respiratory system
TRANSCRIPT

Respiratory SystemDr. Deepak K Gupta
Syllabus1. Functional anatomy of respiratory passage & lungs.2. Physiology of Respiration: External & internal respiration3. Respiratory movements : Muscles of respiration, mechanism of inflation &
deflation of lungs4. Intra pleural & intra pulmonary pressures & their changes during the phases of
respiration.5. Mechanics of breathing - surfactant, compliance & work of breathing.6. Spirometry : Lung volumes & capacities definition, normal values, significance,
factors affecting vital capacity, variations in vital capacity, FEV & its variations.7. Pulmonary ventilation - alveolar ventilation & dead space – ventilation8. Composition of inspired air, alveolar air and expired air.9. Exchange of gases : Diffusing capacity, factors affecting it10. Transport of Oxygen & carbon dioxide in the blood11. Regulation of respiration - Neural & chemical12. Hypoxia, cyanosis, dyspnoea, periodic breathing13. Artificial respiration, pulmonary function tests
https://www.facebook.com/notesdental

Introduction
• The goals of respiration are to provide oxygen tothe tissues and to remove carbon dioxide.
• To achieve these goals, respiration can be divided intofour major functions1. Pulmonary ventilation : which means the inflow and
outflow of air between the atmosphere and the lung alveoli;
2. Diffusion of oxygen and carbon dioxide between the alveoli and the blood;
3. Transport of oxygen and carbon dioxide in the blood and body fluids to and from the body’s tissue cells;
4. Regulation of ventilation and other facets of respiration.
https://www.facebook.com/notesdental

Anatomy of the Lungs
• Gas-exchanging organ
• normal human breathes 12 to 15 times a minute
• 500 mL of air per breath
• 250 mL of O2 enters the body per minute and 200 mL of CO2 is excreted
• Traces of other gases
– Methane from the intestines
– Alcohol and acetone
– 250 different volatile substances
https://www.facebook.com/notesdental

Lungs
https://www.facebook.com/notesdental

Anatomy of the LungsNose/mouth: filtered, warmed, humidified Mucus traps bacteria & foreign debris
Cilia sweep mucus toward throat digested by stomach
Pharynx: throat (passage for food/air) Tonsils: clusters of lymphatic tissue
Larynx: contains vocal cords Epiglottis: covers larynx when liquids/food swallowed
Trachea: windpipe; lined with cartilage (C-shaped)
Bronchi: branches to lungs
Bronchioles: smaller branches
Lungs Alveoli: air sacs for gas exchange
https://www.facebook.com/notesdental

pharynx
https://www.facebook.com/notesdental

Air Passages• Trachea and the alveolar
sacs, the airways divide 23 times
• First 16 generations of passages form the conducting zone -bronchi, bronchioles, and terminal bronchioles
• Remaining 7 generations form the transitional and respiratory zones –respiratory bronchioles, alveolar ducts, and alveoli
https://www.facebook.com/notesdental
https://www.facebook.com/notesdental
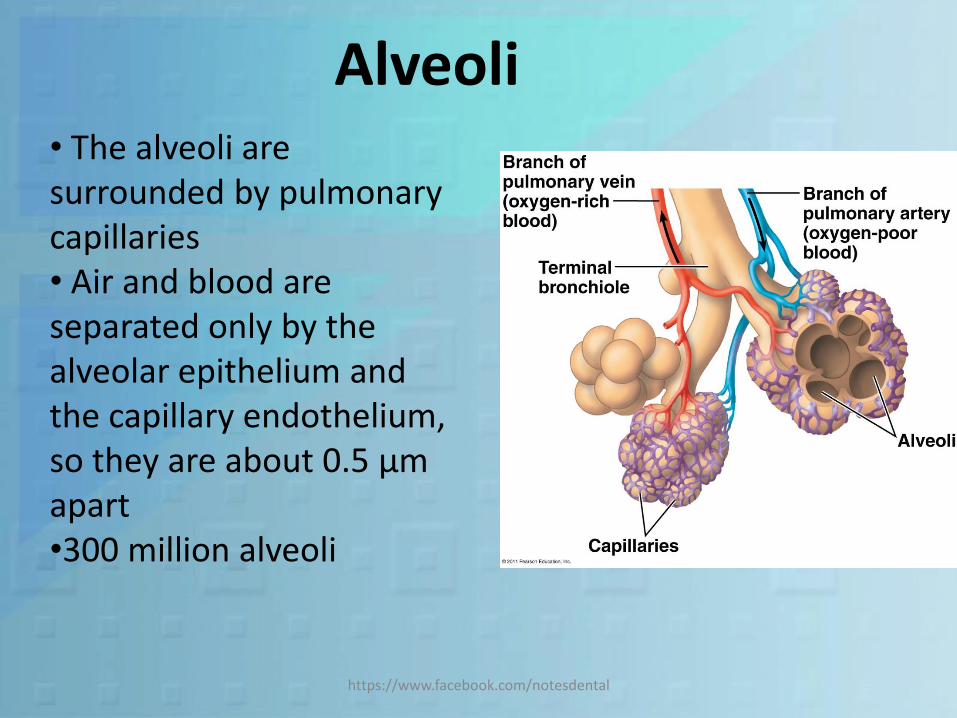
Alveoli• The alveoli are surrounded by pulmonary capillaries • Air and blood are separated only by the alveolar epithelium and the capillary endothelium, so they are about 0.5 μmapart •300 million alveoli
https://www.facebook.com/notesdental

