riesgo de cáncer de ovario - seom.org · fcc: adenoma tubular con dbg. polipo inflamatorio...
TRANSCRIPT
Riesgo de Cáncer de Ovario
Riesgo de CO 10 años después del dx del CM:
BRCA1 12,7%BRCA2 6,8%
Un 25% de la mortalidad en mujeresdiagnosticadas de CM en estadio I será por un Cáncer de Ovario
Paciente 40 a, BRCA1+, menopausia post QT.
¿Qué estrategia recomendarías para la prevención del CO?
1-CRIBADO DEL CO con ECOTV + CA 125 C/ 6-12m.
2-SALPINGO-OOFORECTOMIA BILATERAL PROFILACTICA (SOBP)
3-SALPINGUECTOMIA
¿es efectivo el cribado del CO en BRCA+?
Article moyer: del annals of internal medicine
A pesar del cribado anual, una alta propocion de CO en BRCA son deIntervalo y la mayoria se dx en estadios avanzadosIntervalo y la mayoria se dx en estadios avanzados. Es improbable que tenga un impacto en reducir la mortalidad.
Diciembre 2010: ECOTV I CA 125: NORMALES
Abril 2011: urgencias
ECOTV: Imagen ovárica izquierda de 69x67 mm mixta deECOTV: Imagen ovárica izquierda de 69x67 mm mixta de predominio sólido hipervascularitzada, compatible con proceso neoplásico. Imagen ovárica derecha de 29 mm
Ca 125= 86

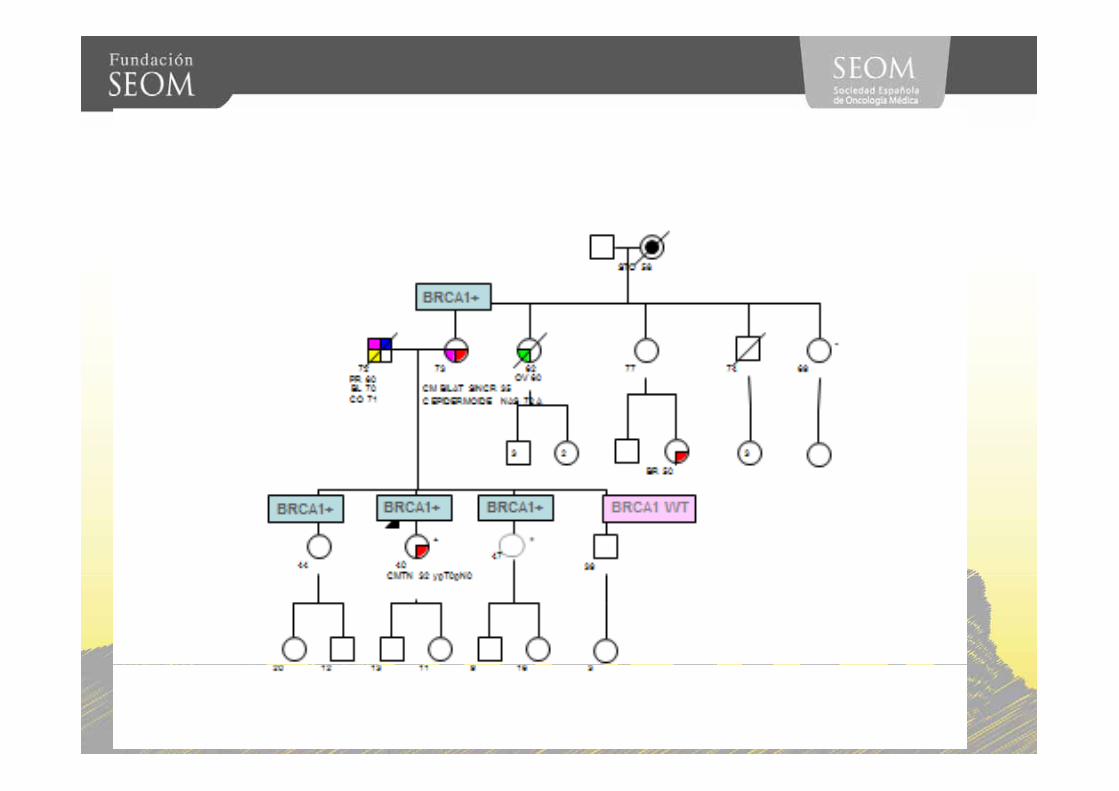
STO 58
+
STO 58
-
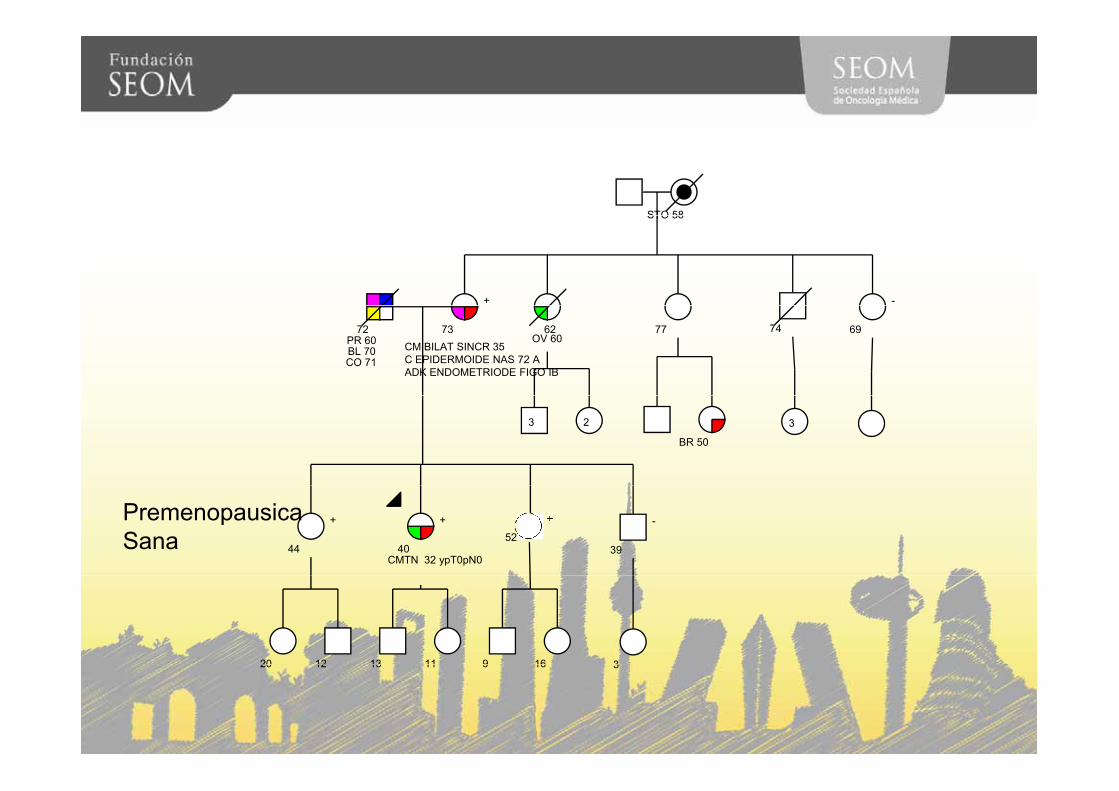
72PR 60BL 70CO 71
73CM BILAT SINCR 35C EPIDERMOIDE NAS 72 AADK ENDOMETRIODE FIGO IB
62OV 60
77 74 69
3 2
BR 50
3
40CMTN 32 ypT0pN0
+
44
+
39
-52
PremenopausicaSana
13 11 9 1620 12 313 11 9 1620 12 3
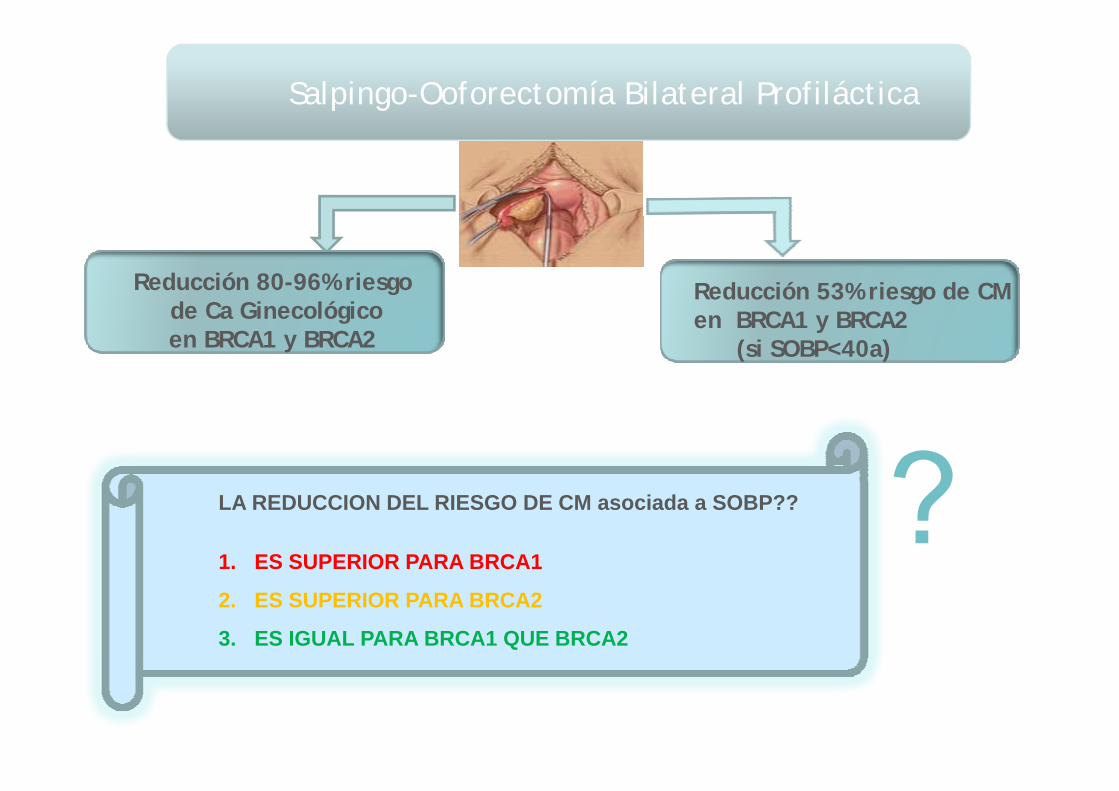
Salpingo-Ooforectomía Bilateral Profiláctica
Reducción 80-96% riesgod C Gi lógi
Reducción 53% riesgo de CM de Ca Ginecológicoen BRCA1 y BRCA2
en BRCA1 y BRCA2(si SOBP<40a)
??LA REDUCCION DEL RIESGO DE CM asociada a SOBP??
