resident conference presented by rachel dunagin, m.d. november 15, 2005
TRANSCRIPT
Resident Conference
Presented by
Rachel Dunagin, M.D.
November 15, 2005

Case Presentation CC: Chronic Cough Mr. DW, a 74yo WM, presented to PHD
for direct admission by PCP: abnormal finding on imaging.
HPI: He complains of a cough Productive of white mucus Duration: past several months 3-4 wks PTA developed “pneumonia” –
treated with Levaquin by PCP; febrile to 102CXR was done at the time the antibiotic was
prescribed and read as normal
Case Presentation2d PTA returned to PCP office for
routine physical exam
Patient continued to complain of “nagging” coughEspecially pronounced after mealsProductive of white mucusDenied fever/chills
PCP ordered CT chest

Patient History PMHx:
Cough 3/05 thru present (6/05)
HTN Arthritis Superficial “clot” of LE 2001
PSHx: Left ear surgery Appendectomy
All: NKDA
Meds: Lotensin/HCTZ 20/12.5 Benzepril 20 Aspirin 81 Tums Flaxseed Oil Vitamin E Claritin D.
SocHx: Married with 4 kids Retired from DISD Denies tobacco or drugs Rare Etoh
FamHx: sister/brother/mom-HTN dad-CVA
ROS: Weight loss (5 pounds in
3wks) Decreased appetite Edema BLE Cough otherwise negative
Physical Exam Vital Signs: stable, afebrile HEENT: NC/AT, pupils equal and
reactive, EOMI, nares patent, OP clear Neck: supple, no JVD, no LAD, no
thyromegaly Heart: RRR, no m/g/r Lungs: CTAB, no w/c/r Abd: soft, NT/ND, NABS, no HSM Ext: 1+ edema LLE, trace RLE, 2+ pulse,
neg Homan’s sign

Labs (from PCP’s office) Na 142 K 4.1 Cl 103 Bicarb 26 BUN 22 Cr
1.6 Glc 138 Ca 9.4 TP 7.1 Alb 4.1 Glob 3 AlkP 78 AST 22 ALT 14 TB 0.7
WBC 6.4 Hgb 14.2 Hct 41.8 MCV 96 Plt 239
TSH 2.35 TG 120 Chol 181 HDL 43 LDL 114 EKG NSR 74 + PVC, no Q waves or ST
changes UA: negative Imaging report

CT Chest: done 1 day prior to admission
CT Chest: done 1 day prior to admission
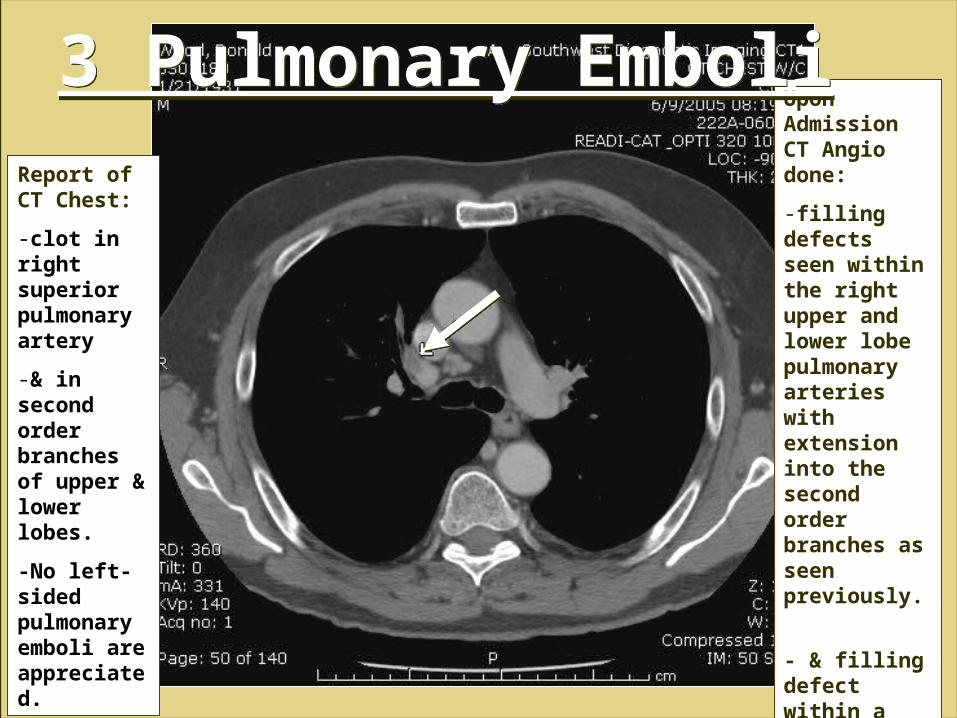
Report of CT Chest:
-clot in right superiorpulmonary artery
-& in second order branches of upper & lower lobes.
-No left-sided pulmonary emboli are appreciated.
Upon Admission CT Angio done:
-filling defects seen within the right upper and lower lobe pulmonary arteries with extension into the second order branches as seen previously.
- & filling defect within a segmental branch supplying the left lower lobe.
3 Pulmonary Emboli3 Pulmonary Emboli

