review article amiodarone-induced cirrhosis of...
TRANSCRIPT

Hindawi Publishing CorporationISRN CardiologyVolume 2013, Article ID 617943, 14 pageshttp://dx.doi.org/10.1155/2013/617943
Review ArticleAmiodarone-Induced Cirrhosis of Liver:What Predicts Mortality?
Nasir Hussain, Anirban Bhattacharyya, and Suartcha Prueksaritanond
Department of Internal Medicine, Saint Joseph Hospital, Resurrection Health Care, 2900 North Lake Shore Drive,Chicago, IL 60657, USA
Correspondence should be addressed to Nasir Hussain; [email protected]
Received 18 January 2013; Accepted 11 February 2013
Academic Editors: A. Bobik, C. Hassager, and B. Strasberg
Copyright © 2013 Nasir Hussain et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction. Amiodarone has been used for more than 5 decades for the treatment of various tachyarrhythmias and previouslyfor the treatment of refractory angina. There are multiple well-established side effects of amiodarone. However, amiodarone-induced cirrhosis (AIC) of liver is an underrecognized complication.Methods. A systematic search of Medline from January 1970to November 2012 by using the following terms, amiodarone and cirrhosis, identified 37 reported cases of which 30 were used inthis analysis. Patients were divided into 2 subsets, survivors versus nonsurvivors, at 5 months. Results. Aspartate aminotransferasewas significantly lower (𝑃 = 0.03) in patients who survived at 5-months (mean 103.33 IU/L) compared to nonsurvivors (mean216.88 IU/L).There was no statistical difference in the levels of prothrombin time, total bilirubin, alanine aminotransferase, alkalinephosphatase, gamma-glutamyl transpeptidase, cumulative dose, and latency period between the two groups. The prevalence ofDM, HTN, HLD, CAD, and CHF was similar in the two groups. None of the above-mentioned variables could be identified as apredictor of survival at 5 months. Conclusion. AIC carries a mortality risk of 60% at 5 months once the diagnosis is established.Further prospective studies are needed to identify predictors of AIC and of mortality or survival in cases of AIC.
1. Introduction
Amiodarone has been used since the 1960s for the manage-ment of various tachyarrhythmias and in the past for refrac-tory angina.There are multiple reported and well-establishedside effects of amiodarone therapy such as effects on the thy-roid, skin, lungs, nerves, and cornea.
The effect of amiodarone on the liver resulting in hepato-toxicity is a recognized complication of amiodarone, but thishepatotoxicity leading to cirrhosis of the liver is unfortunatelyan underrecognized side effect. Little has been written onamiodarone-induced cirrhosis (AIC) of the liver due to itsrarity [1–4]. The purpose of this paper is to review what weknow so far about AIC of the liver.
2. Materials and Methods
2.1. Selection of Studies. A systematic search of Medlinefrom January 1970 to November 2012 by using the following
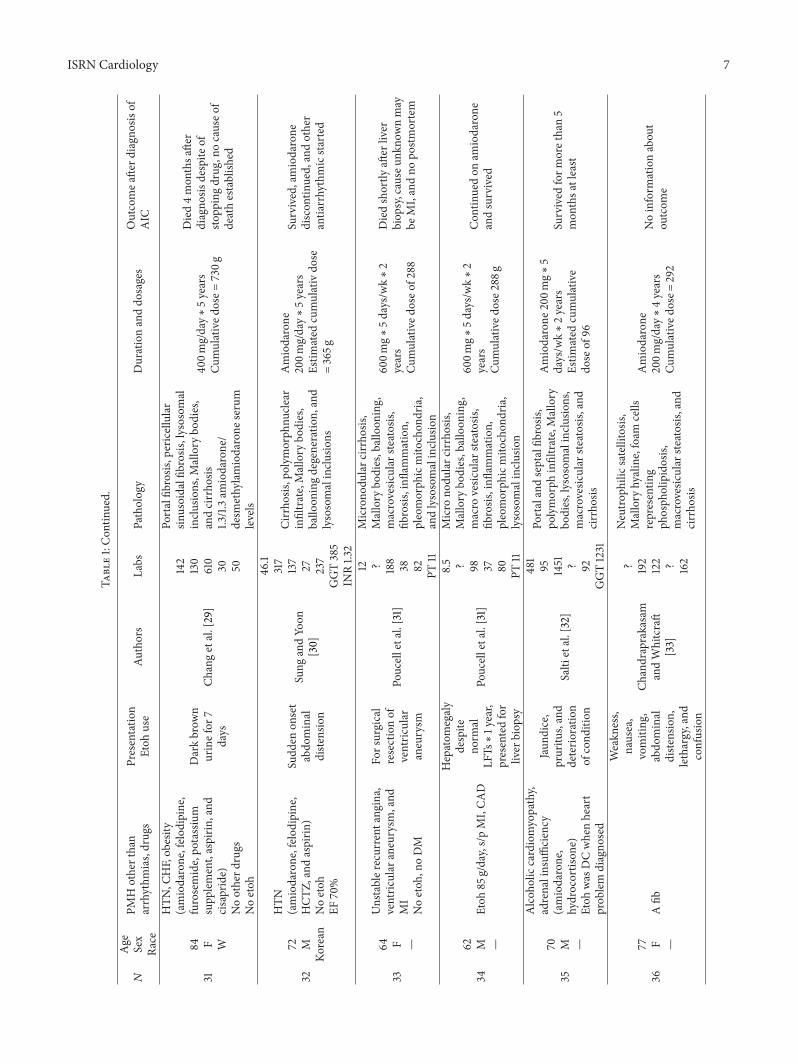
terms, amiodarone and cirrhosis, was performed; 37 reportedcases were identified (Table 1) of which 30 were used inthis analysis. We also searched the reference lists of allreported cases to identify citations that were not identifiedduring the initial search. Data that were extracted for eachpatient included age, gender, latency period in years, whether≥200mg/day amiodarone dosage was used (it is thoughtthat low-dose amiodarone has lesser side effects), cumulativedose, presence or absence of hypertension (HTN), dia-betes (DM), hyperlipidemia (HLD), coronary artery disease(CAD), congestive heart failure (CHF), values of bilirubin,aspartate transaminase (AST), alkaline phosphatase (ALKP), albumin, alanine transaminase (ALT), and prothrombintime. The outcomes in terms of survival or mortality at5 months were used. This specific timeline was selectedbecause more than 50% of patients in these case reportsdied within 5 months after the diagnosis was established.Not all of the studies we found had all these data; however,they were included if the outcome was provided. In some

2 ISRN Cardiology
Table1
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
163 M W
CADs/pCA
BG,D
M,
HLD
,Noetoh
,(amiodarone,w
arfarin
,aspirin
,rosiglitazon
e,and
lovastatin)
Nootherh
epatotoxicdrugs
Abdo
minal
diste
nsion
Pulietal.[2]
23.94
114 ? 23 82
Microno
dularc
irrho
sis,
bridging
fibrosis
,lym
phocytic
infiltrate,macroph
ages,
plasmac
ells,
microvesic
ular
steatosis,
andlysosomal
bodies
onele
ctron
microscop
y
600m
g/dayfor10days,
then
200m
g/dayfor2
2.5
mon
thsc
umulatived
oseo
fapprox.141
g
Survived
281 F —
Digito
xin,
alph
amethyldop
aNoDM,and
noetoh
Cirrho
sisdiagno
sed
durin
gstu
dyGuigu
ietal.[3]
15,28
186,
?,53
GGT151,
PT76%
Portalfib
rosis
,steatosis,
PMN,m
yelin
figures,dense
depo
sits,andcirrho
sis
120mon
ths,cumulative
dosage
of520g
Cou
ldno
testa
blish
anou
tcom
e
372 M W
DM,H
TN,and
CKD
Noetoh
,(am
iodarone,
simvastatin,and
glipizide)
Ascitesa
ndfatig
ueAtiq
etal.[5]
32.49,106,
147,?,75,
PT20
Steatohepatitis,
Mallory
hyaline,neutroph
ilic
infiltrate,andcirrho
sis
200P
Omg/day∗
3years
Cumulatived
oseo
fapp
rox.
