review article the value of peer learning in undergraduate...
TRANSCRIPT
Hindawi Publishing CorporationISRN NursingVolume 2013, Article ID 930901, 10 pageshttp://dx.doi.org/10.1155/2013/930901
Review ArticleThe Value of Peer Learning in Undergraduate NursingEducation: A Systematic Review
Robyn Stone, Simon Cooper, and Robyn Cant
Monash University, School of Nursing and Midwifery, Berwick Campus, 100 Clyde Road, Berwick 3806, Australia
Correspondence should be addressed to Robyn Stone; [email protected]
Received 23 December 2012; Accepted 9 February 2013
Academic Editors: L. H. Beebe and M. M. Funnell
Copyright © 2013 Robyn Stone et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The study examined various methods of peer learning and their effectiveness in undergraduate nursing education. Using a specifi-cally developed search strategy, healthcare databases were systematically searched for peer-reviewed articles, with studies involvingpeer learning and students in undergraduate general nursing courses (in both clinical and theoretical settings) being included.Thestudies were published in English between 2001 and 2010. Both study selection and quality analysis were undertaken independentlyby two researchers using published guidelines and data was thematically analyzed to answer the research questions. Eighteen studiescomprising various research methods were included. The variety of terms used for peer learning and variations between studydesigns and assessment measures affected the reliability of the study. The outcome measures showing improvement in either anobjective effect or subjective assessmentwere considered a positive result with sixteen studies demonstrating positive aspects to peerlearning including increased confidence, competence, and a decrease in anxiety.We conclude that peer learning is a rapidly develop-ing aspect of nursing education which has been shown to develop students’ skills in communication, critical thinking, and self-con-fidence. Peer learning was shown to be as effective as the conventional classroom lecturemethod in teaching undergraduate nursingstudents.
1. Introduction
Nursing education studies have often focused on traditionalteaching methods such as classroom lecture learning, a be-haviourism-based teachingmethod based onpassive learning[1]. More effective student-centric learning methods are nowbeing utilized to encourage active student participation andcreative thinking [2–4]. One of these methods is peer learn-ing, in which peers learn from one another, involving activestudent participation and where the student takes responsi-bility for their learning. Despite being used for many years,one of the barriers to advancement of peer learning is alack of consistency in its definition [5]. It is known by dif-ferent interchangeable titles such as “cooperative learning,”“mentoring,” “peer review learning,” “peer coaching,” “peermentoring,” “problem-based learning,” and “team learning.”
Peer learning has been used in education to addresscritical thinking, psychomotor skills, cognitive development,clinical skills, and academic gains [6–9]. One type of peer
learning is problem-based learning (PBL) which is character-ized by students learning from each other and from indepen-dently sourced information [10]. It is student centered, utiliz-ing group work with the analysis of case studies as a meansof learning. Alternatively “peer tutoring” involves individualsfrom similar settings helping others to learn, which mayoccur one-on-one or as small group sessions [11]. In nursing,high student numbers increase pressures [12] whilst variedand innovative teachingmethods are beneficial [13] with peerlearning offering a strategy that may be advantageous.
The Oxford Dictionary (2009) defines a “peer” as some-one of the same age or someone who was attending the sameuniversity. The term “peer” can also refer to people who haveequivalent skills or a commonality of experiences [14]. Boththese definitions suit the concept of peer learning describedhere. The current study aimed to address the followingresearch questions: (i) do undergraduate nursing studentsbenefit from peer learning? and (ii) what approaches to peerlearning are the most effective?

2 ISRN Nursing
2. Methods
Operational terms as shown in Table 1 were developed afterconsulting several studies. Inclusion and exclusion criteriawere defined. A search was conducted for peer-reviewedpapers published in English between the years 2000 and 2010that discussed any aspect of the curriculum for undergradu-ate or general nursing courses (e.g., clinical skills, communi-cation, patient interaction, or theoretical knowledge).
The literature searchwas undertaken using the PICOalgo-rithm of Participant, Intervention, Comparison, and Out-come and guidelines fromThe Cochrane Handbook [15]. Forthis study the following terms were used:
participant—undergraduate nursing students,
intervention—peer learning,
comparison—classroom lecture learning,
outcome—improvement in theory results or results ofpractical assessment or personal feelings relating tocomfort, confidence, or competence.
A systematic literature search of multiple databases andsearch engines was undertaken using the keywords and thesearch strategy described in the following.Thekeywords usedwere student nurse, undergraduate nurse, peer learning, peertutoring, peer mentoring, education, and opinion leaders.Also used were variations and truncations of these words,for example, peer education, nurse education, and problem-based learning. Each of the key words was searched forindividually and then in combination with all others.
In addition, a number of key nursing journals such asJournal of Advanced Nursing and Journal of Nursing Edu-cation were hand-searched between the years 2000 and 2010.Snowballing, identifying suitable articles from the referencesof the selected studies, was then conducted to locate furtherstudies.
Studies with all levels of evidence that met the criteriawere included because studies in peer learning tendedtowards quasiexperimental, observational, or case studydesigns which are all lower on the hierarchy of evidence [16].
Two reviewers conducted a quality analysis of each studyusing quality criteria for qualitative and quantitative studiesof the Critical Skills Appraisal Programme (CASP) [17].They assessed methodology, validity, sample type, selectionmethod, level of evidence, and any attrition rate and its effect(including biases), to determine selection. Consensus wasreached through discussion. Data extraction and thematicanalysis were undertaken to synthesize the data. Meta-analysiswas not undertaken due to the inconsistent definitionof “peer” and potential for bias if different methods of peerlearning were combined. Although the primary review wasconducted by a single researcher, inclusion and exclusion cri-teria were adhered to, using a transparent reporting processto allow the search to be reproduced.
Data were extracted and summarized in separate tables:quantitative studies (Table 2), qualitative studies (Table 3),and mixed method studies (Table 4). Drawing from this,data outcomes were collated into themes and subthemes; for
Table 1: Operational definitions.
Term Definition
Peer
A person with a comparable or slightly higherlevel of knowledge and experience to the learner.A person of any age can be a peer, that is, a thirdyear student tutoring a first year student but thepeer must be an undergraduate nursing student.
Peer learning Gaining, refining, or improving knowledge frominteraction with a peer as defined previously.
Mentor A peer, who supports, guides, and educates alearner.
Undergraduatenursing student
A nursing student at any stage of study prior toregistration.
Sources: [10, 14, 45, 48–51].
FilterExclude papers not meeting the
criteria after reading the title and
Selection of articles49 papers assessed by both
reviewers
Exclusion of nonnursing, postgraduate
learning, or continuing education articles
Exclude peer/mentor not as defined, books, reports, and
editorials. Assess quality and methodology
Review
18 papers included in systematic review
Literature searchPeer learning in undergraduate nursing in multiple databases
abstract (𝑛 = 1768)
Figure 1: Flow chart of the systematic review selection process.
example, the resources theme had three subthemes: faculty,students, and peers.
3. Results
Initially, 1813 studies were screened using the aforementionedcriteria and 18 studies were selected for review. A flow chart(Figure 1) shows the selection process including number ofstudies excluded at each stage and the reason for exclusion.
