resistant pneumococcal infections - world health organization
TRANSCRIPT

WHO/CDS/CSR/DRS/2001.6ORIGINAL: ENGLISHDISTRIBUTION: GENERAL
World Health Organization
ResistantpneumococcalinfectionsStephanie J. Schrag,Bernard Beall andScott Dowell
Copies can be obtained from the CDS Information Resource CentreWorld Health Organization, 1211 Geneva 27, Switzerland
fax: +41 22 791 42 85 • email: [email protected]

WHO/CDS/CSR/DRS/2001.6ORIGINAL: ENGLISHDISTRIBUTION: GENERAL
Resistant pneumococcalinfections: the burden ofdisease and challenges inmonitoring and controllingantimicrobial resistanceStephanie J. Schrag, Bernard Beall and Scott DowellRespiratory Diseases BranchCenters for Disease Control and PreventionAtlanta, GA, United States of America
World Health Organization
A BACKGROUND DOCUMENT FOR
THE WHO GLOBAL STRATEGY
FOR CONTAINMENT OF
ANTIMICROBIAL
RESISTANCE

Acknowledgement
The World Health Organization wishes to acknowledge the support of the United States Agency for Inter-national Development (USAID) in the production of this document.
© World Health Organization 2001
This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organiza-tion. The document may, however, be freely reviewed, abstracted, reproduced and translated, in part or in whole, but not for sale orfor use in conjunction with commercial purposes.
The views expressed in documents by named authors are solely the responsibility of those authors.
The designations employed and the presentation of the material in this document, including tables and maps, do not imply theexpression of any opinion whatsoever on the part of the secretariat of the World Health Organization concerning the legal status ofany country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines onmaps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended byWHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietaryproducts are distinguished by initial capital letters.
Designed by minimum graphicsPrinted in Switzerland

Contents
iii
WHO/CDS/CSR/DRS/2001.4 DRUG RESISTANC IN MALARIA
Executive Summary 1
Top 5 research recommendations 2
A. Disease incidence and trends 3
1. Populations at risk 32. Geographical distribution 33. Adequacy and quality of data documenting disease 44. Diagnosis: methods, feasibility, accuracy, overlapping clinical syndromes 55. Organisms causing the disease 66. Ecological niche of the organisms 67. Data on current drug-resistance trends and problems 78. Summary: Disease incidence and trends 89. Research needs: Disease incidence and trends 9
B. Causes of resistance 101. Mechanisms of resistance 102. Factors contributing to the spread of resistance 113. Summary: Causes of resistance 134. Research needs: Causes of resistance 13
C. Detection of resistance 151. Laboratory-based methods 152. Clinic-based methods 163. Summary: Detection of resistance 164. Research needs: Detection of resistance 16
D. Treatment 171. Standard treatment guidelines for disease management 172. Definition of cure: no pathogens or no symptoms? 173. Data to support the efficacy of treatment guidelines to cure and the impact
of treatment guidelines on resistance at the individual and population level 174. Data showing relationship between emergence of resistance and drug quality,
misdiagnosis, use of a related drug for another disease, suboptimal regimens,use of drugs in humans and animals 19
5. Strategies for improving treatment and evidence that these will contain spread 206. Ethical issues: benefits to individual vs. benefits to community 207. Drug policy strategies and the data on which they are based: switch, rotation,
reservation, combination of drugs 208. Summary: Treatment 209. Research needs: Treatment 22
E. Prevention of pneumococcal disease 231. Known interventions 232. Interventions currently undergoing testing 233. Summary: Prevention of pneumococcal disease 254. Research needs: Prevention of pneumococcal disease 25

F. Bibliography 26
Appendix 30
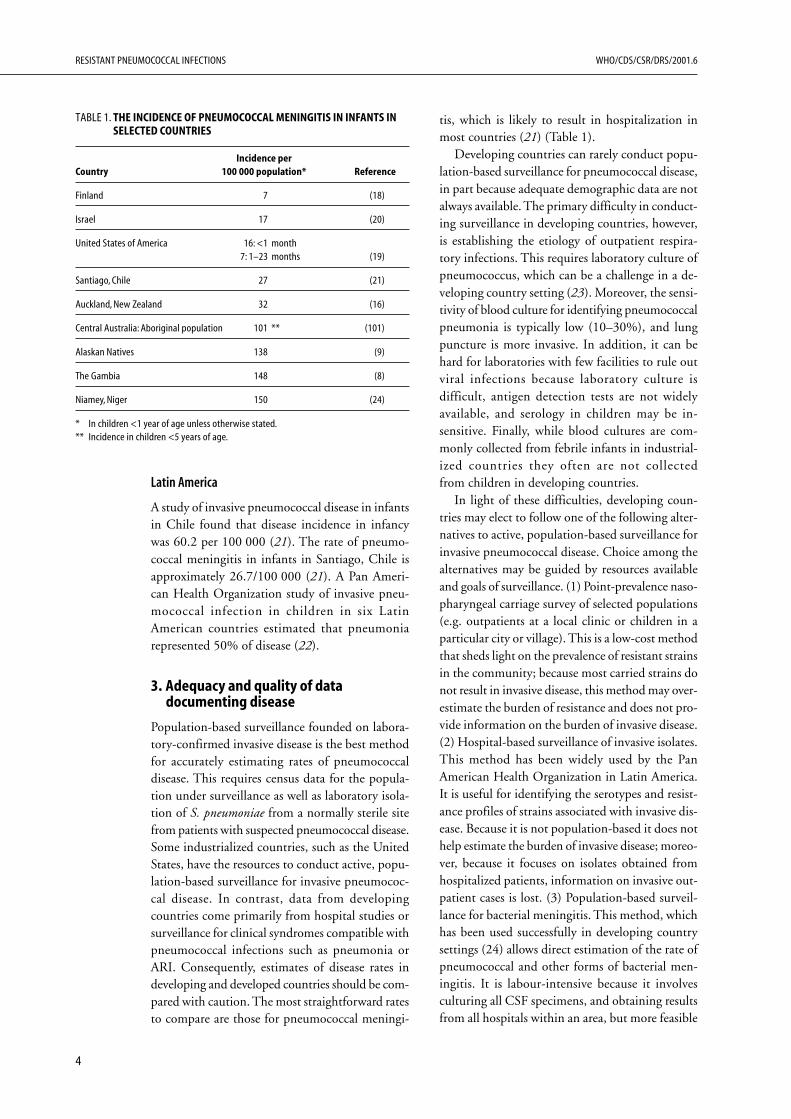
TablesTable 1. The incidence of pneumococcal meningitis in infants in selected countries 4
Table 2. Age-specific prevalence of pneumococcal carriage in different geographical regions 5
Table 3. Genetic mechanisms of pneumococcal antibiotic resistance 11
Table 4. Hypotheses for the mechanisms generating the association between recentantimicrobial therapy and nasopharyngeal (NP) carriage of resistant pneumococci,and distinguishing predictions of each hypothesis 14
Table 5. Advantages and disadvantages of different laboratory methods of pneumococcalsusceptibility testing 15
Table 6. Principles of preventing the development and transmission of resistance due toantimicrobial therapy 21
RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
iv

1
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
Executive Summary
antibiotic use and carriage of resistant strains are notcompletely understood and require further research.
A key factor influencing the emergence andspread of resistant pneumococci is unnecessaryantibiotic use for viral respiratory illnesses in hu-mans. This is due to misdiagnosis of conditionsbecause both viral and bacterial agents can causesymptoms of ARI, as well as physician and patientpressures to prescribe antibiotics. However, whileantibiotic overuse is a problem in some developingsettings, in others, poor access to adequate healthcare is still a primary problem and children requir-ing antibiotic therapy do not receive it.
Pneumococcal resistance can also be inadvert-ently driven by the use of drugs for unrelated con-ditions. This may pose a particularly seriousproblem as mass antibiotic prophylaxis campaignsto eliminate trachoma are introduced in a numberof African countries.
To date, the pneumococcal polysaccharide vac-cine is the principal established intervention toprotect against pneumococcal disease. Because thisvaccine only protects against bacteraemic pneumo-coccal pneumonia, is not indicated for childrenunder 2 years of age, and has no impact on pneu-mococcal carriage, it is not an effective interven-tion against ARI or the spread of drug resistance inmost developing countries.
A pneumococcal conjugate vaccine has now beenapproved for routine infant use in the United States.This vaccine has been shown to be highly effectiveat preventing pneumococcal pneumonia and men-ingitis in young children and infants. Moreover,the vaccine has some efficacy at protecting againstotitis media, and also protects against carriage ofvaccine-included pneumococcal serotypes. Becauseof its unique features, this vaccine holds greatpotential as an “anti-resistance vaccine” whichsimultaneously reduces the burden of invasivedisease and the prevalence of resistant strains. Pro-phylactic use of xylitol, a sugar which inhibits pneu-mococcal growth, may also represent a feasibleintervention against non-invasive disease andresistance in developing countries.
Acute respiratory infections (ARI) are a leadingcause of childhood mortality, causing 25–33% ofall deaths in children in developing countries. Bac-terial ARI are associated with higher case-fatalityratios than infections caused by viruses. Streptococ-cus pneumoniae is the most common cause of bac-terial ARI, and pneumococcal resistance is theprincipal cause for concern regarding treatmentfailures for ARI and meningitis. Therefore, thisreview focuses on pneumococcal resistance.
ARI are often treated empirically with antibiot-ics. Drug-resistance trends are not well documentedin most developing countries due to limitedlaboratory capacity. It is clear, however, that theprevalence of strains resistant to penicillin-relatedcompounds and to co-trimoxazole is increasing.The clinical impact of pneumococcal resistancevaries with the site of infection and is better docu-mented for meningitis and otitis media than forpneumonia.
The ecological niche of S. pneumoniae is thehuman nasopharynx, where it can be carriedasymptomatically and transmitted from person toperson. Children carry S. pneumoniae more com-monly than adults. In contrast to a majority of otherpathogens where drug resistance is a problem, theevolution of drug resistance within a patient dur-ing the course of antibiotic therapy is not commonin S. pneumoniae. This is because resistance con-ferred by single-point mutations alone is rare inpneumococcal clinical isolates. Transformation (theuptake of free DNA from the environment) andconjugative transposons (the transfer of segmentsof genomic DNA during bacterial fusion) are thetwo primary genetic mechanisms conferring pneu-mococcal resistance.
Epidemiological studies have demonstrated thatrecent antibiotic use is strongly associated withcarriage of resistant pneumococci both at the com-munity and individual levels. Among individualswho develop invasive pneumococcal disease, recentantibiotic use is also associated with an increasedrisk of infection with a resistant strain. The biologicalmechanisms behind the association between recent

