role of nutrition in diabetes - american association of ... have diabetes, dyslipidemia and gout. no...
TRANSCRIPT
Role of Nutrition in Diabetes
Osama Hamdy MD PhD FACE Medical Director Obesity Clinical Program
Director of Inpatient Diabetes Management
Joslin Diabetes Center
Assistant Professor of Medicine
Harvard Medical School
You have diabetes dyslipidemia and gout No problem Just avoid any food that contains carbohydrates fat or protein and you will be fine
The Impact of Diet on Diabetes Known Before the Era of Diabetes Medications
1869-1962
Joslin Clinic Boston MA
1879ndash1964
Physiatric Institute Morristown NJ
Elliott P Joslin Frederick M Allen
Die of diabetes or risk inanition ldquoStarvation due to inability to acquire tolerance for any living diet
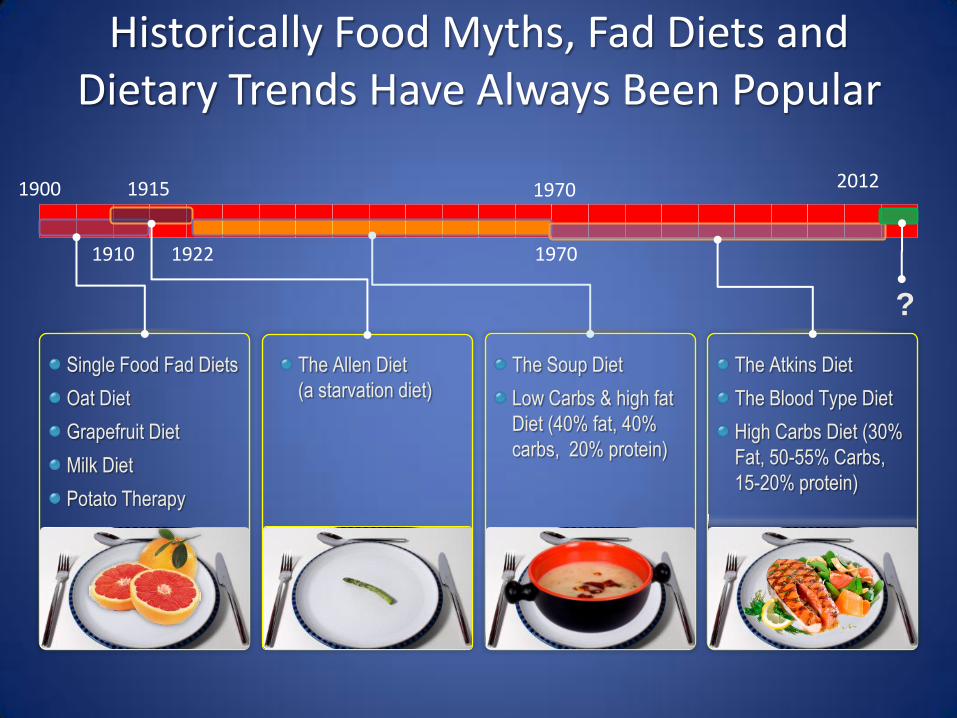
The Allen Diet
(a starvation diet)
The Atkins Diet
The Blood Type Diet
High Carbs Diet (30
Fat 50-55 Carbs
15-20 protein)
The Soup Diet
Low Carbs amp high fat
Diet (40 fat 40
carbs 20 protein)
Single Food Fad Diets
Oat Diet
Grapefruit Diet
Milk Diet
Potato Therapy
Historically Food Myths Fad Diets and Dietary Trends Have Always Been Popular
1900 1915
1922 1910 1970
1970 2012
Objectives
bull Nutrition targets in diabetes management
bull Current recommendations and the slow adaptation of evidence
bull Looking Ahead
ndash Macronutrients
bull Protein content
bull Carbohydrates
ndash Micronutrients
Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
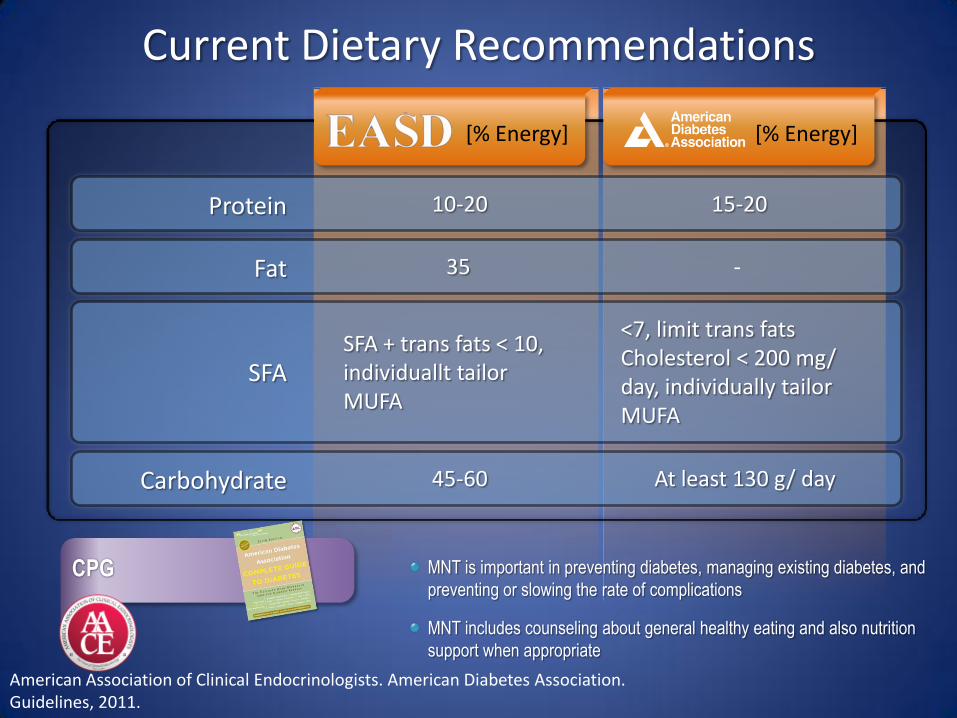
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
You have diabetes dyslipidemia and gout No problem Just avoid any food that contains carbohydrates fat or protein and you will be fine
The Impact of Diet on Diabetes Known Before the Era of Diabetes Medications
1869-1962
Joslin Clinic Boston MA
1879ndash1964