Alveoli• lined by two types of epithelial cells
– Type I cells• flat cells with large cytoplasmic extensions • 95% of the alveolar epithelial surface area
– Type II cells • granular pneumocytes• thicker and contain numerous lamellar inclusion bodies• secrete surfactant• alveolar repair & other cellular physiology
• Specialized cells : pulmonary alveolar macrophages (PAMs, or AMs), lymphocytes, plasma cells, neuroendocrine cells, and mast cells– heparin, various lipids, histamine, and various proteases
that participate in allergic reactions
https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

The Bronchi• Trachea and bronchi –
cartilage in their walls but relatively little smooth muscle
• Ciliated epithelium that contains mucous and serous glands
• Cilia are present as far as the respiratory bronchioles
• But glands are absent from the epithelium of the bronchioles and terminal bronchioles
https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

Innervations• Innervated by the autonomic nervous system
(ANS)• Cholinergic discharge causes bronchoconstriction• Bronchial epithelium and smooth muscle contain ß2- adrenergic receptors– mediate bronchodilation & increase bronchial
secretion.
• α 1 adrenergic receptors inhibit secretion• Noncholinergic, nonadrenergic innervation of
the bronchioles that produces bronchodilation -Vasoactive intestinal polypeptide (VIP)
https://www.facebook.com/notesdental
Anatomy of Blood Flow in the Lung
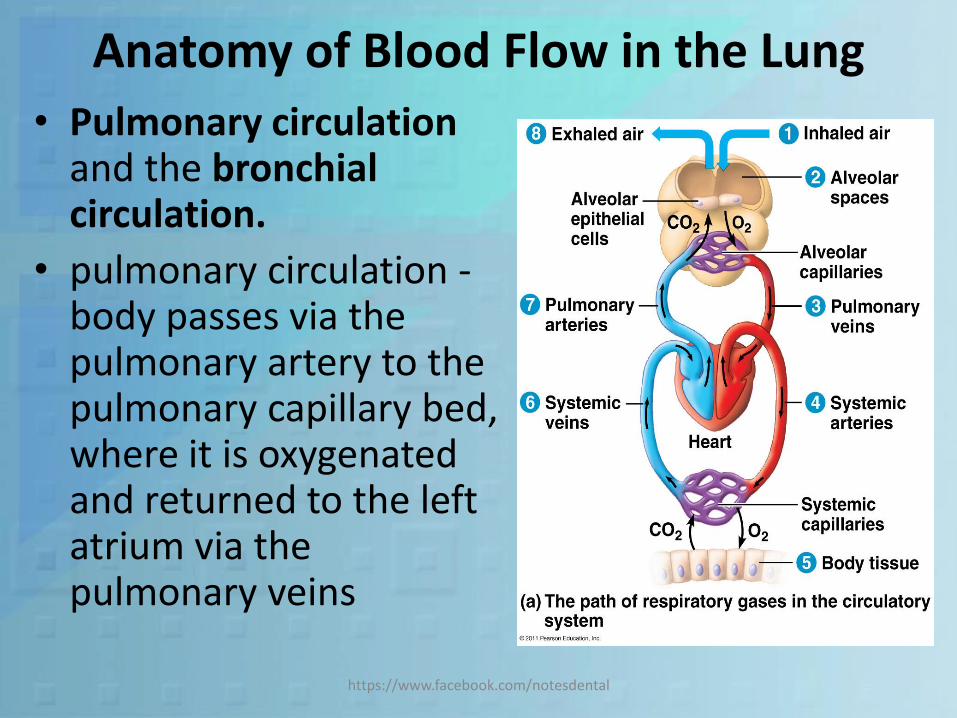
• Pulmonary circulationand the bronchial circulation.
• pulmonary circulation -body passes via the pulmonary artery to the pulmonary capillary bed, where it is oxygenated and returned to the left atrium via the pulmonary veins
https://www.facebook.com/notesdental
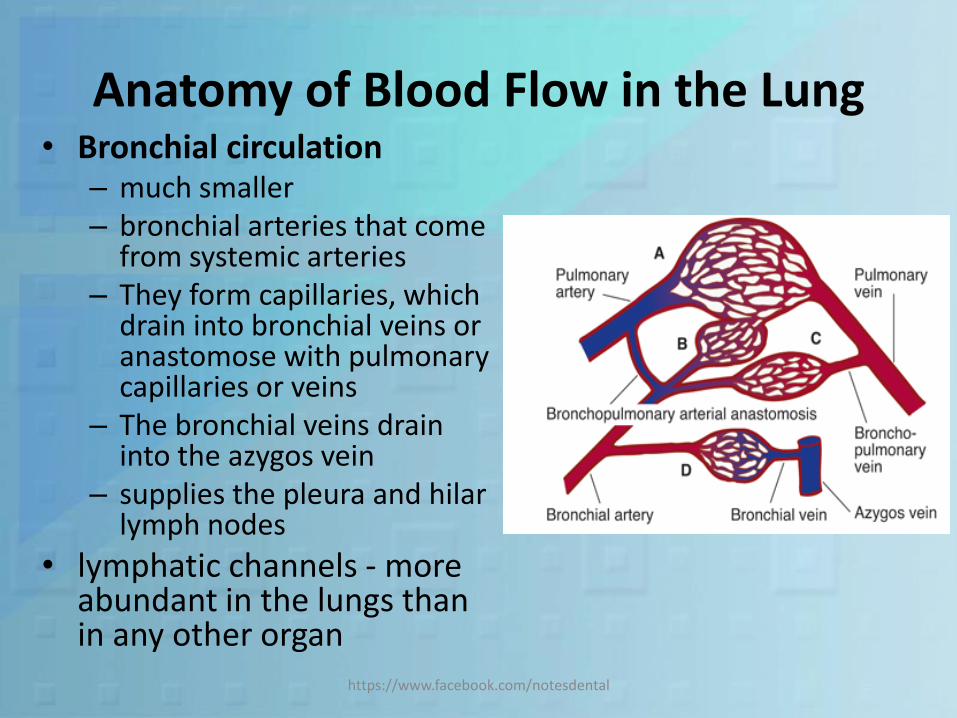
Anatomy of Blood Flow in the Lung• Bronchial circulation
– much smaller– bronchial arteries that come
from systemic arteries– They form capillaries, which
drain into bronchial veins or anastomose with pulmonary capillaries or veins
– The bronchial veins drain into the azygos vein
– supplies the pleura and hilarlymph nodes
• lymphatic channels - more abundant in the lungs than in any other organ
https://www.facebook.com/notesdental