219g
Dieddu
ringthes
ame
admissiondu
eto
complicationof
liver
disease
467 F AA
CAD,C
HF,ands/pAICD
Noetoh
Con
fusio
nAtiq
etal.[5]
? 377
551 ? 277
PT12.7
Mallory
hyaline,neutroph
ilinfiltrate,
peric
ellular/bridging
fibrosis
,anddegeneratin
ghepatocytes
(cirr
hosis
foun
don
autopsy)
Lowdo
se∗2years
Died2weeks
after
the
workup
dueto
cardiopu
lmon
aryfailu
re
563 M —
COPD
,DM,and
hypo
thyroidism
(digoxin,furosem
ide,and
thyroxin)
Abno
rmal
LFTs
onscreening
Rigase
tal.[6]
? 59 207 ? 28
Portal,central,and
sinusoidal
fibrosis
andlossof
lobu
lar
architecturea
ndregenerativ
eno
dules,centralveinsclerosis
,Mallory
bodies,lysosom
alinclu
sion,
andcirrho
sis
400m
g/day
Amiodarone∗18
mon
ths
Cumulatived
ose2
16
Noinform
ationabou
tthe
outcom
e
673 M —
Heartfailu
re,nosig
nificant
etoh
,com
pleter
ight
and
leftanterio
rhem
iblock
(transla
tedthroug
hGoo
gle)
Jaun
dice,
hepatomegaly
Capron
-Chivrac
etal.[7]
269
55 708
68 ? 224
GGT781
Portal,periportalfi
brosis,
mixed
inflammatoryinfiltrate,
ductalproliferatio
n,lysosomalinclu
sions,no
Mallory
bodies,and
cirrho
sis
Amiodarone
100m
g/day∗
5days/w
k∗2
mon
ths
Cumulatived
oseo
f4g
“Wes
trong
lysuspectinthis
case
cirrho
sismay
have
been
duetosomeo
ther
cause”
Died2mon
thsa
fter
stopp
ingam
iodarone,died
ofpu
lmon
aryedem
a
770 F —
—Weightloo
sandblurred
visio
n
Chaabane
etal.
[8]
—Microno
dularc
irrho
sis,
steatoh
epatitis
200m
g/day∗
15years
Cumulatived
oseo
fapp
rox.
1095
g
Cou
ldno
testa
blish
anou
tcom
e

ISRN Cardiology 3
Table1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
862 M —
CAD,H
TN,C
HF,
emph
ysem
a,pu
lmon
ary
HTN
,HLD
,renal
insufficiency,m
igraine,
ulcerativ
ecolitis,
cholelithiasis,and
noetoh
Progressive
weakn
ess,
abdo
minal
discom
fort,
andjaun
dice
Ano
nymou
s[9]
51.3
734
119 29 781
PT12.4
Microno
dularc
irrho
siswith
ballo
oningdegeneratio
nof
hepatocytesa
ndMallory
bodies,som
esteatosis
150–
1000
mg/day,averaging
400m
g/day∗
8.5years
Cumulatived
oseo
fapp
rox.
1241
g
Died2weeks
after
stopp
ing
medicine,prob
ablyhepatic
enceph
alop
athy
973 M —
Obesity,mod
eratea
lcoh
olintake
Fatig
ue,
weakn
ess
Ano
nymou
s[9]
34.2 ? 115 ? 67
Mallory
bodies,m
inim
alfatty
change,and
cirrho
sis
Amiodarone
300m
g/day∗
approx.6
mon
ths
Cumulatived
oseo
fapp
rox.
55g
Survived
form
orethan3
years
1064 M —
Gou
t,CA
D,and
renal
failu
resecond
aryto
lead
intoxicatio
n,MI,
pulm
onaryedem
a,and
sylvianmicroem
bolism
(digoxin,w
arfarin
,diclo
fenac,am
iodarone,
andallopu
rinol)
Fatig
ue,
weightloss,
1-2alcoho
licbeverageso
nsocial
occasio
ns
Richer
andRo
bert
[10]
12 149
176 ? 112
INR2.4
GGT277
Ballo
oned
hepatocytes,
Mallory
bodies,fibrosis,
phosph
olipidosis,
inflammatoryinfiltrate,and
cirrho
sis
2.8g∗4days,then
amiodarone
400m
g–60
0/day∗
13mon
ths,
cumulatived
oseo
fapp
rox.
206g
Died69
days
after
cessation
oftherapy,du
eto
hepatorenalsyn
drom
e
1174 M —
Ischem
icheartd
isease,
CVA,poliomyelitis,
carotid
endarterectomy,and
perip
heraln
europathy
Etoh
Con
sumption=negligible
Muscle
weakn
ess,
hepatomegaly
Gilinsky
etal.[11]
133.4
110 275 16 231
PT17
Fibrosis,
Mallory
hyaline,
lysosomalinclu
sions,
amiodarone,and
desm
ethylamiodarone
conc.
0.6,0.5m
g/L,respectiv
ely
Amiodarone
300–
600m
g/day∗
28mon
ths
Cumulatived
oseo
fapp
rox.
378g
Dieddespite
discon
tinuatio
nof
therapy,
prob
ablyliver
failu
re
1276 F —
Nosig
nificantp
asth
istory
otherthanrecurrentS
VTs
Abdo
minal
pain,
anorexia,and
wastin
g
Tordjm
anetal.
[12]
n 225
317 29 ?
Mallory
bodies,fibrosis,
severelydamaged
hepatocytes,biledu
ctproliferatio
n,andcirrho
sis
200m
gdaily∗5years
Cumulatived
oseo
dapprox.365
g
Died2weeks
after
evaluatio
ndu
etohepatic
enceph
alop
athy
1377 F —
—
Ano
rexia,
abdo
minal
pain,and
malaise
Rene
etal.[13]
20.52
,16
324,39
10,
GGT66
PT70%
Microno
dularc
irrho
sis,
centraland
perip
ortalfi
brosis,
andprob
able
phosph
olipidosis
400m
g/day∗
9years
Cumulatived
oseo
fapp
rox.
1314g
Outcomec
ould
notb
edeterm
ined

4 ISRN CardiologyTa
ble1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
1479 M —
CADs/pCA
BG,H
LDhypo
thyroidism
,and
s/p
pacemaker
(amiodarone,A
SA,
furosemide,atorvastatin,
andranitid
ine)
<2un
itsetoh
/mon
thNoherbalmedicines
Upp
erGI
bleed,
lethargy∗2
mon
ths
Sing
haletal.[14
]
14 67 216 27
GGT44
3
PMNinfiltrate,redu
plicating
biledu
ctsinhepatic
nodu
les,
degeneratin
ghepatocytes,
Mallory
bodies,extensiv
efib
rosis,and
cirrho
sis
200PO
mg/
day∗
33mon
ths
Cumulatived
oseo
fapp
rox.
198g
Died3mon
thsa
fter
diagno
sisdespite
ofsto
pping
amiodarone
duetoheart
andrenalfailure
and
hepatic
enceph
alop
athy
1575 F —
s/pMI,leftventric
ular
aneurysm
,and
norm
alcoronarie
s
Abno
rmal
LFTs —
Bach
etal.[15]
? 140
850 ? ?
Microno
dularc
irrho
sis,
portalfib
rosis
,Mallory
bodies,balloon
ing
hepatocytes,
phosph
olipidosis,
inflammatorycells,and
lysosomalinclu
sions
800m
g/day∗
7mon
ths,
then
600m
g/day∗
24mon
ths,then
200m
g/day
for3
mon
ths
Cumulatived
oseo
fapp
rox.
624g
Survived
form
orethan3
years
1663 F —
Mitralvalves
teno
siss/p
replacem
ent5
yearsa
go,
mod
erateT
R,no
obesity,
andno
diabetes
(amiodarone,cou
madin
deriv
ative)
Asthenia,
anorexia,and
weightlosso
f8kg
for5
mon
ths
Martin
ezetal.
[16]
18.8
198
301
35 86,
GGT475
PT20%
Postmortem
liver
biop
syshow
edincipientcirr
hosis,
portalfib
rosis
,infl
ammatory
ductalinfiltrationandmixed
leuk
ocyticinfiltration,
steatosis,
Mallory
bodies,and
acidop
hilic
change
400mgdaily∗5d
ays/week,
duratio
nno
tspecified,may
be>12
years
Cumulatived
oseo
fapp
rox.
>1152
g
Dieddu
etomassiv
eupp
erGIb
leed
durin
gsame
admission
1758 M —
CAD,M
I(amiodarone,aspirin,
furosemide,diltiazem
,iso
sorbided
initrate,
digoxin,
famotidine)
Noetoh
,noherbsu
sed
Abdo
minal
diste
nsion
andfatig
ue
Cobanetal.