30.6 HUs30.6 HUs

A low density mass measuring approximately 3 cm in diameter is noted. The CT attenuation is approximately 28 Hounsfield units. Adrenal adenoma would be a possibility but cannot be confirmed.
A low density mass measuring approximately 3 cm in diameter is noted. The CT attenuation is approximately 28 Hounsfield units. Adrenal adenoma would be a possibility but cannot be confirmed.
Adrenal Incidentaloma:IntroductionWhat is an adrenal incidentaloma
and why should we care?Definition: “Clinically inapparent
adrenal mass detected through imaging for non-adrenal disease”
First described approx 20 years ago
Is it common?Based on autopsy reports, adrenal
masses are AMONG THE MOST common tumors in humans
Found in ~3% of 50 year oldsFound in up to 10% of elderly
patientsAdvances in imaging (including CT,
MRI, US) may reveal even higher numbers

So…is it time to panic?

So…is it time to panic?
NONO…Most adrenal masses cause no serious health problems
Approx 1 of every 4000 is malignant

Trivia: Which adrenal is affected more frequently?
US studies show right adrenal more often affected
Likely because of better ultrasound visualization of right adrenal gland
Autopsy and CT studies show both adrenal equally affected
OutlineCauses, Prevalence, Natural History
Diagnostic Evaluation
Treatment, Follow-up
Bottom Line for the PCP
Conclusion of Case Presentation
PrevalenceAt autopsy,
<1% in patients <30 years old
~3% in 50 year olds
Up to 10% in elderly
Women > Men
? if this reflects sex differences in undergoing imaging procedures
CausesBenign Adrenocortical Masses
Pheochromocytoma
Adrenocortical carcinoma
Metastases
Other
Benign Adrenocortical Masses (Adenoma) Do not degenerate into malignant
lesions
Incidence increases with age
Its small size makes it difficult to differentiate from focal hyperplasia and accessory cortical nodules
Benign Adrenocortical Masses (Adenoma) Higher incidence in patients with
congenital adrenal hyperplasia (82% in homozygous, 45% in heterozygous)
Size variable: 1.4 – 9cm with mean of 3.3 cm
Majority are non-hypersecretory, but 5-47% secrete cortisol and 1.6-3.3% secrete mineralcorticoids. Extremely rarely secrete androgens/estrogens

Pheochromocytoma Catecholamine-producing tumor
Hypersecretion of norepinephrine, epinephrine and dopamine
Classic Triad: episodic headache, diaphoresis, and palpitations (tachycardia/anxiety)
Half have paroxysmal hypertension, most of the rest have what appears to be essential hypertension.
Pheochromocytoma May see encephalopathy, retinopathy
and proteinuria associated with malignant hypertension
When associated with MEN2 syndrome
1/2 have symptoms
1/3 have hypertension

Pheochromocytoma:Other Symptoms Pallor Orthostatic
hypotension Visual blurring Papilledema Weight loss Polyuria Polydipsia Increased erythrocyte
sedimentation rate (ESR)
Psychiatric disorders Dilated
cardiomyopathy Hyperglycemia Insulin resistance Impaired glucose
tolerance Type 2 diabetes
mellitus
Pheochromocytoma Account for 1.5 – 33% of incidentalomas
Mayo Clinic reviewed 40,078 autopsies between 1928 and 1977 Pheochromocytoma found in 0.13% Only diagnosed in 24% while alive
Histology: large pleiomorphic chromaffin cells
10-13% are malignant However no widely accepted pathological criteria to
differentiate benign from malignant exists. Thus, metastases are the only irrefutable proof of
malignancy
Pheochromocytoma90% located in adrenal glands10% in paraaortic sympathetic
chain, aortic bifurcation, and urinary bladder.
Bilateral in 10% of pts (esp in familial pheochromocytomas associated with MEN IIA and IIB)
Adrenocortical carcinoma Rare Incidence is 0.6 – 2 cases per million per
year Interestingly, Southern Brazil’s incidence
is 10x higher (reasons unknown). Represents 0.02 -0.2% of all cancer-
related deaths Bimodal age distribution: 1st and 5th
decades Functional or nonfunctional Functional tumors: Females > Males Nonfunctional tumors: Males > Females
Functional Tumors Androgen-secreting tumors resulting in
virilization - commonly in kids (84%), less in adults (<10%)
Estrogen-secreting tumors resulting in feminization are rare (<10%)
Hypercortisolism resulting in Cushing’s syndrome (45% adults vs 6% kids) or mixed Cushing-virilizing syndrome (25% adults)
Isolated primary mineralcortisolism – rare (<10%)

