review article home-based multidisciplinary rehabilitation
TRANSCRIPT

Hindawi Publishing CorporationRehabilitation Research and PracticeVolume 2013, Article ID 875968, 10 pageshttp://dx.doi.org/10.1155/2013/875968
Review ArticleHome-Based Multidisciplinary Rehabilitation following HipFracture Surgery: What Is the Evidence?
Kathleen Donohue,1 Richelle Hoevenaars,1 Jocelyn McEachern,1
Erica Zeman,1 and Saurabh Mehta2
1 School of Rehabilitation Science, McMaster University, Hamilton, ON, Canada L8S 1C72 School of Physical Therapy, Marshall University, 2847 5th Avenue, Huntington, WV 25705, USA
Correspondence should be addressed to Saurabh Mehta; [email protected]
Received 30 July 2013; Revised 2 October 2013; Accepted 14 October 2013
Academic Editor: Eva Widerstrom-Noga
Copyright © 2013 Kathleen Donohue et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Objective. To determine the effects of multidisciplinary home rehabilitation (MHR) on functional and quality of life (QOL)outcomes following hip fracture surgery. Methods. Systematic review methodology suggested by Cochrane Collboration wasadopted. Reviewers independently searched the literature, selected the studies, extracted data, and performed critical appraisalof studies. Summary of the results of included studies was provided. Results. Five studies were included. Over the short-term,functional status and lower extremity strength were better in the MHR group compared to the no treatment group (NT). Overthe long-term, theMHR group showed greater improvements in balance confidence, functional status, and lower extremity musclestrength compared toNTgroup,whereas the effect onQOLandmobilitywas inconsistent across the studies. Severalmethodologicalissues related to study design were noted across the studies. Conclusion. The MHR was found to be more effective compared to theNT in improving functional status and lower extremity strength in patients with hip fracture surgery. Results of this review do notmake a strong case for MHR due to high risk of bias in the included studies. Further research is required to accurately characterizethe types of disciplines involved in MHR and frequency and dosage of intervention.
1. Introduction
Hip fracture is common across all age groups but is morecommon in older adults. Most hip fractures are treatedsurgically [1]. Hip fractures place tremendous burden onhealth care systems [2, 3]. Individuals with hip fractureshave increasedmortality, long-term disability, and functionaldependence since most older adults do not attain pre-injuryfunctional levels [4]. Moreover, impairment in quality of life(QOL), psychological and social domains, and fall relatedefficacy are also reported following a hip fracture [5, 6].Specific interventions have been designed to reduce theimpact of hip fracture on these domains. The components ofan intervention depend on targeted outcome.
Individuals with hip fracture consider increase in mobil-ity and functions to be the preferred outcomes when askedabout their recovery expectations following hip fracture [7].Postsurgical rehabilitation programs aim to reduce disability
and improve mobility, functions, balance, strength and QOLfollowing hip fracture [8]. They are implemented in varietyof settings such as inpatient, outpatient, or home-basedrehabilitation. Posthip fracture rehabilitation may involvemultidisciplinary care, which includes services provided bymultiple health disciplines such as physiotherapy (PT), occu-pational therapy (OT), nursing, social work, and dieteticsunder the supervision of a geriatrician or rehabilitationphysician. Previous systematic reviews have indicated thatmultidisciplinary rehabilitation leads to superior outcomes inindividuals following hip fracture surgery [8–10].
While there is evidence to believe that multidisciplinaryrehabilitation is effective in individuals following hip fracturesurgery, whether the recovery patterns differ depending onthe setting (inpatient, outpatient, or home) in which it isprovided is yet to be determined. Literature thus far haslargely focused on examining the benefits of multidisci-plinary rehabilitation rather than specifically investigating

2 Rehabilitation Research and Practice
the influence of treatment setting in which such rehabil-itation is delivered. Home-based rehabilitation presents aviable option compared to rehabilitation services deliveredin inpatient or outpatient rehabilitation setting. Home-basedrehabilitation typically occurs when a patient is dischargedfrom an inpatient setting (acute care or subacute rehabilita-tion) and receives further rehabilitation at home to maintaincontinuum of care. Home-based rehabilitation programsfacilitate early discharge from hospital, thereby reducing thefinancial burden associated with hip fractures. They are alsosafe and efficient in managing individuals following hip frac-tures [11]. Some of the previous studies have demonstratedthat home-based rehabilitation improves physical function,health related quality of life (HRQOL), and balance confi-dence [11, 12]. However, these studies largely incorporate onlyPT services where the intervention is notmultidisciplinary innature. With distinct advantages of managing individuals intheir home setting, it is important to examine the benefits ofmultidisciplinary home rehabilitation (MHR). In particular, acomprehensive reviewof literature to assess the effect ofMHRon functions, mobility, balance, and HRQOL can facilitateunderstanding of appropriate discharge setting following hipfracture surgery.
The purpose of this study was to conduct a systematicreview of randomized control trials (RCTs) to determinethe effects of MHR on outcomes such as functional status,HRQOL, mobility, lower limb muscle strength, and balancefollowing hip fracture surgery.
2. Methods
2.1. Criteria for including Studies. This review considered allparallel RCTs comparing MHR to inpatient, outpatient, orno treatment (NT) in patients following hip fracture surgery.We defined NT as the groups of patients who receivedconventional acute postsurgical care in hospital and wassent home with no further rehabilitation. In contrast, theinpatient and outpatient groups received multidisciplinaryrehabilitation in inpatient and outpatient setting, respectively,following conventional acute care. The home-based groupreceived multidisciplinary rehabilitation at home followingtheir stay in acute care. Functional status, HRQOL, andbalance confidence were the patient reported outcomes con-sidered for this review. Physical mobility, functional status,lower limb strength, ambulation ability, and balance were theperformance-based outcomes considered for the review.