7
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
7. Data on current drug-resistancetrends and problems
Drug-resistance trends
Because methods of conducting surveillance forpneumococcal resistance have not been standard-ized, comparisons using studies from differentcountries are difficult. In particular, surveillancedata typically are based on sterile site isolates fromhospitalized individuals or non-sterile site isolatesfrom randomly selected children and adults in thecommunity. Although sterile site isolates shed lighton the strains directly associated with invasive dis-ease, culture methods are more complicated andtypically result in a lower yield, particularly indeveloping countries. Moreover, screening based onsterile-site isolates is biased towards individualsattending tertiary care facilities. For example, thepercentage of penicillin-resistant invasive isolatesfrom single hospitals within a state in the UnitedStates did not reflect the mean prevalence of peni-cillin resistance for the state as a whole, as estimatedby population-based surveillance (34).
In contrast, nasopharyngeal isolates have a higheryield and are collected directly from the site associ-ated with person-to-person transmission. However,not all pneumococcal strains isolated from thenasopharynx are associated with invasive disease.A number of studies in developing countries com-paring pneumococcal resistance in isolates obtainedfrom blood and from nasopharyngeal swabs havefound that nasopharyngeal carriage isolates approxi-mate the antibiotic-resistance rates found ininvasive isolates (35, 36, 37, 38). Oropharyngealcultures, however, have a much lower yield thannasopharyngeal isolates and should not be used.
Despite limitations in the available surveillancedata, some robust trends are evident. One of themost striking is geographical variation in the preva-lence of antimicrobial-resistant pneumococci. In the1970s penicillin-resistant pneumococci were mostcommon in Israel, Papua New Guinea, Poland,South Africa and Spain as well as some states in theUnited States (39). Now resistant pneumococcihave a worldwide distribution, although only lim-ited surveillance data from a majority of African,Asian and South American countries are available.A recent survey of clinical specimens from 11 Asiancountries from 1996 to 1997 found that penicillinnon-susceptibility ranged from 80% of isolates inthe Republic of Korea to 4% of isolates in India(40). A detailed study of invasive isolates from sixhospitals in India found penicillin non-suscepti-
bility in 1.3% of isolates; resistance to trimetho-prim/sulfamethoxazole was present in 56% ofisolates, and to chloramphenicol in 17% of isolates(41). In Europe, Spain is a focus of penicillin-non-susceptible pneumococcal strains, with a prevalenceof non-susceptibility of over 45% of pneumococ-cal isolates (39). A high incidence of resistance hassimilarly been reported for Eastern European coun-tries.
A smaller but growing number of isolates arealso resistant to multiple antibiotics and some aresusceptible only to parenteral agents (17), posing athreat to the effective treatment of pneumococcaldisease.
Clinical impact of resistance
It is difficult to measure the impact of infectionwith a resistant strain on increased morbidity andmortality for a number of reasons. First, it is oftennot possible to control for risk factors such as un-derlying disease that confound the association withmortality. Second, resistant pneumococci can varygreatly in their degree of resistance to a particulardrug. Resistance is typically measured as MIC, theminimal concentration of antibiotic required toinhibit bacterial growth. The clinical impact ofstrains with an intermediate MIC may be muchless than that of a highly-resistant strain. Third, theclinical impact of antibiotic resistance varies withthe site of infection, the ability of antibiotics topenetrate to that site, and the ability of the im-mune response to clear the infection. Consequently,we consider the major clinical syndromes causedby S. pneumoniae individually.
Meningitis. Antibiotic resistance poses a particu-lar problem for the case of meningitis because mostantibiotics do not penetrate effectively into the cer-ebrospinal fluid (CSF). Because penicillin-resistantpneumococcal meningitis has become common(32), the extended-spectrum cephalosporins arewidely used for treatment of meningitis. Treatmentfailures due to infection with cephalosporin-resist-ant pneumococcus, however, have now been re-ported in both children (42, 43) and adults (44,45). In a rabbit meningitis model, penicillin-resist-ant pneumococci were eradicated from the site ofinfection only if the antibiotic concentration in CSFexceeded the lowest concentration of drug requiredto kill pneumococci by 8- to 10-fold (46). Suchlevels are difficult to achieve, particularly as MICsincrease. Similarly, an in vitro study (47) of theefficacy of high-dose cefotaxime against interme-
RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
8
diate and high-level cephalosporin-resistant pneu-mococci found that only 44% (8/18) of CSF sam-ples obtained from meningitis patients exposed toa high dose of cefotaxime achieved 99.9% killingof pneumococci with high-level resistance. Thisstudy demonstrated wide variation among patientsin antibiotic pharmacokinetics in the CSF. In re-sponse to growing numbers of treatment failures,the American Academy of Pediatrics recommendsthat children with possible pneumococcal menin-gitis be treated with a combination of vancomycinplus cefotaxime or ceftriaxone (48). Animal mod-els have shown that this combination therapyproduces a synergistic effect (49).
Otitis media. There is now clear evidence thatacute otitis media treatment failures have been di-rectly attributable to resistant pneumococci. Forexample, in a study of 78 children under 3 years ofage with acute otitis media caused by S. pneumoniae,only 6% of children infected with a cephalosporin-susceptible strain had bacteriological treatmentfailures following cephalosporin treatment while35% infected with a strain of intermediate resist-ance had bacteriological failures (50). Drugs witha lower activity against pneumococci, such ascefaclor and cefixime, are affected more by increas-ing MICs than drugs such as amoxicillin (50).In response to the rapid dissemination of drug-resistant S. pneumoniae, the Drug Resistant S.pneumoniae Therapeutic Working Group (Appen-dix) recently recommended that amoxicillin remainthe first-line antibiotic for acute otitis media, butthat the dosage should be routinely doubled, andthat clinical failures after 3 days of therapy requirean alternative agent effective against resistantS. pneumoniae and β-lactamase producing patho-gens (51). Antibiotic therapy is recommended foracute otitis media primarily to protect against rarebut severe sequelae of such infections. Up to 80%of cases of otitis media from all causes resolve with-out treatment (52).
Pneumonia. Evidence for treatment failures dueto antibiotic-resistant pneumococcal pneumoniahas been more difficult to document. A number ofstudies in adults and in children have found thatpneumococcal resistance did not influence the out-come of pneumonia treatment (45). These studies,however, included patients with low levels ofβ-lactam resistance (MIC <1µg/ml). Standard treat-ment for pneumococcal pneumonia has been shownto be effective against both susceptible strains andstrains of intermediate resistance. For strains withhigh-level resistance to penicillin (MICs >4µg/ml)
clinical and pharmacodynamic data suggest thatincreased mortality or complications are likely. Ananalysis of population-based active surveillance forpneumococcal pneumonia from nine areas in NorthAmerica found that mortality was associated withpenicillin MICs >=4 and cefotaxime MICs >=2,only after the first four days of hospitalization wereexcluded (53). Mortality in the first four days ofillness, which occurred for almost half of pneumo-coccal pneumonia-associated deaths, is influencedby the severity of presenting illness rather than anyparticular therapeutic intervention. Because resist-ant strains do not typically alter illness presenta-tion (52) increasing levels of resistance may notaffect mortality rates in the early stages of illness.Phamacokinetic/pharmacodynamic evidence sug-gests that β-lactams might not be effective at treat-ing pneumococcal strains with penicillin MICs>8and cefuroxime MICs>4.
8. Summary: Disease incidence and trends
● There is a need for better data on the globalburden of pneumococcal disease. Such informa-tion can be obtained by surveillance for nasopha-ryngeal carriage in children, or by focusing onclinical isolates. These data are difficult to ob-tain for a number of reasons: surveillance sys-tems for invasive disease are not in place in manydeveloping countries; the etiological agents caus-ing pneumonia, meningitis and otitis media arerarely identified; the clinical syndromes associ-ated with pneumococcal disease overlap withthose caused by a wide range of other patho-gens. Moreover, comparisons across countries aredifficult because the threshold for seeking healthcare and for performing diagnostic proceduresvaries greatly.
● Efforts to assess the pneumococcal disease bur-den are also important to help evaluate effectivebut costly interventions such as conjugatevaccines, antibiotic use control programmes, andothers (discussed in section E). Because antimi-crobial resistance concerns overlap with inter-vention concerns, efforts to characterize diseaseburden should be coordinated.
● There is a need for better data on drug resist-ance in developing countries. Surveillance fordrug resistance not only better characterizes themagnitude of the problem but often also leadsto increased awareness of the issue and developsimportant local laboratory capacity. Surveillance

9
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
9. Research needs: Disease incidenceand trends
1. Develop generic protocols for assessing theburden of pneumococcal disease in developingcountries.
2. Assess the disease burden due to pneumococcalresistance to prioritize possibly expensive buteffective interventions such as conjugatevaccines, antibiotic use control programmes andothers (discussed in section E).
3. Compare surveillance for resistant nasopharyn-geal carriage to surveillance for resistant clinicalisolates. Studies should focus on identifying con-ditions when population-based surveillance isrequired, and when point-prevalence clinic-based surveys will suffice.
4. Monitor trends in resistance to new or impor-tant antibiotic agents besides penicillin. Theseinclude: macrolides, co-trimoxazole andquinolones.
for nasopharyngeal carriage rather than focus-ing strictly on clinical isolates has been recom-mended recently by WHO. However, thesemethods have still not been field-tested, andwhether population-based surveillance is worththe added expense depends on the burden ofresistant disease and impact relative to other pri-orities.
● Treatment failures due to pneumococcal resist-ance have been documented for meningitis andotitis media. The clinical impact of resistance inthe treatment of pneumonia has been more dif-ficult to establish. Because pneumonia causes amuch more significant burden of disease thanotitis media in many developing countries, un-derstanding how antibiotic resistance affectspneumococcal pneumonia management shouldremain a priority.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
10
B. Causes of resistance
The genetic mechanisms associated with differ-ent clinically-relevant antibiotic resistance pheno-types are summarized in Table 3.
Association between resistance and serotype
Currently, the vast majority of clinical isolates fromthe United States with high-level resistance toβ-lactam antibiotics belong to serogroups 6, 9, 14,19, and 23. These same serogroups are also oftenassociated with β-lactam resistance in other coun-tries. While the genetic diversity within each ofthese serotypes is striking, resistant isolates withineach serotype typically belong to prevalent, well-documented clonal groups. A majority of theseclonal groups have also acquired numerous otherdrug resistances, including resistance to erythromy-cin, chloramphenicol, trimethoprim/sulfametho-xazole, and tetracycline.
It is not yet clear why these particular serogroupshave a higher probability of containing resistancegenes. It is possible that transformation barriers playa role in preventing some serotypes from acquiringβ-lactam resistance and other horizontally-spreadresistance determinants. The proportion of clini-cal isolates that are transformable in the laboratoryhas not been determined. Optimal competenceconditions differ between strains, and the capsuleitself reduces or totally inhibits transformation. Cellwall barriers imposed by different capsular types,incompatible competence factors between donorand recipient strains, and host endonuclease restric-tion of incoming DNA might all limit the spreadof resistance via transformation among specificserotypes.
Despite evidence of a strong association betweenresistance patterns and serotype, the gene-encod-ing capsular serotype can also be exchanged betweenstrains by transformation (54). Thus, it is possiblethat highly resistant clones may become membersof highly invasive serotypes that are currently notassociated with multidrug resistance.
1. Mechanisms of resistance
The genetic basis of resistance plays a key role indetermining how resistance develops and spreadswithin communities. A number of biologicalfeatures distinguish pneumococci from other patho-gens with acquired drug resistance, such as Myco-bacteria, and Escherichia coli. First, resistance inclinical pneumococcal isolates is rarely due tosingle-point mutations alone or to plasmid carriage.Second, transformation (the uptake and chromo-somal exchange of free DNA from closely relatedstrains or species), and conjugative transposons(transfer and genetic incorporation of smallsegments of DNA during bacterial fusion events)are the most common mode for pneumococci toacquire resistance genes. Third, pneumococci arecommonly carried asymptomatically in thenasopharynx, which is also the source of person-to-person transmission. Fourth, resistant strains candiffer in their degree of resistance to a particulardrug, measured as the MIC (minimum inhibitoryconcentration of a particular antibiotic).
These biological characteristics directly influencethe population dynamics of pneumococcal resist-ance. Because resistance seldom results fromsingle-point mutations alone (single DNA basechanges that occur due to errors during bacterialreplication), evolution of resistant pneumococciwithin a patient during the course of antibiotictreatment rarely occurs. Instead, resistant pneumo-coccal infections result primarily from the acquisi-tion of resistant strains from the community.Moreover, because the preconditions for acquiringresistance by transformation and conjugativetransposons are more stringent than those for pointmutation, resistant pneumococci spread primarilyby clonal amplification rather than repeated de novogeneration. Finally, both infected individuals andasymptomatic carriers can transmit pneumococci.Thus, reducing the number of infected individualsin a population does not necessarily reduce thepotential for transmission of resistant strains withinthe community.

