risk assessment public meeting - 4/9/03 1 premarketing risk assessment: considerations for data...
TRANSCRIPT

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
1
Premarketing Risk Assessment:Premarketing Risk Assessment:Considerations for Data Analysis and Considerations for Data Analysis and
Data PresentationData Presentation
Ellis F. Unger, M.D.Ellis F. Unger, M.D.Division of Clinical Trial Design and AnalysisDivision of Clinical Trial Design and AnalysisOffice of Therapeutics Research and ReviewOffice of Therapeutics Research and Review
Center for Biologics Evaluation and ResearchCenter for Biologics Evaluation and Research

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
2
Considerations for Data Analysis and Considerations for Data Analysis and Data PresentationData Presentation
Many aspects of these topics addressed in:Many aspects of these topics addressed in:
• “ “Guideline for the Format and Content of the Guideline for the Format and Content of the Clinical and Statistical Sections of an Application”Clinical and Statistical Sections of an Application” (1988)(1988)
• “ “ICH guideline for industry E3 Structure and ICH guideline for industry E3 Structure and Content of Clinical Study Reports”Content of Clinical Study Reports” (ICH-E3, 1995) (ICH-E3, 1995)

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
3
Issues for DiscussionIssues for Discussion
• Grouping of adverse eventsGrouping of adverse events• Temporal relations between adverse events andTemporal relations between adverse events and product exposureproduct exposure• Analyses of dose effectsAnalyses of dose effects• Data poolingData pooling• Missing safety dataMissing safety data

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
4
Coding and Grouping of Adverse EventsCoding and Grouping of Adverse Events• MedDRA or other coding dictionary should be MedDRA or other coding dictionary should be used consistently throughout clinical development used consistently throughout clinical development program, with adverse events examined as codedprogram, with adverse events examined as coded
• Specific adverse effects or toxicities (those with Specific adverse effects or toxicities (those with constellation of symptoms and signs; those with constellation of symptoms and signs; those with common pathophysiological bases) may merit common pathophysiological bases) may merit analyses of grouped termsanalyses of grouped terms

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
5
Coding of Adverse EventsCoding of Adverse Events
Utility of Combining Related Terms:Utility of Combining Related Terms:Amplification of weak safety signalsAmplification of weak safety signals: : • Linking terms by pathophysiologic mechanismLinking terms by pathophysiologic mechanism• Linking symptoms, signs, and lab abnormalitiesLinking symptoms, signs, and lab abnormalities
ExampleExample: :
• Ischemic eventsIschemic events - arterial thrombosis/occlusion, - arterial thrombosis/occlusion, embolism, claudication, ischemic necrosis, gangrene, embolism, claudication, ischemic necrosis, gangrene, intestinal ischemia, pulmonary embolism, acute MIintestinal ischemia, pulmonary embolism, acute MI

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
6
Coding of Adverse EventsCoding of Adverse Events
Downside of Combining Related Terms:Downside of Combining Related Terms:
Potential to mask serious, unusual events with less Potential to mask serious, unusual events with less serious, more common events:serious, more common events:
• e.g., toxic megacolon masked by constipatione.g., toxic megacolon masked by constipation

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
7
Coding of Adverse EventsCoding of Adverse Events
Division of One Event into Many Terms:Division of One Event into Many Terms:
Potential to decrease apparent incidence of an Potential to decrease apparent incidence of an adverse event: adverse event:
• e.g., e.g., including pedal edema, generalized edema, including pedal edema, generalized edema, and peripheral edema as separate terms will decrease and peripheral edema as separate terms will decrease the apparent incidence of fluid retentionthe apparent incidence of fluid retention

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
8
Coding of Adverse EventsCoding of Adverse Events
Whenever possible, we recommend that the Whenever possible, we recommend that the sponsor prospectively group adverse event terms sponsor prospectively group adverse event terms and develop case definitions in consultation with and develop case definitions in consultation with FDA. FDA.
We recognize that some groupings can only be We recognize that some groupings can only be constructed after the safety data are obtained.constructed after the safety data are obtained.

