report on rca in mitundu, lilongweapi.ning.com/.../rcareportdec2014mitunduv6.docx · web view3)...
TRANSCRIPT

2 DAY RAPID CARE ANALYSIS IN MITUNDU, LILONGWE, MALAWI
i

ContentsAcronyms and Abbreviations................................................................................................................ iii
Map of Mitundu, Lilongwe, Malawi......................................................................................................iii
Part 1 – Introduction and Background...........................................................................................1
1.1 Introduction.........................................................................................................................1
1.2 About the WE-Care Programme..........................................................................................1
a. Introduction to the programme.............................................................................................1
b. Components of the WE-Care programme.............................................................................1
c. Implications of the ICT component for Malawi......................................................................1
1.3 Study Context.......................................................................................................................2
1.4 About Oxfam-CADECOM Programme.................................................................................3
1.5 Rapid Care Analysis.............................................................................................................3
1.6 Approach and Methodology................................................................................................4
1.7 Limitations...........................................................................................................................5
Part 2 - Rapid Care Analysis (RCA).................................................................................................6
2.1 Care Work Recognition........................................................................................................6
2.1.1 Care Categories..................................................................................................................6
2.1.2 Tools used to conduct the RCA Sessions............................................................................7
2.2 Caring for People..................................................................................................................8
2.3 Who does what work?.........................................................................................................9
2.4 Implications of the unequal distribution of care work between genders.......................16
2.5 Gender and Age Distribution for Care Work....................................................................17
2.6 Age implications of who does more care work?...............................................................18
2.7 Negative and Positive Norms and Perceptions in Care Work.........................................18
2.8 Seasonal Changes verses Care work.................................................................................18
2.9 Most Problematic Care Work............................................................................................19
2.10 Developing Options and Solutions....................................................................................20
2.11 Analysing Specific Options and Solutions to Care Work..................................................21
2.12 Reducing and Redistributing Care Work..........................................................................23
2.13 Conclusion..........................................................................................................................23
ii

Acronyms and Abbreviations
CADECOM Catholic Development Commission in Malawi
CSO Civil Society Organisation
FGD Focus Group Discussion
HCS Household Care Survey
mNutrition Mobile Nutrition Programme
RCA Rapid Care Analysis
RCT Randomised Control Trial
TA Traditional Authority
WE-Care Women’s Economic Empowerment and Care
Map of Mitundu, Lilongwe, Malawi
iii

Part 1 – Introduction and Background1.1Introduction
This Report presents study results arising from a 2 – day exercise on Rapid Care Analysis (RCA) in Mitundu, Lilongwe, Malawi. Fundamentally, the RCA has established pre-project conditions in the Mitundu context, Lilongwe district, in order to generate strategies for project interventions that recognize, reduce and redistribute existing unpaid care work within the household, immediate community (civil society), market (private sector), state authority (central and local governments), and the mNutrition programme.
1.2About the WE-Care Programme
a. Introduction to the programmeOxfam GB with support from the Hewlett Foundation is implementing the WE-Care programme, which aims to build evidence for influencing change on care work. The programme will run from October 2014 to March 2016 (inclusive) and will develop new research methodologies to gather context-specific evidence about care activities, create tools that are accessible to local organisations, use mixed methods and harness new communications technologies. Oxfam and partners will leverage this evidence on care through existing development initiatives and policy advocacy in countries, and monitor outcomes of change strategies and advocacy.
b. Components of the WE-Care programme
c. Implications of the ICT component for MalawiOne of the three main components of the WE-Care programme is to use ICTs for household care data collection to support policy advocacy and influencing of the
1

mNutrition programme. The ICT enabled methodology will first be implemented as a prototype in Malawi and potentially replicated across other countries of the WE-Care programme. There are two different dimensions of the ICT component for Malawi:
i. Influencing mNutrition:Oxfam is the lead partner of the mNutrition consortium in Malawi and will be actively involved in the design of the mNutrition services. Results from the RCA and RCT will be used to influence the design of mNutrition services and content in Malawi. This evidence will be also used to influence the implementation of the mNutrition programme in the other 13 countries and to influence donors like GSMA and DFID.
ii. Awareness raising and national advocacyAn RCA will take place prior to the implementation of the Household Care Surveys (HCS) and the Randomised Control Trials (RCT). The main goal of the RCA is to inform the design of the HCS and to generate some initial evidence to do awareness raising both at the community and national levels.
The ICT enabled methodology will be used to gather household care data in a more scalable way than a conventional HCS. Information generated through the baseline will also be used for awareness raising and for influencing the design of the services and content of the mNutrition programme. The methodology will also include RCT for the selection of the control and treatment groups, which will be linked to mNutrition services and any other interventions identified through the RCA and the baseline, and will serve to evaluate the impact of these interventions on women’s time poverty.
1.3Study Context
2