1. ES SUPERIOR PARA BRCA1
2. ES SUPERIOR PARA BRCA2
3. ES IGUAL PARA BRCA1 QUE BRCA2
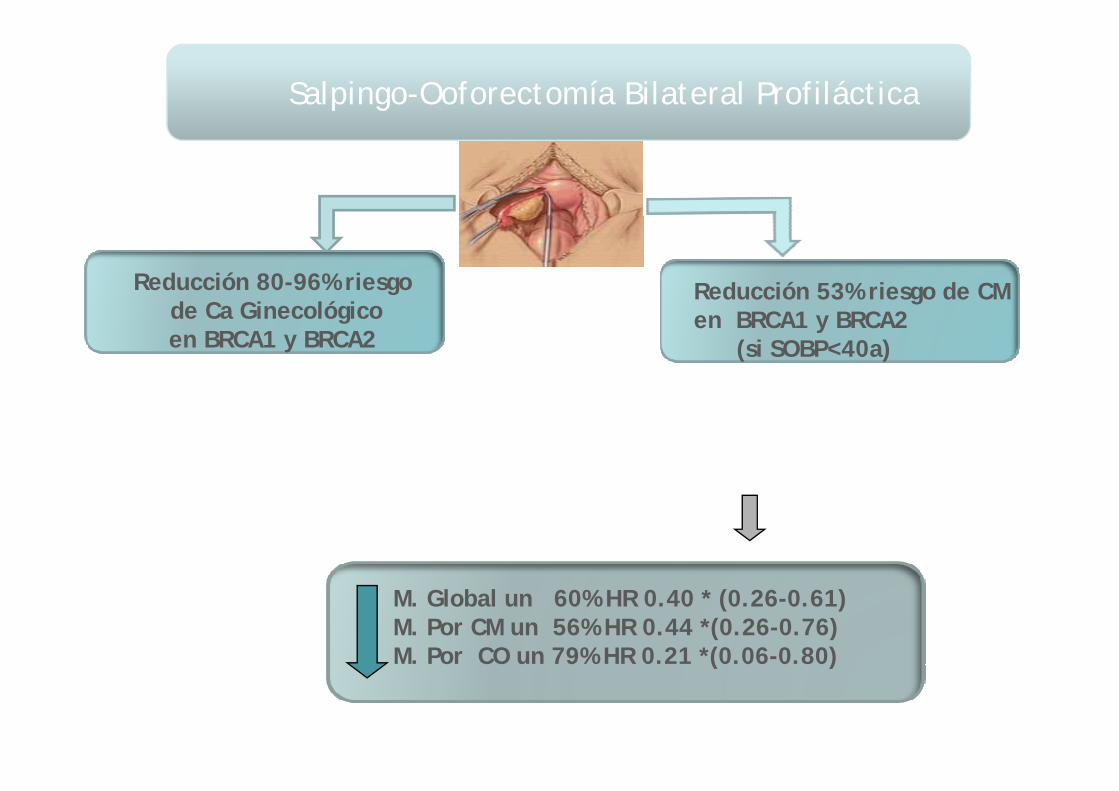
Salpingo-Ooforectomía Bilateral Profiláctica
Reducción 80-96% riesgod C Gi lógi
Reducción 53% riesgo de CM de Ca Ginecológicoen BRCA1 y BRCA2
en BRCA1 y BRCA2(si SOBP<40a)
??¿Reduce la mortalidad?¿Reduce la mortalidad?
Salpingo-Ooforectomía Bilateral Profiláctica
Reducción 80-96% riesgod C Gi lógi
Reducción 53% riesgo de CM de Ca Ginecológicoen BRCA1 y BRCA2
en BRCA1 y BRCA2(si SOBP<40a)
M. Global un 60% HR 0.40 * (0.26-0.61)M. Por CM un 56% HR 0.44 *(0.26-0.76)M. Por CO un 79% HR 0.21 *(0.06-0.80)( )
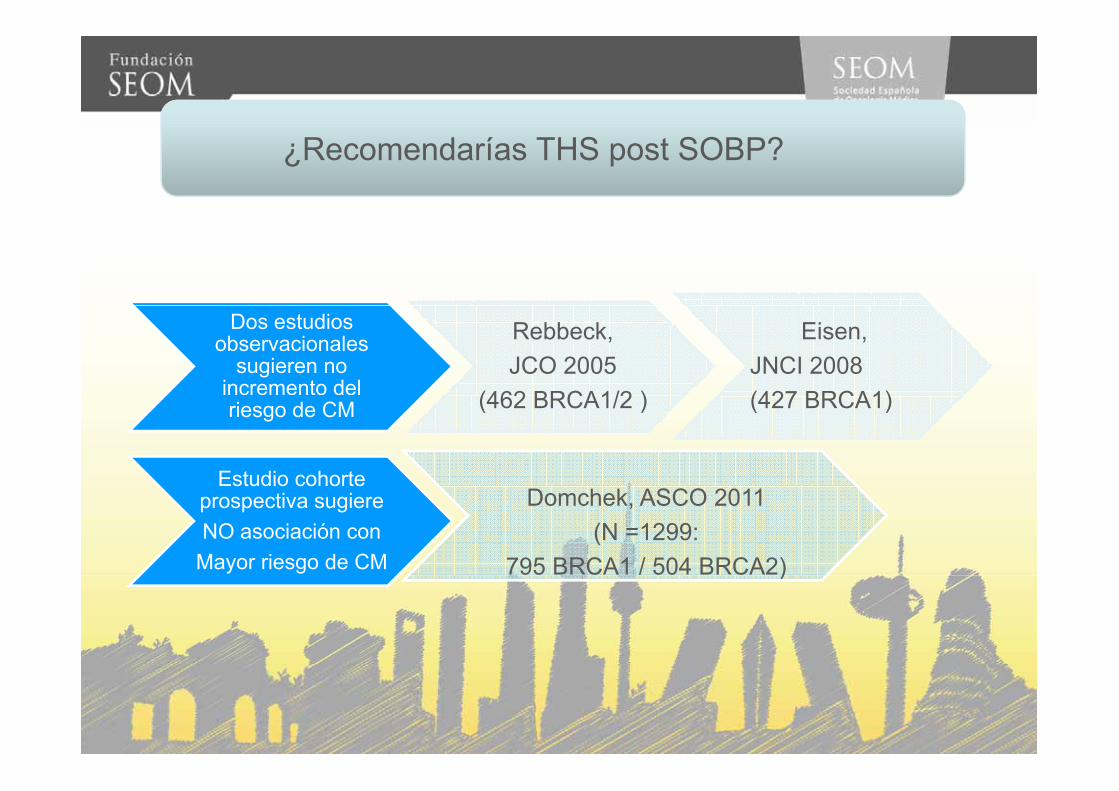
¿Recomendarías THS post SOBP?
Dos estudios observacionales
sugieren no incremento del
Rebbeck, JCO 2005
(462 BRCA1/2 )
Eisen, JNCI 2008 (427 BRCA1)riesgo de CM (462 BRCA1/2 ) (427 BRCA1)
Estudio cohorteEstudio cohorteprospectiva sugiereNO asociación con
Mayor riesgo de CM
Domchek, ASCO 2011 (N =1299:
795 BRCA1 / 504 BRCA2))

52 años BRCA1+ postmenopausica52 años, BRCA1+, postmenopausica.
?¿Que beneficios le aportará una SOBP ?: ?1-reducir el riesgo de Ca Trompa/ovario
2-reducir el riesgo de CM
3-reducir ambos riesgos
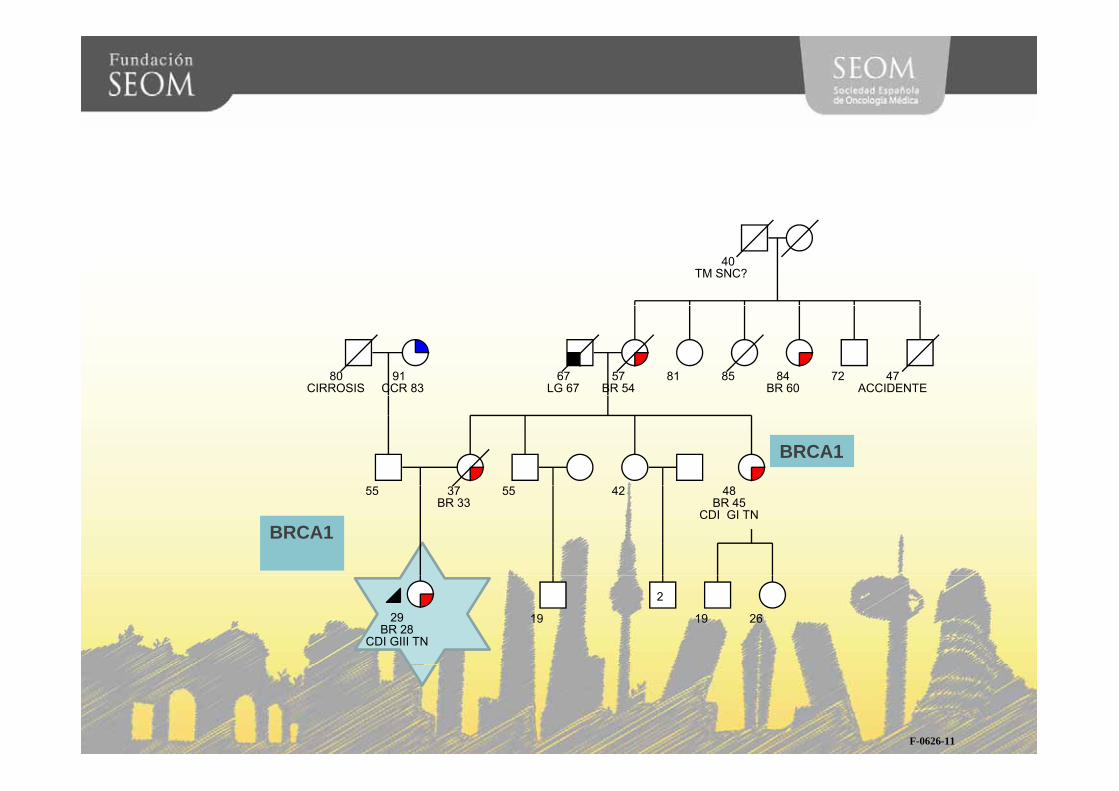
40TM SNC?
