restorative reproductive medicine during this era of healthcare reform: opportunities emerge paul a....
TRANSCRIPT

Restorative Reproductive Medicine During this Era of Healthcare Reform:
Opportunities Emerge
Paul A. Carpentier, MD, CFCMCAccountable Care Associates,
In His Image Family Medicine, andConsultant to the National Gianna Center for Women’s Health and FertilityFormer President of the American Academy of FertilityCare Professionals
Gardner, Massachusetts, USA

Faculty Disclosure
• I have no financial conflicts of interest– Dr. Carpentier

Objectives
• Understand key events during the unfolding healthcare reform movement in the U.S.
• Examine how this could foster the adoption of Restorative Reproductive Medicine (RRM)
• Learn about the economic structure of ACOs• Evaluate potential benefits and pitfalls in
fostering restorative reproductive medicine

The Massachusetts Test-Kitchen
‘Romney-care’ precedes ‘Obamacare’By six years

Romney-Care
• Governor Mitt Romney plans for reform, why?– Too expensive– Not much quality for the price– Jeopardizing other state services– Employers crushed by premiums– So many people without coverage– Emergency rooms misused

Romney-Care
• Step one– Give everyone insurance
• Step two– Figure the rest out later!
• On someone else’s watch• A new legislature
– Let the pressures for change mount• Further understand the crisis• Employers deflect more costs to the employees

Result
• Emergency rooms overrun• PCPs still not utilized• Still uninsured and now underinsured• Hospitals fewer but somewhat stronger
– Doctors and hospitals joining forces– Attorney General anxious
• Employers still not happy• Cities cutting services or nearly bankrupt

Consequences to name a few
• Healthcare Policy Commission Established– Autonomous– Appointed by the governor (Patrick)– One task only – to restrain the rate of rise of costs
• Physician Assisted Suicide narrowly defeated• Legislated coverage of infertility services (IVF)
– But not for Medicaid population– IVF centers become financially powerful
• Insurance companies pass more cost to pt– They become stronger but self spending curbed

Meanwhile
• Wise husband and wife* family physicians in western Massachusetts realize that managing care with quality goals saves money and improves outcomes (greater value)
• They develop IT infrastructure to boil down insurers’ “Big Data” into a usable form right in the doctors’ exam room
• Two insurers are intrigued and launch pilot studies using their tools and care coordinators
* Drs. Philip Gaziano and A. Felicitas Thurmayr, Springfield, MA
Amazing Results
• Improved awareness of the chronic conditions of the complex patients
• PCPs empowered to deliver better results• Much higher quality
– First Massachusetts increase in three decades!– The Two insurers were flabbergasted
• Significantly lower costs– Beyond the benchmarks!

Why better results?
• Chronic diseases were handled with chronic approaches rather than acute care
• Solutions were sought to better manage these chronic diseases
• Acute care is expensive and fails for chr. dis.• Hospitals are oriented to acute care• Chronic diseases are better managed by PCPs
This confirms Dr. Stanford’s intuitions last year (IIRRM Presentation)

Small Practices are Critical Piece
• More responsive to their community• More flexible• Better continuity• Every 1% increase in continuity causes 5%
increase in quality• This is now being recognized
• Most NaPro physicians are in small practices

What does this have to do with RRM?
A Light is Ready to Dawn

Infertility is a chronic disease!
• Acute treatments do not serve chr dis well• Acute treatments are expensive• Pharmaceutical companies remain powerful• And now IVF companies are wealthy• But Commissions, attorneys general and ACOs
are poised to cut cost, power and favor chronic care management for the economic wellbeing of the country