[17]
? 64 ? 11 ?PT
16.9
GGT133
Polymorph
nucle
arinfiltrate,
ductalproliferatio
n,fib
rosis
,bridging
necrosis,
vacuolar
degeneratio
n,lysosomal
inclu
sions
(73+
),andcirrho
sis
200m
gdaily∗1y
ear,
stopp
eddu
etosid
eeffects,
resta
rted
200m
gdaily∗6
years
Cumulatived
oseo
fapp
rox.
511g
Died3mon
thsa
fter
diagno
sisdu
eto
hepatorenalsyn
drom
eand
hepatic
enceph
alop
athy
1885 M —
Ischem
icheartd
isease
Noob
esity,noetoh
,and
noDM
Cardiac
congestio
nOikaw
aetal.[18]
20.52 81 452 ? 35
GGT210
PT59%
Polymorph
nucle
arinfiltrate,
ductalproliferatio
n,fib
rosis
,micro/m
acrovesic
ular
steatosis,
lysosomal
inclu
sions,and
cirrho
sis(cum
ulatived
oseg
iven
byauthor
=528)
400m
gdaily∗17
days,then
200m
gdaily
for8
4mon
ths
Cumulatived
oseo
fapp
rox.
518g
Died5mon
thsa
fter
diagno
sisdu
etorenal
failu
reandpn
eumon
ia
1949 M —
Rheumaticheartd
isease,
endo
carditis,HTN
,and
DM
(amiodarone,acebu
tolol,
andglibencla
mide)
Pain
inRU
Qandfever
Lamproyee
tal.
[19]
n n n n∗
5ULN
PTn
Microno
dularc
irrho
sis,
portalfib
rosis
,leuko
cytic
infiltrates,M
allory
bodies,
micro
andmacrovesic
ular
steatosis
400m
g/day∗
5days
aweek∗
12years
Cumulatived
oseo
fapp
rox.
1152
Noou
tcom
egiven

ISRN Cardiology 5
Table1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
2056 F —
s/ppacemaker,goiter
NoDM,noob
esity,and
noetoh
abuse
(digoxin,aceno
coum
arin,
andam
iodarone
)
—Ba
bany
etal.[20]
15 38 73 ? 63PT
100%
Microno
dularc
irrho
sis,
markedste
atosis,
inflammatoryinfiltrate,
Mallory
bodies,lysosom
alinclu
sions
(268
gcumulative
dose
givenby
author)
Amiodarone
and
N-desmethylamiodarone
plasmac
onc.0.42,0.70g
/L
400m
g/day∗
5days
per
week2years,then
200m
g∗5days
per
week∗
11mon
ths.
Cumulatived
oseo
fapp
rox.
236g
Survived
form
orethan10
mon
ths
2183 F —
Ang
inap
ectoris
NoDM,noob
esity,and
noetoh
abuse
(amiodarone
)
Hepatom
egaly
Babany
etal.[20]
15 63 139 ? 139
PT100%
,GGT46
0
Fibrosis,
steatosis,
Mallory
bodies,infl
ammatory
infiltrate,cirrho
sis,and
lysosomalinclu
sions
onelectro
nmicroscop
y(220
gcumulatived
oseg
iven
byauthor)
Amiodarone
200m
g/day∗
3.5years
Cumulatived
oseo
fapp
rox.
256g
Survived
form
orethan1.5
years
2268 F —
Com
missurotom
yfor
mitralste
nosis
NoDM,N
oob
esity,N
oetoh
abuse
(hydroxyzine,amiodarone,
tiodo
marol,and
clonazepam)
Abno
rmal
LFTs
Babany
etal.[20]
11 43 88 ? 60PT
100%
Mod
eratefi
brosis,
steatosis,
polymorph
nucle
arinfiltrate,
Mallory
bodies,cirr
hosis
,and
lysosomalinclu
sions
(211gcumulatived
oseg
iven
byauthor)
Amiodarone
200m
gdaily∗5days/w
eekfor3
years,then
100m
g/dayfor2
years,andthen
200m
g/day∗
6mon
ths
Cumulatived
oseapprox.
=254g
Survived
atleastm
orethan
9mon
ths
2368 M —
Nosig
.PMH
(isosorbide,w
arfarin
)Noetoh
Nosig
nificant
histo
rybesid
esarrhythm
ia
Rind
eretal.[21]
? 180
422 ? ?
Activ
ecirr
hosis
,ongoing
hepatocytesd
estructio
n,and
Mallory
bodies
(165
ggivenby
author)
Loadingdo
sefor1
mon
th,
then
400m
g/day∗
13.5
mon
ths.Cu
mulatived
ose
ofapprox.162
g
Diedon
emon
thaft
erdiscon
tinuatio
nof
drug
due
tohepatic
enceph
alop
athy
andhepatorenalsyn
drom
e
2464 F —
WPW
synd
rome,no
significantP
MH
(amiodarone,diuretic
,and
betablocker)
Noetoh
used
Weakn
ess,
bedridden,
andascites
Shepherd
etal.
[22]
44 172
150 ? ?
Microno
dularc
irrho
siswith
extensiven
ecrosis
ofregeneratin
gno
dules,fib
rosis,
andsw
ollenhepatocytes
600m
g/day∗
4years
Cumulatived
oseo
fapp
rox.
876g
Dieddu
eto
bron
chop
neum
onia,
diagno
sisof
cirrho
sismade
atpo
stmortem
2576 M —
Ischem
icheartd
isease,
pulm
onaryedem
a(amiodarone,isosorbide
dinitrate,furosemide,and
potassium)
Noetoh
—Jeyamalar
etal.
[23]
? 66 148 35 69
PTno
rmal
Mod
erateinfl
ammatorycells,
nodu
lesenclo
sedin
fibrous
band
s,fatty,bile
ductules
proliferatio
nchange,and
early
cirrho
sisTo
talcum
ulatived
ose2
15g
600m
g/day∗
1week,
400m
g/day∗
1mon
th,and
200m
g∗5days/w
eek∗4
years
Estim
ated
dose
=208.2g
Survived
form
orethan4
years

6 ISRN Cardiology
Table1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
2667 M —
Hypertro
phicob
structiv
ecardiomyopathy,s/pICD,
noob
esity,noetoh
,and
noDM
B/Lhand
tremor
Ishida
etal.[24]
32.49
88 463 ? 167
PT17.4
Microno
dularc
irrho
sis,
swollenhepatocytes,
proliferatin
gbiledu
ctules,
inflammatoryinfiltrate,
micro/m
acrovesic
ular
steatosis,
Mallory
bodies,and
lysosomalinclu
sionbo
dies
Calculated
dose
comes
outto
158
200m
g/day∗
26mon
ths
Cumulatived
oseo
f206
gDied8days
after
admiss
ion
duetoprerenalfailu
re
27
57 M —MI
Lethargy,
abdo
minal
diste
nsion
Harris
onand
Elias[25]
—
Microno
dularc
irrho
sis,
proliferatin
gbiledu
cts,
neutroph
ilinfiltrate,
Ballo
oningdegeneratio
nof
hepatocytes,Mallory
hyaline,
lysosomalinclu
sionbo
dies,
andepith
elioidgranulom
as
200m
gtwice/day∗
4years
6mon
ths
Cumulatived
oseo
fapp
rox.
657g
Neededliver
transplant
2877 F —
HTN
,DM,
hypo
thyroidism
,and
GER
D(Lisino
pril,
glim
epiride,esomeprazole,
levothyroxine,am
iodarone,
furosemide,
spiro
nolacton
e,prop
rano
lol,andiso
sorbide
dinitrate)
Noob
esity,n
oalcoho
l
New
onset
ascitesa
ndvaric
eal
hemorrhage
Abdo
minal
diste
nsion,
lower
extre
mity
swellin
g,and
SOB
Rajaetal.[26]
10.26
54 216 39 32
INR1.2
GGT230
Lymph
ocyticinfiltration,
macro/m
icrovesic
ular
steatosis,
Mallory
hyaline,
ballo
oningdegeneratio
n,peric
ellularfi
brosis,
cirrho
sis,
andbridging
fibrous
septa
Amiodarone
200m
g/day∗
3years
Cumulatived
oseo
fapp
rox.
219g
(Noherbalmedicines)
Survived
morethan6
mon
thsc
onfirmed
with
author
2977 M —
CAD,s/p
MI,s/pCA
BG,
hep.Binfection,
andCH
FNoetoh
forlast14years
(serum
amiodarone
and
N-desmethylamiodarone
levels=3&2.6m
g/L)
Fatig
ue,
weightloss,
and
abdo
minal
swellin
g
Flahartyetal.[27]
46.17
223
459
30 124
PT39
GGT738
Markedfib
rosis,
inflammatoryinfiltrate
Mallory
bodies,cirr
hosis
,proliferatin
gdu
ctules,and
lysosomalinclu
sions
Cumulatived
oseo
f202
g(given
byauthor)
1200
mg∗
13days,
400–
600m
g/day∗
12mon
ths
Cumulatived
oseo
fapp
rox.
