roger h. peters, ph.d., university of south florida; [email protected] co-occurring disorders 102
TRANSCRIPT

Roger H. Peters, Ph.D., Roger H. Peters, Ph.D., University of South Florida; [email protected] of South Florida; [email protected]
Co-Occurring Disorders 102
Goals of this Presentation
Review:• Available screening instrumentsAvailable screening instruments• Conceptual model to drive COD Conceptual model to drive COD
services (Risk-Need-Responsivity)services (Risk-Need-Responsivity)• Treatment modifications for CODsTreatment modifications for CODs• Special populations and CODsSpecial populations and CODs
2

Defining “Co-Occurring Disorders”
The presence of at least two disorders:The presence of at least two disorders: A substance abuse or dependence A substance abuse or dependence
disorderdisorder A DSM-IV major mental disorder, A DSM-IV major mental disorder,
usually Major Depression, Bipolar usually Major Depression, Bipolar Disorder, or SchizophreniaDisorder, or Schizophrenia
3
Survey Results:Offender Screening
Wide variation Wide variation in types of SA in types of SA screening instruments administeredscreening instruments administered
32%32% of sites used no SA screening of sites used no SA screening instrumentsinstruments
42%42% of sites did not use a of sites did not use a standardized SA screening standardized SA screening instrumentinstrument(Taxman et al., 2007)(Taxman et al., 2007)
4
Screening for CODs
• Routine screening for both sets of disordersRoutine screening for both sets of disorders• Criminal risk levelCriminal risk level• Acute MH and SA symptoms:Acute MH and SA symptoms:
• Suicidal thoughts and behaviorSuicidal thoughts and behavior• Depression, hallucinations, delusionsDepression, hallucinations, delusions• Potential for drug/alcohol withdrawalPotential for drug/alcohol withdrawal• History of MH treatment including use of medsHistory of MH treatment including use of meds
• Determine need/urgency for referralDetermine need/urgency for referral

Screening—Mental Health
• Brief Jail Mental Health ScreenBrief Jail Mental Health Screen• Mental Health Screening Form–IIIMental Health Screening Form–III• MINI–MMINI–M• CODSI CODSI (Sacks et al, 2007)(Sacks et al, 2007)
• GAIN–SSGAIN–SS
6

Screening—Substance Abuse
• Simple Screening Instrument Simple Screening Instrument • TCU Drug Screen–II TCU Drug Screen–II • ASI–Alcohol and Drug Abuse sectionsASI–Alcohol and Drug Abuse sections• GAIN–SSGAIN–SS
7
Screening—Trauma and PTSD
• Clinician-Administered PTSD Scale for Clinician-Administered PTSD Scale for DSM-IVDSM-IV
• Impact of Events ScaleImpact of Events Scale• Primary Care PTSD ScreenPrimary Care PTSD Screen• PTSD Checklist–Civilian VersionPTSD Checklist–Civilian Version• Trauma Symptom InventoryTrauma Symptom Inventory
8

Specialized Screens
• BASIS-24 BASIS-24 • Centre for Addiction and Mental Health Centre for Addiction and Mental Health
Concurrent Disorders Screener (CAMH-Concurrent Disorders Screener (CAMH-CDS) CDS)
• Psychiatric Diagnostic Screening Psychiatric Diagnostic Screening Questionnaire (PDSQ) Questionnaire (PDSQ)
9
Instruments for Adolescents • CAFASCAFAS• GAIN GAIN • MAYSI-2MAYSI-2• PESQPESQ• POSIT POSIT
10

Other Screening Domains
• MotivationMotivation• Offender Risk and NeedsOffender Risk and Needs• Trauma and PTSDTrauma and PTSD
11
Instruments—Motivation and Stages of Change • CMRSCMRS
• RCQRCQ
• SOCRATESSOCRATES
• TCU Treatment Motivation ScalesTCU Treatment Motivation Scales
• URICAURICA
12

