report on persuasive design principles, user models and profiles
TRANSCRIPT
Page 1
Multimedia Authoring and Management using your Eyes and Mind
H2020-ICT-2014 - 644780
D5.1 - Report on persuasive design principles, user models and profiles
Dissemination level: Public (PU)
Contractual date of delivery: Month 12, 01/05/2016
Actual date of delivery: Month 12, 30/04/2016
Workpackage: WP5 – User modelling and interface design
Task: T5.1 – Persuasive design principle specification
T5.2 – User modelling and profile generation
Type: Report
Approval Status: Final
Version: 0.4
Number of pages: 77
Filename: D5.1_PersuasiveDesignPrinciples_final.docx
Abstract: The general objective of WP5 is to provide user modelling, and the basic principles and paradigms for interface design. First of all, crucial to MAMEM is modelling of users (based on relevant characteristics as (dis-)abilities, interaction behaviour, emotions, intentions, social abilities and social network, extend to which training is needed, and sensitivity to persuasive strategies. These models will be used as input for several WP’s and tasks. Second, equally important as to user models, is a specification of the persuasive design principles to influence those users (e.g., increase adherence to therapy/exercises, increase trust in the interface). Finally, all the above will be used as the basis to design the necessary interfaces and develop a set of prototype applications that will be
used during the pilot trials.
The information in this document reflects only the author’s views and the European Community is not liable for any use that may be made of the information contained therein. The information in this document is provided as is and no guarantee or warranty is given that the information is fit for any particular purpose. The user thereof uses the information at its sole risk and liability.
co-funded by the European Union
Page 2
Copyright
© Copyright 2015 MAMEM Consortium consisting of:
1. ETHNIKO KENTRO EREVNAS KAI TECHNOLOGIKIS ANAPTYXIS (CERTH)
2. UNIVERSITAT KOBLENZ-LANDAU (UNI KO-LD)
3. EB NEURO SPA (EBNeuro)
4. SENSOMOTORIC INSTRUMENTS GESELLSCHAFT FUR INNOVATIVE SENSORIK MBH (SMI)
5. TECHNISCHE UNIVERSITEIT EINDHOVEN (TU/e),
6. MDA ELLAS SOMATEIO GIA TI FRONTIDATON ATOMON ME NEVROMYIKES PATHISEIS (MDA HELLAS)
7. ARISTOTELIO PANEPISTIMIO THESSALONIKIS (AUTH)
8. MEDICAL RESEARCH INFRASTRUCTURE DEVELOPMENT AND HEALTH SERVICES FUND BY THE SHEBA MEDICAL CENTER (SHEBA)
This document may not be copied, reproduced, or modified in whole or in part for any purpose without written permission from the MAMEM Consortium. In addition to such written permission to copy, reproduce, or modify this document in whole or part, an acknowledgement of the authors of the document and all applicable portions of the copyright notice must be clearly referenced.
All rights reserved.
D5.1 – V0.4
Page 3
History
Version Date Reason Revised by
Vo.1 1/3/2016 SCI user profile and personas Gabi.Zeilig, Amihai Gottlieb
Vo.1 5/3/2016 PD user profile and personas Bostantjopoulou Sevasti
Zoe Katsarou
Vo.1 5/3/2016 NMD user profile and personas Ariana Nichogiannopoulou
v0.1 (alpha)
3/03/2016 Table of Contents Amihai Gottlieb, Nikolopoulos Spiros
v0.2 (beta) 18/04/2016 Beta version Ariana Nichogiannopoulou,
Nikolopoulos Spiros
V0.3 27/04/2016 Pre-final version incorporating the comments of the internal reviewers
Sofia Fountoukidou
V0.4 (final) 30/04/2016 Final version after proof reading Spiros Nikolopoulos
Author list
Organization Name Contact Information
TU/e Sofia Fountoukidou [email protected]
TU/e Jaap Ham [email protected]
AUTH Bostantjopoulou Sevasti [email protected]
AUTH Zoe Katsarou [email protected]
SHEBA Gabi Zeilig [email protected]
MDA Ariana Nichogiannopoulou [email protected]

D5.1 – V0.4
Page 4
Executive Summary
This document was divided in two tasks: the first task was to present a description of the patient groups’ attributes, in the form of user profiles and Personas; the second task was the design and selection of the persuasive strategies to motivate these users to accept, learn and finally use the MAMEM system. The ultimate purpose of the first task was to help the team members to recognize the real users of MAMEM. These are individuals with the following muscular disorders: Spinal cord injury, Parkinson’s disorder and Neuromuscular disorders. The profiles and personas will be used as input for several WP’s and tasks. The overall goal of the second task is to motivate individuals with disabilities to learn to operate the MAMEM system and to use it, in order to increase their social participation. Briefly, the user profiles include users’ characteristics such as demographics, relevant medical information, computer interaction behaviour and attitude towards novel assistive devices. Concerning the selected persuasive strategies, a plethora of tailored strategies has been proposed that take into consideration the needs and requirements of each of the three groups. Overall, the persuasive design has been divided into two phases, according to the pilot trials protocol, with two different objectives: user acceptance and engagement and social inclusion.