Adrenocortical Carcinoma Prognosis – poor; mean survival = 18
months Based on extent of disease, not impacted
by sex or functional status Common Symptoms of Non-functional
tumors: weight loss, weakness, anorexia, nausea, emesis, severe abdominal gas, and myalgia
Abdominal pain + palpable tumor = advanced disease
Fever = tumor necrosis, hemorrhage, or opportunistic infection

Metastases 75% of incidentalomas in cancer patients
are metastatic lesions. Virtually any primary can be origin Large proportion from lymphoma, lung
cancer (35%) and breast cancer (39%) Melanoma, leukemia, kidney and ovarian
cancer also common Review of 1000 consecutive autopsies of
patients with carcinoma, adrenal glands involved 27% of cases.
Other Etiologies Adrenal Myelolipoma
Ganglioneuromas
Adrenal Hyperplasia
Hematomas
Angiomyelolipomas
Malignant Epithelial Carcinoma
Epithelioid Angiosarcoma
Neurinoma
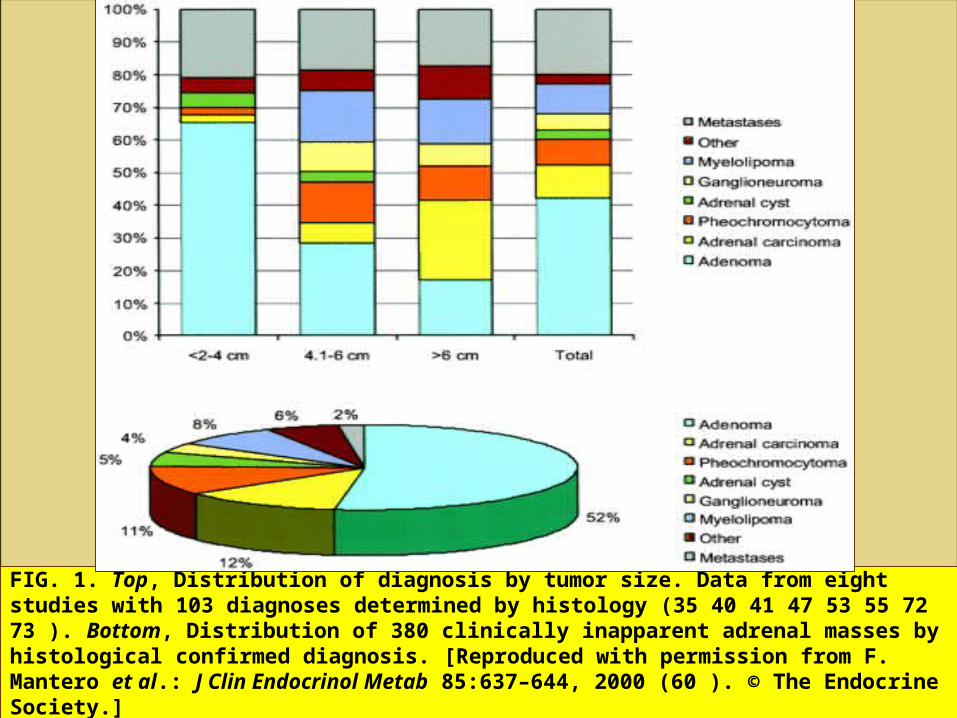
FIG. 1. Top, Distribution of diagnosis by tumor size. Data from eight studies with 103 diagnoses determined by histology (35 40 41 47 53 55 72 73 ). Bottom, Distribution of 380 clinically inapparent adrenal masses by histological confirmed diagnosis. [Reproduced with permission from F. Mantero et al.: J Clin Endocrinol Metab 85:637–644, 2000 (60 ). © The Endocrine Society.]
Natural History Large clinically inapparent adrenal
masses (> 6cm)25% = adrenal cortical carcinoma, thus poor
outcomes (less than 50% 5 year survival) treated surgically
Nonfunctioning adrenal masses 5-25% increase in size by at least 1 cm.Risk of malig = 1/1000Up to 20% develop hormone overproductionMasses > 3 cm more likely to develop
hyperfunctionTransformation rate of small (<3cm)
nonfunctioning masses is low.