200g
Diedon
day21
ofho
spita
lizationdu
eto
bradycardiae
pisode
3062 F W
Noetoh
Weakn
essa
ndjaun
dice
Sniretal.[28]
92.3,520
329,22
131
GGT1493
Microno
dularc
irrho
sis,
mod
eratetosevere
fibrosis
ofpo
rtaltract,peric
ellular
fibrosis
,Mallory
bodies,and
cirrho
sison
postmortem
Amiodarone
800m
g/day
dose∗1y
ear
Estim
ated
cumulative
dose=292g
Dieddu
etoliver
failu
re3
weeks
after
stopp
ingdrug
ISRN Cardiology 7
Table1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
3184 F W
HTN
,CHF,ob
esity
(amiodarone,felod
ipine,
furosemide,po
tassium
supp
lement,aspirin
,and
cisapride)
Nootherd
rugs
Noetoh
Darkbrow
nurinefor
7days
Changetal.[29]
142
130
610 30 50
Portalfib
rosis
,pericellular
sinusoidalfi
brosis,
lysosomal
inclu
sions,M
allory
bodies,
andcirrho
sis1.3
/1.3am
iodarone/
desm
ethylamiodarone
serum
levels
400m
g/day∗
5years
Cumulatived
ose=
730g
Died4mon
thsa
fter
diagno
sisdespite
ofsto
ppingdrug
,nocauseo
fdeathestablish
ed
3272 M
Korean
HTN
(amiodarone,felod
ipine,
HCT
Z,andaspirin
)Noetoh
EF70%
Sudd
enon
set
abdo
minal
diste
nsion
Sung
andYo
on[30]
46.1
317
137 27 237
GGT385
INR1.3
2
Cirrho
sis,polym
orph
nucle
arinfiltrate,Mallory
bodies,
ballo
oningdegeneratio
n,and
lysosomalinclu
sions
Amiodarone
200m
g/day∗
5years
Estim
ated
cumulativdo
se=365g
Survived,amiodarone
discon
tinued,andother
antia
rrhythmicstarted
3364 F —
Unstabler
ecurrent
angina,
ventric
ular
aneurysm
,and
MI
Noetoh
,noDM
Forsurgical
resectionof
ventric
ular
aneurysm
Poucelletal.[31]
12 ? 188 38 82 PT11
Microno
dularc
irrho
sis,
Mallory
bodies,balloon
ing,
macrovesic
ular
steatosis,
fibrosis
,infl
ammation,
pleomorph
icmito
chon
dria,
andlysosomalinclu
sion
600m
g∗5days/w
k∗2
years
Cumulatived
oseo
f288
Diedshortly
after
liver
biop
sy,cause
unkn
ownmay
beMI,andno
postm
ortem
3462 M —
Etoh
85g/day,s/pMI,CA
D
Hepatom
egaly
despite
norm
alLF
Ts∗1y
ear,
presentedfor
liver
biop
sy
Poucelletal.[31]
8.5 ? 98 37 80 PT11
Micro
nodu
larc
irrho
sis,
Mallory
bodies,balloon
ing,
macro
vesic
ular
steatosis,
fibrosis
,infl
ammation,
pleomorph
icmito
chon
dria,
lysosomalinclu
sion
600m
g∗5days/w
k∗2
years
Cumulatived
ose2
88g
Con
tinuedon
amiodarone
andsurvived
3570 M —
Alcoh
oliccardiomyopathy,
adrenalinsuffi
ciency
(amiodarone,
hydrocortison
e)Etoh
was
DCwhenheart
prob
lem
diagno
sed
Jaun
dice,
pruritu
s,and
deterio
ratio
nof
cond
ition
Salti
etal.[32]
481
95 1451 ? 92
GGT1231
Portalandseptalfib
rosis,
polymorph
infiltrate,Mallory
bodies,lysosom
alinclu
sions,
macrovesic
ular
steatosis,
and
cirrho
sis
Amiodarone
200m
g∗5
days/w
k∗2years
Estim
ated
cumulative
dose
of96
Survived
form
orethan5
mon
thsa
tleast
3677 F —
Afib
Weakn
ess,
nausea,
vomiting
,abdo
minal
diste
nsion,
lethargy,and
confusion
Chandraprakasam
andWhitcraft
[33]
? 192
122 ? 162
Neutro
philics
atellitosis,
Mallory
hyaline,foam
cells
representin
gph
osph
olipidosis,
macrovesic
ular
steatosis,
and
cirrho
sis
Amiodarone
200m
g/day∗
4years
Cumulatived
ose=
292
Noinform
ationabou
tou
tcom
e

8 ISRN Cardiology
Table1:Con
tinued.
𝑁
Age Sex
Race
PMHotherthan
arrhythm
ias,drugs
Presentatio
nEtoh
use
Authors
Labs
Patholog
yDurationanddo
sages
Outcomea
fterd
iagn
osisof
AIC
3768 M —
Depression,
heartfailure
(digoxin,doxepin,and
bumetanide)
Vomiting
and
muscle
weakn
esso
fon
emon
thdu
ratio
n
Lim
etal.[34]
28 142
854
29 ?
—
400m
g/day∗
5mon
ths,
then
600m
g/dayfor16
mon
ths
Cumulatived
oseo
fapp
rox.
348g
Dieddu
etoliver
failu
re5
mon
thsa
fterd
iagn
osis
despite
ofsto
pping
amiodarone
𝑁:n
umber,DM:d
iabetesm
ellitus,H
TN:h
ypertension,
HLD
:hyperlip
idem
ia,C
AD:coron
aryartery
disease,CA
BG:coron
aryartery
bypass
graft
ing,
SVT:
supraventric
ular
tachycardia,CH
F:congestiv
eheart
failu
re,etoh:alcoho
l,HCT
Z:hydrochlorothiazide,ASA
:aspirin,
SOB:
shortnesso
fbreath,n:
norm
al,T
R:tricuspidregurgitatio
n,ULN
:upp
erlim
itof
norm
al,and
W:w
hite.
Labs
arewrittenin
thefollo
wingsequ
ence,B
ili,A
ST,A
LKP,Album
in,and
ALT
inalltables.AST,A
LT,A
LKP,andGGTvalues
aregivenin
IU/L,bilirubinisgivenas
Mmol:m
icromole/L(2–17)
norm
alrange,
albu
min
isgivenas
g/L.
∗
ULN
stand
sfor
upperlim
itsof
then
ormalandthew
rittenlabisforA
LTbeing5tim
estheU
LN.

ISRN Cardiology 9
cases, the outcome was not available, authors were contacted,and the outcome was determined. Those cases, for whichoutcome could not be determined, were excluded from thefinal analysis. Of seven cases that were excluded from the finalanalysis, one case had indeterminate cause of cirrhosis andfor the rest of cases, outcome could not be established. Someauthors provided cumulative doses for amiodarone. If totalcumulative dose was not given, a formula (cumulative dose ingrams = 365∗ no. of years∗ total daily dose/1000) was used toestimate the final cumulative doses, with an assumption thatthe patient had been 100% compliant with the medicine.
Prothrombin time for some cases was given as percentageactivity rather than in seconds. We could not find any con-vertor for percentage activity to seconds (which is a normallyreported unit). For cases in which prothrombin time wasreported as a percentage prothrombin activity, values werenot used in this analysis.
2.2. Statistical Analysis. Of 37 cases analyzed, outcome wasavailable only for 31 cases. One case had indeterminate causeof cirrhosis and was excluded, and 30 cases were used for ouranalysis.
Survival at 5 months determined the patient subset andcommon pathophysiologic factors like DM, HTN, HLD,CAD, and CHF; lab values comprising of prothrombin time,total bilirubin, AST, ALT, ALK P, and GGT were comparedbetween these two subsets. Logistic regression was used forcomparing continuous independent variables, and chi-squaretest was used for comparing categorical variables. When theexpected frequency was less than five, Fisher’s exact testwas used for categorical variables. Cox proportional hazardsratios were employed in determining prognosis. All statisticaltests were two tailed with significance set at 95% level (𝑃 <0.05). STATA 11 IC software was used for statistical analysis.