Only RCTs in which one of the groups received MHRfollowing hip fracture surgery were included. Prospectivecohort and case-control studies were excluded from thereview. Studies with patient groups other than those with hipfracture surgery, those with cost comparison as the primaryoutcome, or those with single-discipline home-based rehabil-itation as the experimental group were also excluded. Trialslooking at the effectiveness of multidisciplinary inpatientrehabilitation and those that examined the benefits of home-based physiotherapy alone were also excluded. Studies whichexamined the effects of MHR after elective hip surgery (suchas total hip arthroplasty) were also excluded.
2.2. Search Techniques for Identifying Relevant Studies. Acomprehensive literature search was performed on multipledatabases to identify studies relevant to this review. Fourstudent investigators (Kathleen Donohue, Richelle Hoeve-naars, Jocelyn McEachern, and Erica Zeman) agreed uponthe search terms to be used in each of the databases a priori.Two reviewers (Kathleen Donohue and Richelle Hoevenaars)performed the searches on the Ovid MEDLINE, EMBASE,PubMed, Cochrane Central Register of Controlled Trials,PEDro, CINHAL, and REHABDATA databases in isolation.ProceedingsFirst was searched to identify any relevant con-ferences and workshops abstracts suitable for this review.Relevant masters and/or doctoral theses were searched onProQuest Dissertations and Thesis. The reference lists ofrelevant studies and systematic reviews were also searchedand studies that appeared relevant in these lists were included.
2.3. Data Collection and Analysis
2.3.1. Selection of Studies. The citations obtained from thesearch were screened by two independent reviewers (JocelynMcEachern and Erica Zeman). A final list of eligible studieswas prepared for full text review. Disagreements between thereviewers were resolved by discussion to reach a consensus.Agreement between the reviewers was assessed by examiningunweighted kappa (𝜅).
2.3.2. Data Extraction andManagement. Data extraction wasperformed independently by two reviewers (JocelynMcEach-ern and Erica Zeman). Both reviewers were in the finalyear of their entry-level physiotherapy program at McMasterUniversity, Hamilton, Canada. A standardized data collectionform was generated for this study. Descriptive data regardingnumber of participants, their age and sex, and the studysetting were extracted. Methodology regarding generation ofrandomization sequence, allocation concealment, blinding,and completeness of outcome data were extracted to gaugethe risk of bias [13]. Information related to the interventionsuch as types of rehabilitation, frequency of visits, andduration of treatments was also extracted.
2.3.3. Assessment of Risk of Bias. An assessment of the risk ofbias in the included studies was completed. Bias was definedas a systematic error in the truth of results or inferences[13]. A domain-based evaluation was used for the risk of biasassessment. The domains included were, random sequencegeneration, allocation concealment, blinding of outcomeassessment and incomplete outcome data.
2.3.4. Measurement of Treatment Effect. The outcomes weredivided and examined as being short-term (the first fourmonths) and long-term (12 months) in order to avoid theunit of analysis issues while performing analysis [14]. We hadplanned to examine standardized mean differences for all theoutcomes (patient reported and performance-based) if thedata across the included studies was deemed to be suitablefor pooling. However, we chose to provide the summary ofresults and provide point estimates of treatment effects given

Rehabilitation Research and Practice 3
that themeta-analysis was not feasible due to heterogeneity inthe study design, participants, outcomes, interventions, anddata reporting.
2.3.5. Assessment of Reporting Biases. To determine anyinfluence on the nature or direction of results, reportingbiases were assessed [15]. A funnel plot to assess publicationbias could not be plotted since only five studies were includedin this review. We used comprehensive search including greyliterature such as conference proceedings, dissertations, andmaster and doctoral theses to ensure that the possibility of thepublication bias was minimized. Citation bias was limited asbibliographies of relevant systematic reviews were searched.Location and language biases were minimized by avoidinglocation and language limitations for the literature search.
2.3.6. Subgroup Analysis and Investigation of Heterogeneity.Due to the nature and intensity of the multidisciplinaryrehabilitation provided in different settings, we did not findit appropriate to combine the results and assess the treatmenteffect of MHR versus other comparison groups combinedtogether. Rather, we opted to create subgroups and assess thetreatment effect of the MHR (MHR versus institution-basedrehabilitation and MHR versus NT).
Sensitivity Analysis was not required since no data impu-tations were done.
3. Results
The literature search strategies are outlined in Figure 1. Thepreliminary search identified 2987 citations. Twenty-twostudies were selected for full text review. Five studies metthe predefined inclusion/exclusion criteria and were chosenfor this review. The process used to identify and select thestudies used in this review is depicted in a flow diagramin Table 1. The raw agreement between two independentreviewers (Jocelyn McEachern & Erica Zeman) for inclusionof studies in this review was 86% with an unweighted 𝜅 of0.73, which is considered acceptable [16].