Episodes of Care
• The cost of various options of treatment for an illness can be described as an ‘episode of care’
• For example:– A patient with a cough presents to the ER versus
• CXR, labs, prolonged stay, high utilization, no continuity
– A patient with a cough presents to their PCP• Well known, minimal care needed, same outcome
• Quality Cost Value!!!
Episode of Care
InfertilityTreated by IVF vs NaProTECHNOLOGY
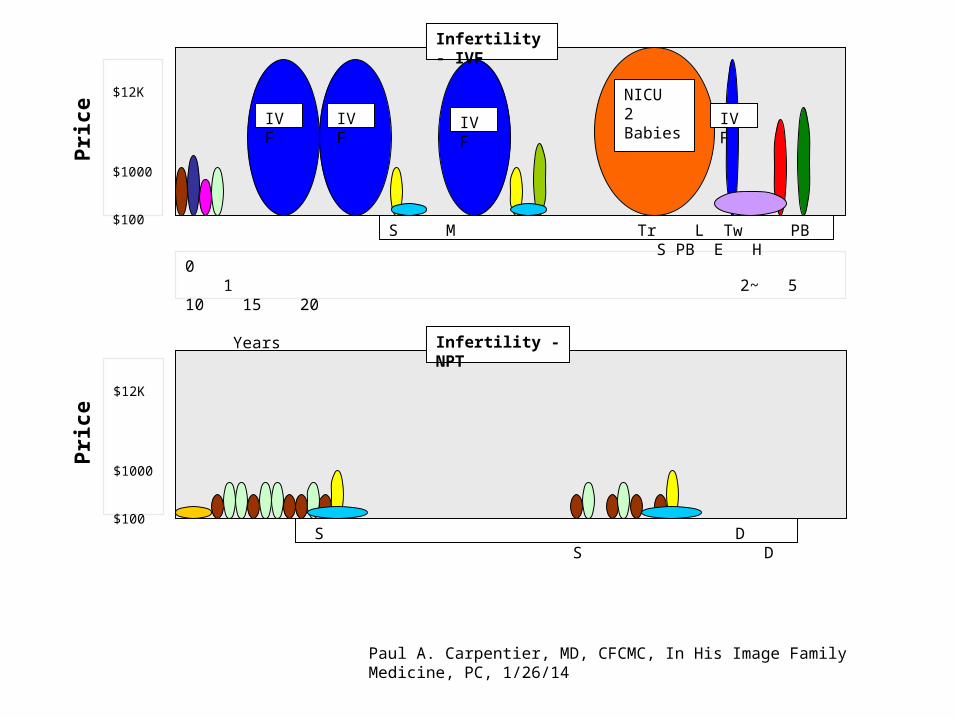
$12K
$1000
$100
0 1 2~ 5 10 15 20 Years
Infertility - IVF
S M Tr L Tw PB S PB E H
IVF
Pri
ce
IVFIVFIVF
NICU2 Babies
Infertility - NPT
S D S D
$12K
$1000
$100
Pri
ce
Paul A. Carpentier, MD, CFCMC, In His Image Family Medicine, PC, 1/26/14

= Doctor Evaluation
= HSG
= Semen analysis
= Lab Tests
= Ultrasound Pelvis
= progesterone support
= Monitoring Loss of One Fetus
= 2 Premature NICU Stay > Month
= Cost of Chronic Illness of Twins
= Endometrial Ablation - DUB
= Hysterectomy / BSO
= FertilityCare Training
OCCURENCESS = Single PregnancyTr = Triplet PregnancyL = Loss of one fetusTw = Twin PregnancyM = MiscarriagePB = Premature BirthE = Endometrial AblationH = HysterectomyD = Normal Delivery
Height of Bubble = CostWidth of Bubble = Time
Ave time to preg with NPT = 6.4 mos; almost always singleton
Paul A. Carpentier, MD, CFCMC, In His Image Family Medicine, PC, 1/26/14
Episode of Care - Key

Obamacare Occurs (ACA)
• National Affordable Care Act• Actually a motivation and mechanism to
change the macro-system• Complicated by the fact that the
administration planted their agenda within it– Abortion– Contraception– Protecting pharmaceutical companies

Obamacare Occurs (ACA)
• Fosters the development of Accountable Care Organizations
• These strive to:– Integrate care– Make physicians liable for the entire cost of their
patients’ care– Manage a patient population as well as individuals– Maintain quality while restraining costs

The Stage is Set
for an enlightened perspective toward infertility management and
other gynecological disorders

Restorative Reproductive Medicine
Gaining Traction!