11
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
2. Factors contributing to the spread ofresistance
Biological
The genetic basis of resistance in S. pneumoniaestrongly influences the population dynamics ofdrug-resistant strains. In contrast to a majority ofbacterial species, antimicrobial resistance in pneu-mococci has not been associated with plasmidcarriage. Moreover, resistance due to single-pointmutations alone is extremely rare in pneumococcalclinical isolates. Transformation is the most com-mon mode of acquisition of resistance genes, and
resistance determinants spread on conjugativetransposons are also common (Table 3). Both ofthese mechanisms depend on the presence of re-sistance genes in closely related species, and thepresence of free DNA in the environment in thecase of transformation, or the opportunity fordonor/recipient cellular contact between a donorwith a conjugative transposon conferring resistanceand a susceptible S. pneumoniae recipient for thecase of conjugative transposons. Transformation re-quires homologous recombination following theuptake of resistance determinants, whereas resist-ance determinants on conjugative transposons can
TABLE 3. GENETIC MECHANISMS OF PNEUMOCOCCAL ANTIBIOTIC RESISTANCE*
Genetic basis Frequency among isolatesPhenotype of resistance Origin resistant to that drug class References
Intermediate Penicillin-binding protein Transformation with PBP genes from All known penicillin-resistant (103, 104)ß- lactam resistance (PBP) gene alterations resistant, closely related species. clinical isolates
High-level penicillin PBP gene alterations Sequential transformation events, All known clinical isolates have mosaic (103, 104)resistance which can also be followed by structures for these 3 genes. Note that
spontaneous mutation events an altered pbp2b gene is required forconferring incremental resistance. high-level penicillin resistance.
High-level resistance to PBP gene mosaics Transformation which can happen All known clinical isolates have mosaic (105)extended spectrum involving pbp1a and pbp2 by a single transformation event. forms of pbp1a and pbp2x. PBP2B is notcephalosporins a target for extended-spectrum(e.g. cefotaxime) cephalosporins.
Intermediate and high- Dihydrofolate reductase Transformation or spontaneous Both mechanisms appear common. (106, 107, 108)level trimethoprim/sulfa- (dhf) gene mosaics and/or mutation. dhf mosaics are possibly moremethoxazole resistance point mutant alleles frequently observed than simple point
mutations involving 3 or fewer bases.
Intermediate erythromycin mefE, efflux mechanism Unknown, probably originated Common (109)resistance through transformation or conjugative
transfer from another species, sincemefE is not found in sensitive strains.
High-level erythromycin ermAM gene Conjugative transfer of transposons, Common (110)resistance including Tn1545 and Tn1545 deletion
derivatives, and Tn3872.
High-level tetracycline –tetM Conjugative transfer of Tn1545 Majority of tetR isolates (111)resistance and its derivatives and Tn5253
–tetO Unknown, probably transformation Less common (112)or transposition
High-level chloramphenicol cat gene Conjugative transfer of Tn5253, Common (111)resistance common
Low-level fluoroquinolone parC mutations Transformation, point mutations Up to 3% resistance of 1997 (108, 113)resistance systemic isolates
High-level fluoroquinolone parC and gyrA Transformation, point mutations Up to 1% of 1997 systemic isolates (108)resistance double mutants
Vancomycin tolerance vncS Newly-recognized, details not Identified only in some serotype (114)currently known 9V isolates
* Reproduced with permission, Schrag et al. Clinical Microbiology Reviews 2000;13:588–601.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
12
be inserted into the chromosome in the absence ofDNA homology.
Because of these requirements, the rate ofacquisition of resistance via these mechanisms maybe lower than that associated with resistance dueto point mutations. In an environment whereneighbouring bacterial strains are not alreadyresistant, there is no potential for sensitive pneu-mococcal strains to acquire resistance by transfor-mation. Consequently, resistant pneumococcalinfections result primarily from the acquisition ofresistant pneumococci from the community ratherthan from the development of resistance during thecourse of an infection. Moreover, the spread of re-sistant pneumococcal strains is primarily by clonalamplification rather than repeated independent denovo origin.
Additionally, in contrast to pathogens that areassociated uniquely with acute infections,S. pneumoniae is commonly carried asympto-matically in the nasopharynx. Thus, resistantbacteria have a reservoir in healthy people in thecommunity.
Finally, the association between resistance andserotype may play a role in the spread of resistanceto the extent that some serotypes may have a higherrate of transmission in the population and a higherprobability of causing invasive disease. In addition,the impact of conjugate vaccines on resistance maybe modified if non-vaccine serotypes acquire resist-ance or if resistant vaccine serotypes undergocapsular switching (Section E).
Therapeutic
A large number of studies, both at the communityand individual levels, have demonstrated an asso-ciation between recent therapy with antibiotics andthe spread of resistant pneumococci.
Studies at the community level. There is evidencefrom several countries that increased consumptionof some antibiotics, such as β-lactams, correlateswith a rise in the prevalence of resistant pneumo-coccal strains (55, 56, 57). For example, a cross-sectional study of antimicrobial consumption andthe carriage rate of penicillin-resistant pneumococciin children in five different communities in Ice-land found that children in communities withhigher levels of antimicrobial consumption were athigher risk for nasopharyngeal carriage of resistantpneumococci (56). Similarly, a longitudinal analy-sis of sentinel surveillance for invasive S. pneumoniaein the United States found that increases in the
prevalence of penicillin-resistant pneumococci inthe early 1990s correlated with increased prescrip-tion rates for certain β-lactam agents, while a fairlyconstant prevalence of tetracycline-resistant pneu-mococci was associated with slight decreases in theprescription rate for tetracycline (58). Additionally,some studies have shown that declines in antibi-otic use at the community level correlate withdeclines in the prevalence of resistant streptococci.The prevalence of penicillin-resistant pneumococciin Hungary (59) and in Iceland (60) declined fol-lowing reduced antimicrobial use. Few studies,however, have collected longitudinal data on boththe prevalence of resistant strains and the volumeof drug use in order to establish a direct link be-tween declines in drug consumption and the preva-lence of resistance.
However, the prevalence of resistance need notalways be proportional to the rate of antibiotic us-age. For example, if resistant strains do not have afitness disadvantage over sensitive strains in theabsence of antibiotics they can be expected to per-sist even if antibiotic usage is reduced or eliminated(61, 62). Since penicillin-binding proteins (PBPs)are essential cell wall synthesis enzymes, it seemslogical that alterations in these enzymes associatedwith a β-lactam-resistant phenotype might resultin growth deficiencies. In fact, resistant clinical iso-lates with PBP alterations also often have dramati-cally altered peptidoglycan structure. These mutantsare not only β-lactam-resistant, but unaffected ingeneral physiology as well, and thus able to persistin the absence of direct antibiotic selection.
Studies at the individual level. A number ofcross-sectional studies have identified recent anti-microbial use by individuals as a risk factor forcarriage of resistant pneumococci by those same in-dividuals. This association has been observed inpopulations with high (15, 63) and more moder-ate prevalences of pneumococcal nasopharyngealcarriage (64). For example, in the Iceland study byArason et al., children with recent antimicrobialuse (within the last 7 weeks) were at higher risk forcarriage of penicillin-resistant pneumococci (57);similarly in a day-care centre in Israel where theprevalence of carriage in children was greater than60%, and resistance to at least one drug was greaterthan 50%, exposure to antimicrobial therapy in theprevious month was significantly associated withthe likelihood of carrying resistant pneumococciin a multivariate analysis (65). In contrast, antibi-otic use in the more distant past (3 months ago orlonger) typically has not been associated with a

13
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
plays only a small role, in contrast to other patho-gens such as HIV and mycobacteria, where re-sistance also poses problem.
● Therapeutic factors play a key role in the spreadof resistance. Increased use of antimicrobials isassociated with an increase in the prevalence ofpneumococcal resistance at the community level.At the individual level, recent antibiotic use isassociated with an increased risk of carrying re-sistant pneumococci, and of acquiring invasivedisease caused by resistant pneumococci.
4. Research needs: Causes of resistance
a. Further investigation of the mechanismsresulting in the association between recent an-tibiotic use and carriage of resistantS. pneumoniae. The biological mechanisms re-sulting in the association between recentantibiotic use and carriage of resistant S.pneumoniae have not been well studied. Possi-ble mechanisms fall into three broad categories:the unmasking of a resistant pneumococcal clonethat was present at a low density in the nasophar-ynx prior to antimicrobial therapy; replacementof sensitive pneumococci with resistant pneu-mococci acquired from the community duringor after antimicrobial therapy; and within-hostevolution of a resistant pneumococcal popula-tion in response to the selective pressure of anti-microbial therapy. Distinguishing features ofthese alternative mechanisms are discussed inmore detail in Table 4.
A better understanding of which of these mecha-nisms generate the observed association wouldprovide an important framework for develop-ing interventions to prevent the spread ofresistance. For example, if replacement ofsensitive strains with resistant strains from thecommunity is the primary mechanism, thenantibiotics which clear the nasopharynx may in-crease the risk of resistant carriage more thanantibiotics which do not. In contrast, if unmask-ing is the primary mechanism then antibioticswhich clear the nasopharynx of both sensitiveand resistant strains may be the most effectivetreatment. Optimal treatment is likely to varywith the prevalence of resistant strains in thecommunity, which influences both the risk ofmultiple carriage and of acquiring resistantstrains during and after treatment. Longitudi-nal studies of nasopharyngeal carriage before and
greater risk of resistant nasopharyngeal carriage(66). Additional factors that cross-sectional stud-ies have often identified as risk factors for resistantpneumococcal carriage include young age (withhighest carriage often in individuals <1 year old)and attendance at day-care centres.
Studies have also shown correlations betweenrecent antibiotic use and the incidence of invasivedisease caused by non-susceptible pneumococci(64). This suggests that recent antimicrobial usenot only increases the risk that an individual willcarry, and therefore potentially transmit resistantpneumococci, but that it also increases the risk thatthe individual will develop invasive pneumococcalillness caused by resistant pneumococci.
Studies investigating the effect of antibiotic useon the nasopharyngeal flora within individuals areless common although they contribute importantlyto understanding how antibiotic use leads to in-creased resistance. Longitudinal studies of individu-als have shown an increase in the relative proportionof resistant pneumococci among carriers followingboth prophylactic antimicrobial treatment (67, 68)and treatment of acute pneumococcal infections(69). This results primarily from a decrease in thecarriage of susceptible pneumococci, and thus isnot necessarily associated with an overall increasein the prevalence of resistance in the study popula-tion.
Non-human use
While antimicrobial use in agriculture and farm-ing poses a concern for a number of enteric patho-gens, non-human use of antibiotics is not of directconcern for the case of pneumococci because it isstrictly a human pathogen and plasmid-borneresistance does not play a key role.
Commercial/economic factors
In developing countries, commercial and economicfactors determine which antibiotics are available.Typically amoxicillin and co-trimoxazole are amongthe most affordable, and thus the most commonlyused antibiotics for respiratory infections.
3. Summary: Causes of resistance
● Transformation, the uptake of free DNA fromclosely related bacterial strains or species, andconjugative transposons carrying resistancegenes, are the key genetic mechanisms confer-ring pneumococcal resistance. Point mutation

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
14
after the initiation of antibiotic treatment pro-vide data that can distinguish among alterna-tive mechanisms for the increased risk of carryingresistant pneumococci following antimicrobialtreatment (Table 4).
b. Further investigation of the association be-tween resistance and serotype. Why someserotypes are not associated with resistancebecomes a question of particular importance asthe pneumococcal conjugate vaccine is intro-duced.
c. How frequent and important is capsularswitching? This genetic event has only beendocumented recently, and it is still unclear how
commonly it occurs. Because both resistance andtransmissibility have an association with pneu-mococcal serotype, frequent capsular switchingcould have an impact on the spread of resist-ance within communities. Moreover, becauseinterventions such as the pneumococcal polysac-charide and conjugate vaccine (discussed insection E) are both designed to confer protec-tion against the most common pneumococcalserotypes, capsular switching could decrease theefficacy of these interventions. In particular,because the conjugate vaccine appears to pro-tect against pneumococci of vaccine-associatedserotypes, mass vaccination may result in strongselection for capsular switching.
TABLE 4. HYPOTHESES FOR THE MECHANISMS GENERATING THE ASSOCIATION BETWEEN RECENT ANTIMICROBIAL THERAPY ANDNASOPHARYNGEAL (NP) CARRIAGE OF RESISTANT PNEUMOCOCCI, AND DISTINGUISHING PREDICTIONS OF EACH HYPOTHESIS*
Hypothesis Predictions
Pre-treatment During treatment Post-treatment
Unmasking: Antibiotic therapy The NP flora consists of a majority The minority population The majority population is geneticallyleads to the amplification of sensitive population and a increases and the majority identical to the pre-treatment minorityminority resistant clones that minority population resistant to population decreases populationcolonized the NP prior to the prescribed antibiotictreatment
Replacement during therapy: The NP flora is sensitive to the The sensitive population declines; The newly-acquired resistant strainColonization by a resistant strain prescribed antibiotic; a minority a genetically-distinct strain dominates; pre-treatment strains are infrom the community occurs resistant population may or may appears; this strain is resistant to the minority, or not detectableduring antibiotic therapy not be present the prescribed antibiotic
Replacement after therapy: The NP flora is sensitive to the The majority population declines NP flora returns to high levels; theAntibiotic therapy reduces the prescribed antibiotic; a minority until carriage reaches low levels majority strain may be sensitive,NP flora sufficiently to increase resistant population may or may or is eradicated resistant to the antibiotic used forthe likelihood of recolonization not be present therapy, or resistant to otherpost-antibiotic therapy antimicrobials, depending on the
prevalence of resistant strains in thecommunity
Within-host evolution of The NP flora is sensitive to the The sensitive population declines; A resistant strain dominates; this strainresistance: Antibiotic-mediated prescribed antibiotic; a minority a resistant population appears is genetically identical to the dominantselection results in amplification resistant clone is not detectable and increases; the resistant pre-treatment strain, except at the lociof a resistant mutant arising population is of the same associated with resistanceeither by point mutation or serotype as the sensitivetransformation before or during populationtreatment
* Reproduced with permission, Schrag et al. Clinical Microbiology Reviews 2000;13:588–601.