3.1. Characteristics of Studies. Participants were undergradu-ate nursing students from first to final year. In line with nurs-ing demography the majority of participants were females.Participant numbers and study duration varied, for example,15 students over a three-year period [18] and 365 students overa two-year period [7]. A variety of peer learning terms andmethods were used. These terms included “peer mentor-ing” [19], “peer tutoring” [7, 20–23], “peer coaching” [24],“inquiry-based learning” [25, 26], “problem-based learning”[27–31], and “team learning” [32].
Of these studies, eight used a qualitative method, sixutilized a quantitative method, and four usedmixedmethods
ISRN Nursing 3
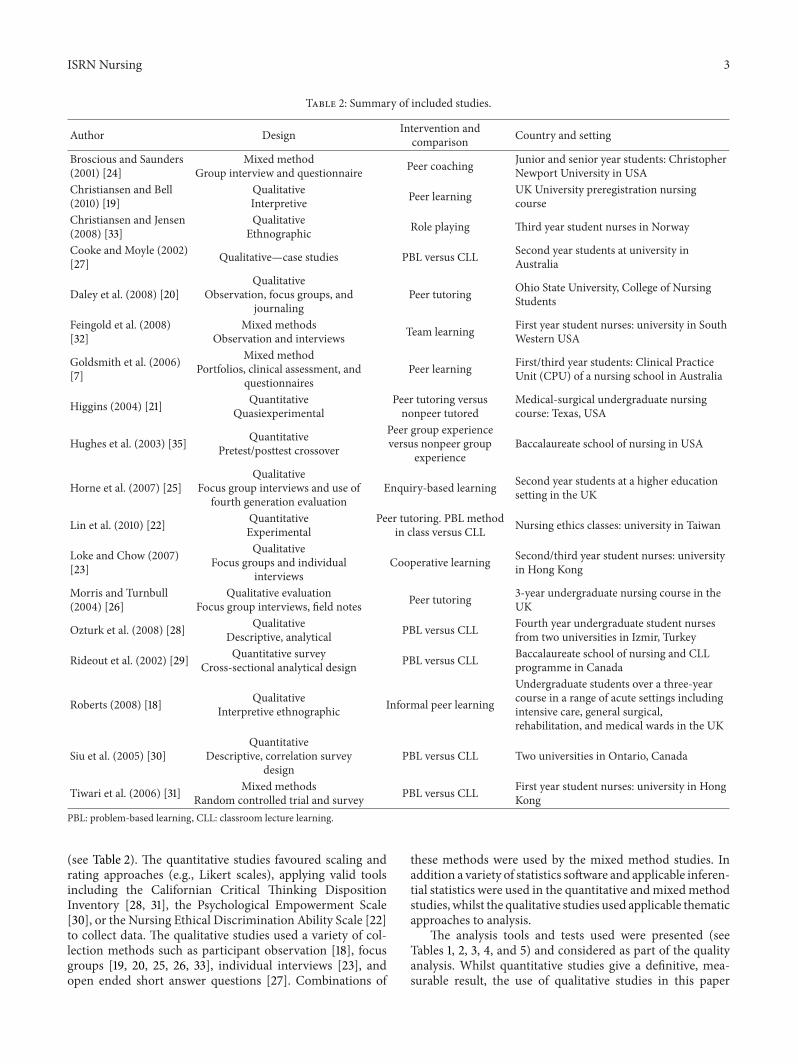
Table 2: Summary of included studies.
Author Design Intervention andcomparison Country and setting
Broscious and Saunders(2001) [24]
Mixed methodGroup interview and questionnaire Peer coaching Junior and senior year students: Christopher
Newport University in USAChristiansen and Bell(2010) [19]
QualitativeInterpretive Peer learning UK University preregistration nursing
courseChristiansen and Jensen(2008) [33]
QualitativeEthnographic Role playing Third year student nurses in Norway
Cooke and Moyle (2002)[27] Qualitative—case studies PBL versus CLL Second year students at university in
Australia
Daley et al. (2008) [20]Qualitative
Observation, focus groups, andjournaling
Peer tutoring Ohio State University, College of NursingStudents
Feingold et al. (2008)[32]
Mixed methodsObservation and interviews Team learning First year student nurses: university in South
Western USA
Goldsmith et al. (2006)[7]
Mixed methodPortfolios, clinical assessment, and
questionnairesPeer learning First/third year students: Clinical Practice
Unit (CPU) of a nursing school in Australia
Higgins (2004) [21] QuantitativeQuasiexperimental
Peer tutoring versusnonpeer tutored
Medical-surgical undergraduate nursingcourse: Texas, USA
Hughes et al. (2003) [35] QuantitativePretest/posttest crossover
Peer group experienceversus nonpeer group
experienceBaccalaureate school of nursing in USA
Horne et al. (2007) [25]Qualitative
Focus group interviews and use offourth generation evaluation
Enquiry-based learning Second year students at a higher educationsetting in the UK
Lin et al. (2010) [22] QuantitativeExperimental
Peer tutoring. PBL methodin class versus CLL Nursing ethics classes: university in Taiwan
Loke and Chow (2007)[23]
QualitativeFocus groups and individual
interviewsCooperative learning Second/third year student nurses: university
in Hong Kong
Morris and Turnbull(2004) [26]
Qualitative evaluationFocus group interviews, field notes Peer tutoring 3-year undergraduate nursing course in the
UK
Ozturk et al. (2008) [28] QualitativeDescriptive, analytical PBL versus CLL Fourth year undergraduate student nurses
from two universities in Izmir, Turkey
Rideout et al. (2002) [29] Quantitative surveyCross-sectional analytical design PBL versus CLL Baccalaureate school of nursing and CLL
programme in Canada
Roberts (2008) [18] QualitativeInterpretive ethnographic Informal peer learning
Undergraduate students over a three-yearcourse in a range of acute settings includingintensive care, general surgical,rehabilitation, and medical wards in the UK
Siu et al. (2005) [30]Quantitative
Descriptive, correlation surveydesign
PBL versus CLL Two universities in Ontario, Canada
Tiwari et al. (2006) [31] Mixed methodsRandom controlled trial and survey PBL versus CLL First year student nurses: university in Hong
KongPBL: problem-based learning, CLL: classroom lecture learning.
(see Table 2). The quantitative studies favoured scaling andrating approaches (e.g., Likert scales), applying valid toolsincluding the Californian Critical Thinking DispositionInventory [28, 31], the Psychological Empowerment Scale[30], or the Nursing Ethical Discrimination Ability Scale [22]to collect data. The qualitative studies used a variety of col-lection methods such as participant observation [18], focusgroups [19, 20, 25, 26, 33], individual interviews [23], andopen ended short answer questions [27]. Combinations of
these methods were used by the mixed method studies. Inaddition a variety of statistics software and applicable inferen-tial statistics were used in the quantitative andmixedmethodstudies, whilst the qualitative studies used applicable thematicapproaches to analysis.