Infertility is a Chronic Disease
• As are many other Gyn problems• They need to be addressed as so
– Quality will improve– Outcomes should improve– Costs should be less
• This will catch the ear of insurers, ACOs and governmental programs
• Lets glance at a few examples of outcomes

New Opportunities in Fallopian Tube Repair:
Effective and Economical Alternatives to IVF
Cara Buskmiller, MSII; Institute of Bioethics and Patient
Care Advancement
A great example from a poster session, Catholic Medical Association, 2013:

ASRM Changes Their Opinion!
• In 2012, the American Society for Reproductive Medicine (ASRM) edited their opinion on tubal surgery, prioritizing fallopian tube repair (FTR, a.k.a. tuboplasty, recanalization) over in-vitro fertilization (IVF) for young women with tubal factor infertility.
• This shift heralds a potential change in mainstream reproductive medicine.
• This presentation compares the cost and effectiveness of IVF with currently available, ethically undisputed techniques of fallopian tube repair.

Detailed Results
HYST=hysteroscopic, LAP=laparoscopic, LEC=linear everting catheter, SS=selective salpingography

The highest pregnancy rate of all techniques
• 55% success with laparoscopic-hysteroscopic fallopian tube repair
• Also competitive were hysteroscopic-only repairs including falloposcopic repair
1. ASRM: The role of tubal reconstructive surgery in the era of assisted reproductive technologies. Fertil Steril 2008;90:S250-3.
2. Update of above, in Fertil Steril 2012;97:539-45.3. ASRM online FAQ, Question 6.4. Health Care Blue Book (healthcarebluebook.com)5. Allahbadia GN, Merchant R: Fallopian tube
recanalization: lessons learnt and future challenges. Womens Health. 2010 Jul;6(4):531-48.
6. Anil G et al: Fluoroscopy-guided, transcervical, selective salpingography and fallopian tube recanalisation. J Obstet Gynaecol. 2011 Nov;31(8):746-50.
7. Tanaka, Y, Tajima, H: Falloposcopic tuboplasty as an option for tubal infertility: an alternative to in vitro fertilization. Fertil Steril. 2011 Jan;95(1):441-3.
8. Das S et al: Proximal tubal disease: the place for tubal cannulation. Reprod Biomed Online. 2007 Oct;15(4):383-8.

Methods (To answer your questions on the sources of the data, $)
• “FTR techniques were considered viable IVF alternatives which appeared in literature published since 2004 and which reported intrauterine pregnancy rates of over 20%.
• These were compared with 2009 CDC data on one cycle of IVF. • Estimated costs were based on publicly-available data.” 3, 4
We’ll not discuss this in the interest of time

Infertility after Endometriosis Surgery
• After endometriosis surgery, this study demonstrated better pregnancy rates for spontaneous attempts versus ovarian stimulation/IUI
• (Summary by Dr. Kyle Beiter, personal communication)• J Minim Invasive Gynecol. 2014 Jan-Feb;21(1):101-8. doi: 10.1016/j.jmig.2013.07.009. Epub
2013 Jul 31
• SETTING: Cleveland Clinic Foundation, tertiary care center
Another Key Example

