rheumatologic emergencies. rheum emergencies life or organ threatening if not recognized within...
TRANSCRIPT

Rheumatologic Emergencies

RHEUM EMERGENCIES
• Life or organ threatening if not recognized within several hours or days
• Conditions that won’t first present to a Rheumatologist…..

Case
• 24 yo female with hx of initial left knee swelling, then right knee swelled
• Also tenosynovitis of wrist
• Asp knee 53,000 WBC
• Gram stain negative

PYOGENIC ARTHRITIS
Bacterial joint space infections are far more destructive than viral or fungal…..

INFECTIOUS (PYOGENIC) ARTHRITIS
• Assume any monoarticular arthritis is infectious until proven otherwise
• Sudden onset and very painful is more suggestive of crystalline dz – bacterial infection peaks over a few days
• If a nearby break in skin, or bacteremia, most definitely approach as infectious process
• Septic joint carries high morbidity and mortality
• Inflammatory arthritis can mimic septic joint!

INFECTIOUS (PYOGENIC) ARTHRITIS
• Risk Factors:– Bacteremia– Adjacent osteomyelitis– Soft tissue infection– Recent injection/aspiration– Penetrating trauma – foreign body
• Differential:– Crystalline– Mono presentation of a polyarticular disease


INFECTIOUS (PYOGENIC) ARTHRITIS
• Approach
– ASPIRATE – culture, gram stain, cell count– > 30,000 would be concerning for infection– Don’t let the presence of crystals fool you– Don’t let scans replace aspiration – Films most likely will be normal – early on– Blood cultures

INFECTIOUS (PYOGENIC) ARTHRITIS
INFECTIOUS (PYOGENIC) ARTHRITIS
• Treat while cultures are pending
– #1 bug - S. aureus– Other bugs include:
• H. flu in kids < than 3 yo• Beta strep in neonates• Various other strep in adults• S. epidermidis and GNR in prosthetic joints• Pseudomonas in IVDA• Salmonella in sickle cell disease

Septic Arthritis
• Staph aureus: Healthy adults, skin breakdown, damaged or replaced joints
• Strep Species: Healthy adults, asplenic
• Neisseria gonorrhea: Sexually active young adults, tenosynovitis
• Gram Negative: Immunocompromised hosts, GI infections
INFECTIOUS (PYOGENIC) ARTHRITIS
• Treatment Recommendations:
– MRSA is a problem => vancomycin– Gram pos => nafcillin – GNR => 3rd gen ceph, add an AG if pseudomonas– Nothing on gram stain => ceftriaxone or cefotaxime– Prosthetic joint => vanco + ciprofoxacin
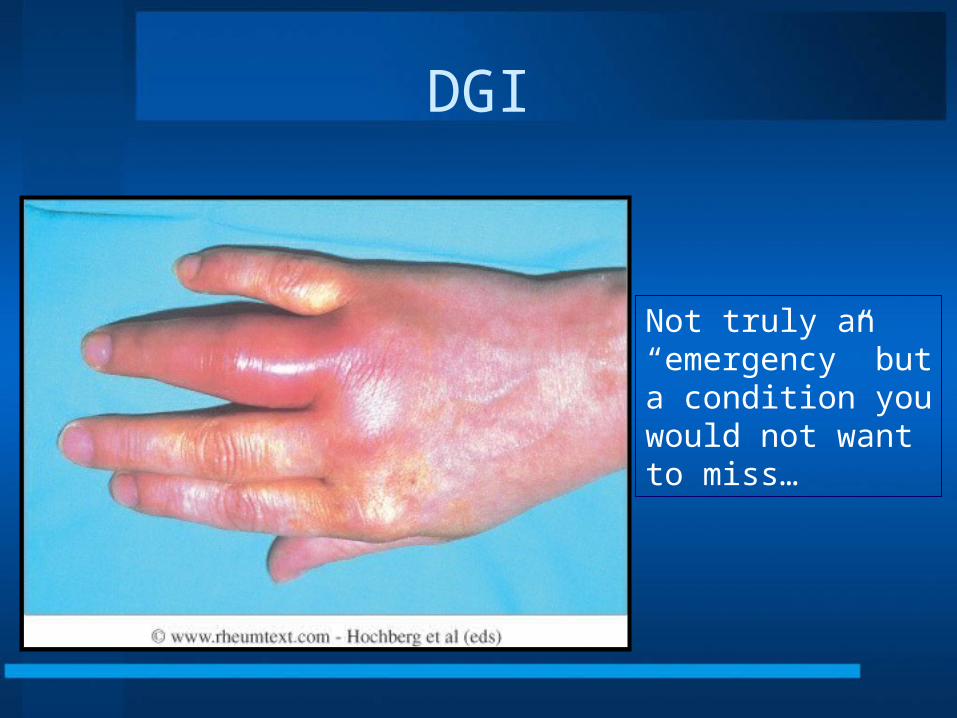
DGI
Not truly an“emergency” buta condition youwould not want to miss…