80CIRROSIS
67LG 67
57BR 54
91CCR 83
81 85 84BR 60
72 47ACCIDENTE
+BRCA1
55 37BR 33
55 42 48BR 45
CDI GI TN BRCA1
29BR 28
CDI GIII TN
19
2
19 26
F-0626-11
TRATAMIENTO DE CM BRCA
TRATAMIENTO QUIRURGICOEdad/ Estadio tm / Preferencias paciente TRATAMIENTO SISTEMICO
CONSERVADOR MASTECTOMIACONSERVADOR
MASTECTOMIAUNILATERAL
MASTECTOMIABILATERALPROFILACTICA
RIESGO DE 2ºCM IPSILATERAL(RECIDIVA/2º TM)
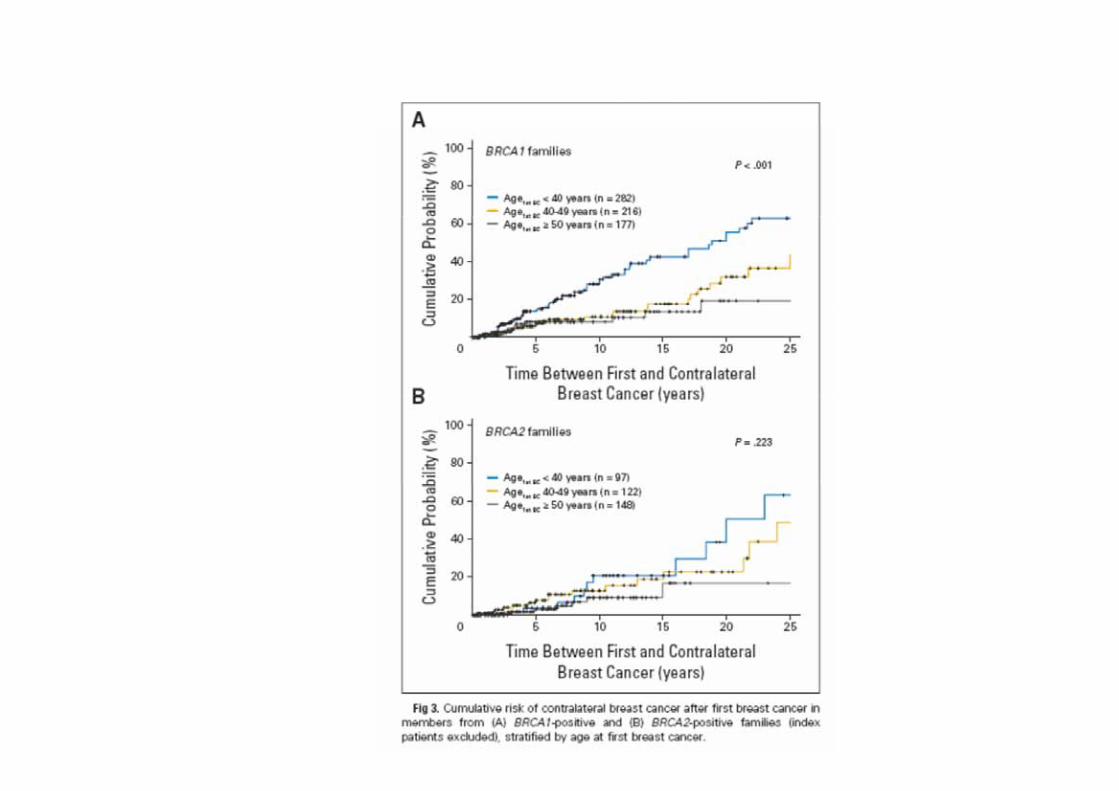
RIESGO DE CMCONTRALATERAL
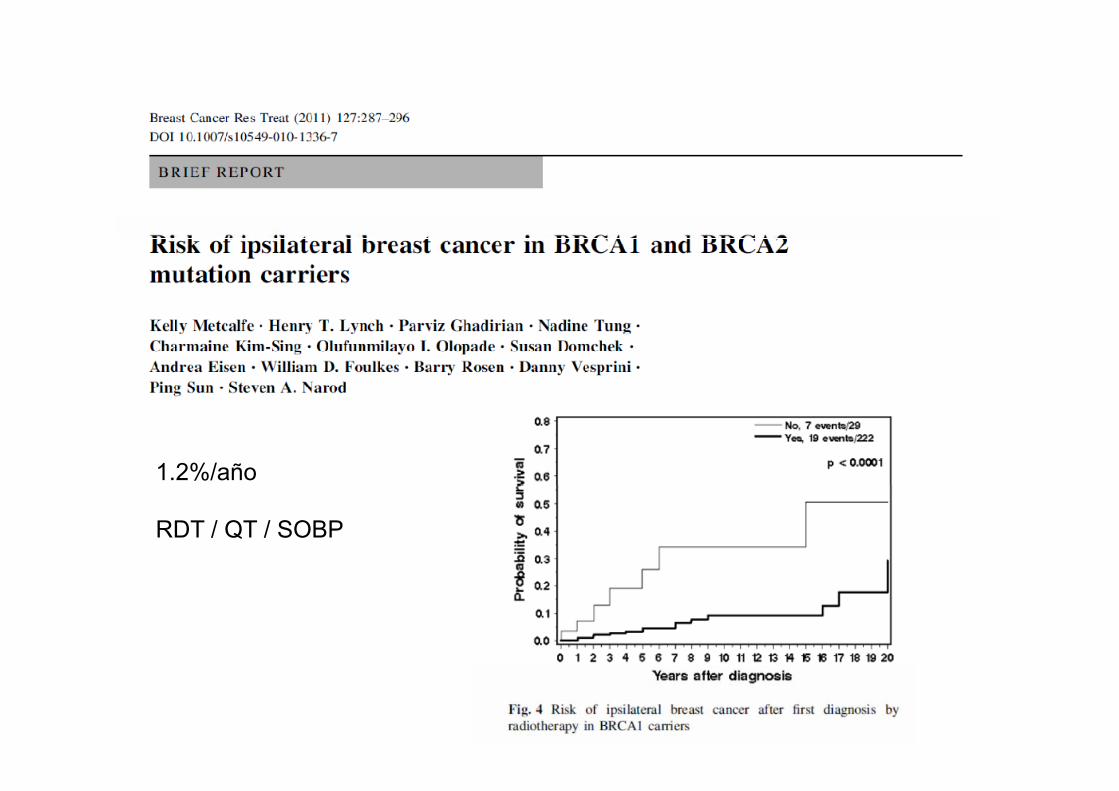
1.2%/año
RDT / QT / SOBP
TRATAMIENTO DE CM BRCA
TRATAMIENTO QUIRURGICOEdad/ Estadio tm / Preferencias paciente TRATAMIENTO SISTEMICO
CONSERVADOR MASTECTOMIACONSERVADOR
MASTECTOMIAUNILATERAL
MASTECTOMIABILATERALPROFILACTICA
RIESGO DE 2ºCM IPSILATERAL(RECIDIVA/2º TM)
RIESGO DE CMCONTRALATERAL
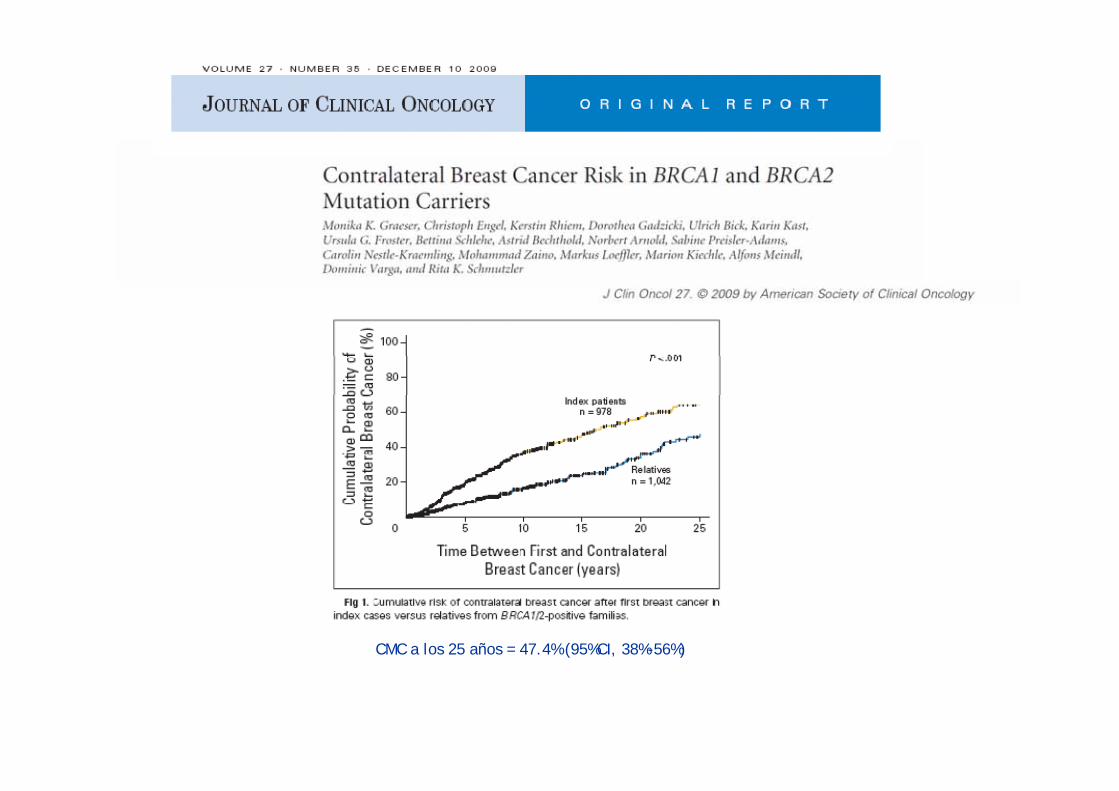
CMC a los 25 años = 47.4% (95%CI, 38%-56%)
¿Si esta paciente, tuviera 51 años, le recomendarías una Mastectomía contralateral?
SISINO
¿Cómo reducir este riesgo de CMC?¿Cómo reducir este riesgo de CMC?
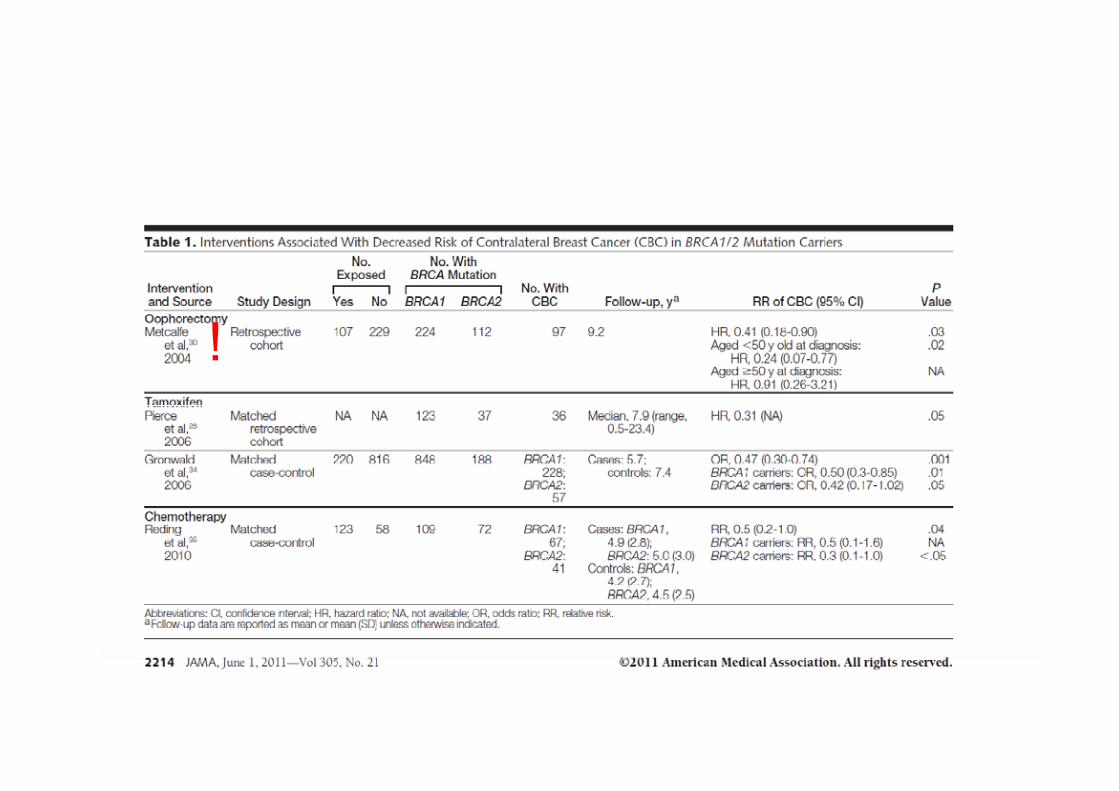
!
¿Impacto en la Mortalidad?SINONO
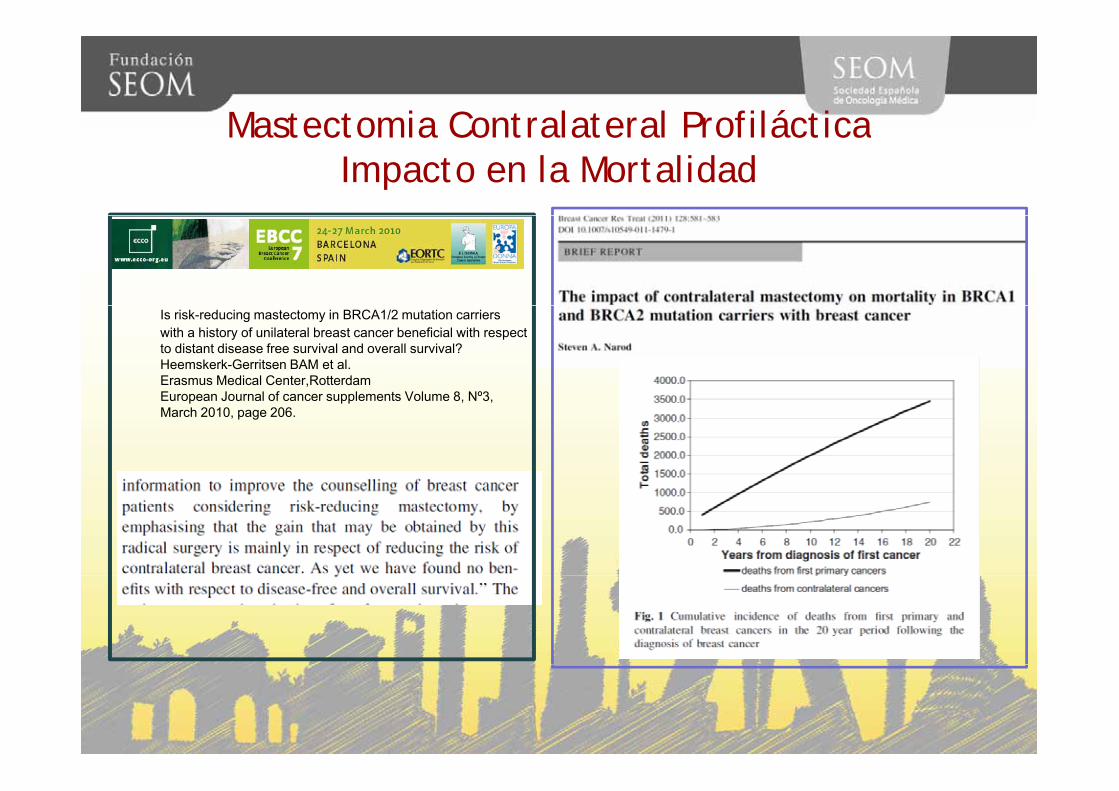
Mastectomia Contralateral ProfilácticaMastectomia Contralateral ProfilácticaImpacto en la Mortalidad
Is risk-reducing mastectomy in BRCA1/2 mutation carrierswith a history of unilateral breast cancer beneficial with respectto distant disease free survival and overall survival?Heemskerk-Gerritsen BAM et al.Erasmus Medical Center,RotterdamEuropean Journal of cancer supplements Volume 8 Nº3European Journal of cancer supplements Volume 8, Nº3, March 2010, page 206.