Mitundu is situated in Lilongwe Rural West, 38.3km away from Lilongwe City with about 12,460 farm families cultivating an average of 1.26 hectares of land. Over the past decade, smallholder farmers in Mitundu especially women from Traditional Authority (TA) Masula have been experiencing low agricultural production and post harvest loses. There has also been poor participation in market chains as a result of lack of access to market information, low access to working capital, credit and agro-processing equipment for adding value. As a result, despite Mitundu being an agricultural area in Lilongwe, most smallholder farmers, especially women, have not benefited from Agriculture. Still more, Mitundu still remains an area with high Agriculture potential.
1.4About Oxfam-CADECOM Programme
The Catholic Development Commission in Malawi (CADECOM) is the relief and developmental arm of the Episcopal Conference of Malawi. The ECM is an assembly of eight Catholic Bishops in Malawi with a total of eight Dioceses namely Blantyre Archdiocese, Lilongwe Archdiocese, Chikwawa, Dedza, Mangochi, Mzuzu, Zomba and Karonga Dioceses. The Bishops have their Secretariat in Lilongwe, which was formed in 1961 and is headed by the Secretary General. CADECOM’s mission aims at creating awareness and empowering disadvantaged men, women and the youth at all levels to undertake development which is integral, gender and environment sensitive, it is sustainable and which promotes Justice, Human Dignity and Self Reliance with the active participation of the people themselves so that they take up the responsibility of their own destiny.
OXFAM in partnership with CADECOM is implementing a 1½ year project on ‘Women access to value chains and climate change adaptation’ which is being implemented in TA Masula in Mitundu, Lilongwe District. The main focus of the project is to improve poor women’s economic, social and environmental resilience through participation in value chains, increased status and adaptation to climate change. Hence the targeted population are the female headed households. The project looks at several areas; improved production levels and quality of groundnuts, improved access to formal markets, agro processing, enterprise development, mainstreaming climate change and advocacy. The project is targeting 3500 women from the TA with special focus on groundnuts.
Currently, there are 114 farmer clubs (65 active) which were formed in order to carry these activities but they also serve as Village Savings and Loans groups.
1.5Rapid Care Analysis
The RCA entailed a set of exercises for the rapid assessment of unpaid household work and the care of people in the immediate communities. The RCA exercise had four objectives, namely:
1. Provide women and men with a space to explore the issue of care together and to collaboratively develop practical solutions/ ‘care strategies’.
2. Recognise care work, identify the most problematic care activities and develop proposals to reduce and redistribute care work. It included the
3

following four steps: 1) exploring relationships of care in the community, 2) identifying unpaid and paid work activities performed by women and men, 3) identifying gendered patterns in care work, changes in care patterns, and ‘most problematic’ care activities and 4) discussing available services and infrastructure and options to reduce and redistribute care work.
3. Be quick to use and easy to integrate into existing exercises for programme design and/or monitoring. The RCA exercises further aimed at assisting in the assessment of how women’s involvement in care work may impact on their participation in development projects, and
4. Identifying how wider programmes such as this initiative can ensure adequate care for vulnerable people.
1.6Approach and Methodology
The RCA Study adopted a four step approach, namely, inception, field visits, analysis and reporting phases.
Phase One (Inception Phase): Oxfam in country team and global advisers agreed on a joint work-plan to RCA implementation, RCA participant profiles, RCA facilitator profiles and RCA logistic requirements. This phase culminated in a meeting with RCA facilitators to ensure a common understanding of RCA objectives, tools and methodology.
Phase Two (Field Phase): The RCA was carried out over 2 days from Tuesday 2nd of December 2014 to Wednesday 3rd of December 2014. The 2 RCA sessions were held with a total number of 32 participants, as originally planned (16 participants per group session). The sessions were conducted by facilitators who are fluent in Chichewa language and with a command of the Mitundu socio-economic context (i.e. three facilitators - one male and two female; and one documentation facilitator).
The RCA facilitators interfaced with the participants and moderated the sessions to discuss the socio-cultural economic and even political factors influencing care work in Mitundu. Global adviser provided guidance during RCA sessions alongside the facilitators. Each RCA session commenced with the introduction and clarification of what unpaid care work is guided by the facilitators, and the sessions lasted for 6-7 hours. At appropriate moments the 16 participants were divided into males and females groups and tasked to discuss in detail particular thematic issues and accordingly draw its action plan. This was followed by group presentation to give feedback on the issues raised during group work and to offer other participants an opportunity to have their input in that thematic area of which they were not members.
Phase Three (Analysis and RCA Reporting Phase): Oxfam in country team and global advisers are preparing this draft report which includes an analysis of the initial findings of the RCA.
Phase Four (Informing ICT enabled methodology and awareness raising): The initial findings of the RCA will be used during the design of the ICT enabled
4