Physiatric Institute Morristown NJ
Elliott P Joslin Frederick M Allen
Die of diabetes or risk inanition ldquoStarvation due to inability to acquire tolerance for any living diet
The Allen Diet
(a starvation diet)
The Atkins Diet
The Blood Type Diet
High Carbs Diet (30
Fat 50-55 Carbs
15-20 protein)
The Soup Diet
Low Carbs amp high fat
Diet (40 fat 40
carbs 20 protein)
Single Food Fad Diets
Oat Diet
Grapefruit Diet
Milk Diet
Potato Therapy
Historically Food Myths Fad Diets and Dietary Trends Have Always Been Popular
1900 1915
1922 1910 1970
1970 2012
Objectives
bull Nutrition targets in diabetes management
bull Current recommendations and the slow adaptation of evidence
bull Looking Ahead
ndash Macronutrients
bull Protein content
bull Carbohydrates
ndash Micronutrients
Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
The Impact of Diet on Diabetes Known Before the Era of Diabetes Medications
1869-1962
Joslin Clinic Boston MA
1879ndash1964
Physiatric Institute Morristown NJ
Elliott P Joslin Frederick M Allen
Die of diabetes or risk inanition ldquoStarvation due to inability to acquire tolerance for any living diet
The Allen Diet
(a starvation diet)
The Atkins Diet
The Blood Type Diet
High Carbs Diet (30
Fat 50-55 Carbs
15-20 protein)
The Soup Diet
Low Carbs amp high fat
Diet (40 fat 40
carbs 20 protein)
Single Food Fad Diets
Oat Diet
Grapefruit Diet
Milk Diet
Potato Therapy
Historically Food Myths Fad Diets and Dietary Trends Have Always Been Popular
1900 1915
1922 1910 1970
1970 2012
Objectives
bull Nutrition targets in diabetes management
bull Current recommendations and the slow adaptation of evidence
bull Looking Ahead
ndash Macronutrients
bull Protein content
bull Carbohydrates
ndash Micronutrients
Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
The Allen Diet
(a starvation diet)