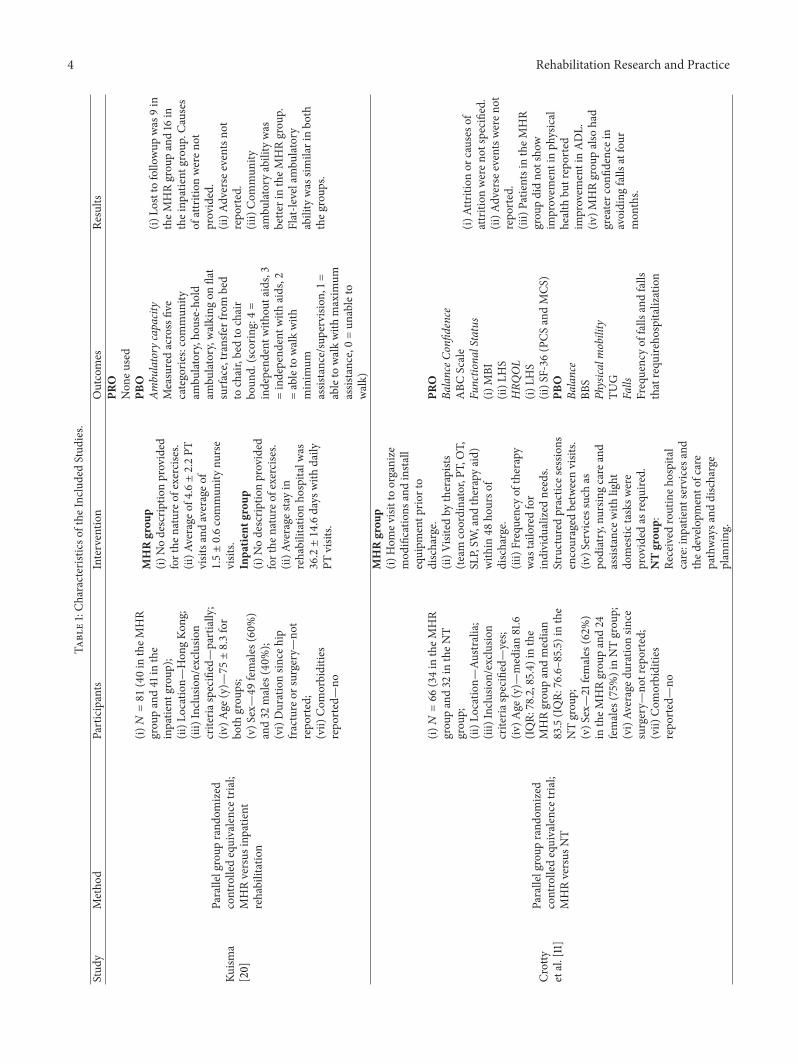
3.1. Description of Included Studies. Of the five studiesincluded, two were conducted in Sweden [17, 18], two in Aus-tralia [11, 19], and one in Hong Kong [20]. Comparator groupwas inpatient hospital-based setting in one [20] andNT in theother four studies [11, 17–19].The treatment groups within allstudies were discharged from inpatient hospital care to homewhere they received MHR. The number and disciplines thatcomposed the multidisciplinary rehabilitation team variedbetween studies but all of them included physiotherapy (PT).The follow-up period varied between 1 month and 12 monthsbetween studies. A detailed description and characteristics ofall included studies are expressed in Table 1.
3.2. Description of Excluded Studies. Nineteen studies wereexcluded after full text review.The reasons for exclusion werethat the intervention was not provided by a multidisciplinaryteam (𝑛 = 11), participants had elective hip replacementsurgery (𝑛 = 3), comparator group of interest was lacking
Articles identified on preliminary search
N = 2987
Reasons: not treatment of interest, not comparison of interest, not hip fracture surgery, and not RCTs
Potentially relevant articlesN = 1389
Duplicates (exact and close match) removed
N = 1598
Studies included for the full-text review N = 22
Studies included in the review N = 5
Studies excluded after full-text review N = 19
Excluded N = 1367
Figure 1: Flow Diagram.
(treatment and control group both had home-based inter-vention) (𝑛 = 2), treatment group did not have home-basedintervention (𝑛 = 1), there was no RCT design (𝑛 = 1). Arecent study conducted by Tseng et al. [21] was also excludedafter careful review. The objective of their study was toassess the effects of interdisciplinary intervention on differenttrajectories of recovery (poor, moderate, and excellent) inindividuals with hip fractures and not necessarily provide adirect comparison between the MHR group and the usualcare group.
3.3. Risk of Bias in Included Studies. The agreement betweenreviewers for assessing the risk of bias was substantial, withan unweighted 𝜅 of 0.70 and a raw agreement of 84% [16].Table 2 summarizes risk of bias assessment for the includedstudies.
Despite the assumption that the original and follow-uparticles would have identical protocols, the risk of bias in theincluded studies was assessed for Crotty et al. [11, 19] studiesas well as the Ziden et al. [17, 18] with both the pairs reportingshort-term and long-term results of their respective projects.This is because some of the aspects of the publication such asthe blinding of outcomes assessors at different time points,incomplete outcome data reporting, and selective outcomereporting could be different for the same study for whichthe results were reported in two separate publications. WhileCrotty et al. [19] had very low risk of bias, their earlierpublication [11] had risk of bias due to inadequate details ofallocation concealment and incomplete data reporting. The
4 Rehabilitation Research and PracticeTa
ble1:Ch
aracteris
ticso
fthe
Inclu
dedStud
ies.
Stud
yMetho
dParticipants
Interventio
nOutcomes
Results
Kuism
a[20]
Parallelgroup
rand
omized
controlledequivalencetria
l;MHRversus
inpatie
ntrehabilitation
(i)𝑁=81(40in
theM
HR
grou
pand41
inthe
inpatie
ntgrou
p);
(ii)L
ocation—
Hon
gKo
ng;
(iii)Inclu
sion/exclu
sion
criteria
specified—partially;
(iv)A
ge(y)—75±8.3for
both
grou
ps;
(v)S
ex—49
females
(60%
)and32
males
(40%
);(vi)Durationsin
cehip
fracture
orsurgery—
not
repo
rted;
(vii)
Com
orbiditie
srepo
rted—no
MHRgrou
p(i)
Nodescrip
tionprovided
forthe
nature
ofexercises.
(ii)A
verage
of4.6±2.2PT
visitsa
ndaverageo
f1.5±0.6commun
itynu
rse
visits.
Inpa
tient
grou
p(i)
Nodescrip
tionprovided
forthe
nature
ofexercises.
(ii)A
verage
stayin
rehabilitationho
spita
lwas
36.2±14.6days
with
daily
PTvisits.
PRO
Non
eused
PBO
Ambu
latory
capacity
Measuredacrossfive
categorie
s:commun
ityam
bulatory,hou
se-hold
ambu
latory,w
alking
onflat
surfa
ce,transferfrom
bed
tochair,bedto
chair
boun
d.(scorin
g:4=
independ
entw
ithou
taids,3
=independ
entw
ithaids,2
=ableto
walkwith
minim
umassistance/supervision
,1=
ableto
walkwith
maxim
umassistance,0=un
ableto
walk)
(i)Lo
stto
follo
wup
was
9in
theM
HRgrou
pand16
intheinp
atient
grou
p.Ca
uses
ofattrition
weren
otprovided.