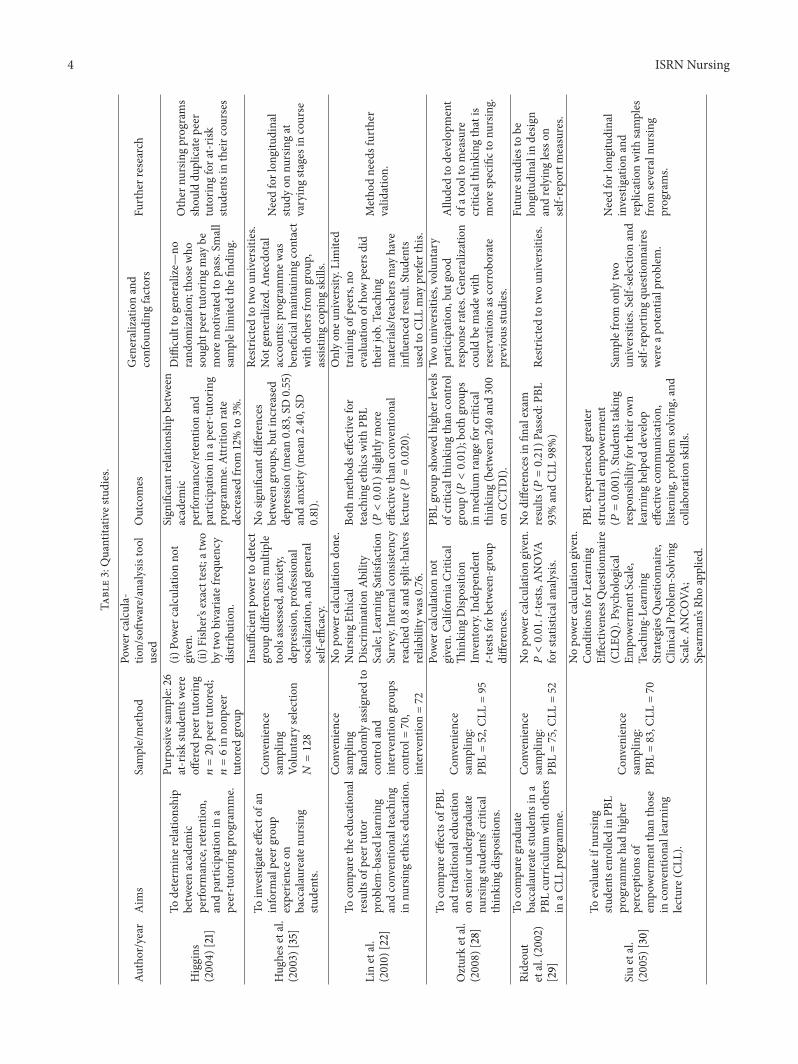
The analysis tools and tests used were presented (seeTables 1, 2, 3, 4, and 5) and considered as part of the qualityanalysis. Whilst quantitative studies give a definitive, mea-surable result, the use of qualitative studies in this paper
4 ISRN Nursing
Table3:Quantitativ
estudies.
Author/year
Aim
sSample/metho
dPo
wer
calcula-
tion/softw
are/analysistool
used
Outcomes
Generalizationand
confou
ndingfactors
Furtherresearch
Higgins
(200
4)[21]
Todeterm
iner
elationship
betweenacadem
icperfo
rmance,retentio
n,andparticipationin
apeer-tu
torin
gprogramme.
Purposives
ample:26
at-risk
studentsw
ere
offered
peer
tutorin
g𝑛=20peer
tutored;
𝑛=6in
nonp
eer
tutoredgrou
p
(i)Po
wer
calculationno
tgiven.
(ii)F
isher’sexacttest;atwo
bytwobivaria
tefre
quency
distr
ibution.
Sign
ificant
relationshipbetween
academ
icperfo
rmance/retentio
nand
participationin
apeer-tutorin
gprogramme.Attrition
rate
decreasedfro
m12%to
3%.
Diffi
cultto
generalize—
norand
omization;
thosew
hosoug
htpeer
tutorin
gmay
bemorem
otivated
topass.Small
samplelim
itedthefi
nding.
Other
nursingprograms
shou
lddu
plicatep
eer
tutorin
gfora
t-risk
studentsintheirc
ourses
Hug
hese
tal.
(2003)
[35]
Toinvestigatee
ffectof
aninform
alpeer
grou
pexperie
nceo
nbaccalaureaten
ursin
gstu
dents.
Con
venience
sampling
Voluntaryselection
𝑁=128
Insufficientp
ower
todetect
grou
pdifferences;m
ultip
letoolsa
ssessed,anxiety,
depressio
n,professio
nal
socialization,
andgeneral
self-effi
cacy.
Nosig
nificantd
ifferences
betweengrou
ps,but
increased
depressio
n(m
ean0.83,SD0.55)
andanxiety(m
ean2.40
,SD
0.81).
Restric
tedto
twoun
iversities.
Not
generalized.A
necdotal
accoun
ts:programmew
asbeneficialm
aintaining
contact
with
othersfro
mgrou
p,assis
tingcoping
skills.
Needforlon
gitudinal
study
onnu
rsingat
varyingsta
gesincourse
Linetal.
(2010)
[22]
Tocompare
thee
ducatio
nal
results
ofpeer
tutor
prob
lem-based
learning
andconventio
nalteaching
innu
rsingethics
education.
Con
venience
sampling
Rand
omlyassig
nedto
controland
interventio
ngrou
pscontrol=
70,
interventio
n=72
Nopo
wer
calculationdo
ne.
Nursin
gEthical
Disc
riminationAb
ility
Scale;Learning
Satisfaction
Survey.Internalcon
sistency
reached0.8andsplit-halves
reliabilitywas
0.76.
Both
metho
dseffectiv
efor
teaching
ethics
with
PBL
(𝑃<0.01)slightlymore
effectiv
ethanconventio
nal
lecture(𝑃=0.020).
Onlyon
euniversity.Lim
ited
training
ofpeers,no
evaluatio
nof
howpeersd
idtheirjob.Teaching
materials/teachersmay
have
influ
encedresult.
Stud
ents
used
toCL
Lmay
prefer
this.
Metho
dneedsfurther
valid
ation.
Ozturketal.
(2008)
[28]
Tocompare
effectsof
PBL
andtradition
aleducation
onsenior
undergradu
ate
nursingstu
dents’critical
thinking
disposition
s.
Con
venience
sampling:
PBL=52,C
LL=95
Power
calculationno
tgiven.
CaliforniaC
ritical
Thinking
Disp
osition
Inventory.Independ
ent
t-tests
forb
etween-grou
pdifferences.
PBLgrou
pshow
edhigh
erlevels
ofcriticalthink
ingthan
control
grou
p(𝑃<0.01);bo
thgrou
psin
medium
rangefor
critical
thinking
(between240and300
onCC
TDI).
Twoun
iversities,voluntary
participation,
butgoo
drespon
serates.Generalization
couldbe
madew
ithreservations
ascorrob
orate
previous
studies.
Allu
dedto
developm
ent
ofatoo
ltomeasure
criticalthink
ingthatis
mores
pecific
tonu
rsing.