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
9
Temporal Associations Between Temporal Associations Between Adverse Events and Product ExposureAdverse Events and Product Exposure
Time to Event Analyses are Appropriate for:Time to Event Analyses are Appropriate for:
• Clinically important events that occur on a Clinically important events that occur on a delayed basis, e.g., progression of disability, delayed basis, e.g., progression of disability, development of cardiac toxicity, need for surgical development of cardiac toxicity, need for surgical intervention, malignancyintervention, malignancy
• Adverse events that occur at initiation of Adverse events that occur at initiation of treatment but diminish in frequency over timetreatment but diminish in frequency over time

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
10
Time-to-Event Analyses of Adverse EventsTime-to-Event Analyses of Adverse Events
Suggested Methods:Suggested Methods:
Descriptions of risk as a function of duration of Descriptions of risk as a function of duration of exposure or time since initial exposure (i.e., life exposure or time since initial exposure (i.e., life table analyses for cumulative incidence)table analyses for cumulative incidence) Assessment of risk within discrete time intervals Assessment of risk within discrete time intervals over the observation period (i.e., a hazard rate over the observation period (i.e., a hazard rate curve) to illustrate the change in risk over timecurve) to illustrate the change in risk over time

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
11
Time to First Malignancy: Rheumatoid Arthritis Patients Time to First Malignancy: Rheumatoid Arthritis Patients Treated with AdalimumabTreated with Adalimumab
(Abbott - Arthritis Advisory Committee Meeting; 3/4/03)(Abbott - Arthritis Advisory Committee Meeting; 3/4/03)
(n=2468)(n=2468)

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
12
Flu-Like Symptoms vs. Time (Interferon Flu-Like Symptoms vs. Time (Interferon -1b)-1b)
0 24 48 72 96 120 144
Time (weeks)0
5
10
15
20
25
30%
wit
h e
ven
t
Interferon beta-1b
Placebo

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
13
Analyses of Adverse Events by Dose Analyses of Adverse Events by Dose
The relationship between adverse events and The relationship between adverse events and exposure may help determine whether an exposure may help determine whether an event is actually related to the product and, if event is actually related to the product and, if so, the magnitude of the risk.so, the magnitude of the risk.