D5.1 – V0.4
Page 5
Abbreviations and Acronyms
ALS Amyotrophic Lateral Sclerosis
BCI Brain Computer Interface
DMD Duchenne Muscular Dystrophy
EEG ElectroEncephaloGram
IM Intervention Mapping
NMD Neuromuscular Disorders
PD Parkinson’s Disorder
PS Persuasive strategy
QOL Quality of Life
SCI Spinal Cord Injury
SMA Spinal Muscular Atrophy
* Additional abbreviations are spelled out within the document
D5.1 – V0.4
Page 6
Table of Contents
1 INTRODUCTION ......................................................................................................... 9
2 USER PROFILES AND PERSONAS ............................................................................... 10
2.1 User profiles ........................................................................................................ 10 2.1.1 SCI user profile ..................................................................................................................... 10 2.1.2 PD user profile ..................................................................................................................... 14 2.1.3 NMD user profile .................................................................................................................. 18 2.1.4 NMD computer operation ................................................................................................... 22
2.2 Personas .............................................................................................................. 24 2.2.1 SCI sets of personas ............................................................................................................. 25 2.2.2 PD set of personas ............................................................................................................... 29 2.2.3 NMD sets of personas .......................................................................................................... 33
3 THEORETICAL BACKGROUND OF PERSUASIVE STRATEGIES ....................................... 37
3.1 Persuasive technology ......................................................................................... 37 3.1.1 Self-determination theory ................................................................................................... 37 3.1.2 Self-regulation theory (goal setting) .................................................................................... 38 3.1.3 Dual processes ..................................................................................................................... 38 3.1.4 Social Cognitive Learning Theory ......................................................................................... 38 3.1.5 Theories on emotions .......................................................................................................... 39 3.1.6 Theory of Planned Behaviour .............................................................................................. 39 3.1.7 Principles of social influence ................................................................................................ 40 3.1.8 Social influence theories ...................................................................................................... 40
3.2 Persuasive design ................................................................................................ 41 3.2.1 Functional Triad ................................................................................................................... 41 3.2.2 The Persuasive Systems Design model ................................................................................ 43 3.2.3 Design with Intent ................................................................................................................ 45
4 SELECTION OF PERSUASIVE STRATEGIES FOR MAMEM ............................................. 47
4.1 Developing persuasive strategies for Phase I: user acceptance and training .......... 47 4.1.1 Intervention Mapping framework ....................................................................................... 47 4.1.2 Selected persuasion strategies ............................................................................................ 53
4.2 Developing persuasive strategies for Phase II: Social inclusion.............................. 58 4.2.1 Reciprocation theory ........................................................................................................... 58 4.2.2 Consistency .......................................................................................................................... 58 4.2.3 Social validation ................................................................................................................... 59 4.2.4 Theories of discrete emotions ............................................................................................. 59
4.3 Selected persuasive strategy: hierarchical memberships ...................................... 59
D5.1 – V0.4
Page 7
4.3.1 Selection of measuring activity indicators ........................................................................... 59 4.3.2 Users’ membership decision ................................................................................................ 61 4.3.3 Users’ rewards decision ....................................................................................................... 61
4.4 The motivation interface of MAMEM ................................................................... 62
5. CONCLUSIONS ............................................................................................................. 63
REFERENCES ................................................................................................................... 64
APPENDIX 1. VARIABLE MAPPING FOR PERSONAS CREATION FOR EACH GROUP ............. 71
APPENDIX 2. BEHAVIOUR CHANGE OBJECTIVE MATRICES ................................................ 74
D5.1 – V0.4
Page 8
List of Figures