Mechanics of Respiration• Lungs and the chest wall
are elastic structures
• A thin layer of fluid is present between the lungs and the chest wall (intrapleural space)
• Intrapleural pressure –subatmospheric.
• lungs slide easily on the chest wall, but resist being pulled away
https://www.facebook.com/notesdental

Inspiration
• Inspiration is an active process• Contraction of the inspiratory
muscles increases intrathoracicvolume
• At start - normally about –2.5 mm which decreases to about –6 mm of Hg at the end.
• Pulled into a more expanded position
• Air flows into the lungs• Strong inspiratory efforts reduce
intrapleural pressure to values as low as –30 mm Hg
https://www.facebook.com/notesdental

Expiration
• Expiration during quiet breathing is passive.
• No muscles contract.
• Some contraction of the inspiratory muscles occurs in the early part of expiration - exerts a braking action on the recoil forces and slows expiration
https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

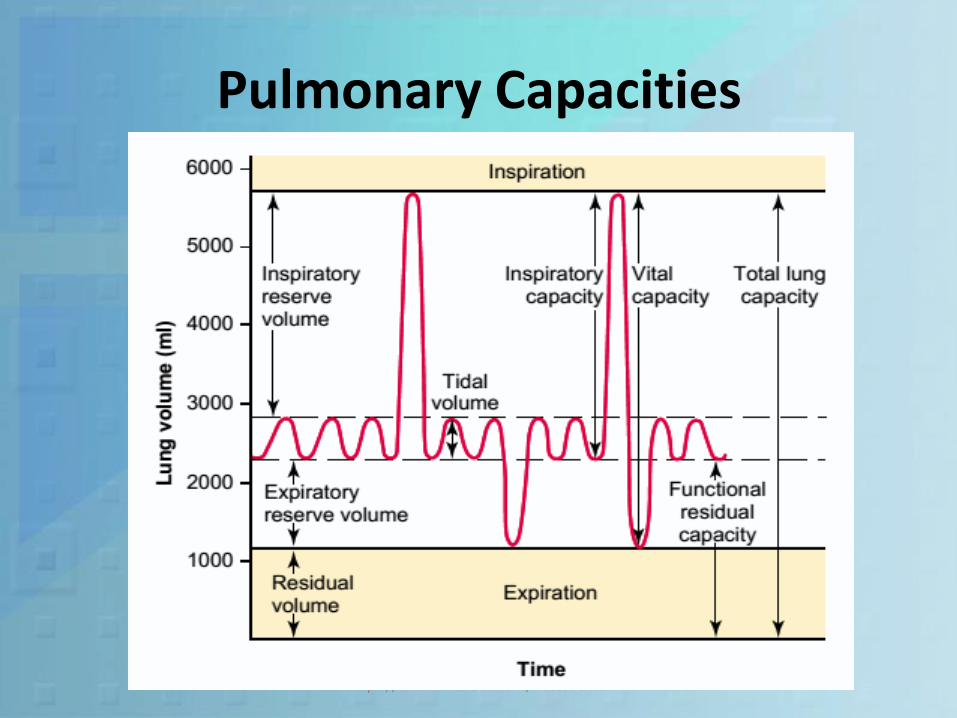
Lung Volume• Tidal volume (TV) : The amount
of air that moves into the lungs with each inspiration.
• Inspiratory Reserve Volume (IRV) : The air inspired with a maximal inspiratory effort in excess of the tidal volume.
• Expiratory Reserve Volume (ERV):The volume expelled by an active expiratory effort after passive expiration
• Residual Volume (RV): air left in the lungs after a maximal expiratory effort
https://www.facebook.com/notesdental
Lung Volume Amount (ml)
TV 500
IRV 3000
ERV 1100
RV 1200
Pulmonary Capacities
• Inspiratory capacity : the amount of air a person can breathe in, beginning at the normal expiratory level and distending the lungs to the maximum amount.
• Functional residual capacity : the amount of air that remains in the lungs at the end of normal expiration
• Vital Capacity: maximum amount of air a person can expel from the lungs after first filling the lungs to their maximum extent and then expiring to the maximum extent
• Total lung capacity: maximum volume to which the lungs can be expanded with the greatest possible effort
https://www.facebook.com/notesdental