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
14
Adverse Events by Dose: Methods of AnalysisAdverse Events by Dose: Methods of Analysis
• Adverse events as a function of administered Adverse events as a function of administered dose (especially for dose-ranging studies, or dose (especially for dose-ranging studies, or development programs that evaluate >1 dose)development programs that evaluate >1 dose)
• Adverse events as a function of weight- or Adverse events as a function of weight- or body surface area-adjusted dose body surface area-adjusted dose
• Adverse events as a function of cumulative Adverse events as a function of cumulative dose received prior to eventdose received prior to event
• Adverse events as a function of drug plasma Adverse events as a function of drug plasma concentrationconcentration
Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
15
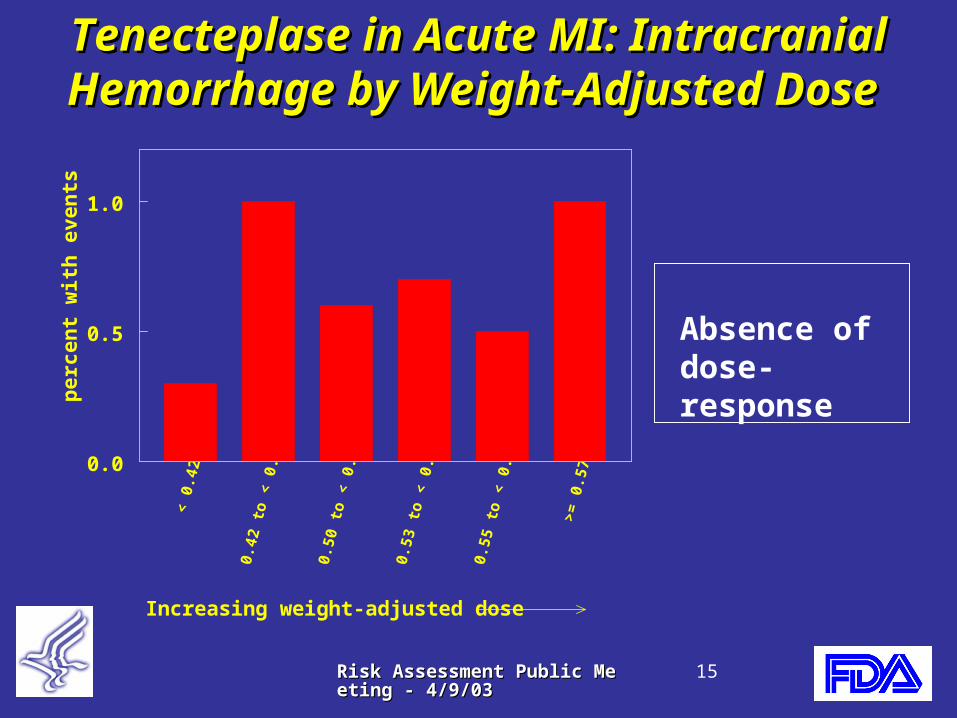
Tenecteplase in Acute MI: Intracranial Tenecteplase in Acute MI: Intracranial Hemorrhage by Weight-Adjusted Dose Hemorrhage by Weight-Adjusted Dose
< 0
.42
0.42
to
< 0
.50
0.50
to
< 0
.53
0.53
to
< 0
.55
0.55
to
< 0
.57
>=
0.5
7
Increasing weight-adjusted dose
0.0
0.5
1.0
pe
rce
nt
wit
h e
ve
nts
Absence of dose-response

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
16
Darbepoetin alfa vs. Epoetin alfa for Anemia of Chronic Darbepoetin alfa vs. Epoetin alfa for Anemia of Chronic Renal Failure: Renal Failure: Dyspnea/TachypneaDyspnea/Tachypnea by Total Weight- by Total Weight-
Adjusted Dose Administered in the 4 Weeks Preceding EventAdjusted Dose Administered in the 4 Weeks Preceding Event
Q-tile 1 Q-tile 2 Q-tile 3 Q-tile 4
Increasing weight-adjusted dose
0
20
40
60
80
100
dys
pn
ea,
tach
ypn
ea e
ven
ts darbepoetin alfa
epoetin alfa
Presence of apparent dose-response

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
17
Q-tile 1 Q-tile 2 Q-tile 3 Q-tile 4
Increasing weight-adjusted dose
0
20
40
60
80
100
dys
pn
ea,
tach
ypn
ea e
ven
ts darbepoetin alfa
epoetin alfa
Absence of dose-response
Darbepoetin alfa vs. Epoetin alfa for Anemia of Chronic Darbepoetin alfa vs. Epoetin alfa for Anemia of Chronic Renal Failure: Renal Failure: Back PainBack Pain by Total Weight-Adjusted Dose by Total Weight-Adjusted Dose
Administered in the 4 Weeks Preceding EventAdministered in the 4 Weeks Preceding Event
Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
18
Stepped Dosing Algorithm (Incremental dosing Stepped Dosing Algorithm (Incremental dosing Based on Age, Weight, or BSA)Based on Age, Weight, or BSA)
• Cut points are necessarily arbitrary.Cut points are necessarily arbitrary.
• Important to make a specific effort to Important to make a specific effort to examine safety (and efficacy) at doses just examine safety (and efficacy) at doses just above and below the cut points.above and below the cut points.

