rondout valley central school district -...
TRANSCRIPT
RONDOUT VALLEY CENTRAL SCHOOL DISTRICT P.O. Box 9
Accord, New York 12404
Mr. Rosario Agostaro Dr. Timothy Wade
Superintendent of Schools Deputy Superintendent
845-687-2400 Ext. 4802 845-687-2400 Ext. 4863
Mrs. Lisa Pacht Mrs. Debra Kosinski
Executive Director for Curriculum & Instruction School Business Administrator
845-687-2400 Ext. 4805 845-687-2400 Ext. 4812
SPRING 2015
Dear Parent/Guardian,
Attached you will find a lottery application for anticipated Universal Pre-Kindergarten seats for the 2015-
2016 academic year. Seats will be offered based on a public lottery to be held on May 19 at 6:00 p.m. at the
Middle School Lecture Hall.
You must be a resident of the Rondout School District
Your child must be 4 years old on/before December 1, 2015.
Complete the enclosed Lottery Application and UPK Registration Forms.
Return both forms to the Rondout Valley Central School District Office by 4:00 p.m. on May 18, 2015.
Please review the enclosed information carefully. All required documents (see page 2) must be received no
later than July 1, 2015 in order for your child to attend school in September.
(We must have a Physical form and Updated Immunizations before they can attend UPK)
You may bring your required documents to the District Office and we will copy them for you,
or they may be faxed to: Atten: UPK 845-687-0945
or mailed to: Rondout Valley CSD
DO-PPS-UPK
PO Box 9
Accord, NY 12404
All are welcome to attend the lottery on May 19 although your presence is not required.
Please Note: The New York State budget has not been adopted as of March 27, 2015. Providing Universal
Pre-Kindergarten for residents of the Rondout Valley School District is dependent upon the State grant.
Parents will be contacted in July with results of lottery.
Robin Doick
CSE/CPSE Chairperson
Pupil Personnel Services
845-687-2400 Ext. 4863
Please keep this page for your information
Due to NYS Immunization requirements we must ask for documentation. All Preschoolers must be up to date on immunizations and Well Child exam before attending school.
*PLEASE NOTE: DOCUMENTS REQUIRED BY JULY 1st 1)Proof of Residency- copy of bill/receipt with name and physical address 2)Copy of Birth Certificate 3)Copy of Shot Records 4)Copy of Physical Exam -physical must be done between 9/14-9/15 – (please take enclosed Health
Assessment Form to your Doctor)
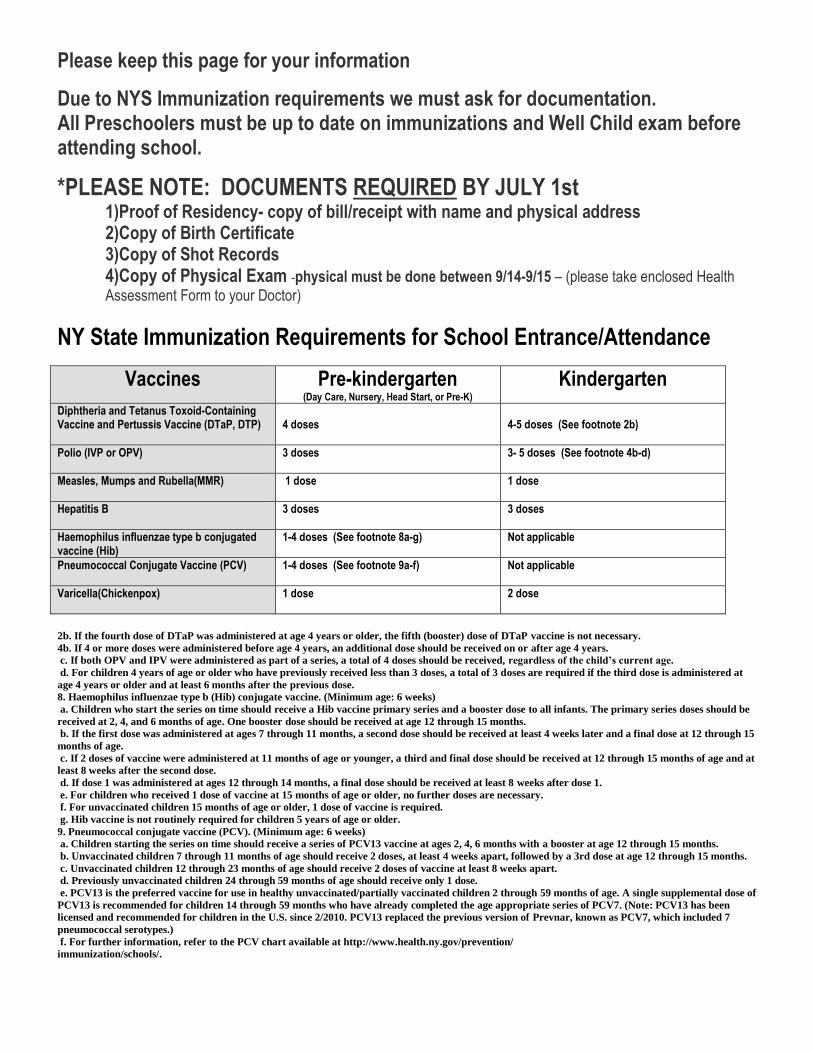
NY State Immunization Requirements for School Entrance/Attendance
Vaccines Pre-kindergarten (Day Care, Nursery, Head Start, or Pre-K)
Kindergarten
Diphtheria and Tetanus Toxoid-Containing Vaccine and Pertussis Vaccine (DTaP, DTP)
4 doses
4-5 doses (See footnote 2b)
Polio (IVP or OPV) 3 doses 3- 5 doses (See footnote 4b-d)
Measles, Mumps and Rubella(MMR) 1 dose 1 dose
Hepatitis B 3 doses 3 doses
Haemophilus influenzae type b conjugated vaccine (Hib)
1-4 doses (See footnote 8a-g)
Not applicable
