right iliac fossa pain modality directed diagnostic approach right iliac fossa pain – modality...
TRANSCRIPT
Right iliac fossa pain Right iliac fossa pain – modality modality directed diagnostic approachdirected diagnostic approach
John-Henry CorbettDiagnostic Radiology
University of the Free State03/2012

• Acute right iliac fossa pain is a common clinical emergency
• Requires prompt investigation and diagnosis to limit morbidity and mortality
• Physical and laboratory findings are often non-specific
• Clinical presentations of potential causes overlap
• Diagnostic imaging is used increasingly at an earlier time to aid in diagnosis
• Acute appendicitis is the most common condition• In up to one third the cause is not apparent
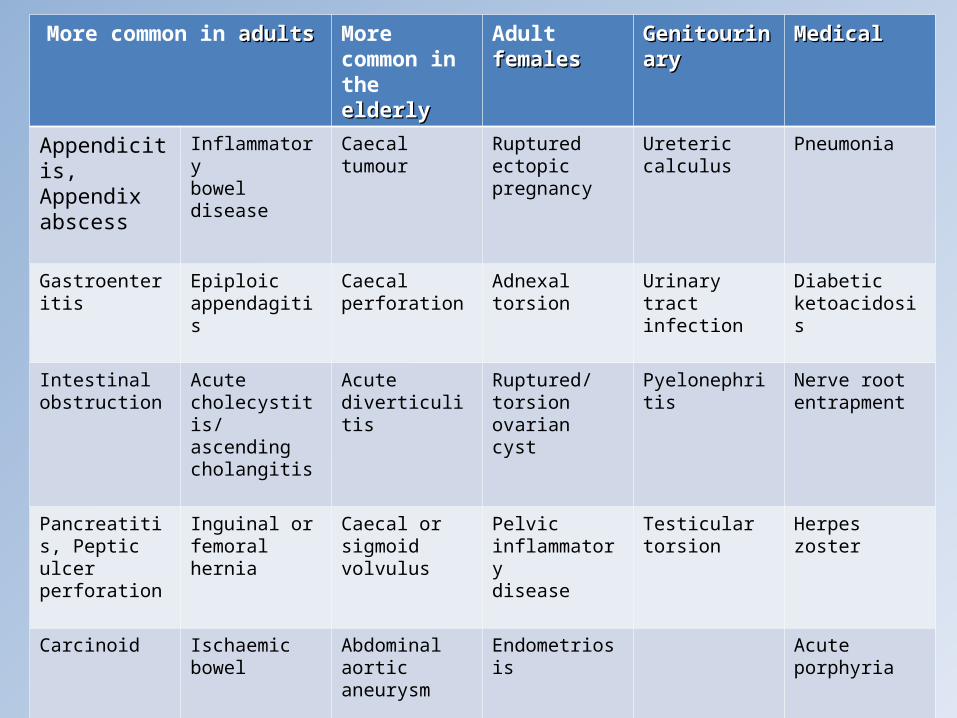
More common in adultsadults More common in the elderlyelderly
Adult femalesfemales GenitourinaryGenitourinary MedicalMedical
Appendicitis, Appendix abscess
Inflammatorybowel disease
Caecal tumour Ruptured ectopicpregnancy
Ureteric calculus Pneumonia
Gastroenteritis Epiploic appendagitis
Caecal perforation
Adnexal torsion Urinary tractinfection
Diabetic ketoacidosis
Intestinal obstruction
Acute cholecystitis/ascending cholangitis
Acute diverticulitis
Ruptured/torsionovarian cyst
Pyelonephritis Nerve rootentrapment
Pancreatitis, Peptic ulcer perforation
Inguinal or femoralhernia
Caecal or sigmoidvolvulus
Pelvic inflammatorydisease
Testicular torsion Herpes zoster
Carcinoid Ischaemic bowel Abdominal aorticaneurysm
Endometriosis Acute porphyria
Lymphoma Constipation Ruptured ovarianfollicle

Selection of the most appropriate Selection of the most appropriate imaging modalityimaging modality
• Depends on– 1) Patient age and body habitus
• < 20 years– Ultrasound initially, regardless of suspected pathology– Then CT or MRI if additional information is required
• > 20 years– Ultrasound initially in young, slim adults
» Particularly women of reproductive age
• Older or obese patients– CT
• Depends on – 2) Suspected pathology, based on clinical and
laboratory findings• Appendicitis• Renal colic• Gynaecological• Hernia• Bowel related• Vascular
Selection of the most appropriate Selection of the most appropriate imaging modalityimaging modality
Acute appendicitis• Most common cause of acute RIF pain• Clinical diagnosis on patient history and physical
examination– Any age, but most common 10-20 years– Abdominal pain
• Colicky, central abdominal pain• Followed by vomiting and migration of pain to RIF (50%)
– Loss of appetite, constipation, nausea – Pyrexia, tachycardia and localized tenderness– Accuracy for clinical diagnosis
• Men : 80-90% Women : 60-80%

Alvarado score Alvarado score • 0-4 could be discharged without imaging•scores of 4-6 undergo imaging evaluation•scores of 7 or above receive surgical consultation
• Conventional surgical wisdom is based on the belief that an inverse relationship exists between the negative appendectomy rate (NAR), i.e. removal of a non-inflamed appendix, and the perforation rate
• Thus, a false-negative appendectomy rate of 15–23% is regarded as an index of appropriate management and the failure to maintain such a surgical threshold is an indication of insufficient surgical aggression, with an attendant risk of an excessive rate of perforation
Acute appendicitis