For your reference (not to be reviewed today)
• J Minim Invasive Gynecol. 2014 Jan-Feb;21(1):101-8. doi: 10.1016/j.jmig.2013.07.009. Epub 2013 Jul 31.
• Determining the fertility benefit of controlled ovarian hyperstimulation with intrauterine insemination after operative laparoscopy in patients with endometriosis.
• Gandhi AR1, Carvalho LF2, Nutter B3, Falcone T4.• Author information • 1Cleveland Clinic, Cleveland, Ohio; Cleveland Clinic Lerner College of Medicine of Case Western
Reserve University, Cleveland, Ohio.• 2Department of Obstetrics and Gynecology, São Paulo University, São Paulo, Brazil.• 3Cleveland Clinic, Cleveland, Ohio.• 4Cleveland Clinic, Cleveland, Ohio; Cleveland Clinic Lerner College of Medicine of Case Western
Reserve University, Cleveland, Ohio. Electronic address: [email protected].• Abstract• STUDY OBJECTIVE: • To determine the fertility benefit of controlled ovarian hyperstimulation (COH) and intrauterine
insemination (IUI) in surgically treated endometriosis.• DESIGN: • Retrospective cohort study (Canadian Task Force classification II-2).

For your reference (not to be reviewed today)• SETTING: • Cleveland Clinic Foundation, tertiary care center.• PATIENTS: • Ninety-six women of reproductive age who underwent operative laparoscopy to treat endometriosis-related
infertility (endometriosis stage I/II n = 67; stage III/IV n = 29) from 2001 to 2011 at the Cleveland Clinic Foundation.• INTERVENTIONS: • COH via letrozole, clomiphene, or gonadotropins, with or without IUI.• MEASUREMENTS AND MAIN RESULTS: • Kaplan-Meier estimations of cumulative pregnancy rates were compared by stage between COH/IUI and
spontaneous cycles. Patients with stage I/II endometriosis attempted spontaneous pregnancy for 669 months and 216 COH + IUI cycles, and patients with stage III/IV endometriosis attempted spontaneous pregnancy for 379 months and 74 COH + IUI cycles. Crude pregnancy rates were 45.7% in stage I/II and 40.5% in stage III/IV. Twelve-month cumulative pregnancy rates in stage I/II were 45% for spontaneous attempts and 42% for COH + IUI, and in stage III/IV were 20% for spontaneous attempts and 10% for COH + IUI (not significant). Cumulative pregnancy rates for COH/IUI in stage I/II were significantly higher than in stage III/IV. Monthly fecundity rates were 3.81% for stage I/II spontaneous, 4.59% for COH/IUI, 3.05% for stage III/IV spontaneous, and 1.68% for COH/IUI (not significant).
• CONCLUSIONS: • COH + IUI did not improve pregnancy rates in any stage of endometriosis. In stage III/IV we recommend
postoperative in vitro fertilization.• Copyright © 2014 AAGL. Published by Elsevier Inc. All rights reserved.• KEYWORDS: • ASRM staging system; Controlled ovarian hyperstimulation; Endometriosis; Intrauterine insemination; Laparoscopy• PMID: 23911563 [PubMed - indexed for MEDLINE]
RRM

Value-based Care
• Value Quality Cost
• Accountable Care Organizations make the physician ‘accountable’ for the value of the care that he or she delivers– Financially– Quality Outcomes

Value-based Care
• High Quality includes– Outcomes
• Compared to other approaches• Patient satisfaction• Ethics could be factored, based on the design
– Increased focus lately on Cultural Competence– Increased focus on ethics and religious freedom
– Reporting– Meeting Thresholds– Access, timeliness, meeting standards

Cost EffectivenessValue!
NaProTECHNOLOGYvs
Artificial Reproductive Technologies
Produced by Pope Paul VI Institute for the Study of Human Reproduction
2004

Cost Effectiveness
InfertilityCost per cycle (2004 data)
NaProTechnology $ 322IVF $ 9,226
Cost of prematurity (NICU stay)Severe $500,000
Cost of Twins (maternal, compared to singleton pregnancy) 2 x
Cost of Triplets (maternal, compared to singleton pregnancy) 5 x

Success Rates
Prematurity
Prematurity RatePope Paul VI Institute 7.0% 3.6%Traditional Care 12.1%
Severe Prematurity RatePope Paul VI Institute 1.3%Traditional Care 3.9%