methodology, RCT and to initiate awareness raising activities at the local and national levels, as well as to influence key stakeholders involved in the mNutrition programme.
1.7Limitations
In the case of the RCA, there could have been potentially biased answers as RCA participants might have known CADECOM staff involved in some of the RCA sessions.
Age of participants and literacy levels can pose a great challenge during the implementation of the RCA. The first session (with older participants) took much longer and not all the exercises were covered, as extra time was required to support participants during the exercises.
Based on learning from previous RCAs (e.g. Uganda and Ethiopia), the team managed to overcome the vast majority of limitations previously encountered during the implementation of the RCA (e.g. logistics, profiles of attendees, childcare and food provision among others).
5

Part 2 - Rapid Care Analysis (RCA)
2.1Care Work Recognition
2.1.1 Care Categories
The universal care categories that guided the RCA sessions in the Mitundu context is summarised in the Table below:
Table1: Care Categories Domestic work Direct care of persons
Meal preparation Fetching safe water Fetching wood fuel (energy) Clean space Clean clothes Buying food and clothes from the
market
Child care Care of dependent adults Care of community members
Prior to engaging each of the two RCA sessions, participants were guided by the facilitators in qualifying individual contributions from members on what is and what is not care work in their communities. The following common understanding on unpaid care work and what is not care work in Mitundu context is summarised in the Tables 2 and 3 below:
Table 2: Common Mitundu understanding of care workUnderstanding of unpaid care work Understanding of what is not care work
Beneficial for the family or community Intention to be beneficial for family or
community Physical and/or moral involvement Love and labour Unpaid Usually done by women and “assumed to
be women’s responsibility” Usually not recognised/ visible Usually not valued much Usually performed as part of routine work Fits categories of care work: Meal
Preparation, Water, Energy, Buying Food and Clothes in the Market, Clean Space, Clean Clothes, Child Care, Care of Dependent Adults, Care of Community Members
Given the strong Christian background of all attendees, praying for ill members of the family was considered care work, as “praying is the best thing you can do if you really care for someone”
Maintenance (Repairing a bicycle; Building a house)
Looking after animals Subsistence farming Planting food to eat/ Starting a kitchen
garden Commercial farming Funding care work (Giving money to buy
clothes; Giving money to buy food; Paying school fees or bills)
Attending community meetings Having sexual relations with partner Socializing for leisure
6