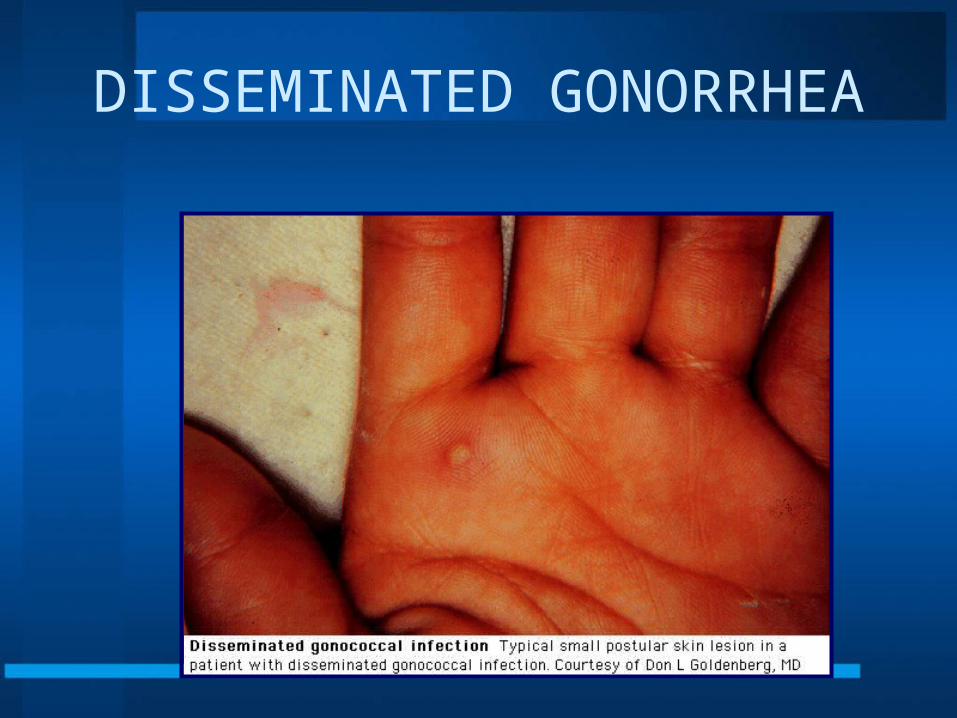
DISSEMINATED GONORRHEA
• Most common cause of septic arthritis and tenosynovitis in young adults in N.A.
• Complicates less than 1% of all GC cases
• Often have an asymptomatic mucosal infection
• Major risk factor is absence of C5-8 complement (….remember this for boards)

DGI
DISSEMINATED GONORRHEA
• Clues:– Migratory or additive acute oligo (<4) arthritis– Tenosynovitis of wrists / ankles / foot– Fever / chills– Females more commonly affected than
males and often within 1 week of menses – 2/3 have rash but it may be scant

DGI
May have only ONE vesicle orpustule – so look carefully…
DISSEMINATED GONORRHEA