Pneumococcal Conjugate Vaccine (PCV) 1-4 doses (See footnote 9a-f)
Not applicable
Varicella(Chickenpox) 1 dose 2 dose
2b. If the fourth dose of DTaP was administered at age 4 years or older, the fifth (booster) dose of DTaP vaccine is not necessary.
4b. If 4 or more doses were administered before age 4 years, an additional dose should be received on or after age 4 years.
c. If both OPV and IPV were administered as part of a series, a total of 4 doses should be received, regardless of the child’s current age.
d. For children 4 years of age or older who have previously received less than 3 doses, a total of 3 doses are required if the third dose is administered at
age 4 years or older and at least 6 months after the previous dose.
8. Haemophilus influenzae type b (Hib) conjugate vaccine. (Minimum age: 6 weeks)
a. Children who start the series on time should receive a Hib vaccine primary series and a booster dose to all infants. The primary series doses should be
received at 2, 4, and 6 months of age. One booster dose should be received at age 12 through 15 months.
b. If the first dose was administered at ages 7 through 11 months, a second dose should be received at least 4 weeks later and a final dose at 12 through 15
months of age.
c. If 2 doses of vaccine were administered at 11 months of age or younger, a third and final dose should be received at 12 through 15 months of age and at
least 8 weeks after the second dose.
d. If dose 1 was administered at ages 12 through 14 months, a final dose should be received at least 8 weeks after dose 1.
e. For children who received 1 dose of vaccine at 15 months of age or older, no further doses are necessary.
f. For unvaccinated children 15 months of age or older, 1 dose of vaccine is required.
g. Hib vaccine is not routinely required for children 5 years of age or older.
9. Pneumococcal conjugate vaccine (PCV). (Minimum age: 6 weeks)
a. Children starting the series on time should receive a series of PCV13 vaccine at ages 2, 4, 6 months with a booster at age 12 through 15 months.
b. Unvaccinated children 7 through 11 months of age should receive 2 doses, at least 4 weeks apart, followed by a 3rd dose at age 12 through 15 months.
c. Unvaccinated children 12 through 23 months of age should receive 2 doses of vaccine at least 8 weeks apart.
d. Previously unvaccinated children 24 through 59 months of age should receive only 1 dose.
e. PCV13 is the preferred vaccine for use in healthy unvaccinated/partially vaccinated children 2 through 59 months of age. A single supplemental dose of
PCV13 is recommended for children 14 through 59 months who have already completed the age appropriate series of PCV7. (Note: PCV13 has been
licensed and recommended for children in the U.S. since 2/2010. PCV13 replaced the previous version of Prevnar, known as PCV7, which included 7
pneumococcal serotypes.)
f. For further information, refer to the PCV chart available at http://www.health.ny.gov/prevention/
immunization/schools/.