3. Results
AST was significantly lower (𝑃 = 0.03) in patients whosurvived at 5 months (mean 103.33 IU/L) compared to non-survivors (mean 216.88 IU/L). AST levels overall were raisedin both groups and ranged between 64 IU/L and 734 IU/L(Tables 2 and 3). There was no significant difference in thelevels of prothrombin time, total bilirubin, ALT, ALK P, andGGT between the two groups. The prevalence of DM, HTN,HLD, CAD, and CHF was similar in these two groups. Meancumulative dose in cases of AIC was 280 g with a medianlatency period of 2.92 years and was statistically nonsignifi-cant.
The risk of dying at 5 months was marginally higher inpatients with high aspartate aminotransferase. Hazard ratiofor death is 1.003 (95% CI ranging between 1.001 and 1.006).This finding was statistically significant (𝑃 = 0.03) (Table 3).Prothrombin time, total bilirubin, ALT, ALK P, GGT, andcoexistence of DM, HTN, HLD, CAD, and CHF did notpredict survival. Results are summarized in Tables 2 and 3.
Median age at the time of diagnosis of AIC was 68 yearsfor all cases, 69.5 among survivors, and 67.5 among non-survivors. Most cases of AIC were observed among femalesthough most who died were males.
4. Discussion
4.1. Pathogenesis of AIC. Amiodarone is a lipophilic agent[5] and tends to accumulate in lipid-laden organelles suchas the liver. Amiodarone causes liver damage by differentpathogenic mechanisms, one of which may include phos-pholipidosis. There are two different mechanisms by whichamiodarone causes phospholipidosis.
(I) Amiodarone and its metabolites (N-desmethylam-iodarone) accumulate in lysosomes of hepatocytes,bile duct epithelium, and kupffer cells and leads toinhibition of phospholipase A1 andA2 [35, 36], whichthereby inhibits removal of lysosomal lipids and leadsto phospholipidosis.
(II) Amiodarone binds to phospholipids in lysosomes andforms a nondigestible complex [37, 38], which leads tophospholipidosis.
The exact mechanism of phospholipidosis-induced liverdamage is unclear. Phospholipidosis has been reported tooccur within two months of starting amiodarone therapy[6, 7]. Phospholipidosis occurs in amuch larger percentage ofpatients receiving amiodarone [5] than actual hepatocellulardamage (1% to 3%), which suggests that phospholipidosismay ormay not have a role in the pathogenesis of AIC. In fact,development of phospholipidosis is considered a marker foraccumulation of amiodarone [4] rather than a marker ofhepatotoxicity.
Leakage [3, 4, 39, 40] of proteolytic enzymes from abnor-mal lysosomes represents another pathogenic mechanism ofamiodarone-induced liver damage. Leakage of proteolyticenzymes may contribute to the elevation of aminotrans-ferases and may over time lead to hepatic necrosis, fibrosis,and eventually cirrhosis.
Immunologic mechanisms may be involved in pathogen-esis in instances of amiodarone-induced acute hepatitis inpatients with positive Coombs’ test [41].
Amiodarone-induced inhibition of cellular respirationis another possible pathogenic mechanism for amiodarone-induced liver damage. Impairment of mitochondrial 𝛽-oxi-dation and uncoupling of oxidative phosphorylation leads tothe formation of reactive oxygen species, which in turn has arole in the development of AIC [42–44].
4.2. Pathology. On histologic examination of biopsy samplesobtained fromamiodarone-induced cirrhotic patients; leuko-cytic infiltrate and strikingly high Mallory’s hyaline alongwith other usual pathologic findings of cirrhosis are noted.High Mallory’s hyaline or Mallory’s bodies are suggestive ofAIC.
Mallory’s hyaline is an eosinophilic inclusion made upof intermediate keratin filaments. Mallory’s hyaline is notspecific for AIC andmay be seen in primary biliary cirrhosis,alcoholic cirrhosis or hepatitis, nonalcoholic cirrhosis, hepa-tocellular cancer, morbid obesity, and some other conditions.Mallory hyaline in AIC is present in zone 1 of acinus, whereasin alcoholic liver disease they are located usually in zone 3 [4].
Histologic findings in patients with amiodarone-inducedhepatic damage are similar to those caused by alcohol [4, 45].

10 ISRN Cardiology
Table 2: Characteristics of reported cases.
All cases,𝑁 = 30 Survivors𝑁 = 12
Nonsurvivors at 5 months𝑁 = 18
𝑃
Median age (years) 68 (56–85) 69.5 (56–83) 67.5 (58–85) 0.84Male/female 18/12 7/5 11/7 1.00Diabetes 𝑁 = 3 2 1 0.23HTN 𝑁 = 7 2 5 1.00Hyperlipidemia 𝑁 = 5 2 3 1.00CAD 𝑁 = 16 5 11 0.26CHF 𝑁 = 11 3 8 0.39>200mg/<200mgAmiodarone dose given 18/12 5/7 13/5 0.33
Latency period 2.92 (0.5–12) 3.06 (0.5–5.5) 2.54 (1–12) 0.45Cumulative dose 279.92 (55–1241) 279.92 (55–657) 465 (165–1241) 0.07Prothrombin time 16.76 (11–39) 13.68 (11–17) 18.92 (11–39) 0.08Bilirubin (micromole/liter) 55.73 (9–481) 71.67 (9–481) 46.16 (12–142) 0.53AST 177.58 (64–734) 103.33 (38–317) 216.88 (64–734) 0.03ALK P 352.96 (73–1451) 331.5 (73–1451) 365.59 (119–854) 0.78Albumin 28 (11–39) 31 (23–39) 26.91 (11–38) 0.32ALT 134.59 (32–781) 92.1 (32–237) 170 (35–781) 0.16GGT 569 (133–1493) 640.33 (230–1231) 538.43 (133–1493) 0.74𝑁 refers to the number of patients in each group. Not all studies had data on all variables.Median values given for latency period, and for all other variables, mean values are given.
The complete pathologic spectrum of alcoholic like liverinjury due to amiodarone includes micro- and macrove-sicular steatosis, steatonecrosis, mega mitochondria, portalinflammation, fibrosis, and cirrhosis. Amiodarone-associat-ed epithelloid granulomas have also been reported [8].
Presence of phospholipids laden lamellar lysosomal in-clusion bodies on electron microscopy [1, 4, 37] is anothercharacteristic pathologic finding of AIC of liver. Yap et al.observed that amiodarone-induced lysosomal inclusionsdeveloped in nearly 100% of patients at a period of 2 weeks[46].
4.3. Diagnostic Workup. AIC is a diagnosis of exclusion.Extensive workups are normally done to exclude other diag-noses including viral etiology, Wilson’s disease, hemochro-matosis, alpha 1 antitrypsin deficiency, alcoholic hepatitis,congestive liver damage, autoimmune liver pathologies, andhepatitis due to other drugs and toxins. There is no specificdiagnostic lab test for AIC of the liver.
Furthermore, there is no specific imaging characteristicfor AIC of the liver although sometimes increased liver den-sitymay be noted on a noncontract CT scan of liver. Increasedliver density is thought to be secondary to increased iodinecontent in the liver. Amiodarone has two atoms of iodine thatconstitute 37% of molecular weight of the drug. Enhanceddensity due to amiodarone is reversible upon discontinuationof amiodarone [47].
Diagnosis of AIC is usually based on liver biopsy.Malloryhyaline and lamellar lysosomal inclusions are typical ofamiodarone-induced liver damage.
4.4. Presentation. Amiodarone-induced liver damage maypresent as Reye’s syndrome in kids [9] and may present as
asymptomatic elevation of liver enzymes in adults. Asymp-tomatic liver enzyme elevation occurs in 25% of the popu-lation treated with amiodarone [1] and is usually reversibleupon discontinuation of therapy [45]. Normalization of liverenzymes may take place anywhere from three weeks to ninemonths [48]. Symptomatic hepatic dysfunction occurs inless than 1% of the population treated with amiodaroneand includes acute and chronic liver injuries. Acute liverinjury includes acute hepatitis (idiosyncratic reaction maybe involved in pathogenesis), whereas chronic liver injuryincludes steatosis (macro and microvesicular steatosis) andcirrhosis.