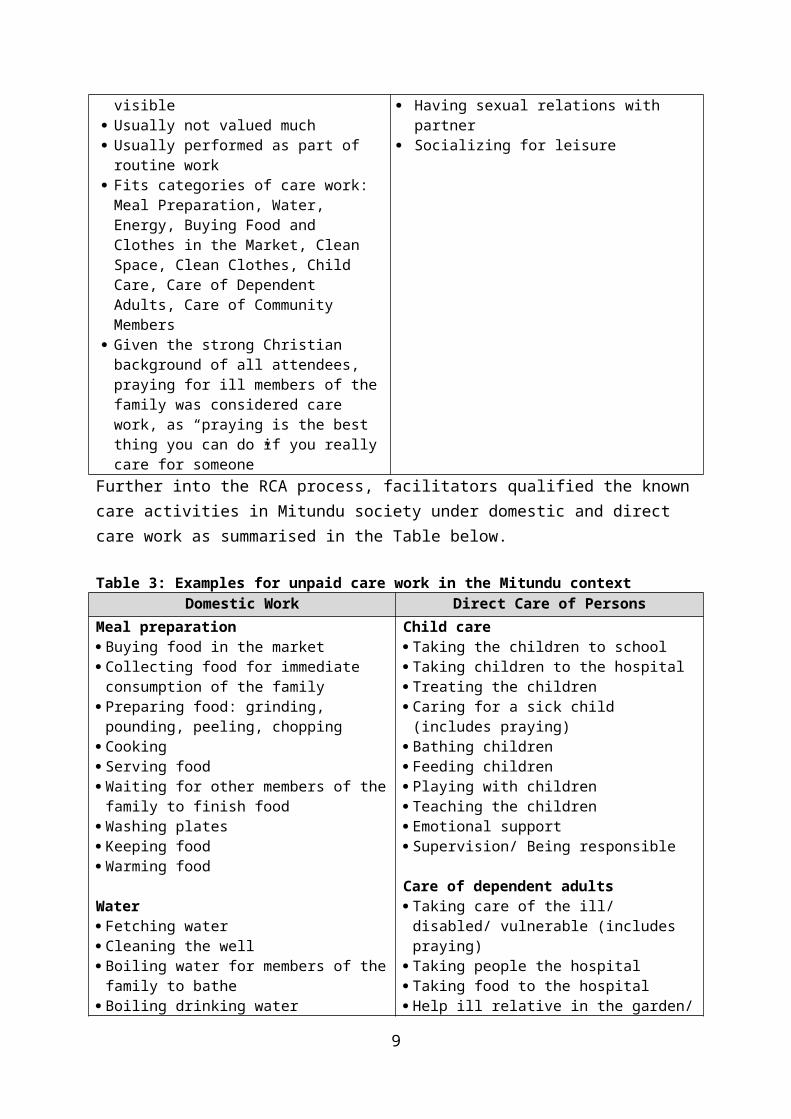
Further into the RCA process, facilitators qualified the known care activities in Mitundu society under domestic and direct care work as summarised in the Table below.
Table 3: Examples for unpaid care work in the Mitundu contextDomestic Work Direct Care of Persons
Meal preparation Buying food in the market Collecting food for immediate consumption
of the family Preparing food: grinding, pounding, peeling,
chopping Cooking Serving food Waiting for other members of the family to
finish food Washing plates Keeping food Warming food
Water Fetching water Cleaning the well Boiling water for members of the family to
bathe Boiling drinking water
Energy Collecting firewood Cutting the trees Splitting firewood Lightening the fire Maintaining the fire
Cleaning Cleaning the house Sweeping the house Sweeping the outside of the house Tidying/ organizing the house
Clothes Washing clothes Mending clothes Ironing clothes Buying clothes
Child care Taking the children to school Taking children to the hospital Treating the children Caring for a sick child (includes praying) Bathing children Feeding children Playing with children Teaching the children Emotional support Supervision/ Being responsible
Care of dependent adults Taking care of the ill/ disabled/ vulnerable
(includes praying) Taking people the hospital Taking food to the hospital Help ill relative in the garden/ home Providing emotional support/ listening to
someone’s problems
Care of community members Carry things for elderly Cleaning the communal well Looking after/ supervising someone else’s
children Unpaid help to cook for/ prepare funerals/
weddings Settling disputes/ counselling Collective action that benefits the community
directly
2.1.2 Tools used to conduct the RCA SessionsThe tools used in the RCA included:
a) Care Diamond to explain the role different actors play on care work b) Relationship Diagram that showed the rationale of why someone is important in
another’s life
7
c) Time Allocation Table which was used to detail the time spent by each participant within 24 hours of a “typical” (non-festive) day
d) Weekly Main Activity and Simultaneous Activity Table which summarises total hours spent on each activity by all participants of the RCA and the average time dedicated by women and men for each activity
e) Problematic Care Rating Matrix which identified the “most difficult to do” care work and identifies how this affects different age groups
f) Seasonal Calendar Table which enabled participants to identify which months are more problematic depending on the care activity
g) Care Reduction Options Table which identified potential ways (including strategies and stakeholders) to tackle the top 4 most problematic care activities.
2.2Caring for People
Experience with RCA sessions showed that both the ordinary community residents and leaders recognized that women did more unpaid care work compared to their men. They attributed this to the roles they are ascribed by society. Community members linked women unpaid care work such as washing clothes, cooking, fetching firewood and collecting water with their role as mothers which involves caring for children and having to put up with most of the family welfare requirements that necessitates caring. This perception was particularly acute among younger men and women and less strong among elder populations. Pregnancy and young babies, particularly new-borns, suppose an additional time and mobility constraint for women, which prevent them from engaging more in income generating activities.
Woman “Looking after children is a burden because we postpone doing other things like going to the field in order to prepare them for school but sometimes, during farming season, women neglect the children as they want to concentrate on farming activities”
Additionally, younger men prefer if women do not get involved in income generating activities. These views were reiterated by participants as below:
Man “The way it is in the society, we (men) are the household heads therefore the breadwinners so it doesn’t make sense for women to be busy doing Income Generating Activities when a man is around. I wouldn’t feel comfortable for my wife to be doing Income Generating Activities, I am the financial controller”
Woman “Men don’t like it when women are involved in income generating activities; it gives a picture that the man has failed to provide for his family. That is the reason why most women don’t do any Income Generating Activities like businesses”
Physical limitations of elder men limit their engagement in farm activities and free up part of their time which is sometimes used to relief women’s burden of care work. However, in certain care activities elder men just engage when there is no one else to perform them.
Woman “Elderly people only cook when they don’t have someone to cook for them or when no one is around”
8