Instruments—Offender Risk and Needs• HCR-20HCR-20
• LCSFLCSF
• LSI-RLSI-R
• PCL-SVPCL-SV
• RANTRANT
• STARTSTART
13
Trauma and Victimization
• Female offenders frequently have been Female offenders frequently have been victims of physical or sexual violencevictims of physical or sexual violence
• Trauma history—should be expectation Trauma history—should be expectation for women in CJ settingsfor women in CJ settings
• Impact of violence is widespread, can Impact of violence is widespread, can impair recovery from MH and SA impair recovery from MH and SA disordersdisorders
Trauma and PTSD Screening Issues
• PTSD and trauma are often PTSD and trauma are often overlooked in screeningoverlooked in screening
• Other diagnoses are used to Other diagnoses are used to explain symptomsexplain symptoms
• Result—lack of specialized Result—lack of specialized treatment, symptoms masked, poor treatment, symptoms masked, poor outcomesoutcomes
Screening for Trauma and PTSD• All women should be screened for trauma All women should be screened for trauma
history across different justice settingshistory across different justice settings• Initial screen does not have to be conducted Initial screen does not have to be conducted
by a mental health clinician; doesn’t require by a mental health clinician; doesn’t require discussion of specific detailsdiscussion of specific details
• Many simple, non-proprietary screening Many simple, non-proprietary screening instruments availableinstruments available
• Positive screens should be referred for more Positive screens should be referred for more comprehensive assessment comprehensive assessment
16

Screening Instruments for Trauma and PTSD
• Clinician-Administered PTSD Scale for Clinician-Administered PTSD Scale for DSM-IV (CAPS) DSM-IV (CAPS)
• Impact of Events Scale (IES)Impact of Events Scale (IES)• Primary Care PTSD Screen (PC-PTSD)Primary Care PTSD Screen (PC-PTSD)• PTSD Checklist—Civilian Version (PCL-PTSD Checklist—Civilian Version (PCL-
C)C)• Trauma Symptom Inventory (TSI) Trauma Symptom Inventory (TSI)
17
Admission Criteria and CODs• Excluding persons with CODs is NOT a viable Excluding persons with CODs is NOT a viable
optionoption• How to determine eligibility for services?How to determine eligibility for services?• Triage to specialized COD servicesTriage to specialized COD services• Target moderate to high criminal risk levelsTarget moderate to high criminal risk levels