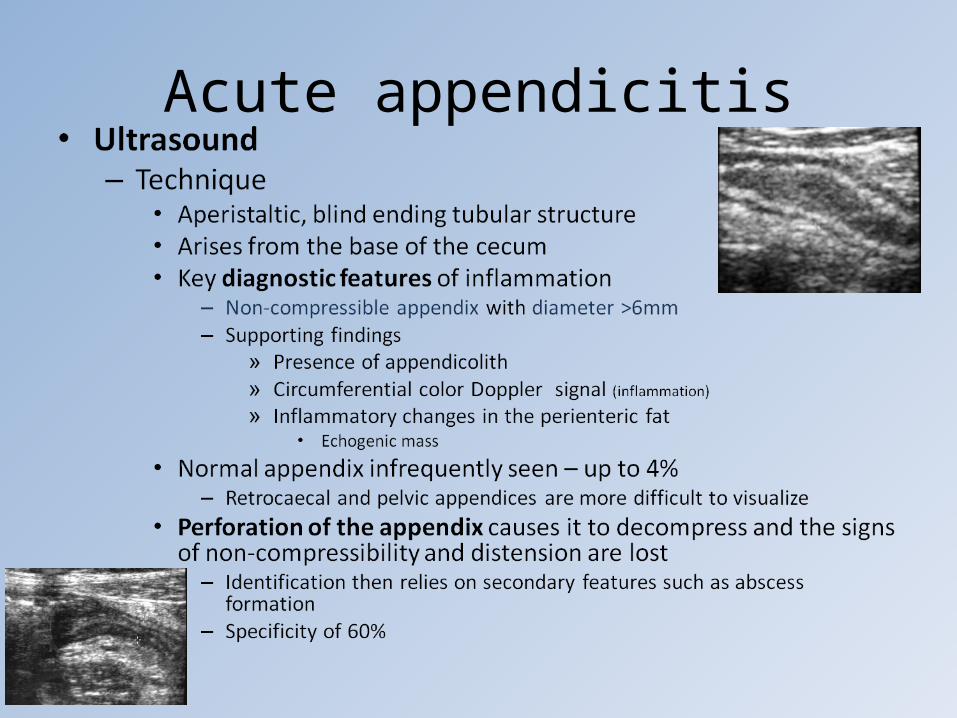
• Ultrasound– Advantages
• Widely available and inexpensive• Avoidance of ionizing radiation
– Especially women of reproductive age and children– Gynecological disease gives further reason for U/S evaluation
• Usefull in identifying an alternative diagnosis– Disadvantages
• Operator dependant – Technique
• Graded compression with high frequency linear probe– gradual and constant increase in the compression by the US
probe in the right iliac fossa – displaces normal, air-filled bowel, or compresses it against the
posterior abdominal wall – abnormal, non-compressible appendix is thus revealed
Acute appendicitis
Acute appendicitis

Transverse U/S : Inflammed appendix (between calipers) ; adjacent inflamed fat (arrow) ; terminal ileum with air (curved arrow)
Longitudinal U/S : inflammed appendix with proximal appendicolith

Acute appendicitis• CT
– Technique• Variety of techniques in an attempt to
– Reduce radiation dose– Maximize diagnostic yield – Minimize preparation time for the scan
• Variation in – Amount of abdomen imaged– Use of IV, oral and rectal contrast
• All share same basic concept– Acquiring thin collimation images (5mm or less) in a single breath
hold
• Unenhanced CT abdomen (No IVI, oral or rectal contrast) – Reduces delay for patient preparation and reduces per patient cost– Relies on intra-abdominal fat to provide contrast
» Difficult to obtain good results in thin patients– More difficult to interpret initially, but just as accurate when
experienced

Acute appendicitis• CT
– Appearance on CT• Filling of appendix with oral contrast is an important negative feature• Normal appendix wall 1-2mm in thickness• Periappendiceal fat should appear homogenous
– CT diagnosis of acute appendicitis can be made if• Abnormal appendix identified
– Appendix diameter > 6mm– With homogenously enhancing wall – Mural edema may produce a target sign– Periappendiceal inflammation in 98%
» Fat stranding• Calcified appendicolith with pericecal inflammation
– Perforated appendicitis • Accompanied by pericecal phlegmon or abscess• Associated findings
– Extraluminal air– Ileocecal thickening– Localized lymphadenopathy– Peritoneal enhancement– Small bowel obstruction
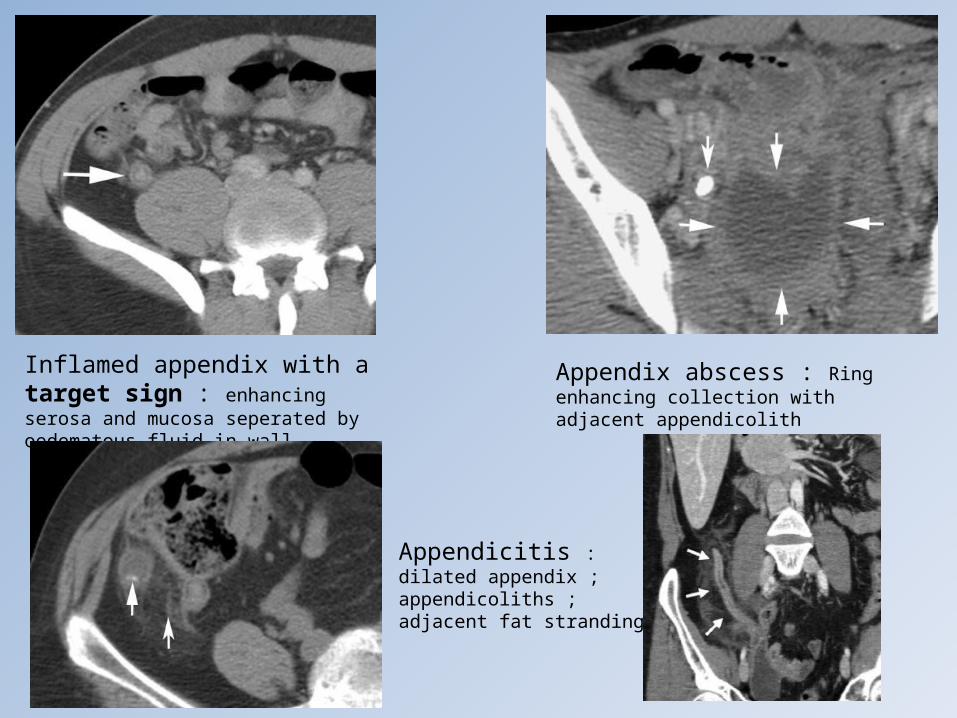
Inflamed appendix with a target sign : enhancing serosa and mucosa seperated by oedematous fluid in wall
Appendix abscess : Ring enhancing collection with adjacent appendicolith
Appendicitis : dilated appendix ; appendicoliths ; adjacent fat stranding