Figure 1. The Persuasive Systems Design model (PSD) (taken from Oinas-Kukkonen & Harjumaa, 2009) ....................................................................................................................... 43
Figure 2. Phases in Persuasive Systems Development (taken from Oinas-Kukkonen2009) .... 45
Figure 3. Iterative steps of Intervention Mapping Approach (taken from Bartholomew et al., 2001). ........................................................................................................................................ 48
Figure 4. Basic concept underlying user acceptance models (adapted from Venkatesh et al., 2003). ........................................................................................................................................ 50
Figure 5. A unified model that integrates elements across the eight models (adapted from Venkatesh et al., 2003). ............................................................................................................ 50
List of Tables
Table 1. Intervention Mapping terms and definitions (Bartholomew et al., 2001) ................. 53
Table 2: Determinants of technology acceptance and use (Venkatesh et al., 2003) .............. 55
Table 3: Performance expectancy: constructs and definitions (adapted from (Venkatesh et al., 2003) ................................................................................................................................... 56
Table 4: Effort expectancy: constructs and definitions (adapted from (Venkatesh et al., 2003). ........................................................................................................................................ 56
Table 5: Social influence: constructs and definitions adapted from (Venkatesh et al., 2003). 56
Table 6: Facilitating conditions: constructs and definitions .................................................... 57
Table 7: Selected change objectives/determinants and theories and persuasive technologies for phase I……………………………………………………………………………………………………………………………59
D5.1 – V0.4
Page 9
1
Individuals who suffer from loss of voluntary muscular control while preserving cognitive functions are marginalized and unable to keep up with the rest of the society in a digitized world. MAMEM’s goal is to integrate these people back into society by increasing their potential for communication. In this direction, MAMEM will deliver the technology to enable interface channels that can be controlled through eye-movements and mental commands. MAMEM, for demonstrating enablement, will engage three different cohorts of patients: subjects with Spinal Cord Injury (SCI), Parkinson’s Disorder (PD) and Neuromuscular Disorders (NMD). In the WP6, clinical requirements were obtained by adopting the following approach: they conducted three focus groups, each one centred on each patient’s cohort, in which clinical specialists brainstormed about the needs and requirements to the add-ons that MAMEM can provide. The results of these focus groups are described in the Deliverable 56.1. The second pillar of approach was to administer questionnaires to approximately 15 users of each of the three groups and their caregivers, in order to extract clinical requirements from the point of view of the end-user. The analysis of the questionnaires is described in the Deliverable D6.2. In this document our purpose is twofold; to create user profiles of the three end groups and to select persuasive designed strategies in order to motivate users to accept and use MAMEM as well as to keep using it for online social activities. Therefore, in this deliverable, we started by describing the creation of the user profiles for each of the three groups. The user profiles were based on the results derived from D6.1 and D6.2 as well as on the review of relevant literature. The user profiles cover domains, such as medical information, computer difficulties, habits and attitudes with regard to users’ current computer operation. What is more, the user profiles formed the basis for the creation of sets of Personas for all three groups. As a result, 2 Personas were developed for each patient group. These Personas contain information, among other, about end-users’ demographics, physical disabilities, computer interaction behaviour, goals and attitudes. With regard to the second task which is related to the persuasive design of MAMEM, we started by examining an extensive literature review of theories and mechanisms underpinning persuasive technology most relevant to MAMEM. Next, using the Intervention Mapping approach, persuasive strategies were selected to motivate users to accept MAMEM and engage in the initial training needed. Lastly, following a different approach we selected persuasive strategy of hierarchical memberships to influence user to increase their online social participation. In a closing discussion we will summarize all findings and make some recommendations for future work within MAMEM and the field of persuasive technology.
D5.1 – V0.4
Page 10
2
The user profile is a method of presenting data from studies of user characteristics. In other words, a user profile of the target group contains collective information about mental, physical and demographic data for the user population as well as other characteristics. The ultimate goal of using user profiles is to help the team members (i.e. designers) to recognize or learn about the real user by presenting them with a description of a real user’s attributes. User profile does not necessarily mirror or present a complete collection of a whole user population’s attributes. The essence of user profiles is an accurate and simple collection of end-users’ characteristics *1+.
The user profile is almost the same as a persona, i.e. some kind of fictitious person as a collection of attributes (e.g. age, skills, attitudes, motivation level). However, while a user profile covers a range of characteristics of the target population, a persona uses specific characteristics (e.g. gender, experience and skill level), which are usually derived from the user profile.