The Atkins Diet
The Blood Type Diet
High Carbs Diet (30
Fat 50-55 Carbs
15-20 protein)
The Soup Diet
Low Carbs amp high fat
Diet (40 fat 40
carbs 20 protein)
Single Food Fad Diets
Oat Diet
Grapefruit Diet
Milk Diet
Potato Therapy
Historically Food Myths Fad Diets and Dietary Trends Have Always Been Popular
1900 1915
1922 1910 1970
1970 2012
Objectives
bull Nutrition targets in diabetes management
bull Current recommendations and the slow adaptation of evidence
bull Looking Ahead
ndash Macronutrients
bull Protein content
bull Carbohydrates
ndash Micronutrients
Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
Objectives
bull Nutrition targets in diabetes management
bull Current recommendations and the slow adaptation of evidence
bull Looking Ahead
ndash Macronutrients
bull Protein content
bull Carbohydrates
ndash Micronutrients
Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Overweight or obese (+ large waist line) Postprandial hyperglycemia Postprandial hypertriglyceridemia Insulin resistance (increased HGP and decreased PGD) Hyperinsulinemia (pre- and early diabetes) Low HDL Increased cytokines (inflammatory coagulation) Endothelial dysfunction High risk for coronary and cerebral vascular disease Continue to gain weight on medications Decreased EE (decreased PA and TEF)
Major Problems in Patients with Type 2 DM (Nutrition Targets)
Hypertension + High small dense-LDL
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
Current Dietary Recommendations
[ Energy] [ Energy]
10-20 15-20 Protein
35 - Fat
SFA + trans fats lt 10 individuallt tailor MUFA
lt7 limit trans fats Cholesterol lt 200 mg day individually tailor MUFA
SFA
45-60 At least 130 g day Carbohydrate
CPG MNT is important in preventing diabetes managing existing diabetes and
preventing or slowing the rate of complications
