resuc paper review
TRANSCRIPT
1
Teaching Life Support Competencies in Health Care –Assessment of
Current Practice and Recommendations
Bentham L, RN1, Lilford L, MD, PhD2, Mohammed M, MD3, Bullock I, MD 5
Bradburn S6, Fawdry R, MD4, Barach Paul, MD, MPH7
1Research Nurse, 2Professor of Clinical Epidemiology, 3Senior Research Fellow, Department
of Public Health and Epidemiology, 4Consultant Obstetrician, The University of
Birmingham, Edgbaston, Birmingham B15 2TT; 5RCN Institute, Radcliffe Infirmary, Oxford
OX2 6HE; 6University Hospitals Birmingham NHS Trust, Queen Elizabeth Hospital,
Birmingham; 7 Associate Professor, Department of Anesthesiology, University of Miami,
Florida, USA
Corresponding Author:
Professor R.J.Lilford
Tel: 0121 414 2226
Fax: 0121 414 7878
Email: [email protected]
Counts: Total Words = 5997; Abstract word: 368; Tables 2; Figures 3.

2
ABSTRACT
Objectives: The study sought: 1) to survey the type of courses teaching adult life support and
pre cardiac arrest management provided by UK hospitals and medical schools and required
by professional bodies; 2) to describe both the curriculum content and applied teaching
methods used the most popular in-hospital adult life support courses; and 3) to examine the
fidelity of adult life support courses and their implementation in England; 4) to stimulate
policy makers in other countries that are examining the utility and effectiveness of life
support courses
Methodology: We surveyed the prevalence, distribution and impact of the resuscitation
training population among UK health trusts. We conducted semi-structured telephone
interviews with a randomised sample (n=30), and then a detailed thematic analysis of written
and online course materials.
Results: We found a large number of both providers and types of life support courses for
health care professions, the public and special groups such as divers. All but one of the thirty
English NHS Hospitals surveyed provided adult life support courses. The Resuscitation
Council UK Advanced Life Support (ALS) course was run by a majority (n=20) of the acute
hospital trusts surveyed. Many hospitals ran ‘in-house’ courses alongside or in addition to the
national (franchised) courses. Our survey revealed that courses aimed at the recognition and
management of pre-arrest deterioration are now widely taught in hospitals (n=25). The survey
of UK medical schools (n=25) revealed that while life support training was provided at all
sites, courses varied and those aimed at the recognition and management of acutely ill
patients were provided by only six sites. Only three professional colleges surveyed (n=16)
required members to provide evidence of life support skill competence. Although many
hospital sites have endeavoured to customize the three most widely provided courses to
3
produce ‘in-house’ courses, the franchised course format was followed with meticulous
fidelity.
Conclusions: There are a small number of market leaders for the main franchised
resuscitation courses. The teaching and provision of life support courses is now
institutionalised in the hospital sector. Courses are implemented with great fidelity when
compared by curriculum content. There has been a large increase in uptake of ‘pre-arrest’
courses. More study is needed to assess the impact of these courses on clinical care and
patient outcomes.
Key Words: Education, Resuscitation, Training, Advanced Life Support, patient safety,
simulation
4
INTRODUCTION
Cardiopulmonary resuscitation has become an integral part of modern health care.
Cardiac arrest survival rates have been relatively static at around 20%, in recent years (1-3).
CPR is attempted in increasing numbers of patients and many of these patients are unlikely to
benefit from CPR (ref? Perkins/Soar). A United Kingdom (UK) meta-analysis of studies
examining survival rates of adult in-hospital patients after cardiopulmonary resuscitation
reported an immediate survival rate of one in three, with only one in eight patients likely to
survive to discharge (1).
In-hospital cardiac arrest improved survival is associated with rapid recognition of
need, initiation of resuscitation, the experience of the team and a shock-responsive rhythm.
The latter however, is particularly associated with short term survival (4-8). Variables
associated with decreased survival to discharge rates include infection on the day prior to
resuscitation, cancers, dementias, hypovolaemia, coronary artery disease and patient age over
65 years (1). Organisations such as ILCOR (the International Liaison Committee on
Resuscitation), the ERC (European Resuscitation Council) and the Resuscitation Council UK
(9) have developed treatment and education guidelines that form the basis of courses dealing
with the evaluation and management of cardiac arrest (10-12).
This study, commissioned by the National Patient Safety Agency (NPSA) to describe
life support courses currently available, is part of a larger study entitled ‘Teaching life
support and resuscitation competencies in health care – current practice and strategies for
future research’(13). The first section of the report compared and contrasted teaching
methods currently used in life support and resuscitation training against contemporary
educational theories of best practice, and against results of existing comparative studies of
different methods used to teach life support and resuscitation.
5
The aim of this study, which forms the second section of the NPSA commissioned
report (13), was to describe current practice and address key issues by conducting four
separate studies of increasing focus (see Figure 1):
1. To provide a broad survey of all courses teaching life support for clinicians that are
currently available in the UK;
2. To survey courses dealing specifically with adult life support and identification and
management of antecedents to cardiac arrest (we refer to these in the text as ‘pre-
arrest management courses’), provided by UK hospitals and medical schools and to
examine the life support training requirements set by professional bodies;
3. To describe the organisation and teaching methods prescribed by three of the most
widely provided courses; and,
4. To examine the fidelity with which the prescribed courses are implemented in
England.
Deterioration leading to a cardiac arrest is often not sudden. Symptoms indicating
physiological deterioration have been recorded in patient notes around a mean of 6.5 hours
prior to cardiac arrest (14-16). The need for preventative clinical strategies, highlighted in
several studies, has led to the development of courses dealing with the recognition and
treatment of acute life-threatening conditions (15-18). There have been some intriguing data
from Australia and the US suggesting better patient survival with rapid response teams (19),
although Hillman, et al, in a multi-center study failed to show benefit (Hillman et al.
Introduction of the MET system: A cluster randomized controlled trial. Lancet
2005;365:2091-7).
In 2002 a Royal College of Physicians of London Working Party (20) recommended
that medical school postgraduate courses include in their curricula an acute medical