Acute appendicitis• MRI
– Currently limited to patients with right iliac fossa pain during pregnancy
• Avoiding ionizing radiation is of prime importance
– Limited information available• small number of studies with little
patient numbers– Imaging techniques used
• no IV contrast• axial, coronal and sagittal noncontiguous T2-weighted single-shot fast
spin-echo (SE) sequences • axial fat-suppressed T2-weighted fast SE sequences• axial T1-weighted gradient-recalled-echo sequences• axial and coronal inversion-recovery sequences performed through
the lower abdomen and pelvis– Illustrates normal and abnormal appendix
• May be useful in diagnosing adnexal pathology

Appendicitis : dilated appendix (black
arrowhead) ; appendicolith (black arrow) ; adjacent fat stranding (white arrowheads)

Crohn’s disease• Although inflammatory bowel disease is usually a
chronic condition, flare-ups may present acutely• Peak age of onset 15-30 years• Many cases of Crohn’s diagnosed during work-up of
acute LRQP since ileocecal region is most commonly affected– Apposed to ulcerative colitis which dominates the left colon
• CT best imaging modality– Two most common imaging findings
• Eccentric wall thickening• Mucosal hyperenhancement
Crohn’s disease• CT imaging
– Presence of intramural fat indicates chronic changes– Segmental involvement with skipped (normal) regions
• vs ulcerative colitis – involves bowel in more continuous fashion
– Comb sign• Engorgement of the vasa recta penetrating the bowel wall• Advanced, extensive and active Chron’s disease
– Creeping fat sign • Fibrofatty proliferation along the mesenteric border of the
affected bowel - almost pathagnomonic
– Complications• Small bowel strictures causing obstruction• Fistulas and abscesses

Crohn’s disease : Thickened terminal ileum ; diagnosis confirmed at histology
Thickened terminal ileum ; strictures ; mucosal hyperenhancement ; proliferation of mesenteric fat (black arrow)
Y shaped fistula : Cecum (arrowhead) ; terminal ileum (white
arrow) ; psoas abscess (*)
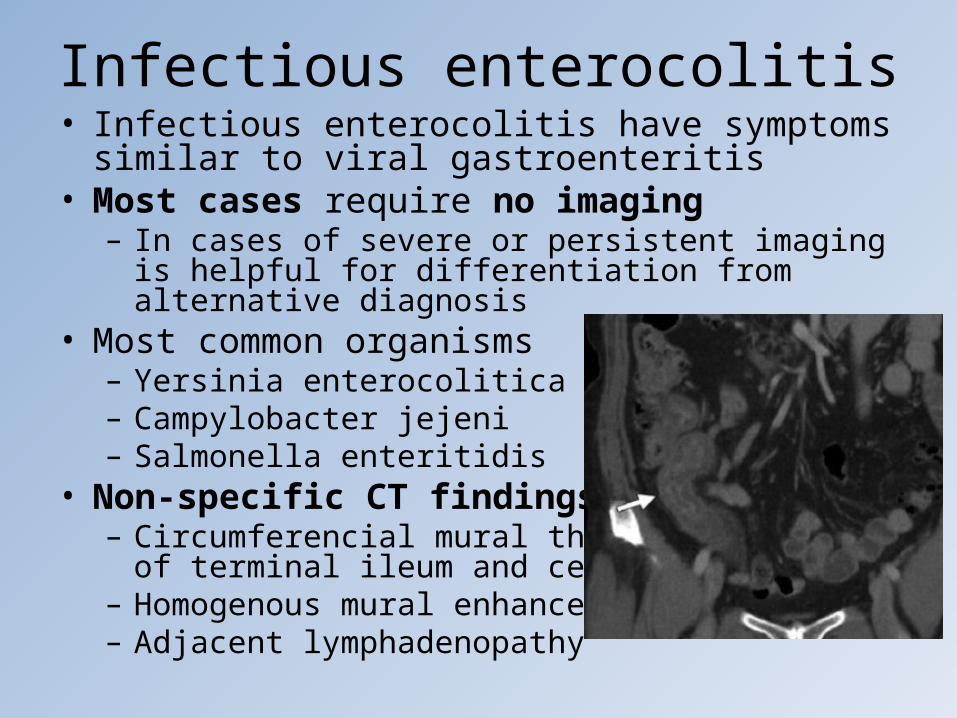
Infectious enterocolitis• Infectious enterocolitis have symptoms similar to viral
gastroenteritis• Most cases require no imaging
– In cases of severe or persistent imaging is helpful for differentiation from alternative diagnosis
• Most common organisms– Yersinia enterocolitica– Campylobacter jejeni– Salmonella enteritidis
• Non-specific CT findings– Circumferencial mural thickening
of terminal ileum and cecum– Homogenous mural enhancement– Adjacent lymphadenopathy

Neutropenic colitis (Typhlitis)• Neutropenic patient undergoing chemotherapy• RLQP, fever, diarrhoea, ± peritonitis• CT is study of choice if suspected
– Risk of bowel perforation with contrast enema or colonoscopy
• Typhlitis usually involves the right colon, but terminal ileum and transverse colon may be involved
• CT findings– Cecal distension– Circumferential wall thickening with areas of low
attenuation due to edema or necrosis– Inflammatory stranding of adjacent mesenteric fat, ±
lymphadenopathy
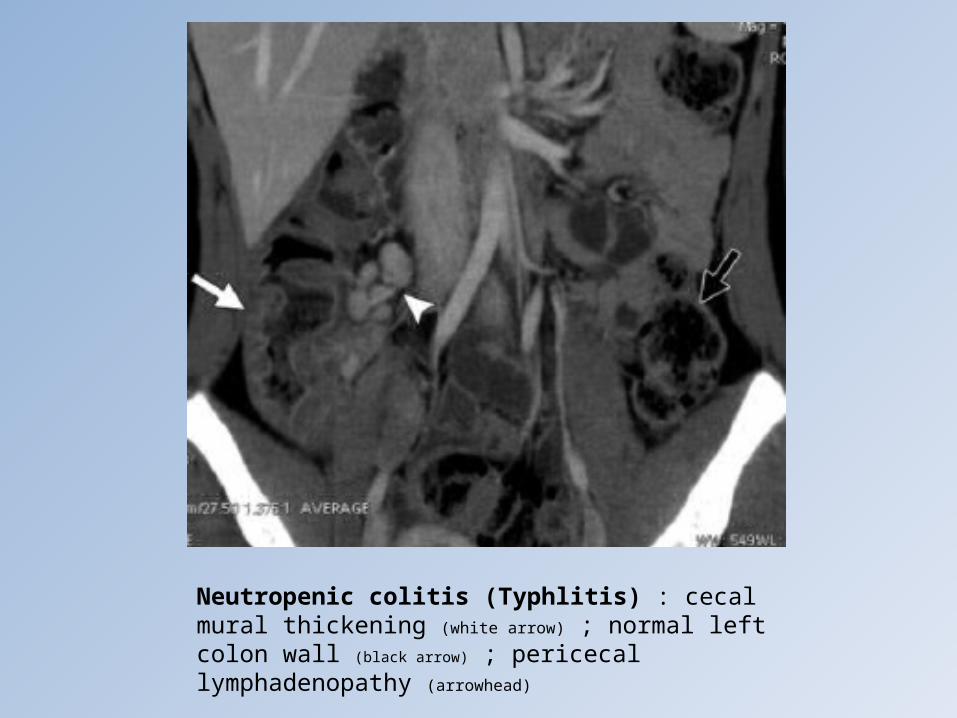
Neutropenic colitis (Typhlitis) : cecal mural thickening (white arrow) ; normal left colon wall (black arrow) ; pericecal lymphadenopathy (arrowhead)
Diverticulitis• One of the most common causes of acute
abdominal pain in the elderly• Left and sigmoid colon predominantly affected• Less commonly right colon and cecum may be
affected – mimicking appendicitis• CT investigation of choice
– Asymmetric or circumferential colonic wall thickening– Associated focal pericolic fat stranding– Inflammed diverticulum often visible at level of
maximal fat stranding– Normal appendix is important in differentiating from
appendicitis– Pericolic lymphnodes suggests malignancy rather than
diverticulitis