5. General Discussion
Amiodarone is an iodinated benzofuran derivative, lipophilicdrug with a half-life of 35–110 days and a very large volumeof distribution (VD). Amiodarone comes as number eightin drugs that cause drug-related hepatic fatalities [9]. Majormetabolite of amiodarone, N-desmethylamiodarone, is notonly pharmacologically active but has a longer eliminationhalf-life and a larger VD than the parent drug [1, 10, 49–51].Amiodarone and N-desmethylamiodarone may be detectedeven months after stopping the drug [51] as amiodaroneaccumulates in lipid reservoirs and is released slowly fromthese reservoirs. Due to this storage mechanism, amiodaroneconcentration in liver may be as high as 500-fold of serumlevel [52]. Based on these facts, damaging effects of amio-darone may persist up to one year after complete discontinu-ation of therapy [1]. Since amiodarone is mainly metabolizedin the liver, any damage to the liver from any cause wouldhamper amiodarone metabolism and lead to a vicious cycle

ISRN Cardiology 11
Table 3: Prognostic indicators of 5-month survival.
Hazardratio
95% Confidenceinterval 𝑃
Age 0.99 (0.94–1.05) 0.80Sex 0.90 (0.34–2.37) 0.83Diabetes 0.40 (0.05–3.08) 0.32HTN 1.34 (0.43–4.10) 0.62Hyperlipidemia 1.09 (0.29–4.03) 0.90CAD 1.49 (0.51–4.36) 0.46CHF 1.74 (0.52–5.80) 0.36>200mg/ <200mgAmiodarone dosegiven
1.35 (0.48–3.84) 0.56
Latency period 1.12 (0.90–1.38) 0.33Cumulative dose 1.001 (0.999–1.003) 0.09Prothrombin time 1.04 (0.97–1.11) 0.36Bilirubin(micromole/liter) 0.998 (0.99–1.00) 0.45
AST 1.003 (1.001–1.006) 0.03ALK P 1.000 (0.999–1.001) 0.98Albumin 0.99 (0.91–1.09) 0.89ALT 1.002 (0.999–1.005) 0.21GGT 1.000 (0.998–1.002) 0.87Not all studies had data on all the variables.
of accumulation of amiodarone and further amiodarone-induced hepatic damage [53].
Why some patients develop cirrhosis or hepatic damageas a side effect of amiodarone is not entirely clear. It has beensuggested that differing sensitivity to amiodarone toxicity inpopulation may exist [54]. Most patients who developed AICusually used amiodarone PO 200mg or more per day formore than 1-2 years. In light of the above-mentioned fact,researchers propose that the total cumulative dose of amio-daronemay be important in estimating the risk of irreversibleliver injury [55]. A cumulative dose of 380 g is suggested toassociate with hepatotoxicity leading to cirrhosis [50]. Otherprospective studies showed that amiodarone hepatic toxicitycorrelates to steady state serum levels of amiodarone ratherthan daily or cumulative doses [54, 56–58]. For example,if daily dosage of amiodarone during long-term therapy isreduced, despite increasing lifetime cumulative dose, thesteady state serum concentration will still be reduced andthus decreasing risk of hepatotoxicity from amiodarone.Researchers have suggested that amiodarone level less than1.5mg/L has a minimal risk of hepatotoxicity, whereas a levelabove 2.5mg/L may have a risk up to 6% for hepatotoxicity[5]. Patients with lower eject fraction may be more prone tohepatotoxic effects of amiodarone as suggested by Tisdale etal. [59]. Although it seems logical that patients with preexist-ing liver damage may be more prone to amiodarone-inducedAIC of the liver, results by Kum et al. suggest otherwise [60].
Besides chronic liver injury due to prolonged amiodaroneuse, acute hepatic side effects from amiodarone intravenousloading dose have been reported and are thought to be caused
by polysorbate 80; a solvent used in drug preparation. Thisformof acute hepatotoxicity usually improveswith discontin-uation of medication, although fatalities have been reported[61].
To prevent amiodarone-induced cirrhosis, the amio-darone should be titrated to lowest effective dose. Patientsshould have baseline LFTs and then periodic monitoring ofLFTs while on amiodarone (at 1, 3, and 6 months and thensemiannually) [62]. Studies have suggested that baseline LFTsmonitoring is performed only in 44% of patients, and afollow-up testing at 6 months and 1 year is done in only41% and 35% of patients, respectively [63]. Patients foundto have asymptomatic elevation of transaminases while onamiodarone should have a thorough investigation of thecause [56]; repeated testing may be necessary before label-ing diagnosis of amiodarone-induced hepatotoxicity [45].According to some authors, discontinuation of amiodaronefor liver-related toxicity may not be necessary [57]. Kumet al. noted in their study that 50% of patients with increasedtransaminases while on amiodarone did not improve evenafter 1.5 years of drugwithdrawal [60].However,most authorssuggest that if aminotransferases are two times above baselinevalue or above three times the upper normal limit, thenamiodarone either should be reduced or discontinued [58, 61,64, 65]. Withdrawal of drug, when irreversible liver damagehas already occurred, has a very little effect on restoration ofliver function. Despite what is said, discontinuation of amio-darone for liver-related hepatotoxicity may not be necessaryexcept in cases to prevent irreversible loss of liver function[11]. After discontinuation of amiodarone, monitoring periodshould continue for at least one year as the damaging effect ofamiodarone might persist. Patients on amiodarone should beadvised to avoid any potentially hepatotoxic agent to preventadditive hepatic damage. Discontinuation of amiodarone isreported to occur in nearly 20–40% of patients if changes inaminotransferases are detected during amiodarone therapy[66].
To date, the role of routine monitoring of amiodarone orits metabolite’s serum levels for predicting hepatic damageis not well established. Nonetheless, there are numerouspatients who may develop AIC without any abnormality inliver enzymes. Such patient population will not be detecteduntil very late. Routine imagingmay have a role in this subsetof patients, but there is no study to support this.
Based on our review (Table 1), we noted that AIC isextremely rare. However, once the diagnosis is established,the mortality risk may be as high as 60% at 5 months. Themost common cause of death among reported cases was dueto liver- and GI-related complications. Ethnic predispositionto AIC could not be determined due to lack of the publishedliterature.Themost common symptoms reportedwere gener-alized weakness, abdominal pain, and abdominal distension.
A cumulative dose of 380 g has been suggested to asso-ciate with cirrhosis. By reviewing published cases, we realizethat cirrhosis has been reported to occur with a cumulativedose as low as 55 g [9]. Why some patients with a cumulativedose of 200 g develop cirrhosis and others do not untilcumulative dose crosses above 1000 g is unclear, but it doessuggest that it may be a steady state concentration rather

12 ISRN Cardiology
than cumulative dose that may be important in predictingrisk of cirrhosis. The diagnosis in most patients was madeby liver biopsy. Although Mallory hyaline and lysosomalinclusions are characteristic features of amiodarone-inducedcirrhosis, the dilemma is that the above-mentioned patho-logic characteristics may be identified in patients on amio-darone who do not have cirrhosis. Liver biopsy alone fordiagnosis of AIC may not be enough. In fact, a thoroughevaluation for all possible causes of cirrhosis should be done.Once all possible causes of cirrhosis have been ruled out,then only the presence of Mallory hyaline and lysosomalinclusions in cirrhotic liver may be suggestive of AIC ofthe liver. In all published cases, a thorough investigation forthe cause of cirrhosis was carried out. In most publishedcases, obesity, DM, and ethanol consumption were givenspecial attention to rule out the possibility of alcoholic andnonalcoholic steatohepatitis (NASH). Risk factors for devel-opment of amiodarone-induced hepatotoxicity and cirrhosishave not been clearly defined. Whether it is cumulative doseor steady state concentration of amiodarone that predictsrisk of cirrhosis has not been determined. In most patientseven after discontinuation of amiodarone, toxicity effectsdid not subside. Majority of patients have had amiodarone-related hepatotoxicity before onset of cirrhosis leading to adecrease in dose or discontinuation of the drug. However, thedrug was restarted for various reasons, which unfortunatelylead to cirrhosis. Although AST and ALTs are said to bemainly elevated in amiodarone-related hepatotoxicity andnot the ALK P or GGT [56], our analysis suggests otherwise.According to our analysis, the only statistically significantvariable different among survivors versus nonsurvivors at 5months was the level of AST at time of diagnosis of AIC.We suggest that if patients on amiodarone have a persistentincrease in aminotransferases, a liver imaging and a liverbiopsy should be done.
There is no treatment available for amiodarone-inducedhepatotoxicity or cirrhosis besides discontinuation of theoffending agent and switching to some other antiarrhythmicagent. Previously, antioxidants vitamin E and selenium havebeen tried without any success.We recommend against usingantioxidants for counteracting amiodarone hepatotoxicity, asthere is no strong scientific evidence for such practices.
We are aware that there are limitations in our studybecause of the smaller sample size, which may have affectedour analysis. Future prospective studies using larger patientpopulation may be able to identify predictors of survival incase of AIC.