Rideou
tetal.(2002)
[29]
Tocompare
graduate
baccalaureates
tudentsina
PBLcurriculum
with
others
inaC
LLprogramme.
Con
venience
sampling:
PBL=75,C
LL=52
Nopo
wercalculationgiven.
𝑃<0.01.t-te
sts,A
NOVA
forstatistic
alanalysis.
Nodifferences
infin
alexam
results
(𝑃=0.21)P
assed:PB
L93%andCL
L98%)
Restric
tedto
twoun
iversities.
Future
studies
tobe
long
itudinalindesig
nandrelyinglesson
self-repo
rtmeasures.
Siuetal.
(2005)
[30]
Toevaluateifnu
rsing
studentse
nrolledin
PBL
programmeh
adhigh
erperceptio
nsof
empo
wermentthanthose
inconventio
nallearning
lecture(CL
L).
Con
venience
sampling:
PBL=83,C
LL=70
Nopo
wercalculationgiven.
Con
ditio
nsforL
earning
Effectiv
enessQ
uestion
naire
(CLE
Q).Psycho
logical
Empo
wermentS
cale,
Teaching
-Learning
Strategies
Question
naire
,ClinicalProb
lem-Solving
Scale.ANCO
VA;
Spearm
an’sRh
oapplied.
PBLexperie
nced
greater
structuralem
powerment
(𝑃=0.001).Stud
entstaking
respon
sibilityfortheirow
nlearning
helped
develop
effectiv
ecom
mun
ication,
listening
,problem
solving,and
collabo
ratio
nskills.
Samplefrom
onlytwo
universities.Self-selectionand
self-repo
rtingqu
estio
nnaires
werea
potentialproblem
.
Needforlon
gitudinal
investigationand
replicationwith
samples
from
severaln
ursin
gprograms.

ISRN Nursing 5
Table4:Qualitatives
tudies.
Author/year
Aim
sParticipantsele
ction
Assessmentm
easures
Outcomes
Suggestedresearch
Chris
tiansen
andBe
ll(2010)
[19]
Toexploreimpactof
peer
learning
initiativetofacilitate
mutually
supp
ortiv
elearning
betweenstu
dent
nurses.
Purposively
selected.
𝑁=54.
Focusg
roup
interviews.
Narrativ
edatea
nalyzed
them
atically.
Datac
ollected
over
18mon
thsw
ith3
coho
rtso
fstudents.
Activ
esup
portfro
mpeersc
anredu
cenegativ
efeelin
gsexperie
nced
byfirstyear
student
nurses.Itassistsc
oping
anddecreasesa
ttrition
rates.Peersb
enefitedby
gaining
confi
dencea
ndincreasedreadinessfor
registe
redpractic
e.
Exploreimpactof
peer
learning
onmentorsin
the
workplace.
Chris
tiansen
andJensen
(2008)
[33]
Toexplorec
lassroom
-based
peer
learning
enablin
gstu
dentstocultivatetheir
mod
esof
expressio
n.
Voluntaryselectionfro
m288stu
dentsd
oing
third
year
commun
ication
course;16stu
dentstoo
kpartin
roleplay
and8in
focusg
roup
interview.
Observatio
nsandfocus
grou
ps.
Providetoo
lsthatcanbe
used
inclinicalpractice.Stud
ents
learnt
from
each
othera
ndappreciatedbeingableto
experie
nced
ifferentroles.
Furtherstudy
onstu
dentse
motional
learning
durin
gperio
dsof
clinical
practic
e.
Coo
keand
Moyle(2002)
[27]
Toexplorea
ndevaluatethe
useo
fPBL
over
aone-m
onth
perio
din
programmethat
uses
CLL.
130stu
dents—
100
respon
dedto
questio
nnaire.
Openendedqu
estio
nnaire.
Gavem
orec
ontro
loverlearningandaddedrespon
sibility,
prom
otingindepend
ent,self-directed
learning
.PBL
was
enjoyable.
Non
ementio
ned.
Daley
etal.,
(2008)
[20]
Toevaluateap
eer-tutorin
gapproach
toteaching
desig
ned
tomeetn
eeds
oftwodifferent
levelsof
students.
Allfirstyear
andsome
senior
studentsina
leadership
and
managem
entcou
rse.
Observatio
ns,con
ferences,
focusg
roup
s,andjournals.
Multip
lelevelsof
evaluatio
n.
Assig
nmento
fhighera
cuity
patie
ntstofirstyears.
Con
fidence
ofweakerstudentsincreased.B
etter
understand
ingof
roleof
team
mem
ber,im
provem
entin
cogn
itive
andmotor
skills,increasedcomfortin
asking
questio
ns/disc
ussin
gconcepts,
andaw
arenesso
fafuture
roleas
mentor.
Additio
nalw
orkand
form
alevaluatio
nof
programme.
Horne
etal.
(2007)
[25]
Toevaluatestu
dent
and
facilitator
perspectives
ofhybrid
mod
elof
prob
lem-based
learning
.
All121secon
dyear
studentsa
nd15
facilitators.
Focusg
roup
interviewsa
nduseo
fFou
rthGeneration
Evaluatio
n(nom
inalgrou
ptechniqu
e).
PBLaideddevelopm
ento
find
ependent
learning
skills,
self-aw
areness,andconfi
dences
kills.Improved
interpersonal/c
ommun
icationskillsb
utdepend
edon
grou
pcollabo
ratio
nandconcerns
abou
tteamworkand
grou
pdynamics.
Furtherstudy
ofeffectiv
enessfor
large
grou
psof
students
>100.
Loke
and
Chow
(2007)
[23]
Tofacilitatethe
developm
ent
of“coo
perativ
elearning”
amon
gnu
rsingstu
dents
throug
hpeer
tutorin
g.
Voluntaryselectionof
14third
year
studentsa
stutorsand16
second
year-studentsa
stutees.
Focusg
roup
sand
individu
alinterviewsa
thalf
way
andendof
10-w
eek
tutorin
gperio
d.
Positives
inclu
dedenhancem
ento
fdeeplearning
,critical
thinking
,problem
solving,commun
icationskills,
confi
denceinow
nlearning
,and
timem
anagem
ent.
Negatives
inclu
dedparticipantsbeinglateo
rfeelin
gof
not
having
adequatekn
owledgetosharew
ithon
eano
ther
and
mism
atched
person
alities.
Furtherstudies
toexam
ine
peer-tu
torin
geffects
onstu
dentsinall
years.
Morris
and
Turnbu
ll(200
4)[26]
Toexplorev
iabilityandvalue
ofusingstu
dent
nurses
asteachersin
inqu
iry-based
nursingcurriculum
.
Apu
rposives
ampleo
f240stu
dent
nurses
(36%
)participated
ininterviews.
Focusg
roup
interviews,
field
notes,interviews
audio-taped,transcrib
ed,
andanalyzed
using
them
aticanalysis.
Stud
entn
ursesw
ereu
ncom
fortablewith
thismetho
dand
thou
ghtitm
ostly
inapprop
riate,alth
ough
itmay
beapprop
riatein
somec
ircum
stances.U
seof
parallel
resource
sessions
inan
onfacilitated
forum
isprob
lematic.