MNT includes counseling about general healthy eating and also nutrition
support when appropriate
American Association of Clinical Endocrinologists American Diabetes Association Guidelines 2011
Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Current Protein Recommendations
bull Diabetes and normal renal function 15-20 of total energy intake (E)
bull Diabetes with early stages of CKD 08-1 gmkgday (B)
bull Diabetes with later stages of CKD 08 gmkgday (B)
bull High protein diet are not recommended as method for weight loss at this time (E)
bull MNT that favorably affects cardiovascular risk factors may improve microvascular complications (retinopathy nephropathy) (C)
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
What About Protein
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
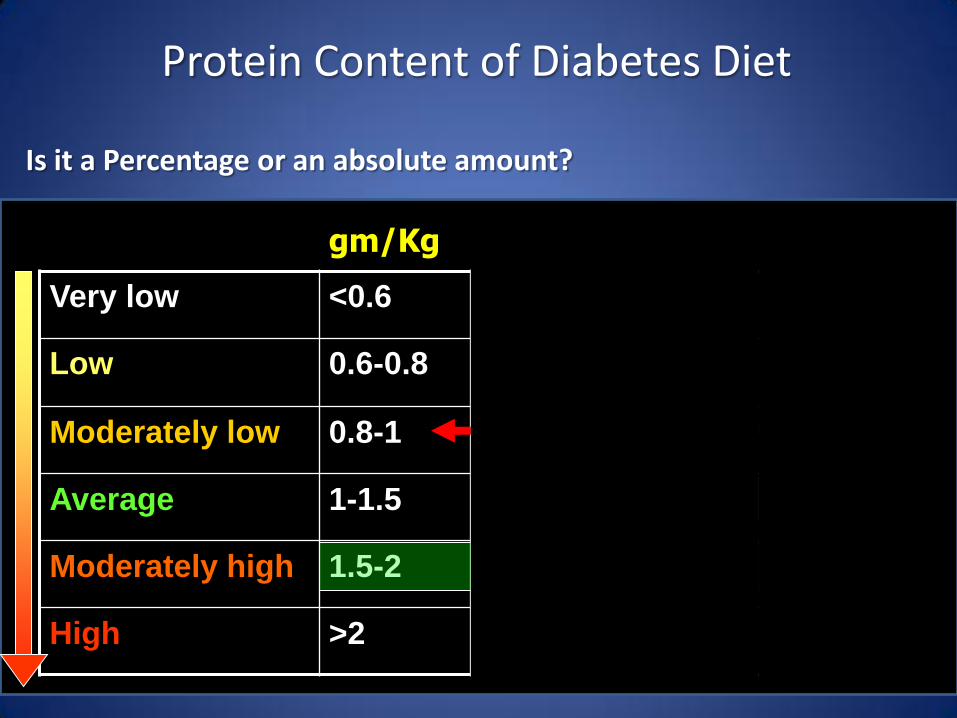
Protein Content of Diabetes Diet
Is it a Percentage or an absolute amount
Very low lt06 lt35 lt7 lt26
Low 06-08 35-56 7-11 26-41
Moderately low 08-1 56-70 11-14 41-52
Average 1-15 70-105 14-21 52-79
Moderately high 15-2 105-140 21-28 79-105
High gt2 gt140 gt28 gt105
gmKg 2000 Cal 1500
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
Low Protein and Progression of Kidney disease in Diabetic Patients
Type 1 DM Many RCTs showed that reducing protein intake to 08 gmkgday in patients with overt nephropathy decreases proteinuria reduces the decline in GFR risk of renal failure and death
Type 2 DM Very little or no data
No evidence to show that increased protein intake in patients with
normal kidney function will induce microalbuminuria or cause decline
in GFR
High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

High Protein Diets Improve CV Outcomes (Nurses Health Study)
Hu et al Am J Clin Nutr 1999 70221
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