Diagnostic Evaluation
2 Main Questions
1. Hormonally active or nonfunctioning?
2. Malignant or benign?
Detailed Endocrine EvaluationGoal: determine if patient has
pheochromocytoma, subtle glucocorticoid excess, primary aldosteronism, virilizing or feminizing tumors.
History of or episodic hypertension, tachycardia, profuse sweating
Hirstuism, striae, central obesity, gynecomastia
Specific Hormonal EvaluationSubclinical Hypercortisolism (5-47%
of adrenal incidentalomas):Overnight 1mg dexamethasone
suppression testNormal individual, 0800 serum cortisol
concentration is suppressed to <139.75nmol/L (<5μg/dL).
>10 μg/dL are suggestive of Cushing’s syndrome
Levels inbetween are equivocal
Specific Hormonal Evaluation Hyperaldosteronism (1.6-3.8% of adrenal
incidentalomas): If patient has HTN, check serum K and
plasma aldosterone concentration:plasma renin activity ratio
Historically, spontaneous hypokalemia (<3.5mmol/L) was hallmark of primary aldosteronism in hypertensive pts.
But NORMOkalemic primary aldosteronism appears at frequency 7-38% higher than previously thought (Bravo 1994, Stowasser 2001 & 2003)
Specific Hormonal Evaluation
Of 90 normokalemic patients with adrenal
incidentaloma and HTN, at least 5.5% were
found to have primary aldosteronism
(Bernini 2002)
Of 90 normokalemic patients with adrenal
incidentaloma and HTN, at least 5.5% were
found to have primary aldosteronism
(Bernini 2002)
If Aldosterone(μg/dL):Renin(μg/mL/hr) > 30 &
plasma aldosterone concentration is
>0.5nmol/L – highly suggestive of
autonomous aldosterone production

Specific Hormonal Evaluation
Note patients with kidney failure and those on Beta blockers and antisympathetic agents that may result in false positives by reducing plasma renin levels, or calcium channel blockers that may increase plasma renin and decrease aldosterone.
Note patients with kidney failure and those on Beta blockers and antisympathetic agents that may result in false positives by reducing plasma renin levels, or calcium channel blockers that may increase plasma renin and decrease aldosterone.
Additional Tests: 25mg Captopril Test, Salt-loading tests, or fludrocortisone suppression test confirm the diagnosis; Elevated level urinary excretion of methyloxygentaed cortisol metabolites (18-hydroxycortisol and 18-oxo-cortisol).
Specific Hormonal Evaluation Pheochromocytoma:
Elevated 24hr urinary excretion of free catecholamines (norepinephrine and epinephrine) or catecholamine metabolites [vanillylmandelic acid (VMA) and total metanephrines]
Specific Hormonal Evaluation
Plasma free metanephrines (normetanephrine and metanephrine) have good specificity and sensitivity and are recommended screening tests; however plasma catecholamines are not recommended due to poor sensitivity and specificity leading to false positives
Caution: Acetaminophen use interferes with assays of plasma free metanephrines, results in false-positive tests
Other possible tests: pharmacologic testing with glucagon or clonidine
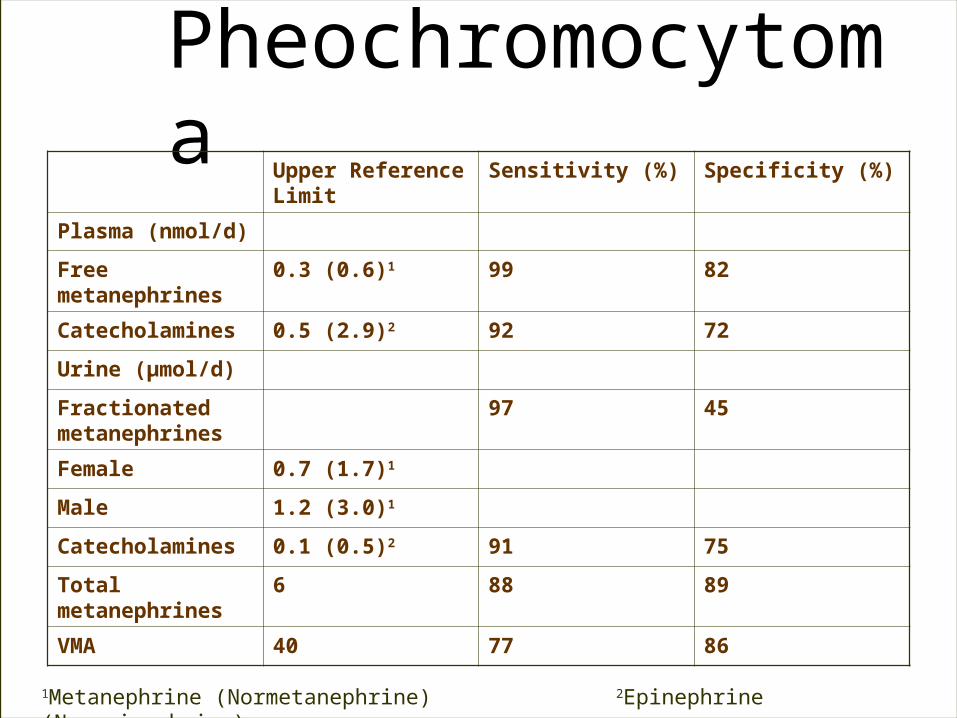
Pheochromocytoma
Upper Reference Limit
Sensitivity (%) Specificity (%)
Plasma (nmol/d)
Free metanephrines
0.3 (0.6)1 99 82
Catecholamines 0.5 (2.9)2 92 72
Urine (µmol/d)
Fractionated metanephrines
97 45
Female 0.7 (1.7)1
Male 1.2 (3.0)1
Catecholamines 0.1 (0.5)2 91 75
Total metanephrines
6 88 89
VMA 40 77 86
1Metanephrine (Normetanephrine) 2Epinephrine (Norepinephrine)