(ii)A
dverse
eventsno
trepo
rted.
(iii)Com
mun
ityam
bulatory
abilitywas
bette
rintheM
HRgrou
p.Flat-le
velambu
latory
abilitywas
similarinbo
ththeg
roup
s.
Crotty
etal.[11]
Parallelgroup
rand
omized
controlledequivalencetria
l;MHRversus
NT
(i)𝑁=66(34in
theM
HR
grou
pand32
intheN
Tgrou
p;(ii)L
ocation—
Australia;
(iii)Inclu
sion/exclu
sion
criteria
specified—yes;
(iv)A
ge(y)—
median81.6
(IQR:
78.2,85.4)
inthe
MHRgrou
pandmedian
83.5(IQ
R:76.6–85.5)
inthe
NTgrou
p;(v)S
ex—21
females
(62%
)in
theM
HRgrou
pand24
females
(75%
)inNTgrou
p;(vi)Av
eraged
urationsin
cesurgery—
notreported;
(vii)
Com
orbiditie
srepo
rted—no
MHRgrou
p(i)
Hom
evisittoorganize
mod
ificatio
nsandinsta
llequipm
entp
riorto
discharge.
(ii)V
isitedby
therapists
(team
coordinator,PT
,OT,
SLP,SW
,and
therapyaid)
with
in48
hourso
fdischarge.
(iii)Frequencyof
therapy
was
tailo
redfor
individu
alized
needs.
Structured
practic
esessio
nsencouraged
betweenvisits.
(iv)S
ervicessuchas
podiatry,nursin
gcare
and
assistancew
ithlight
domestic
tasksw
ere
provided
asrequ
ired.
NTgrou
p:Re
ceived
routineh
ospital
care:inp
atient
services
and
thed
evelo
pmento
fcare
pathwaysa
nddischarge
planning
.
PRO
BalanceC
onfid
ence
ABC
Scale
Functio
nalStatus
(i)MBI
(ii)L
HS
HRQ
OL
(i)LH
S(ii)S
F-36
(PCS
andMCS
)PB
OBa
lance
BBS
Physica
lmobility
TUG
Falls
Frequencyof
falls
andfalls
thatrequ
ireho
spita
lization
(i)Attrition
orcauses
ofattrition
weren
otspecified.
(ii)A
dverse
eventsweren
otrepo
rted.
(iii)Patie
ntsintheM
HR
grou
pdidno
tsho
wim
provem
entinph
ysical
health
butreported
improvem
entinADL.
(iv)M
HRgrou
palso
had
greaterc
onfid
ence
inavoiding
falls
atfour
mon
ths.

Rehabilitation Research and Practice 5
Table1:Con
tinued.
Stud
yMetho
dParticipants
Interventio
nOutcomes
Results
Zidenet
al.[17]
Parallelgroup
rand
omized
controlledequivalencetria
l;MHRversus
NT
(i)𝑁=102(48in
MHR
grou
pand54
inNTgrou
p);
(ii)L
ocation—
Sweden;
(iii)Inclu
sion/exclu
sion
criteria
specified—yes
(iv)A
ge(y)—81.2±5.9in
MHRgrou
pand82.5±7.6
inNTgrou
p;(v)S
ex—29
females
(60.4%
)intheM
HRgrou
pand42
females
(77.8
%)in
theN
Tgrou
p;(vi)Com
orbiditie
srepo
rted—yes.
MHRgrou
p(i)
Threew
eeks
ofrehabilitationthatinclu
ded
PTto
encourage
self-effi
cacy
andOTto
encouragea
ctivity
and
independ
ence
inADL.
(ii)P
artic
ipantsreceived
ameanof
4.9(±0.4)
multip
rofessionalh
ome
visits;2.4PT
(±1.7
)and
1.6OT(±1.7
)visits.
(iii)Ev
eryfourth
patie
ntreceived
avisitb
yan
urse.
NTgrou
pNoadditio
naltreatment
after
beingdischarged
from
hospita
l.
PRO
BalanceC
onfid
ence
Swedish
versionof
theF
ES(S)
Functio
nalStatus
(i)FIM
motor
scale
(ii)Instrum
entalA
ctivity
Measure
(measuresd
egree
ofindepend
ence
ineight
advanced
activ
ities)
(iii)Frenchay’sAc
tivity
Index(determines
the
frequ
ency
ofperfo
rming
socialandcomplex
daily
activ
ities)
PBO
Physica
lMobility
TUG
Lowe
rExtremity
Strength
STStest
(i)Lo
stto
follo
wup
was
6in
theM
HRgrou
p;causes
ofattrition
werep
rovided.
(ii)N
oadversee
ventsw
ere
repo
rted
(iii)Th
eMHRgrou
pshow
edsig
nificant
improvem
entson
theF
ES,
TUG,STS
,FIM
,Instr
umentalA
ctivity
Measure,and
the
Frenchay’sAc
tivity
Index
onem
onth
after
discharge
comparedto
theN
Tgrou
p.
Zidenet
al.[18]
Parallelgroup
rand
omized
controlledequivalencetria
l;MHRversus
NT
(i)𝑁=102(48in
theM
HR
grou
p,54
intheN
Tgrou
p);
(ii)L
ocation—
Sweden;
(iii)Inclu
sion/exclu
sion
criteria
specified—partially;
(iv)A
ge(y)—81.2±5.9in
MHRgrou
pand82.5±7.6
inNTgrou
p;(v)S
ex—29
females
(60.4%
)intheM
HRgrou
pand42
females
(77.8
%)
females
intheN
Tgrou
p;(vi)Av
eraged
urationsin
cesurgery—
notreported;
(vii)
Com
orbiditie
srepo
rted—yes
MHRgrou
p(i)
Threew
eeks
ofrehabilitationthatinclu
ded
PTto
encourage
self-effi
cacy
andOTto
encouragea
ctivity
and
independ
ence
inADL.