Diverticulitis • Rare causes
– Aquired small bowel diverticula• Mucosal herniation of bowel at sites of vscular entry• Mesenteric border of terminal ileum < 7,5 cm from
ileocecal valve
– Meckel diverticulum• Most common congenital abnormality of the GI tract• Omphalomesenteric duct does not obliterate during
development • Anti-mesenteric border of ileum, ± 100 cm from
ileocecal valve• May contain ectopic gastric mucosa
– Mucosal ulceration and GIT bleeding

Diverticulitis : Multiple right colonic diverticula ; adjacent fat stranding (arrow) ; sigmoid diverticula with no fat stranding (arrowheads)
Diverticulitis : Multiple sigmoid diverticula (straight white arrows) ; thick walled sigmoid colon (curved white arrow) ; mesenteric fat stranding (black arrow)

Epiploic appendagitis• Round fat containing peritoneal pouches
arising from serosal surface of the colon – 0,5 – 5 cm in lentgh– More common in left and sigmoid colon
• Uncommon and self limiting condition• Mostly middle aged men• Caused by torsion or
venous thrombosis of the epiploic appendages
• CT findings– Pericolic, round tot oval lesion
of fat attenuation with a hyperattenuating rim
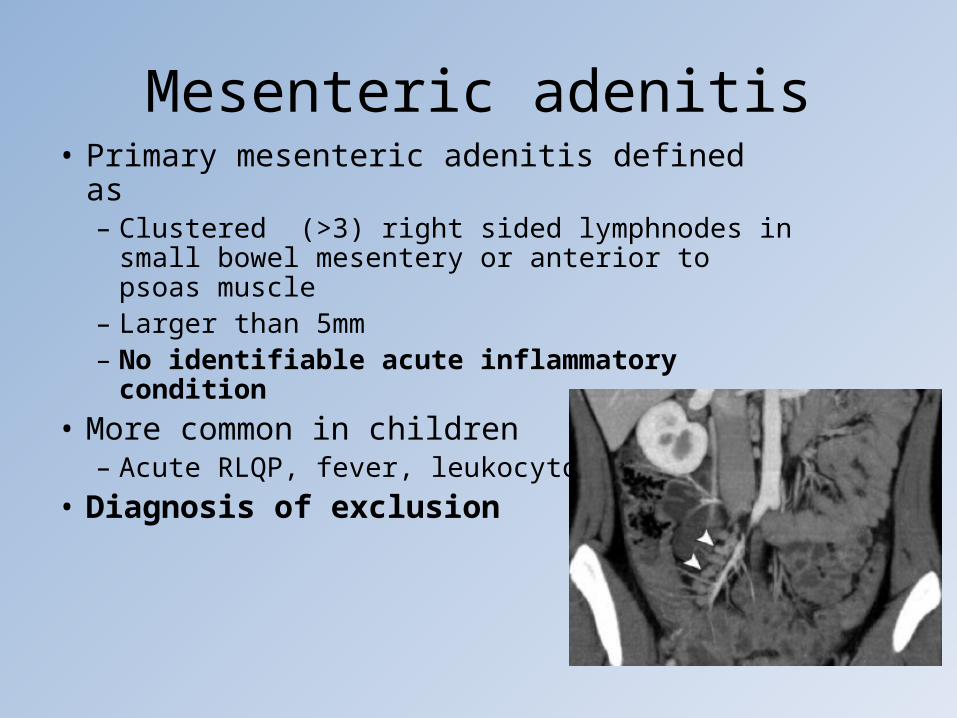
Mesenteric adenitis• Primary mesenteric adenitis defined as
– Clustered (>3) right sided lymphnodes in small bowel mesentery or anterior to psoas muscle
– Larger than 5mm– No identifiable acute inflammatory condition
• More common in children– Acute RLQP, fever, leukocytosis
• Diagnosis of exclusion
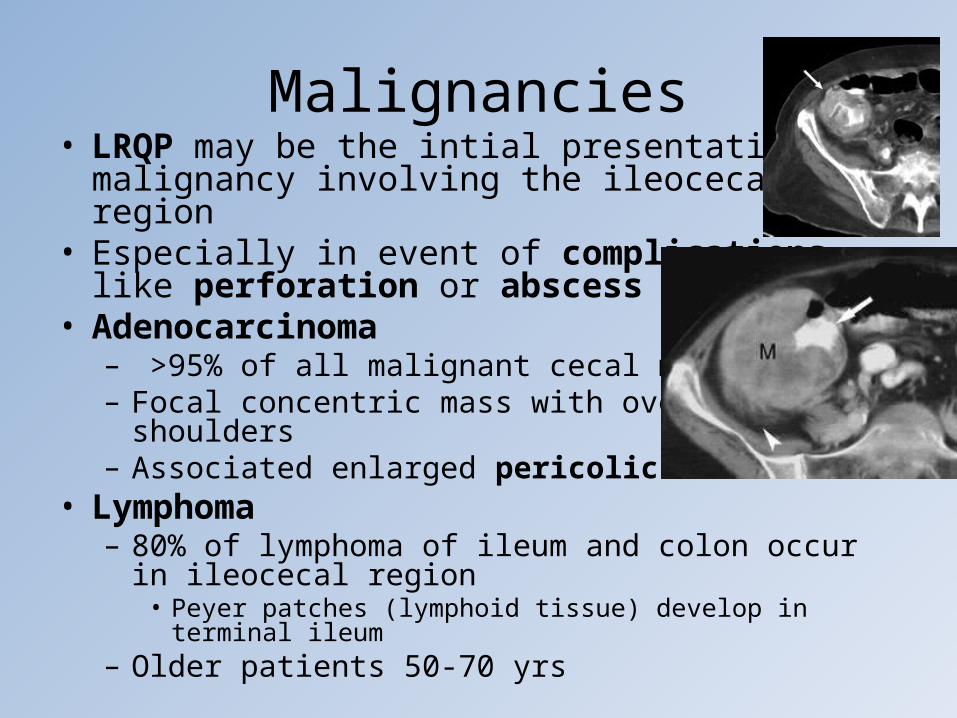
Malignancies• LRQP may be the intial presentation of
malignancy involving the ileocecal region• Especially in event of complications
like perforation or abscess • Adenocarcinoma
– >95% of all malignant cecal masses– Focal concentric mass with overhanging
shoulders– Associated enlarged pericolic nodes
• Lymphoma– 80% of lymphoma of ileum and colon occur in ileocecal
region• Peyer patches (lymphoid tissue) develop in terminal ileum
– Older patients 50-70 yrs