Participantsdidno
tthink
thatskillsw
eretransferable.
Furtherresearch
requ
iredon
theu
seof
studentsa
steachers.
Roberts
(2008)
[18]
Toexploreifstudentslearn
from
each
othera
ndho
w,when/where
thistakesp
lace.
Voluntaryselectionof
15stu
dents.
Audio-tapedconversatio
nsof
studentsa
ndfield
notes;
them
aticanalysis.
Friend
shipsa
reim
portanttolearning
.Peerlearningin
clinicalpracticeisinformalandconsidered
partof
thejob.
Ithelped
studentstoaskqu
estio
nsandcontrib
utetothe
ward.Stud
entswerea
pproachablea
ndhadmoretim
efor
teaching
.Studentsv
aluedpeersinclinicalsettin
ghelping
each
othertocope
with
demands
ofclinicalpractice.
Replicates
tudy
with
otherg
roup
sof
studentsindifferent
locatio
nsand
branches
ofnu
rsing.

6 ISRN Nursing
Table5:Mixed
metho
dstu
dies.
Year/autho
r/Aim
sSetting
Participant
selection
Assessment
measures
Outcomes
Generalizations
and
limitatio
nsSuggested
research
Brosciou
sandSaun
ders
(2001)[24]
Toim
plem
enta
strategyto
redu
cestu
dent
anxiety
durin
gtheirfi
rst
clinicalexp
erience.
Junior/seniory
ear
studentsin
universityin
USA
20senior
students
and25
junior
students.
Con
venience
sampleo
fall
studentsinyear.
Group
interview
andLikertscale
survey:scalehad
statem
ents
presentedas
descrip
tionof
student
experie
nces.
On5-po
intL
ikertscale(onlymeans
repo
rted)
studentsreporteddecreasedsenseo
fanx
iety
(mean4.29),increasin
gconfi
dence(mean
4.08),im
proved
organizatio
n(m
ean3.91),and
perceptio
nof
beingam
embero
fthe
team
(mean3.83).Senior
studentsp
racticed
leadership
skill
(mean4.53),establish
edpriorities(mean4.4),and
developedplan
ofcare
(4.4).Re
iteratedam
ount
learnt
bysenior.
Impactof
coachdecreasedin
subsequent
clinicalsessio
n.
Smallsam
plea
ndvoluntaryselection
limits
generalization.
Furtherstudy
bymod
ifyingand
different
sites
andlarger
sample.
Feingold
etal.(2008)
[32]
Toevaluatestu
dent
perceptio
nof
team
learning
andeffect
oncla
ssinteraction
andengagement.
Firstyearstudent
nurses
ata
universityin
south-western
USA
Firstyearstudents
incourse.
Con
venience
sample:for
interview—10%,
respon
ses—
21%.
Observatio
nand
interviews
(Qualitative).
STRO
BEcla
ssroom
observationtool
(Quantitativ
e).
Team
learning
prom
oted
student
engagement
andwas
predom
inantly
interactive.Over3
05minutes,m
oststudentsw
eree
ngaged/ontask
for8
4%of
time,with
70%of
timeb
eing
learner
tolearnere
ngagem
entand
further8
%of
time
beingused
forself-eng
agem
ent.Main
behaviou
rwas
learnertolearnere
ngagem
ent.
Recogn
ized
benefit
ofdiscussio
nof
prob
lems.
Thec
oncept
couldbe
generalized.Small
samplem
ayno
tbe
representativ
eoffi
rst
year
students
(non
rand
om,
self-selected).
Furtherstudy
tohelprefin
eteam
learning
process
andto
guide
implem
entatio
nof
interactive
learning
strategies.
Goldsmith
etal.(2006)
[7]
Toexploreimpact
ofpeer
learning
onanxietyof
firstyear
student
nurses
whenun
dertaking
clinicalskills
assessments.
First/3
rdyear
studentsinClinical
Practic
eUnit
(CPU
)inAu
stralia
(Con
ducted
over
twoyearsa
ndtwo
campu
ses)
First/3
rdyear
studentsin2-year
timeframe.First
year
coho
rtof
187;
3rdyear:178.
Portfolio
subm
issionas
3rd
year,clin
icalskills
assessmentfor
first
year
students.Bo
thgrou
pscompleted
questio
nnaires.
Learning
enhanced
byexperie
nce.
Evaluatio
ncompleted
after
2years;good
representatio
nsof
both
campu
ses/years.
Learning
enhanced
byexperie
nce.Po
sitive
answ
erstoqu
estio
nswereg
iven
byam
ajority
ofbo
th1st/3
rdyearsw
ith3rdyearsm
orelikely
togive
positiver
espo
nses.
Onlytwocampu
seso
fon
euniversity.L
ate
developm
ento
fassessmenttoo
lwith
notallstu
dentsg
iven
oppo
rtun
ityto
complete
questio
nnaire.
Voluntarycompletion
ofqu
estio
nnaire
which
may
noth
ave
been
representativ
e.
Not
repo
rted.
Tiwarietal.
(200
6)[31]
Tocompare
effects
ofprob
lem-based
learning
and
lecturing
approaches
ondevelopm
ento
fstu
dents’critical
thinking
.
Firstyearstudent
nurses
inon
eun
iversityin
Hon
gKo
ng
All79
studentsin
firstyear
rand
omly
assig
nedto
control
andinterventio
ngrou
ps.P
BL=40
,CL
L=39.Selectio
nby
ballo
t.
Multiv
ariate
regressio
n,1and
2samplet-te
sts.
Nosig
nificantd
ifference
betweengrou
psat
initialtesting(𝑃=0.48).2n
dand3rddata
collectionpo
intsshow
edsig
nificantd
ifference
inoverallC
CDTI
scores
betweenPB
Land
controlgroup
s(𝑃=0.0048,𝑃=0.0083).Th
e4thcollectionpo
intsho
wed
high
erscoreo
ntheC
CDTI
forP
BLgrou
pbu
tnon
significant
difference(𝑃=0.1159).PB
Lstu
dentsfou
ndtheirc
oursem
oree
njoyable/in
spiring
than
lectureg
roup
.
Onlyon
euniversity
andas
mallsam
ple.
Results
may
have
been
influ
encedby
howlectures
were
cond
ucted.Use
ofself-repo
rtingtool.
Mon
itorin
gof
grou
pscritical
thinking
insubsequent
years.

ISRN Nursing 7
examined how the participants felt about a different methodof learning and how it impacted on them. These opinionswould be important if peer learning was to gain acceptancefrom the students and peers. Qualitative studies had muchsmaller participant numbers and whilst larger numbers mayhave provided a more comprehensive sample, there weresaturation and repetition of concepts even with the smallersamples.
Experimental studies with the highest level of evidence,that is, random controlled trials (RCTs), were not a commonmethod of evaluating peer learning as they may not repro-duce the true situation in an educational setting [34].
