risposta immunitaria -...
TRANSCRIPT

RISPOSTA IMMUNITARIA • INSUFFICIENTE
Immunodeficienze • INADEGUATA
Autoimmunità (rivolta contro il bersaglio sbagliato) • ECCESSIVA
Ipersensibilità
IMMUNE RESPONSE Adaptive immunity serves the important function of host defense
against microbial infections, but immune responses are also capable of causing tissue injury and disease.
Disorders caused by immune responses are cal led hypersensitivity diseases.
This term arose from the clinical definition of immunity as "sensitivity," which is based on the observation that an individual who has been exposed to an antigen exhibits a detectable reaction, or is "sensitive," to subsequent encounters with that antigen.
Normally, the immune response eradicates infecting organisms without serious injury to host tissues. However, sometimes these responses are inadequately controlled or inappropriately targeted to host tissues, and in these situations, the normally beneficial response is the cause of disease.

IPERSENSIBILTA’ e I MISFATTI DELLA RISPOSTA IMMUNITARIA
• Risposta immunitaria diretta specificamente verso definite strutture molecolari (antigeni)
• Risposta infiammatoria, processo aspecifico innescato da “ogni tipo” di danno tessutale e varia poco a seconda del tipo dell’agente scatenante
• Ipersensibilità è l’eccessiva o non necessaria risposta immunitaria (anticorpale o dei linfociti T) che determina un rischio maggiore dell’antigene che l’ha evocata.
• Classificazione secondo Coombs e Gell (1975)
There are four types of hypersensitivity reaction mediated by immunological mechanisms that cause
tissue damage
Types I, II and III are antibody-mediated and are distinguished by the different types of antigens recognized and the different classes of antibody involved.
Type I responses are mediated by IgE, which induces mast-cell activation, Type II responses are directed against cell-surface or matrix antigens Type III responses are directed against soluble antigens, and the tissue
damage involved is caused by responses triggered by immune complexes. Types II and III are mediated by IgG, which can engage Fc-receptor and
complement-mediated effector mechanisms to varying degrees, depending on the subclass of IgG and the nature of the antigen involved.
Type IV hypersensitivity reactions are T cell-mediated and can be subdivided
into three groups. In the first group, tissue damage is caused by the activation of macrophages by TH1 cells, which results in an inflammatory response. In the second, damage is caused by the activation by TH2 cells of inflammatory responses in which eosinophils predominate; in the third, damage is caused directly by cytotoxic T cells (CTL).



Ipersensibilità di tipo I: allergia • Reazioni allergiche si manifestano quando un individuo
che ha già prodotto IgE in risposta ad un antigene innocuo (allergene) viene successivamente in contatto con lo stesso Ag
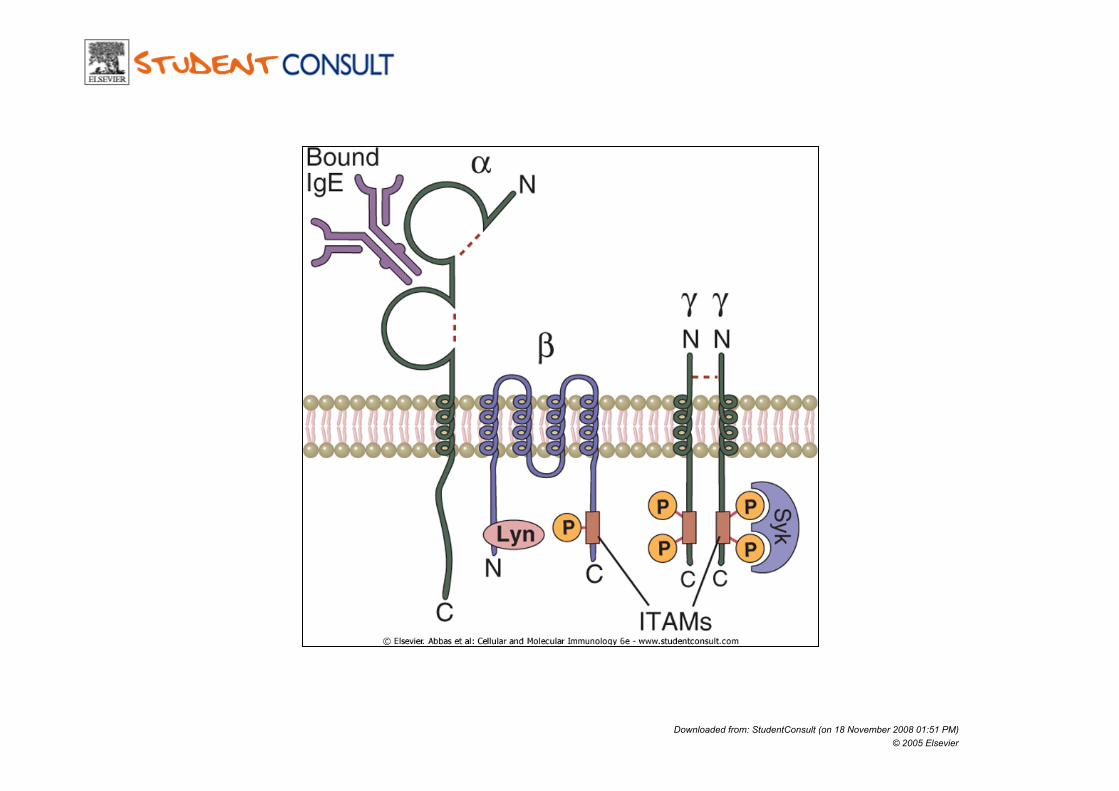
• IgE presenti principalmente nei tessuti si legano alla superficie dei mastociti attraverso il recettore ad alta affinità FcεRI causando dopo legame con l’allergene un cross-link dei recettori e stimolando la secrezione di mediatori chimici
• FcεRI sono presenti anche su basofili ed eosinofili attivati