TRATAMIENTO DE CM BRCATRATAMIENTO DE CM BRCA
TRATAMIENTO QUIRURGICOEdad/ Estadio tm / Preferencias paciente TRATAMIENTO SISTEMICO
CONSERVADOR MASTECTOMIACONSERVADOR
MASTECTOMIAUNILATERAL
MASTECTOMIABILATERALPROFILACTICA
RIESGO DE 2ºCM IPSILATERAL(RECIDIVA/2º TM)
RIESGO DE CMCONTRALATERAL
¿Antes de la QT?
Preservación fertilidad:• Criopreservación de embrionesp• Criopreservacion de óvulos
Informar opcion DGPI en un futurop

So far, only five pregnancies after PGD for BRCA1/2 have been reported since the first was described in 2008 (1) The slow uptake reflects not just thethe first was described in 2008.(1) The slow uptake reflects not just the controversial nature of the procedure, but also concerns over patient selection and the safety of hormonal stimulation for IVF in women at risk themselves of breast and ovarian cancers.breast and ovarian cancers.
renc
e,nn
ualc
onfe
mbr
iolo
gyan
ion
and
Em
Rep
rodu
cti
yof
Hum
an
AN
Soc
iety
)E
UR
OP
EA
July
2012
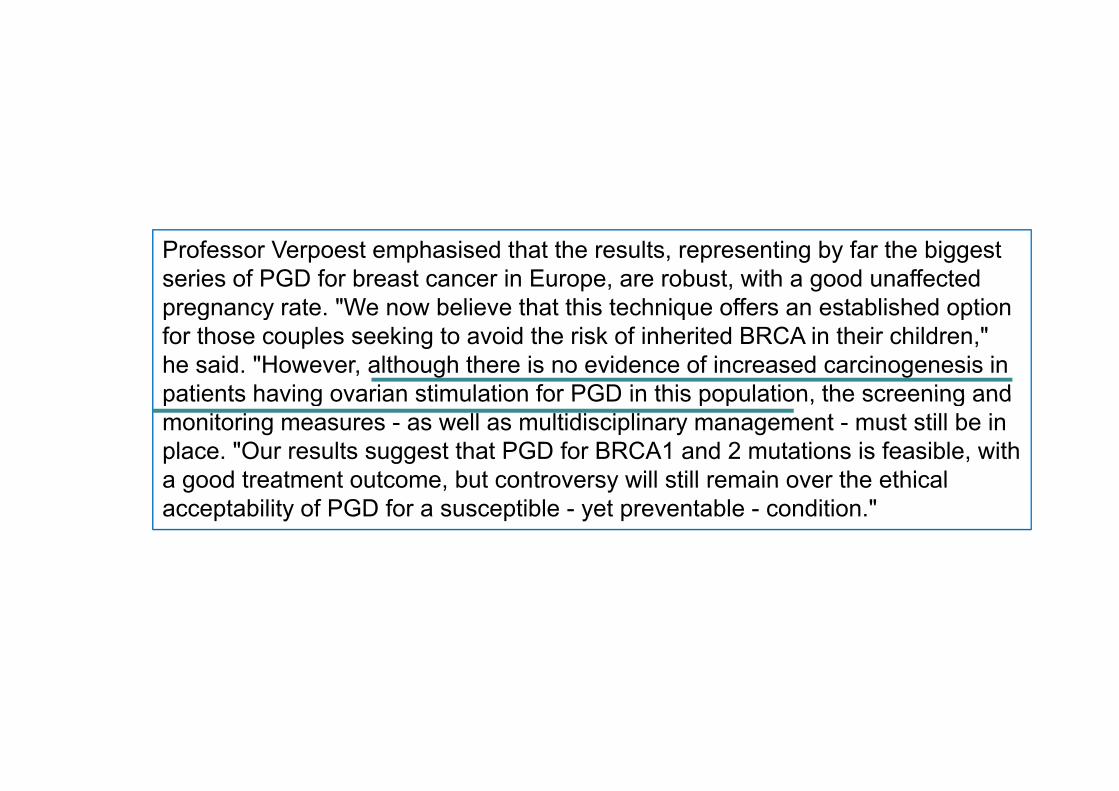
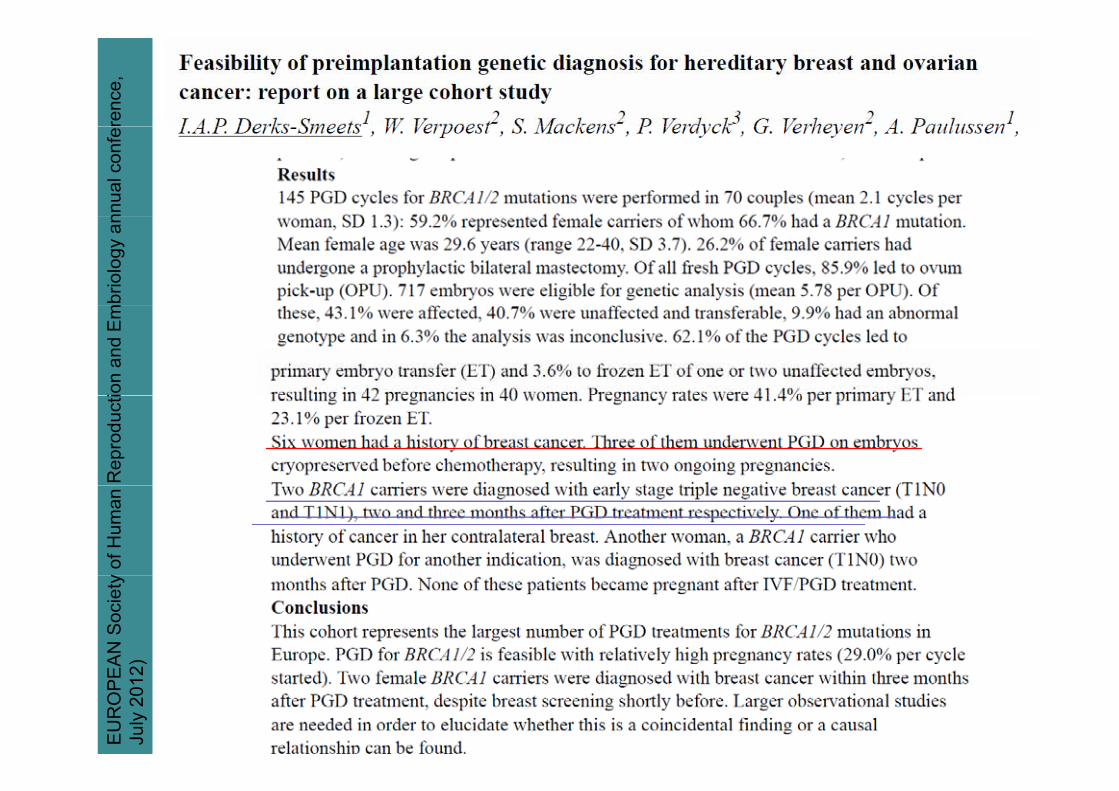
Professor Verpoest emphasised that the results, representing by far the biggest series of PGD for breast cancer in Europe, are robust, with a good unaffected pregnancy rate "We now believe that this technique offers an established optionpregnancy rate. We now believe that this technique offers an established option for those couples seeking to avoid the risk of inherited BRCA in their children," he said. "However, although there is no evidence of increased carcinogenesis in patients having ovarian stimulation for PGD in this population the screening andpatients having ovarian stimulation for PGD in this population, the screening and monitoring measures - as well as multidisciplinary management - must still be in place. "Our results suggest that PGD for BRCA1 and 2 mutations is feasible, with a good treatment outcome, but controversy will still remain over the ethicala good treatment outcome, but controversy will still remain over the ethical acceptability of PGD for a susceptible - yet preventable - condition."