Malignancies • Lymphoma
– Non-specific symptoms (weight loss and abd pain), so often presents late
– Four forms of ileocecal lymphoma• Circumferential or constrictive
– Most common and may mimic adenocarcinoma
– Usually longer segment affected more gradual transition fromtumor to normal bowel
– Lack of bowel obstruction in presence of a large massshould raise suspicion of lymphoma
• Polypoid• Ulcerative• Aneurysmal
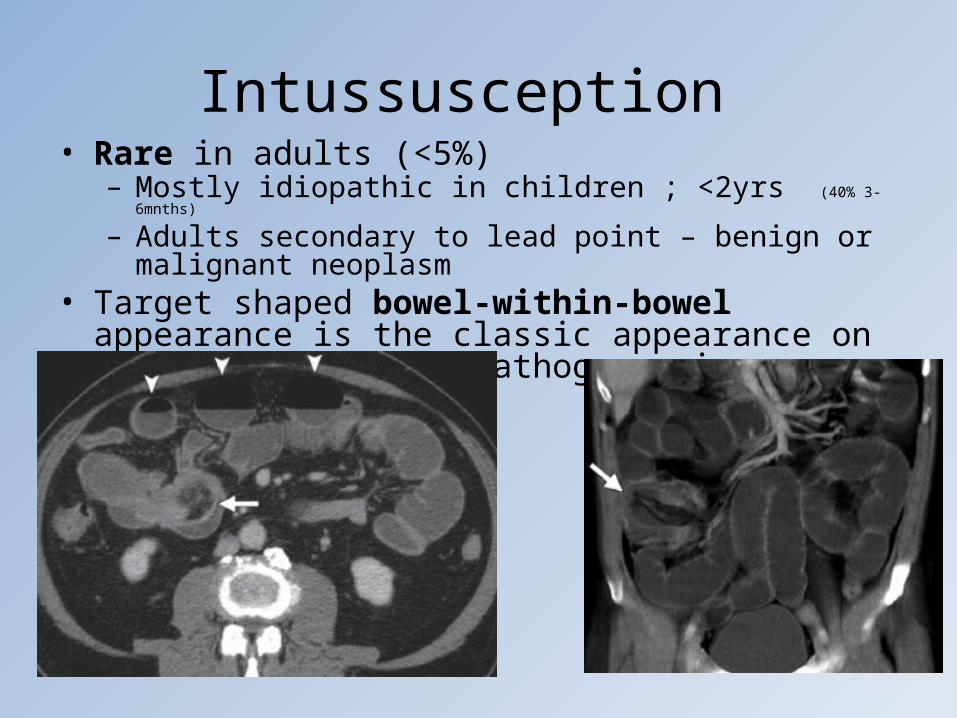
Intussusception • Rare in adults (<5%)
– Mostly idiopathic in children ; <2yrs (40% 3-6mnths)
– Adults secondary to lead point – benign or malignant neoplasm• Target shaped bowel-within-bowel appearance is the
classic appearance on axial scans and is pathognomonic
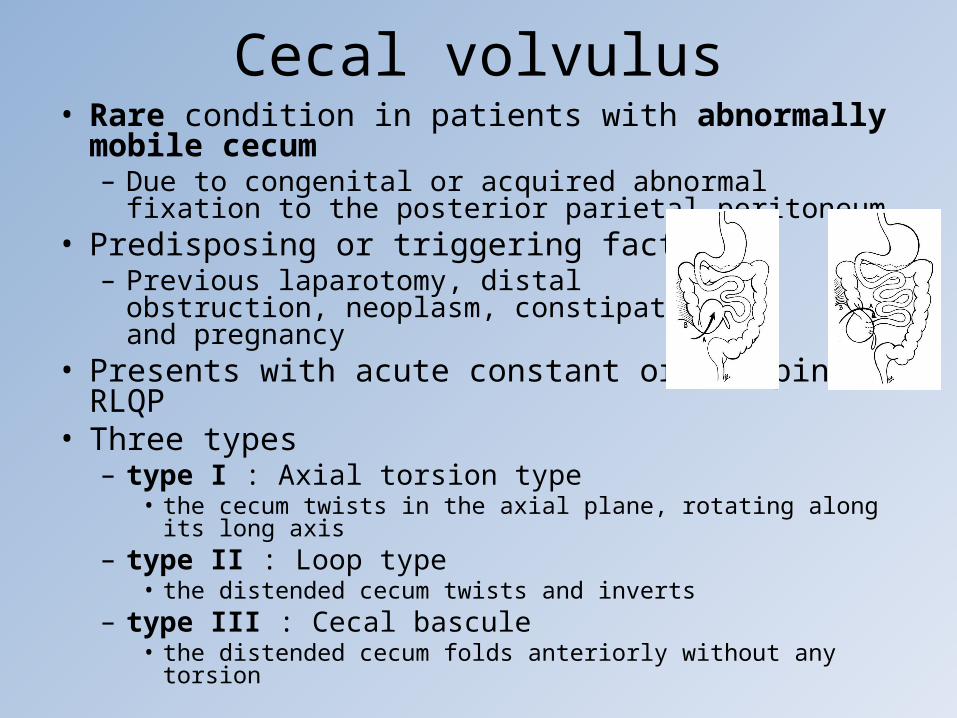
Cecal volvulus• Rare condition in patients with abnormally mobile
cecum– Due to congenital or acquired abnormal fixation to the
posterior parietal peritoneum• Predisposing or triggering factors
– Previous laparotomy, distal obstruction, neoplasm, constipation and pregnancy
• Presents with acute constant or cramping RLQP • Three types
– type I : Axial torsion type • the cecum twists in the axial plane, rotating along its long axis
– type II : Loop type• the distended cecum twists and inverts
– type III : Cecal bascule• the distended cecum folds anteriorly without any torsion