IgE • La produzione di IgE è favorita da particolari Ag e dal
modo in cui essi sono presentati • I CD4 Th2 promuovono lo switch di anticorpi da IgM a
IgE e da IgG2 a IgG4
• Dose dell’antigene • Via di inoculo • Cellule presentanti (via di inoculo) • Caratteristiche dell’antigene (attività proteolitica)

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier

• Allergic reactions occur when an individual who has produced IgE antibody in response to an innocuous antigen, or allergen, subsequently encounters the same allergen. The allergen triggers the activation of IgE-binding mast cells in the exposed tissue, leading to a series of responses that are characteristic of allergy. There are circumstances in which IgE is involved in protective immunity, especially in response to parasitic worms, which are prevalent in less developed countries. In the industrialized countries, however, IgE responses to innocuous antigens predominate and allergy is an important cause of disease. Almost half the populations of North America and Europe have allergies to one or more common environmental antigens and, although rarely life-threatening, these cause much distress and lost time from school and work. Because of the medical importance of allergy in industrialized societies, much more is known about the pathophysiology of IgE-mediated responses than about the normal physiological role of IgE.
• The term allergy was originally defined by Clemens Von Pirquet as "an altered capacity of the body to react to a foreign substance," which was an extremely broad definition that included all immunological reactions. Allergy is now defined in a much more restricted manner as "disease following a response by the immune system to an otherwise innocuous antigen." Allergy is one of a class of immune system responses that are termed hypersensitivity reactions. These are harmful immune responses that produce tissue injury and may cause serious disease. Hypersensitivity reactions were classified into four types by Coombs and Gell. Allergy is often equated with type I hypersensitivity (immediate-type hypersensitivity reactions mediated by IgE), and will be used in this sense here.
• The mechanisms that favor the production of IgE. The pathophysiological consequences of the interaction between antigen and IgE that is bound by the high-affinity Fc receptor (Fc RI) on mast cells. The causes and consequences of other types of immunological hypersensitivity reactions.