6. Conclusion
Although amiodarone does have very serious and fatal effectson the liver, such effects are rare. With a closer monitoringand taking appropriate actions when prompted, amiodaronecan be safely used on long-term basis. Further prospectivestudies are needed to identify predictors of AIC and ofmortality or survival in cases of AIC. Role of routine imagingand biopsy of the liver in patients taking amiodarone isunclear; future studies are needed to address this issue.
References
[1] J. H. Lewis, R. C. Ranard, A. Caruso et al., “Amiodaronehepatotoxicity: prevalence and clinicopathologic correlationsamong 104 patients,”Hepatology, vol. 9, no. 5, pp. 679–685, 1989.
[2] S. R. Puli, M. A. Fraley, V. Puli, A. B. Kuperman, and M. A.Alpert, “Hepatic cirrhosis caused by low-dose oral amiodaronetherapy,” American Journal of the Medical Sciences, vol. 330, no.5, pp. 257–261, 2005.
[3] B. Guigui, S. Perrot, J. P. Berry et al., “Amiodarone-induced hep-atic phospholipidosis: a morphological alteration independentof pseudoalcoholic liver disease,” Hepatology, vol. 8, no. 5, pp.1063–1068, 1988.
[4] J. H. Lewis, F.Mullick, K. G. Ishak et al., “Histopathologic analy-sis of suspected amiodarone hepatotoxicity,”Human Pathology,vol. 21, no. 1, pp. 59–67, 1990.
[5] M. Atiq, J. C. Davis, L. W. Lamps, S. S. Beland, and J. E.Rose, “Amiodarone induced liver cirrhosis. Report of two cases,”Journal of Gastrointestinal and Liver Diseases, vol. 18, no. 2, pp.233–235, 2009.
[6] B. Rigas, L. E. Rosenfeld, and K.W. Barwick, “Amiodarone hep-atotoxicity. A clinicopathologic study of five patients,” Annals ofInternal Medicine, vol. 104, no. 3, pp. 348–351, 1986.
[7] D. Capron-Chivrac, N. Reix, C. Quenum, and J. P. Capron,“Amiodarone hepatopathy. Study of a case and review of theliterature,” Gastroenterologie Clinique et Biologique, vol. 9, no.6-7, pp. 535–539, 1985.
[8] N. B. Chaabane, O. Hellara, L. Safer et al., “Cirrhosis withincreased density of the liver: amiodarone-induced hepatotox-icity,” Tunisie Medicale, vol. 90, no. 6, pp. 487–488, 2012.
[9] http://livertox.nih.gov/Amiodarone.htm.[10] M. Richer and S. Robert, “Fatal hepatotoxicity following oral
administration of amiodarone,” Annals of Pharmacotherapy,vol. 29, no. 6, pp. 582–586, 1995.
[11] N. H. Gilinsky, G. W. Briscoe, and C. S. Kuo, “Fatal amiodaronehepatoxicity,” American Journal of Gastroenterology, vol. 83, no.2, pp. 161–163, 1988.
[12] K. Tordjman, I. Katz, M. Brusztyn, and T. Rosenthal, “Amio-darone and the liver,” Annals of Internal Medicine, vol. 102, no.3, pp. 411–412, 1985.
[13] J. M. Rene, J. Buenestado, B. Pais, and M. C. Pinol, “Cirrosiscausada por amiodarona,” Revista Espanola de EnfermedadesDigestivas, vol. 87, no. 5, pp. 399–402, 1995.
[14] A. Singhal, P. Ghosh, and S. A. Khan, “Low dose amiodaronecausing pseudo-alcoholic cirrhosis,”Age and Ageing, vol. 32, no.2, pp. 224–225, 2003.
[15] N. Bach, B. L. Schultz, L. B. Cohen et al., “Amiodaronehepatotoxicity: progression from steatosis to cirrhosis,” MountSinai Journal of Medicine, vol. 56, no. 4, pp. 293–296, 1989.
[16] R. Martinez, E. Saperas, J. Vilaseca, P. Tornos, and H. Allende,“Cirrosis hepatica inducida por amiodarona,”Gastroenterologiay Hepatologia, vol. 17, no. 9, pp. 482–484, 1994.
[17] S. Coban, S. Koklu,H. Sencer, F. Ekiz, andN. Ormeci, “Lowdoseamiodarone associated cirrhosis,” Journal of Gastroenterologyand Hepatology, vol. 22, no. 1, pp. 140–141, 2007.
[18] H. Oikawa, C. Maesawa, R. Sato et al., “Liver cirrhosis inducedby long-term administration of a daily low dose of amiodarone:a case report,”World Journal of Gastroenterology, vol. 11, no. 34,pp. 5394–5397, 2005.
[19] A. Lamproye, J. Ramos, D. Larrey, and J. Belaiche, “Pseudo-alcoholic hepatitis and cirrhosis caused by Amiodarone (Cor-darone),” Revue Medicale de Liege, vol. 53, pp. 120–124, 1998.
ISRN Cardiology 13
[20] G. Babany, A. Mallat, and E. S. Zafrani, “Chronic liver diseaseafter low daily doses of amiodarone. Report of three cases,”Journal of Hepatology, vol. 3, no. 2, pp. 228–232, 1986.
[21] H. M. Rinder, J. C. Love, and R. Wexler, “Amiodarone hepato-toxicity,” The New England Journal of Medicine, vol. 314, no. 5,pp. 318–319, 1986.
[22] N. A. Shepherd, A.M.Dawson, P. R. Crocker, andD.A. Levison,“Granular cells as a marker of early amiodarone hepatotoxicity:a pathological and analytical study,” Journal of Clinical Pathol-ogy, vol. 40, no. 4, pp. 418–423, 1987.
[23] R. Jeyamalar, R. Pathmanathan, D.Wong, and P. Kannan, “Hep-atotoxicity of amiodarone,” Annals of the Academy of MedicineSingapore, vol. 21, no. 6, pp. 838–840, 1992.
[24] S. Ishida, M. Sugino, T. Hosokawa et al., “Amiodarone-inducedliver cirrhosis and parkinsonism: a case report,” Clinical Neu-ropathology, vol. 29, no. 2, pp. 84–88, 2010.
[25] R. F. Harrison and E. Elias, “Amiodarone-associated cirrhosiswith hepatic and lymph node granulomas,”Histopathology, vol.22, no. 1, pp. 80–82, 1993.
[26] K. Raja, S. N. Thung, M. I. Fiel, and C. Chang, “Drug-induced steatohepatitis leading to cirrhosis: long-term toxicityof amiodarone use,” Seminars in Liver Disease, vol. 29, no. 4, pp.423–428, 2009.
[27] K. K. Flaharty, S. L. Chase, H. M. Yaghsezian, and R. Rubin,“Hepatotoxicity associated with amiodarone therapy,” Pharma-cotherapy, vol. 9, no. 1, pp. 39–44, 1989.
[28] Y. Snir, N. Pick, K. Riesenberg, I. Yanai-Inbar, H. Zirkin, and F.Schlaeffer, “Fatal hepatic failure due to prolonged amiodaronetreatment,” Journal of Clinical Gastroenterology, vol. 20, no. 3,pp. 265–266, 1995.
[29] C. C. Chang, M. Petrelli, J. F. Tomashefski, and A. J. McCul-lough, “Severe intrahepatic cholestasis caused by amiodaronetoxicity after withdrawal of the drug: a case report and reviewof the literature,”Archives of Pathology and LaboratoryMedicine,vol. 123, no. 3, pp. 251–256, 1999.
[30] P. S. Sung and S. K. Yoon, “Amiodarone hepatotoxicity,” Hepa-tology, vol. 55, no. 1, pp. 325–326, 2012.
[31] S. Poucell, J. Ireton, and P. Valencia-Mayoral, “Amiodarone-associated phospholipidosis and fibrosis of the liver. Light,immunohistochemical, and electron microscopic studies,”Gas-troenterology, vol. 86, no. 5 I, pp. 926–936, 1984.
[32] Z. Salti, P. Cloche, P. Weber, G. Houssemand, and F. Vollmer, “Acase of amiodarone-induced cholestatic hepatitis,” Annales deCardiologie et d’Angeiologie, vol. 38, no. 1, pp. 13–16, 1989.
[33] S. Chandraprakasam and M. Whitcraft, “Pseudo-alcoholic cir-rhosis: an interesting case of amiodarone induced hepatotoxic-ity,”The Internet Journal of Gastroenterology, vol. 11, no. 1, 2012.