15
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
C. Detection of resistance
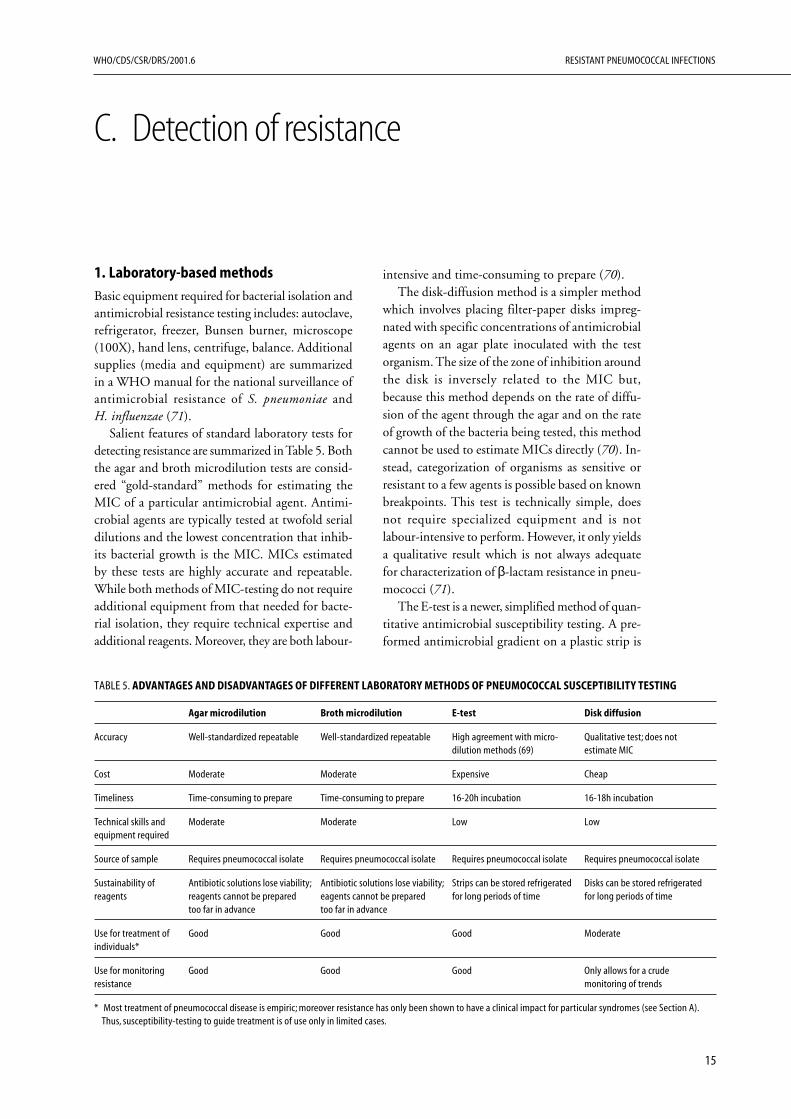
intensive and time-consuming to prepare (70).The disk-diffusion method is a simpler method
which involves placing filter-paper disks impreg-nated with specific concentrations of antimicrobialagents on an agar plate inoculated with the testorganism. The size of the zone of inhibition aroundthe disk is inversely related to the MIC but,because this method depends on the rate of diffu-sion of the agent through the agar and on the rateof growth of the bacteria being tested, this methodcannot be used to estimate MICs directly (70). In-stead, categorization of organisms as sensitive orresistant to a few agents is possible based on knownbreakpoints. This test is technically simple, doesnot require specialized equipment and is notlabour-intensive to perform. However, it only yieldsa qualitative result which is not always adequatefor characterization of β-lactam resistance in pneu-mococci (71).
The E-test is a newer, simplified method of quan-titative antimicrobial susceptibility testing. A pre-formed antimicrobial gradient on a plastic strip is
1. Laboratory-based methods
Basic equipment required for bacterial isolation andantimicrobial resistance testing includes: autoclave,refrigerator, freezer, Bunsen burner, microscope(100X), hand lens, centrifuge, balance. Additionalsupplies (media and equipment) are summarizedin a WHO manual for the national surveillance ofantimicrobial resistance of S. pneumoniae andH. influenzae (71).
Salient features of standard laboratory tests fordetecting resistance are summarized in Table 5. Boththe agar and broth microdilution tests are consid-ered “gold-standard” methods for estimating theMIC of a particular antimicrobial agent. Antimi-crobial agents are typically tested at twofold serialdilutions and the lowest concentration that inhib-its bacterial growth is the MIC. MICs estimatedby these tests are highly accurate and repeatable.While both methods of MIC-testing do not requireadditional equipment from that needed for bacte-rial isolation, they require technical expertise andadditional reagents. Moreover, they are both labour-
TABLE 5. ADVANTAGES AND DISADVANTAGES OF DIFFERENT LABORATORY METHODS OF PNEUMOCOCCAL SUSCEPTIBILITY TESTING
Agar microdilution Broth microdilution E-test Disk diffusion
Accuracy Well-standardized repeatable Well-standardized repeatable High agreement with micro- Qualitative test; does notdilution methods (69) estimate MIC
Cost Moderate Moderate Expensive Cheap
Timeliness Time-consuming to prepare Time-consuming to prepare 16-20h incubation 16-18h incubation
Technical skills and Moderate Moderate Low Lowequipment required
Source of sample Requires pneumococcal isolate Requires pneumococcal isolate Requires pneumococcal isolate Requires pneumococcal isolate
Sustainability of Antibiotic solutions lose viability; Antibiotic solutions lose viability; Strips can be stored refrigerated Disks can be stored refrigeratedreagents reagents cannot be prepared eagents cannot be prepared for long periods of time for long periods of time
too far in advance too far in advance
Use for treatment of Good Good Good Moderateindividuals*
Use for monitoring Good Good Good Only allows for a cruderesistance monitoring of trends
* Most treatment of pneumococcal disease is empiric; moreover resistance has only been shown to have a clinical impact for particular syndromes (see Section A).Thus, susceptibility-testing to guide treatment is of use only in limited cases.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
16
allowed to diffuse onto an agar plate inoculated withthe test organism. Several strips with different agentscan be placed on a single plate. The MIC is read asthe concentration of antibiotic at the point wherethe zone of inhibition intersects with the strip. Thistest combines the simplicity of disk-diffusion withthe quantitative results of dilution methods. How-ever, the pre-formed plastic strips are significantlymore expensive than the reagents necessary for theabove methods.
Rapid methods for detecting β-lactam andsulfamethoxazole resistance
Currently, isolating pneumococci from clinicalspecimens and determining penicillin susceptibil-ity takes 2–3 days. Assessment of β-lactam ortrimethoprim resistance can also be obtained byDNA sequence analysis of resistance geneamplicons. Such analysis is faster than culture-basedapproaches and has a low probability of generatingartefactual results. Newer, fingerprinting and nestedPCR approaches have the potential to allow forpneumococcal identification and susceptibility test-ing within a few hours.
All of these tests require an extremely high levelof technical expertise and highly-specialized PCRand sequencing equipment as well as high-qualitylaboratory facilities. These methods are currentlystill under development and are not standardizedor routinely performed. They are not at this pointfeasible for the vast majority of developing coun-tries although specialized laboratories are beginningto utilize these techniques.
2. Clinic-based methods
Currently there are no clinic-based methods foridentification of pneumococcal resistance. Pneumo-coccal isolation is required and this must be per-formed in a laboratory. A urine antigen test iscurrently under development. The utility of such atest at this point remains unclear; it appears todetect pneumococcal carriage as well as infectionand thus is unlikely to be a useful diagnostic tool,particularly for children where pneumococcal car-riage is common. Additionally, because an isolateis not obtained, this test does not allow for sero-type or resistance testing.
3. Summary: Detection of resistance
● Methods of detecting pneumococcal resistanceappropriate for developing country laboratoriesare summarized in a WHO manual for thenational surveillance of antimicrobial resistanceof S. pneumoniae and H. influenzae. The goldstandards are broth and agar microdilution.
● All methods require isolation of a pure bacterialculture, followed by susceptibility testing, andtake at least 3 days to complete.
● There are no clinic-based tests that can be per-formed to assess resistance.
4. Research needs: Detection of resistance
More research into rapid, inexpensive methods fordetecting resistance is necessary. The E-test offers apromising alternative to broth and agar micro-dilution but currently remains more expensive thanmost developing countries can afford. It may bepossible to determine meaningful cut-offs for thedisk diffusion method that can serve as a surrogatefor quantitative MIC testing.