Pulmonary Capacities
Pulmonary Capacities Volumes Capacity (ml)
IC TV+IRV 3500
FRC ERV + RV 2300
VC IRV + VT + ERVIC + ERV
4600
TLC IC + FRCVC + RV
5800
https://www.facebook.com/notesdental
• All pulmonary volumes and capacities are about 20 to 25 per cent less in women than in men• Greater in large and athletic people than in small and asthenic people
Spirometry• A simple method for studying pulmonary
ventilation is to record the volume movement of air into and out of the lungs
• It consists of a drum inverted over a chamber of water, with the drum counterbalanced by a weight.
• In the drum is a breathing gas, usually air or oxygen;
• A tube connects the mouth with the gas chamber.• When one breathes into and out of the chamber,
the drum rises and falls, • And an appropriate recording is made on a moving
sheet of paperhttps://www.facebook.com/notesdental

Spirometry
https://www.facebook.com/notesdental
Pulmonary Capacities
https://www.facebook.com/notesdental

Helium Dilution Method
• An indirect method to measure the residual volume –essential to know FRC which is important parameter for pulmonary disease
• Steps– A spirometer of known volume is filled with air mixed with
known helium concentration– Person expires normally– End of this expiration - the remaining volume in the lungs is
equal to the functional residual capacity– Now subject immediately begins to breathe from the
spirometer,– Gases of the spirometer mix with the gases of the lungs. – Helium becomes diluted by the functional residual capacity
gases
https://www.facebook.com/notesdental

Helium Dilution Method
• CiHe is initialconcentration of helium in the spirometer
• CfHe is final concentration of helium
• ViSpir - initial volume of the spirometer
RV = FRC – ERV
https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

Pulmonary Ventilationhttps://www.facebook.com/notesdental

Minute Respiratory Volume
• The total amount of new air moved into the respiratory passages each minute - 6 L/min on an average
MRV = TV X RR
• A person will die if minute respiratory volume falls as low as 1.5 L/min or RR falls below 2-4 breath/min
• Also known pulmonary ventillation
https://www.facebook.com/notesdental

Dead Space• The volume of gas that occupies the rest of the
respiratory system which is not available for gas exchange with pulmonary capillary blood.– Anatomic Dead Space– Total (physiologic) dead space
• Anatomic dead space is approximately equal to the body weight in pounds.
• For ex: a man weighing 150 lb, will have anatomic dead space of 150 ml.
• In diseased individual there is difference in this 2 values
• Its measured by single breath nitrogen wash out method
https://www.facebook.com/notesdental

Anatomical Dead space
• Extends from nose to terminal bronchioles –pharynx, trachea, bronchi and branches of bronchi up to terminal bronchioles
• Serves only as a passage for air movement
• Gas exchange doesn’t take place in these structures
https://www.facebook.com/notesdental

Physiological Dead Space
• Total volume which is not taking part in exchange of gases with pulmonary blood. It includes
– Volume of gases in non exchange passage
– Non-functional alveoli
– Non-perfusion alveoli
• It increased during respiratory disease, which affect the pulmonary blood flow
https://www.facebook.com/notesdental
Wasted Ventillation

Alveolar Ventilation
• Alveolar ventilation per minute is the total volume of new air entering the alveoli and adjacent gas exchange areas each minute
VA = RR X (TV-DV)
• Because of the dead space at the same respiratory minute volume – Rapid shallow breathing - less alveolar ventilation
– Slow deep breathing – greater alveolar ventillation
https://www.facebook.com/notesdental

Principles of Gas Exchange
https://www.facebook.com/notesdental

Introduction
• Oxygen is required for every cells to derive energy for its working and in return carbon dioxide is given out – cellular respiration
• So to carry out these, there is exchange of gases at
– Pulmonary exchange: O2 diffuses into blood and CO2 diffuses out of the blood
– Cellular Exchange: CO2 diffuses into the blood and O2 diffuses out to cell
https://www.facebook.com/notesdental

Physics involved in exchange
• Partial Pressure : the pressure exerted by individual gas. It depends totally on the % of its constituent. For example
– Atmospheric air exerts 760 mm of Hg
– Oxygen % = 21 % (approx)
– Partial pressure exerted PO2= 21% X 760 = 160 mm of Hg
• Diffusion : passage of gases/solute from higher pressure to low pressure
https://www.facebook.com/notesdental

Composition of Alveolar Air
• Don’t have same concentrations of gases as atmospheric air. Its mainly of 4 reasons
– alveolar air is only partially replaced by atmospheric air with each breath
– oxygen is constantly being absorbed into the pulmonary blood from the alveolar air
– carbon dioxide is constantly diffusing from the pulmonary blood into the alveoli
– atmospheric air that enters the respiratory passages ishumidified even before it reaches the alveoli
https://www.facebook.com/notesdental

https://www.facebook.com/notesdental

Oxygen Concentration and PartialPressure in the Alveoli
• Its controlled by
– the rate of absorption of oxygen into the blood and
– the rate of entry of new oxygen into the lungs by the ventilatory process.
https://www.facebook.com/notesdental

CO2 Concentration and PartialPressure in the Alveoli
• Its again dependent
– Alveolar PCO2 decreases in inverse proportion toalveolar ventilation
– Alveolar PCO2 increases directly in proportionto the rate of carbon dioxide excretion
https://www.facebook.com/notesdental