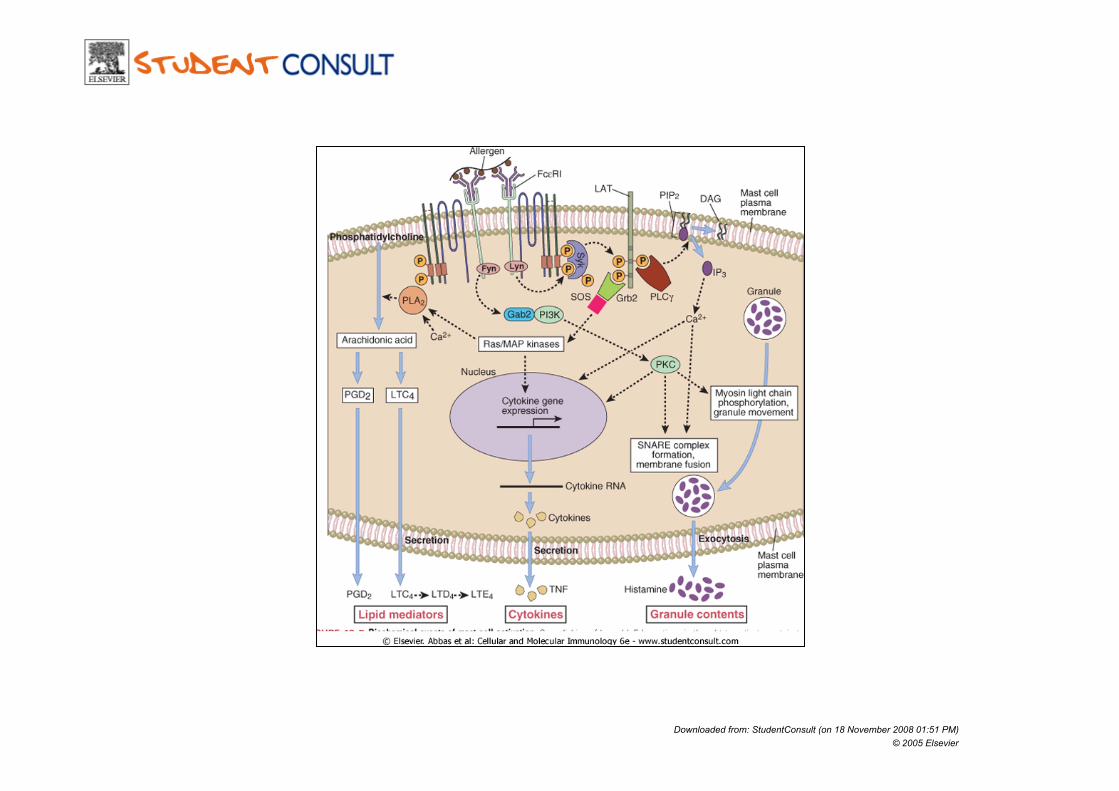
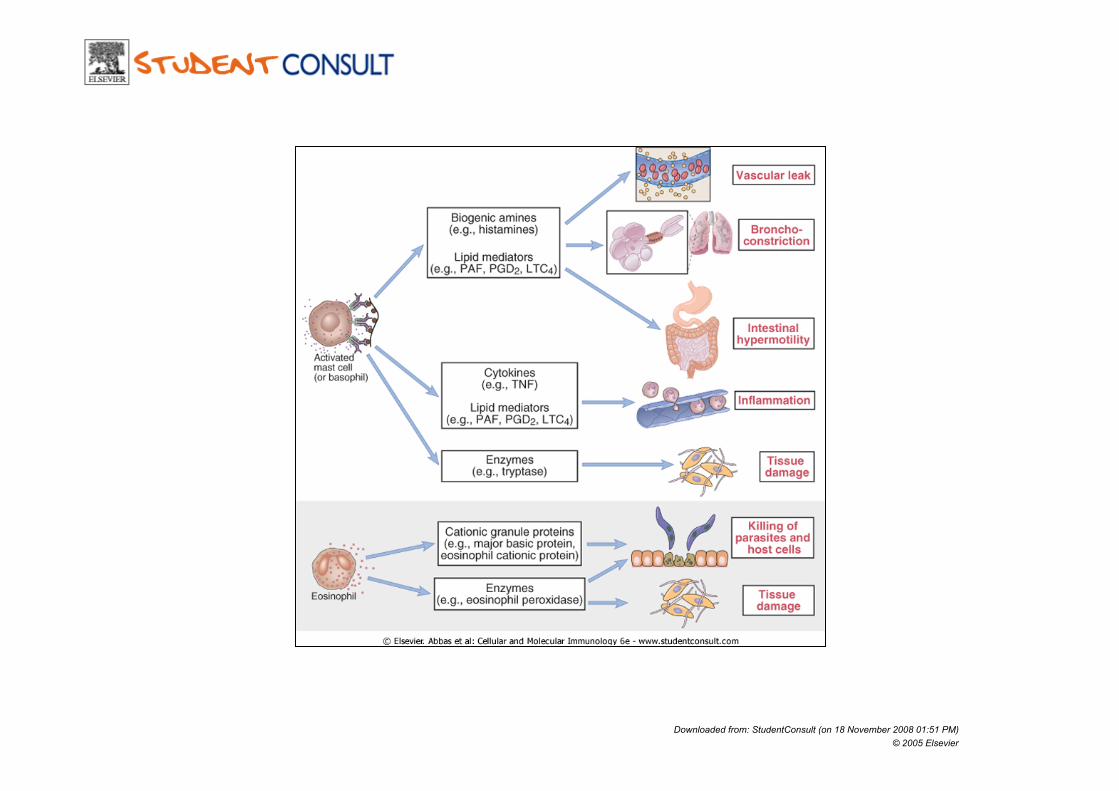
Molecules released by mast cells on activation
MEDIATORI PRIMARI
Enzymes and toxic mediators are released from the preformed granules
MEDIATORI SECONDARI
c y t o k i n e s , chemokines, and lipid mediators are synthesized after activation.