17
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
D. Treatment
In response to the emergence of antibiotic-resistant pneumococci, practitioners in industrial-ized countries are starting to revise managementstrategies for pneumococcal infections.
Kaplan and Mason (45) review a number of pro-posed modifications for the treatment of meningi-tis, bacteraemia, pneumonia, and upper respiratoryinfections caused by resistant pneumococci. Arecent report from the Drug-resistant Streptococcuspneumoniae Therapeutic Working Group recom-mends oral amoxicillin as the first-line antibioticfor the treatment of acute otitis media, but recom-mends increasing the standard dosage to 80–90 mg/kg/day (51).
2. Definition of cure: no pathogensor no symptoms?
Clinical outcome is typically the primary outcomeof concern for pneumococcal infections. However,bacterial eradication is more sensitive in differenti-ating effective from ineffective treatments. Eradi-cation of the pathogen can be difficult, but a recentstudy showed that successful early bacterial eradi-cation in children with acute otitis media resultedin a better clinical outcome (74). Additionally, bac-teriological outcome often can only be measuredby an invasive procedure, for example bloodculture or tympanocentesis. Moreover, becausepneumococcus is normally carried as a commensalin the nasopharynx, eradication of carriage is not afeasible outcome.
3. Data to support the efficacy of treat-ment guidelines to cure and the impactof treatment guidelines on resistance atthe individual and population level
Efficacy of treatment guidelines
A number of studies have assessed the effectivenessof the WHO ARI-management strategy at improv-ing childhood survival. A review of six publishedstudies assessing pneumonia case-managementfound that infant mortality was reduced by 15.9deaths per 1000 live births and that mortality
1. Standard treatment guidelines fordisease management
As part of IMCI, WHO developed guidelines forthe management of ARI that rely on detection ofcases based on simple clinical signs (25). Recom-mended outpatient antibiotic therapy includeseither co-trimoxazole bid, for 5 days (children <1yr should receive 1/2 adult tablet per dose; chil-dren 1–5 years should receive 1 adult tablet) oramoxicillin, tid for 5 days (approximately 40 mg/kg/day). For ear problems, WHO guidelines rec-ommend the following: patients with mastoiditisshould be given an immediate dose of antibioticsand be referred to a hospital for further treatment;children with acute ear infections should be pre-scribed a 5-day course of antibiotics; those withchronic ear problems should not be given anti-biotic therapy but should be followed. Similarly,patients with serious pneumonia should be hospi-talized and given a dose of antibiotics immediately.Less severe pneumonia should be treated with a5-day course of antibiotics. Patients with coughsand colds should not be given antibiotic therapy.Meningitis patients require immediate hospitaliza-tion and antibiotics. Children with any clinical signsand severe malnutrition are also categorized in thesevere disease category. While the threshold for pre-scribing antibiotic therapy for respiratory infectionin children with severe malnutrition or immuno-suppression may be lower, it is equally importantin these children to use antibiotics prudently be-cause resistant infections pose an even greater threatto these children.
The WHO guidelines are not intended for in-dustrialized countries. Most of these countries donot have unified guidelines for the treatment ofpneumococcal disease, although professional soci-eties, for example the American Thoracic Society(72) and the Infectious Diseases Society of America(73), have published recommendations for thetreatment of community-acquired pneumonia inadults. In the recommendations from these twosocieties, first-line agents for outpatient therapyinclude macrolides and tetracycline.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
18
among children <5 years of age was reduced by 36deaths/1000 live births (2). A controlled interven-tion trial among children under 5 years in Nepalfound that subdistricts that were served by healthcare workers using the WHO strategy had a 28%reduction in the risk of death from all causes bythe third year of implementation (75). The great-est risk reduction was in infants and deaths due toother conditions such as diarrhoea and measles alsodeclined. A similar targeted ARI programme inrural Bangladesh led to a 28% decline in ARI mor-tality in the intervention area; the combination ofARI-targeted programmes with non-ARI specificinterventions reduced overall mortality by as muchas 50% (76).
Efficacy of treatment guidelines to limit resistance
Programmes to encourage judicious antibiotic useare the only treatment guidelines that have beenevaluated for their impact on pneumococcal resist-ance. Countrywide initiatives to reduce antibioticresistance by reducing antibiotic use were attemptedin Finland for the case of macrolide-resistant groupA streptococci (GAS), and in Iceland for the caseof penicillin-resistant S. pneumoniae. GAS has somefeatures in common with S. pneumoniae includingthe genetic mechanism of erythromycin resistanceand a carriage state. In Finland, in response to adramatic rise in the prevalence of erythromycin-resistant GAS from 5% in 1988–1989 to 13% in1990, national guidelines recommending reduc-tions in the outpatient use of macrolide antibioticswere issued in 1991. Total macrolide consumptionin outpatient therapy declined from 2.4 daily dosesper 1000 inhabitants in 1991 to a level of 1.38 in1992; the daily doses per 1000 inhabitants re-mained between 1.28 and 1.74 during the next 5years (77). From 1992 to1996 the prevalence oferythromycin-resistant GAS isolates also decreasedfrom 16.5% in 1992 to 8.6% in 1996. This de-cline was evident after 1993, approximately twoyears after the release of national guidelines. Thus,a reduction in antibiotic use was associated with asubsequent decline in the prevalence of resistantGAS strains although a causal link cannot beestablished because of the observational study de-sign. However, although the prevalence of resist-ant GAS declined, it remained at close to 9%;moreover an apparent increase in the consumptionof azithromycin and roxithromycin that correlatedwith declines in erythromycin use may reflect a shift,rather than a sustained reduction in macrolide use.
In Iceland, the incidence of penicillin-resistantpneumococci among patients with invasive pneu-mococcal disease increased from 0% in 1988 to16.3% in 1992 (78). A majority of penicillin-resistant strains were also resistant to macrolide an-tibiotics and to trimethoprim/sulfamethoxazole.The country responded to this rapid increase inresistant pneumococci by launching a public healthcampaign against the overuse of antibiotics that wasaimed both at the public and at physicians. Addi-tionally, children undergoing antibiotic therapy, andknown carriers of non-susceptible pneumococciwith colds or coughs were discouraged from goingto day-care centres. The number of daily doses ofantibiotics in Iceland decreased from 23.6/1000inhabitants in 1990 to 21.4 in 1994, due largely todecreased use of macrolides and trimethoprim/sulfamethoxazole (78). The incidence of penicil-lin-resistant invasive pneumococcal isolates declinedfrom a peak of 19.8% in 1993 to 18.6% in 1994;among pneumococcal carriers, the proportion ofhealthy children attending day care that were colo-nized by a resistant strain decreased from 20% in1992 to 16% in 1995 (78). These data are also sug-gestive of a decline particularly within the contextof rapid rise in resistance in Iceland in previousyears.
Two recent controlled studies assessed the im-pact of well-defined judicious antibiotic use inter-ventions on antibiotic prescribing practices and theincidence of resistant pneumococcal strains. Theimpact on antibiotic prescription rates of an inter-vention targeting four adult primary care practicesin Denver, Colorado, United States was evaluatedusing a prospective, non-randomized controlledtrial design (79). The intervention, which wasaimed at reducing antibiotic prescribing for outpa-tient adults diagnosed with uncomplicated acutebronchitis, consisted of household and office-basedpatient educational materials, and clinician educa-tion, practice profiling and academic detailing.During the one-year study period, practices whichreceived the full intervention showed a significantdecline in antibiotic prescription rates, from 74%to 48%, whereas no significant decline was detectedfor control sites (79). Practices which received onlya limited intervention, which consisted solely ofoffice-based educational materials, also did notshow significant declines. While this study did notaddress the impact of reduced prescription rates onthe incidence of resistant pneumococci, it does sug-gest that active education of clinicians about theimportance of judicious antibiotic use can lead to
19
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
reduced rates of antibiotic prescription.An evaluation of judicious antibiotic use inter-
ventions in Alaskan villages (80) was designed toevaluate both antibiotic prescribing rates and theprevalence of non-susceptible pneumococci invillages receiving the intervention and in controlvillages. The intervention focused on otitis mediaand consisted of an educational programme forvillage health aides and their consultants, workshopson the appropriate diagnosis of otitis media, andinformation sheets to providers, and village resi-dents. Respiratory health care visits for children <5years decreased by 23% and antimicrobial prescrip-tions per respiratory visit decreased by 22% in theintervention region while no declines were evidentin control villages which did not receive the inter-vention (81). Additionally, although the overallprevalence of pneumococcal carriers did not de-crease in the intervention area, the proportion ofall pneumococcal isolates that were non-suscepti-ble to penicillin (MIC ≤0.1 mg/ml) declined by28% in the intervention region, but did not de-cline significantly in the control regions (81).
Thus, studies from the village to country levelsdemonstrate that judicious antibiotic use interven-tions can result in reduced antibiotic prescriptions.Evidence that such interventions also lead to de-creases in pneumococcal resistance is less strong.Declines in penicillin-resistant pneumococci in Ice-land, and in Alaskan villages receiving interventionssuggest that judicious use campaigns may have thepotential to limit the spread of resistant pneumo-cocci. Controlled studies of interventions designedto look at the prevalence of resistant pneumococcias an outcome are needed to further address theeffectiveness of this class of interventions.
4. Data showing relationship betweenemergence of resistance and drugquality, misdiagnosis, use of a relateddrug for another disease, suboptimalregimens, use of drugs in humans andanimals
The key factor influencing the emergence of resist-ant pneumococci is unnecessary antibiotic use forviral respiratory infections in humans. This is duein part to misdiagnosis of conditions because bothviral and bacterial agents can cause clinical syn-dromes associated with pneumococcal infection,and community-acquired pneumonia, otitis mediaand acute respiratory infections are typically treatedempirically. It is also due to overuse of antibioticsin humans because of a variety of factors includ-
ing: lack of awareness among physicians of the as-sociation between increased antibiotic use and theincreased risk of resistant disease in their individualpatients; pressure from patients for a rapid cure fortheir illness; and the speed and simplicity of pre-scribing an antibiotic rather than explaining to apatient why one is not necessary. In some develop-ing countries antibiotics are available without pre-scriptions and this potentially facilitates overuse,although the expense of antibiotics often detersindiscriminate use of antibiotics in these settings.We note, however, that while unnecessary anti-biotic use is a problem in some cases, in develop-ing countries where access to health care is difficulta number of children requiring antibiotic therapydo not have the opportunity or resources to receiveit. Thus while inappropriate antibiotic use is a keyproblem contributing to resistance, the issues arenot exactly analogous to those in the developingworld.
The use of similar drugs for unrelated condi-tions also contributes to the problems of resistance.For example, widespread use of sulfadoxine/pyrimethamine as a treatment for malaria leads toan increased risk of carrying co-trimoxazole-resistant pneumococci (82). It is also possible thatwidespread use of co-trimoxazole to treat respira-tory infections contributes to Fansidar-resistantPlasmodium in malaria-endemic regions.
Mass chemoprophylaxis campaigns to preventconditions such as trachoma and sexually-transmit-ted diseases also have the potential to increase theburden of pneumococcal resistance in a number ofdeveloping countries where resistance does not cur-rently pose a serious public health threat. A recentinitiative in a number of African countries to eradi-cate trachoma using mass azithromycin prophylaxismay lead to increases in resistant pneumococci. Astudy of the impact of mass prophylaxis in an abo-riginal village in Australia found that macrolideresistance increased from very low levels (1%) to ashigh as 21% of isolates 2 months after treatment,and persisted above the baseline level for the entire6-month observation period (67). While macrolidesare not commonly used to treat respiratory infec-tions in developing countries because of their highcost, macrolide resistance in pneumococci is oftenassociated with resistance to other more commonlyused antibiotics such as amoxicillin and co-trimoxazole. The biological basis of this association,which has been observed repeatedly, is not fullyunderstood and may be driven in part by the asso-ciation between serotype and resistance profiles. If

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
20
6. Ethical issues: benefits to individual vs.benefits to community
Judicious antibiotic use has the potential to ben-efit individuals as well as the community. At thecommunity-level, the incidence of antibiotic usecorrelates with the prevalence of resistance. Moreo-ver, communities which have implemented poli-cies to reduce antibiotic use have often experienceddeclines in the prevalence of resistant pathogens (57,77). Benefits to the community are likely long termsince the time scale for declines can be slow. Forthe case of individuals, recent antibiotic use is as-sociated with an increased risk that individuals carryresistant pneumococci after treatment. Thus indi-viduals who use antibiotics judiciously are at areduced risk of carrying resistant pneumococci com-pared to those that take them indiscriminately. Theyare also at a reduced risk of developing invasive dis-ease caused by a resistant strain. This benefit is shortterm, since the average duration of pneumococcalcarriage is 2–3 months.
7. Drug policy strategies and the data onwhich they are based: switch, rotation,reservation, combination drugs
The strategies of drug switching and drug cyclingwere developed primarily in the context of noso-comially-acquired infections, such as those causedby vancomycin-resistant enterococci or methicil-lin-resistant Staphylococcus aureus. In contrast, thevast majority of pneumococcal infections are com-munity acquired, and the implementation of drugcycling at a community level is not straightforward.Moreover, the success of drug cycling at reducingthe spread of resistance remains controversial evenin the nosocomial setting. Combination therapyfor pneumococcal disease is used in some cases toincrease clinical efficacy, but has not been used as amethod of preventing resistance. Because within-host evolution of resistant pneumococci by pointmutation is extremely rare, it is not clear whethercombination therapy represents an effective inter-vention, as it does in the case of tuberculosis andHIV (Table 6).
8. Summary: Treatment
● The WHO algorithm for the treatment of ARIas part of the IMCI programme is the recom-mended method of managing pneumococcal dis-ease among children in developing countries.
mass chemoprophylaxis against trachoma results inan increase in the prevalence of pneumococci thatare resistant to β-lactams and co-trimoxazole, thiswould pose a serious threat to the effective treat-ment of acute respiratory infections in these coun-tries, and would also increase the potential for suchstrains to spread to regions where trachoma con-trol programmes are not implemented.
Other factors such as reduced drug quality andsuboptimal regimens may also play a role in theemergence of pneumococcal resistance. Suboptimaland long-duration regimens increase the opportu-nity for acquisition and/or amplification of resist-ant S. pneumoniae. The importance of these factorsis difficult to determine, but is likely to play asmaller role than inappropriate use of antibiotics(e.g. use of antibiotics for viral respiratory infec-tions). Use of similar antibiotics in animals is notan issue of central concern for pneumococci,because animals are not a reservoir for this bacteriaand plasmid-borne resistance is rare relative to thatconferred by transformation and conjugativetransposons.
5. Strategies for improving treatment andevidence that these will contain spread
Because the primary genetic mechanism of resist-ance in pneumococci is transformation as opposedto point mutation, resistance is thought to arise denovo only rarely in individuals. Interventions tocontain the spread of resistance in pneumococcithus differ in important ways from those used forpathogens where resistance typically evolves frominitially sensitive pathogen populations in responseto antibiotic-mediated selective pressure (Table 6).
One potential area for intervention is modifica-tion of standard antibiotic treatment regimens.Recent evidence suggests that shorter treatmentcourses are sometimes clinically as effective as stand-ard treatments. Shorter-course therapies are easierfor patients to complete with a high level of com-pliance. Observational studies have also suggestedthat short-course, high-dose therapy may reducethe risk that individuals carry resistant pneumo-cocci after antibiotic therapy (83). Simple modifi-cations of treatment regimens represent a feasible,low-cost intervention to limit the spread of resist-ance in developing countries.