At the beginning of both RCA sessions, men considered care work as not being a big burden of work. The view held by men is traditionally focused on commercial and income generating activities which they commonly see as the best way forward to secure the welfare of their households. This perception is representative of the value placed by communities on unpaid care work, particularly from the angle of not having an economic contribution to the welfare of the household.
After going through the individual one-day recall exercise, both men and women also recognised that care work was labour intensive and mostly left to women. The one-day recall exercise brought out vivid discussions between men and women that led to an increased recognition of the unequal distribution of care work and its negative impact on women’s time poverty. With women observing that they in addition to care work they do unpaid work like gardening for food security in the home. These views were reiterated by participants as below:
Man “Traditionally, it is women who are supposed to be providing care work so it is not a surprise that they have more hours on care work than men. It is just how it is supposed to be”
Man “We have learnt a lot from this exercise, we took for granted the work that women do, but now we will begin to share responsibilities at home so that we free up some time for the women”
Community Leader “At first when we were just starting the exercise, I thought to myself, why we are discussing care work? This is sure a waste of time but as we went on with the exercise, seeing the results that were coming out, it became interesting. I didn’t know that men take so much time sleeping and other non work in this community we will definitely change after seeing this and put our time to better use, helping the women”
2.3Who does what work?
During the RCA facilitators discussed with attendees 6 types of work categories:
• Work to produce products for sale . This includes farming crops for market (cash crops) and other business activities (including home-based businesses)
• Paid labour and paid services . This includes waged work on farms, and other waged work
• Unpaid care work . This includes the direct care of persons, housework that facilitates the care of persons and the collection of water or fuelwood
• Unpaid work producing products for home consumption or for the family . This includes gardening, rearing animals, making furniture, and subsistence agriculture
• Unpaid community work. This includes attendance at committees, and community work related to health, education, natural resources, and religious or cultural events
• Non-work . This includes personal care (bathing, resting), sleep, entertainment and recreation
9
Participants were then asked to recall the hours spent on each of the 6 work categories on a normal (non-festive) day. They were asked to do this exercise considering both main and simultaneous activities.
Considering all questionnaires filled by the attendants of both RCA, Oxfam in country team has produced a questionnaire for women, pregnant women and men to show the average activities performed by each of these groups:
Individual 1 day recall of daily activities - Average woman in Mitundu:
10
Supporting family members

Individual 1 day recall of daily activities - Average pregnant woman in Mitundu:
11

Individual 1 day recall of daily activities - Average man in Mitundu:
12

Each participant then calculated their weekly average for each activity, taking into account that on Sunday time allocation tend to differ from a normal day. The totals were then captured on different tables for men and women:
Session 1 (02.12.2014) – Older Group, Women:
Session 1 (02.12.2014) – Older Group, Men:
13

Session 2 (03.12.2014) – Older Group, Women:
Session 2 (03.12.2014) – Older Group, Men:
The total weekly hours obtained were then divided by the number of attendees (women and men separated) to obtain the weekly average for men and women. In both RCA sessions, women reported more unpaid care work than men as both main and simultaneous activity.
These averages were then captured on a table reflecting work hours for both men and women. In this way attendees could see the unequal distribution of work between genders without seeing themselves exposed in front of the community. The results are captured in the tables below:
14

Session 1 (02.12.2014) – Older Group:
Session 2 (03.12.2014) – Younger Group:
Average of both sessions
15

