respiratory paediatrics dr pamela lewis. 6yr male emergency department sudden onset wheeze and dib...
TRANSCRIPT

RESPIRATORY RESPIRATORY PAEDIATRICSPAEDIATRICS
Dr Pamela LewisDr Pamela Lewis
6yr Male Emergency 6yr Male Emergency DepartmentDepartment
• Sudden onset wheeze and DIB• Preceding URTI• Atopic• Interval symptoms
Acute AsthmaAcute AsthmaAssessment of severityAssessment of severity
• Talking• Respiratory rate• Accessory muscle use• Heart rate• Oxygen saturations• Peak Flow

Acute Asthma ManagementAcute Asthma Management• ABC and Oxygen• B2 Agonist (LVS or Neb)• Steroids (oral prednisolone/iv
hydrocortisone)• Ipratropium bromide neb• Aminphyline/iv salbutamol• Magnesium sulphate• www.brit-thoracic.org.uk
Asthma- Chronic Asthma- Chronic ManagementManagement
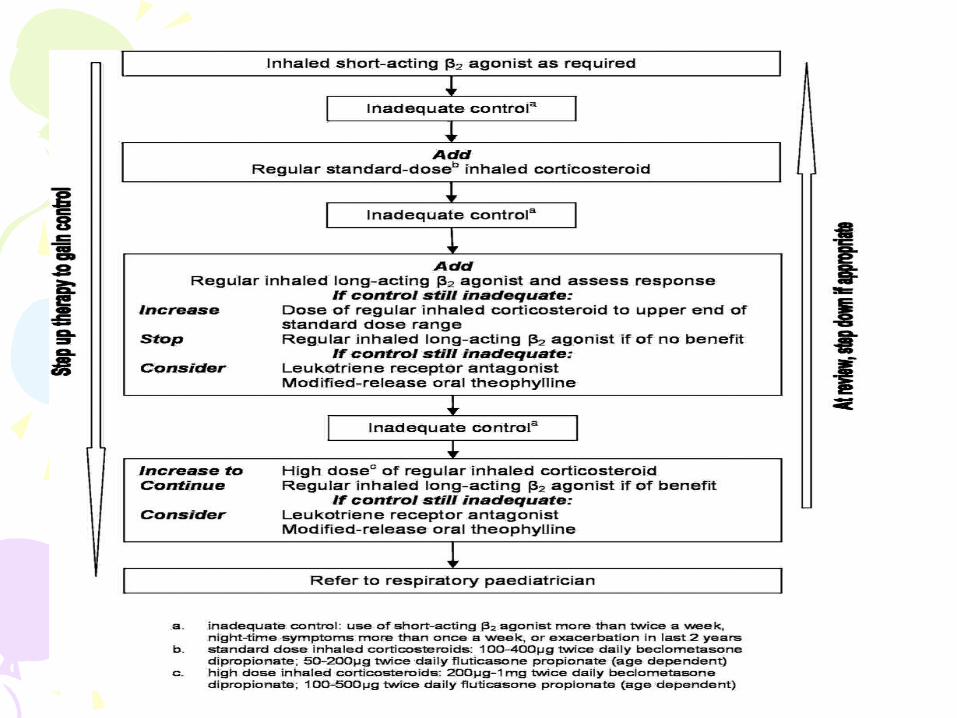
• Interval symptoms and exacerbations• Adherence• Inhaler and spacer technique• Growth• Examination • PF FEV1/FVC• Medication BTS stepwise approach• www.brit-thoracic.org.uk

3 month Female Emergency 3 month Female Emergency DepartmentDepartment
• Cough, coryza, fever and poor feeding
• Preterm 25/40, oxygen until 6 wks of age
• Parental smoking• Respiratory distress with bilateral
crackles and wheeze

Bronchiolitis assessmentBronchiolitis assessment• Feeding (<50%)• RR (>70)• Nasal flare, grunting,recession• Oxygen sats <92%• History of apnoeas
Bronchiolitis ManagementBronchiolitis Management• Oxygen• Fluids• Consider blood investigations if diagnosis
in doubt or severe• CXR not routine• In deterioration CPAP/IPPV• Palivixumab prophylaxis for risk groups• www.sign.ac.uk
10 Yr Male Emergency 10 Yr Male Emergency DepartmentDepartment
• 2 days cough, fever> 39, abdominal pain and rigors
• No prior respiratory history• HR 130 Refill 3 seconds BP 100/60
RR 36 dull to PN right base with crackles


Pneumonia ManagementPneumonia Management• ABC and Oxygen• Fluids • Antibiotics• CXR BC FBC Electrolytes• Sputum culture• Complications Empyema, SIADH• www.brit-thoracic.org.uk

4 yr Female Emergency 4 yr Female Emergency DepartmentDepartment
• Temperature 40, marked respiratory distress, soft stridor, drooling
• Unvaccinated

EpiglotitisEpiglotitis• SHOUT FOR HELP• Senior anaesthetist, paediatrician,
ENT• Rapid sequence induction of
anaesthesia• Antibiotics ceftriaxone (Hib)

Childrens OutpatientsChildrens Outpatients6 month Male6 month Male
• Recent arrival in UK ( Europe)• FTT • Recent right upper lobe pneumonia• Loose stools, good appetite• Examination, weight < 0.4th (BW 50th)
cough and mild i.c recession

Cystic FibrosisCystic Fibrosis• AR chromosome 7, CFTR
defect ,DF508• UK 1:2500, gene carrier 1:25• Multi organ involvement• Respiratory: decreased mucocilliary
clearance, diminished local defences and increased bacterial adherence, progressive loss of respiratory function

CF DiagnosisCF Diagnosis• UK screening programme• Heel Test at 6 days IRT • Genetic testing CF mutations• Sweat test Chloride > 60 (sodium <
Chloride)

CF ManagementCF Management• Multi disciplinary• Infections prophylactic and treatment• Nutrition• Physiotherapy• Psychology• Screening for complications: liver,
diabetes
Childrens Outpatients 3yr Childrens Outpatients 3yr FemaleFemale
• Refugee from Somalia• Protracted cough, fevers, FTT• Limited Family history no vaccination
history• CXR hilar lymphadenopathy and RUL
collapse


TB Diagnosis TB Diagnosis • Latent v Active TB• Mantoux < 6mm negative, >6mm
positive in those without prior BCG, >15mm positive in those with BCG
• Consider Gamma Interferon testing• Sputum• DON’T FORGET HIV

Treatment TBTreatment TB• 6 month regime• 2 months Rifampicin, isoniazid,
pyrayinamide and ethambutol then• 4 months rifampicin and isoniazid• DOTS• Public health and contact tracing