21
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
● The goal of treatment is clinical cure; bacterio-logical cure is often a better outcome for clini-cal efficacy trials.
● Inappropriate use of antibiotics is a key factordriving pneumococcal resistance. Overuse forviral respiratory infections contributes toresistance; this is common in industrializedcountries and in some developing settings. In-terventions encouraging judicious antibioticuse can address this problem, and have had someimpact in industrialized countries. In somedeveloping settings, however, limited access tohealth care still prevents children from receiv-ing antibiotics when they are necessary, andjudicious antibiotic use campaigns have not beena high public health priority.
● Use of closely related drugs for other conditionsalso plays a role in the spread of resistance.
● Use of Fansidar to treat malaria can lead to anincrease in co-trimoxazole-resistant pneumo-cocci.
● Mass antibiotic chemoprophylaxis for conditionssuch as trachoma and sexually-transmitted dis-eases also has the potential to increase resistancein respiratory pathogens.
● Alterations of antibiotic dose and duration oftreatment that maintain clinical efficacy maydecrease an individual’s risk of acquiring resist-ant pneumococci post treatment
TABLE 6. PRINCIPLES OF PREVENTING THE DEVELOPMENT AND TRANSMISSION OF RESISTANCE DUE TO ANTIMICROBIAL THERAPY*
Pathogens where a carrier state is uncommon** Pathogens with a carrier state
Examples of pathogens Plasmodium falciparum, Shigella, Mycobaterium S. pneumoniae, Haemophilus influenzae,, Moraxella catarrhalis,tuberculosis group A streptococci
Overall goal To prevent the development of resistance during treatment To prevent the acquisition or amplification of resistant strains at thesite of carriage during treatment
Method 1: Avoid Minor concern Major concernunnecessary antibiotics(e.g. for viral infections)
Method 2: Modify Longer-course treatment is preferred over short course to Short-course therapy may be advantageous because the timetreatment duration ensure the pathogen has been eradicated. Failure to eradicate period during which an individual may acquire a resistant strain is
the pathogen results in clinical treatment failure reduced. Eradication of the pathogen from the site of carriage is nota practical therapeutic goal
Method 3: Use high Rationale: High dosages can eradicate both intermediate and Impact on bacterial carriage unknown. Eradication of pathogendosages high-level resistant pathogens facilitating pathogen eradication from the site of carriage is not a practical therapeutic goal, even for
and reducing the opportunity for resistant mutants to proliferate high dose therapy
Method 4: Treat with drugs Likely to have only a minor impact; drugs which do not exert a Likely to have only a minor impact. May reduce the probability ofthat minimize the selection strong selective pressure are typically less efficient at eradicating unmasking of minority resistant strains or acquisition of resistant for resistance the pathogen strains from the community
Method 5: Treat with Rationale: Resistance is often due to point mutations, insertions, Impact unknown. May not be effective for pneumococci, since demultiple drugs deletions. The likelihood of a single genetic event conferring novo resistance due to point mutations, insertions and deletions
resistance to multiple drugs is the product of the separate alone is rarelikelihoods
Method 6: Cycling of drugs Impact unclear; may be useful for hospital-acquired infections Unlikely to be effective because the majority of infections arecommunity-acquired, and because the pathogens are often exposedto drugs used for the treatment of unrelated conditions
Method 7: Encourage Erratic treatment allows pathogen to proliferate at sub- Unclear whether poor compliance increases or decreases the risk ofadherence to treatment therapeutic MICs, increasing the opportunity for resistant carrying resistant pneumococciregimen mutants to amplify
* Reproduced with permission, Schrag et al. Clinical Microbiology Reviews 2000;13:588–601.** Carrier state refers to cases where pathogen populations are commonly present asymptomatically in the nasopharynx, vaginal or intestinal tract, and where such
asymptomatic populations serve as primary reservoirs for disease transmission. While diseases such as HIV and TB have latent periods, these periods are associatedwith low levels of pathogen replication and are thus not associated with high risk of acquiring resistance or transmitting the disease.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
22
9. Research needs: Treatment
1. Study the effect on pneumococcal resistance ofdrugs used for other conditions
a. The impact of co-trimoxazole use on Fansidarresistance.
b. The impact of mass azithromycin prophylaxison respiratory pathogen resistance.
2. Study the impact of dose and duration of treat-ment on the risk of carrying resistant pneumo-cocci post treatment.
3. Evaluate the effectiveness of the WHO algorithmfor managing adult ARI.
4. Assess the impact of antibiotic control pro-grammes on pneumococcal resistance.

23
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
E. Prevention of pneumococcal disease
nary data suggest that these vaccines are appropri-ate for children <2 years of age. No significant safetyproblems associated with vaccination have occurredin Phase I-III trials conducted since 1992 (85).Clinical trials show that the vaccine is highly effec-tive at preventing invasive disease due to serotypesincluded in the vaccine (86, 87). The vaccine alsohas some efficacy against non-invasive disease (85).
It is likely that the cost of the vaccine will makeit unavailable to many developing countries. Inaddition to preventing invasive pneumococcal dis-ease, however, the conjugate pneumococcal vaccinealso has great potential as an “anti-resistance” vac-cine. There are also preliminary data suggesting thatthe pneumococcal conjugate vaccine reducescarriage of vaccine serotypes (88, 89), similar tothe conjugate Haemophilus influenzae type b vac-cine (e.g. (90)). This effect has been demonstratedin infants (89) as well as toddlers (63), and raisesthe possibility that the conjugate vaccine may beeffective at preventing colonization with vaccine-related serotypes, thus reducing the opportunity fortransmission of these serotypes within communi-ties. Because the serotypes in current formulationsof the vaccine include paediatric serotypes that arecommonly associated with antibiotic resistance,vaccination of infants may potentially reduce thecirculation of antibiotic-resistant strains (89).Additionally, if the conjugate vaccine is effective atpreventing invasive disease in children, and in par-ticular if it reduces the rate of otitis media, antimi-crobial therapy for pneumococcal infections is likelyto decline, thus reducing the selective pressure forresistance. There is the possibility, however, thatthe vaccine prevents carriage of vaccine-includedserotypes only. Evidence from a vaccine trial in theGambia (88) and a recent study of day-careattendees in Israel (91) suggest that carriage of non-vaccine serotypes increases following vaccination,although a previous study in Israel did not findevidence of increased carriage of non-vaccineserotypes in toddlers in Israel (92). The impact ofmass vaccination on carriage of non-vaccineserotypes remains to be seen, as well as whether
1. Known interventions
Pneumococcal polysaccharide vaccine
A polysaccharide vaccine is currently availablewhich can protect individuals >2 years of age againstinvasive pneumococcal infections caused by com-mon S. pneumoniae serotypes. The efficacy of thisvaccine varies depending on a person’s age and im-mune status; in case-control studies the effective-ness of the vaccine against invasive disease hasranged from 56% to 81% (84). Strongest recom-mendations for vaccination are for people over 65years of age, and people aged 2–64 years with thefollowing risk factors: chronic cardiovascular dis-ease, chronic pulmonary disease, diabetes mellitus,or functional asplenia (84).
The polysaccharide vaccine has the followinglimitations: it does not induce an effective immuneresponse in children less than 2 years old, an agegroup with a high burden of disease in developingcountries; it does not protect against non-bacteraemic pneumococcal disease or commonupper respiratory diseases (e.g. acute otitis media,sinusitis); it does not protect against carriage ofpneumococci; declining antibody levels followingvaccination suggest that vaccine-induced immunitymay wane over a 5–10 year period.
The fact that the vaccine is not indicated forchildren <2 years of age and is primarily recom-mended for the elderly prevents it from being aneffective intervention against pneumococcal diseasein most developing country settings.
2. Interventions currently undergoingtesting
Pneumococcal conjugate vaccine
Pneumococcal conjugate vaccines, where purifiedpolysaccharide of the epidemiologically most im-portant serotypes are conjugated to a carrier pro-tein, are currently undergoing clinical trials. A7-valent formulation is expected to obtain FDAlicensure by the year 2000, and an 11-valent for-mulation is also undergoing clinical trials. Prelimi-

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
24
widespread use of the conjugate vaccine increasesthe selective pressure for serotype switching or theacquisition of antibiotic resistance in strains notcovered by the vaccine. Whether widespread use ofthe conjugate vaccine will increase the selective pres-sure for serotype switching in the serotypes cov-ered by the conjugate vaccine, and whether thenon-vaccine serotypes will be more likely to acquireantibiotic resistance if populations of the commonpaediatric serotypes decline remain to be seen.
Because of the great potential of the conjugatevaccine to reduce both the burden of disease andresistance, evaluation of the impact of the conju-gate vaccine is a top research priority.
Vitamin A
High-dose vitamin A supplements have been shownto reduce morbidity and mortality in children withacute measles infection (93). This, along with evi-dence that vitamin A plays a role in maintainingmucosal and lymphoid tissues and that reducedvitamin A levels in serum are associated withmeasles, varicella and respiratory syncitial virus in-fections (94), has led to the hypothesis that vita-min A supplements may be an effective interventionagainst ARI in children. A clinical trial testingwhether high-dose vitamin A enhanced recoveryof children 3 months to 10 years of age hospital-ized for community-acquired pneumonia in Perufound that vitamin A was associated with increasedrather than decreased clinical severity relative to theplacebo group. The role of vitamin A in protectingagainst severe pneumococcal infections has not beendirectly investigated, although studies in develop-ing countries have in some cases suggested thatvitamin A supplements may protect against severeARI in children (95, 96). Clinical trials of high-dose vitamin A in children with respiratory syncitialvirus infection have failed to find a benefit to sup-plementation (97) and in one case found a detri-mental effect of vitamin A supplementation (98).Consequently, use of high-dose vitamin A as a thera-peutic intervention for ARI should be consideredwith caution in patients without known vitamin Adeficiency or concurrent measles infection untilfurther evidence is available.
Xylitol sugar
Xylitol is a sugar that has been used as a sweeten-ing substitute for sucrose because it has a preven-tive effect against dental caries. Recent evidencesuggests that in addition to inhibiting growth of
Streptococcus mutans, the primary cause of dentalcaries, this sugar can inhibit the growth of S.pneumoniae, and possibly also of other bacterialcolonizers of the nasopharynx such as H. influenzae(99, 100).
A controlled trial of healthy children attendingday-care centres in Finland randomized childrento control groups which received syrup, chewinggum and lozenges sweetened with sucrose and alow concentration of xylitol, or treatment groupswhich received a high daily dose of xylitol in theform of syrup, chewing gum or lozenges (99). Thechildren were then followed for a 3-month periodand information on respiratory infections, acuteotitis media, and antibiotic therapy was collected.While the xylitol exposure did not reduce the meannumber of respiratory infections in treatmentgroups relative to their respective control groups,children who regularly received xylitol in the formof syrup or chewing gum had a significant 30–40%reduction in the occurrence of acute otitis media,and all treatment groups received fewer antibioticprescriptions than controls (99). Prophylactic useof xylitol may thus protect against acute otitis me-dia, particularly for children with high exposure toS. pneumoniae, such as those attending day-care cen-tres. In this study, xylitol in all groups was admin-istered 5 times per day; such frequent dosing maybe difficult to achieve and studies of the minimumdosing required to get a significant protectiveeffect would be useful. Xylitol syrup or chewinggum may be a feasible prophylactic measure in somedeveloping settings, with the potential of reducingantibiotic use.
Additional interventions
Indoor air pollution: Exposure to cigarette smokeand to smoke from some woodburning stoves hasbeen identified as risk factors for invasive pneumo-coccal disease. Thus, limiting exposure to smokemay help reduce the pneumococcal disease burdenin children. Because pneumococcal disease is notwaterborne, and because the primary reservoir isthe human nasopharynx, interventions to improvewater quality and environmental sanitation are notlikely to have any impact on pneumococcaldisease. Educational campaigns to increase handwashing may have a small impact on limiting trans-mission.