These tables illustrate how the unequal distribution of care work is more acute among younger populations (Women: 49 h/w main & 35 h/w simultaneous vs Men: 6 h/w main & 2 h/w simultaneous) than older ones (Women: 38 h/w main & 35 h/w simultaneous vs Men: 15 h/w main & 8 h/w simultaneous). On average, these findings also highlight the critical role played by women in unpaid work producing products for home consumption (Women: 23 h/w main & 2 h/w simultaneous vs Men: 16.5 h/w main & 3.5 h/w simultaneous). The combination of these activities results in a more unequal distribution of non-work activities between genders (Women: 63 h/w main & 6 h/w simultaneous vs Men: 87.5 h/w main & 27.5 h/w simultaneous).
The unequal distribution of care work between genders constraint women in Mitundu from engaging in political participation and income generating activities, limiting their decision making power and control over the assets at the household level. Moreover, it prevents women from fully enjoy basic needs/rights like sleeping or personal care, and has a direct negative impact on women’s wellbeing.
2.4Implications of the unequal distribution of care work between genders
Public engagement including political participation: Care work as can be observed across accessing safe water, basic health and education, to food security for the homestead is intense and demanding, yet someone has to perform these activities. The noticeable absence of women in public dialogues like their male counterparts is to a large measure linked to their necessity to care for the household and at times communities, at the expense of their active public participation.
Social empowerment (in addition to social norms): The unfavourable conditions in which women find themselves are mainly perpetuated by cultural restrictions, marginalisation in decision making, and ignorance due to limited exposure and education. Women are most times confined to the household due to the household members’ own expectations that the woman is to perform all manner of care work.
Personal empowerment and confidence: The genesis of care work being regarded as “petty” or not worthwhile of men’ time draws from the division of labour in which traditionally women are charged with more non-monetised activities such as collecting firewood, child-upbringing, fetching water, and tilling the land. With the responsibility of food availability in the home, women are left almost with no time to pursue anything that they may choose for their own personal development. Meanwhile, men who are regarded heads of households own all the factors of production and as such make nearly all the important decisions in the household, and have a lot of leisure time to socialise and pursue personal interests and development.
Women’ participation in productive work: The majority of women work from dawn to dusk and such work is not recognised as work at all. They remain the primary care givers in the household; often they are the major contributors to the markets as well. Even when they may be working longer hours than men, their work is regarded as falling into the realm of caring, nurturing, and household duties, not into the realm of “economic” activity as such. This poor or negative attitude towards women in engaging in income generating activities and earning their own income appear to cement the
16

view that non-income generating work is a preserve of women, even if the work is technically productive (i.e. kitchen gardens). This attitude over time has become to be the norm. As a result women do not control proceeds of whatever is produced or what is sold in the market
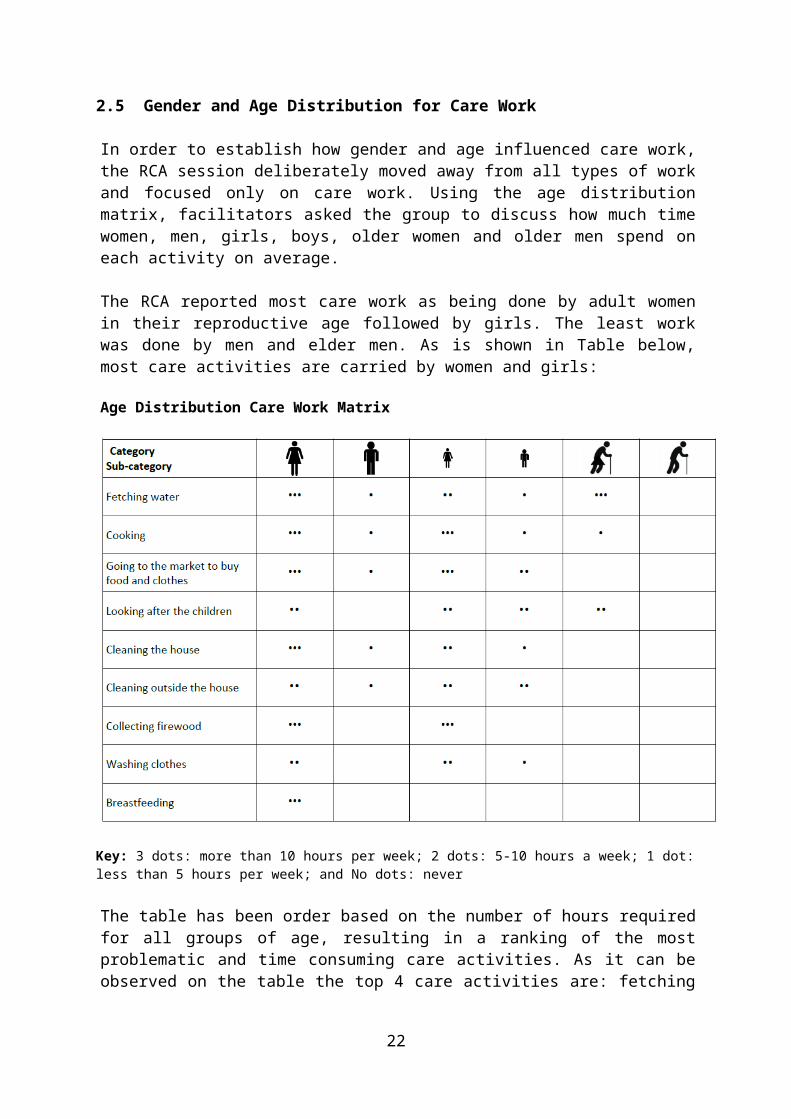
2.5Gender and Age Distribution for Care Work
In order to establish how gender and age influenced care work, the RCA session deliberately moved away from all types of work and focused only on care work. Using the age distribution matrix, facilitators asked the group to discuss how much time women, men, girls, boys, older women and older men spend on each activity on average.
The RCA reported most care work as being done by adult women in their reproductive age followed by girls. The least work was done by men and elder men. As is shown in Table below, most care activities are carried by women and girls:
Age Distribution Care Work Matrix
Key: 3 dots: more than 10 hours per week; 2 dots: 5-10 hours a week; 1 dot: less than 5 hours per week; and No dots: never
The table has been order based on the number of hours required for all groups of age, resulting in a ranking of the most problematic and time consuming care activities. As it can be observed on the table the top 4 care activities are: fetching water, cooking, buying food and clothes from the market and looking after the children.
17