DISSEMINATED GONORRHEA

DISSEMINATED GONORRHEA
• Approach:– Less than 25% of synovial cultures are positive– Less than 10% of blood cultures are positive– Skin biopsy culture is hardly ever positive but may be
able to see on gram stain– Best yield is to cultures/DNA probe the mucosal site– Remember the concomitant infection (HIV, syphilis,
NSU)– Rx with 3rd generation cephalosporin– Often add doxycycline to cover for Chlamydia

Gram Stain of GC

Case
• 53 yo female with hx of SLE c/o acute onset of dyspnea and cough
• Had previously been stable
• Hgb 7.4, PLT 111,
• UA 4+ protein, RBC casts
• ds-DNA >370 (markedly positive)
• ESR 85
PULMONARY-RENAL SYNDROMES
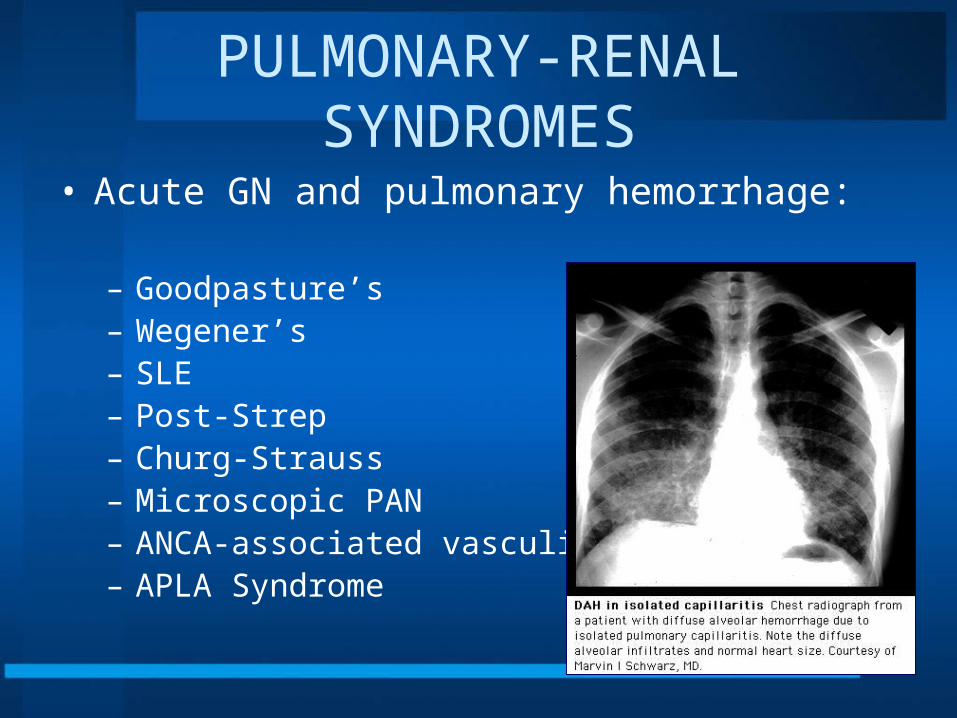
• Acute GN and pulmonary hemorrhage:
– Goodpasture’s– Wegener’s– SLE– Post-Strep– Churg-Strauss– Microscopic PAN– ANCA-associated vasculitis– APLA Syndrome

DIFFUSE ALVEOLAR HEMORRHAGE SYNDROME• Capillaritis- Wegener’s, Microscopic PAN,
HSP, Cryoglobulinemia, Behcet’s, SLE, RA, MCTD, Scleroderma, Polymyositis
• Bland Hemorrhage-Goodpasture’s, SLE, Pulmonary hemosiderosis, Mitral stenosis
• Diffuse Alveolar Damage- SLE, Cytotoxic drugs, Cocaine, Infections