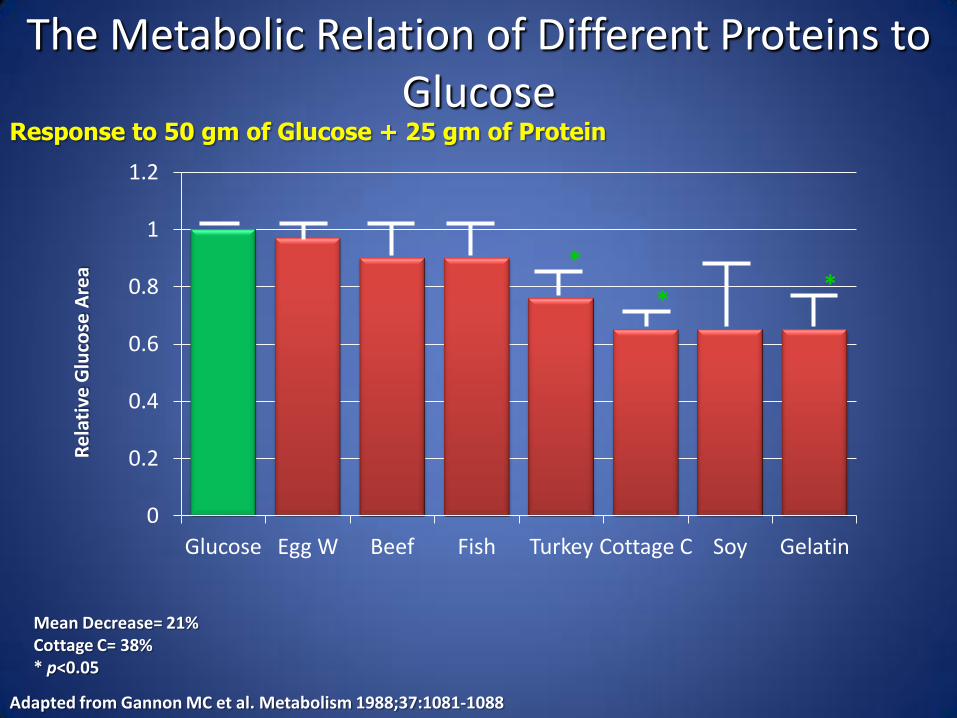
Response to 50 gm of Glucose + 25 gm of Protein
Adapted from Gannon MC et al Metabolism 1988371081-1088
The Metabolic Relation of Different Proteins to Glucose
Re
lati
ve G
luco
se A
rea
Mean Decrease= 21 Cottage C= 38 plt005
0
02
04
06
08
1
12
Glucose Egg W Beef Fish Turkey Cottage C Soy Gelatin
Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Change in HbA1c after 5 weeks
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different Protein Ratios in Type 2 DM
Ch
ange
in H
bA
1c
n= 12
-1
-08
-06
-04
-02
0
02
0 1 2 3 4 5
15 protein
30 protein
Weeks
Pioglitazone 45 mg 16 weeks - 07 Metformin 2500 mg 29 weeks - 14 30 protein diet 5 weeks - 08 (16)
Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Effect of High Protein Intake on Renal Function (Nurses Health Study)
plt005
Normal Renal Function
n=1153
Mild Renal Insufficiency
n=489
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Unadjusted
-025
(95CI -078-128)
-169
(95CI -293- -045)
Decline of estimated GFR10 grams of protein increase
(mlmin173 m2)
Adjusted
-114
(95CI -383-475)
-772
(95CI -1552-008)
Study Conclusion High protein intake was not associated with renal function decline in women with normal kidney function
Knight et al Ann Intern Med 2003138460-467
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
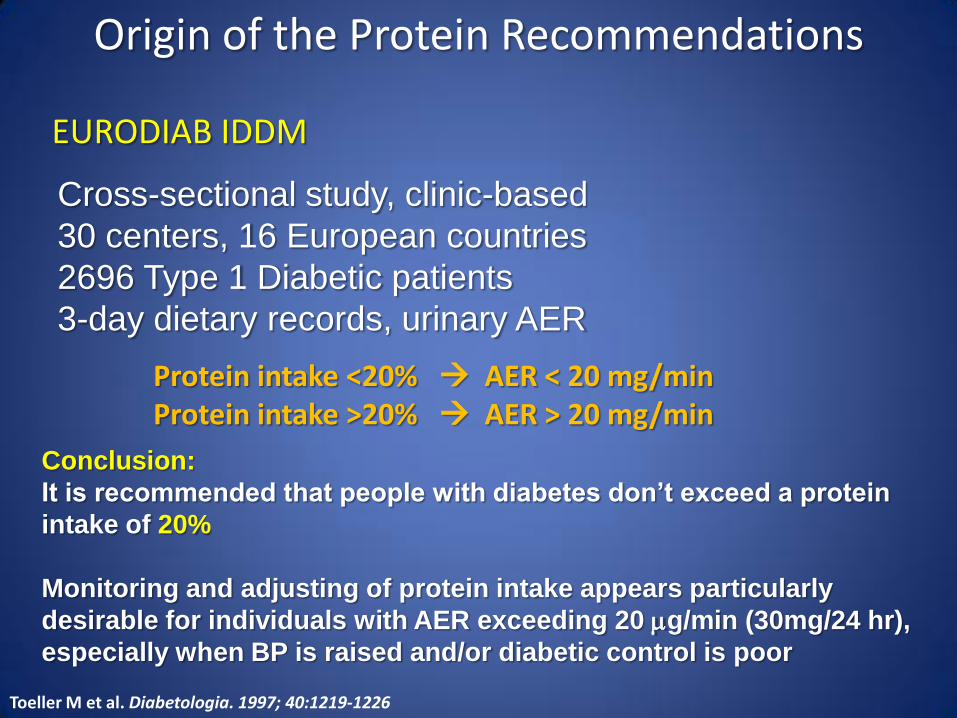
Cross-sectional study clinic-based
30 centers 16 European countries
2696 Type 1 Diabetic patients
3-day dietary records urinary AER
Origin of the Protein Recommendations
Toeller M et al Diabetologia 1997 401219-1226
EURODIAB IDDM
Protein intake lt20 AER lt 20 mgmin Protein intake gt20 AER gt 20 mgmin Conclusion
It is recommended that people with diabetes donrsquot exceed a protein
intake of 20
Monitoring and adjusting of protein intake appears particularly