Respiratory Unit
• Composed of a respiratory bronchiole, alveolar ducts, atria, and alveoli.
• About 300 million alveoli in the two lungs, and each alveolus has an average diameter of about 0.2 mm.
https://www.facebook.com/notesdental

Respiratory Unit
• Extremely thin, and between the alveoli is an almost solid network of interconnecting capillaries
• “sheet” of flowing blood
https://www.facebook.com/notesdental

Pulmonary membrane• Gas exchange between
the alveolar air and the pulmonary blood occurs through the membranesof all the terminal portions of the lungs
• Collectively known as the respiratory membrane, also called the pulmonary membrane.
https://www.facebook.com/notesdental

Respiratory membrane
• It consists of following layers– A layer of fluid lining the alveolus and containing
surfactant that reduces the surface tension of the alveolar fluid
– alveolar epithelium composed of thin epithelial cells– epithelial basement membrane– thin interstitial space between the alveolar
epithelium and the capillary membrane– capillary basement membrane that in many places
fuses with the alveolar epithelial basement membrane
– capillary endothelial membrane
https://www.facebook.com/notesdental

Respiratory membrane
• Thinnest at 0.2 micrometer, and it averages about 0.6 micrometer
• Normal adult human male : Total surface area = 70 m2
• floor area of a 25–by-30–foot room
• Blood volume spread on this area - any given instant is 60 to 140 milliliters.
https://www.facebook.com/notesdental
Respiratory membrane
• Oxygen and carbon dioxide need not pass through significant amounts of plasma
– they diffuse between the alveolus and the red cell
– pulmonary capillaries diameter - 5 micrometers
• All this factors allows rapid diffusion of gases across the membrane
https://www.facebook.com/notesdental

Factors That Affect the Rate of Gas Diffusion
• factors that determine how rapidly a gas will pass through the membrane are
– thickness of the membrane. Ex : edema, fibrosis
– surface area of the membrane,
– diffusion coefficient of the gas in the substance of the membrane,
– the partial pressure difference of the gas between the two sides of the membrane
https://www.facebook.com/notesdental

Complete Picture of transport of Gases
• It involves following step1. Diffusion of O2 from the
Alveoli to the Pulmonary Capillary Blood
2. Transport of O2 in the Arterial Blood
3. Diffusion of O2 from the Peripheral Capillaries into the Tissue Fluid & Tissue Cells
4. Diffusion of CO2 from the Peripheral Tissue Cells into the peripheral Capillaries
5. Transport of CO2 in venous blood
6. Diffusion of CO2 from the Pulmonary Capillaries into the Alveoli
https://www.facebook.com/notesdental

Diffusion of Oxygen from the Alveoli to the Pulmonary Capillary Blood
• Po2 of alveolus averages = 104 mm Hg
• Po2 of blood entering pulmonary capillary = 40 mm Hg
• This pressure difference cause exchange of O2
https://www.facebook.com/notesdental
Transport of Oxygen in theArterial Blood
• 98 % of blood that enters left atrium comes from after pulmonary ventilation = Po2 (104 mm of Hg)
• 2 % as shunted blood that supplies deep structures of lungs which remains deoxygenated = Po2 (40 mm of Hg)
• The combination of this produces effective Po2
= 95 mm of Hg that reaches systemic circulation - venous admixture of blood
https://www.facebook.com/notesdental

Changes in Po2
https://www.facebook.com/notesdental

Transport of Oxygen
• 97 % – chemical combination with hemoglobin in the red blood cells
• 3 per cent - transported in the dissolved state in the water of the plasma and blood cells
• It combines loosely and reversibly with the hemeportion of hemoglobin
https://www.facebook.com/notesdental

Transport of Oxygen
https://www.facebook.com/notesdental

Oxygen-Hemoglobin Dissociation Curve
• Progressive increase in the % of hemoglobin bound with O2 as blood Po2 increases
• Also known as per cent saturation of hemoglobin• Usual oxygen saturation of systemic arterial blood
averages 97 per cent - Po2 of about 95 mm Hg
https://www.facebook.com/notesdental

Oxygen-Hemoglobin Dissociation Curve
• blood of a normal person contains about
• 15 g of hemoglobin in each 100 ml of blood
1 g of HG = 1.34 ml of O2 (1.39 ml in pure HG)
• Total amount of O2 in 100 ml of blood = 15 X 1.34 = 20.1 ml of O2
• Also known as volume percent
• So at 97 % (95 of Hg) amount of O2 is 19.4 ml and 75 % (40 mm of Hg) it falls to 14.4 ml
https://www.facebook.com/notesdental

Diffusion of Oxygen from the Peripheral Capillaries into the Tissue
Fluid• Po2 in the interstitial fluid that surrounds the
tissue cells averages only 40 mm Hg• This cause rapid diffusion of O2 from the capillary• pH - Increase in CO2 in the blood causes O2 to
be displaced from the hemoglobin - Bohr effect
https://www.facebook.com/notesdental

Diffusion of Oxygen from the Peripheral Capillaries to the
Tissue Cells• Po2 intracellular - 5 mm Hg to as high as 40
mm Hg (averaging 23 mm Hg)
• Normal Po2 required for full support of the chemical processes that use oxygen in the cell : 1 to 3 mm Hg
• Adequate and provides a large safety factor
https://www.facebook.com/notesdental