Eight studies used a comparison group [21, 22, 27–31, 35],and all except two [27, 31] were quantitative studies. Validtools were used by 9 of the 10 quantitative or mixed methodstudies. It was concluded that valid tools measured what theauthors intended, and hence data were an accurate represen-tation of what had occurred and were credible. However, onestudy [21] failed to report the number of control and interven-tion group participants who passed their course.The qualita-tive studies documented the research process clearly, and thefindings were consistent with the data provided. The detailsin description of the research process and findings variedbetween studies, whilst within individual studies, sample size,location, and the subjects taught were all potentially limiting;for example, small sample size, specific location, or subjectmay have caused a bias in the results, hence affecting thetransferability of results [24, 31]. Publication bias was notevident as the included studies reported both the positive andnegative results, for example, using comments from partici-pants [26] or differences in means [35].
3.2. Effects of Peer Learning. Peer learning encouraged inde-pendent study, critical thinking, and problem solving skills. Itcould give students a sense of autonomy when they acceptedresponsibility for their own education. Peer learning wasassociated with increased levels of knowledge in a number ofareas such as problem solving and communication [20, 25].Tiwari et al. [31] showed that critical thinking was improvedin students using PBL (𝑃 = 0.0048) whilst Daley et al. [20]reported that students showed improvement in cognitive andmotor skills. An advantage of peer learning was that bothgroups learned and benefited from the interaction [23, 24].The benefits differed between the students and peers with thepeers gaining experience in communication and leadership,reinforcing their prior learning and discovering what theywere capable of achieving in the mentoring/teaching fields[19, 24]. On the other hand, students gained confidence andexperienced a decrease in anxiety when dealing with certainsituations such as clinical placements. PBLwas reported to beeffective particularly in the theoretical learning component ofeducation whilst peer tutoring, peer coaching, peer mentor-ing, and the use of role play as a form of peer learning wereall effective, both in clinical and theoretical aspects of nursingeducation.
One negative aspect was related to anxiety levels. Grouplearning showed an increase in anxiety in both control andintervention groups [35], whilst other methods such as peer
coaching showed a decrease in anxiety in the clinical setting[24].The students indicated that having another person assistthemdecreased their anxiety levelswhichwas pertinentwhenthey were beginning their careers and were uncertain andanxious about what was expected of them [18]. Informal peerlearning also benefited the students by providing them with“survival” skills that are not taught in lectures or text books,which in turn assisted in decreasing anxiety [18].
In addition to decreasing anxiety [24], many studentsshowed an increase in satisfaction when peer learning wasused [22, 29], appreciating having to think for themselves,problem-solve, andwork as a team [20, 24, 27, 30].The level ofsatisfaction is higher with peer learning [29] than the passiveCLL method although some students still prefer CLL as itmaybe better suited their individual learning style [22].Whilst none of the studies in this paper directly investigatedthe link between course satisfaction and academic results,Higgins [21] noted a decrease in attrition rate but did notspecify student satisfaction levels.
Four studies [20, 23–25] examined confidence in studentswhen utilizing peer learning. They showed a subjectiveincrease in confidence levels when completing clinical skills,problem solving, and critical thinking. In addition, 11 stud-ies indicated that students appreciated interactive learningsessions and the emphasis on active participation, whichencouraged them to take ownership and responsibility fortheir own learning.
3.3. Utilization. Peer learning was utilized in multiple sit-uations from teaching ethics [22] and critical thinking [31]to helping students deal with emotional situations [19] withpatients. In clinical situations peer learning was successfuland improved integration into the ward situations [18] andstudents’ confidence when dealing with actual patients ratherthan a simulator [20]. Further, a number of studies identifiedoutcome measures showing an improvement in either anobjective or subjective assessment.
4. Discussion
The purpose of this research was to ascertain whether under-graduate nursing students benefit from peer learning. Sixteenof eighteen studies demonstrated positive aspects to peerlearning with outcome measures showing improvement ineither an objective effect or a subjective assessment (suchas a self-rated increase in student confidence). Furthermore,learning from peers was shown to be acceptable to most stu-dents. Much of the research into peer learning concentratedon formal peer learning with the evidence supporting theconcept that peer learning may be an equally, if not more,effective method of delivering information in undergraduatenursing education.
Peer learning can be utilized to pass information to largegroups of students with less faculty member involvement.At a time when there is pressure to train more nurses andminimize costs [12], peer learning could utilize resourcesmore effectively with students teaching and supervisingmore

8 ISRN Nursing
junior students, thus decreasing the demand on the respon-sible faculty members.Therefore it may have cost benefits formanaging some aspects of nursing education; however thistheory requires further investigation as it was not the focusof any of the papers mentioned in this paper.
Regardless of any decrease in active involvement by lec-turers, the need for student supervision remains important.If peers are not knowledgeable or do not have the appro-priate skills, then they cannot accurately pass informationonto another student. The learning of inaccurate informa-tion could potentially cause issues for students when theseinaccuracies were demonstrated in exams and on clinicalplacements. Without supervision, learning may not be effec-tive as shown in an earlier study by Parkin [4] who foundthat observation and supervision were required in all peerlearning to ensure that correct and current information wasbeing exchanged.
4.1. Advantages and Disadvantages. Peer learning may resultin information being more readily accepted by a student asindividuals often turn to others who have similar experiences,for advice and guidance. This could decrease anxiety asso-ciated with learning due to familiarity of the peer with thestudent’s issues. As noted in the results, anxiety may occurwhen individuals are exposed to new concepts, whether theyare novice or proficient learners [36]. In prior research [37],peer learning helped to decrease the student’s anxiety andassisted them to fit into a ward situation and feel like partof the team. This sense of belonging has social implicationsparticularly when it is known that learning occurs moreeffectively when there is socialization [38, 39].
Further, social interaction and collaboration betweenpeer and student may have contributed to an increased learn-ing curve and acquisition of further knowledge than wouldhave occurred if students were studying independently. Thiswas illustrated in this paper with students who had been indanger of failing and had received peer tutoring [21]. Theygained additional knowledge and improved their academicresult. This method may also allow junior students toproblem-solve issues with their patients more independentlyand care for higher acuity patients, leading to an increase intheir self-confidence.This conceptwas previously reported byVygotsky [40], Aston and Molassiotis [41], and Secomb [5]who found that peer learning promoted self-confidence injunior students whilst assisting senior students with mentor-ing and teaching skills. Secomb [5] also showed that peerlearning was an effective learning tool in clinical situationswith both nursing and other health professionals. Peers per-ceived an increase in patient care competence when peerlearning was utilized. Secomb [5] noted, however, that issuessuch as inappropriate pairing of students and peers should beaddressed prior to the intervention.
Student satisfactionmay play a part in scholastic achieve-ment through acceptance of an active learning method suchas peer learning. Four studies investigating this component[22, 28–30] discovered that students were satisfied with peerlearning as the educational method. This may be because thestudent takes more responsibility and actively participates in
their education, giving them a sense of autonomy. WhilstOzturk et al. [28] reported a higher satisfaction level with PBLbut no significant difference in academic scores, previousstudies have shown a positive association between studentsatisfaction and grades achieved [42, 43].