6
emergencies course such as the Acute Life-threatening Events – Recognition and Treatment
(ALERT™) course. More recently a multi-agency working group (The Acute Care
Undergraduate Teaching Initiative – ACUTE) has been set up by the Resuscitation Council
UK to develop a module on safe care of acutely ill patients for the national undergraduate
medical curriculum (21).
Figure 1 goes @ here

7
Project 1. A broad survey of al l courses teaching l i fe support for cl inicians , special ist groups and the public, that are currently avai lable in the UK
METHODS
This section contains a brief précis of the methodology for each survey in the study. A
more detailed account of the methodology is given in our report - ‘Teaching life support and
resuscitation competencies in health care - current practice and strategies for future
research’(13).
Compilation of UK Life Support courses
The survey compiled a database of courses in the UK that teach resuscitation, ranging
from adult life support and life support for particular groups of patients and courses for the
general public. This was achieved by carrying out expert input, internet searches, and by
conducting telephone inquiries.
A. Survey of adult life support courses and ‘pre-arrest management’ courses Hospital adult life support and ‘pre-arrest management courses’
The survey was undertaken to examine the number and type of courses teaching life
support in English NHS hospital trusts. Because of the considerable number and type of life
support courses currently available, including specialist courses, we focussed the survey on
courses concerned with the recognition and management of the collapsed or deteriorating
adult patient. An independent statistician was employed to make a random selection from a
list of 161 acute NHS hospital trusts obtained from an NHS website (22). Sites were allocated
a sample number (from 1 to 161). A random selection sample interval of 5.367 gave a
sample of 30 sites of 161 sites (first number 4.717). If a Resuscitation Officer could not be
contacted, or did not reply after 5 attempts by telephone interviewers, the next site on the list
of acute hospitals would be contacted.
A semi-structured telephone interview with resuscitation officers and resuscitation
managers was used at randomly selected sites to elicit the following information (13):
8
1. The proportion of sites running hospital life support courses with automated external
defibrillation versus the proportion of hospital life support courses with manual
defibrillation;
2. The proportion of advanced life support courses that are ‘formally approved by
national bodies’ (we call these ‘franchised’) versus advanced life support courses, that
are ‘hospital designed, operated and quality assessed’ (we call these ‘in-house’).
3. The difference in the length of ‘franchised’ life support courses versus ‘in-house’ life
support courses.
4. The proportion of candidates attending ‘in-house’ versus ‘franchised’ hospital life
support courses of similar type.
5. The proportion of instructors to candidates in ‘franchised’ courses versus ‘in-house’
courses.
The questionnaire used to obtain this data is included in the main report as Appendix 3(a)
(13) and in this report as Appendix A.
B. Survey of life support training requirements for specialist health practitioners, by
professional accreditation or standard setting bodies
The survey identified life support training required by post-graduate medical
practitioners, professionals allied to medicine, midwives and nurses, in order to qualify for
membership of specialist medical or health colleges in the UK. The survey also identified the
continuing professional development training requirements of specialist medical
practitioners, nurses, midwives and professionals allied to medicine of each UK professional
accreditation or standard setting body.
Data were collected from on-line guidelines and course curricula, expert input, and
by contacting education departments of colleges included: Courses that trainees are required
to attend in order to achieve membership; Continuing Professional Development training
9
requirements in order to maintain membership; Courses that trainees are recommended to
attend with no membership consequences.
C. Survey of UK medical school training
The survey identified the life support training offered to medical undergraduates from
a sample of 24 medical schools in the UK (23). Twenty-four medical schools were identified,
with successful data collection from twenty-one sites (87.5%). Information about training
requirements was established by obtaining online undergraduate curriculum (n = 4);
contacting the undergraduate dean or a sub-dean of each medical school (n =16); and by
contacting resuscitation officers (n =1).
D. Survey of course pedagogy
Life support courses
We studied the pedagogy of the most frequently provided (nationally approved -
‘franchised’) life support courses and focussed on courses dealing with the following
circumstances: the initial resuscitation of an adult, that has had an acute collapse in the
hospital, but not in the intensive care department or operating room (13). The study focussed
on courses provided by the Resuscitation Council (RCUK), the Advanced Life Support
Group (ALSG), and the Royal College of Surgeons (RCS Eng). Course materials and
instructor’s manuals were examined and senior teachers (typically course co-ordinators or
resuscitation officers) were interviewed in order to confirm our understanding of course
materials and explore the thinking on which the educational methods were predicated. The
number of trainees in 2002 attending each type of life support course developed by course
providers was established through telephone interviews with senior people from these groups
(13).
Courses for the recognition and management of adult acute life-threatening illnesses (‘pre-
arrest management courses’)
10
The survey included courses designed to teach health practitioners about the early
identification and management of deteriorating patients. Courses that met the survey criteria
were identified during the telephone interviews with course coordinators of life support
courses, during telephone interviews with staff, while surveying internet sites of professional
accreditation/ standard setting bodies, and using internet search engines. Collection of data
concerning these courses was completed by a semi-structured telephone interview with life
support course coordinators; with organisers of courses with internet sites; and by
examination of course manuals, timetables and guidelines.
E. Detailed analysis of the fidelity with which courses are implemented