25
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
3. Summary: Prevention of pneumococcaldisease
● A pneumococcal polysaccharide vaccine cur-rently is licensed and offers protection againstinvasive pneumococcal pneumonia. This vaccineis recommended primarily for use in the elderlyand people with risk factors for pneumococcaldisease; it is not recommended for children <2years of age. It is unlikely that this vaccine willdecrease the prevalence of pneumococcal resist-ance.
● A pneumococcal conjugate vaccine is currentlyundergoing Phase III clinical trials and licensurewas anticipated by the year 2000. This vaccineinduces immunity in children <2 years of age,and appears highly effective at preventing inva-sive disease due to the serotypes covered by thevaccine. The vaccine also has some efficacyagainst non-invasive pneumococcal disease, andreduces carriage of vaccine-serotypes. Althoughexpensive, this vaccine has great potential to re-duce the burden of pneumococcal disease inchildren, and to reduce carriage of antibiotic-resistant strains covered by the 7- and 11-valentformulations.
● Xylitol sugar reduces otitis media and antibioticuse by 30%.
● Reduced exposure to smoke may help reduce therisk of pneumococcal disease; vitamin A sup-plementation should be approached withcaution because of observed adverse effects insome studies.
4. Research needs: Prevention ofpneumococcal disease
1. The pneumococcal conjugate vaccine is the mostpromising intervention to date to reduce theburden of pneumococcal disease in children.Because the vaccine has the potential to reducethe incidence of pneumococcal disease and re-sistance, investigations of the impact of the con-jugate vaccine should be a high research priority.Beyond clinical efficacy against invasive disease,a number of areas should be investigated oncevaccine licensure is obtained:
— Measure the efficacy of the vaccine atpreventing carriage of vaccine-includedserotypes
— Assess the impact of vaccination on theprevalence of antibiotic-resistant S. pneumo-niae in nasopharyngeal and invasive diseaseisolates
— Determine whether non-vaccine serotypesreplace vaccine serotypes in the nasophar-ynx
— Determine whether invasive disease due tonon-vaccine serotypes increases
— Measure the efficacy of the vaccine at pre-venting acute otitis media and mild pneu-monia
— Assess whether vaccination reduces anti-biotic use in children <5 years of age
— Determine whether vaccination results inherd immunity.
2. Conduct large controlled clinical trials in devel-oped and developing countries to assess theeffectiveness of xylitol sugar at reducing acuteotitis media and antibiotic use in children.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
26
F. Bibliography
15. Leach AJ et al. Report of a multidrug resistant cloneof Streptococcus pneumoniae in aboriginal infants inthe Northern Territory. Communic Dis Intelligence1995;19:134–137.
16. Voss L et al. Invasive pneumococcal disease in apediatric population, Auckland, New Zealand.Pediatr Infect Dis J 1994;13:873–878.
17. Jernigan DB, Cetron MS, Breiman RF. Minimizingthe impact of drug-resistant Streptococcus pneumoniae(DRSP): A strategy from the DRSP Working Group.JAMA 1996;275:206–209.
18. Eskola J et al. Epidemiology of invasive pneumo-coccal infections in children in Finland. JAMA1992;268:3323–3327.
19. Schuchat A et al. Bacterial meningitis in the UnitedStates in 1995. N Engl J Med 1997; 337:970–976.
20. Dagan R, Englehard D, Piccard E. Epidemiology ofinvasive childhood pneumococcal infections in Is-rael. JAMA 1992;268:3328–3332.
21. Levine MM et al. Epidemiology of invasive pneu-mococcal infections in infants and young childrenin Metropolitan Santiago, Chile, a newly industri-alizing country. Pediatr Infect Dis J 1998;17:287–293.
22. Kertesz DA et al. Invasive Streptococcus pneumoniaeinfection in Latin American children: results of thePan American Health Organization SurveillanceStudy. Clin Diagn Lab Immunol 1998;5:176–180.
23. Forgie IM et al. Etiology of acute lower respiratorytract infections in children in a rural community inThe Gambia. Pediatr Infect Dis J 1992;11:466–473.
24. Campagne G et al. Epidemiology of bacterial men-ingitis in Niamey, Niger, 1981–1996. Bull WorldHealth Org 1999;77:499–508.
25. Gove S. Integrated management of childhood ill-ness by outpatient health workers: technical basisand overview. Bull World Health Org 1997;75 (Suppl.1):7–24.
26. Zenni MK et al. Streptococcus pneumoniae coloniza-tion in the young child: association with otitismedia and resistance to penicillin. J Pediatr 1995;127:533–537.
27. Gray BM, Converse GM, Dillon HC. Epidemio-logic studies of Streptococcus pneumoniae in infants:acquisition, carriage , and infection during the first24 months of life. J Infect Dis 1980; 142:923–933.
1. Berman S. Epidemiology of acute respiratory infec-tions in children of developing countries. Rev InfectDis 1991;13 (Suppl. 6):S454–S462.
2. Sazawal S, Black RE. Meta-analysis of interventiontrials on case-management of pneumonia in com-munity settings. Lancet 1992;340:528–533.
3. Obaro SK, Monteil MA, Henderson DC. Fort-nightly review: the pneumococcal problem. Br MedJ 1996;312:1521–1525.
4. O’Dempsey TJD et al. A study of risk-factors forpneumococcal disease among children in a rural areaof West Africa. Int J Epidemiol 1996;25:885–893.
5. Gesner M et al. Streptococcus pneumoniae in humanimmunodeficiency virus type 1-infected children.Pediatr Infect Dis J 1994;13:697–703.
6. Gilks CF et al. Life-threatening bacteraemia in HIV-1 seropositive adults admitted to hospital in Nai-robi, Kenya. Lancet 1990;336:545–549.
7. Nathan EA. A report on pneumonia at the PremierDiamond Mine. Transvaal Med J 1907;2:154–159.
8. O’Dempsey TJ et al. Pneumococcal disease amongchildren in a rural area of West Africa. Pediatr InfectDis J 1996;15:431–437.
9. Davidson M et al. The epidemiology of invasivepneumococcal disease in Alaska, 1986–1990. J In-fect Dis 1994;170:368–376.
10. Hofmann J et al. The prevalence of drug-resistantStreptococcus pneumoniae in Atlanta. New Engl J Med1995;333:481–486.
11. Whitney C et al. Increasing prevalence of multidrug-resistant Streptococcus pneumoniae in the UnitedStates. N Engl J Med 2000;343:1917–1924
12. Usen S et al. Epidemiology of invasive pneumococ-cal disease in the Western Region, The Gambia.Pediatr Infect Dis J 1998;17:23–28.
13. Gratten M et al. Colonisation of Haemophilusinfluenzae and Streptococcus pneumoniae in the up-per respiratory tract of neonates in Papua NewGuinea: Primary acquisition, duration of carriage,and relationship to carriage in mothers. Biol Neonate1986;50:114–120.
14. Gratten M et al. Multiple colonization of the upperrespiratory tract of Papua New Guinea childrenwith Haemophilus influenzae and Streptococcuspneumoniae. SE Asian J Trop Med Pub Health1989;20:501–509.

27
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
28. Brook I, Gober AE. Bacterial interference in thenasopharynx following antimicrobial therapy ofacute otitis media. J Antimicrob Chemother 1998;41:489–492.
29. Vives M et al. Nasopharyngeal colonization in CostaRican children during the first year of life. PediatrInfect Dis J 1997;16:852–858.
30. Hansman D et al. Pneumococcal carriage amongstAustralian aborigines in Alice Springs, NorthernTerritory. J Hyg 1985;95:677–684.
31. Hodges RG, MacLeod CM, Bernhard WG. Epi-demic pneumococcal pneumonia. III. Pneumococ-cal carrier studies. Am J Hygiene 1946;44:207.
32. Klugman KP. Pneumococcal resistance to antibiot-ics. Clin Microbiol Rev 1990; 3:171–196.
33. Smith T et al. Acquisition and invasiveness of dif-ferent serotypes of Streptococcus pneumoniae in youngchildren. Epidemiol Infect 1993;111:27–39.
34. Centers for Disease Control and Prevention. Geo-graphic variation in penicillin resistance in Strepto-coccus pneumoniae—Selected sites, United States,1997. MMWR 1999;48:656–661.
35. Mastro TD et al. Use of nasopharyngeal isolates ofStreptococcus pneumoniae and Haemophilus influenzaefrom children in Pakistan for surveillance for anti-microbial resistance. Pediatr Infect Dis J 1993;12:824–830.
36. Ostroff SM et al. Resistance patterns of Streptococ-cus pneumoniae and Haemophilus influenzae isolatesrecovered in Egypt from children with pneumonia.Clin Infect Dis 1996; 23:1069–1074.
37. Lehmann D, Gratten M, Montgomery J. Suscepti-biltiy of pneumococcal carriage isolates to penicillinprovides a conservative estimate of susceptibiltiy ofinvasive pneumococci. Pediatr Infect Dis J 1997;16:297–305.
38. Kellener JD et al. The use of Streptococcus pneumoniaenasopharyngeal isolates from healthy children topredict features of invasive disease. Pediatr Infect DisJ 1998; 17:279–286.
39. Appelbaum PC. Antimicrobial resistance in Strepto-coccus pneumoniae: an overview. Clin Infect Dis1992;15:77–83.
40. Song JH et al. Spread of drug-resistant Streptococcuspneumoniae in Asian countries: Asian Network forSurveillance of Resistant Pathogens Study. Clin In-fect Dis 1999;28:1206–1211.
41. Kurien T. Invasive Bacterial Infection SurveillanceGroup, International Clinical Epidemiology Net-work. Prospective multicentre hospital surveillanceof Streptococcus pneumoniae disease in India. Lancet1999;353:1216–1221.
42. John CC. Treatment failure with use of a third-gen-eration cephalosporin for penicillin-resistant pneu-mococcal meningitis: case report and review. ClinInfect Dis 1994;18:188–193.
43. Guibert M et al. Failure of cefotaxime treatment intwo chidlren with meningitis caused by highly re-sistant penicillin-resistant Streptococcus pneumoniae.Ann Pediatr 1995;84:831–833.
44. Lonks JR et al. Meningitis due to ceftriaxone-resist-ant Streptococcus pneumoniae. New Engl J Med1995;332:893–894.
45. Kaplan SL, Mason EO. Management of infectionsdue to antibiotic-resistant Streptococcus pneumoniae.Clin Microbiol Rev 1998;11:628–644.
46. Schaad UB et al. Pharmacokinetics and bacteriologicefficacy of moxalactam, cefotaxime, cefoperazone,and rocephin in experimental bacterial meningitis.J Infect Dis 1981;143:156–163.
47. Friedland IR, Klugman KP. Cerebrospinal fluid bac-tericidal activity against cephalosporin resistant Strep-tococcus pneumoniae in children with meningitistreated with high dosage cefotaxime. AntimicrobAgents Chemother 1997;41:1888–1891.
48. American Academy of Pediatrics Committee onInfectious Diseases. Therapy for children with invasivepneumococcal infections. Pediatr 1997;99:289–299.
49. Klugman KP, Friedland IR, Bradley JS. Bactericidalactivity against cephalosporin-resistant Streptococcuspneumoniae in cerebrospinal fluid of children withacute bacterial meningitis. Antimicrob AgentsChemother 1995;39:1988–1992.
50. Dagan R et al. Impaired bacteriologic response tooral cephalosporins in acute otitis media caused bypneumococci with intermediate resistance to peni-cillin. Pediatr Infect Dis J 1996;15:980–985.
51. Dowell SF et al. Acute otitis media: managementand surveillance in an era of pneumococcal resist-ance—a report from the Drug-resistant Streptococ-cus pneumoniae Therapeutic Working Group. PediatrInfect Dis J 1999;18:1–9.
52. Friedland IR, McCracken GH. Management of in-fections caused by antibiotic resistant Streptococcuspneumoniae. Drug Therapy 1994;331:377–382.
53. Feikin DR et al. Mortality from invasive pneumo-coccal pneumonia in the era of antibiotic resistance,1995–1997. Am J Pub Health 2000;90:223–229.
54. Coffey TJ et al. Recombinational exchanges at thecapsular polysaccharide biosynthetic locus lead to fre-quent serotype changes among natural isolates of Strep-tococcus pneumoniae. Mol Microbiol 1998; 27:73–83.
55. Kristinsson KG. Epidemiology of penicillin resist-ant pneumococci in Iceland. Microb Drug Resist1995;1:121–125.
56. Baquero F. Epidemiology and management of peni-cillin-resistant pneumococci. Curr Opin Infect Dis1996;9:372–379.
57. Arason VA et al. Do antimicrobials increase the car-riage rate of penicillin resistant pneumococci in chil-dren? Cross sectional prevalence study. Br Med J1996;313:387–391.

RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
28
58. Butler JC et al. The continued emergence of drug-resistant Streptococcus pneumoniae in the UnitedStates: An update from the Centers for Disease Con-trol and Prevention’s pneumococcal sentinel surveil-lance system. J Infect Dis 1996;174:986–993.
59. Nowak R. Hungary sees an improvement in peni-cillin resistance. Science 1994;264:364.
60. Kristinsson KG. Effect of antimicrobial use and otherrisk factors on antimicrobial resistance in pneumo-cocci. Microb Drug Resist 1997;3:117–123.
61. Smith HW. Persistence of tetracycline resistance inpig E. coli. Nature 1975;258:628–630.
62. Schrag SJ, Perrot V. Reducing antibiotic resistance.Nature 1996;381:120–21.
63. Dagan R et al. Nasopharyngeal colonization insouthern Israel with antibiotic-resistant pneumococciduring the first 2 years of life: relation to serotypeslikely to be included in pneumococcal conjugatevaccines. J Infect Dis 1996;174:1352–1355.
64. Dowell SF, Schwartz B. Resistant pneumococci: pro-tecting patients through judicious use of antibiot-ics. Am Fam Physician 1997;55:1647–1654.
65. Yagupsky P et al. Acquisition, carriage, and trans-mission of pneumonococci with decreased antibi-otic susceptibility in young children attending a daycare facility in southern Israel. J Infect Dis 1998;177:1003–1012.
66. Arnold KE et al. Risk factors for carriage of drug-resistant Streptococcus pneumoniae among childrenin Memphis, Tennessee. J Pediatr 1996;128:757–764.
67. Leach AJ et al. A prospective study of the impact ofcommunity-based azithromycin treatment of tra-choma on carriage and resistance in Streptococcuspneumoniae. Clin Infect Dis 1997; 24:356–362.
68. Brook I, Gober AE. Prophylaxis with amoxicillin orsulfisoxazole for otitis media: effect on the recoveryof penicillin-resistant bacteria from children. ClinInfect Dis 1996;22:143–145.
69. Cohen R et al. Change in nasopharyngeal carriageof Streptococcus pneumoniaeresulting from antibiotictherapy for acute otitis media in children. PediatrInfect Dis J 1997;16:555–560.
70. Woods GL, Washington JA. Antibacterial suscepti-bility tests: dilution and disk diffusion methods. In:Murray PR, Baron EJ, Pfaller MA, Tenover FC,Yolken RH, eds. Manual of Clinical Microbiology,1995:1327–49.
71. World Health Organization. Manual for the nationalsurveillance for antimicrobial resistance ofS. pneumoniae and H. influenzae: epidemiologicaland microbiological methods. Geneva: World HealthOrganization, World Health Organization andCenters for Disease Control and Prevention, 1994.
72. Society AT. Guidelines for the initial managementof adults with community-acquired pneumonia:
diagnosis, assessment of severity, and initial antimicro-bial therapy. Am Rev Resp Dis 1993;148:1418–1426.
73. Bartlett JG et al. Community-acquired pneumoniain adults: guidelines for management. Clin Infect Dis1998;26:811–838.
74. Dagan R et al. Early eradication of pathogens frommiddle ear fluid during antibiotic treatment of acuteotitis media is associated with improved clinical out-come. Pediatr Infect Dis J 1998;17:776–782.
75. Pandey MR et al. Reduction in total under-fivemortality in western Nepal through community-based antimicrobial treatment of pneumonia. Lan-cet 1991;338:993–997.
76. Fauveau V et al. Impact on mortality of a commu-nity-based programme to control acute lower respi-ratory tract infections. Bull World Health Org1992;70:109–116.
77. Seppälä H et al. The effect of changes in the con-sumption of macrolide antibiotics on erythromycinresistance in group A streptococci in Finland. N EnglJ Med 1997;337:441–446.
78. Kristinsson KG, Hualmarsdottir MA, Gudnason T.Epidemiology of penicillin-resistant pneumococci inIceland—Hope for the future? Abstract C9, 35thInterscience Conference on Antimicrobial Agents andChemotherapy, San Francisco, 1995. American Soci-ety of Microbiology.
79. Gonzales R et al. Decreasing antibiotic use in am-bulatory practice: impact of a multidimensional in-tervention on the treatment of uncomplicated acutebronchitis in adults. JAMA 1999;281:1512–1519.
80. Petersen K et al. Education in Alaska villages to re-duce resistant S. pneumoniae, Seventh InternationalSymposium on Recent Advances in Otitis Media, FortLauderdale, FL, 1999.
81. Petersen K et al. Provider and community educationdecreases antimicrobial use and carriage of penicillin-resistant Streptococcus pneumoniae (PRSP) in ruralAlaska communities, Infectious Diseases Society ofAmerica, Philadelphia, PA, 1999.
82. Feikin DR et al. The effect of malaria treatment withsulfadoxine/pyrimethamine on trimethoprim/sulfamethoxazole resistance in Streptococcuspneumoniae. In press.
83. Guillemot D et al. Low dosage and long treatmentduration of β-lactam: Risk factors for carriage ofpenicillin-resistant Streptococcus pneumoniae. JAMA1998;279:365–370.
84. Centers for Disease Control and Prevention. Pre-vention of pneumococcal disease: Recommendationsof the Advisory Committee on Immunization Prac-tices. MMWR 1997;46:RR–8.
85. Eskola J, Anttila M. Pneumococcal conjugatevaccines. Pediatr Inf Dis J 1999;18:543–551.
86. Leach A et al. Pilot trial of a pentavalent/proteinconjugate vaccine in Gambian infants. PediatrInfect Dis J 1996;15:333–339.

29
WHO/CDS/CSR/DRS/2001.6 RESISTANT PNEUMOCOCCAL INFECTIONS
87. Black S et al. Efficacy of hepatavalent conjugatepneumococcal vaccine (Wyeth Lederle) in 37,000infants and children: results of the northern Cali-fornia Kaiser Permanente efficacy trial, abstr. LB-9,38th Interscience Conference on Antimicrobial Agentsand Chemotherapy, San Diego, CA, 1998. AmericanSociety of Microbiology.
88. Obaro SK et al. Carriage of pneumococci after pneu-mococcal vaccination. Lancet 1996;348:271–272.
89. Dagan R et al. Reduction of pneumococcal nasopha-ryngeal carriage in early infancy after immunizationwith tetravalent pneumococcal vaccines conjugatedto either tetanus toxoid or diphtheria toxoid. PediatrInf Dis J 1997;16:1060–1064.
90. Mohle-Boetani JC et al. Carriage of Haemophilusinfluenzae type b in children after widespread vacci-nation with conjugate Haemophilus influenzae typeb vaccines. Pediatr Infect Dis J 1993;12:589–593.
91. Dagan R et al. Effect of 9-valent pneumococcalvaccine conjugated to CRM197 (PNcCRM9) onnasopharyngeal (NP) carriage of vaccine type andnon-vaccine type S. pneumoniae (PNc) strains amongday care center attendees, abstr. G-52, 38thInterscience Conference on Antimicrobial Agents andChemotherapy, San Diego, CA, 1998. AmericanSociety of Microbiology.
92. Dagan R et al. Reduction of nasopharyngeal car-riage of pneumococci during the second year of lifeby a hepatavalent conjugate pneumococcal vaccine.J Infect Dis 1996;174:1271–1278.
93. Hussey GD, Klein M. A randomized, controlled trialof vitamin A in children with severe measles. NewEngl J Med 1990;323:160–164.
94. Quinlan KP, Hayani KC. Vitamin A and respira-tory syncytial virus infection: serum levels and sup-plementation trial. Arch Pediatr Adolesc Med1996;150:25–30.
95. Rahman MM et al. Acute respiratory infections pre-vent improvement of vitamin A status in younginfants supplemented with vitamin A. J Nutrition1996;126:628–633.
96. Dudley L et al. Vitamin A status, other risk factorsand acute respiratory infection morbidity in chil-dren. S Afr Med J 1997;87:65–70.
97. Dowell SF et al. Treatment of respiratory syncitialvirus infection with vitamin A: a randomized,placebo-controlled trial in Santiago, Chile. PediatrInfect Dis J 1996;15:782–786.
98. Bresee JS et al. Vitamin A therapy for children withrespiratory syncitial virus infection: a multicentertrial in the United States. Pediatr Infect Dis J 1996;15:777–782.
99. Uhari M, Kontiokari T, Niemela M. A novel useof xylitol sugar in preventing acute otitis media.Pediatr 1998;102:879–884.
100. Uhari M, Kontiokari T, Niemela M. Xylitol chew-ing gum in prevention of acute otitis media;double blind randomised trial. Br Med J 1996;313:1180–1184.
101. Torzillo PJ et al. Invasive pneumococcal disease incentral Australia. Med J Austral 1995;162:182–186.
102. Woolfson A et al. Nasopharyngeal carriage of com-munity-acquired, antibiotic-resistant Streptococcuspneumonaie in a Zambian paediatric population.Bull World Health Org 1997;75:453–462.
103. Hackenbeck R. β-lactam resistant Streptococcuspneumonaie: epidemiology and evolutionarymechanism. Chemother 1999;45:83–94.
104. Tomasz A. Antibiotic resistance in Streptococcuspneumonaie. Clin Infect Dis 1997;24:S85–S88.
105. Hackenbeck R, Tornette S, Adkinson NF. Interac-tion of non-lytic β-lactams with penicillin bind-ing proteins in Streptococcus pneumonaie. J GenMicrobiol 1987; 133:755–760.
106. Pikis A et al. A conservative amino acid mutationin the chromsome-encoded dihydrofolate reduct-ase confers trimethoprim resistance in Streptococ-cus pneumoniae. J Infect Dis 1998;178:700–706.
107. Adrian PV, Klugman KP. Mutations in the dihydro-folate reductase gene of trimethoprim-resistantisolates of Streptococcus pneumonaie. AntimicrobAgents Chemother 1998;41:2406–2413.
108. Gherardi G et al. Major related sets of antibiotic-resistant pneumococci in the United States asdetermined by pulsed-field gel electrophoresis andpbp1a-pbp2b-pbp2x-dhf restriction profiles. J In-fect Dis 2000;181:216–229.
109. Tait-Kamradt A et al. mefE is necessary for theerythromycin-resistant M phenotype in Streptococ-cus pneumonaie. Antimicrob Agents Chemother1997;41:2251–2255.
110. Courvalin P, Carlier C. Transposable multipleantibiotic resistance in Streptococcus pneumoniae.Mol Gen Genet 1986;205:291–297.
111. Ayoubi P, Kilie AO, Vijayakumar MN. n5253, thepneumococcal (cat tet) element, is a compositestructure of 2 conjugative transposons, Tn5251 andTn5252. J. Bacteriol 1991;173:1617–1622.
112. Widdowson CA, Klugman KP, Hanslo D. Identi-fication of the tetracycline resistance gene tetO, inStreptococcus pneumonaie. Antimicrob AgentsChemother 1996; 40:2891–2893.
113. Janoir C et al. High-level fluoroquinolone resist-ance in Streptococcus pneumonaie requires mutationsin parC and gyrA. Antimicrob Agents Chemother1996;40:2505–2510.
114. Novak R et al. Emergence of vancomycin toler-ance in Streptococcus pneumoniae. Nature 1999;399:590–593.

AppendixParticipants in the Drug Resistant S. pneumoniae Therapeutic Working Group (DRSPTWG)consensus meeting on pneumococcal otitis media
Dr David Bell, National Center for Infectious Dis-eases, Centers for Disease Control and Preven-tion
Dr Robert Breiman, National Vaccine ProgramOffice, Centers for Disease Control and Preven-tion
Dr Daniel J. Burch, Pharmaceutical Research,Manufacturers Association
Dr Jay C. Butler, Respiratory Diseases Branch,Centers for Disease Control and Prevention
Dr Matthew Cartter, Council of State and Territo-rial Epidemiologists
Dr Martin Cetron, Division of Quarantine, Centersfor Disease Control and Prevention
Dr Joan Chesney, American Academy of Pediatrics
Dr William Craig, Infectious Diseases Society ofAmerica
Dr Ron Dagan, Pediatric Infectious Disease Unit,Soroka Medical Center, Beer Sheva, Israel
Dr Scott F. Dowell, Respiratory Diseases Branch,Centers for Disease Control and Prevention
Dr Kathryn Edwards, Vanderbilt University
Dr Kenneth Gershman, Council of State and Ter-ritorial Epidemiologists
Dr Bruce Gellin, National Institutes of Health
Dr G. Scott Giebink, Otitis Media Research Center,University of Minnesota Medical Center
Dr Mary Gilchrist, Association of State and Terri-torial Public Health Laboratory Directors
Dr Sheryl Henderson, Emory University
Dr Michael Jacobs, Department of Pathology, CaseWestern Reserve University School of Medicine
Dr Dan Jernigan, Washington State Departmentof Health
Dr Ronald N. Jones, American Society for Micro-biology; Dr James H. Jorgensen, NCCLS
Dr Sheldon Kaplan, American Academy ofPediatrics
Dr Jerome O. Klein, Maxwell Finland Lab for In-fectious Diseases
Dr Keith Klugman, South African Institute forMedical Research
Dr Leah Raye Mabry, American Academy of Fam-ily Physicians
Dr Daniel R. Martin, Society for Academic Emer-gency Medicine
Dr William Martone, National Foundation for In-fectious Diseases
Dr Daniel M. Musher, American College of Physi-cians
Dr Tom O’Brien, World Health Organization Net-work
Dr Jack Paradise, Children’s Hospital, Pittsburgh,PA; Dr Michael A. Pfaller, College of AmericanPathologists
Dr Joseph F. Plouffe, Ohio State University Medi-cal Center
Dr Michael Poole, American Academy of Otolaryn-gology—Head and Neck Surgery
Dr Alexander Rakowsky, Food and Drug Admin-istration
Dr Frederick Ruben, American Thoracic Society/American Lung Association
Dr Benjamin Schwartz, Respiratory DiseasesBranch, Centers for Disease Control and Pre-vention
Dr Fred Tenover, Hospital Infections Program,Centers for Disease Control and Prevention
Dr George Zhanel, Society of Infectious DiseasePharmacists.
RESISTANT PNEUMOCOCCAL INFECTIONS WHO/CDS/CSR/DRS/2001.6
30