DIFFUSE ALVEOLAR HEMORRHAGE SYNDROME
• Approach:– Bronch – lavage – ANA– ASO/DNase– ANCA (C-WG / P-MPAN)– Anti-GBM
• Treatment:– High dose steroids / cyclophosphamide– Plasmapheresis for Goodpasture’s, possibly SLE
- UA- HRCT
Reminder: ANA and RF are not “screens” for autoimmune diseaseANA simply “rules out” SLE if (-)

Case
• 35 yo with SLE
• New leg paresthesias and increasing bilateral weakness
• Unable to urinate
• New fever

TRANSVERSE MYELITIS
• Clues:– Leg paresthesias and bilateral weakness– Dermatomal sensory loss– Urinary retention and fecal incontinence– Fever/ axial pain– Abnormal CSF
• Approach:– MRI – diffuse edema– Pulse steroids 1000 mg Solumedrol IV for 3 days
/plasmapheresis /cyclophosphamide
- arteritis of spinal cord- APLA, SLE- hematomas/tumor/fx


CAUDA EQUINA SYNDROME• Ankylosing spondylitis• Spinal / epidural anesthesia• Central herniation / epidural abscess• Dysfunction in multiple
lumbosacral nerve roots• Clues:
– back pain / rectal pain / posterior leg pain– loss of bowel / bladder control or saddle anes– foot drop
• Image and decompress – you have 48 hours!

Cauda Equina Syndrome

Case
• 18 yo male with fever
• Large joint swelling on/off over last week
• Recent sore throat
• New murmur

What is this rash?

Erythema Marginatumof - ACUTE RHEUMATIC FEVER

ACUTE RHEUMATIC FEVER
• Post group A strep, Strep pyogenes• Clinical dz is self-limited; valvular dz is not• Clues:
– Migratory, large joint arthritis– Carditis / valvulitis– Erythema marginatum / sub-Q nodules– Fever – Preceding strep infection– CNS involvement (Sydenham’s chorea)

ACUTE RHEUMATIC FEVER

Mneumonic for Jones’ major criteria
• J – Joint swelling• ♥ - Carditis – 2002 update – get an echo• N - Nodules• E – Erythema Marginatum rash• S – Syndenham’s Chorea
– Minor Criteria - “PREAF”• PR• Elevated ESR/CRP• ASA – DNase going up• Fever

ARF- Cross Reactivity Between Strep/Human Tissue
• Cell Walls• Plasma
Membranes• Polysaccharides• Cell membranes• M Protein
• Myocardium• Myocardial
membrane• Heart Valves• Caudate/thalmic
neurons• Cardiac Myosin
ACUTE RHEUMATIC FEVER • Approach:
– EKG (look for prolonged PR)– Echo-heart valves/carditis – CXR– CBC / ESR / ASO / DNase / throat culture
• Not rapid strep
– Rx with high dose ASA and give PCN prophylaxis monthly for 5 years
– Steroids for heart valve involvement

How Long do you treat?
• 10 YEARS Or until 40 – if carditis progressing
• 10 YEARS or until 21 – if carditis improves
• 5 YEARS or until 21 – no carditis ever

Case
• 72 yo male
• Mild fever and headache
• Arthralgia in shoulders and knees
• Cannot get out of chair easily over last week
• Difficult to eat
• ESR 87