We further selected three types of courses – Immediate Life Support (ILS), Advanced
Life Support (ALS) and Advanced Trauma Life Support (ATLS). A survey of Basic Life
Support (BLS) courses has previously been published (24). A list of teaching centres for each
type of course was obtained from the course website or by consulting the provider of each
course. A semi-structured telephone interview was conducted (13) to determine, firstly, the
fidelity with which the course followed the prescribed pattern, and secondly, the reasoning
behind any deviations. The questionnaire used for this survey is included in the main report
as Appendix 3(b) (13). Findings from both the interview and questionnaire were analysed and
compared to increase the validity of data collected.
RESULTS
Narrative summary of results of UK Life Support courses
The search for courses revealed a large number of providers, offering many basic
and advanced life support courses. The courses are aimed at people ranging from hospital
staff to the general public. The type of courses varied from basic life support to specialised
courses. It became apparent from this search that a limited number of courses had become
11
‘best of breed’ in their field. Detailed results of this search can be found in Appendix 9 of the
main report (13).
Narrative summary of the survey of adult life support courses at UK hospitals
Comparison of adult life support courses at NHS hospitals
Of the thirty hospitals that responded all but one ran life support courses. The site not
running courses did not have a resuscitation officer in post. The manager of the coronary care
unit (CCU) reported that there were no courses run by the hospital at the time of the survey.
This observation from our study indicates the importance of both training structures and
appropriate personnel to ensure that the essential training is provided. Figure 2 illustrates the
total number of basic life support (BLS), hospital life support with defibrillation (ILS) and
advanced life support (ALS) courses run by each site. It can be seen at once that while all but
one hospital ran courses, the type and number of courses is extremely variable.
Basic Life Support
‘Basic life support’ (BLS) courses in the survey included in-hospital BLS with or
without training in the use of airway adjuncts, and with or without training in practical skills
needed to support a cardiac arrest team. Twenty-one of the thirty sites (70%) described their
BLS courses as a mandatory requirement for all clinical staff, usually a response to the
Clinical Negligence Scheme for Trusts (CNST) that determine levels of insurance premiums.
Twenty-eight out of thirty sites surveyed (93%) ran a BLS course. Eleven (37%) sites ran an
‘out-of-hospital’ BLS course teaching life support without equipment. One site ran an in-
hospital life support course with automated external defibrillation, instead of a BLS course.
The results of the numbers of courses run by each site are detailed in Figure 2.
Immediate life support
Immediate life support (ILS) type courses consist of training in hospital life support
and include training in the use of manual or automated external defibrillation. Twenty-eight
12
(93%) out of the thirty sites surveyed ran such courses. The RCUK ILS course was run by
twenty sites. Ten (33%) of the thirty sites ran both RCUK and ‘in-hospital’ courses. Eighteen
of the thirty sites surveyed ran only their own ‘in-hospital’ life support course with automated
external defibrillation or manual defibrillation training. Although the authors recognise that at
the time of data collection, the ILS course was still in its relative infancy (recent figures
demonstrate a large uptake of this course nationally, with 4,700 ILS one day and half day
recertification courses run and more than 40,000 candidates attending during 2004).
Of the fifty-three ILS type courses at the thirty sites surveyed, the total number of
hospital life support courses with manual defibrillation was twenty (38%), compared with a
total of thirty-three (62%) courses teaching hospital life support with automated external
defibrillation training. Of the fifty-three courses, twenty-three (43%) were franchised
Resuscitation Council UK courses, while the remaining thirty courses (57%) were in-house
designed, and operated.
Advanced Life Support
Advanced life support (ALS) courses consist of ILS plus teaching about team
leadership, drugs and peri-arrest situations and recognition of contributing causes such as
pneumothorax. Twenty (67%) of the thirty sites surveyed ran the Resuscitation Council UK
(RCUK) ALS course. Six of those sites also ran an in-house designed and operated course.
Six sites (20%) surveyed ran only an in-house designed, and operated ALS course. Four
(13%) of the sites surveyed did not run an ALS course.
Some resuscitation officers interviewed for the survey were concerned by not being
able to run more RCUK ALS courses. Reasons cited include: insufficient funding to provide
recommended RCUK life support courses (11 sites); lack of staff cover in order to release
medical and nursing staff attending a 3 day course (9 sites); and inability to employ enough
qualified instructors to run the course as per RCUK guidelines (5 sites). However, other
13
resuscitation officers (7 sites) reported that they were sufficiently skilled and experienced in
designing and running courses teaching life support skills and did not require RCUK course
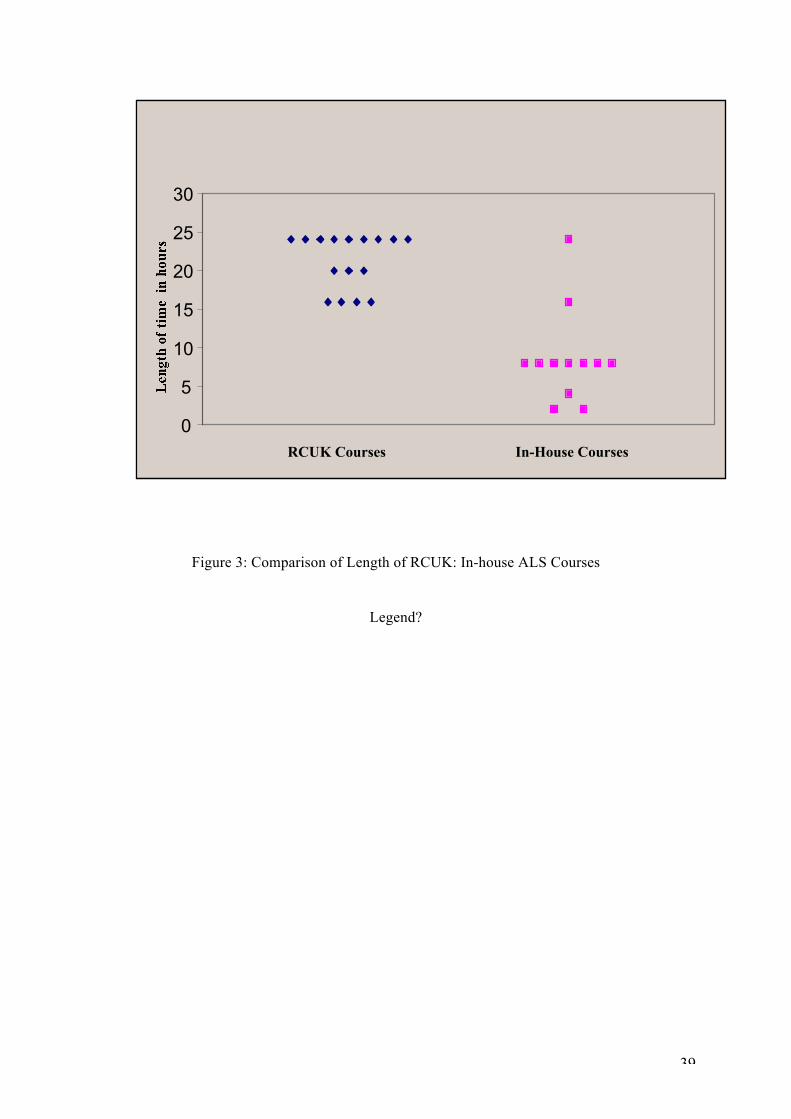
guidance. Our survey found that ‘in-house’ ALS courses are generally shorter than those
prescribed by the RCUK. Figure 3 illustrates this trend. Our survey also revealed that the
proportion of ‘Instructors to Candidates’ on courses was higher on RCUK ALS courses than
with in-house designed and operated ALS courses.
Hospital life support courses teaching manual defibrillation
Safe and effective manual defibrillation skills are required by medical staff that are
required to attend cardiac arrest calls, and those working in specialist fields (e.g.,
anaesthetics, coronary and intensive care), and by nurses working in specialist clinical areas
(e.g., coronary care, intensive treatment units and accident and emergency departments). The
RCUK recommends that staff requiring such training attend either the ILS or ALS course
(12). Where sites were unable, or did not wish to run the RCUK ALS course for these staff,
some reported that they ran the RCUK ILS course with manual defibrillation skills training,
while other sites reported that they ran their own in-house designed course to teach manual
defibrillation skills.