Fax Physical & Immunizations to: Mail to: Rondout Valley CSD-PPS-UPK
845-687-0945 PO Box 9
Accord, NY 12404
RONDOUT VALLEY CENTRAL SCHOOL DISTRICT
HEALTH SERVICES
P.O. BOX 9, ACCORD, N.Y. 12404
NYSED requires an annual physical exam for UPK, new entrants, students in Grades K, 2, 4, 7 and 10, sports, working permits and triennially for the Committee
on Special Education (CSE)
HEALTH ASSESSMENT FORM
Name: _____________________________________________________ Date of Birth: _____________________________________
School: ____________________________________________________ Gender: M F Grade: ______________________
Immunization on record attached Sickle Cell Screen: Positive Negative Not Done Date: _____________ No immunizations given today PPD: Positive Negative Not Done Date: _____________ Immunizations given since last Health Appraisal: Elevated Lead: Yes No Not Done Date: _____________
Dental Referral Yes No Not Done Date: _____________
_____________________________________________________________________________________________________________________________
Significant Medical/Surgical History: see attached ___________________________________________________________________________________________
____________________________________________________________________________________________________________________________________________
Specify current diseases: Asthma Diabetes: Type 1 Type 2 Hyperlipidemia Hypertension
Other: _______________________________________________________________________________________________
Allergies: LIFE THREATENING Food: _______________________________ Insect: _______________ Other: _________________________________
Seasonal Medication: ______________________________ _________________________________
Height: ________________ Weight: _______________ Blood Pressure: ________________ Date of Exam: _____________
EXAM ENTIRELY NORMAL Tanner: l. ll. IIl. lV. V. Scoliosis: Negative Positive: ____________________
Specify any abnormality (use reverse of form if needed): ____________________________________________________________________________________
__________________________________________________________________________________________________________________________________
Medications (list all): None Additional medications listed on physician letter head stationary
Name: _____________________________________________________ Dosage/ Time: ________________________________________________________
Name: ____________________________________________________ Dosage/Time: ________________________________________________________
If AM dose is missed at home: ________________________________________________________________________________________________________ I assess this student to be self directed Yes No Student may self carry and self administer medication Yes No Note: Nurse will also assess self-direction for the school setting. Please advise parent to send in additional medication in the event that emergency sheltering is necessary at school or if morning medication has not been given.
Free from contagions & physically qualified for all physical education, sports, playground, work & school activities OR only as checked:
___ Limited contact: cheerlead, gymnastics, ski, volleyball, cross-country, handball, fence, baseball, floor hockey, softball.
___ Non-contact: badminton, bowl, golf, swim, table tennis, archery, riflery, weight train, crew, dance, track, run, walk, rope jump.
Specify medical accommodations needed for school: __________________________________________________________________ None
Known or suspected disability: ____________________________________________________________________________________ Please monitor
Restrictions: ___________________________________________________________________________________________________ Please monitor
Protective equipment required: Athletic Cup Support goggles/impact resistant eyewear Other: _________________________________
Provider’s Signature: __________________________________________________________________ Phone: _____________________________
Provider’s Name/ address: ______________________________________________________________ Fax: _______________________________
Parent Signature: _____________________________________________________________________ Date: ______________________________
This exam complies with NYSED requirements above and is valid for twelve months, with the exception of any illness or injury lasting more that five days that will
require review by private healthcare and the school medical director. DH #6new 1/08
IMMUNIZATIONS/ HEALTH HISTORY
PHYSICAL EXAMS
Body Mass Index: ______ ______ - ______
Weight Status Category (BMI Percentile):
Less than 5th 5th through 49th 50th through 84th
85th through 94th 95th through 98th 99th and higher
Vision - without glasses/contact lenses R L
Vision – with glasses/ contact lenses R L
Vision – Near Point R L
Hearing ___ Pass 20 db sc both ears or: R L
MEDICATIONS
PHYSICAL EDUCATION / SPORTS / PLAYGROUND / WORK QUALIFICATION / CSE CONSIDERATION
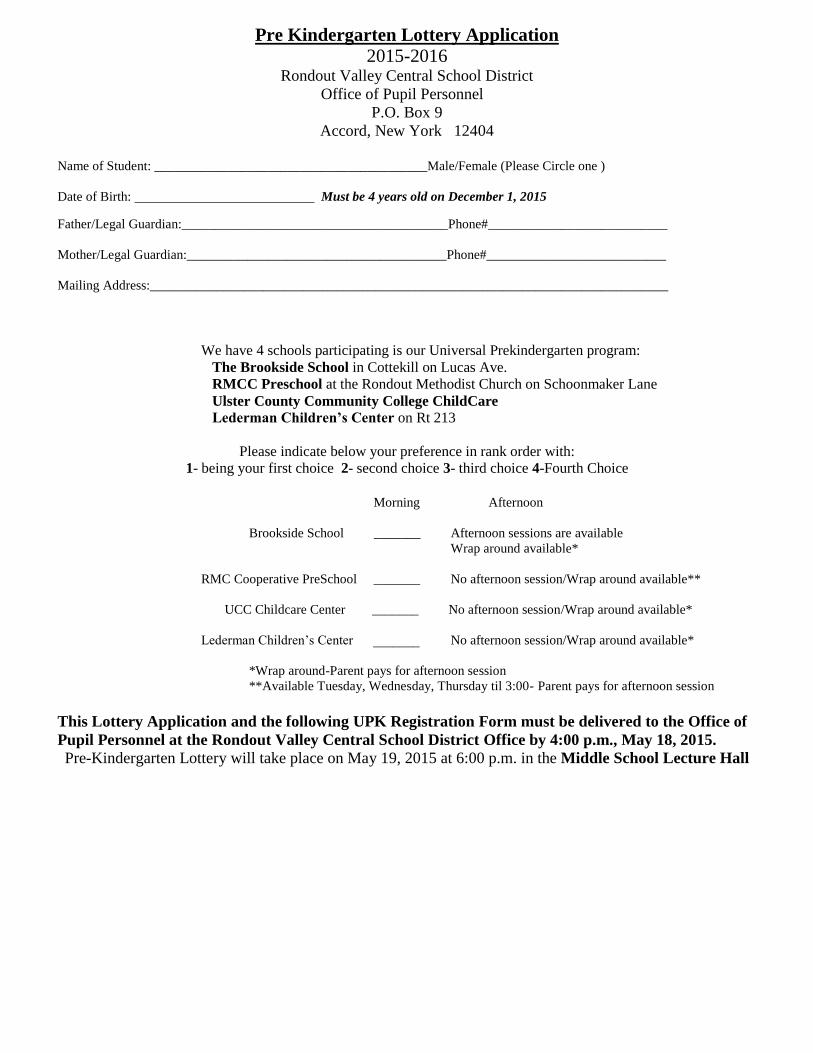
Pre Kindergarten Lottery Application
2015-2016 Rondout Valley Central School District
Office of Pupil Personnel
P.O. Box 9
Accord, New York 12404
Name of Student: _________________________________________Male/Female (Please Circle one )
Date of Birth: Must be 4 years old on December 1, 2015
Father/Legal Guardian:________________________________________Phone#___________________________
Mother/Legal Guardian:_______________________________________Phone#___________________________
Mailing Address:______________________________________________________________________________
We have 4 schools participating is our Universal Prekindergarten program:
The Brookside School in Cottekill on Lucas Ave.
RMCC Preschool at the Rondout Methodist Church on Schoonmaker Lane
Ulster County Community College ChildCare
Lederman Children’s Center on Rt 213
Please indicate below your preference in rank order with:
1- being your first choice 2- second choice 3- third choice 4-Fourth Choice
Morning Afternoon
Brookside School _______ Afternoon sessions are available
Wrap around available*
RMC Cooperative PreSchool _______ No afternoon session/Wrap around available**
UCC Childcare Center _______ No afternoon session/Wrap around available*
Lederman Children’s Center _______ No afternoon session/Wrap around available*
*Wrap around-Parent pays for afternoon session
**Available Tuesday, Wednesday, Thursday til 3:00- Parent pays for afternoon session
This Lottery Application and the following UPK Registration Form must be delivered to the Office of
Pupil Personnel at the Rondout Valley Central School District Office by 4:00 p.m., May 18, 2015.