Eosinophils secrete a range of highly toxic granule proteins and other inflammatory mediators

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
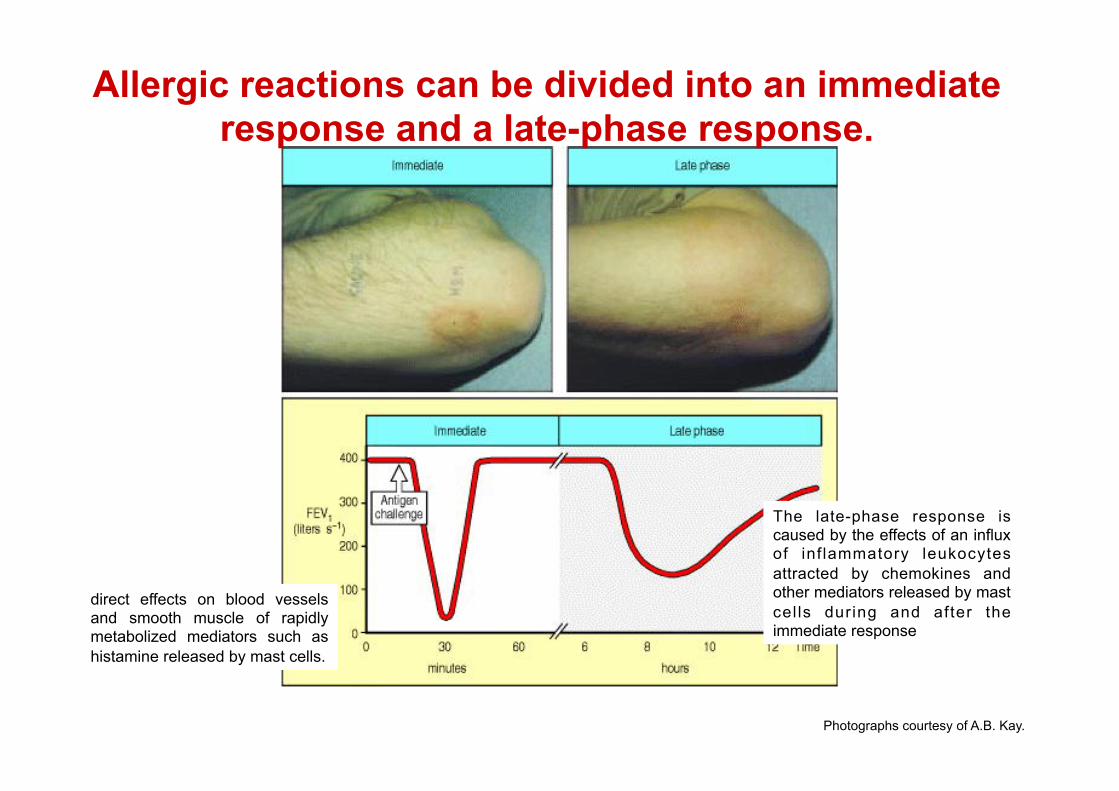
direct effects on blood vessels and smooth muscle of rapidly metabolized mediators such as histamine released by mast cells.
The late-phase response is caused by the effects of an influx of inf lammatory leukocytes attracted by chemokines and other mediators released by mast cel ls during and after the immediate response
Photographs courtesy of A.B. Kay.
Allergic reactions can be divided into an immediate response and a late-phase response.