14

15
Table 1 demonstrates the results of the survey question posed by the team as to whether the
in-house designed hospital life support courses with manual defibrillation training may be
taught to a greater number of candidates than ‘nationally formally approved (franchised)’
hospital life support courses with manual defibrillation. Results demonstrate that a greater
number of candidates are taught an ‘in-house manual defibrillation’ course than with the
RCUK manual defibrillation course.
Other ‘Pre-arrest management courses’
Twenty-five (83%) out of thirty sites run a course in the recognition and management
of acutely ill patients. Twenty-three (76%) out of thirty sites run the ALERT™ course. A
course teaching the recognition and treatment of anaphylaxis was offered to clinical staff at
fourteen (47%) of the thirty sites surveyed. Rhythm recognition was taught, as a separate
course, to clinical staff at ten of the sites. A course teaching Altered Airway Resuscitation
was only taught at one of the thirty sites in our sample. None of the thirty sites surveyed
purchased courses from private companies. However five (17%) of the thirty sites ran the
RCSEng Advanced Trauma Life Support (ATLS®) Course.
FIGURE 3 GOES @ HERE
TABLE 1 GOES @ HERe

16
17
Narrative summary of survey of professional requirements
The General Medical Council (GMC), Nursing and Midwifery Council (NMC), nine
specialist medical colleges, ten colleges for Professions Allied to Medicine (PAMs), and four
medical/nursing support and representation bodies were included in this survey. Our detailed
findings are represented in Appendix 8 of the main report (13). Overall we noted an absence
of emphasis on life support training, other than a GMC recommendation on undergraduate
medical education. There were however three notable exceptions – the Royal College of
Anaesthetists and the Royal College of Paediatrics and Child Health, who require members to
be competent in advanced life support skills, and the Royal College of General Practitioners
(RCGP), which requires trainees to provide evidence of successful BLS training in order to
register.
Narrative summary of survey of UK medical schools
Data were successfully collected from associate, vice or sub-deans at twenty-one of
the twenty-four UK medical schools. More detailed results of this survey can be found in
Appendix 7 of the main report (13). An online undergraduate curriculum with information
about life support training was available from five medical schools. Fourteen sites responded
to our request for information, by email. Data were successfully obtained from four sites by
telephone. Life support training was provided at all twenty-one medical schools that
responded. In summary:
1. BLS was taught in 1st year at fifteen medical schools; in 3rd year at two sites and in
4th year at one 1 site.
2. ILS (RCUK) was taught in 3rd year at two sites. BLS and Defibrillation (non-RCUK)
was taught in 3rd year at three sites. ILS (RCUK) was taught in 5th year at seven sites.
3. ALS (RCUK) was taught in 4th year at three sites and in 5th year at four sites.
Advanced cardiac life support (ACLS/ non RCUK) was taught in 3rd year at one site.
18
Survey of the content and pedagogy of life support and ‘pre-arrest management’ courses Life support courses
The survey results are reported in Appendix 4 of our main report (13). The content
and pedagogy of the three well defined, widely accessible courses can be are in table 2. We
contacted the course providers to establish the number of each course type run annually, and
the number of candidates attending courses annually. In summary:
• The RCUK ILS and ALS courses; the Royal College of Surgeons ATLS® course; the
Advanced Life Support Group MedicALS, and ALERT™ were the most widely
taught courses. The most widely provided course of those surveyed was the RCUK
ILS, of which 1833 courses were held in 2002. In the UK a total of 16,880 people
attended ILS courses in 2002. Detailed results of this survey are contained in
Appendix 6 of the main document (13).
‘Pre-arrest management’ courses
Of the five courses identified, six course coordinators were contacted to complete the
telephone interview. Appendix 5 of the main report contains a detailed results table (13). Two
of the six courses surveyed were ALERT™ (18). There was little variation between the two
ALERT™ courses surveyed in pedagogy or content apart from the amount of time spent on
practical skills teaching. There was, however, considerable variation in the pedagogy and
content of the remaining four courses. Trainees on the ALERT, MedicALS and IMPACT
courses spend a large amount of the overall course time in practical skills training, whereas M
& K Update and CB Nursing Updates provide only theoretical/didactic teaching. ALERT™,
MedicALS and IMPACT courses provide a pre-course manual for candidates while M & K
Update and CB Nursing Updates do not.
The ratio of trainee to instructor also varies considerably. MedicALS, IMPACT and
ALERT have ratios of 2 to 4 trainees to 1 instructor, while M & K Update and CB Nursing
19
Updates both have ratios of 30 trainees to 1 instructor. Trainees on the MedicALS and the
IMPACT courses are assessed whereas the remaining courses had no assessment. The
ALERT™, M & K Update and CB Nursing Updates courses are aimed at a multidisciplinary
group, whereas the MedicALS and IMPACT courses are intended only for medical
practitioners. Trainees on all courses surveyed are able to claim Continuing Professional
Development points for attendance. It would seem that courses run by independent
commercial companies such as CB Nursing Updates and M & K Nursing Updates are
becoming increasingly popular. In 2002 alone, CB Nursing Updates ran 15 Acute Medical
Nursing Emergencies courses for a total of 600 nursing staff.
Fidelity of the Implementation of Courses
Immediate Life Support Courses (RCUK ILS)
ILS courses are provided and accredited by the RCUK. We surveyed a total of six ILS
courses from different hospital sites. Detailed results of this survey are contained in Appendix
4(a) of the main report (13). One site in the survey ran 2 different ILS courses. All our
sample courses had a pre-course manual, which was sent out to students in advance. Only
two of our sample courses altered their course content from that prescribed by the RCUK.
One course was aimed at final year medical students and the other course had two additional
lectures covering ‘do not attempt resuscitation’ policies, and clinical audit.
All sampled courses used the prescribed 4-stage teaching method (26) centred on
various clinical scenarios. All but one course used a 15-minute “Demonstration” exercise.
Two courses used “individual teaching” at skills stations, i.e., 1 instructor: 1 trainee, although
there was no requirement to do so. There was wide variation in the ratio of manikins to
trainees (1:2 to 1:5). Peer-led education was used in half of the surveyed courses. A formal
assessment process is not prescribed, although three courses incorporated a formal
assessment of skills such as defibrillation.