(ii)M
edianof
visits4
.5(w
ithmedianof
3PT
visits
and1.5
OTvisits,11patie
nts
werev
isitedby
anurse).
NTgrou
pNoadditio
naltreatment
after
beingdischarged
from
hospita
l.
PRO
BalanceC
onfid
ence
FES(S)
Functio
nalStatus
(i)FIM
(ii)Instrum
entalA
ctivity
Measure
(iii)Frenchay’sAc
tivity
Index
HRQ
OL
SF-36
Mood
Centre
forE
pidemiological
Stud
iesD
epressionScale
(screening
instr
umentto
measure
depressiv
esymptom
s)PB
OPh
ysica
lMobility
TUG
Lowe
rExtremity
Strength
STS
(i)One
participantinthe
MHRgrou
pand3in
the
NTgrou
pwerelostat
6-mon
thfollo
wup
;additio
nal3
participantsin
theM
HRgrou
pand4
participantsin
theN
Tgrou
pwerelosttofollo
wup
at1-y
ear(reason
sfor
attrition
werep
rovided).
(ii)Th
eMHRgrou
phad
greaterb
alance
confi
dence
andph
ysicalfunctio
nthan
theN
Tgrou
pover
1year
perio
daft
erhipfracture.
(iii)One
year
after
discharge2
9%of
thep
eople
intheM
HRgrou
pconsidered
them
selves
fully
recovered,comparedto
only9%
intheN
Tgrou
p.

6 Rehabilitation Research and Practice
Table1:Con
tinued.
Stud
yMetho
dParticipants
Interventio
nOutcomes
Results
Crotty
etal.
[19]
Parallelgroup
rand
omized
controlledequivalencetria
l;MHRversus
NT
(i)𝑁=56(not
clear
abou
tho
wmanyin
each
grou
p);
(ii)L
ocation—
Australia;
(iii)Inclu
sion/exclu
sion
criteria
specified—yes
(iv)A
ge(y)—
meanof
81.8±7.2forb
othgrou
pscombined;
(v)S
ex—41
(73%
)fem
ales
forb
othgrou
pscombined;
(vi)Av
eraged
urationsin
cesurgery—
notreported;
(vii)
Com
orbiditie
srepo
rted—no
.
MHRgrou
p(i)
Hom
evisitsby
PT,O
T,SLP,SW
,and
therapyaides.
(ii)S
ervicessuchas
podiatry,nursin
gcare,and
assistancew
ithlight
domestic
tasksw
ere
provided
asrequ
ired.
NTgrou
p:Re
ceived
routineh
ospital
care,inp
atient
services,
developm
ento
fcare
pathways,anddischarge
planning
.
PRO
Functio
nalStatus
Mod
ified
BarthelInd
exHRQ
OL
SF-36(M
CS&PC
S)PB
OPh
ysica
lMobility
TUG
(i)Tenpatie
ntsu
navailable
for12-mon
thfollo
wup
(reasons
fora
ttrition
were
provided).
(ii)A
t12mon
ths,there
weren
odifferences
betweentheg
roup
sfor
scores
ontheM
BI,T
UG,or
SF-36ou
tcom
es(PCS
and
MCS
).
MHR:
multid
isciplin
aryho
merehabilitation;
IQR:
interquartile
range;NT:
notre
atment;PT
:physio
therapist;O
T:occupatio
naltherapist;
SLP:
speech
lang
uage
pathologist;SW:socialw
orker;ADL:
activ
ities
ofdaily
living;PR
O:patient-reportedou
tcom
e;PB
O:perform
ance-based
outcom
es;A
BC:activity
-specific
balancec
onfid
ence
scale;MBI:M
odified
BarthelInd
ex;LHS:Lo
ndon
HandicapScale;SF-36:Sh
ort-F
orm-
36;P
CS:physic
alcompo
nent
summary;MCS
:mentalcom
ponent
summary;BB
S:Be
rgbalances
cale;T
UG:tim
edup
andgo
test;
FES:falls
efficacy
scale;FIM:fun
ctionalind
ependent
measure;STS
:sit-to-stand
.

Rehabilitation Research and Practice 7
Table 2: Risk of bias assessment of included studies (Yes—No risk of bias, No—clear risk of bias, Unclear—indicates that risk of bias isunclear).
Random sequencegeneration
(selection bias)
Allocationconcealment(selection bias)
Blinding of outcomeassessment (detection
bias)
Incompleteoutcome data(attrition bias)
Selectivereporting
(reporting bias)Crotty et al. 2002 [11] Yes Unclear Yes Unclear YesCrotty et al. 2003 [19] Yes Yes Yes Yes YesKuisma 2002 [20] Unclear Yes Yes No NoZiden et al. 2008 [17] Unclear Yes No Yes YesZiden et al. 2010 [18] Unclear Yes No Yes Yes
overall risk of bias was low in one study [19], unclear in threestudies [11, 17, 18], and high in one study [20].
3.4. Effects of Interventions. After comparing the results ofoutcomes reported either on the same scale or across differentscales that measure the same construct, it was determinedthat pooling the results was not possible or appropriate.Therefore, a narrative summary of results was provided forshort- and long-term time frames. The study by Kuisma [20]is being excluded from the following summary of results dueto high risk of bias and lack of reporting of outcomes ofinterest.
3.4.1. Patient Reported Balance Confidence. The effect ofMHR on balance confidence over short-term was inconsis-tent across two studies [11, 17]. Crotty et al. [11] assessedbalance confidence using the Activity Specific Balance Con-fidence (ABC) Scale and the FES. No significant differenceswere reported between the MHR group and the NT groupon the ABC scale at 4 months (MHR median: 61.3, IQR:45.5, 75.2; NT median: 53.3, IQR: 26.8, 74.6; 𝑃 > 0.05);significant improvements in the FES scores were reported(MHR median: 90.5, IQR: 80.5, 98.0; NT median: 79.5, IQR:40.0, 92.5; 𝑃 < 0.05). Ziden et al. [17] measured patientreported balance confidence using the FES and found that theindividuals in MHR group had increased balance confidencecompared to those of the NT group at one-month followup(MHRmean (SD): 30.6 (19.3), NTmean (SD): 13.5 (20.9), and𝑃 = 0.0004).