Pre-Kindergarten Lottery will take place on May 19, 2015 at 6:00 p.m. in the Middle School Lecture Hall

RONDOUT VALLEY CENTRAL SCHOOL DISTRICT – UPK REGISTRATION FORM
Student First Name Middle Name
Student Last Name
Physical Address
(Street Address) (City) (State) (Zip)
Mailing Address
(if different)
(PO Box/address) (City) (State) (Zip)
Town/Village of Residence Email Address:
Mother Father (Please circle one)
Father/Legal Guardian’s Name: Mother/Legal Guardian’s Name:
Student’s Sex M F
Student’s Date of Birth: Special Programs/IEP:
Student’s Place of Birth
(City) (State) (Zip)
Date of Entry (if not born in US)
Country of Origin
Number of years in US Schools: What languages does the student understand?
Home Language
What language does student:
Read
Write
Race (circle one) Hispanic Non-Hispanic International Adoption?
YES NO
Date of Adoption ____________
Ethnicity (circle one):
I – American Indian or Native America
A – Asian
B- Black or African American
H – Hispanic or Latino
P – Native American or other Pacific Islander
W - White
Citizenship Status (check one)
Dual Nation:
Non-resident alien:
US Citizen:
Other:
Date of 1st Polio
Immunization:
RESIDENCY INFORMATION –( please circle one)
Student lives with: Both Parents Father Mother Legal Guardian Stepparent
Relative Relationship:
Foster Home PLEASE NOTE PLACEMENT AGENCY & ADDRESS:
STUDENT LIVING ARRANGEMENTS
Is the student homeless? …………………………………………………………………………………………..
Is the student living in a shelter:……………………………………………………………………………………
Is the student living with relatives due to lack of housing?................................................................. .....................
Is the student living in an abandoned apartment/building?.......................................................................................
Is the student living in a motel/hotel?...................................................................................... ..................................
Is the student living in a campground, car, train/bus station or other similar situation due to lack of alternative,
adequate housing?.................................................................................................... ..................................................
Is the student temporarily housed in a shelter awaiting OCF’S permanent foster care placement?.........................
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO

TELEPHONE NUMBERS
(Fill out employer information only for parent(s), Legal Guardian or Relative that student lives with)
HOME# WORK# CELL#
Father
Father’s Employer
Mother
Mother’s Employer
Guardian
Guardian’s Employer
Relative
Relative’s Employer
****EMERGENCY NUMBERS****
Name
Relationship
Address Permission to pick up student: YES NO
Phone # Cell #
OTHER CHILDREN
Sex Date of Birth Attending Rondout?
Brother’s Names Yes No
Sister’s Names
RONDOUT VALLEY CENTRAL SCHOOL DISTRICT P.O. Box 9
Accord, New York 12404
Mr. Rosario Agostaro Dr. Timothy Wade
Superintendent of Schools Deputy Superintendent