20
Advanced Life Support Courses
We surveyed five ALS courses franchised by the RCUK at 5 different hospital sites.
Detailed results are presented in table form in Appendix 4(b) of the main report (13). All our
sample courses provided a pre-course manual, which was sent out to students in advance. No
variation in course content was seen between prescribed and sampled courses. Some variation
in pedagogy was found. One course simplified the course content and modified the prescribed
RCUK teaching algorithms. Whilst there is no requirement for 1:1 teaching, two courses
adopted 1:1 teaching at skills stations, arguing that this was essential to ensure proper transfer
of skills. Three of our sampled courses took twice as long (30 minutes) with
“Demonstrations”, compared to the prescribed 15 minutes. All courses surveyed used the
prescribed 4-stage teaching methods centred on various clinical scenarios (DETAILS)? Peer-
led education was used in all our surveyed courses. All surveyed courses assessed four basic
skills using a written assessment based on one or more clinical scenarios.
Advanced Trauma Life Support Courses
ATLS® courses are purveyed and prescribed by the Royal College of Surgeons of
England (RCSEng). We surveyed five ATLS® courses from different hospital sites. Detailed
results of this survey are presented in Appendix 4(c) of the main report (13). All courses in
our sample had a pre-course manual sent out to students in advance. None of our sample
courses altered their course content from that prescribed by the RCSEng.
Some variation in pedagogy was found. All but one (citing time constraints) of our
sampled courses used the prescribed 4-stage teaching method centred on various clinical
scenarios. Whilst the franchised course does not prescribe 1:1 teaching, three sites adopted a
1 instructor to 1 candidate ratio, if the instructors thought a candidate would benefit from
additional practical skills training in a skills station. One of the courses surveyed employed
actors to play patient roles, whereas the remainder used a manikin. Four of the courses used
21
animal cadavers, but one did not. Education staff at the RCSEng, who were interviewed state
that animal cadavers need not be used, although the ATLS® manual indicates their use.
There was no variation in the mode of assessment and the number of skills assessed in our
sample courses.
DISCUSSION
Our study demonstrated that resuscitation training has become a widespread activity
across the UK hospital trusts, with courses available across a diverse range of situations.
Courses range from BLS for carers of people with heart disease to deep-sea diving courses.
Within hospitals it is now ‘institutionalised’ in the sense that permanent posts exist at most
centres and large numbers of staff attend courses. Indeed the coverage within hospitals is far
more comprehensive than in medical schools or professional colleges, suggesting that the
NHS, far from responding to the educational and standard setting bodies, has led the way. We
have no doubt that organisations such as the RCUK have been very influential in mentoring
this process.
One of our most striking findings is the extent to which ‘pre-arrest’ courses teaching
recognition and management of the deteriorating patient have caught on; the finding that
nearly half of all unexpected cardiac arrests are preceded by clear evidence of deteriorating
physiology to which no response is made, has been taken to heart. Research evidence is
currently being generated to measure the impact this has on mortality and morbidity, with a
real possibility existing that this will help reduce the number of both events and inappropriate
admissions to intensive care (16).
The team interviewed staff from independent commercial companies about the
number of nursing staff taking up places on their courses. One possible reason for the high
uptake of these two courses could be the relatively low cost for course attendance in
comparison to other courses, and that they provide practitioners with Continuing Professional
22
Development points for attendance. Our survey revealed that only didactic teaching was used
to teach these courses. Given the emphasis that other course developers and educationalists
place on the use of practical skills training (12) the research team feel that questions remain
about the suitability or effectiveness, of courses offering only large-group lecture-based
teaching (29). Recent direction from one of the main providers (RCUK) demonstrates the
importance of adult learning principles shaping curriculum delivery, with high candidate
participation, experiential tools (standardized patients and simulation) and interactivity.
While the above courses might be insufficiently intensive many other courses may err
in the opposite direction. This applies particularly to the franchised RCUK courses. The
evidence we have presented shows that many hospitals prefer to run in house courses that are
less expensive in direct costs and in staff time. For example the RCUK ALS course, at the
time of the survey, involved 3 days of intensive training. There is some research evidence
(from educational theory) and direct evidence (from randomised trials) (13), casting doubt on
the benefits of such ‘deep immersion’ courses over shorter, modular (spaced) courses.
Although there is a very wide range of pre-existing knowledge and skill of
multidisciplinary staff undertaking some life support courses, it was interesting to note that of
all courses surveyed, only two sites tested the pre-course (baseline) knowledge and skill of
candidates. The recent ILCOR Advisory Statement on Education in Resuscitation (30)
emphasizes the importance of adapting course contents and teaching methods to the needs of
the candidate group being taught. Where there is no prior knowledge of a candidate’s skill
level a short baseline measure, or pre-test, provides instructors with the necessary knowledge
about a candidate’s training needs. Applying the same pre- and post-course test would also
provide useful feedback to instructors and researchers on the effectiveness of the course
contents as indicated by measurable behavioural change, i.e., practical life support skills