desirable for individuals with AER exceeding 20 mgmin (30mg24 hr)
especially when BP is raised andor diabetic control is poor
HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

HbA1c lt64 (n=1007)
HbA1c gt64 (n=999)
Hypertensives (619)
Normotensives (2050)
Toeller M et al Diabetologia 1997 401219-1226
Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Higher Dietary Fat Correlates with Microalbuminuria whereas Higher Protein Correlates with Lower Urine Albumin Levels
Riley MD Dwyer T Am J Clin Nutr 199867(1)50-7
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
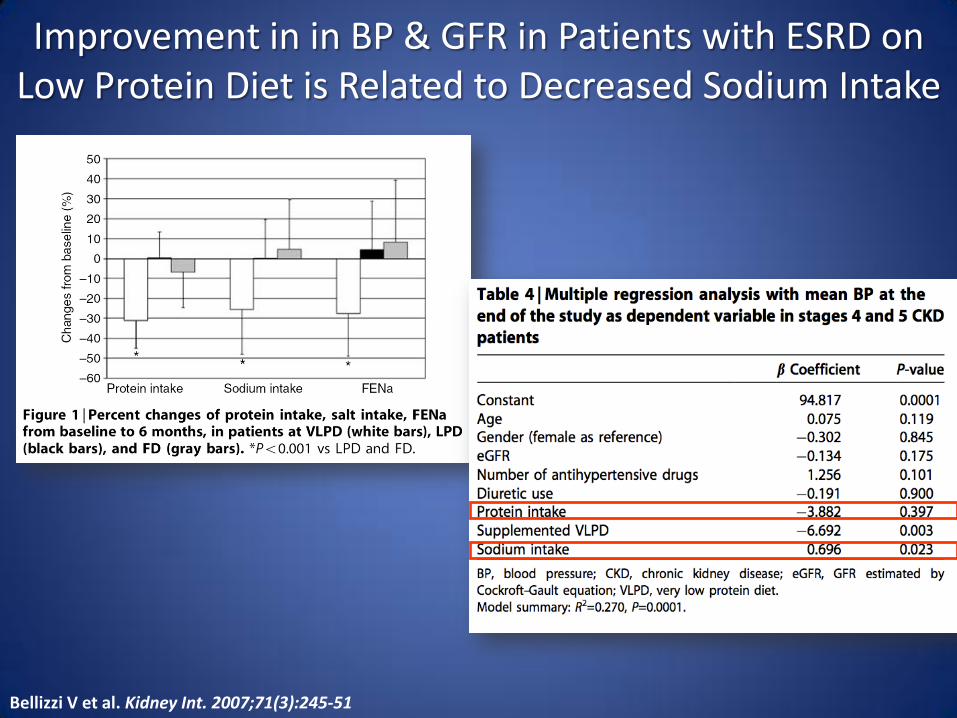
Bellizzi V et al Kidney Int 200771(3)245-51
Improvement in in BP amp GFR in Patients with ESRD on Low Protein Diet is Related to Decreased Sodium Intake
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
What about Carbohydrates
General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

General Carbohydrates Recommendations
bull 50-60 of total kcal
bull Three types of carbohydrates (sugars starch and fiber) with different impact on blood glucose level
bull Consume at least 7-10 servingsday of healthy carbohydrates (fresh fruits vegetables pulses [legumes beans and peas] and whole grains)
bull Low glycemic index foods (lt 55) facilitate glycemic control
bull Fiber intake should be 14 g1000 kcald or 25-30 gd
bull Sugar substitutes are safe within ranges provided by the US FDA
Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Twenty-fourndashhour plasma glucose
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from control diet
P lt 005
Twenty-fourndashhour triacylglycerol
response of subjects to the control (15
protein) and high-protein (30 protein)
diets
Significantly different from the fasting
control value P lt 003
Adapted from Gannon MC et al Amer J Clin Nutr 200378734-741