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
19
Stepped Dosing Algorithm: Tenecteplase Stepped Dosing Algorithm: Tenecteplase (Thrombolytic Agent) in Acute MI(Thrombolytic Agent) in Acute MI
Patient TNKaseWeight (mg)
(kg)
< 60 30>/= 60 to < 70 35>/= 70 to < 80 40>/= 80 to < 90 45
>/= 90 50
Tenecteplase dose
Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
20
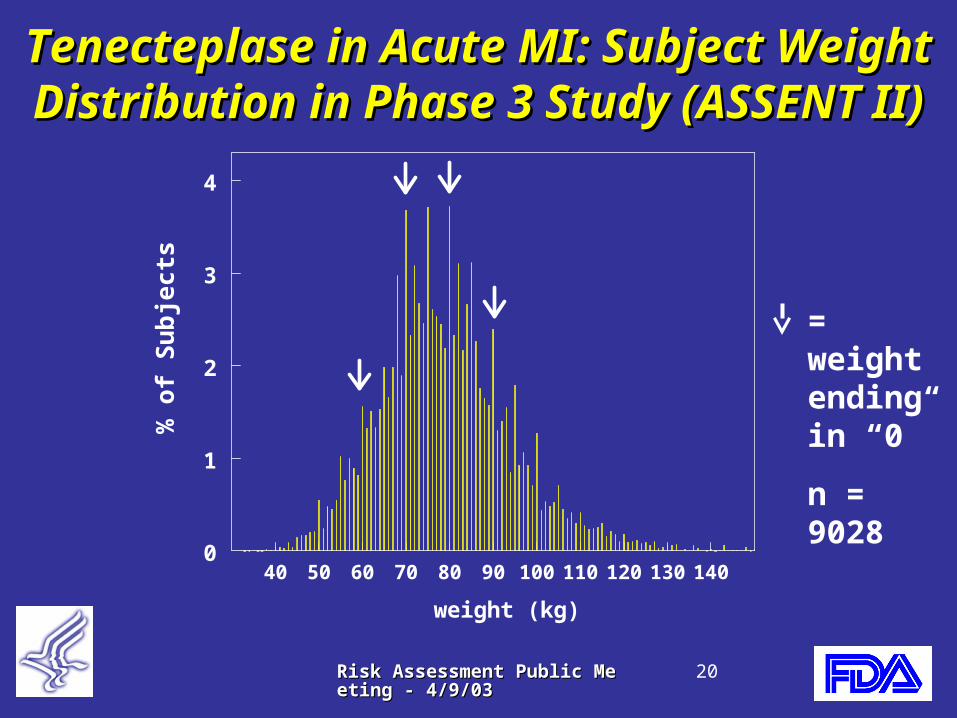
Tenecteplase in Acute MI: Subject Weight Tenecteplase in Acute MI: Subject Weight Distribution in Phase 3 Study (ASSENT II)Distribution in Phase 3 Study (ASSENT II)
40 50 60 70 80 90 100 110 120 130 140
weight (kg)
0
1
2
3
4%
of
Su
bje
cts
= weight ending in “0”
n = 9028

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
21
Tenecteplase in Acute MI: Tenecteplase in Acute MI: Rounding Weight to the Nearest 10 kg Rounding Weight to the Nearest 10 kg
Increases DoseIncreases Dose Patient TNKaseWeight (mg)
(kg)
< 60 30>/= 60 to < 70 35>/= 70 to < 80 40>/= 80 to < 90 45
>/= 90 50
Tenecteplase dose

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
22
Tenecteplase in Acute MI: Intracranial Tenecteplase in Acute MI: Intracranial Hemorrhage by Last Digit of Hemorrhage by Last Digit of EstimatedEstimated Weight Weight
(Patients with no recorded weight, n=3861)(Patients with no recorded weight, n=3861)
Similar frequency of intracranial hemorrhage
0 o
r 1
2 o
r 3
4 o
r 5
6 o
r 7
8 o
r 9
0.0
1.0
2.0
intr
ac
ran
ial h
em
orr
ha
ge
(%
)

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
23
Role of Data Pooling in Risk Assessment Role of Data Pooling in Risk Assessment
Pooling is actually a meta-analysis of Pooling is actually a meta-analysis of individual patient data (i.e., retrospectively individual patient data (i.e., retrospectively combining patient-level data from different combining patient-level data from different clinical studies to assess a safety outcome of clinical studies to assess a safety outcome of interest). interest).