Diffusion of Carbon Dioxide fromthe Peripheral Tissue Cells into the
Capillaries• Oxygen is used by the cells - virtually all of it
becomes carbon dioxide - increases the intracellular Pco2
• Carbon dioxide diffuses from the cells into the tissue capillaries
• Carbon dioxide can diffuse about 20 times as rapidly as oxygen – so requires less pressure difference comparably
https://www.facebook.com/notesdental

Transport of CO2 in venous blood
• CO2 is transported mainly 3 forms i.e
– Dissolved state in plasma – 7%
– Bicarbonate ion – 70 %
– Haemoglobulin – 23 %
https://www.facebook.com/notesdental

Transport of CO2 in venous blood
https://www.facebook.com/notesdental

Transport of Carbon Dioxide in the Form of Bicarbonate Ion
• Dissolved CO2 reacts with water in RBC to form carbonic acid
• In the presence of enzyme carbonic anhydrases
– Increases the reaction rate about 5000-fold
– small fraction of a second
• In another fraction - carbonic acid dissociates into H+ and HCO3– ion
• H+ reacts with hemoglobin – HG protein powefulacid-base buffer
https://www.facebook.com/notesdental

Chloride Shift
• Bicarbonate ions diffuse from the RBC into the plasma and chloride ions diffuse into the RBC.
• This occurs through - special bicarbonate-chloride carrier protein channel in RBC membrane
• chloride content of venous RBC is greater than that of arterial RBC
• This phenomenon is called the chloride shift
https://www.facebook.com/notesdental

Chloride Shift
https://www.facebook.com/notesdental

Transport of Carbon Dioxide in Combination with Hemoglobin and
Plasma Proteins —carbaminohemoglobin
• CO2 reacts directly with amine radicals of the hemoglobin molecule - carbaminohemoglobin(CO2Hgb)
• Reversible reaction that occurs with a loose bond -easily released into the alveoli,
• Small amount of carbon dioxide – reacts same way with the plasma proteins - much less significant
• Much slower than the reaction than that of water
https://www.facebook.com/notesdental

Diffusion of CO2 from the Pulmonary
Capillaries into the Alveoli
• Pco2 of the blood entering the pulmonarycapillaries at the arterial end, 45 mm Hg
• Pco2 of the alveolar air, 40 mm Hg
• 5 mm Hg pressure difference causes all the required carbon dioxide diffusion
https://www.facebook.com/notesdental
Haldane Effect
• Binding of oxygen with hemoglobin tends to displace carbon dioxide from the blood.
• Oxyhemoglobin – stronger acid
• This causes– Decrease of tendency Hemoglobin to combine with
carbon dioxide to form carbaminohemoglobin
– release an excess of hydrogen ions, and these bind with bicarbonate ions to form carbonic acid -dissociates into water and carbon dioxide
https://www.facebook.com/notesdental

Regulations of Respiratory System
https://www.facebook.com/notesdental

Introduction
• Nervous system normally adjusts the rate ofalveolar ventilation almost exactly to the demands of the body
• Partial pressures of respiratory gases almost remains same even during heavy exercise and most other types of respiratory stress.
• Two separate neural mechanisms regulate respiration– Voluntary control: cerebral cortex and sends impulses
to the respiratory motor neurons via the corticospinaltracts
– Automatic control : regulated by Respiratory Center located in medulla oblongata
https://www.facebook.com/notesdental
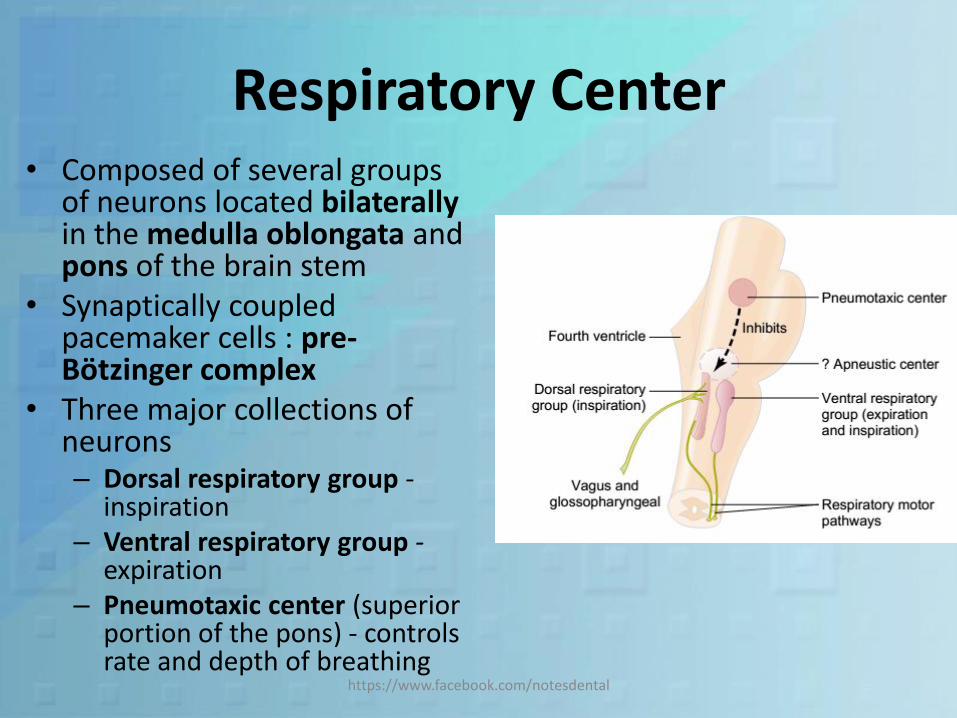
Respiratory Center• Composed of several groups
of neurons located bilaterallyin the medulla oblongata and pons of the brain stem
• Synaptically coupled pacemaker cells : pre-Bötzinger complex
• Three major collections of neurons– Dorsal respiratory group -
inspiration– Ventral respiratory group -
expiration– Pneumotaxic center (superior
portion of the pons) - controls rate and depth of breathing
https://www.facebook.com/notesdental