The Metabolic Effect of Different ProteinCarbohydrates Ratios in Type 2 DM
Protein to carbohydrate to fat 304030 Versus 155530
-40 Reduction
50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

50
100
150
Before Diet
After Diet
-50
-40
-30
-20
-10
0
High Carbohydrates
Low Carbohydrates V
isce
ral F
at (
cm2)
D
ecr
eas
e in
bas
al I
nsu
lin
(Week)
Miyashita Y et al Diabetes Res Clin Pract 2004 Sep65(3)235-41
Effects of Lower Carbohydrates in Low Calorie Diet on
Visceral Fat and Basal Insulin in Obese Patients with Type 2
Diabetes C F P Low Carbs 39 35 25 High Carbs 62 10 26
-10
0
10
20
C
han
ge in
HD
L-C
No Difference in Reduction of Weight Lean Mass Total Fat TC TG 1 2 3 4
Week
n= 22 plt005
plt001
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
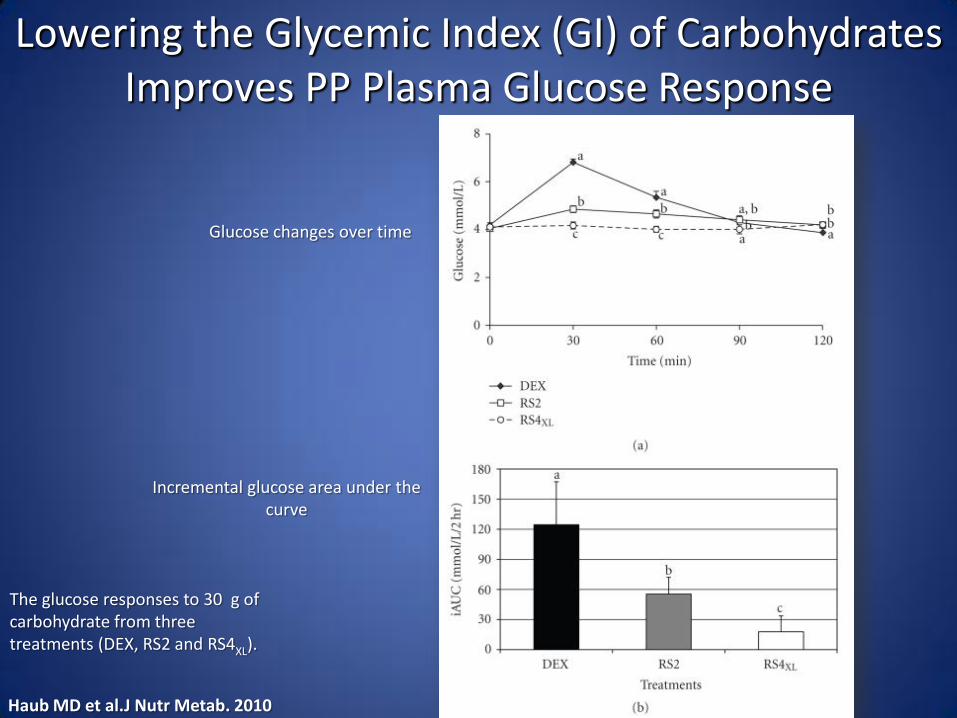
The glucose responses to 30 g of carbohydrate from three treatments (DEX RS2 and RS4XL)
Haub MD et alJ Nutr Metab 2010
Glucose changes over time
Incremental glucose area under the curve
Lowering the Glycemic Index (GI) of Carbohydrates Improves PP Plasma Glucose Response
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
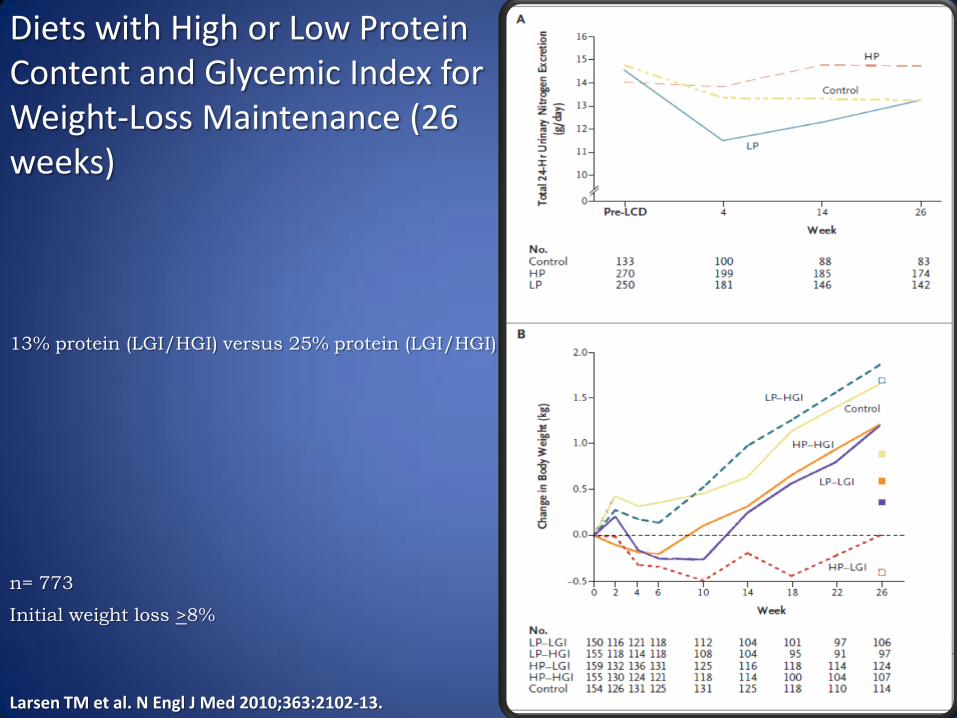
Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance (26 weeks)
Initial weight loss gt8
n= 773
Larsen TM et al N Engl J Med 20103632102-13
13 protein (LGIHGI) versus 25 protein (LGIHGI)
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
What about Weight Reduction
bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

bull Maintenance of body weight requires 25-30 kcalkgday
bull Weight reduction of 5-10 has significant impact on metabolic and cardiovascular risk factors in overweight and obese patients with diabetes Aim for a BMI of 20-25 kgM2
bull Modest caloric reduction of ~500 kcald results in a weight loss of 1 poundwk