Wait.. What was this about Clonidine and Glucagon? Clondine Suppression Test
Clonidine, a central alpha-2 agonist, normally suppresses sympathetic nervous system activity, but does not decrease catecholamine secretion from pheochromocytoma
If plasma norepinephrine levels decrease >50% or to less than 2.96nmol/L after clonidine = normal response.
If remains consistently elevated before and after clonidine, indicates pheochromocytoma.
False-positives if on diuretics or tricyclic antidepressants
Serious complication: hypotension
Wait.. What was this about Clonidine and Glucagon? Glucagon Stimulation Test
Used when high plasma levels of normetanephrine or metanephrine and normal to slightly elevated plasma catecholamine levels
Give 1-2mg IV glucagon, after 2 minutes > 3x increase in norepinephrine indicates pheochromocytoma with high specificity, simultaneous increase in blood pressure may occur.
Test is not sensitive, thus negative result does not exclude the diagnosis
Serious complication: hypertensive crisis, so only done with experience operator
Specific Hormone EvaluationSex Hormone-secreting Masses:
Benign adenomas rarely secrete sex hormones, so routine evaluation of testosterone and estradiol is not recommended in patients with adrenal masses
Exception = Clinically suspected virilizing or feminizing tumor or if adrenocortical carcinoma is suspected based on radiology or history
Imaging
CT
MRI
US
CT Lesions <4cm usually benign Adrenal adenomas
small, homogeneous, well-defined lesions with clear margins, constant in size
contain large amount intracytoplasmic lipidallows a quantitative evaluation by
measurement of the attenuation value of the lesions (expressed as Hounsfield units)
usually have < 18 HUs on noncontrast CTs.100% Specificity with 68-89% sensitivity at
20-21 HUs.Conclusion of several studies, no further w/u
necessary if < 10 HUs (suggests lipid-rich adrenal adenoma)
CT The problem: Lipid-poor adenomas
represent 10-40% of adenomasThey have a higher attenuation value than
lipid-rich adenomasTherefore, not all adenomas can be
characterized using non-contrasted CTSolution: 3-minute delayed contrast CT using
thresholds between 64 and 70HUs to differentiate adenoma from nonadenoma
Washout Method – calculate % enhancement washout after 10-15min delay. If relative washout is >40-50% = highly suggestive of benign mass (sensitivity 96%, specificity 100%), is lower relative washout value suggests malignancy.