Assessing Program Eligibility 1.1. Review existing program resources to work Review existing program resources to work
with co-occurring disorderswith co-occurring disorders Staff with MH and SA treatment experience Staff with MH and SA treatment experience Linkages with institutional and community-Linkages with institutional and community-
based MH and SA services based MH and SA services Specialized “tracks,” groups, or other Specialized “tracks,” groups, or other
services for co-occurring disordersservices for co-occurring disorders Psychiatric/medication consultationPsychiatric/medication consultation
19
Assessing Program Eligibility 2. Determine functioning level required for 2. Determine functioning level required for
program participationprogram participation Treatment groups Treatment groups Therapeutic communities Therapeutic communities Community supervision Community supervision Employment and peer support Employment and peer support
programsprograms
20
Assessing Program Eligibility 3. Examine broad categories of functioning3. Examine broad categories of functioning
Cognitive functioningCognitive functioning Major mental health symptomsMajor mental health symptoms Unusual behaviorsUnusual behaviors Ability to interact with staff and Ability to interact with staff and
participants (e.g., group settings)participants (e.g., group settings) How responds to stressHow responds to stress Reading, language abilitiesReading, language abilities
21
Key Assessment Information
• Scope and severityScope and severity of MH and SA disorders of MH and SA disorders• Pattern of interactionPattern of interaction between the disorders between the disorders• Conditions associated with Conditions associated with occurrence and occurrence and
maintenancemaintenance of the disorders of the disorders• Criminal-antisocial beliefsCriminal-antisocial beliefs• MotivationMotivation for treatmentfor treatment• Family and social Family and social relationshipsrelationships• Physical healthPhysical health status and medical history status and medical history
22
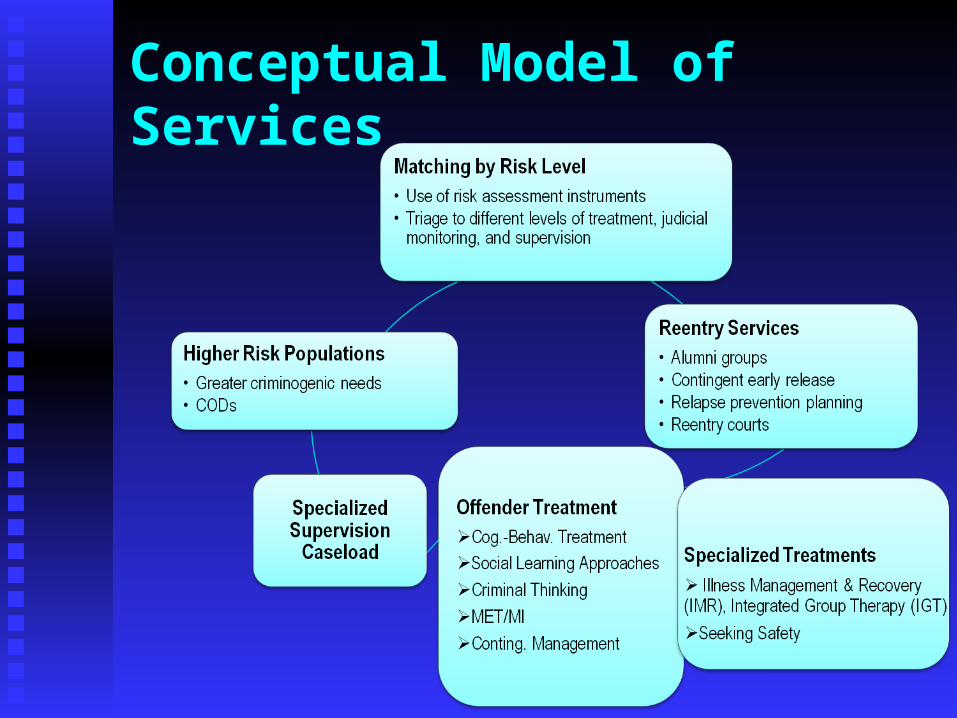
Conceptual Model of Services
Risk-Need-Responsivity (RNR)• The RISK principle tell us WHO to The RISK principle tell us WHO to
targettarget
• The NEED principle tells us WHAT to The NEED principle tells us WHAT to targettarget
• The RESPONSIVITY principle tells us The RESPONSIVITY principle tells us HOW to targetHOW to target

“Risk” Principle
• Goal is to match the level of services to Goal is to match the level of services to the offender’s likelihood to re-offendthe offender’s likelihood to re-offend
• Provides guidance re. WHO to target for Provides guidance re. WHO to target for program interventionsprogram interventions
• Adjust interventions, structure, and Adjust interventions, structure, and supervision by risk levelsupervision by risk level

“Need” Principle
• Assess Assess criminogenic needs criminogenic needs and and address these needs through focused address these needs through focused interventionsinterventions
• Place higher-risk/higher-need offenders Place higher-risk/higher-need offenders in treatment servicesin treatment services
• Prioritize a person’s “high” needs in Prioritize a person’s “high” needs in coordinating servicescoordinating services

Criminogenic Needs
Dynamic or Dynamic or changeablechangeable factors that factors that contribute to the likelihood that contribute to the likelihood that someone will commit a crimesomeone will commit a crime
““People involved in the justice system People involved in the justice system have many needs deserving have many needs deserving treatment, but not all of these needs treatment, but not all of these needs are associated with criminal behavior” are associated with criminal behavior” Andrews & Bonta (2006)Andrews & Bonta (2006)
Criminogenic Needs—“Big 8”
1. Antisocial attitudes2. Antisocial friends and peers3. Antisocial personality pattern
4. Substance abuse
5. Family and/or marital factors6. Lack of education7. Poor employment history8. Lack of prosocial leisure activities