Peer learningmay also bemore successful when peers areclose in experience or stage of training as it provides a morerelaxed, less intimidating,more “user friendly” learning expe-rience than sessions conducted by registered nurses. Priorto the current study, El Ansari and Oskrochi [44], Eisen [45],and Secomb [5] also reported this finding whilst morerecently Bensfield et al. [46] reported that first year studentshad comfortable learning with more experienced peers.
There is, however, a different perspective. Whilst peerlearning has been used for years and might be becoming thenorm, students may not be fully familiar with it and there-fore be apprehensive about what it offers. Some studentsreported anxiety and apprehension when taking part in peerlearning which was linked to feeling responsible for another’seducation [25, 26], being underprepared [23] or concernedthat their own grades would be negatively affected by groupwork or dynamics [25, 26, 32]. Further, it was reported thatenforcing the educational role of a peer may lead to resent-ment, particularly if the nurse felt unprepared or unwillingto undertake the role [26]. Previously Bensfield et al. [46]showed that whilst nurses have a responsibility to teachothers, many are reluctant to do so as they feel unprepared forthe role. Due to these issues, students who are familiar andcomfortable with CLL may continue to prefer this learningmethod over peer learning.
4.2. Confusing Terminology Used in Peer Learning. Finally,this paper raises issues around the confusing terminologyused to refer to peer learning. As mentioned, multiple termssuch as peer teaching, peer mentoring, and peer coachingwere used interchangeably with debate about whether theymeant the same thing or referred to subtle differences inmeaning. A clearer definition of each of the terms is needed toincrease the rigor of nursing education research, as was alsoraised by Secomb [5], Eisen [45], and McKenna and French[47] who found a lack of clarity as to what peer educationentailed due to the interchanging of terminology. We suggestamalgamation of some of the terms, for example, team learn-ing and cooperative learning or peer mentoring and peercoaching and having distinct differences in definitionsbetween other terms.
5. Limitations
Some limitations of this study were recognized. Only studiespublished in English were included. Despite a rigorous searchstrategy, some relevant articles may have been omitted owingto the search terms used. The mix of study designs andvarious methods of reporting meant that direct comparisonbetween studies was limited. Some studies were location- ortopic-specific, and some studies collected data using indirectoutcomemeasures. However, the collection and review of thediverse papers that were selected offered the best option for

ISRN Nursing 9
determining the overall impact of peer learning in educationof nursing students.
6. Conclusion
Peer learning: learning from others who possess a similarlevel of knowledge, is becoming a part of nursing education.This study showed that undergraduate nursing students couldbenefit from peer learning, with an increase in confidenceand competence and a decrease in anxiety. Their peers alsogained skills to prepare them for their role as a registerednurse. Conduct of peer learning within the curriculum wasshown to require adequate academic supervision to be effec-tive. It was difficult to ascertain the most effective learningmethods because of the inherent variation between studymethodologies, terminology, subjects, and settings. Inconsis-tency terminology was identified as a problem that should beaddressed in order to provide clarity in future research.
7. Further Research
Further research is needed to fully investigate peer learningwith the use of larger samples, various targeted curricula,courses, and locations to increase the validity of studies. Thecost effectiveness of peer learning should be further inves-tigated and compared to that of CLL to ascertain how thisoption could impact nursing education in terms of resources,time management, and effectiveness.
References
[1] C. L. Iwasiw, D. Goldenderg, and M. A. Andrusyszyn, Cur-riculum Development in Nursing Education, Jones & Bartlett,Boston, Mass, USA, 2nd edition, 2009.
[2] M. Banning, “Approaches to teaching: current opinions andrelated research,”Nurse Education Today, vol. 25, no. 7, pp. 502–508, 2005.
[3] S. Paterson and R. Stone, “Educational leadership beyondbehaviourism, the lessons we have learnt from art education,”Australian Art Education, vol. 29, no. 1, pp. 76–83, 2006.
[4] V. Parkin, “Peer education: the nursing experience,” Journal ofContinuing Education in Nursing, vol. 37, no. 6, pp. 257–264,2006.
[5] J. Secomb, “A systematic review of peer teaching and learningin clinical education,” Journal of Clinical Nursing, vol. 17, no. 6,pp. 703–716, 2008.
[6] L. D. Owens and D. J. Walden, “Peer instruction in the learninglaboratory: a strategy to decrease student anxiety,” Journal ofNursing Education, vol. 40, no. 8, pp. 375–377, 2001.
[7] M. Goldsmith, L. Stewart, and L. Ferguson, “Peer learningpartnership: an innovative strategy to enhance skill acquisitionin nursing students,” Nurse Education Today, vol. 26, no. 2, pp.123–130, 2006.
[8] S. Blowers, P. Ramsey, C. Merriman, and J. Grooms, “Patternsof peer tutoring in nursing,” Journal of Nursing Education, vol.42, no. 5, pp. 204–211, 2003.
[9] H. Yuan, B. A. Williams, and L. Fan, “A systematic review ofselected evidence on developing nursing students’ critical
thinking through problem-based learning,” Nurse EducationToday, vol. 28, no. 6, pp. 657–663, 2008.
[10] A. J. Neville, “Problem-based learning and medical educationforty years on: a review of its effects on knowledge and clinicalperformance,”Medical Principles and Practice, vol. 18, no. 1, pp.1–9, 2008.
[11] D. Nestel and J. Kidd, “Peer tutoring in patient-centred inter-viewing skills: experience of a project for first-year students,”Medical Teacher, vol. 25, no. 4, pp. 398–403, 2003.
[12] H. T. Allan, P. A. Smith, and M. Lorentzon, “Leadership forlearning: a literature study of leadership for learning in clinicalpractice,” Journal of NursingManagement, vol. 16, no. 5, pp. 545–555, 2008.
[13] D. Shipman and J. Hooten, “Without enough nurse educatorsthere will be a continual decline in RNs and the quality of nurs-ing care: contending with the faculty shortage,” Nurse Educa-tion Today, vol. 28, no. 5, pp. 521–523, 2008.
[14] J. Green, “Peer education,” Promotion & Education, vol. 8, no. 2,pp. 65–68, 2001.
[15] J. P. T. Higgins and S. Green, “Cochrane Handbook for sys-tematic reviews of interventions:The Cochrane Collaboration,”2009, http://www.cochrane-handbook.org/ .
[16] The National Health and Medical Research Council, NHMRCAdditional Levels of Evidence and Grades for Recommendationsfor Developers of Guidelines. Stage 2 Consultation, The Aus-tralian Government, Parkes ACT, Australia, 2009.
[17] Public Health Resource Unit, “Critical Appraisal Skills Pro-gramme Making sense of evidence, 10 questions to helpyou make sense of reviews,” 2006, http://www.phru.nhs.uk/Doc Links/S.Reviews%20Appraisal%20Tool.pdf.
[18] D. Roberts, “Learning in clinical practice: the importance ofpeers,” Nursing Standard, vol. 23, no. 12, pp. 35–41, 2008.
[19] A.Christiansen andA. Bell, “Peer learning partnerships: explor-ing the experience of pre-registration nursing students,” Journalof Clinical Nursing, vol. 19, no. 5-6, pp. 803–810, 2010.