In more detail, personas have been defined as hypothetical archetypes of actual users. They are not real people but they represent real people during the design process. Personas have proper names and are represented with pictures. Although they are imaginary, they are defined with significant rigor and precision. The purpose of a persona is to make the users seem more real and help designers to keep realistic ideas of users throughout the design process. Designers and evaluators can refer to the personas when considering design specifics. They put a name, face, and characteristics on users to keep the users in the forefront of design decisions [2].
2.1 User profiles
The user profiles for MAMEM were generated from an extensive literature review of our target groups, as well as patients’ questionnaire analysis and focus groups with professionals (derived from the Deliverables 6.1 and 6.2) [3, 4]. The following two subsections contain the user profiles and sets of personas for the three target groups (Spinal cord Injury, Parkinson’s disease and Neuromuscular disorders).
2.1.1 SCI user profile
In the following text, the user profile for SCI is described, covering areas such as disease range and characteristics, level of injury, physical symptoms, emotional functioning, cognitive functioning, motivation, computer operation and assistive devices.
SCI range:
• In Europe, the prevalence number of individuals with Spinal Cord Injury (SCI) is 330.000 and the occurrence number of new injuries per year is 11.000 [5].
• The average age of persons with SCI is about 40 years and the majority of them are males [6].
• Approximately 55% of all SCI individuals are tetraplegic with the majority of them (∼28%) having a neurological level of lesion at C4 and C5 at the time of discharge from acute care to rehabilitation facilities [7].
D5.1 – V0.4
Page 11
SCI Characteristics at C1-C4 levels of injury:
• Most severe of the spinal cord injury levels • Paralysis in arms, hands, trunk and legs • Patient may not be able to breathe on his or her own, cough, or control bowel or
bladder movements. • Ability to speak is sometimes impaired or reduced. • When all four limbs are affected, this is called tetraplegia or quadriplegia. • Requires complete assistance with activities of daily living, such as eating,
dressing, bathing, and getting in or out of bed • May be able to use powered wheelchairs with special controls to move around on
their own • Requires 24-hour-a-day personal care
Completeness or incompleteness of the injury:
• The completeness or incompleteness of the users’ injury in MAMEM will be: A, B and C
• Individuals with grades A and B have motor complete injuries, while those with grades C have some levels of motor function.
Medical symptoms:
Spasticity: • Spasticity is an increased, involuntary, velocity dependent, movement disorder
characterized by high muscle tone. Two thirds of the SCI have spasticity which interfere with their function [8].
Pain and fatigue: • Chronic neuropathic and/or musculoskeletal pain may interfere with functionality
and quality of life. Concentration and attention deficit could follow the pain. No treatment that definitely resolve these two conditions is available [9].
• About 25% of SCI report fatigue, severe enough to affect their quality of life, especially in persons aging with SCI [10].
Autonomic Dysfunction: • Orthostatic hypertension is a common condition in which blood pressure
suddenly falls; this may lead the SCI to change their wheelchair position from upright position to semi-upright or to lying position [11].
Respiratory and breathing issues: • Tetraplegics especially those with above C4 lesions have serious respiratory
problems; 3. 5% of the total SCI population have permanent dysfunction of the respiratory function and need artificial ventilation [7].
Emotional functioning:
• Regarding the psychological adjustment to SCI, negative emotional reposes (e.g. depression, anxiety), disengagement type coping (e.g. denial, avoidance) and the severity and impact of disability were found to be related to low levels of adaption [12].
D5.1 – V0.4
Page 12
• SCI people show lower level of life satisfaction; social support appears to be the most important variable in terms of social satisfaction [13]
• Depression is also high and escape/avoidance coping has been shown to play an essential role. However, many SCI individuals exhibit psychological resilience [13, 14].
• Influences on affective subjective wellbeing (related to emotions) are: general self-efficacy, perceived social support, perceived health and injury [15].
Cognitive functioning:
• Cognitive function can be normal, but a substantial number of SCI PEOPLE have significant deficits in one or more cognitive domains: moderate attention and processing speed deficits, mild deficits in processing speed, executive processing difficulties, or moderate memory impairments [16].
Motivational factors:
• Factors found to enhance participation of the SCI are: using cognitive and behavioural strategies (i.e., finding a role mode, creating routine and goal setting, recalling previous experiences and acquiring new knowledge); finding supportive environmental solutions (like social support), exploring motivation post injury (i.e. gaining and maintain independence, becoming a role model, being competitive and experiencing activity pleasure) [17].
• An enhancement of self-confidence of the SCI to increase their wellbeing could be achieved by providing positive reinforcement, accurate feedback, using role models and social support (e.g., information about support groups and social and recreational activities) [15].