InterventionsCognitive skills to address ‘criminal thinking’, positive peer supports, problem-solving skills
InterventionsCognitive skills to address ‘criminal thinking’, positive peer supports, problem-solving skills
InterventionsSubstance abuse treatmentCo-occurring disorders treatmentJob training/employment readiness
InterventionsSubstance abuse treatmentCo-occurring disorders treatmentJob training/employment readiness
“Responsivity” Principle
• Optimizing offenders’ engagement, Optimizing offenders’ engagement, learning, and skill-buildinglearning, and skill-building
• Allows offenders to Allows offenders to respond effectivelyrespond effectively to interventionsto interventions
Responsivity—general strategies• General approaches for providing General approaches for providing
interventions for offenders with CODsinterventions for offenders with CODs
- Cognitive-behavioralCognitive-behavioral
- Social learningSocial learning

Responsivity—fine tuning • Fine tuning interventions based on:Fine tuning interventions based on:
- Individual strengths and abilitiesIndividual strengths and abilities
- Learning styleLearning style
- Psychological functioning (e.g., CODs)Psychological functioning (e.g., CODs)
- Motivation levelMotivation level
- Gender (e.g., with history of trauma/PTSD)Gender (e.g., with history of trauma/PTSD)
- Race/ethnicityRace/ethnicity
Key Features of COD Treatment Programs
Highly structured therapeutic approachHighly structured therapeutic approach Destigmatize mental illnessDestigmatize mental illness Focus on symptom management vs. cure Focus on symptom management vs. cure Education regarding individual diagnoses Education regarding individual diagnoses
and interactive effects of CODsand interactive effects of CODs ““Criminal thinking” groups Criminal thinking” groups Basic life management and problem-Basic life management and problem-
solving skillssolving skills
33

Structural Features of Offender Treatment Programs
Therapeutic communities Therapeutic communities Isolated treatment units Isolated treatment units Program phasesProgram phases Blending of MH and SA servicesBlending of MH and SA services AssessmentAssessment Specialized mental health servicesSpecialized mental health services Transition and reentry servicesTransition and reentry services
34
Stage-Specific Treatment
• People with CODs who have had contact with People with CODs who have had contact with the CJ system come to treatment with varying the CJ system come to treatment with varying degrees of degrees of readiness and motivationreadiness and motivation
• Assessment of individuals’ stages of change Assessment of individuals’ stages of change is valuable in treatment planningis valuable in treatment planning
• Allows development of Allows development of stage-specific stage-specific treatmenttreatment for co-occurring disorders for co-occurring disorders
• Interventions are more likely to address goals Interventions are more likely to address goals that are valued by the individualthat are valued by the individual
35

COD Program Phases
Orientation Orientation Intensive treatment Intensive treatment Relapse prevention/transition Relapse prevention/transition
36
Orientation Phase
• Comprehensive assessment Comprehensive assessment • Persuasion and engagement Persuasion and engagement
groups groups • Treatment plan or contract Treatment plan or contract • Introduction to recovery process Introduction to recovery process
37

Intensive Treatment Phase
• Individual and group treatment Individual and group treatment
• Broad array of cognitive-behavioral Broad array of cognitive-behavioral interventions interventions
• Specialized dual diagnosis Specialized dual diagnosis interventionsinterventions
38