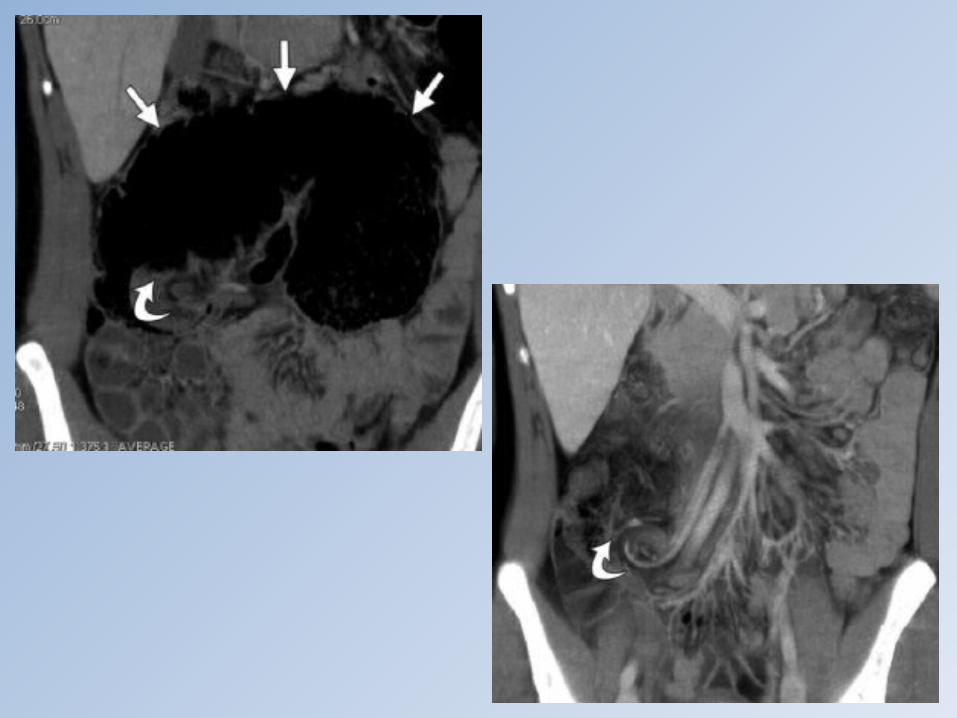
Cecal volvulus• Diagnosis on plain radiography < 50% of cases• MDCT can recognize subtypes and
complications (ischemia and obstruction)– combination of a distended ectopic cecum and
the swirl of the mesenteric vessels is seen in type I and II
– type II volvulus (the loop type), the cecum usually occupies the left upper quadrant
– in the bascule type, the swirl of the vessels is not present
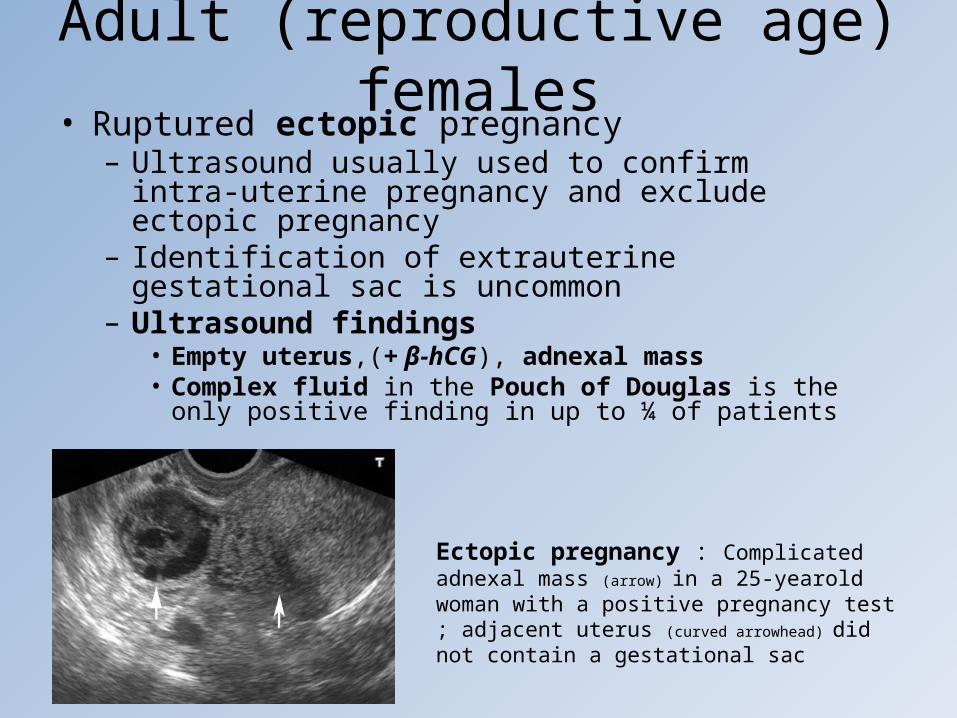
Adult (reproductive age) females• Ruptured ectopic pregnancy
– Ultrasound usually used to confirm intra-uterine pregnancy and exclude ectopic pregnancy
– Identification of extrauterine gestational sac is uncommon
– Ultrasound findings• Empty uterus,(+ β-hCG), adnexal mass• Complex fluid in the Pouch of Douglas is the only positive
finding in up to ¼ of patients
Ectopic pregnancy : Complicated adnexal mass (arrow) in a 25-yearold woman with a positive pregnancy test ; adjacent uterus (curved
arrowhead) did not contain a gestational sac
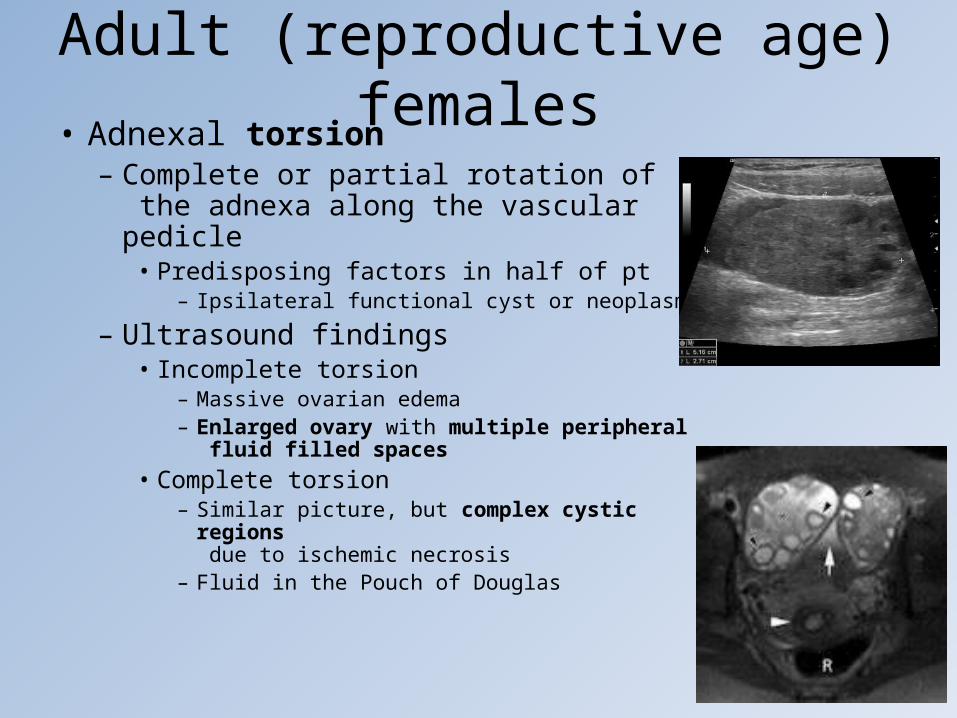
