risk and professional regulation development claire herbert & guy rubin general dental council a...
TRANSCRIPT
Risk and Professional Regulation Development
Claire Herbert & Guy RubinGeneral Dental Council
a think piece for the Improving professional regulation conference
Friday 28th March 2014, Cumberland Lodge, Windsor Great Park
www.gdc-uk.org www.gdc-uk.org
Understanding risk – for regulation policy development
• Risk – likelihood that a hazard will occur• Hazard – potential source of harm e.g.
patient/public protection not maintained• Risk that Standards are not maintained e.g.
impairment of practice• Risk Factors – variables that give rise to risk
www.gdc-uk.org

GDC and regulation development
• GDC made no decisions about a risk-based approach
• Currently exploring potential
• Presentation does not represent GDC policy
• In discussion mode – internally and externally
www.gdc-uk.org
Risk and regulation
• GDC purpose to protect the public
• Regulation inherently about managing/controlling risk
• Understand risk as ‘likelihood of a hazard occurring’
• GDC manages a range of risks – operational, reputational, financial etc.
• Regulatory risk – risk of harm to patients.
www.gdc-uk.org

GDC and managing riskProactive:• Setting standards and QA of pre-
registration education
• Managing access to the register and practice of dentistry
• Setting standards of practice
• Enforcing CPD
• Maintaining FTP procedures (including as deterrent)
Reactive:• Auditing CPD
compliance
• Dealing with concerns through FTP
• Mediating consumer complaints (through Dental Complaints Service)
www.gdc-uk.org
Trend towards understanding risk
• Hampton Review 2005
• Enabling Excellence – Revalidation proportionate to risk
• Right touch regulation – PSA and continuing assurance
www.gdc-uk.org
Example– Civil Aviation Authority• Risk-based approach: monitors risk associated with all
parts of aviation, based on a range of data analysis , including performance of personnel.
• Seven risks currently identified
• Have conducted a comprehensive review of ‘human factors’.
www.gdc-uk.org
Example – Solicitors Regulation Authority
• Risk-based approach: risks to the non-achievement of regulatory objectives are assessed in terms of likelihood and impact of any harm they cause to desired outcomes…this approach ensures that regulatory activities and resources are prioritised and applied proportionately – SRA
• Risk Index - 6 categories of risk, with underpinning ‘factors’ • Developed a dedicated team – the Risk Centre to assess internally
and externally sourced data• Aim to become an outcomes-based regulator
www.gdc-uk.org
Health regulators: increasing interest in research to understand risk
December 2013 Joint Department of Health and PSA seminar on regulatory research• Health regulators identified understanding risk
as a key shared research priority• Particular interest in the relationship between
systemic risk and professional performance
www.gdc-uk.org
GDC Research: Case Study 1Practising dentistry independently: Identifying risks in transition of new qualified dentists to fully unsupervised practise
• What types of risk are there to patient safety in dentistry, and within other healthcare professions, what are the reasons for them and how significant are they?
• How do the risks vary across types of dental professionals and why?
• What issues and risks are there with confidence, knowledge, competence and skills levels of new dental and other health professionals over the four areas of clinical, communication, management and leadership, and professionalism. How may this vary and what are the reasons?
www.gdc-uk.org

Methods
• Seven online databases searched
• Literature in English, since 2000
• Grey literature - regulators in English-speaking world
• 700 papers retrieved and reviewed
• 204 papers selected for review and inclusion in the report
www.gdc-uk.org
Findings & Recommendations
www.gdc-uk.org
• Shortage of good quality studies - mainly focus on students about to graduate or in foundation year. Few look at early years of practice.
• No evidence about risk could be drawn from GDC FtP data. Little analysis of Fitness to Practice (FtP) data by other regulators (except
GMC, GOSC). • No comparative evidence about how risk varies across groups .
• Some potential risk factors:
Competence Confidence Knowledge
• Recommended mitigation of potential risk : supervision and support mechanisms in place
GDC: Evidence not sufficiently strong to support regulatory change but further analysis and monitoring to be carried out.
GDC Research: Case Study 2Performance Management of Dentists
The GDC commissioned independent research from the Picker Institute Europe in 2012 to inform Revalidation/Continued Assurance.
Research Focus
• What are the types of evidence already used across dentistry to assess performance and quality of the practice of individual dentists?
• What are the purposes of each evidence type?• What is the extent of consistency in application of evidence types and
standardisation in format across the four countries of the UK and practice settings?
• What contribution could they make to assessing practice in accordance with the GDC’s Standards?
• What criteria could be used to evaluate compliance with GDC’s standards?
• Could thresholds of (un)acceptable practice be identified and agreed?
www.gdc-uk.org
Methods
Mixed method approach• Website search and literature review• Semi-structured interviews• Online surveys
www.gdc-uk.org