Dorsal Respiratory Group• Located dorsally and extending to entire length of
the medulla
• Neurons are located within the nucleus of the tractus solitarius
• The nucleus consists of sensory termination of both the vagal and the glossopharyngeal nerves– peripheral chemoreceptors,
– Baroreceptors
– Several types of receptors in the lungs
• DRG acts by Rhythmical Inspiratory Discharges or inspiratory “Ramp” Signal
https://www.facebook.com/notesdental

Inspiratory “Ramp” Signal
• Nervous signal that is transmitted to the inspiratory muscles, mainly the diaphragm, is not an instantaneous
• Begins weakly and increases steadily in a ramp manner for about 2 seconds
• Stops abruptly for approximately the next 3 seconds -turns off the excitation of the diaphragm and allows elastic recoil of the lungs and the chest wall to cause expiration
• And again the new cycle begins
https://www.facebook.com/notesdental
2 Secs 3 Secs 2 Secs

Pneumotaxic Center
• Limits the duration of inspiration and increases the respiratory rate.
• Located in nucleus parabrachialis - upper pons• It transmits inhibitory signal to inspiratory area -
“switch-off” point of the inspiratoryramp
• The signal may extend the inspiration from 0.5 sec to 5 sec
• The inspiratory rate solely decides the expiratory rate, so overall respiratory rate is controlled by Pneumotaxic Center
https://www.facebook.com/notesdental

Ventral Respiratory Group
• It controls both Inspiration and Expiration.• On each side of the medulla - 5 mm anterior and lateral to
the DRG• It consists of nucleus ambiguus and the nucleus
retroambiguus.• Remain almost totally inactive during normal quiet
respiration.• When there is increased respiratory drive, the inspiratory
signal spills from DRG which in turn activates VRG• It prolongs inspiration and in turn powerful expiratory
signals to the abdominal muscles.• Its mostly active in Heavy excercise
https://www.facebook.com/notesdental
Hering-Breuer Inflation Reflex
• Sensory nerve signals from the lung due to its expansion - control respiration.
• Stretch receptors : transmit signals through the vagus to DRG.
• This again creates a “switches off” –inspiratory ramp
• Its not activated in humans till the T.V. reaches 3 times the normal value
https://www.facebook.com/notesdental
Overall Control of RespiratoryCenter Activity
• All this control mechanism works under the demand of pulmonary ventilation
• It increase 20 times during heavy exercise of work.
• So to meet this requirement, lungs should work in a very controlled manner.
https://www.facebook.com/notesdental

Chemical Control of Respiration• Excess CO2 or H2 ions in the
blood mainly act directly on the respiratory center.– increased strength of both the
inspiratory and the expiratory motor signals
• Oxygen - does not have a significant direct effect on the respiratory center
• Acts almost entirely on peripheral chemoreceptorslocated in the carotid and aortic bodies
https://www.facebook.com/notesdental
Carbon Dioxide and Hydrogen Ions
• Chemosensitive Area of the Respiratory Center
– an additional neuronal area, located bilaterally beneath the ventral surface of medulla
– sensitive to changes in either blood Pco2 orhydrogen ion concentration
– in turn excites the other portions of the respiratory center
https://www.facebook.com/notesdental

Carbon Dioxide and Hydrogen Ions
• H2 Ions is likely to be the primary stimulus – as the chemosensitive area is more sensitive to it.
• But it doesn’t crosses Blood Brain Barrier (BBB) -so can’t act directly.
• CO2 easily crosses BBB, which reacts with water present in medulla and forms carbonic acid which later dissociates to H+ ions.
https://www.facebook.com/notesdental

Carbon Dioxide and Hydrogen Ions
• Excitation of the RC by CO2 is great the first few hours
• Then it gradually declines over the next 1 to 2 days -one fifth the initial effect
• This is mainly due to increased – renal filtration of H+ ions out of the blood
– Intake of bicarbonate ion which in turn neutralizes H+ ions
• Finally almost a normal H+ ions is achieved –desensitizing RC
• Potent acute effect on controlling respiratory drive but only a weak chronic effect
https://www.facebook.com/notesdental

Carbon Dioxide and Hydrogen Ions
• Marked increase in ventilation caused by anincrease in Pco2 in the normal range between 35 and 75 mm Hg
• Tremendous effect that CO2changes have in controlling respiration
• Normal amounts of oxygen to the tissues even when the pulmonary Po2 changes from 60 mm Hg to 1000 mm Hg
https://www.facebook.com/notesdental

Role of Oxygen in Respiratory Control
• Important for detecting changes in oxygenin the blood, lesser extent to CO2 and H+ ion concentrations
• It does so mainly by 2 bodies– Carotid bodies
• located bilaterally in the bifurcations of the common carotid arteries.
• afferent nerve fibers pass through Hering’s nerves tothe glossopharyngeal nerves and then to the DRG
– Aortic bodies• along the arch of the aorta• Afferent nerve fibers pass through the vagi then to the DRG
• Beside this two, a very few are located elsewhere in association with other arteries of the thoracic and abdominal regions
https://www.facebook.com/notesdental