Only Ziden et al. [18] measured patient reported balanceconfidence using the FES in the long-term (1 year afterdischarge). The FES scores indicated significantly higherbalance confidence inMHRgroup compared to theNTgroup(MHR median (min-max): 128 (61–130); NT median (min-max): 102 (13–130); 𝑃 < 0.001).
3.4.2. Patient Reported Functional Status. The effect of MHRon functional status over short-term was also inconsistentacross two studies [11, 17]. Crotty et al. [11] found no differencein functional status between theMHR and theNT groups at 4months as measured by the London Handicap scores (MHRmedian: 0.70, IQR: 0.63,0.77; NT median: 0.65, IQR: 0.58,0.73; 𝑃 > 0.05). Ziden et al. [17] measured patient reportedfunctional status using Frenchay’s Activity (FAI). The resultsindicated that the scores on the FAI domestic activities
subscale were significantly higher in the MHR group (MHRmean (SD): 9.0 (5.0); NT mean (SD): 6.4 (5.3); 𝑃 = 0.0119).Similarly, the scores on the outdoor activities subscale werealso significantly higher in theMHRgroup (MHRmean (SD):5.7 (4.8); NT mean (SD): 2.7 (3.8); 𝑃 = 0.0007). However, thescores on the leisure and work activity subscale did not differbetween the groups at the one-month followup (MHR mean(SD): 3.4 (2.3); NT mean (SD): 2.6 (2.3); 𝑃 = 0.1057).
3.4.3. Patient Reported Functional Status (Long-Term). Zidenet al. [18] evaluated functional status using the FAI in thelong-term (1 year after discharge). Significantly higher scoresin favour of the MHR group were found (𝑃 = 0.028) at 12months (MHR median: (min-max), 27 (0–40); NT median:(min-max) 20 (0–42)).
3.4.4. Patient Reported QOL (Short-Term). Crotty et al. [11]evaluatedQOL at 4months using the LondonHandicap Scaleand the SF-36 and found no significant differences betweengroups. (London Handicap Scale (MHRmean (95% CI): 0.70(0.63–0.77), NT mean (95% CI): 0.65 (0.58–0.73); SF-36 onboth the PCS component (NT mean (95% CI): 26.9 (10.2–42.0), MHR mean (95% CI): 38.3 (27.9–48.7), 𝑃 > 0.05) andthe MCS component (NT mean (95% CI): 42.8 (31.2–54.4);MHR mean (95% CI): 46.4 (36.2–56.6); 𝑃 > 0.05).
Crotty et al. [19] and Ziden et al. [18] evaluated QOL overa longer term using SF-36. The effect of MHR on QOL wasinconsistent across both studies. Crotty et al. [19] found nosignificant differences between groups on the SF-36 for boththe PCS component (mean difference (95% CI): −2.3(−7.6–3.0), 𝑃 = 0.386) and the MCS component (mean difference(95%CI): 0.7 (−3.8–5.3);𝑃 = 0.733). Ziden et al. [18] reporteda significant improvement in the SF-36 domains of physicalfunctioning (𝑃 = 0.001) and bodily pain (𝑃 = 0.042) in theMHR group at one-year followup.
3.4.5. Mobility. The effect of MHR on mobility as assessedby the timed up and go (TUG) over a short-term periodwas inconsistent across two studies [11, 17]. Crotty et al. [11]found no significant difference in TUG scores at four monthsbetween the MHR and the NT groups (MHR median: 23.0,IQR: 15.3, 33.0; NTmedian: 28.0, IQR: 18.0, 42.5). In contrast,Ziden et al. [17] found significant differences in the TUGscores in favor of the MHR group compared to the NT group

8 Rehabilitation Research and Practice
at one month (MRR mean (SD): 24.9 (15.4); NT mean (SD):30.8 (6.0); 𝑃 = 0.0139).
3.4.6. Mobility (Long-Term). Similar to the short-term fol-lowup, the effect of MHR onmobility as assessed by the TUGwas also inconsistent across two studies [18, 19]. Crotty etal. [19] found that the median difference between the TUGscores of the MHR and the NT groups at 12 months was notsignificant (median difference (95% CI): −3.0 (−11.0 to 3.0);𝑃 = 0.314), while Ziden et al. [18] reported that TUG scoresin the MHR group were significantly better than NT group(𝑃 = 0.005) at 12 months.
3.4.7. Lower Extremity Functional Strength (Short-Term andLong-Term). Ziden et al. [17] found that lower extremitystrength assessed by the Sit-to-Stand (STS) test was signifi-cantly better the MHR group (𝑃 = 0.011) in comparison tothe NT group in. This improvement was sustained over the12-month followup as well and the MHR group continued toshow significantly better lower extremity strength comparedto the NT group (𝑃 < 0.001) [18].
3.4.8. Balance (Short-Term). The balance was assessed atfour-months followup using the Berg Balance Scale in onlyone study [11]. The result indicated that the MHR group hadhigher scores indicating greater improvement compared tothe NT group at four months; however the difference was notsignificant (MHR median: 43.5, IQR: 34.3, 52.5; NT median:37.5 IQR: 26.3, 45.3; 𝑃 > 0.05).
3.4.9. Adverse Events. No adverse effects of the MHR groupwere reported in any of the studies reviewed [11, 17–19].
4. Discussion
In the short-term, the MHR group showed greater improve-ments in functional status and lower extremity strengthbut no difference in balance and HRQOL compared to theNT group. The effect of MHR on balance confidence andmobility was inconsistent across the studies, and thereforeno inferences can be made whether MHR is effective inimproving these outcomes.