Adult (reproductive age) females• Adnexal torsion
– Complete or partial rotation of the adnexa along the vascular pedicle
• Predisposing factors in half of pt– Ipsilateral functional cyst or neoplasm
– Ultrasound findings• Incomplete torsion
– Massive ovarian edema– Enlarged ovary with multiple peripheral
fluid filled spaces• Complete torsion
– Similar picture, but complex cystic regions due to ischemic necrosis
– Fluid in the Pouch of Douglas
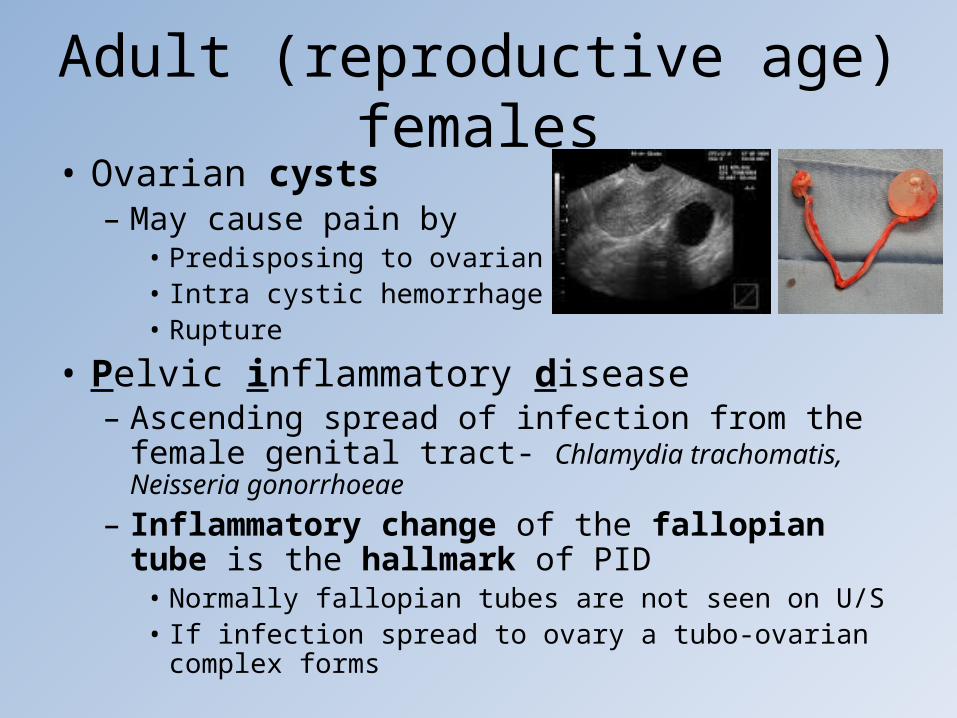
Adult (reproductive age) females• Ovarian cysts
– May cause pain by • Predisposing to ovarian torsion• Intra cystic hemorrhage• Rupture
• Pelvic inflammatory disease – Ascending spread of infection from the female genital
tract- Chlamydia trachomatis, Neisseria gonorrhoeae
– Inflammatory change of the fallopian tube is the hallmark of PID
• Normally fallopian tubes are not seen on U/S• If infection spread to ovary a tubo-ovarian complex forms
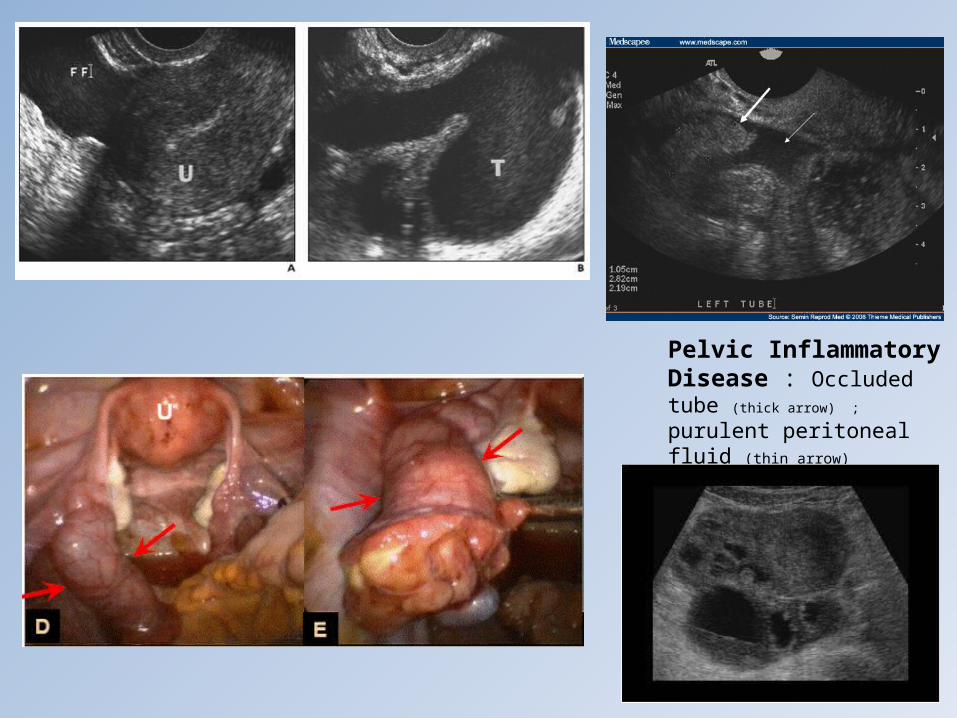
Pelvic Inflammatory Disease : Occluded tube (thick arrow) ; purulent peritoneal fluid (thin arrow)