23
acquisition and retention. Assessing the knowledge, skills and attitudes of the trainees would
help increase the chances of positive outcomes and sustained gains.
Although it was not a primary aim of the study, the research team was interested in
the efforts of course providers to update the life support treatment and management evidence
base of the course contents. ILCOR, the ERC and the RCUK, provide a good example of
groups working to provide a contemporary evidence base for clinicians. This evidence is
disseminated at a clinical level through the work of NHS trust resuscitation officers and
others involved in the teaching of RCUK courses. In a meeting with management staff of the
ALSG, the team discovered that the contents of courses is continually updated as new
evidence emerges. On completing an ALSG course, candidates are advised to log on
regularly to the BestBETS website (31) to update their knowledge.
What should be taught and to whom?
The need for life support skills is an issue faced by all healthcare professionals, not
just those who form emergency teams. Given that most clinicians will seldom be called upon
to do life support and that skills decay, a basic set of ALS skills must be taught to a wide
community while a smaller number receive training in a more extensive advanced skill set. A
recent ILCOR advisory statement on Resuscitation in Education (32) after an extensive
review of life support teaching studies, recommended the development of evidence-based,
educationally sound basic life support courses targeting providers that would be most likely
to attend a cardiac arrest. The idea of organisational training needs assessments also emerges
very strongly in the Salas and Cannon-Bowers review on the science behind training (33).
The challenge facing the training community is in targeting training to reflect the range and
scope of individual clinician’s clinical practice and required competencies.
The number of Resuscitation Officers (ROs or RTOs) has increased over the past 10
years and most hospitals now have a Resuscitation Service. The level and type of life support
24
courses used to train various grades of hospital staff is decided by trust Resuscitation
Committees. These are strongly influenced by the European Council Guidelines on Basic and
Advanced Life Support. BLS forms the major part of the standard level of resuscitation
training in most hospitals (34).
We found that:
1. When a hospital sets out to deliver a package of training they do so in a very
homogeneous way, both with respect to content and pedagogy.
2. There is considerable disagreement over who should receive which package. While
some hospitals (such as hospital 8 in our study) provide over 500 training slots per
year in BLS, but only a handful of slots at a more advanced level. Others, such as
hospital 9, offer many opportunities in immediate life support. Indeed, hospital 9
stopped using BLS and provides only ILS or ALS.
This invites the obvious question – should AED training be incorporated into all BLS
training courses thereby effectively converting them to ILS courses? The idea is supported by
the epidemiology - resuscitation is at least four times more successful when carried out in the
context of a shock-responsive rhythm than in other circumstances. Moreover, standard
monitors contain the ‘intelligence’ to discern such rhythms (35). It seems almost perverse to
install defibrillators in airports, stations, and shopping malls yet not make such equipment
available in acute hospital settings. Even if the proportion of cardiac arrests that have a
shock-responsive rhythm is higher in pre-hospital cases, than in hospital, the absolute
numbers in hospital are likely to be higher. Moreover the outcomes of cardiac arrest on the
wards have improved substantially since the installation of AEDs, and training in their use
was instituted, at the Hammersmith Hospital (36). We feel that all staff should be trained in
ILS pending much more widespread introduction of AED in hospitals. The controversy over
whether attempted defibrillation should be preceded or followed by chest compressions does
25
not need to be resolved in order to reach the conclusion that AED should be part of the most
basic life support training repertoire.
Historical precedent should no longer be allowed to dictate the provision of facilities
for defibrillation in hospitals. While defibrillation programmes have traditionally been
limited to critical care areas where nurses and physicians work together in recognising and
treating ventricular defibrillation, we think that defibrillators should now be more widely
available. These decisions should be informed by a detailed process mapping of needs
coupled with cost-effectiveness modelling. Early indications from the Department of Health
National Defibrillation Programme suggest that such a widespread provision would be cost
effective. Further work in this area is needed. The traditional idea that staff outside the
critical care area would be trained only to maintain the circulation until the arrival of the
resuscitation team is no longer defensible. Given that the success of defibrillation depends
more on the duration of ‘downtime’ than on the expertise of the practitioner (especially with
modern devices) it would seem sensible to make defibrillators more widely available.
A larger question is whether all clinical staff could be trained to provide such
widespread defibrillation cost effectively. Kaye and colleagues (37) have demonstrated that
staff located outside the critical care wards can easily be trained to use AEDs. Indeed staff
that had already been trained in BLS whether qualified or not can be trained to use AEDs in a
2-hour class. In short, little more is required than political will to modify existing courses
which staff are expected to take. Would it be cost effective to follow the policy explicated
here? We have argued that including defibrillation training in the repertoire of BLS would be
inexpensive, and the price of AEDs has fallen rapidly in recent years. Such modelling would
require an estimate of the frequency with which defibrillation is required on the general
wards along with estimates of the marginal gains in survival through the availability of local
AEDs. A single study in Italy (38) reports that 24 patients required resuscitation in the first 9