Computer operation:
Computer and internet use: • The majority of the SCI (over two thirds) has access to a computer and most of
them are daily internet users. • Factors that contribute to high computer use and internet access are: age (those
injured before the age of 30 and especially before the age of 18 year) education (people with college or graduate degrees) and race (i.e. white individuals).
• The level of neurologic injury have not been found to negatively affect the computer and internet use of the SCI [18]. Entertainment, access to information (i.e. disability and health, transportation, employment and education) and social connection via the internet have been found to have an impact on the health-related quality of life of the SCI [19].
• It has been observed that the level of perceived of social support as a consequence of the computer use may be different from the actual change in individual’s network *20].
• According to the clinical specialists, common barriers that the SCI face when operating computers are: working positioning, screen positing, low level of accuracy, slow work, fatigue efforts and pain, limited computer working time,
D5.1 – V0.4
Page 13
spasticity, significant motivational difficulty, lack of spontaneity, need for constant assistance, need of training of the caregivers, funding difficulties [3].
Computer use habits: • The three most important computer uses are: productive activities and
recreation, social participation, study and information. • The three most important computer contribution to their lives are: educational
attainment, work and employment status/potential, interpersonal interactions and relationships [4].
Difficulties in computer operations: • Difficulties performing on a computer are: using two keys at the same time,
typing with the keyboard, selecting and dragging, resizing windows, moving the cursor on the screen and using keyboard.
• SCI patients stated that they have considerable difficulty creating text. • The majority of the SCI points on the screen with an assistive device and create
text either by the keyboard or by using a typing stick [4]. Current working environment: • The majority operates the computer at home; other locations of use are
university, a friends’ house, or at work. • Both stationary and portable computers are used. • The computer is mostly located on a desk and the SWCI sit on a wheelchair during
the computer operation. • SCI respondents reported a considerable impact of their physical condition on the
following computer use aspects: endurance, effectiveness and fatigue [4]. Needs, missing functions and demands for improvement: • The computer operation that some of the patients miss are games and computer
functions related to keyboard and mouse. • The majority of the patients were positive but with conditions in using an assistive
device system based on mental commands. Based on some answers, such a device would enable them to better use the cursor and the keyboard and to surf the web.
• Most of them are positive but with conditions in using AD based on eye movements.
• However, almost half of the respondents said that they would not wear a cap for recording EEG; they were more positive in wearing glasses for recording eye movements [4].
Assistive device use: • The most common assistive devices used by SCI persons are joy- sticks for the
hand or the chin, suck-and-puff control, voice control, and eye-tracking systems [7].
• The more sophisticated and complex a system is, the more functionality can be obtained from it, but the more difficult it is to use. On the other hand, if the device is too simple and general, computer interaction becomes slow and tedious [21].
D5.1 – V0.4
Page 14
• The majority of SCI people use assistive devices (87, 8%), with the most popular being the typing stick. Their level of AD satisfaction was rate as above average [4].
Brain computer interfaces:
• Factors that limiting the successful use of BCI, are: technology related (e.g. need for gel electrodes, expert’s setup and supervision), user specific (i.e. general cognitive problems of the older population such as attention and concertation deficits, medication, acute stress syndromes and depression) and infrastructure dependent [7].
• Paraplegic patients found to achieve satisfactory results with EEG-based BCI while for some tetraplegic, it is expected that extensive training is needed to achieve good BCI performance [22].
BCI training:
• High physical and mental workload is needed, during a training for the BCI operation [23].
• For high-level tetraplegic, an extensive BCI training does not necessarily lead to superior results.
• It should be communicated with participants that their BCI performance can be low or moderate; this is, to avoid a false impression that in addition to their body even their brains do not work properly [24].
2.1.2 PD user profile
In the following text, the user profile for PD is described, covering areas such as disease range, motor and non-motor symptoms, medication, cognitive functioning, quality of life, motivation, computer operation and assistive devices.
PD range:
PD is a common neurodegenerative disorder affecting approximately 1% of the population over the age of 60 years. It has an age adjusted frequency of 1.3 cases per 100.000 people younger than 45 years of age and 310 cases per 100.00 in those aged 75-85 years. The median of onset is 60 years although 15% of cases present before the age of 45 years.
PD is 1.5 times more frequent in men than women [25].
Most of PD patients are married with adult children and they live with their spouses [4].