2.6Age implications of who does more care work?
RCA session participants pointed out that older people tend to do less care work because of their advanced age. Women between 30-40 years however care the most because not only do they have strength and ability but do not want to be seen failing in their core role of looking after their own family. This household members’ expectation is what drives the adult woman to work much more than anybody else.
Young women with little children also care more compared to elderly women. This is because their children are too young to render a hand in the care work, small children demand more attention on care work related to their feeding, washing, protection and treatment and young women are likely to have more school-going children.
As women grow older, they tend to attain much respect from their daughter in laws, young girls in the family, their men and sons. Elderly women are also likely to be cared for by their own married daughters especially when considered weaker.
2.7Negative and Positive Norms and Perceptions in Care Work
The moderators facilitated discussions in which RCA participants were probed on social norms that are known to either hinder or enhance care work at household and community levels. From the RCA sessions it became clear that the practice of men leaving care work to their women is much to do with attitude, tradition, and society perception towards care work.
Man “There are some households that have embraced the sharing of household care work between men and women however, society brands men who cook as being under the woman’s spell (love portion) or not being man enough”
Woman “Care work can be a really big burden especially when it comes to cooking. Even when we are sick, we still have to do the cooking instead of the men helping us”
The culturally entrenched position is that, it is not socially acceptable for men to perform certain care activities as defined in this study. Some men indicated their concern about what their neighbours or their women would think of them if they took on care work such as cooking or washing clothes.
2.8Seasonal Changes verses Care work
The RCA used a seasonal calendar to map how the top 4 care activities are affected depending on the moment of the year. The rainy season was identified as the key factor that increases or decreases the amount of time needed to perform each of the care activities.
• Fetching water becomes particularly difficult between August and November, which are the months preceding the rainy season
• Cooking becomes particularly challenging during the rainy season (Dec-Feb), as it is more difficult to find dry wood to start the cooking fire
18

• Buying food and clothes from the market requires extra time during the rainy season, as the roads flood or become muddy
• Taking care of the children also becomes more difficult during the rainy season. Kids play in the mud, increasing the time needed for washing clothes and the likelihood of having sick children at home
Table below shows a 12-month calendar and maps where each of the top 4 care work activities are more intense.
Seasonal Changes in Care Work
Woman “Looking after children becomes more demanding during the rainy season because kids like playing in the mud hence you have to give more attention to them to make sure that they don’t hurt themselves and also the washing becomes more intensive. Sicknesses like diarrhoea become more problematic during this season”
2.9Most Problematic Care Work
To determine which care activities are most problematic to guide developing solutions to address those issues, the RCA sessions prompted discussions among men and women to list the top 4 most problematic care activities in the matrix. For each problematic care activity, the group assigned dots to assess a) how much it is a time burden, b) how much it affects mobility, c)how much it affects health, and d) how risky it is to perform the task.
Fetching water was identified as the most problematic activity, as it restricts mobility of women and is time consuming. It can also be risky as in occasions people encounter wild animals while carrying the water.
19

Cooking is also a problematic activity as it is extremely time consuming and has an adverse impact on health due to the use of firewood for cooking. Surprisingly, attendees agreed that it doesn’t have a negative impact on mobility, as women have flexibility on when to cook depending on other activities.
Looking after the children is the most time consuming activity and carrying them was identified as having a negative impact on health.
Buying food and clothes from the market was identified as relatively less problematic than the other activities but constraining mobility of women. The table below summarizes the discussion:
Comparative analysis of the ‘burden’ of care on women
Key: ... Most challenging; .. Manageable; . Simple
2.10 Developing Options and Solutions
In order to come up with solutions for most problematic care activities that are feasible and impactful, the RCA facilitators reviewed with the participants the care diamond and “4Rs”. This was later followed by brainstorming by the participants on options to recognize, reduce and redistribute care work in their community. The group agreed on 4 different strategies, each of them addressing a different problematic care activity.
During the first session (2nd December 2014), the group agreed on the following solutions for each of the top 4 most problematic activities:
Care Activity Potential SolutionFetching water Drill Boreholes the CommunitiesCooking Plant Trees in the CommunitiesBuying food from market Homestead gardens + LivestockChild Care Community Based Child Care Centre
20