Relapse Prevention/Transition Phase
• Education about the relapse Education about the relapse process process
• Relapse prevention plan Relapse prevention plan
• Transition plan Transition plan
• Case managers or transition Case managers or transition coordinatorscoordinators
39
Treatment Modifications
Longer duration of treatment Longer duration of treatment More extensive assessmentMore extensive assessment Emphasis on psychoeducational Emphasis on psychoeducational
and supportive approachesand supportive approaches Higher staff ratio, more MH staffHigher staff ratio, more MH staff
40
Treatment Modifications
Shorter meetings and activitiesShorter meetings and activities Information presented gradually, in Information presented gradually, in
small units, and with repetitionsmall units, and with repetition Supportive versus confrontational Supportive versus confrontational
approachapproach More time provided for engagement and More time provided for engagement and
stabilizationstabilization
41

Modifying Treatment for Cognitive Impairment • Minimize need for abstraction (e.g., Minimize need for abstraction (e.g.,
use concrete, specific scenarios) use concrete, specific scenarios)
• Have demonstrate skills Have demonstrate skills
• Keep instructions brief Keep instructions brief
• Use audiovisual aids Use audiovisual aids • Keep role plays short and focusedKeep role plays short and focused
(Bellack, 2003)(Bellack, 2003)
42

Treating Female Offenders with CODs• Focus on trauma and spousal abuseFocus on trauma and spousal abuse
• Emphasis on education and job trainingEmphasis on education and job training
• Parenting skillsParenting skills
• Female role models and peer supportFemale role models and peer support
• Assertive outreach and crisis Assertive outreach and crisis interventionintervention
43

Treatments for Trauma and Substance Abuse• Seeking Safety (Najavits, 2002)Seeking Safety (Najavits, 2002)• Trauma Recovery and Empowerment Trauma Recovery and Empowerment
(TREM) (Harris, 1998)(TREM) (Harris, 1998)• Treating concurrent PTSD and cocaine Treating concurrent PTSD and cocaine
dependence (Brady et al., 2001)dependence (Brady et al., 2001)• Substance Dependence Posttraumatic Stress Substance Dependence Posttraumatic Stress
Disorder Therapy (Triffleman, et al., 1999)Disorder Therapy (Triffleman, et al., 1999)
44

Key Transition Services
• Development of Development of re-entry or transition planre-entry or transition plan • Assistance to engage in Assistance to engage in community-based community-based
SA and MH treatment SA and MH treatment • Engagement in Engagement in peer support and self-help peer support and self-help
networksnetworks to assist in recovery to assist in recovery• Stable Stable housinghousing• Vocational training Vocational training and employment supportand employment support• CaseCase managementmanagement and community and community
supervisionsupervision
45

The APIC Model
• AAssess clinical and social needs and ssess clinical and social needs and risk levelrisk level
• PPlan for treatment and services lan for treatment and services
• IIdentify required community programsdentify required community programs• CCoordinate the transition plan servicesoordinate the transition plan services
(Osher, Steadman, & Barr, 2002)(Osher, Steadman, & Barr, 2002)
46