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
24
Used Appropriately, Pooled Analyses Can:Used Appropriately, Pooled Analyses Can:• Facilitate detection of relatively rare Facilitate detection of relatively rare eventsevents
• Enhance the power to detect a statistical Enhance the power to detect a statistical associationassociation
• Aid interpretation of chance findings in Aid interpretation of chance findings in individual studiesindividual studies
• Provide more reliable estimates of the Provide more reliable estimates of the magnitude and constancy of risk over timemagnitude and constancy of risk over time

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
25
Characteristics of Valid Pooled Analyses:Characteristics of Valid Pooled Analyses:• Phase 1 pharmacokinetic and Phase 1 pharmacokinetic and pharmacodynamic studies excludedpharmacodynamic studies excluded
• Risk of safety outcome of interest is Risk of safety outcome of interest is expressed in person-years, or a time-to-expressed in person-years, or a time-to-event analysis is conductedevent analysis is conducted
• Pooled patient population is relatively Pooled patient population is relatively homogeneoushomogeneous
• Studies use similar methods of adverse Studies use similar methods of adverse event ascertainmentevent ascertainment

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
26
Data Pooling: Interpretation of Negative ResultsData Pooling: Interpretation of Negative Results
• A negative result from a pooled analysis A negative result from a pooled analysis does not does not proveprove absence of risk. absence of risk.
• Negative results should be interpreted in Negative results should be interpreted in the context of the potential limitations of the the context of the potential limitations of the analysis.analysis.
• Ensure that the previously mentioned Ensure that the previously mentioned principles have been appropriately principles have been appropriately considered in the analysis.considered in the analysis.

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
27
What is the Role of Subgroup What is the Role of Subgroup Analysis in the Safety Assessment?Analysis in the Safety Assessment?
Subgroup analyses are critical to the overall Subgroup analyses are critical to the overall risk-benefit assessment, and should be risk-benefit assessment, and should be addressed in NDA/BLA submissions in detail:addressed in NDA/BLA submissions in detail:
• DemographicsDemographics• Baseline disease statusBaseline disease status• Concomitant illnessConcomitant illness• Concomitant therapyConcomitant therapy
Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
28
How Can the Analyses of Missing How Can the Analyses of Missing Safety Data be Most Informative?Safety Data be Most Informative?
FDA would be interested in public comment FDA would be interested in public comment on ways this issue affects risk assessment on ways this issue affects risk assessment and/or unique methods that could be used to and/or unique methods that could be used to address the challenge that missing data address the challenge that missing data presents.presents.

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
29
Important Aspects of Data Presentation (1)Important Aspects of Data Presentation (1)
• Relationship of exposure time to the Relationship of exposure time to the development of the adverse eventdevelopment of the adverse event
• Summary of adverse event rates using a Summary of adverse event rates using a range of more restrictive to less restrictive range of more restrictive to less restrictive definitions (e.g., myocardial infarction versus definitions (e.g., myocardial infarction versus myocardial ischemia)myocardial ischemia)
• Summary of the distribution of important Summary of the distribution of important demographic variables across the pooled demographic variables across the pooled datadata

Risk Assessment Public Meeting - 4Risk Assessment Public Meeting - 4/9/03/9/03
30
Important Aspects of Data Presentation (2)Important Aspects of Data Presentation (2)
• Where complete case report forms are Where complete case report forms are called for [21 CFR 314.50], hospital records, called for [21 CFR 314.50], hospital records, autopsy reports, biopsy reports, and autopsy reports, biopsy reports, and radiological reports should also be included, radiological reports should also be included, where applicablewhere applicable
• Assuring that narrative summaries include important supplementary data (e.g., pertinent lab data, ECG data, biopsy data), as previously articulated in guidance