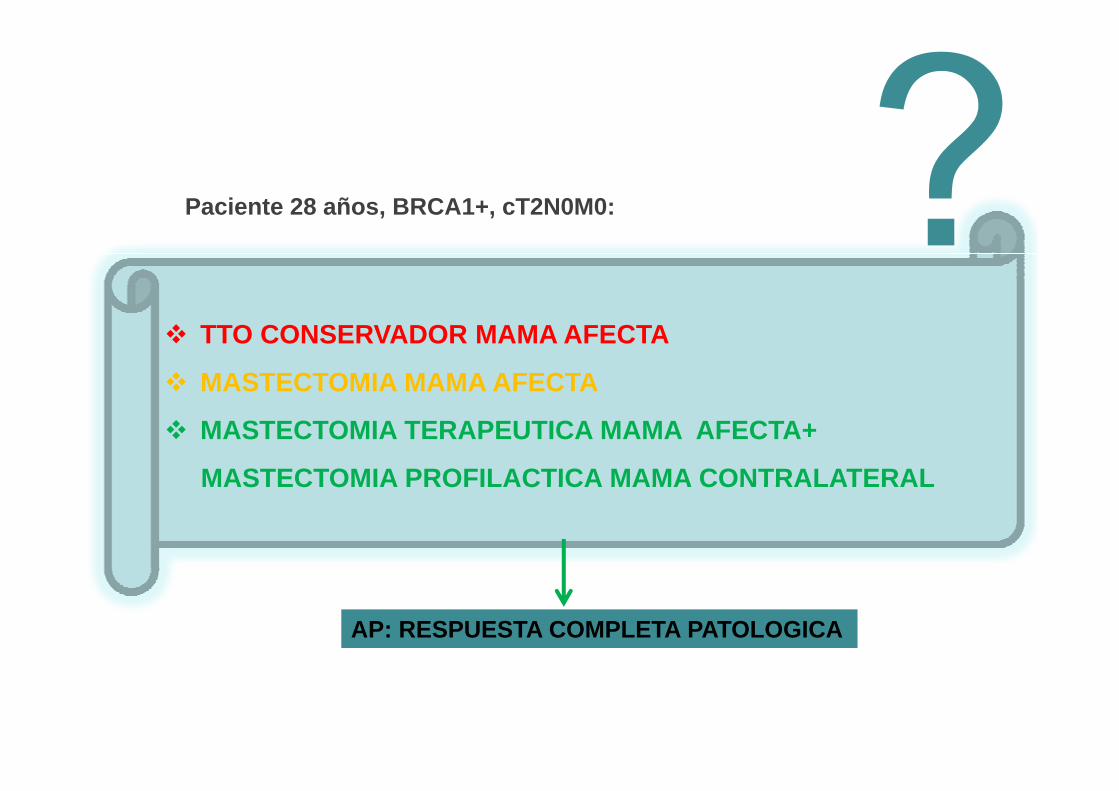
Paciente 28 años, BRCA1+, cT2N0M0: , ,
TTO CONSERVADOR MAMA AFECTA
MASTECTOMIA MAMA AFECTA
MASTECTOMIA TERAPEUTICA MAMA AFECTA+
MASTECTOMIA PROFILACTICA MAMA CONTRALATERALMASTECTOMIA PROFILACTICA MAMA CONTRALATERAL
AP: RESPUESTA COMPLETA PATOLOGICA
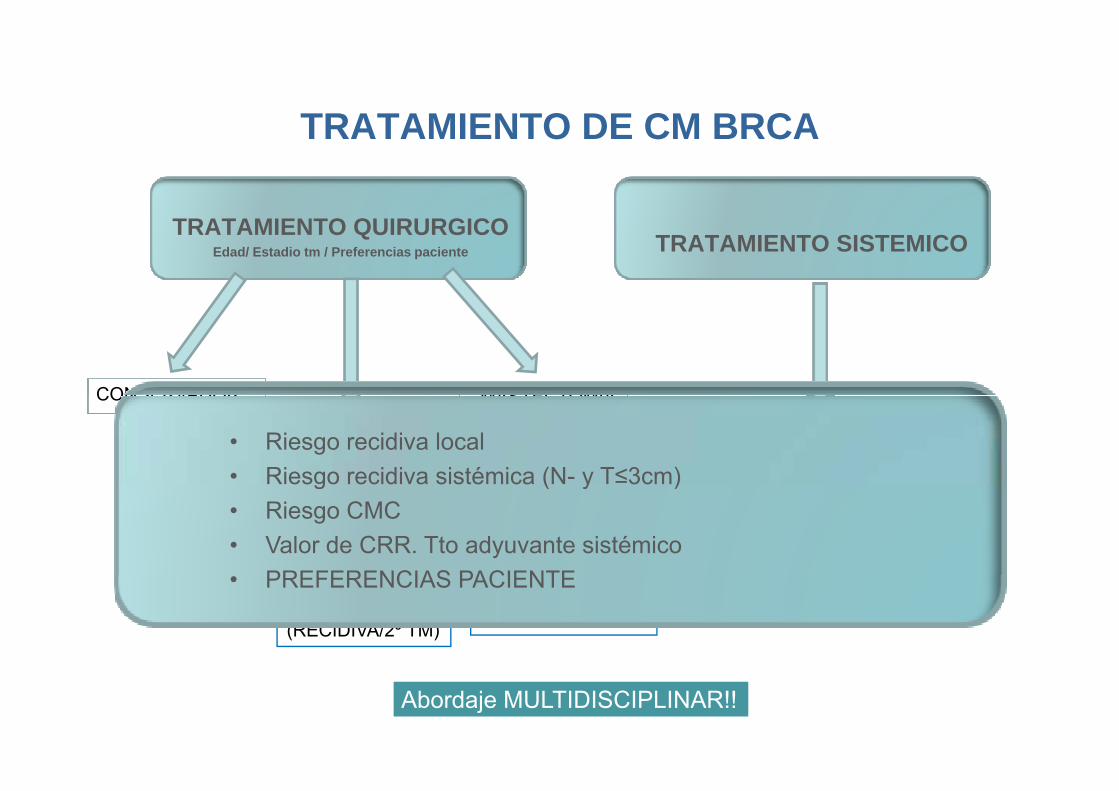
TRATAMIENTO DE CM BRCATRATAMIENTO DE CM BRCA
TRATAMIENTO QUIRURGICOEdad/ Estadio tm / Preferencias paciente TRATAMIENTO SISTEMICO
CONSERVADOR MASTECTOMIACONSERVADOR
MASTECTOMIAUNILATERAL
MASTECTOMIABILATERALPROFILACTICA ¿El CM en BRCA+ es mas
Sensible a la QT que el CM ádi ??
• Riesgo recidiva local• Riesgo recidiva sistémica (N- y T≤3cm)
esporádico??
Tto INDIVIDUALIZADO en BRCA?
E d i i t i
g ( y )• Riesgo CMC• Valor de CRR. Tto adyuvante sistémico
PREFERENCIAS PACIENTERIESGO DE 2ºCM IPSILATERAL(RECIDIVA/2º TM)
RIESGO DE CMCONTRALATERAL
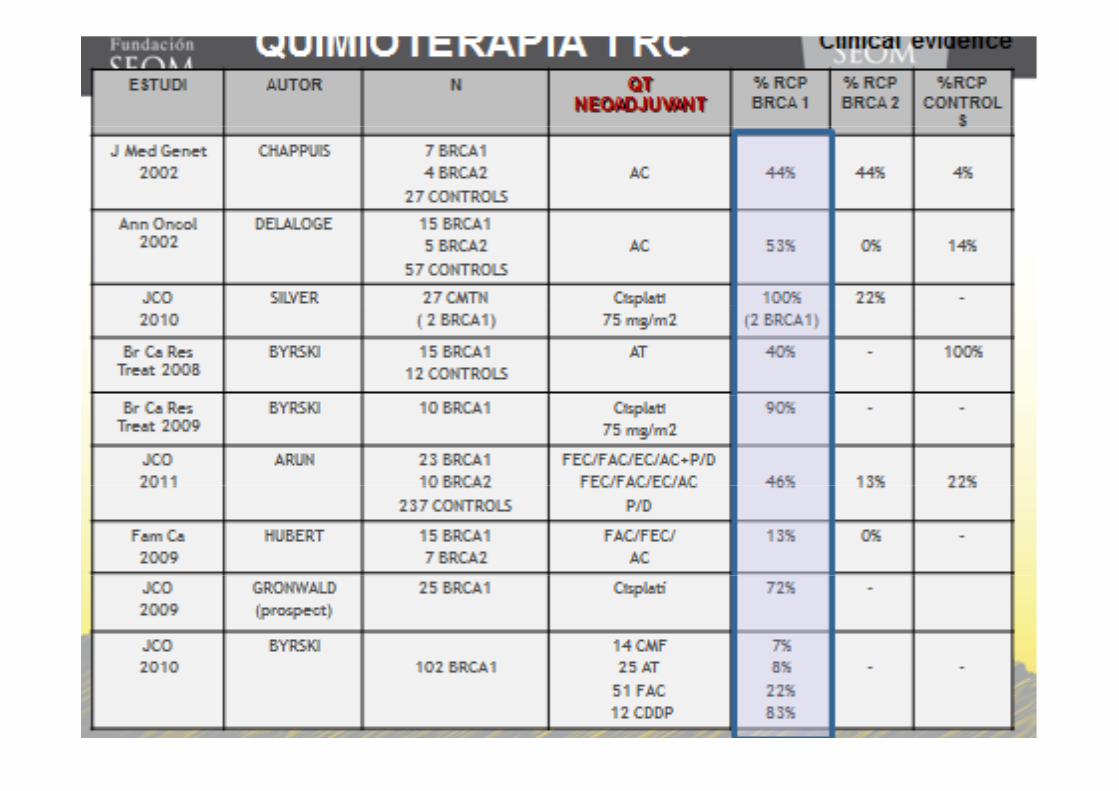
¿Esquema de quimioterapia recomendarías a BRCA+?
• PREFERENCIAS PACIENTE
Abordaje MULTIDISCIPLINAR!!
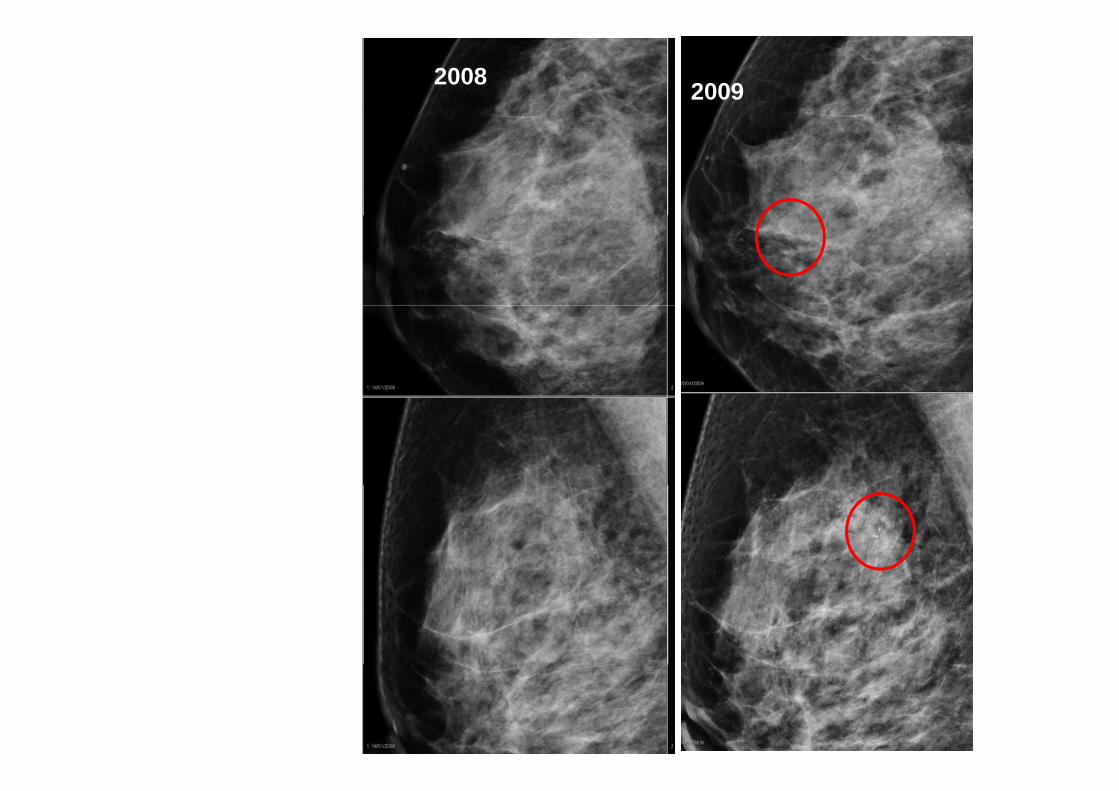
2008 2009
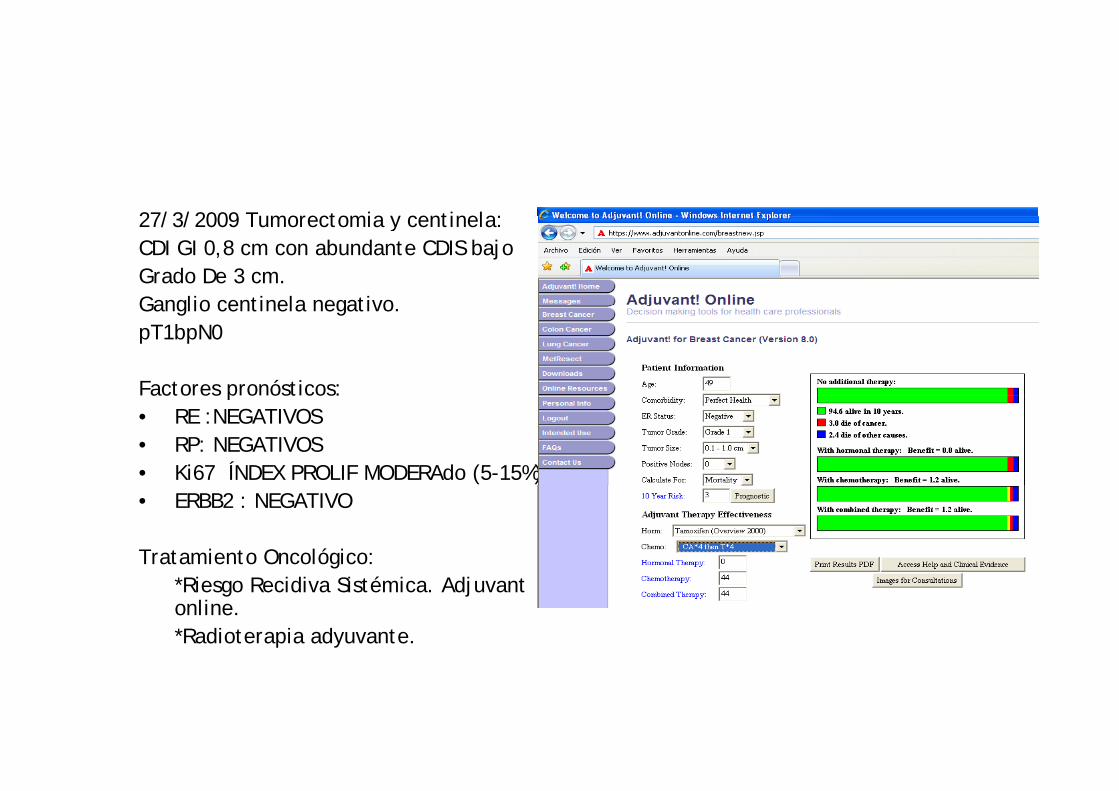
27/3/2009 Tumorectomia y centinela:27/3/2009 Tumorectomia y centinela:CDI GI 0,8 cm con abundante CDIS bajo Grado De 3 cm. Ganglio centinela negativoGanglio centinela negativo.pT1bpN0
Factores pronósticos:acto es p o óst cos:• RE :NEGATIVOS• RP: NEGATIVOS• Ki67 ÍNDEX PROLIF MODERAdo (5-15%)• ERBB2 : NEGATIVO
Tratamiento Oncológico: *Riesgo Recidiva Sistémica. Adjuvant online.*Radioterapia adyuvante.