[20] L. K. Daley, E. Menke, B. Kirkpatrick, and D. Sheets, “Partnersin practice: a win-win model for clinical education,” Journal ofNursing Education, vol. 47, no. 1, pp. 30–32, 2008.
[21] B. Higgins, “Relationship between retention and peer tutoringfor at-risk students,” Journal of Nursing Education, vol. 43, no. 7,pp. 319–321, 2004.
[22] C. F. Lin, M. S. Lu, C. C. Chung, and C.M. Yang, “A comparisonof problem-based learning and conventional teaching in nurs-ing ethics education,” Nursing Ethics, vol. 17, no. 3, pp. 373–382,2010.
[23] A. Y. Loke and F. L. W. Chow, “Learning partnership-the expe-rience of peer tutoring among nursing students: a qualitativestudy,” International Journal of Nursing Studies, vol. 44, no. 2,pp. 237–244, 2007.
[24] S. K. Broscious and D. J. Saunders, “Peer coaching,” Nurse Edu-cator, vol. 26, no. 5, pp. 212–214, 2001.
[25] M. Horne, K. Woodhead, L. Morgan, L. Smithies, D. Megson,and G. Lyte, “Using enquiry in learning: from vision to realityin higher education,” Nurse Education Today, vol. 27, no. 2, pp.103–112, 2007.
[26] D. Morris and P. Turnbull, “Using student nurses as teachers ininquiry-based learning,” Journal of Advanced Nursing, vol. 45,no. 2, pp. 136–144, 2004.
[27] M. Cooke and K. Moyle, “Students’ evaluation of problem-based learning,” Nurse Education Today, vol. 22, no. 4, pp. 330–339, 2002.

10 ISRN Nursing
[28] C. Ozturk, G. K. Muslu, and A. Dicle, “A comparison ofproblem-based and traditional education on nursing students’critical thinking dispositions,” Nurse Education Today, vol. 28,no. 5, pp. 627–632, 2008.
[29] E. Rideout, V. England-Oxford, B. Brown et al., “A comparisonof problem-based and conventional curricula in nursing edu-cation,” Advances in Health Sciences Education, vol. 7, no. 1, pp.3–17, 2002.
[30] H. M. Siu, H. K. Spence Laschinger, and E. Vingilis, “The effectof problem-based learning on nursing students’ perceptions ofempowerment,” Journal of Nursing Education, vol. 44, no. 10, pp.459–469, 2005.
[31] A. Tiwari, P. Lai, M. So, and K. Yuen, “A comparison of theeffects of problem-based learning and lecturing on the develop-ment of students’ critical thinking,”Medical Education, vol. 40,no. 6, pp. 547–554, 2006.
[32] C. E. Feingold, M. D. Cobb, R. Hernandez Givens, J. Arnold, S.Joslin, and J. L. Keller, “Student perceptions of team learning innursing education,” Journal of Nursing Education, vol. 47, no. 5,pp. 214–222, 2008.
[33] B. Christiansen and K. Jensen, “Emotional learning within theframework of nursing education,” Nurse Education in Practice,vol. 8, no. 5, pp. 328–334, 2008.
[34] B. Jolly, “Control and validity in medical educational research,”Medical Education, vol. 35, no. 10, pp. 920–921, 2001.
[35] L. C. Hughes, P. Romick, M. K. Sandor et al., “Evaluation ofan informal peer group experience on baccalaureate nursingstudents’ emotional well-being and professional socialization,”Journal of Professional Nursing, vol. 19, no. 1, pp. 38–48, 2003.
[36] L. T. Adams, “Nursing shortage solutions and America’s eco-nomic recovery,” Nursing Education Perspectives, vol. 30, no. 6,p. 349, 2009.
[37] P. Benner, “Using the dreyfus model of skill acquisition todescribe and interpret skill acquisition and clinical judgment innursing practice and education,” Bulletin of Science, Technologyand Society, vol. 24, no. 3, pp. 188–199, 2004.
[38] J. M. Parr and M. A. R. Townsend, “Environments, processes,and mechanisms in peer learning,” International Journal ofEducational Research, vol. 37, no. 5, pp. 403–423, 2002.
[39] I. A. G. Wilkinson, “Peer influences on learning: where arethey?” International Journal of Educational Research, vol. 37, no.5, pp. 395–401, 2002.
[40] L. S. Vygotsky, Biological and Social Factors in Education. Edu-cational Psychology, St. Lucie Press, Boca Raton, Fla, USA, 1997.
[41] L. Aston and A. Molassiotis, “Supervising and supporting stu-dent nurses in clinical placements: the peer support initiative,”Nurse Education Today, vol. 23, no. 3, pp. 202–210, 2003.
[42] B. Sinclair and K. Ferguson, “Integrating simulated teaching/learning strategies in undergraduate nursing education,” Inter-national Journal of Nursing Education Scholarship, vol. 6, no. 1,p. 7, 2009.
[43] P. M. Casey, D. Magrane, and T. G. Lesnick, “Improved per-formance and student satisfaction after implementation of aproblem-based preclinical obstetrics and gynecology curricu-lum,” American Journal of Obstetrics and Gynecology, vol. 193,no. 5, pp. 1874–1878, 2005.
[44] W. El Ansari and R. Oskrochi, “What matters most? Predictorsof student satisfaction in public health educational courses,”Public Health, vol. 120, no. 5, pp. 462–473, 2006.
[45] M. J. Eisen, “Peer-based professional development viewedthrough the lens of transformative learning,” Holistic NursingPractice, vol. 16, no. 1, pp. 30–42, 2001.
[46] L. Bensfield, P. A. Solari-Twadell, and S. Sommer, “The use ofpeer leadership to teach fundamental nursing skills,”Nurse Edu-cator, vol. 33, no. 4, pp. 155–158, 2008.
[47] L. McKenna and J. French, “A step ahead: teaching undergrad-uate students to be peer teachers,” Nurse Education in Practice,vol. 11, no. 2, pp. 141–145, 2011.
[48] D. Nestel and J. Kidd, “Peer assisted learning in patient-centredinterviewing: the impact on student tutors,” Medical Teacher,vol. 27, no. 5, pp. 439–444, 2005.
[49] R. Duggan, “A little help from your PALs,” Nursing Standard,vol. 14, no. 38, p. 55, 2000.
[50] J. E. Duchscher, “Peer learning: a clinical teaching strategy topromote active learning,”Nurse Educator, vol. 26, no. 2, pp. 59–60, 2001.
[51] S. Dennison, “Peer mentoring: untapped potential,” Journal ofNursing Education, vol. 49, no. 6, pp. 340–342, 2010.
Submit your manuscripts athttp://www.hindawi.com
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Breast CancerInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
HematologyAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PediatricsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Urology
HepatologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
InflammationInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgery Research and Practice
Current Gerontology& Geriatrics Research
Hindawi Publishing Corporationhttp://www.hindawi.com
Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
NursingResearch and Practice
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
HypertensionInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Prostate CancerHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgical OncologyInternational Journal of