Adult (reproductive age) females• Endometriosis
– Most common cause of chronic pelvic pain • May occasionally present acutely
– Endometrial tissue present outside the uterus • Pouch of Douglas, ovaries, pelvic peritoneum• GIT
– Rectosigmoid colon– Ileum, jejunum and cecum– Appendix <1%
– Transvaginal U/S of value in acute setting if suspected

– MRI of pelvis in more elective situation• Endometriomas high signal on T1 and heterogenous
high T2• Fat-Sat increases sensitivity• Lesions > 1cm routinely seen

Adult (reproductive age) females
• Ruptured ovarian follicle– During mid cycle rupture may realease small
amount of blood– Resultant peritoneal irritation may cause transient
pain – mittelschmertz
Food for thoughtFood for thought• Diagnostic laparoscopy in the evaluation of right lower abdominal pain: a one-year audit.• Authors : Lim GH, Shabbir A, So JB Institution Department of Surgery, National University Hospital,Singapore. • Source : Singapore Med J 2008 Jun; 49(6) :451-3.Abstract
• INTRODUCTIONAcute appendicitis is the commonest cause for right lower abdominal pain. Clinical features, laboratory and imaging investigations are either not very sensitive or specific, and neither is therapeutic. We aimed to define the role of diagnostic laparoscopy in patients with right lower abdominal pain.METHODSData was collected retrospectively from January 1, 2005 to December 31, 2005. Patients admitted to the Emergency Department and subsequently transferred to the Department of Surgery, National University Hospital, Singapore, with right lower abdominal pain and who eventually underwent diagnostic laparoscopy were evaluated.RESULTS691 patients with right lower abdominal pain were admitted with suspected diagnosis of appendicitis. Diagnostic laparoscopy was undertaken in 103 patients aged 17-71 years old. Of the 83 females, 78 (94 percent) were premenopausal . Histology-proven acute appendicitis was diagnosed in 78 (75.7 percent) patients. Interestingly, within this group, 25.6 percent had other concomitant pathologies found on laparoscopy. 25 patients had a normal appendix; gynaecological causes accounted for pain in 15 of these 25 (60 percent) cases. In four (3.9 percent) patients, no pathology was found. Complication rate was 1.9 percent, which included ileus in two patients. In 32 (31.1 percent) patients, diagnostic laparoscopy altered the management plan, requiring either intervention or care by a subspecialty.CONCLUSIONDiagnostic laparoscopy is useful in evaluating patients with right lower abdominal pain, especially in those with equivocal signs of acute appendicitis. It also has the additional benefit of being therapeutic. Premenopausal women benefit the most from this procedure.

Food for thoughtFood for thought• Right iliac fossa pain in women. Conventional diagnostic approach
versus primary laparoscopy. A controlled study (65 cases)Authors Champault G, Rizk N, Lauroy J, et al.
• Institution Service de Chirurgie Générale et Digestive, Hôpital Jean-Verdier, Bondy.Source Ann Chir 1993; 47(4) :316-9. Abstract
In a series of 187 patients with acute abdominal pain syndrome, 65 young women reported non specific pain in right iliac or pelvic area. A controlled study compared 33 patients with immediate laparoscopy and 32 explored with a laboratory contrast or imaging approach. In the laparoscopic group, an exact diagnosis was made in 97% of the patients, allowing in 2/3 of cases the endoscopic treatment. Only 28% in the second group had an exact diagnosis. Hospital stay was shorter in the laparoscopic group (4.18 vs 6.16 days; p = 0.01) decreasing the hospital cost. The authors suggest that immediate laparoscopy should be performed in young women presenting with non-specific abdominal pain.

References • Hoeffel C, Crema MD, Belkacem A et al. Multi-detector row CT: spectrum
of diseases involving the ileocecal area. RadioGraphics 2006; 26: 1373-1390.
• Pedrosa I, Zeikus EA, Levine D & Rofsky NM. MR imaging of acute right lower quadrant pain in pregnant and nonpregnant patients. RadioGraphics 2007; 27: 721-753.
• Purysko AS, Remer EM, Leao Filho HM et al. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. RadioGraphics 2011; 31: 927-947.
• Anderson EM & Bungay HK. Imaging investigation of acute right iliac fossa pain. Imaging 2006; 18: 257-267.
• Department of Health Western Australia. Diagnostic imaging pathways: acute right iliac fossa pain on www.imagingpathways.health.wa.gov.au (last accessed on 07/03/2012).