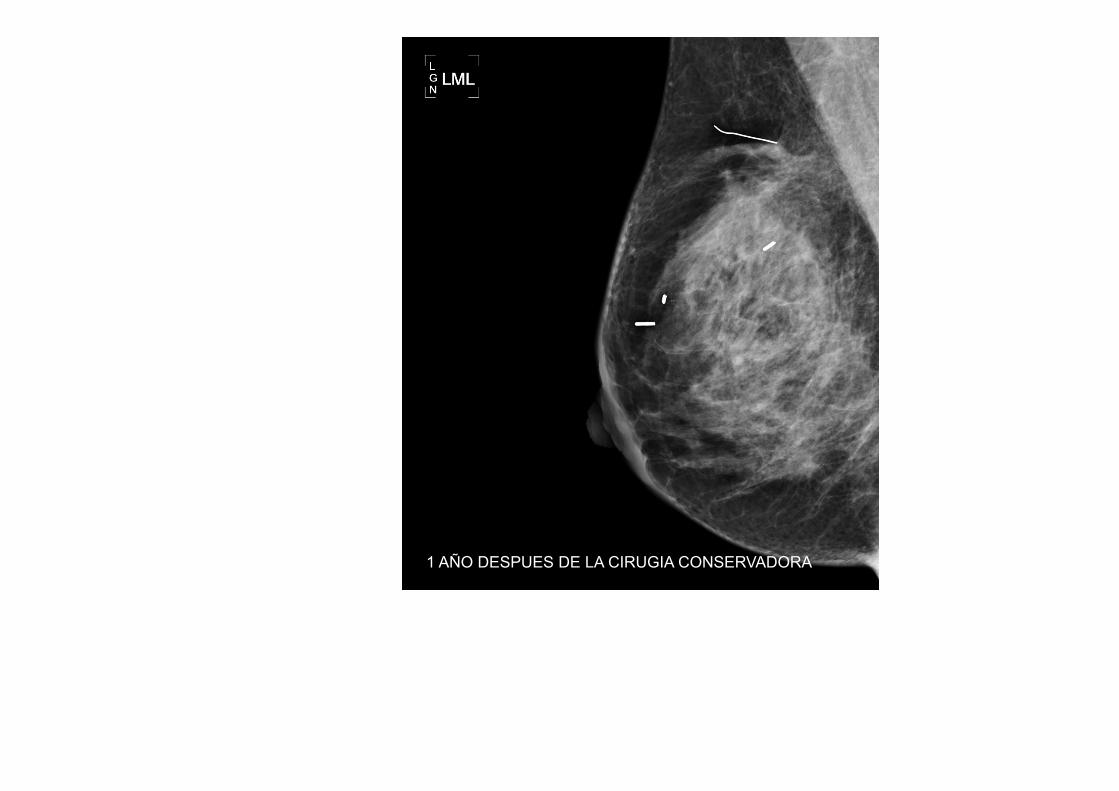
1 AÑO DESPUES DE LA CIRUGIA CONSERVADORA
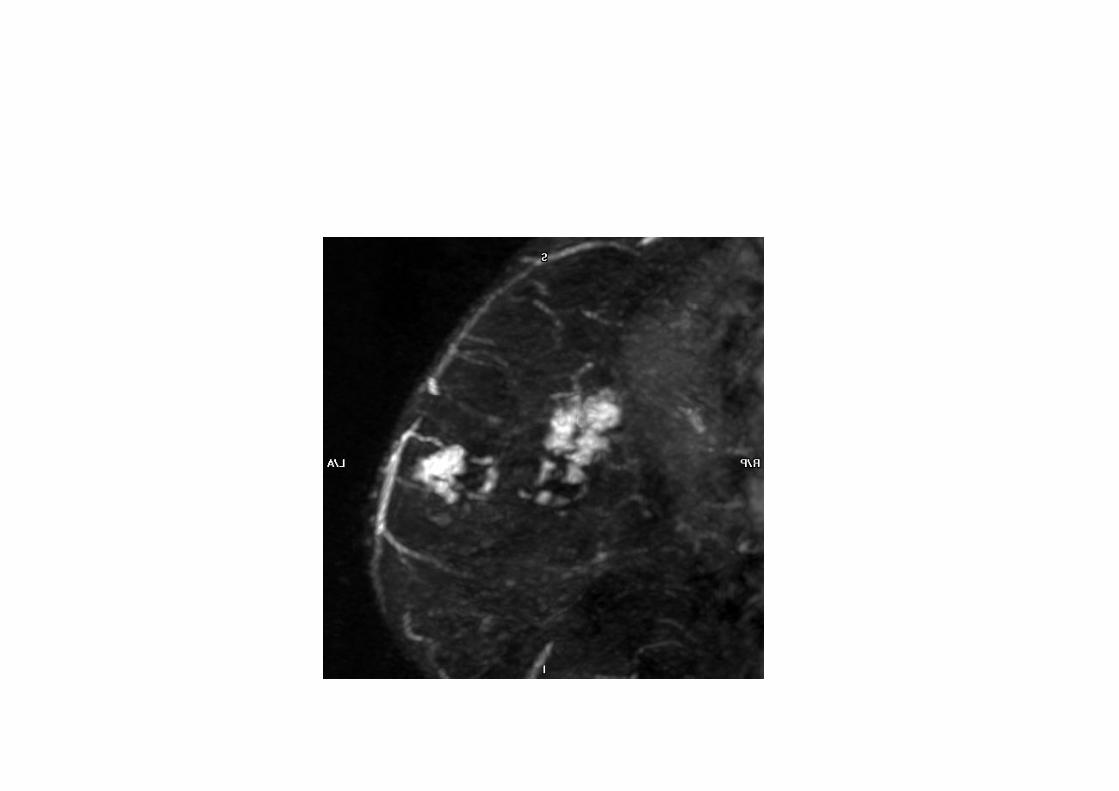
MAYO 2010
• Biopsia CSE MI: AP: CDIS ALTO GRADO COMEDOCARCINOMA CON FENOMENOS DE DUDOSA INFILTRACION B5a
• Decisión terapéutica : Mastectomía.

200 fam SL: 23 CM en pacientes MMR+ y 18 CM en mujeres MMR WT:65% CM IHQ –35% MSI-H.
Aproximadamente el 50% de los CM presentan deficiencia de MMR típico de los tumores del espectro de LS.
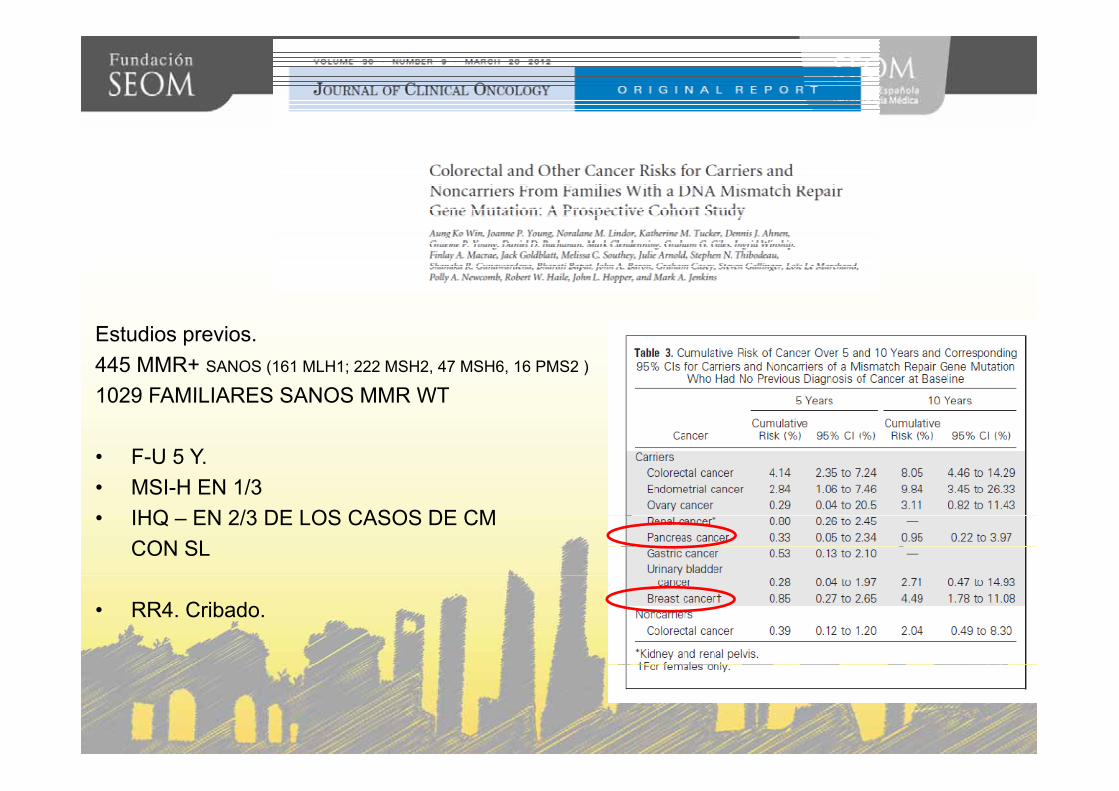
Estudios previos. 445 MMR+ SANOS (161 MLH1; 222 MSH2, 47 MSH6, 16 PMS2 )
1029 FAMILIARES SANOS MMR WT1029 FAMILIARES SANOS MMR WT
• F-U 5 Y.• MSI H EN 1/3• MSI-H EN 1/3 • IHQ – EN 2/3 DE LOS CASOS DE CM
CON SL
• RR4. Cribado.