APIC Reentry Checklist: Primary Domains♦ ♦ Mental health servicesMental health services♦ ♦ Psychotropic medicationsPsychotropic medications♦ ♦ HousingHousing♦ ♦ Substance abuse servicesSubstance abuse services♦ ♦ Health care/benefitsHealth care/benefits♦ ♦ Income/benefitsIncome/benefits♦ ♦ Food/clothingFood/clothing♦ ♦ TransportationTransportation♦ ♦ Other Other
47
48
0
10
20
30
40
50
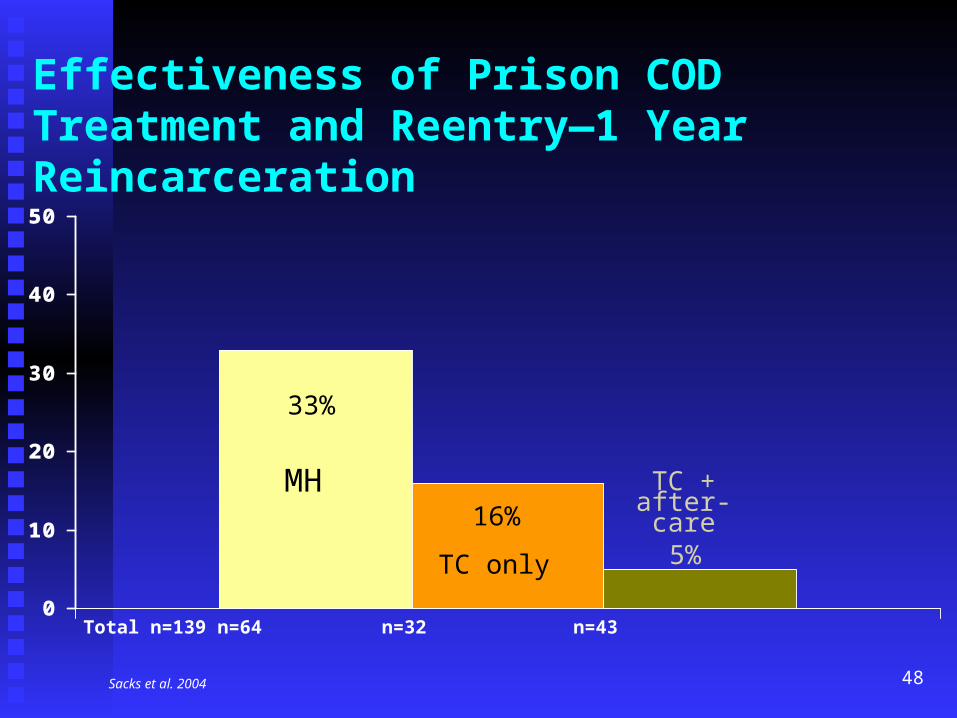
MH
33%
TC only
16%
5%
TC +after-care
Total n=139 n=64 n=32 n=43
Sacks et al. 2004
Effectiveness of Prison COD Treatment and Reentry—1 Year Reincarceration
Court Hearings and Judicial Monitoring• More frequent court hearings may be neededMore frequent court hearings may be needed• Hearings provide a good opportunity to Hearings provide a good opportunity to
recognize and reward positive behavioral recognize and reward positive behavioral changechange
• Specialized dockets Specialized dockets - Less formal, smaller, more private- Less formal, smaller, more private- More frequent- More frequent- Greater interaction between judge and - Greater interaction between judge and participantsparticipants- Include mental health professionals- Include mental health professionals

Community Supervision
• Active involvement in court and community Active involvement in court and community treatment teams, in-reach to jail and prisontreatment teams, in-reach to jail and prison
• Rapid crisis response capabilityRapid crisis response capability• Monitor medication compliance (MH Monitor medication compliance (MH
agencies)agencies)• Home visits usefulHome visits useful• ““Fugitive” warrants receive priorityFugitive” warrants receive priority• Taper supervision over timeTaper supervision over time
Specialized Caseloads
• Specialized MH/COD caseloadsSpecialized MH/COD caseloads• Smaller caseloads with more intensive Smaller caseloads with more intensive
services (e.g., < 45)services (e.g., < 45)• Sustained and specialized officer trainingSustained and specialized officer training• Dual focus on treatment and surveillanceDual focus on treatment and surveillance• Active engagement in Active engagement in SA and MH servicesSA and MH services
Specialized Caseloads
• Relationship quality important (trust, caring-Relationship quality important (trust, caring-fairness, avoid punitive stance)—“firm but fair”fairness, avoid punitive stance)—“firm but fair”
• Problem-solving approach vs. reliance on sanctionsProblem-solving approach vs. reliance on sanctions• Wide range of incentives and sanctionsWide range of incentives and sanctions• Flexibly apply sanctionsFlexibly apply sanctions• Avoid sanctions that remove participants from Avoid sanctions that remove participants from
treatmenttreatment• Higher revocation thresholdHigher revocation threshold• Improved outcomes—lower rates of revocation, Improved outcomes—lower rates of revocation,
arrest, and incarceration (Skeem et al., 2009)arrest, and incarceration (Skeem et al., 2009)