FIG. 4. Radiological panel of an adrenal cortical adenoma. Findings in a 66-yr-old woman with a history of breast cancer. Panels A and B demonstrate the use of CT for calculation of the relative enhancement washout. A, The contrast-enhanced CT shows a left-sided 1.5-cm adrenal mass (arrow) with a mean attenuation of 32.9 HU. B, On the 12-min delayed image, the attenuation of the left adrenal (arrow) is 12.9 HU. The relative enhancement washout is calculated using the following equation: percentage of relative enhancement washout = (1 – delayed enhanced HU value/initial enhanced HU value) x 100. With a relative washout of (1 – 12.9 /32.9) x 100 = 61%, the delayed enhanced CT is indicative of an adrenal adenoma (196 215 )
CT (cont) Lesions >6cm more likely to be
malignant – consider surgery
Pheochromocytomas Rounded or oval masses, density similar to
liver on noncontrast CT

CT (cont)Larger lesions show cystic component due
to central necrosis or hemorrhage
10% have calcification
Are hypervascular, so have intense enhancement with contrast.
CT Sensitivity = 93-100%
However, nearly 1/3 show nonspecific appearance that may overlap with adrenocortical carcinoma
MRI Malignant masses
Denser than benign masses because of higher fluid content
Therefore appear brighter on T2-weighted images Useful in staging adrenal carcinomas
Especially extent of infiltration into IVC Pheochromocytomas
Low T1 and bright T2 signal intensities Central necrosis
Metastases Hypointense compared to liver on T1-weighted
images and hyperintense on T2-weighted images Strong contrast enhancement with delayed washout
after paramagnetic contrast injection

CT vs MRITrials comparing noncontrast MRI
to combined non-contrast/contrast CT found superior, similar and inferior MRI test performance, depending on which technique was used (chemical-shift MRI, adrenal mass to reference organ ratio, etc)
McNicholas 1995, vanErkel 1994, Krestin 1991, Schwartz 2000
CT vs MRIStudies on qualitative comparison
of test accuracy concluded that combined noncontrast/contrast MRI was superior to both combined noncontrast/contrast CT and noncontrast MRI alone.
Krestin 1991
UltrasoundOperator dependent
Compounding factors: obesity,
overlying gas
Decreased sensitivity compared to
CT/MRI

Ultrasound1995 Suzuki reported series of 61
patients with adrenal massesUS correctly identified all adrenal
tumors > 3cmIdentified 65% of masses < 3cmCT/MRI identified 100%
Usefulness: follow-up benign lesions
On the horizon: EUS
Fine Needle Aspiration Performed under CT or US guidance
Based on review of 8 studies
investigating the test performance for
FNA to diagnose adrenal masses:Sensitivity 81-100%
Specificity 83-100% to diagnose malignancy
Higher sensitivity and accuracy if mass > 3
cm or needle > 19 gauge
Fine Needle Aspiration
No conclusions of risk of needle-track metastases from FNA biopsy of adrenal carcinoma can be drawn from present studies.
In total, 36 complications (4%) have been reported on 888 adrenal mass biopsies, including 26 complications that were potentially serious and 9 patients (1%) requiring in-hospital treatment.
Wide range of biopsy technique, incomplete/unclear reporting, and small study sizes make it difficult to evaluate the risk of biopsies.

Fine Needle AspirationMay be useful in the diagnostic
evaluation of patients with a history of malignancy (particularly lung, breast and kidney) and a suspicious adrenal mass on imaging (particularly if heterogeneous and >20HUs)
May be useful in the diagnostic evaluation of patients with a history of malignancy (particularly lung, breast and kidney) and a suspicious adrenal mass on imaging (particularly if heterogeneous and >20HUs).
Pheochromocytoma MUST be ruled out before FNA attempted due to potential of life-threatening hypertensive crisis

Surgery or NonSurgical Management?Functional Lesions
Glucocorticoids, Mineralcorticoids, Adrenal sex hormones, CatecholaminesConfirmed biochemicallyAdrenalectomy – Treatment of ChoiceOr medical therapy
Inhibitors of adrenal cortical steroid hormone biosynthesis (ie in patients with Cushing syndrome who are poor surgical candidates)
Aldosterone antagonists for aldosterone-secreting tumors.