845-687-2400 Ext. 4802 845-687-2400 Ext. 4863
Mrs. Lisa Pacht Mrs. Debra Kosinski
Executive Director for Curriculum & Instruction School Business Administrator
845-687-2400 Ext. 4805 845-687-2400 Ext. 4812
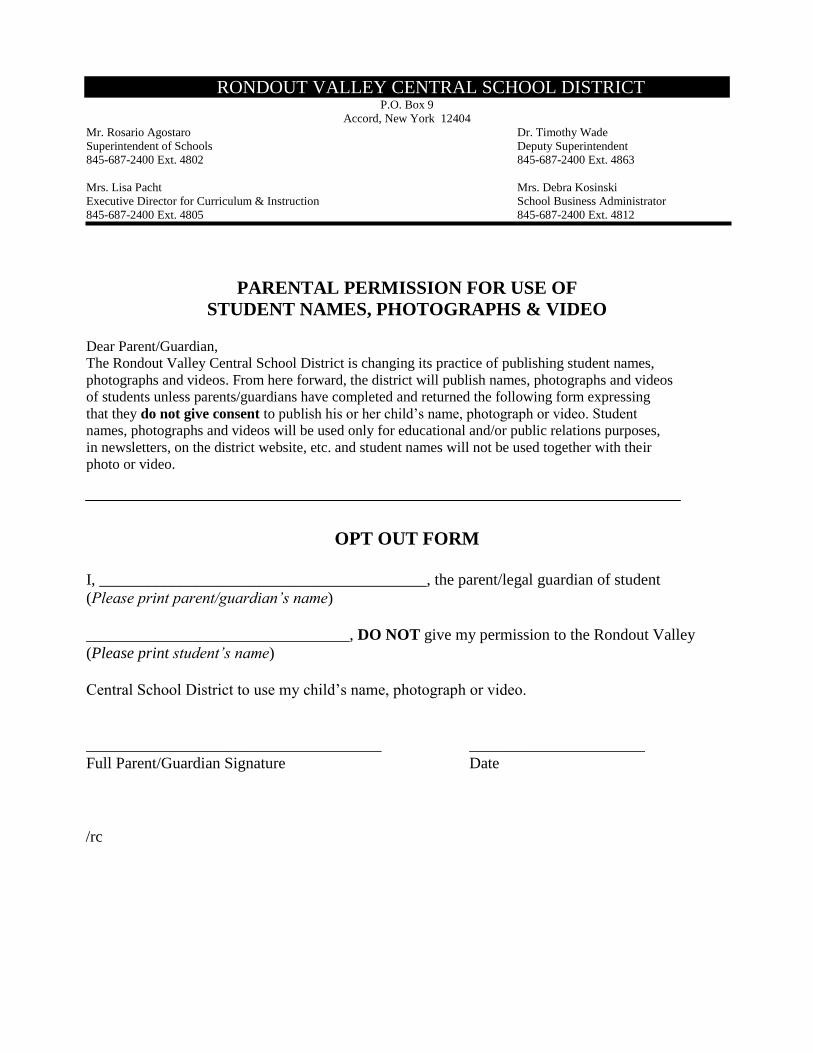
PARENTAL PERMISSION FOR USE OF
STUDENT NAMES, PHOTOGRAPHS & VIDEO Dear Parent/Guardian,
The Rondout Valley Central School District is changing its practice of publishing student names,
photographs and videos. From here forward, the district will publish names, photographs and videos
of students unless parents/guardians have completed and returned the following form expressing
that they do not give consent to publish his or her child’s name, photograph or video. Student
names, photographs and videos will be used only for educational and/or public relations purposes,
in newsletters, on the district website, etc. and student names will not be used together with their
photo or video.
OPT OUT FORM
I, _________________________________________, the parent/legal guardian of student
(Please print parent/guardian’s name)
_________________________________, DO NOT give my permission to the Rondout Valley
(Please print student’s name)
Central School District to use my child’s name, photograph or video.
_____________________________________ ______________________
Full Parent/Guardian Signature Date
/rc
RONDOUT VALLEY CENTRAL SCHOOL DISTRICT P.O. Box 9
Accord, New York 12404 Mr. Rosario Agostaro Dr. Timothy Wade Superintendent of Schools Deputy Superintendent 845-687-2400 Ext. 4802 845-687-2400 Ext. 4863 Mrs. Lisa I. Pacht Mrs. Debra Kosinski Executive Director of Curriculum & Instruction School Business Administrator 845-687-2400 Ext. 4805 845-687-2400 Ext. 4812
Dear Parent/Guardian, We have the capability of sending phone calls, e-mails, and/or text messages to inform you of school delays, emergency closings, and upcoming events in the district. This is accomplished through an automated system which we use to contact parents, students, and staff. If you would like the district to register you for this service, please fill in this form and either return it to your child’s school or mail it to RVCSD, Attn: Louann Miszko, P.O. Box 9, Accord, NY 12404. Thank you, Superintendent Rosario Agostaro
Parent/Guardian Name________________________________________________________ Student Name _______________________________________________________________ I would like the Rondout Valley Central School District to send me notifications about:
Emergency Closings/Delays ____ Upcoming Community Events ____
Please list information below regarding how you would like to receive the reminders. I prefer to receive notifications through a(n):
Phone call @__________________________ @____________________________
E‐mail @__________________________ @____________________________
Text message @__________________________ @____________________________
Should you have any questions, please contact Ms. Randi Chase in the Technology Office at the following phone number: 845-687-2400 extension 4851.