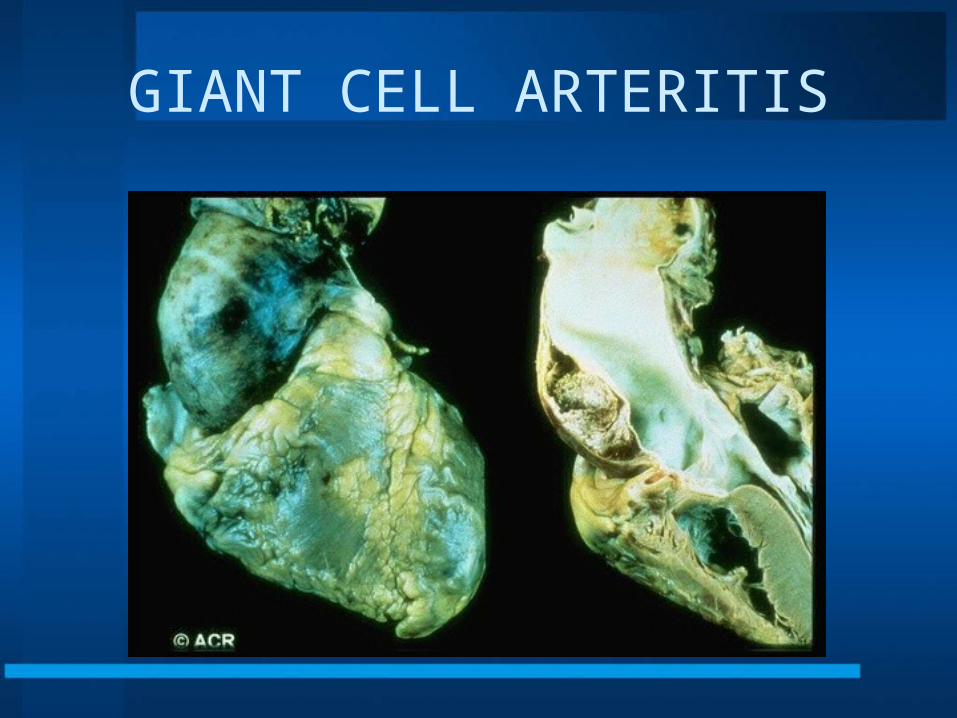
GIANT CELL ARTERITIS

GIANT CELL ARTERITIS• Clues:
– > 50 yo– NEW headache (not chronic)– Jaw claudication or arm claudication– Sudden visual loss, diplopia– Systemically ill with many markers of systemic
inflammation, increased A. Phos, Ferr, ESR
• Approach:– TREAT and then biopsy !! – You have 2 weeks to get the biopsy

Treatment
• GCA-High dose prednisone 1 mg/kd or standardly 60-100 mg daily. Continue for several weeks and taper as ESR decreases
• Treatment for over 2 years, mostly chronically at low doses < 5 mg pred qd
• PMR-start with 20 mg prednisone, taper with watching ESR to < 5 mg pred qd

GIANT CELL ARTERITIS
GIANT CELL ARTERITIS

GIANT CELL ARTERITIS

GCA
Fundus photograph showing optic atrophy secondary to giant cell arteritis

GCA-PMR SPECTRUM

Navy Trivia
• GEEDUNK – – Ice cream, candy, potato chips and other
assorted junk food– Or even the place where they can be
purchased

Possibilities of origin
• In the 1920's a comic strip character named Harold Teen and his friends spent a great amount of time at Pop's candy store. The store's owner called it The Geedunk for reasons never explained.
• The Chinese word meaning a place of idleness sounds something like gee dung.
• Geedunk is the sound made by a vending machine when it dispenses a soft drink in a cup.
• It may be derived from the German word tunk meaning to dip or sop either in gravy or coffee. Dunking was a common practice in days when bread, not always obtained fresh, needed a bit of tunking to soften it.
• The ge is a German unaccented prefix denoting repetition. • In time it may have changed from getunk to geedunk.

Case
• 64 yo female with 30 year hx of poorly controlled RA
• Paresthesias in extremites with neck movement
• Scheduled for cholecystectomy next week
• From too much Geedunk

CERVICAL SUBLUXATION WITH RA

CERVICAL SUBLUXATION WITH RA

CERVICAL SUBLUXATION WITH RA
• Clues:– Long-standing RA with or without neck pain
• Presentation:– Hyperreflexia / VBI symptoms– Sphincter dysfunction– Sensory findings in extremities– C1-C2 subluxation greater than 9 mm; presence of atlantoaxial
impaction, worse prognosis-neurosurgical evaluation.
• Approach:– Caution in C-spine manipulation– Image (plain films and MRI)