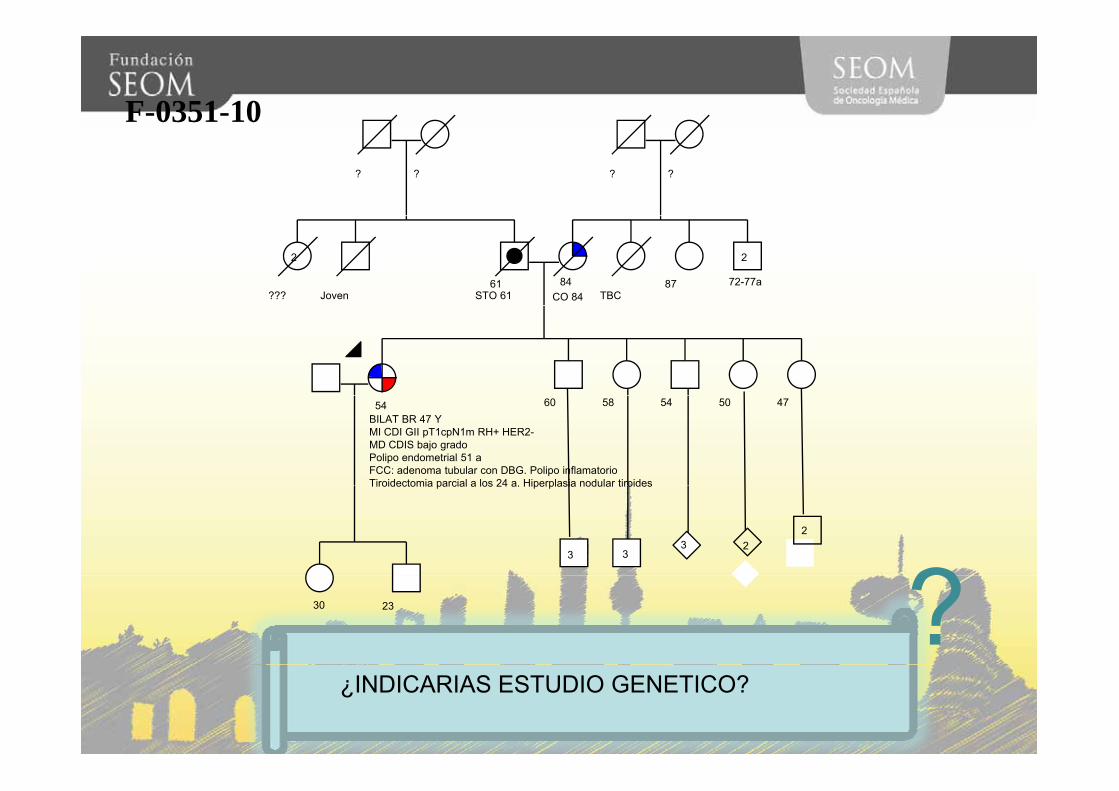
F-0351-10
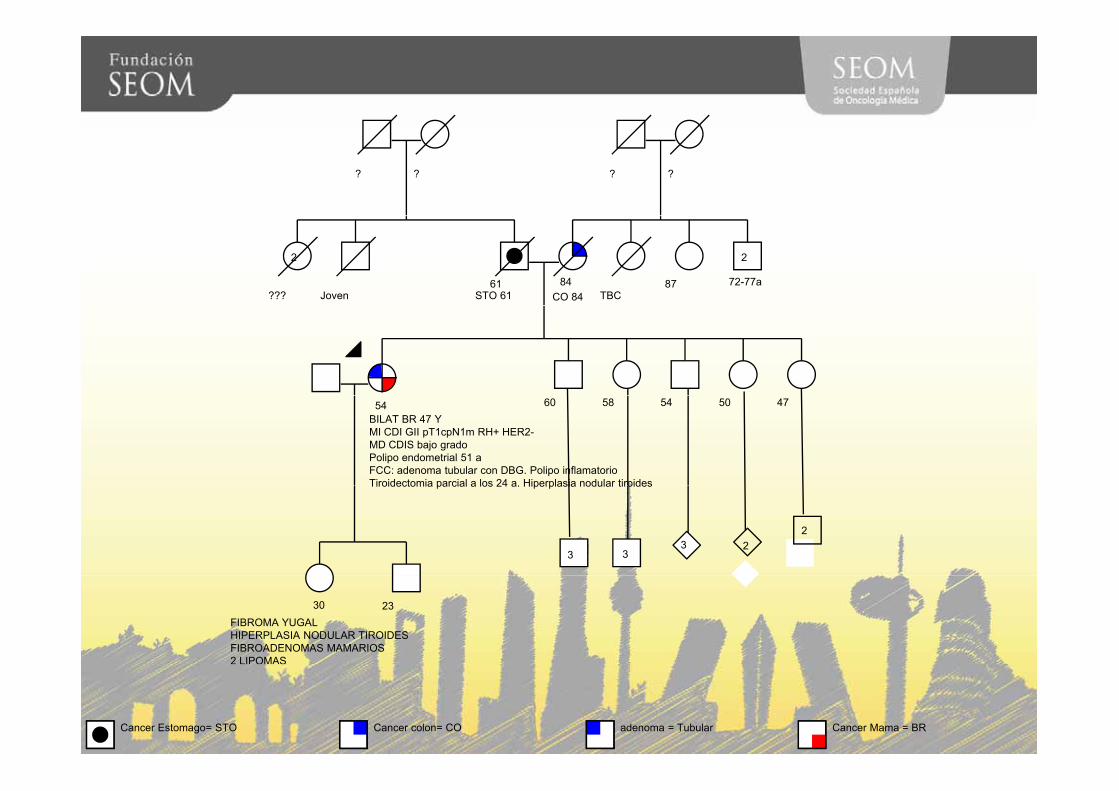
? ? ? ?
61STO 61
84CO 84???
2
Joven TBC 87 72-77a
2
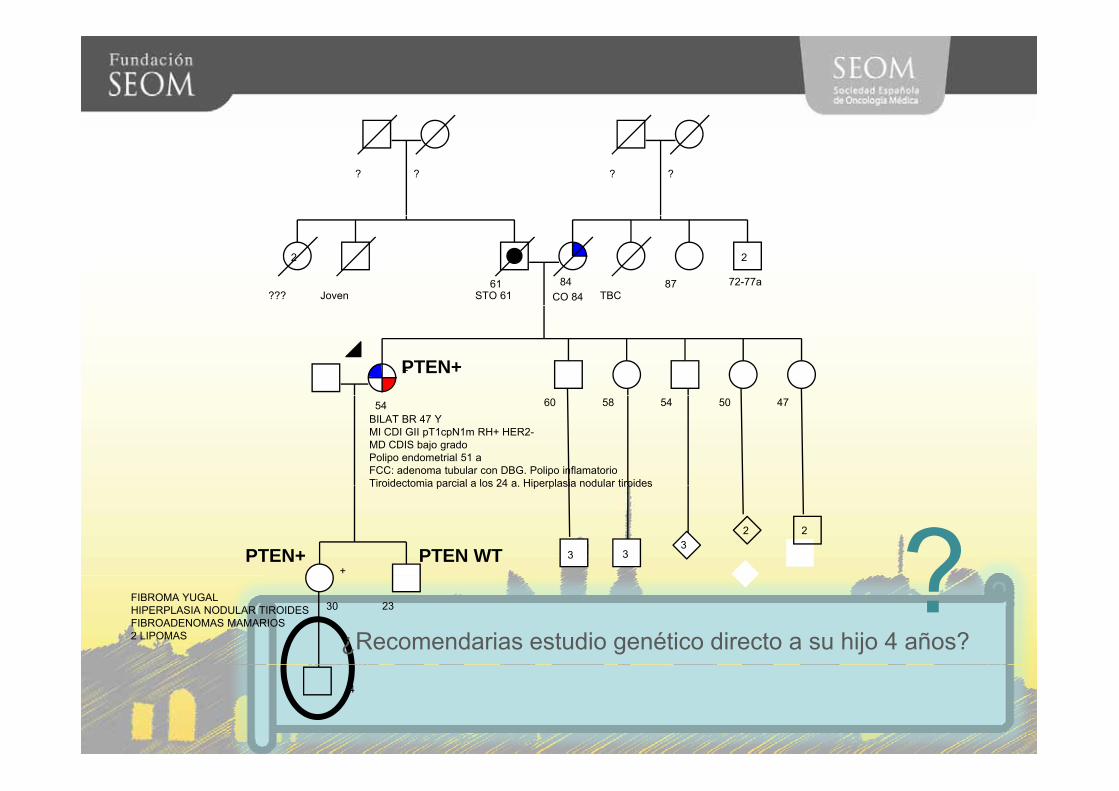
5854BILAT BR 47 YMI CDI GII pT1cpN1m RH+ HER2-MD CDIS bajo gradoPolipo endometrial 51 aFCC: adenoma tubular con DBG. Polipo inflamatorioTiroidectomia parcial a los 24 a Hiperplasia nodular tiroides
60 54 50 47
3
Tiroidectomia parcial a los 24 a. Hiperplasia nodular tiroides
33
22
?30 23 ?¿INDICARIAS ESTUDIO GENETICO?
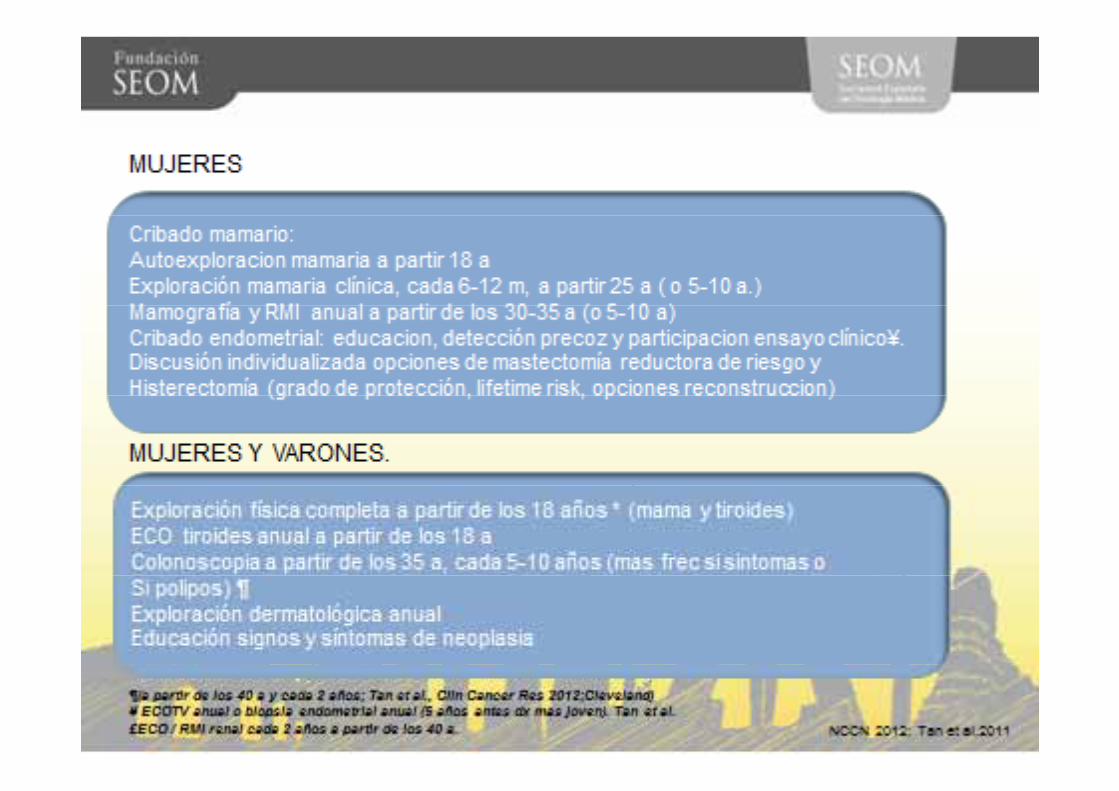
EXPLORACION FISICA.