Surgery or NonSurgical Management?Nonfunctional Lesion
Management is not straightforwardSilent Pheochromocytoma: high risk
for hypertensive crisis thus should undergo adrenalectomy
Next question – Benign vs Malignant
Benign vs Malignant: A Question of Size> 6cm: Excise the lesion< 4 cm: low risk, unlikely to have
malignant potential, not resectedLesions between 4 and 6 cm, either
close follow-up or adrenalectomyAdrenalectomy strongly considered if
rapid growth rate, decreased lipid content on imaging or other imaging findings suggestive of malignancy
Follow-up Most adrenal lesions remain stable, but 5-25%
enlarge and 3-4% decrease in size Imaging – if not excised, lesion should be re-
evaluated with CT in 6-12 months If does not increase in size, no data to support
further imaging. Hormone excess may develop in up to 20% of
patient during follow-up but is unlikely in patients smaller than 3cm.
Cortisol hypersecretion is the most common and is usually subclinical
Risk for tumor hyperfunction plateaus after 3-4 years
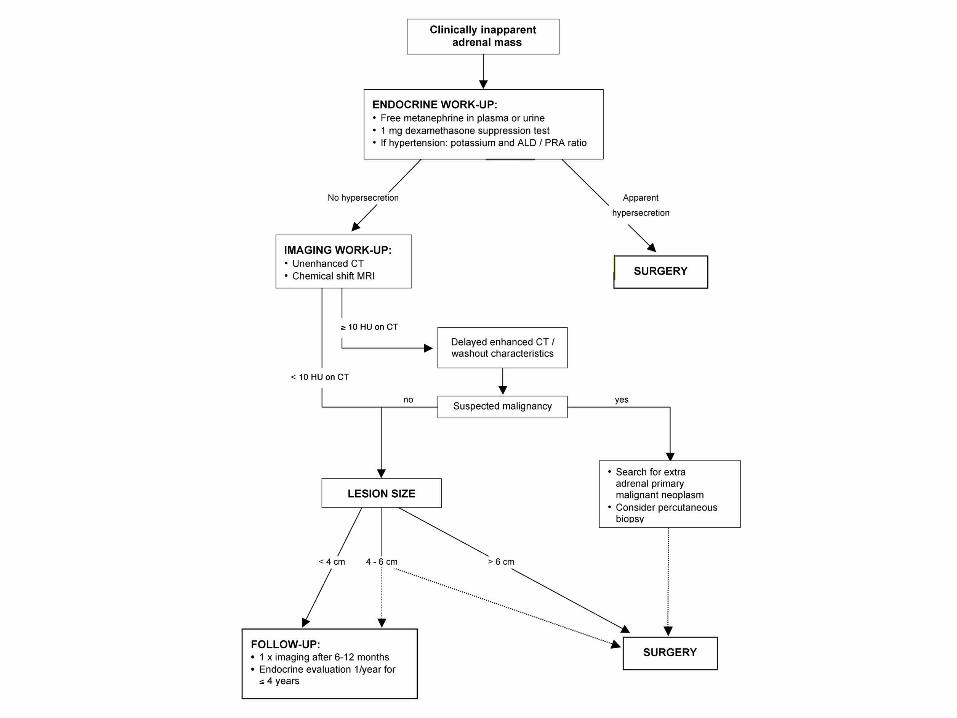
Bottom Line from NIH Conference All patients with an incidentaloma
should have a 1-mg dexamethasone suppression test and measurement of plasma free metanephrines.
Patients with hypertension should also undergo measurement of serum potassium and plasma aldosterone concentration-plasma renin activity ratio.
A homogeneous mass with a low attenuation value (<10 HUs) on computed tomography is probably a benign adenoma.
Bottom Line from NIH Conference Surgery should be considered in all
patients with functional adrenal cortical tumors that are clinically apparent
All patients with biochemical evidence of pheochromocytoma should undergo surgery
Data are insufficient to indicate the superiority of a surgical or nonsurgical approach to manage patients with subclinical hyperfunctioning adrenal cortical adenomas
Bottom Line from NIH Conference Recommendations for surgery based on
tumor size are derived from studies not standardized for inclusion criteria, length of follow-up, or methods of estimating the risk for carcinoma. Nevertheless, patients with tumors >6cm usually are treated surgically, while those with tumors <4cm are generally monitored. In patients with tumors between 4 and 6cm, criteria in addition to size should be considered in the decision to monitor or proceed to adrenalectomy