26
months following implementation of a first responder AED program. Nine of these patients
were in ventricular defibrillation and three survived to discharge. The research team
recommended that the NPSA convene a series of stakeholder meetings to develop a national
policy on this issue (13). We have recommended that a formal cost-effectiveness model be
commissioned to inform this point.
Conclusions
A large cottage industry has grown around the provision of life support courses.
Individual hospitals provide many original in-house courses and also purchase training via
external providers who franchise a smaller number of validated courses, e.g., RCUK ALS
and ILS courses. Most courses are associated with high opportunity costs such as requiring
staff to attend during work hours. As educational interventions, these courses have limited
evaluation in the same way as many other services for either effectiveness or cost
effectiveness.
Studies evaluating courses to teach life support have found that the effect on patient
mortality has not been measured with great precision. Any improvement appears to be
modest perhaps as a result of the well-documented decay in acquired skills. Inappropriate
cardiac arrest interventions in an ageing population in the absence of clear resuscitation status
decisions may also be a contributory factor. Recent trends are far more encouraging
following the emergence of the AED, supported by the wide spread training provision
discussed in this paper. Finally, having national courses based on accepted published
standards with defined regulations and assessments allows healthcare professionals to have
transferable skills between and across organizations.
Before and after studies show that knowledge improves and participants enjoy the
courses. Traditionally courses have been based on Basic, Immediate and Advanced skills.
Epidemiology shows that defibrillation is the most effective life support skill so this needs to
27
be introduced at the most basic level, along with increasing availability of AEDs. Individual
trusts, based on national minimum published standards should define the level of
defibrillation competency expected. Of the provision in the UK: there are a small number of
market leaders for the main externally franchised courses. These are implemented with great
fidelity when compared with the written curriculum description. Nationally, simulation
centres have been established to provide training and research opportunities. There has been a
large (and we think welcome) increase in uptake of ‘pre-arrest’ courses.
Overall, the courses are consistent with theory but there are still some unanswered
questions, for example: What is the optimum intensity and duration of courses? How well do
skills in the lab translate into actual clinical practice? What is the role of experiential learning
tools? How best to sustain this knowledge? How best to train teams of providers?

28
Acknowledgements
We would like to acknowledge and thank the following individuals for their significant
contribution to this project:
o Members of The Resuscitation Council UK in London - Sarah Mitchell, Jerry Nolan
o Members of The Advanced Life Support Group in Manchester – Sue Wieteska, Mike
Davis - assisted the research team by meeting to describe the organisation and
function of the ALSG, and by providing a matrix of course details.
o Representatives of the Royal College of Surgeons of England – Samantha Dilgert,
ATLS/PHTLS Coordinator; Judy Murfitt, BST Course Manager met with members of
the research team to provide details of the courses run by the RCSEng and to describe
the function and organisation of their education department.
o Gary Smith Consultant in Intensive Care Medicine, Honorary Senior Lecturer in
Critical Care, Portsmouth Hospitals NHS Trust & School of Postgraduate Medicine &
Director of the ALERT Course
o Above all, we thank the National Patient Safety Agency (NPSA) who sponsored the
study.
29
References
1. Ebell M, Becker L, Barry H, Hagen M. Survival After In-Hospital Cardiopulmonary
Resuscitation. A Meta-Analysis. Journal of General Internal Medicine 1998;13(12):805.
2. Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, et al.
Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests
from the National Registry of Cardiopulmonary Resuscitation. Resuscitation
2003;58(3):297-308.
3. Rudiger A, Tobler D, Estlinbaum W. Frequency and outcome of in-hospital resuscitation
outside the ICU-setting. Swiss.Med.Wkly. 2004;134(3-4):59-62.
4. Dane FC, et al. In-hospital resuscitation: association between ACLS training and survival to
discharge. Resuscitation 2000;47:83-7.
5. Gwinnutt CL, Columb M, Harris R. Outcome after cardiac arrest in adults in UK hospitals:
effect of the 1997 guidelines. Resuscitation 2000;47(2):125-35.
6. Lowenstein SR, Sabyan EM, Lassen CF, Kern DC. Benefits of training physicians in
advanced cardiac life support. Chest 1986;89(4):512-6.

30
7. Sandroni C, Ferro G, Santangelo S, Tortora F, Mistura L, Cavallaro F et al. In-hospital
cardiac arrest: survival depends mainly on the effectiveness of the emergency response.
Resuscitation 2004;62(3):291-7.
8. Treanor G, Spearpoint K, Brett S. Survival from in-hospital cardiac arrest: the potential
impact of infection. Resuscitation 2005;64(1):59-62.
9. European Resuscitation Council. European Resuscitation Council website. 10-13-2003.
10. American Heart Association. ILCOR statements. American Heart Association
website.Searchword: ILCOR . 2003.
11. Klein HH, Arntz HR. Perspectives and new approaches for improving cardiopulmonary
resuscitation in adults beyond current guidelines. Z.Kardiol. 2004;93(1):18-22.
12. Cardiopulmonary resusciation standards for clinical practice and training in the UK.
Resuscitation 2005;64(1);13-19.
13. Barach P, Bentham L, Bion J, Bradburn S, Bullock I, Daniels H, Fawdry R, Lilford R, and
Mohammed MA. Teaching life support and resuscitation competencies in health care –
current practice and strategies for future research. 2005. London, National Patient Safety
Agency. 4-19-2005.