Success RatesLive Newborn Rates in Infertility (Due to):
EndometriosisPope Paul VI Institute 56 - 76%Johns Hopkins Surgical Approach 57%IVF (one cycle)21%
Polycystic Ovarian DiseasePope Paul VI Institute 63 – 80%Johns Hopkins Surgical Approach 42%IVF (one cycle) 26%
Tubal OcclusionPope Paul VI Institute 38%IVF (one cycle) 27%
Recurrent MiscarriagePope Paul VI Institute for the Study of Human Reproduction 79% DeliverTraditional (wide ranges reported but all are) Fewer

Success Rates
Post Partum DepressionPope Paul VI Institute 97%
over 1-10 daysTraditional (antidepressants and anxiolytics) slow improvement
over 6-12 months
Premenstrual Dysphoric Disorder (PMS)Pope Paul VI Institute 95%Traditional (antidepressants) 43%
Hysterectomy Rate for Chronic Pelvic PainPope Paul VI Institute 12%Traditional Approach 40%

Signs of Hope
Gianna CenterAccountable Care Associates
Dr. Patrick Yeung’s Center

The National Gianna Center for Women’s Health and Fertility
•“She hopes that couples struggling with infertility who might be thinking of IVF will discover that ‘there is an alternative that is effective, less expensive and morally acceptable that will allow them to conceive through a natural act of intercourse.’”•The Gianna Center accepts most major medical insurance plans including Medicaid.
“New women's health center offers reproductive care, gynecology”
Catholic New York — December 31, 2009
Anne Nolte, MD, CFCMCRon Rak, CEO, St. Peters Univ Hospital
Michele GiuilianoKyle Beiter, MD, CFCMC

Accountable Care Associates
• Phil Gaziano, MD – Visionary in Healthcare reform
• Innovation in Info Technology – Feli Thurmeyer, MD
• Largest National ACO• World Leading Care Management
– Patient is a person!– Physician/Pt relationship is precious
• Highest Quality in the Nation• Reducing Expenditures Tremendously

Accountable Care Associates
• Therefore, insurers are Coming to Them to develop innovative programs
• CMS is impressed with Savings and Quality• Other Entrepreneurs are coming with related
ideas and businesses• Dr. Gaziano recruits Dr. Carpentier to help to
foster RRM nationwide, possibly worldwide
Patrick Yeung, MD and other Centers of Surgical Excellence
• More Effective than Most Teaching Hospitals– Surgical Excellence– Attending to Outcomes Data– Near Contact Laparoscopy– National Reputation
• Championed and Trained by Dr. Hilgers• Another early leader was Dr. Redwine• Soon other centers will be trying to catch up

Challenges & Next Steps
Surgical TrainingEnough FCP’s
Insurance Support

Will we be able to meet the needs?If RRM is adopted, advocated
• CFCPs, CFCMCs/NPs• Especially NaProSurgeons• Can PPVI Institute Train More?
– Funding from insurers to do more per year– New training sites elsewhere
• Increased funding per surgery might help

Who will set the standards?
• Factors involved:– Price, price, price– Power
• Health Policy Commissions• Attorneys General
– Political agenda– Access– Professional Organizations
• Institute of Med, DPH, FDA

Barriers to Implementation
• Burdensome regulations• Corporate struggles• Lack of religious conscience protections• Public not educated on systems and costs• Lack of formation• Population control, feminist, gay rights lobbies• Medicaid covers abortion but not infertility
Potential Gains
• Compounding pharmacies – more business• Religious liberties – increased understanding• Reimbursements for FCPs – improved• Healthier women/families• Less:
• breast cancer• Prematurity and NICU stays• hysterectomies

Culture of Life GainsFrom Respect for Restorative Approach
• Authentic Feminism• Life is a Gift• Dignity of the Embryo
– Personhood at earliest stages– Increased respect– Less embryo selection
• Role of Husband/father appreciated again• Value of Marriage

Discussion
Insights to shareQuestions