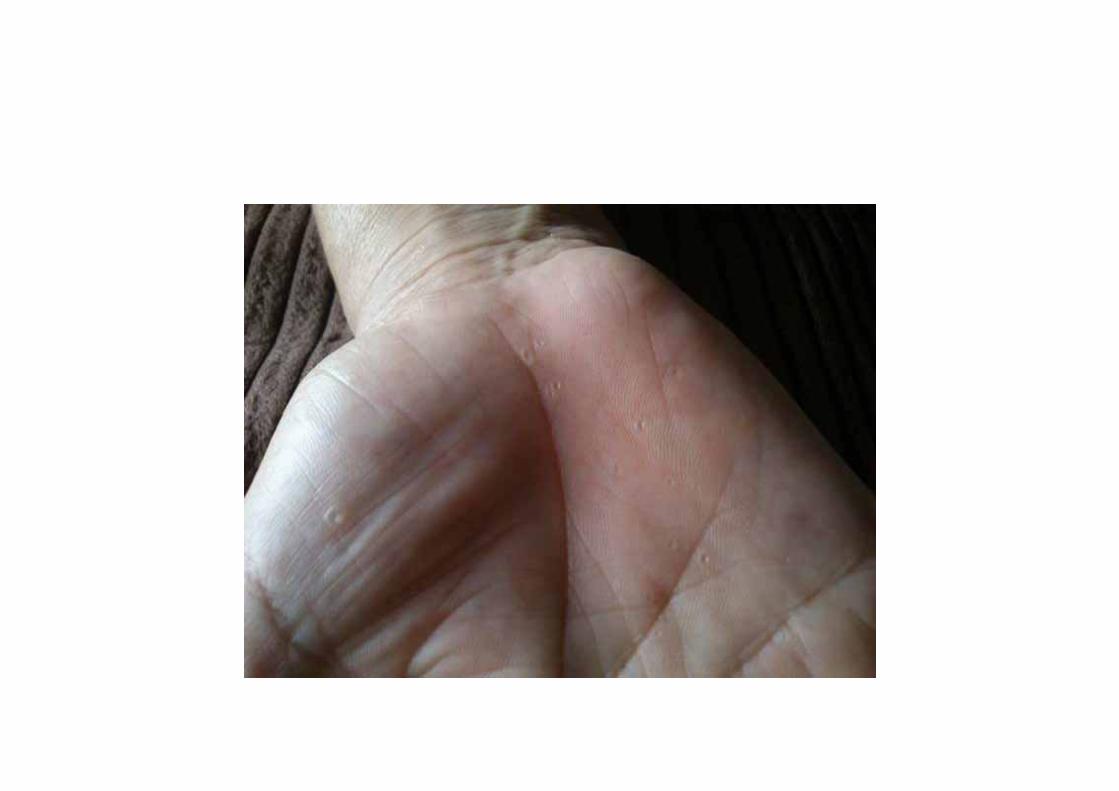
• NO MACROCEFALIA• NO LESIONES CUTANEAS FACIALES• NO LESIONES MUCOSAS• NO PAPILOMATOSIS.NO PAPILOMATOSIS.
? ? ? ?
61STO 61
84CO 84???
2
Joven TBC 87 72-77a
2
5854BILAT BR 47 YMI CDI GII pT1cpN1m RH+ HER2-MD CDIS bajo gradoPolipo endometrial 51 aFCC: adenoma tubular con DBG. Polipo inflamatorioTiroidectomia parcial a los 24 a Hiperplasia nodular tiroides
60 54 50 47
3
Tiroidectomia parcial a los 24 a. Hiperplasia nodular tiroides
33
22
30 23FIBROMA YUGALHIPERPLASIA NODULAR TIROIDESFIBROADENOMAS MAMARIOS2 LIPOMAS
Cancer Estomago= STO Cancer colon= CO adenoma = Tubular Cancer Mama = BR
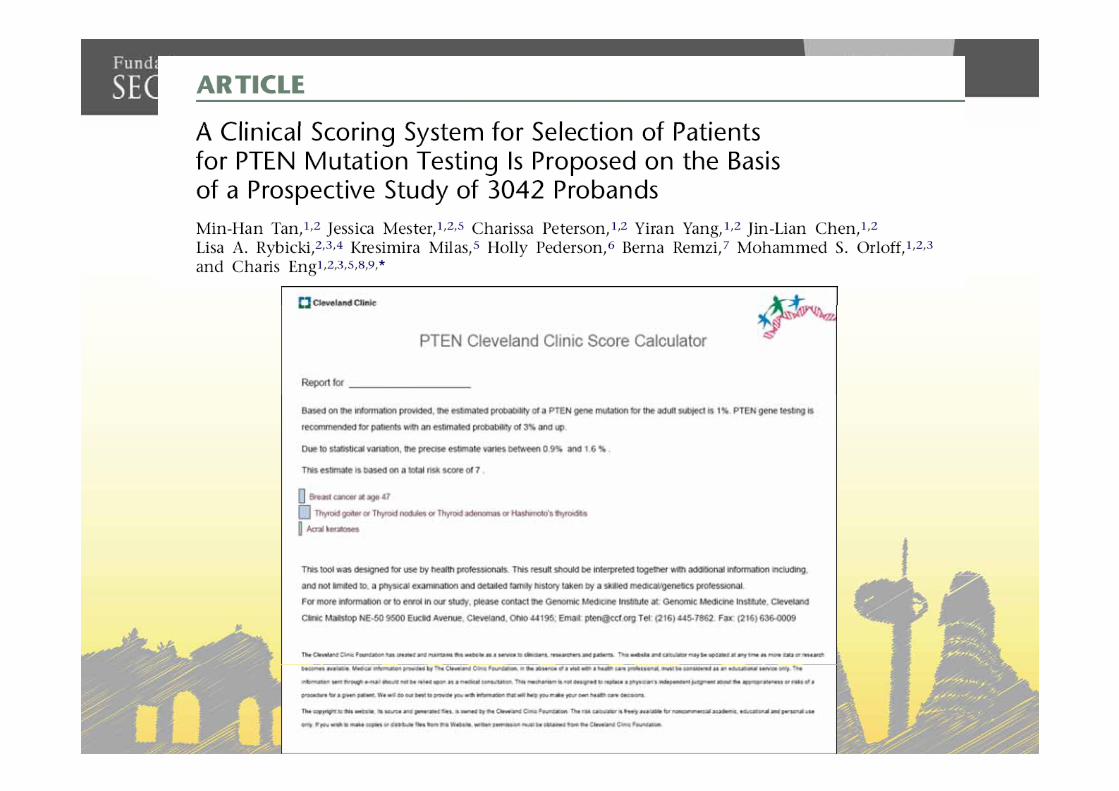
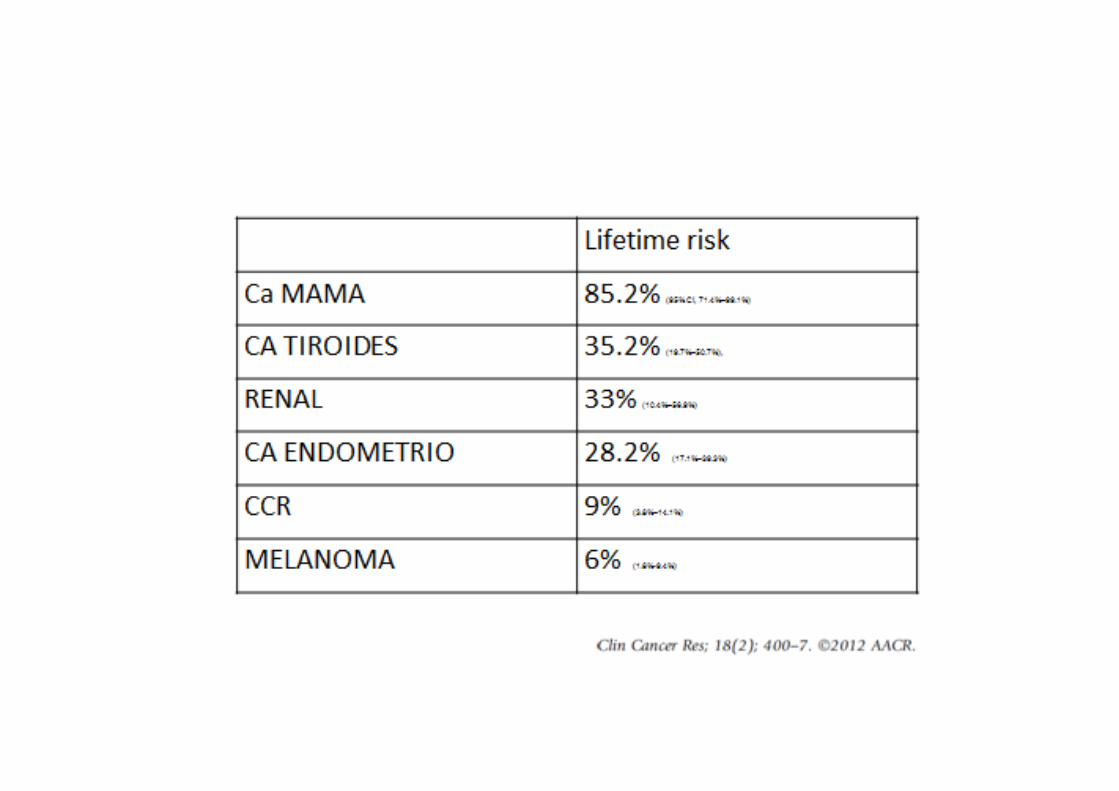
SD COWDENSD COWDEN
• Pertenece al Sd PTEN Hamartoma Tumor, q incluye: Sd Cowden en adultos y , q y yel Sd de Bannayan Riley Ruvalcaba en niñosniños
• Herencia AD. Alta penetrancia• Incidencia 1/200.000
? ? ? ?
61STO 61
84CO 84???
2
Joven TBC 87 72-77a
2
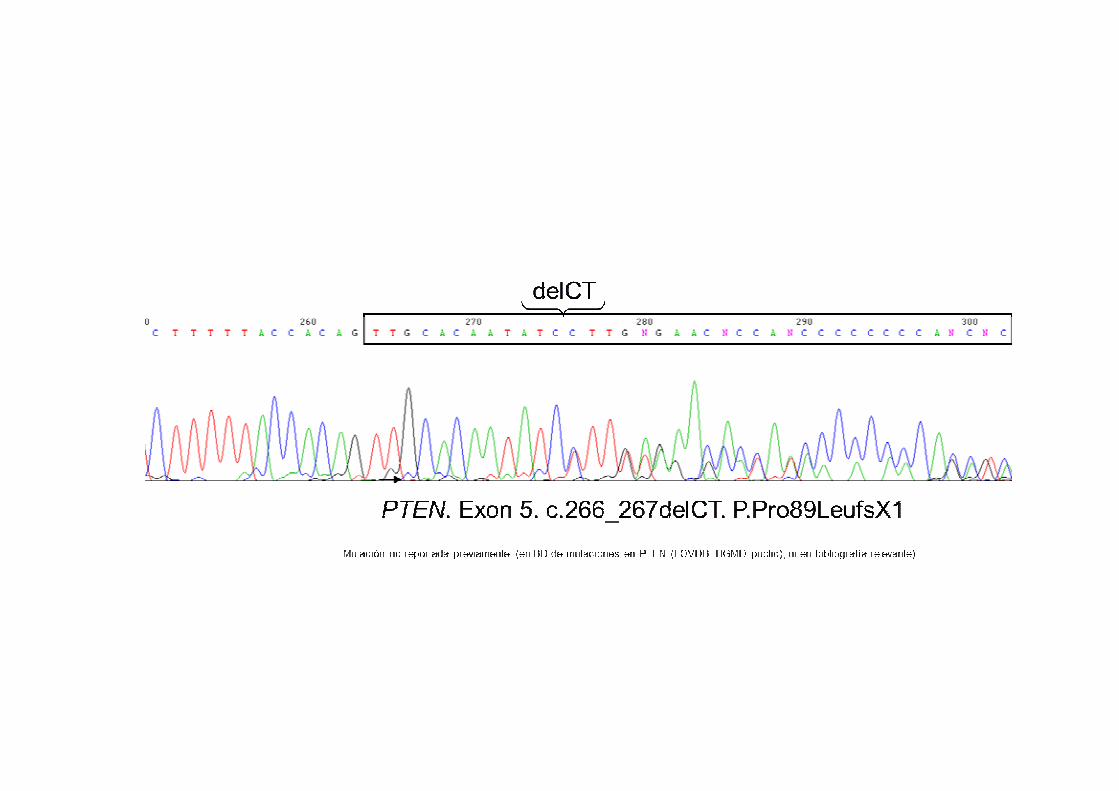
+PTEN+
5854 60 54 50 47BILAT BR 47 YMI CDI GII pT1cpN1m RH+ HER2-MD CDIS bajo gradoPolipo endometrial 51 aFCC: adenoma tubular con DBG. Polipo inflamatorioTiroidectomia parcial a los 24 a Hiperplasia nodular tiroides
3+
33
22
PTEN+ PTEN WT
Tiroidectomia parcial a los 24 a. Hiperplasia nodular tiroides
?30 23
¿Recomendarias estudio genético directo a su hijo 4 años?
FIBROMA YUGALHIPERPLASIA NODULAR TIROIDES FIBROADENOMAS MAMARIOS2 LIPOMAS
??4