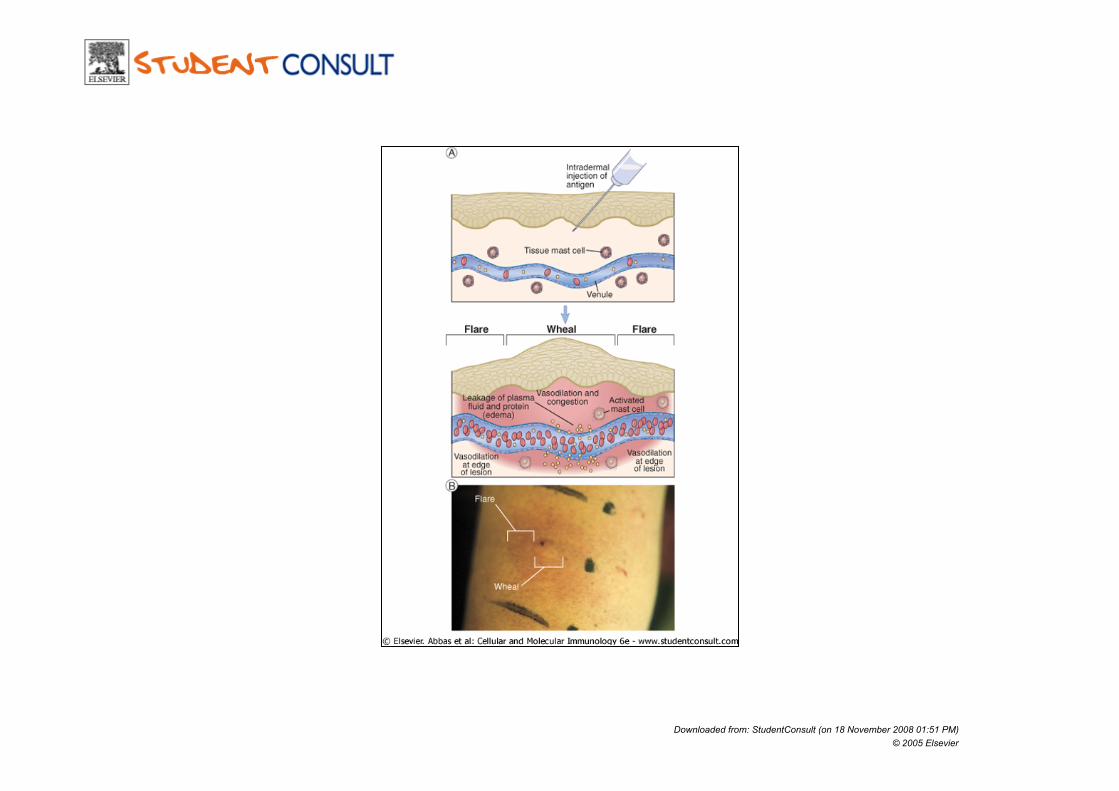
The dose and route of allergen administration determine the type of IgE-mediated allergic
reaction that results. There are two main anatomical distributions of mast cells: those associated with
vascularized connective tissues, called connective tissue mast cells, and those found in submucosal layers of the gut and respiratory tract, called mucosal mast cells. In an allergic individual, all of these are loaded with IgE directed against specific allergens.
The overall response to an allergen then depends on which mast cells are activated. Allergen in the bloodstream activates connective tissue mast cells throughout the body,
resulting in the systemic release of histamine and other mediators. Subcutaneous administration of allergen activates only local connective tissue mast cells,
leading to a local inflammatory reaction. Inhaled allergen, penetrating across epithelia, activates mainly mucosal mast cells,
causing smooth muscle contraction in the lower airways; this leads to bronchoconstriction and difficulty in expelling inhaled air.
Mucosal mast-cell activation also increases the local secretion of mucus by epithelial cells and causes irritation.
Ingested allergen penetrates across gut epithelia, causing vomiting due to intestinal smooth muscle contraction and diarrhea due to outflow of fluid across the gut epithelium.
Food allergens can also be disseminated in the bloodstream, causing urticaria (hives) when the food allergen reaches the skin.