In the long-term, the MHR group showed greaterimprovements in balance confidence, functional status, andlower extremity muscle strength compared to NT group.Theeffect of MHR on HRQOL and mobility was inconsistentacross the studies.
The studies evaluated within this review suggest a trendtowards positive outcomes from MHR program of carecompared to no treatment following hip fracture surgery.Due to the low number of studies that fit the criteria for thisreview, robust conclusions cannot be made. Meta-analysisallows combining data across many studies and enables toderive “pooled” effect.However, the lack of consistency acrossoutcome measures used in the studies limited our ability toperform meta-analysis. Furthermore, applying the evidenceincluded in this review will be difficult, as the studies did notprovide clear descriptions of the interventions administered.
Thoughwe realize that itmay be unrealistic to provide explicitprotocols, as treatment in a MHR setting will naturally varybetween geographical areas, at least a detailed informationregarding the specific roles of health care providers involvedin the MHR plan would have been useful.
Althoughwe only included the studies that reflect the bestevidence into this review by deciding, a priori, to limit oursearch to RCTs alone, the quality of the included studies waslimited both by risk of bias and methodological issues. Someof the keymethodological issues observed across the includedstudies such as unclear in reporting methods of randomsequence generation, lack of blinding of outcome assessment,and incomplete outcome data reporting can highly influencethe results. Furthermore, many of these studies did notadequately describe the MHR provided, which further limitsthe generalizability of the results.Therefore, the results of thisreview do not allow us to make robust conclusions regardingthe usefulness of the MHR following hip fracture surgery incomparison to no treatment.
A comprehensive search strategy performed in duplica-tion, an assessment of agreement for selection of studies, andrisk of bias assessment for included studies all contributed tothe strength of this review. Criteria for inclusion/exclusion ofstudies were determined a priori and two reviewers extracteddata from the studies using a previously developed andstandardized data extraction form.
The comprehensive search strategies utilized in thisreview helped to minimize potential bias in the reviewprocess. Having two reviewers independently performingliterature searche on a multitude of databases helped toensure that all relevant articles were located and includedin this review. However, outside of the reviewer’s control,publication bias may still have influenced our outcomes.Although we set out to locate all studies on the topic ofinterest, it is possible that unpublished studies exist that mayor may not have changed the results of our review.
In the study selection and data collection processes,we again minimized bias by performing these processes induplicate. In the end there was some disagreement amongstreviewers as to which studies to include in the review and onthe quality of included studies. Although this was resolvedthrough discussion amongst all reviewers, it is possible thatthe subjectivity of this processmay have introduced somebiasinto the review.
Lastly, studies did not clearly report details of the treat-ment delivered to the MHR group. Therefore, it is possiblethat the treatments varied in terms of content, duration,and frequency among the MHR groups across studies. Wedid not account for this variation when determining thetreatment effect of MHR after hip fracture surgery. This mayhave introduced bias into the review, however we determinedthat the variation amongst home-based treatments could beoverlooked as this is likely a realistic representation of theapproach taken to home-based treatments in the community.
This systematic review expands on our systematic reviewby Mehta and Roy [22], which concluded that home-basedphysiotherapy was effective in improving patient reportedhealth related QOL following hip fracture surgery. Theoutcomes investigated in this review were different from

Rehabilitation Research and Practice 9
those of other similar reviews that assessed outcomes suchas mortality or admission to long-term care homes [23, 24].Moreover, the objective of our review was different in that itcompared multidisciplinary rehabilitation provided in homeversus that provided in institution as well as no treatmentfollowing discharge from acute hospital setting. However, ourresults agree with those of Handoll et al. [8] who suggestedthat multidisciplinary rehabilitation may have some benefitto patients following hip fracture but emphasized the need forhigh quality RCT to comprehensively examine the benefits ofmultidisciplinary rehabilitation.
5. Conclusions
Our findings show a trend to support MHR compared toNT following hip fracture surgery. In all instances, MHRwas found to be at least as effective as, if not more than,NT. However, no conclusive directives can be made to adoptMHR following hip fracture surgery due to risk of biasacross included studies and insufficient details regarding thecomponents of the MHR in the studies. The poor method-ological quality of studies included in this review underscoresthe need to conduct studies with superior methodologicalquality to investigate the effects of MHR in comparison withNT or institution-based care (inpatient or outpatient) inindividuals with hip fracture surgery. Furthermore, futurestudies can accurately characterize the types of disciplinesinvolved in MHR and frequency and dosage of intervention.Moreover, researchers involved in assessing the outcomes ofhip fracture surgery can develop a core set of measures fordifferent constructs (e.g. functional status, balance) relevantto hip fracture population. This will facilitate use of similarmeasures across future studies allowing meta-analysis andassessment of pooled effect of an intervention in individualswith hip fracture. Lastly, a cost analysis comparing NT orinstitution-based rehabilitation to home-based is necessary toascertain the cost benefits of each mode of treatment.
Acknowledgments
The authors report no conflict of interests. The authors aloneare responsible for the content and writing of the paper.Authors Donohue, Hoevenaars, McEachern, and Zemanwere enrolled in the entry-level Physical Therapy programat McMaster University (M.S. (PT)) while performing thissystematic review. This review was part of their Research &Evidence Based Practice (REBP) Project which they com-pleted under the mentorship of Saurabh Mehta.
References
[1] H. H. Handoll, C. Sherrington, and J. C. Mak, “Interventionsfor improving mobility after hip fracture surgery in adults,”Cochrane Database of Systematic Reviews, no. 3, Article IDCD001704, 2011.
[2] S. Kaffashian, P. Raina, M. Oremus et al., “The burden of osteo-porotic fractures beyond acute care: the Canadian MulticentreOsteoporosis Study (CaMos),”Age and Ageing, vol. 40, no. 5, pp.602–607, 2011.
[3] W. D. Leslie, C. J. Metge, M. Azimaee et al., “Direct costs offractures in Canada and trends 1996–2006: a population-basedcost-of-illness analysis,” Journal of Bone and Mineral Research,vol. 26, no. 10, pp. 2419–2429, 2011.