Structure of Peripheral Chemoreceptor
• Receives its own special blood supply through a minute artery directly from the adjacent arterial trunk
• Blood flow through these bodies is extreme, 20 times the weight of the bodies themselves each minute
• % of oxygen removed from the flowing blood is virtually zero.
• So this bodies are exposed at all times to arterial blood, not venous blood
• highly characteristic glandular-like cells, called glomus cells, that synapse directly or indirectly with the nerve endings
https://www.facebook.com/notesdental

Stimulation of the Peripheral Chemoreceptors
• Decrease Arterial Oxygen
– particularly sensitive to changes in arterial Po2 in the range down to 60
• Carbon Dioxide and Hydrogen Ion Concentration
– The stimulation by the central chemoreceptorsoccurs as much as five times as rapidly as peripheral stimulation
https://www.facebook.com/notesdental

Other Factors That Affect Respiration
• Voluntary Control of Respiration : respiration can be controlled voluntarily
• Effect of Irritant Receptors in the Airways : trachea, bronchi, and bronchioles is supplied withsensory nerve endings called pulmonary irritant receptors– stimulated by many incidents
– coughing and sneezing
– cause bronchial constriction in such diseases as asthma and emphysema.
https://www.facebook.com/notesdental

Other Factors That Affect Respiration
• Function of Lung “J Receptors”– sensory nerve endings in the alveolar walls in
juxtaposition to the pulmonary capillaries– pulmonary capillaries become engorged with blood or when
pulmonary edema
• Effect of Brain Edema– depressed or even inactivated by acute brain edema resulting
from brain concussion– relieved temporarily by intravenous injection of hypertonic
solutions such as highly concentrated mannitol solution
• Anesthesia– prevalent cause of respiratory depression and respiratory arrest
is overdosage with anesthetics or narcotics
https://www.facebook.com/notesdental

Periodic Breathing
• An abnormality of respiration
• Occurs in a number of disease conditions.
• Person breathes deeply for a short interval and then breathes slightly or not at all for an additional interval
• This cycle repeating itself over and over
• Cheyne-Stokes breathing is a type of periodic breathing
https://www.facebook.com/notesdental

Hypoxia
• Decrease supply of oxygen to cells
• It may be either due to
– Inadequate oxygenation of the blood in the lungs because of extrinsic reasons
– Pulmonary disease
– inadequate oxygen transport to the tissues by the blood
– Inadequate tissue capability of using oxygen
https://www.facebook.com/notesdental

Effects of Hypoxia on the Body
• If severe enough, can cause death of cells throughout the body
• But in less severe degrees it causes principally
– Depressed mental activity, sometimes culminating in coma
– Reduced work capacity of the muscles.
https://www.facebook.com/notesdental

Cyanosis• blueness of the skin• Its cause is excessive amounts of deoxygenated
hemoglobin in the skin blood vessels - especially in the capillaries
• Whenever the arterial blood contains more than 5 g of deoxygenated hemoglobin in each 100 ml of blood
• A person with anemia almost never becomes cyanotic because there is not enough hemoglobin
• A person with excess red blood cells, as occurs in polycythemia vera - great excess of available hemoglobin that can become deoxygenated leads frequently to cyanosis even under normal conditions
https://www.facebook.com/notesdental

Dyspnea• Air hunger
• Mental anguish associated with inability to ventilate enough to satisfy the demand for air
• This may occur due to– abnormality of respiratory gases in the body fluids,
especially hypercapnia and, to a much less extent, hypoxia
– the amount of work that must be performed by the respiratory muscles to provide adequate ventilation
– state of mind.
• Neurogenic dyspnea or emotional dyspnea: person’s respiratory functions may be normal and still dyspneamay be experienced because of an abnormal state of mind
https://www.facebook.com/notesdental

Artificial Respiration• There are various devices available for artificial
respiration.• Its mainly of 2 types• Resuscitator
– a tank supply of oxygen or air– mechanism for applying intermittent positive pressure– a mask that fits over the face of the patient or– or a connector for joining the equipment to an
endotracheal tube
• Earlier resuscitators often caused damage to the lungs because of excessive positive pressure
https://www.facebook.com/notesdental

Resuscitator
https://www.facebook.com/notesdental

Tank Respirator• “Iron-Lung”• Patient’s body inside the
tank• Head protruding through
a flexible but airtight collar.
• a motor-driven leather diaphragm moves backand forth with sufficient excursion to raise and lower the pressure inside the tank
https://www.facebook.com/notesdental

Effect of Artificial Respiration
• Pressure inside the lungs becomes greater than pressure everywhere else in the body during artificial respiration
• Flow of blood into the chest and heart from the peripheral veins becomes impeded
• Reduces the cardiac output—sometimes to lethal levels
• Continuous exposure for more than a few minutes to greater than 30 mm Hg positive pressure in the lungs can cause death
• Inadequate venous return to the heart
https://www.facebook.com/notesdental

Refrences
• Guyton_human physiology_11th edition
• Ganong’s Review of Medical Physiology - 23rd Ed
• human_physiology__the_basis_of_medicine__3rd edition
• Netter atlas of physiology
https://www.facebook.com/notesdental