Findings
• The research considered 11 commonly used performance management tools in a diverse range of practice settings.
• In wide and variable use across the UK and in different practice settings. Little standardised approach to use or delivery.
• Some indication that engagement in some performance management processes may improve the quality of dentist’s practice.
• Used within a carefully designed appraisal-based system, with an appropriately trained and matched appraiser, most [evidence types]have the potential to contribute to a decision about practice for some, if not all, dentists.
www.gdc-uk.org

GDC Case Study 3: Patient perceptions and attitudes to risk• Evaluation of risk is built into patient attitudes to care and treatment• Research consistently shows that confidence in dental professionals
performance and competence is high and much is taken on trust and/or assumption.
However…• some evidence that patients routinely evaluate risk and make judgments
(whether informed or not) about it in relation to their care and treatmentFor example:
Are there characteristics (e.g. age, length of service etc. ) that make some dental professionals more likely to put patients at risk? Are dental professionals sufficiently well qualified and trained to practice? Is evidence about poor treatment shared effectively by regulators and others in order to protect patients from risk of harm?
.
www.gdc-uk.org
GDC Case Study 3: Patient perceptions and attitudes to riskAre dental professionals sufficiently well qualified and trained to practise?
• Qualitative research with patients: expressed concerns that older, more experienced dentists may actually be more of a ‘risk’ due to old fashioned practices.
“What is quite interesting is that the dentist who has 30 years experience, unless he gets retrained or goes on courses, who is to say he is in touch with the latest practices?”
(Patient and Public Attitudes to Standards for Dental Professionals 2010)
www.gdc-uk.org
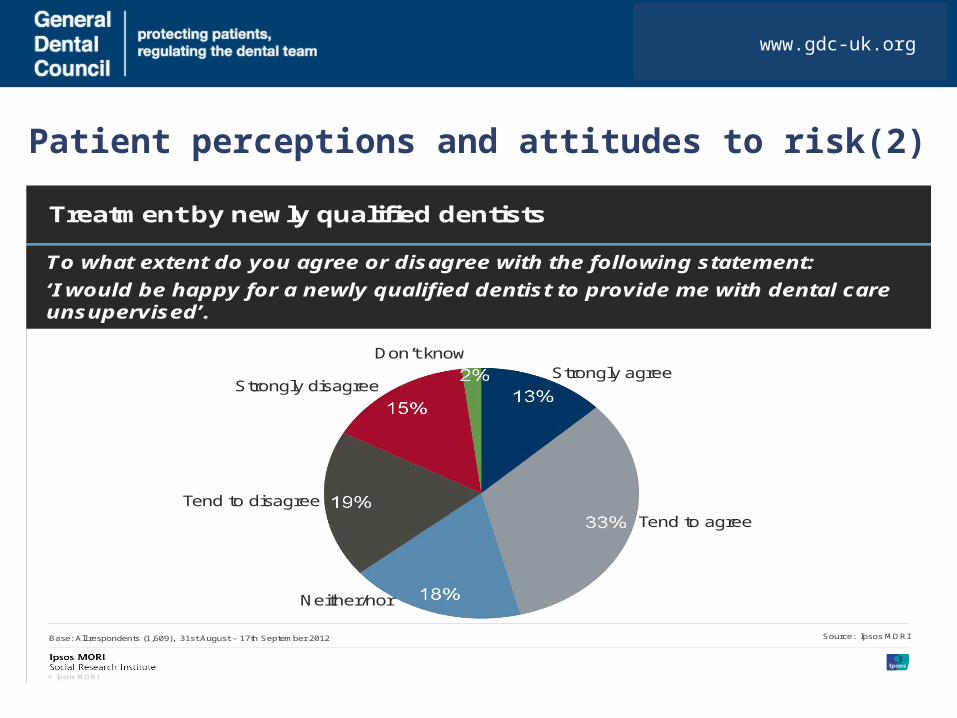
Patient perceptions and attitudes to risk(2)
www.gdc-uk.org
© Ipsos MORI
To what extent do you agree or disagree with the following statement:
‘I would be happy for a newly qualified dentist to provide me with dental care unsupervised’.
Treatment by newly qualified dentists
Base: All respondents (1,609), 31st August – 17th September 2012 Source: Ipsos MORI
Strongly agree
Tend to agree
Neither/nor
Strongly disagree
Tend to disagree
Don’t know
Version 1 | Internal Use Only© Ipsos MORI
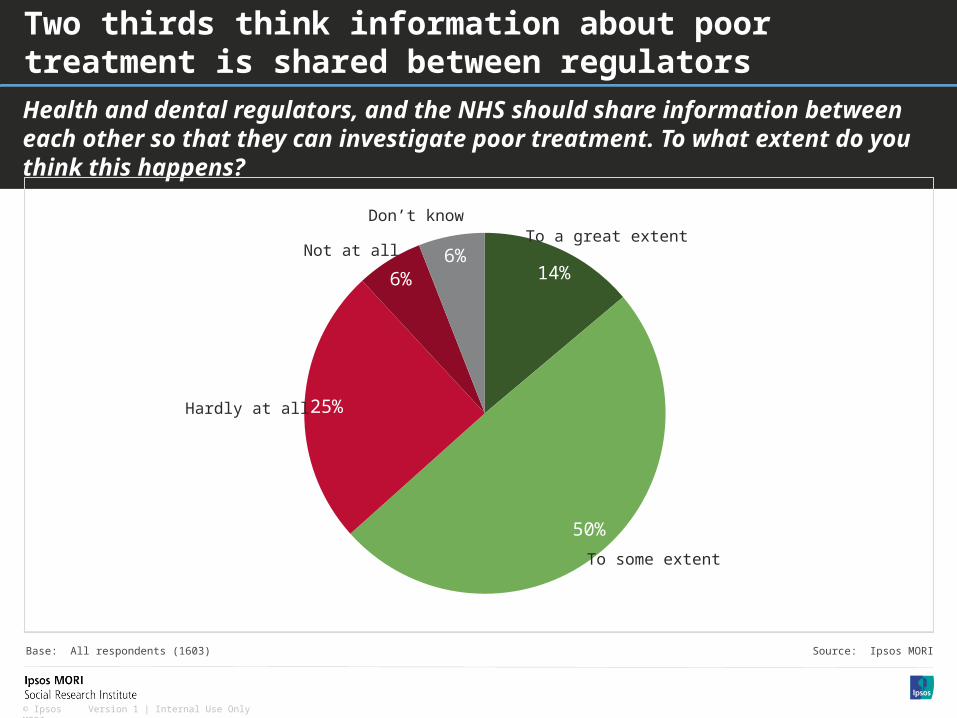
Health and dental regulators, and the NHS should share information between each other so that they can investigate poor treatment. To what extent do you think this happens?
Two thirds think information about poor treatment is shared between regulators
14%
50%
25%
6%
6%To a great extent
To some extent
Hardly at all
Not at all
Don’t know
Base: All respondents (1603) Source: Ipsos MORI
Developing a practical and strategic approach?
www.gdc-uk.org
FactorsCategorising risk
Human factors
System Factors
Questions?• What are the root causes,
causal or contributing factors?• What are the precursors? e.g.
pathway to risk• How can they be categorised?
e.g. conduct, competence, context
• Do the risks apply equally or differently across the register?
www.gdc-uk.org

Data sources - opportunitiesOpportunities
• GDC FTP determinations and cases• GDC FTP/DCS complaints data• Wider dentistry complaints• Performance management/clinical governance• Insurance & indemnity• Occupational, behavioural and educational
literature• Perceptions and attitudes• Horizon scanning
www.gdc-uk.org

Data sources - challenges
• Using datasets for different purposes• Access to external data• Limited investigation and expertise• Legal constraints• Unpredictability• System support• ‘Risk’ culture
www.gdc-uk.org

To consider• What regulatory outcomes are anticipated as a consequence of
identifying and understanding risk?• What can be learned from/shared with other organisations?• What resources are required?• How can a ‘risk’ alert culture be further developed in regulation?• How do patients evaluate risk to make judgements about the care
and treatment? • What role can regulators play in informing patient judgements?
www.gdc-uk.org