31
14. Medical Emergency Team, Simpson Centre for Health Service Innovation L. H. S.
Implementation of the MET system into your hospital. Simpson Centre. 1999. Simpson
Centre, South Western Sydney Area Health Service. 5-19-2005.
15. Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospital
cardiopulmonary arrest. Chest 1999;98(6):1388-92.
16. Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of
antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia
and New Zealand, and the United Kingdom--the ACADEMIA study. Resuscitation
2004;62(3):275-82.
17. Smith AF, Wood J. Can some in-hospital cardio-respiratory arrests be prevented? A
prospective survey. Resuscitation 1998;37(3):133-7.
18. Smith GB, Osgood VM, Crane S. ALERT--a multiprofessional training course in the care
of the acutely ill adult patient. Resuscitation 2002;52(3):281-6.
19. Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart G, Opdam H et al. Prospective
controlled trial of effect of medical emergency team on postoperative morbidity and
mortality rates. Crit Care Med 2004;32(4):916-21.
32
20. Royal College of Physicians of London. Working Party Report August 5th 2002: The
interface between Acute General Medicine and Critical Care. Recommendations. 2002.
21. Resuscitation Council (UK). The Acute Care Undergraduate TEaching (ACUTE) initiative.
Resuscitation Council (UK). 1-11-2004. 2-16-2004.
22. Department of Health. NHS England acute bed list.
www.doh.gov.uk/hospitalactivity/data_requests/download/beds_open_overnight/bed_03_su
mmary.xls . 2003.
23. www.helpdoctor.co.uk. UK Medical Schools. www.helpdoctor.co.uk . 11-18-2002. 11-18.
24. Woods M. First Aid Training: Retention of Skills and Knowledge. A Summary of the
Literature [dissertation]. Medical Sciences Unit, Health and Safety Executive; 2002.
25. Resuscitation Council UK. Immediate Life Support Course Manual. 1st Edition. 2002.
26. British Medical Association. Pocket Guide to Teaching for Medical Instructors. London:
BMJ Books; 1999.
27. Resuscitation Council UK. Advanced Life Support Course Manual. London: Resuscitation
Council UK; 2000.
33
28. American College of Surgeons. Advanced Trauma Life Support Instructor Course Manual.
6thed. Chicago: American College of Surgeons; 1997.
29. Baker DP, Salas E, King H, Battles J, Barach P. The role of teamwork in the professional
education of physicians: current status and assessment recommendations. Jt Comm J Qual
Patient Saf 2005;31(4):185-202.
30. Chamberlain DA, Hazinski MF. Education in resuscitation. Resuscitation 2003;59(1):11-
43.
31. The Emergency Department, Manchester Royal Infirmary. BestBETS. Advanced Life
Support Group. 10-21-2003.
32. Chamberlain DA, Hazinski MF. Education in resuscitation. Resuscitation 2003;59(1):11-
43.
33. Salas E, Cannon-Bowers JA. The science of training: a decade of progress. Annu Rev
Psychol. 2001;52:471-99.
34. Handley AJ, Bahr J, Baskett P, Bossaert L, Chamberlain D, Dick W, et al. The 1998
European Resuscitation Council guidelines for adult single rescuer basic life support: A

34
statement from the Working Group on Basic Life Support, and approved by the executive
committee. Resuscitation1998;37(2):67-80.
35. Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O'Hearn N et al. Quality of
cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA 2005;293(3):305-
10.
36. Spearpoint, K. AEDs and Hammersmith Hospital. 2005. 2-17-2005.
37. Kaye W, Mancini ME, Giuliano KK, Richards N, Nagid DM, Marler CA, et al.
Strengthening the in-hospital chain of survival with rapid defibrillation by first responders
using automated external defibrillators: training and retention issues. Ann Emerg.Med
1995;25(2):163-8.
38. Destro A, Marzaloni M, Sermasi S, Rossi F. Automatic external defibrillators in the
hospital as well? Resuscitation 1996;31(1):39-43.

35
TABLES AND FIGURES
Table 1. Comparison of Franchised (RCUK) manual defibrillation candidate numbers with
In-house candidate numbers
Site Number
Candidate Numbers (02-03)(Franchised)
Site Number
Candidate Numbers (02-03 )(In-house)
1 210 1 180 2 72 2 84 3 48 4 330 4 96 6 90 6 120 5 120 7 180 8 1248 8 120 9 175 9 432 10 180 11 48 11 250 12 384 13 36 13 288 14 36 14 240 15 72 15 72 16 96 16 336 17 20 17 32 18 120 18 210 19 144 20 48 22 192 21 180 23 282 22 150 24 36 30 84 27 180
Total 3350 (46.39%) Total 3871 (53.60%)

36
Course Key
Features Candidates Instructor:
Student ratio Duration Theory:
practical training
Assessment
RC ILS Ambu bag AED Role Play Teamwork
30 1:6 1 day
1:5 Written
RC ALS
ILS plus Leadership, drugs, arrthymias Simulation Peer-led education
30 1:3 3 day 1:4 Written 4 skills
RCS ATLS
ALS plus teamwork
20 1:2 3 day 1:4 Written Oral on 12 key tasks
Table 2—Comparison of the 3 main resuscitation courses

37
Figure 1. Schematic representation of the increasing focus of this research programme, beginning with a general summary of all courses and working toward a survey of pedagogic detail of particular courses
Project 1. A broad survey of all courses teaching life support for clinicians, specialist
groups and the public, currently
available in the UK.
Project 2. A survey of adult life support courses offered in UK hospitals
and medical schools, and of the life support training requirements set by
professional bodies. Summary of ‘pre-arrest management courses’.
Project 3. Detailed analysis of the contents and pedagogic methods of
the most widely purveyed adult life support courses in
England.
Project 4. A study of the
fidelity with which the
prescribed courses are
implemented in
England.

38
Figure 2. Survey of Adult Life Support Courses provided by NHS hospitals
-50
50
150
250
350
450
550
Sites surveyed
Num
ber
of C
ours
es fr
om D
ec 2
002
to D
ec 2
003
Basic Life Support 348 104 340 10 348 100 216 520 0 159 312 362 48 26 96 120 126 156 200 100 100 404 260 213 0 350 50 220 349 16
Immediate Life Support 48 167 24 18 40 114 67 12 276 70 60 24 25 29 12 24 6 22 0 24 69 72 41 53 0 30 15 260 12 15
Advanced Life Support 7 3 2 14 12 4 6 108 7 30 2 8 2 11 15 4 2 3 12 2 4 5 12 18 0 0 2 0 4 2
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
39
0
5
10
15
20
25
30
RCUK Courses In-House Courses
Figure 3: Comparison of Length of RCUK: In-house ALS Courses
Legend?