Case – Not Hunky-Dori

SCLEROMALACIA PERFORANS

RA EYE INVOLVEMENT

RHEUMATOID ARTHRITIS EYE DISEASE
• Episcleritis
• Anterior scleritis with corneal melt
• Scleromalacia
• Scleromalacia perforans

EPISCLERITIS

SCLERITIS / CORNEAL MELT

SCLEROMALACIA

Case
• 43 yo female with SLE
• New mental status changes
• Fever, nausea
• Joint Pain
• Bruising
• New thrombocytopenia 43 K, Hgb 8.3
• Creatinine 3.4

AUTOIMMUNE COAG DISORDERS
• TTP-Neurologic changes, fever, renal failure, thrombocytopenia, microangiopathic hemolytic anemia
• Plasmapheresis, Pulse steroids
• DIC, AIHA• APS Syndrome –

CATASTROPHIC ANTIPHOLPHOLIPID SYNDROME
-Gangrene of limb-Recurrent fetal loss-Livedo reticularis-Migraine-Renal insufficiency-PHTN-PE / DVT-Neuro deficits-AVN-Endocarditis-:ow plts – (Sneddon’s syndrome is low plts, stroke, and livedo)
Mortality 50%-TX with - anticoagulation/plasmaphesis

What is this called?

AUTOIMMUNE COAG DISORDER

Don’t Confuse with:Cutis Marmorata Telangiectatica Congenita
“We believe that cutis marmorata telangiectaticacongenita is a relatively mild condition. The prognosisis usually good, with minor associated anomalies.Improvement of the mottled, vascular pattern is usuallyobserved within 2 years. We recommend careful clinicalexamination of all patients to exclude any associatedanomalies. Patients should be referred to a neurologistor an ophthalmologist only if symptoms are present orif vascular lesions are present around the eyes.”
Arch Dermatol. 1999;135:34-38
Case
• 43 yo female with scleroderma
• Recently was given prednisone for joint pain by PCM
• BP 182/108
• Creatinine 4.3
• Hgb 8.3 helmet cells on smear

SCLERODERMA RENAL CRISIS

SCLERODERMA RENAL CRISIS
• Silent renal failure• Cardiac decompensation• HTN (relative)• Microangiopathic hemolytic anemia
Rx with ACE InhibitorCaptopril in increasing doses
Do not stop the ACE

SCLERODERMA RENAL CRISIS

SCLERODERMA RENAL CRISIS

SCLERODERMA RENAL CRISIS

Case
• 24 yo male
• New onset of testicular pain
• Purpuric rash
• New foot drop
• BP 158/108
SYSTEMIC VASCULITIS
• Mononeuritis multiplex• Glomerulonephritis• Skin infarction / ulceration• Neurologic dysfunction• Multi-organ infarctions
Always think of systemic vasculitis in the setting of multi-organ disease!
Major Vasculitidies
• Polyarteritis Nodosa• Microscopic Polyangiitis• Churg-Strauss Syndrome• Wegener’s Granulomatosis• Cryoglobulinemia
• Start high dose 60-100 mg day• Or pulse steroids 1 gram Solumedrol for 3 days• Add cyclophosphamide to Wegener’s treatment

Case
• 72 yo with ASCVD
• 3 days S/P catheterization
• Complained of blue toes
• Creatinine 2.7
• microhematuria
• Mild eosinophilia

Blue Toes

CHOLESTEROL EMBOLIC SYNDROME
- Blue toes after an intervention- TIA- ARF- Microhematuria- Fever- Oschemic bowel- Eosinophilia- ESR increased- Heparinization may worsen by releasing clefts from plaques

The Dreaded Friday afternoon Consult
• 35 year old female• Tearful in office• Total body pain, worst pain of her life• Abdominal pain, urinary urgency issues• Severe Fatigue• Cannot perform ADL’s• Has been to several physicians for these
complaints

Fibromyalgia Fulminans
• Treatment
• Empathy from the doctor
• Detailed explanation of the condition
• Prescription for slowly increased exercise – Log book– F/u with PCM (that may be you)

RHEUMATOLOGIC EMERGENCIES
????? ???