Bottom Line from NIH Conference
The literature on adrenal incidentaloma has proliferated in the last several years. Unfortunately, the lack of controlled studies makes formulating diagnostic and treatment strategies difficult. Because of the complexity of the problem, the management of patients with adrenal incidentalomas will be optimized by a multidisciplinary team approach involving physicians with expertise in endocrino-logy, radiology, surgery and pathology. The paucity of evidence-based data highlights the need for well-designed prospective studies.
Bottom Line from NIH Conference Open or laparoscopic adrenalectomy is
an acceptable procedure for resection of an adrenal mass. The procedure choice will depend on the likelihood of an invasive adrenal cortical carcinoma, technical issues, and the experience of the surgical team.
Open or laparoscopic adrenalectomy is an acceptable procedure for resection of an adrenal mass. The procedure choice will depend on the likelihood of an invasive adrenal cortical carcinoma, technical issues, and the experience of the surgical team.
In patients with tumors that remain stable on two imaging studies done over at least 6 months apart and do not exhibit hormonal hypersecretion over 4 years, further follow-up may not be warranted.Grumbach, M. M. et. al. Ann Intern Med 2003;138:424-429
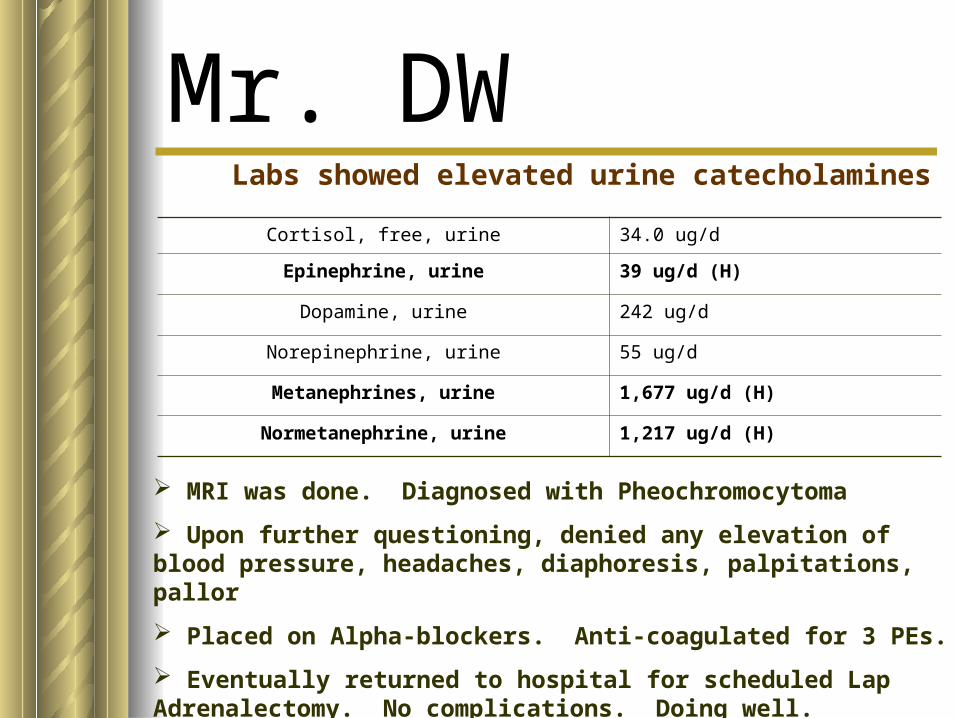
Mr. DWLabs showed elevated urine catecholamines
Cortisol, free, urine 34.0 ug/d
Epinephrine, urine 39 ug/d (H)
Dopamine, urine 242 ug/d
Norepinephrine, urine 55 ug/d
Metanephrines, urine 1,677 ug/d (H)
Normetanephrine, urine 1,217 ug/d (H)
MRI was done. Diagnosed with Pheochromocytoma
Upon further questioning, denied any elevation of blood pressure, headaches, diaphoresis, palpitations, pallor
Placed on Alpha-blockers. Anti-coagulated for 3 PEs.
Eventually returned to hospital for scheduled Lap Adrenalectomy. No complications. Doing well.
ReferencesBarzon, Luisa. Risk Factors and Long-Term Follow-Up of Adrenal
Incidentalomas. Journal of Clinical Endocrinology and Metabolism 84(2):520-526.
Bravo, M. Evolving concepts in the pathophysiology, diagnosis, and treatment of pheochormocytoma. Endocrine Review 15:356-368.
Grumbach, Melvin. NIH Conference: Management of Clinically Inapparent Adrenal Mass (“Incidentaloma”) Annals of Internal Medicine 138(5): 424-430.
Mansmann, Georg. The Clincally Inapparent Adrenal Mass: Update in Diagnosis and Management Endocrine Reviews 25(2): 309-340.
Pacak, K. Recent Advances in genetics, localization, and treatment of pheochromocytoma. Annals of Internal Medicine 134:315-329
Slawik, Marc. Adrenal Incidentaloma. www.endotext.com (ch.20)Sjoberg, RJ. The clonidine suppression test for pheochromocytoma. A
review of its utility and pitfalls. Archives of Internal Medicine. 152:1193-1197.
www.vectorpoint.ws/illuspages/panic.htmlYoung, William. The Adrenal Incidentaloma. www.Uptodate.com

End of Show
Other:Adrenal Myelolipoma Benign, composed of fat and
hematopoietic tissue Majority are functionally inactive Patients asymptomatic, but can become
symptomatic if large (pain/ retroperitoneal hemorrhaging)
Slow growing, <5cm No therapy unless:
rare, large type (can be >5.5kg)symptomaticor rapid growing, then surgery is curative.