[4] M. Crotty, K. Unroe, I. D. Cameron, M. Miller, G. Ramirez,and L. Couzner, “Rehabilitation interventions for improvingphysical and psychosocial functioning after hip fracture in olderpeople,” Cochrane Database of Systematic Reviews, no. 1, ArticleID CD007624, 2010.
[5] M.-H. Chiu, H.-F. Hwang, H.-D. Lee, D.-K. Chien, C.-Y. Chen,andM.-R. Lin, “Effect of fracture type on health-related qualityof life among older women in Taiwan,” Archives of PhysicalMedicine and Rehabilitation, vol. 93, no. 3, pp. 512–519, 2012.
[6] J. Visschedijk, B. R. van, C. Hertogh, and W. Achterberg,“Fear of falling in patients with hip fractures: prevalence andrelated psychological factors,” Journal of the American MedicalDirectors Association, vol. 14, no. 3, pp. 218–220, 2013.
[7] R. Milte, J. Ratcliffe, M. Miller, C. Whitehead, I. D. Cameron,and M. Crotty, “What are frail older people prepared to endureto achieve improvedmobility following hip fracture? ADiscreteChoice Experiment,” Journal of Rehabilitation Medicine, vol. 45,no. 1, pp. 81–86, 2013.
[8] H. H. Handoll, I. D. Cameron, J. C. Mak, and T. P. Finnegan,“Multidisciplinary rehabilitation for older people with hipfractures,” Cochrane Database of Systematic Reviews, no. 4,Article ID CD007125, 2009.
[9] A. M. Momsen, J. O. Rasmussen, C. V. Nielsen, M. D. Iversen,and H. Lund, “Multidisciplinary team care in rehabilitation: anoverview of reviews,” Journal of RehabilitationMedicine, vol. 44,no. 11, pp. 901–912, 2012.
[10] I. D. Cameron, “Coordinated multidisciplinary rehabilitationafter hip fracture,” Disability and Rehabilitation, vol. 27, no. 18-19, pp. 1081–1090, 2005.
[11] M. Crotty, C. H. Whitehead, S. Gray, and P. M. Finucane,“Early discharge and home rehabilitation after hip fractureachieves functional improvements: a randomized controlledtrial,” Clinical Rehabilitation, vol. 16, no. 4, pp. 406–413, 2002.
[12] J.-Y. Tsauo, W.-S. Leu, Y.-T. Chen, and R.-S. Yang, “Effectson function and quality of life of postoperative home-basedphysical therapy for patients with hip fracture,” Archives ofPhysical Medicine and Rehabilitation, vol. 86, no. 10, pp. 1953–1957, 2005.
[13] J. P. T. Higgins and D. G. Altman, “Assessing risk of bias inincluded studies,” inCochrane Handbook for Systematic Reviewsof Interventions Version 5.0.1, J. P. T. Higgins and S. Green, Eds.,chapter 8, The Cochrane Collaboration, 2008.
[14] J. J. Deeks, J. P. T. Higgins, and D. G. Altman, “Analysing dataand undertaking meta-analyses,” in Cochrane Handbook forSystematic Reviews of Interventions Version 5.0.1, J. P. T. Higginsand S. Green, Eds., chapter 9, The Cochrane Collaboration,2008.
[15] J. A. C. Sterne, M. Egger, and D. Moher, “Addressing reportingbiases,” in Cochrane Handbook for Systematic Reviews of Inter-vention. Version 5.0.1, J. P. T. Higgins and S. Green, Eds., chapter10, The Cochrane Collaboration, 2008.
[16] J. R. Landis and G. G. Koch, “The measurement of observeragreement for categorical data,” Biometrics, vol. 33, no. 1, pp.159–174, 1977.
[17] L. Ziden, K. Frandin, and M. Kreuter, “Home rehabilitationafter hip fracture. A randomized controlled study on balanceconfidence, physical function and everyday activities,” ClinicalRehabilitation, vol. 22, no. 12, pp. 1019–1033, 2008.

10 Rehabilitation Research and Practice
[18] L. Ziden, M. Kreuter, and K. Franndin, “Long-term effectsof home rehabilitation after hip fracture—1-year follow-up offunctioning, balance confidence, and health-related quality oflife in elderly people,” Disability and Rehabilitation, vol. 32, no.1, pp. 18–32, 2010.
[19] M. Crotty, C. Whitehead, M. Miller, and S. Gray, “Patient andcaregiver outcomes 12 months after home-based therapy forhip fracture: a randomized controlled trial,” Archives of PhysicalMedicine and Rehabilitation, vol. 84, no. 8, pp. 1237–1239, 2003.
[20] R. Kuisma, “A randomized, controlled comparison of homeversus institutional rehabilitation of patients with hip fracture,”Clinical Rehabilitation, vol. 16, no. 5, pp. 553–561, 2002.
[21] M. Y. Tseng, Y. I. Shyu, and J. Liang, “Functional recovery ofolder hip-fracture patients after interdisciplinary interventionfollows three distinct trajectories,” Gerontologist, vol. 52, no. 6,pp. 833–842, 2012.
[22] S. P. Mehta and J.-S. Roy, “Systematic review of home phys-iotherapy after hip fracture surgery,” Journal of RehabilitationMedicine, vol. 43, no. 6, pp. 477–480, 2011.
[23] J. Halbert, M. Crotty, C. Whitehead et al., “Multi-disciplinaryrehabilitation after hip fracture is associatedwith improved out-come: a systematic review,” Journal of Rehabilitation Medicine,vol. 39, no. 7, pp. 507–512, 2007.
[24] S. Bachmann, C. Finger, A. Huss, M. Egger, A. E. Stuck, and K.M. Clough-Gorr, “Inpatient rehabilitation specifically designedfor geriatric patients: systematic review and meta-analysis ofrandomised controlled trials,” British Medical Journal, vol. 340,article c1718, 2010.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com