[34] P. K. Lim, P. N. Trewby, G. C. A. Storey, and D. W. Holt, “Neu-ropathy and fatal hepatitis in a patient receiving amiodarone,”British Medical Journal, vol. 288, no. 6431, pp. 1638–1639, 1984.
[35] K. Itostetler,M. Reasor, andB.W. Frazee, “Mechanisms of amio-darone toxicity: inhibition of phospholipase A,”Circulation, vol.79, p. 240, 1984.
[36] M. F. Heath, F. R. Costa-Jussa, J. M. Jacobs, and W. Jacobson,“The induction of pulmonary phospholipidosis and the inhibi-tion of lysosomal phospholipases by amiodarone,” British Jour-nal of Experimental Pathology, vol. 66, no. 4, pp. 391–397, 1985.
[37] R. Luallmann-Rauch and G. H. Reil, “Chlorphentermine-induced lipidosis-like ultrastructural alterations in lungs andadrenal glands of several species,” Toxicology and AppliedPharmacology, vol. 30, pp. 408–421, 1974.
[38] M. Pirovino, O. Muller, T. Zysset, and U. Honegger, “Amio-darone-induced hepatic phospholipidosis: correlation of mor-phological and biochemical findings in an animal model,”Hepatology, vol. 8, no. 3, pp. 591–598, 1988.
[39] P. Yagupsky, E. Gazala, and S. Sofer, “Fatal hepatic failure andencephalopathy associated with amiodarone therapy,” Journalof Pediatrics, vol. 107, no. 6, pp. 967–970, 1985.
[40] A. Vereckei, E. Feher, I. Gyorgy et al., “Possibilities of antiox-idant therapy in the prevention of side effects of amiodarone,”Orvosi Hetilap, vol. 132, no. 23, pp. 1265–1268, 1991.
[41] H. W. M. Breuer, W. Bossek, C. Haferland, M. Schmidt, H.Neumann, and J. Gruszka, “Amiodarone-induced severe hep-atitis mediated by immunological mechanisms,” InternationalJournal of Clinical Pharmacology and Therapeutics, vol. 36, no.6, pp. 350–352, 1998.
[42] P. Kaufmann, M. Torok, A. Hanni, P. Roberts, R. Gasser, and S.Krahenbuhl, “Mechanisms of benzarone and benzbromarone-induced hepatic toxicity,”Hepatology, vol. 41, no. 4, pp. 925–935,2005.
[43] B. Fromenty, C. Fisch, G. Labbe et al., “Amiodarone inhibitsthe mitochondrial 𝛽-oxidation and fatty acids and producesmicrovesicular steatosis of the liver inmice,” Journal of Pharma-cology and Experimental Therapeutics, vol. 255, no. 3, pp. 1371–1376, 1990.
[44] B. Fromenty, C. Fisch, A. Berson, P. Letteron, D. Larrey, andD. Pessayre, “Dual effect of amiodarone on mitochondrialrespiration. Initial protonophoric uncoupling effect followedby inhibition of the respiratory chain at the levels of complexI and complex II,” Journal of Pharmacology and ExperimentalTherapeutics, vol. 255, no. 3, pp. 1377–1384, 1990.
[45] P. T. Pollak, “How toxic is amiodarone to the liver?” Journal ofGastrointestinal and Liver Diseases, vol. 19, no. 1, pp. 11–13, 2010.
[46] S. H. Yap, P. J. M. Rijntjes, H. J. Moshage, H. Croes, and P. H.K. Jap, “Amiodarone-induced lysosomal inclusions in primarycultures of human hepatocytes,” Gastroenterology, vol. 92, no. 1,pp. 272–273, 1987.
[47] S. Kojima, S. Kojima, H. Ueno, M. Takeya, and H. Ogawa,“Increased density of the liver and amiodarone associatedphospholipidosis,” Cardiol Res Pract, vol. 2009, Article ID598940, 3 pages, 2009.
[48] L. Llanos, R. Moreu, A. M. Peiro et al., “Causality assessment ofliver injury after chronic oral amiodarone intake,”Pharmacoepi-demiology and Drug Safety, vol. 18, no. 4, pp. 291–300, 2009.
[49] J. Gill, R. C. Heel, and A. Fitton, “Amiodarone. An overview ofits pharmacological properties, and review of its therapeutic usein cardiac arrhythmias,” Drugs, vol. 43, no. 1, pp. 69–110, 1992.
[50] P. C. Adams, M. K. Bennett, and D. W. Holt, “Hepatic effectsof amiodarone,” British Journal of Clinical Practice. Supplement,vol. 44, pp. 81–95, 1986.
[51] J. B. Simon, P. N. Manley, J. F. Brien, and P. W. Armstrong,“Amiodarone hepatotoxicity simulating alcoholic liver disease,”TheNew England Journal of Medicine, vol. 311, no. 3, pp. 167–172,1984.
[52] J. F. Brien, S. Jimmo, and F. J. Brennan, “Distribution of amio-darone and its metabolite, desethylamiodarone, in humantissues,” Canadian Journal of Physiology and Pharmacology, vol.65, no. 3, pp. 360–364, 1987.
[53] P. Letteron, A. Sutton, A. Mansouri, B. Fromenty, and D.Pessayre, “Inhibition of microsomal triglyceride transfer pro-tein: another mechanism for drug-induced steatosis in mice,”Hepatology, vol. 38, no. 1, pp. 133–140, 2003.

14 ISRN Cardiology
[54] N. Gluck, M. Fried, and R. Porat, “Acute amiodarone liver toxi-city likely due to Ischemic hepatitis,” Israel Medical AssociationJournal, vol. 13, no. 12, pp. 748–752, 2011.
[55] U. Klotz, “Antiarrhythmics: elimination and dosage considera-tions in hepatic impairment,”Clinical Pharmacokinetics, vol. 46,no. 12, pp. 985–996, 2007.
[56] D. S. Pratt and M. M. Kaplan, “Evaluation of abnormal liver-enzyme results in asymptomatic patients,” The New EnglandJournal of Medicine, vol. 342, no. 17, pp. 1266–1271, 2000.
[57] W.Mattar, B. Juliar, I. Gradus-Pizlo, and P. Y. Kwo, “Amiodaronehepatotoxicity in the context of the metabolic syndrome andright-sided heart failure,” Journal of Gastrointestinal and LiverDiseases, vol. 18, no. 4, pp. 419–423, 2009.
[58] M. Babatin, S. S. Lee, and P. T. Pollak, “Amiodarone hepatotoxi-city,” Current Vascular Pharmacology, vol. 6, no. 3, pp. 228–236,2008.
[59] J. E. Tisdale, S. L. Follin, A. Ordelova, and C. R. Webb,“Risk factors for the development of specific noncardiovascularadverse effects associated with amiodarone,” Journal of ClinicalPharmacology, vol. 35, no. 4, pp. 351–356, 1995.
[60] L. C. C. Kum, W. W. L. Chan, H. H. Y. Hui et al., “Prevalence ofamiodarone-related hepatotoxicity in 720Chinese patients withor without baseline liver dysfunction,” Clinical Cardiology, vol.29, no. 7, pp. 295–299, 2006.
[61] A. E. Ratz Bravo, J. Drewe, R. G. Schlienger, S. Krahenbuhl,H. Pargger, and W. Ummenhofer, “Hepatotoxicity during rapidintravenous loading with amiodarone: description of threecases and review of the literature,” Critical Care Medicine, vol.33, no. 1, pp. 128–134, 2005.
[62] P. T. Pollak and S. L. Shafer, “Use of population modelingto define rational monitoring of amiodarone hepatic effects,”Clinical Pharmacology andTherapeutics, vol. 75, no. 4, pp. 342–351, 2004.
[63] C. Burgess, A. Blaikie, T. Ingham, G. Robinson, and S.Narasimhan, “Monitoring the use of amiodarone: compliancewith guidelines,” Internal Medicine Journal, vol. 36, no. 5, pp.289–293, 2006.
[64] P. T. Pollak and Y. D. You, “Monitoring of hepatic functionduring amiodarone therapy,” American Journal of Cardiology,vol. 91, no. 5, pp. 613–616, 2003.
[65] P. T. Pollak, A. D. Sharma, and S. G. Carruthers, “Relationof amiodarone hepatic and pulmonary toxicity to serum drugconcentrations and superoxide dismutase activity,” AmericanJournal of Cardiology, vol. 65, no. 18, pp. 1185–1191, 1990.
[66] P. J. Podrid, “Amiodarone: reevaluation of an old drug,” Annalsof Internal Medicine, vol. 122, no. 9, pp. 689–700, 1995.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com