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
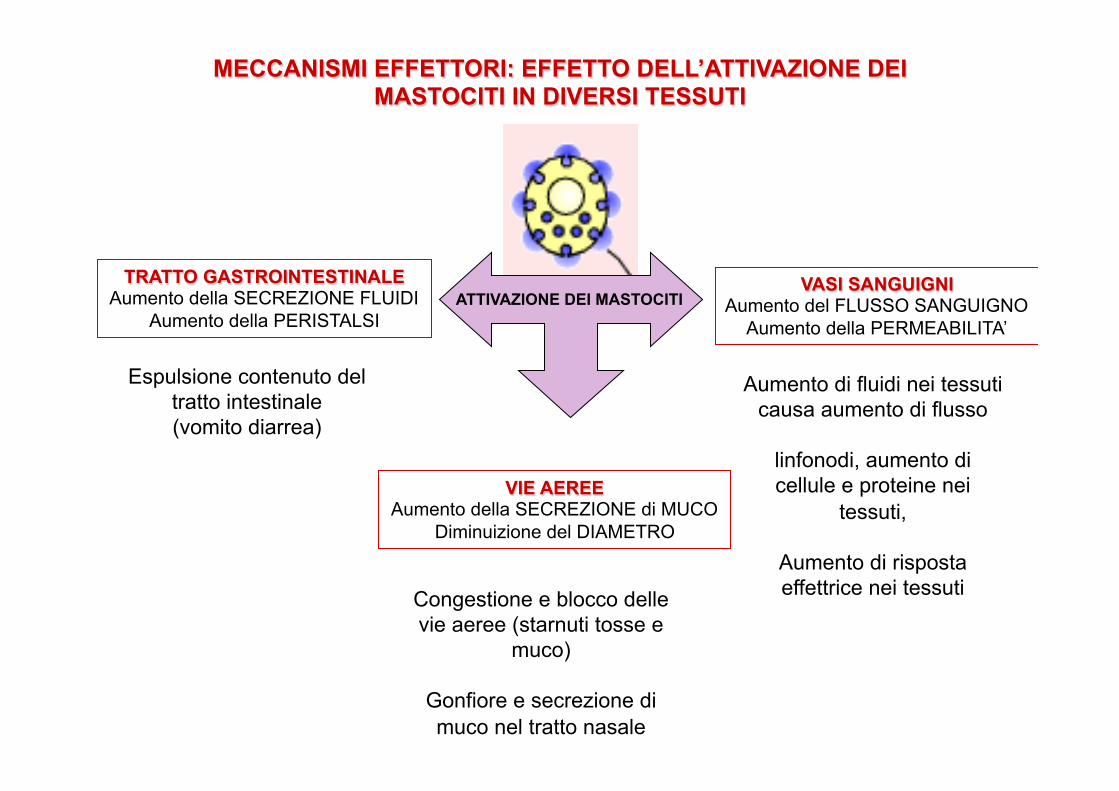
ATTIVAZIONE DEI MASTOCITI TRATTO GASTROINTESTINALE
Aumento della SECREZIONE FLUIDI Aumento della PERISTALSI
VASI SANGUIGNI Aumento del FLUSSO SANGUIGNO
Aumento della PERMEABILITA’
VIE AEREE Aumento della SECREZIONE di MUCO
Diminuizione del DIAMETRO
Espulsione contenuto del tratto intestinale (vomito diarrea)
Congestione e blocco delle vie aeree (starnuti tosse e
muco)
Gonfiore e secrezione di muco nel tratto nasale
Aumento di fluidi nei tessuti causa aumento di flusso
linfonodi, aumento di cellule e proteine nei
tessuti,
Aumento di risposta effettrice nei tessuti
MECCANISMI EFFETTORI: EFFETTO DELL’ATTIVAZIONE DEI MASTOCITI IN DIVERSI TESSUTI

IgE-mediated reactions to extrinsic antigens
© 2001 by Garland Science
All IgE-mediated responses involve mast-cell degranulation, but the symptoms experienced by the patient can be very different depending on whether the allergen is injected, inhaled, or eaten, and depending also on the dose of the allergen.