Participants of the second session (3rd December 2014) proposed a different set of solutions for each of the top 4 most problematic activities:
Care Activity Potential SolutionFetching water Borehole/Concrete wellCooking Getting men to share tasks with
womenBuying food from market Kitchen GardensChild Care Community Based Child Care Centre
2.11 Analysing Specific Options and Solutions to Care Work
In order to rank the different potential solutions and identify key stakeholders for the most problematic care activities, the group discussed the following issues: a) Level of Investment Required, b) Requirement of other people’s goodwill, c) Can be done without external support?, d) Level of social acceptability, e) Amount of time freed for women, f) Free or paid service?, g) actors who can help.
The result for each of the sessions is shown on the tables below:
Session 1 (02.12.2014)
Drill Boreholes in the Communities
Plant Trees in the Communities
Homestead gardens + Livestock
Community Based Child Care Centre
Level of Investment Required
Low High High High
Relies on other people’s goodwill?
Yes Yes Yes Yes
Can be done without external support?
No No Yes No
Level of social acceptability
High High High High
Amount of time freed for women
High High High High
Free or paid service?
Free Free Free Paid- small contributions
Actors who can help
Government/NGOs like OXFAM
NGO- Total Land Care
Self/NGOs Government/ NGOs
Drilling Boreholes or Concrete wells will require low investment because some of the activities needed materials like bricks would be offered by community members
21

Planting trees would help free up the time that women take to fetch firewood as a result time taken when cooking would also be reduced. This could never be done without external support as the community would need support with seedlings and watering canes. Additional extension services would also be needed
Gardens and livestock will help reduce the time women spend going to the market to buy relish.
Community Based Child Care Centres cannot be free as the communities will have to contribute something to feeding the children at the centres
“We need nursery schools even if we have to pay something because this will help reduce the time we spend taking care of the children”
Session 2 (03.12.2014)
On the second RCA, participants agreed to replace ‘planting trees’ as a solution, with ‘getting men to share some of the tasks’. The participants felt that getting men to share some of the tasks would be more practical in providing immediate help as compared to planting trees
Borehole/Concrete well
Getting men to share tasks with women
Gardens Community Based Child Care Centre
Level of Investment Required
High Medium Low High
Relies on other people’s goodwill?
Yes NO Yes Yes
Can be done without external support?
No/Yes Yes Yes No
Level of social acceptability
High Low High High
Amount of time freed for women
High Low Medium High
Freed or paid service?
Free Free Free Free
Those who can help
Self/ NGOs/ Govt Self Self/NGOs/Govt Self/ NGOs/ Govt
The level of investment required to get men to share tasks would be medium, as it would mainly require time to educate them on the acceptance of sharing responsibilities. The amount of time freed up would be medium as women expected that the contribution of men would not be much
“The level of acceptability could be low, as traditionally women are the ones who are expected to do care work”
22
Having good kitchen gardens at home can free up time dedicated by women to go to the market to buy Relish as they would just be sourcing from the garden
NGOs could help providing seeds for the gardens while the government could help in providing extension services
Community Based Child Care Centres would need high investment, as it would need bricks, sand and iron sheets to build the structures
2.12 Reducing and Redistributing Care Work
Both groups agreed on the importance of discussing the reduction and redistribution of care work at the household level and highlighted the need for deeper dialogues with men and traditional leaders, who play a major role around cultural values and norms. The challenges of reducing and ultimately re-distributing care work appear to be rooted in defined societal perception and acceptance of men and women doing designated tasks in a home. Moreover, power dynamics appear to be in play as men fear to be perceived weak if they are found performing some care activities.
2.13 Conclusion
Both RCA sessions showed the unequal distribution of care work between men and women, being this particularly acute among younger members of the society. Attendees explained this based on traditional norms and believes. Participants linked women’s unpaid care work such as washing clothes, cooking, fetching firewood and collecting water with their traditional roles as mothers which involves caring for children and having to put up with most of the family welfare requirements that necessitates caring.
The RCA and group discussions helped men Recognise the unequal distribution of care work between men and women and the need to Reduce or even Redistribute this burden of work. Care rooted time poverty has prevented women from fully participating in decision-making and leadership processes, income generating activities, and negatively affects the wellbeing of women in the Mitundu community.
This RCA has demonstrated that dialogues of this nature are possible. Both sessions cultivated an appreciation of the realities in terms of care work load and implications of when the household mature partners engage in taking on some of the care work that has earlier on been a “given” for women.
23