratory transmission of virus
Replication in nasopharynx and regional lymph nodes

Measles Clinical Features
Incubation period 10-12 daysFever, cough, coryza, conjunctivitis2-4 days after prodrome, 14 days after exposureMaculopapular rash Begins on face and headPersists 5-6 daysComplications:Diarrhea,Otitis media,Pneumonia,
Encephalitis, Death

Measles can cause long-lasting disabilities: Children with Post-Measles Corneal Scars


Vitamin A Supplementation
9 to 12 months: First dose: With measles vaccine: 1Lac IU ( 1ml= ½ spoon)
More than 12 to 59 months: Second to ninth dose at the intervals of six months : 2 Lac IU (2 ml= 1 spoon)

Why is Vitamin A supplementation important?Why is Vitamin A supplementation important?
Vitamin A Deficiency (VAD) initially compromises the integrity of the epithelial barriers and the immune system, this is then followed by impairment of the visual system. Consequently, there is increased severity of some infections and increased risk of death, especially among children.
Vitamin A Supplementation can reduce the risk of mortality from measles by about 50 % and overall mortality by 25-35%

Vitamin A Supplementation
9 to 12 months: First dose: With measles vaccine: 1Lac IU ( 1ml= ½ spoon)
More than 12 to 60 months: Second to ninth dose at the intervals of six months : 2 Lac IU (2 ml= 1 spoon)
Measles Epidemiology
Reservoir Human
Transmission Respiratory Airborne
Communicability 4 days before to 4 days after rash onset

Measles Vaccine
Composition Live virus
Duration ofImmunity Lifelong
Schedule One dose

· Minor illnesses such as upper respiratory infections or diarrhoea, mild fever (< 38.5°C)
· Allergy, asthma· Prematurity, underweight newborn child· Malnutrition· Child being breastfed· Family history of convulsions· Treatment with antibiotics· Dermatoses, eczema or localized skin infection· Chronic diseases of the heart, lung, kidney and liver· Stable neurological conditions, such as cerebral palsy and Down's
syndrome· History of jaundice after birth
These are not contraindications to Routine Immunization

AEFI
Vaccines are safe and effectiveLife threatening adverse events are extremely rareMild side effects are commonly seen and can be self limiting and easily manageableBenefits of immunization greatly outweighs the risks of AEFIMajority are due to unsafe injection practices and procedures




AEFI---- Rare, more severe reactions
Include : seizures,
thrombocytopenia, hypotonic-hypo responsive episodes, persistent inconsolable screaming
In most cases they are self-limiting and lead to no long-term problems
Anaphylaxis, while potentially fatal, is treatable without any long-term effects

COLD CHAIN
Cold Chain is a system of transporting and storing vaccines at recommended temperature from the point of manufacture to the point of use
COLD CHAINAll Vaccines tend to lose potency on exposure to heat above +80 C
Some Vaccines lose potency when exposed to freezing temperatures
The damage is irreversible


COLD CHAIN EQUIPMENTS
WALK IN COOLERS & FREEZERSICE LINED REFRIGERATORSDEEP FREEZERSVACCINE CARRIERSDAY CARRIERSCOLD BOXESDOMESTIC REFRIGERATORS-IN DELHI

VACCINE VIAL MONITOR
3 = bad:Don’t Utilize
4 = bad:Don’t Utilize
The central square is equal to, or darker than the surrounding circle
X
X
1 = good:Utilize
2 = good:Utilize
The central square is lighter than the surrounding circle

AD SYRINGES•Impossible to reuse•Lowest risk of person to person transmission of blood borne infections.•Fixed needle reduces dead space so less wastages. Also eliminates chances of air bubble entry due to loose fitting earlier.•Dose specific-ensure correct dose•Presterilized-no use of bulky equipment.

AD SYRINGE
Do not use if damaged/tornTear pack from plunger side.Remove needle cover& discardTake dose – do not touch needle or rubber capDraw dose. If bubble just shake, administer. Push plunger completely. Do not recap.

AD SYRINGE
Cut the needle immediately from the hub with the help of the hub cutter. It will go to the white sturdy container. NO UNTREATED BIO-MEDICAL WASTE SHALL BE STORED BEYOND A PRRIOD OF 48 HOURS.

Auto-Disable SyringesAdvantages of the AD syringes:
AD syringe is designed to prevent the re-use of non-sterile syringes.
The fixed-needle design reduces the dead space in the syringe that wastes vaccine. And eliminates the chances of air bubble entry into the syringe due to loose fitting of the needle
The AD syringe are made dose specific (0.5 ml & 0.1 ML) and hence with drawing the plunger to the full length ensures correct dose. No adjustment is required.
AD syringes are pre-sterilized therefore; eliminating the need to carry bulky equipment such as pressure cooker / stove /kerosene etc to session site.
AD syringes being pre sterilized will be advantageous to Health worker as they would not spend any time on sterilization

WASTE GENERATION
AD SYRINGES TO BE USED WHERE SAFE DISPOSAL POSSIBLEWASTE CONSISTS OF:
1. PACKAGING MATERIAL2. SYRINGES3. NEEDLES4. BROKEN/DISCARDED VIALS
What is Surveillance
WHO – “The continuous scrutiny of the factors that determine the occurrence of disease and other conditions of ill health. Surveillance is essential for effective control and prevention and includes the collection, analysis, interpretation and distribution of relevant data for action”“Data collection for Action"

Five steps in Surveillance
Collection of data
Compilation of data
Analysis and interpretation
Follow up action
Feed back

Prerequisites for effective Surveillance
Use of Standard Case DefinitionsEnsuring Regularity of the ReportsAction on ReportsMedical Officer must be clear about:– What information to gather– How often to compile & analyze the data– How often & to whom to report– What Performa or formats to use– What action to take