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier

Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier
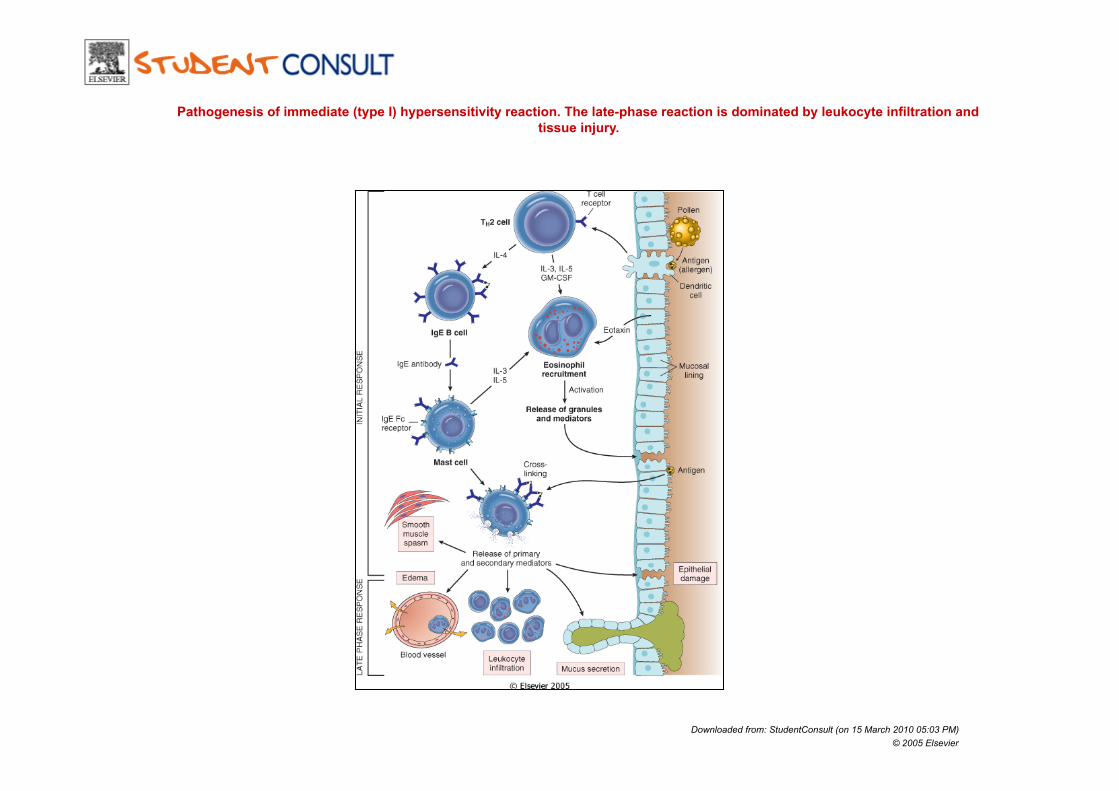
Pathogenesis of immediate (type I) hypersensitivity reaction. The late-phase reaction is dominated by leukocyte infiltration and tissue injury.
Downloaded from: StudentConsult (on 15 March 2010 05:03 PM) © 2005 Elsevier

Role of B cells in the pathogenesis of chronic allergic disease, with specific attention to the role of B cells as antigen-presenting cells.

Rationale The role of B cells in allergic asthma remains undefined.
One mechanism by which B cells clearly contribute to allergic disease is via the production of specific immunoglobulin, and especially IgE.
Cognate interactions with specific T cells result in T cell help for B cells, resulting in differentiation and immunoglobulin secretion. Proximal to (and required for) T cell-dependent immunoglobulin production, however, is antigen presentation by B cells.
While interaction with T cells clearly has implications for B cell function and differentiation, this study investigated the role that B cells have in shaping the T cell response during chronic allergic lung disease.

Methodology/Principal Findings The authors used a clinically relevant mouse model of chronic allergic
lung disease to study the role of B cells and B cell antigen presentation in this disease.
Novel findings: 1) Lung B cells from chronically allergen challenged mice up-
regulated MHC II and costimulatory molecules CD40, CD80 and CD86.
2) 2) Using in vitro studies, B cells from the lungs of allergen challenged mice could present antigen to T cells, as assessed by T cell proliferation and the preferential production of Th2 cytokines.
3) 3) Following chronic allergen challenge, the levels of Th2 cytokines IL-4 and IL-5 in the lungs and airways were significantly attenuated in B cell −/− mice, relative to controls.
4) 4) B cell driven Th2 responses and mucus hyper secretion in the lungs were dependent upon MHC II expression by B cells.

(A) Chronic model of cockroach antigen-induced allergic lung disease. Mice were immunized intraperitoneally (i.p.) and subcutaneously (s.c.), followed by 4 intranasal (i.n.) challenges, and two intratracheal (i.t.) inoculations. (B) Kinetics of B and T cell accumulation in the lungs of allergen challenged mice. The numbers of CD4+, CD8+, and CD19+ cells were determined by flow cytometric analysis of enzymatically digested lungs. Each time point represents the mean of 5 mice per group 6SEM * = p,0.05 vs. naıve lung . Similar results were observed in two independent experiments. (C) Cockroach antigen-specific B cells in the lungs, lymph nodes, spleen, and bone-marrow of naıve and allergen challenged (day 37) mice. The frequency of specific B cells was determined by a combination of ELISPOT and flow cytometry. Bars represent the mean of 5 mice per group 6SEM * = p,0.05 vs. naıve. Similar results were observed in two independent experiments.
Accumulation of B cells in the lungs during chronic allergic lung disease.

Expression of MHC II and costimulatory molecules by B cells from the lungs of chronic allergen challenged mice (day37)

Th2 cytokine production in pulmonary B cell/T cell co-cultures

In vitro proliferative responses of T cells co-cultured with pulmonary B cells.