bull Reduction of total carbohydrates to ~40 of the caloric intake and increase of protein to 15-2 gmadjusted body weight are effective dietary tools
bull Diabetes specific meal replacements are useful tools (1-2day)
bull Increase of physical activity to 175-300 minweek in short bouts of 10 min each with emphasis on strength training are effective for weight reduction and maintenance
Weight Reduction Improves Metabolic and CV Risk Factors
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
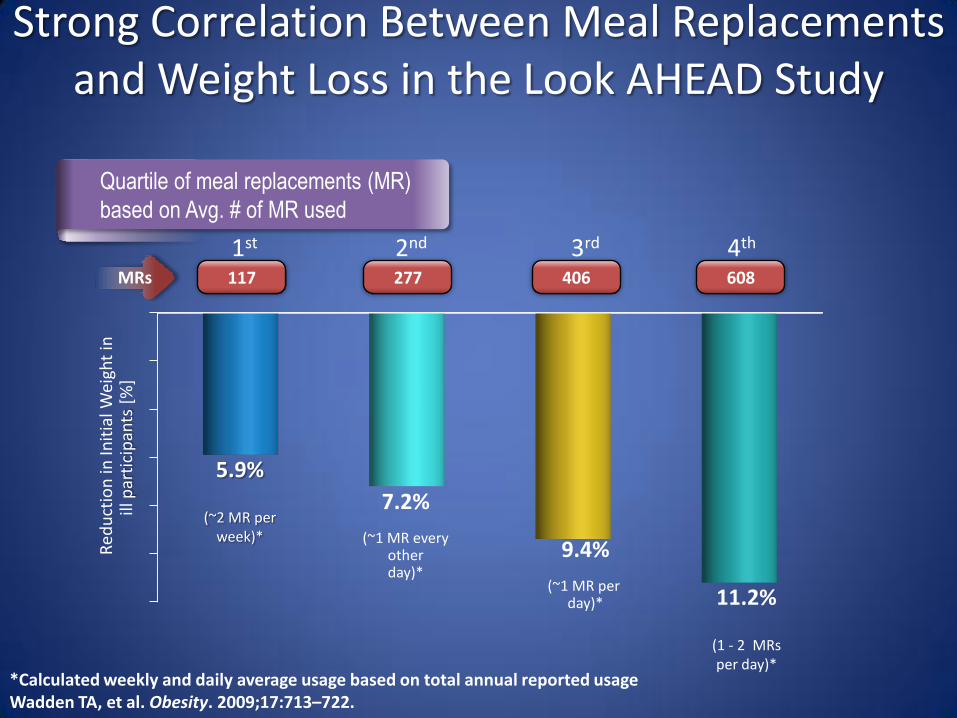
Strong Correlation Between Meal Replacements and Weight Loss in the Look AHEAD Study
Quartile of meal replacements (MR)
based on Avg of MR used
Red
uct
ion
in In
itia
l Wei
ght
in
ill p
arti
cip
ants
[
]
117 277 406 608 MRs
1st 2nd 3rd 4th
Calculated weekly and daily average usage based on total annual reported usage Wadden TA et al Obesity 200917713ndash722
59
(~2 MR per week)
72
(~1 MR every other day)
94
(~1 MR per day) 112
(1 - 2 MRs per day)
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012
Take Home Message
1 Medical Nutrition Therapy is a key component of overall diabetes management
2 Many targets in comprehensive diabetes care are missed with the current diabetes nutrition recommendations
3 Protein intake may be increased in the nutrition plan of patients with type 2 diabetes and normal kidney function
4 Protein should be calculated as gmkg especially when hypocaloric diet is recommended
5 Reduction of carbohydrates load to ~40-45 may improve diurnal plasma glucose and triglycerides increase HDL-cholesterol and reduce visceral fat
6 Meal replacement is a key component of weight reduction for overweight and obese patients with type 2 diabetes
7 Adequacy of micronutrients is integral part of MNT for patients with diabetes
Thank You 5232012

Thank You 5232012