Th1/Th2 associated cytokines in the lungs of allergen challenged mice.
B cell -/- and control mice were chronically challenged with allergen, and cytokine levels were assesed in bronchoalveolar lavage (B) and lung homogenates (A) via Bioplex multiplex assay. Bars represent the mean of 6 mice per group 6SEM, except naive, for which n = 2
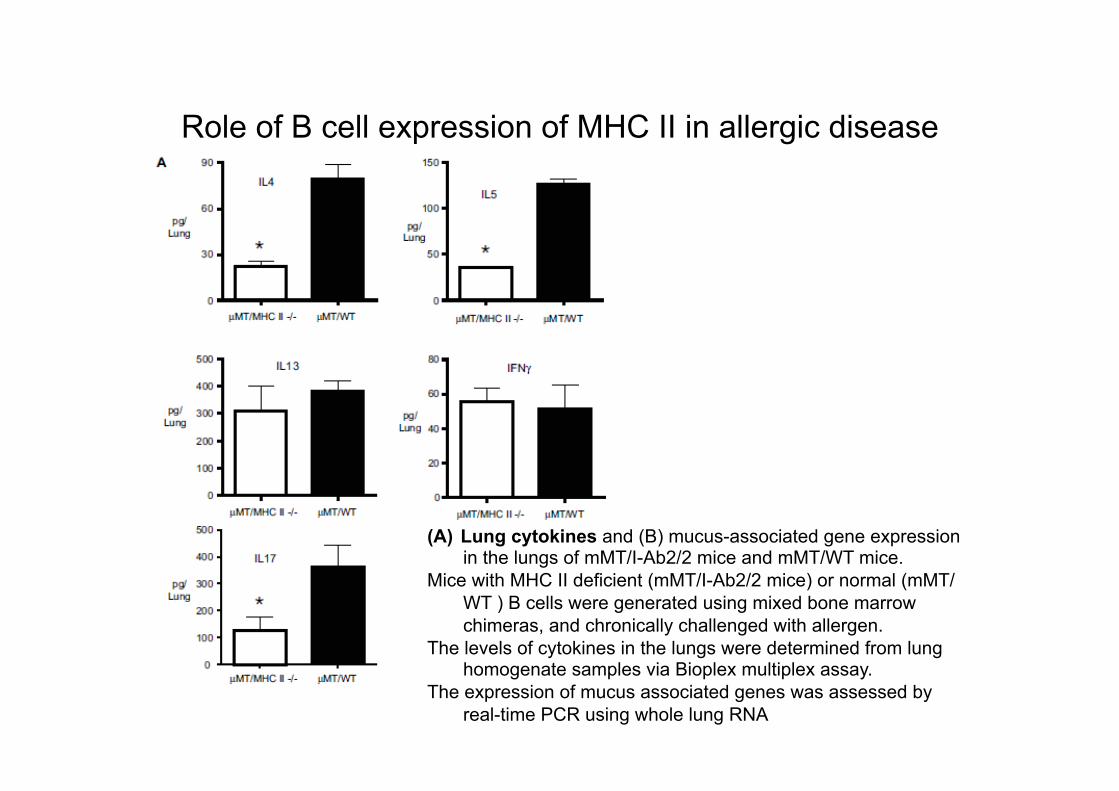
Role of B cell expression of MHC II in allergic disease
(A) Lung cytokines and (B) mucus-associated gene expression in the lungs of mMT/I-Ab2/2 mice and mMT/WT mice.
Mice with MHC II deficient (mMT/I-Ab2/2 mice) or normal (mMT/WT ) B cells were generated using mixed bone marrow chimeras, and chronically challenged with allergen.
The levels of cytokines in the lungs were determined from lung homogenate samples via Bioplex multiplex assay.
The expression of mucus associated genes was assessed by real-time PCR using whole lung RNA

Role of B cell expression of MHC II in allergic disease
(A) Lung cytokines and (B) mucus-associated gene expression in the lungs of mMT/I-Ab2/2 mice and mMT/WT mice.
Mice with MHC II deficient (mMT/I-Ab2/2 mice) or normal (mMT/WT ) B cells were generated using mixed bone marrow chimeras, and chronically challenged with allergen.
The levels of cytokines in the lungs were determined from lung homogenate samples via Bioplex multiplex assay.
The expression of mucus associated genes was assessed by real-time PCR using whole lung RNA
Conclusion
Collectively, these results provide evidence for antigen presentation as a novel mechanism by which B cells contribute to chronic allergic disease.
These findings give new insight into the mechanisms by which B cells promote asthma and other chronic diseases.