Motor PD symptoms:
Basic motor symptoms in PD include bradykinesia/akinesia, tremor at rest, rigidity, postural instability, flexed posture and freezing. The predominant type of motor symptom can be either tremor or akinesia/rigidity [26].
Bradykinesia/akinesia:
D5.1 – V0.4
Page 15
Bradykinesia encompasses delayed motor initiation, slowed and diminished voluntary movements, difficulty in executing sequential actions and inability to perform simultaneous actions [27, 28].
Tremor:
It affects about 70% of PD patients.
It affects various body parts, eg hands, feet, jaw, feet. It can be very mild but in some patients it can be severe and continuous [29].
Posture/loss of postural reflexes and freezing:
As the disease progresses patients begin to assume a flexed posture and they can experience a loss of postural reflexes
Freezing consists of sudden, transient (sec) inability to move [30, 31]. Rigidity:
It is characterized by increased muscle tone to passive motion and it can be smooth or jerky [32].
Oculomotor function and ophthalmological features:
Oculomotor alterations have been found in PD, such as impaired smooth pursuit, increased latency of visually guided reactive saccades, reduced saccadic gain and difficulties to inhibit unwarranted reactions [33].
Many complaints and deficits have been reported in patients with PD, ranging from blurred vision and diplopia to impairments of contrast and colour discriminations, reduced cognition of facial expression and impaired motor detection [34].
Non motor symptoms:
Anxiety:
30.7%-55.8% of PD patients experiences symptoms of anxiety [35].
Most common feelings of anxiety described are restlessness, feeling tense and worrying thoughts.
Factors associated with anxiety are gender and age; females and younger patients are more prone to anxiety.
Often there is an aggravation of parkinsonian motor symptoms during periods of emotional arousal [36].
Depression:
Depressive symptoms are present to 22, 5 -56% of PD population [37].
Depression has been associated with sleep dysfunction, decreased functionality, cognitive decline and caregiver stress [38].
Apathy:
Apathy is diagnosed in 20-36% of new-onset patients.
Patients with apathy are more likely to be men, older and with more a severe motor impairment.
Apathy is related to 4 subdomains: decrease in emotional resonance, decrease in cognitive interests, emotional distress and absence of self-initiated behaviours [39].
Fatigue and pain:
D5.1 – V0.4
Page 16
Fatigue affects 58% of all people with PD.
Fatigue and pain can discourage patients to complete the (rehabilitation) programs and negatively affect the time PD patients spend on the computer [40].
Pain has a prevalence range from 30-83 %.
Pain has a multifactorial origin (ie. musculoskeletal, chronic pain) and reduces quality of life [41].
Medication:
Levodopa is the most effective antiparkinsonian agent [42]. With the disease progression and the long exposure to L-Dopa patients develop a wide range of Levodopa induced complications, which include motor and non-motor symptoms. Motor complications include fluctuations and dyskinesia. Non-motor fluctuations include neuropsychiatric symptoms, autonomic and sensory symptoms [41].
Cognitive functioning:
Mind cognitive impairment (MCI) in PD individuals is associated with increasing age, disease duration and disease severity [37, 43].
The frequency of cognitive dysfunction is from 36% at the time of diagnosis to as high as 93% in more advanced stages of the disease.
The most frequently encountered domains of cognitive dysfunction involve: executive functions, memory, visuospatial skills, attention, and mental processing speed.
Preserved functions include basic attentional processes and many language abilities (particularly comprehension) [44].
Quality of life (QoL):
PD patients are vulnerable to deterioration of QoL, due to significant motor disabilities, depression, communication, difficulties, social isolation, loss of employment and social embarrassment [10].
Patients with early onset of PD (EOPD) are more affected, because the longer the disease, the higher the physical, economical and psychosocial burden is.
EOPD patients show more severe depression and more impaired emotional domain of QoL [46].
Motivation:
Feedback in terms of their achievement and progress, constant encouragement and being forgiving of the nature of their disease can increase motivation to PD patients.
High levels of motivation is needed to both relearn the computer and also how to use the computer fluently.
D5.1 – V0.4
Page 17
Prompting and continuous presentation of new stimuli, activities than can catch the interest of PD patients, but do not require effort can increase PD patients’ motivation.
It has been shown that PD patients preferred a more abstracted feedback that data of their performance and particularly data that could reflect over time.
Positive learning reinforcement during the training periods can be helpful.
The social element is important. Establishing an online community as a way to expand social circles and reach out to others who might need help is appealing to PD patients [47].
It is important to view each patient as an individual, experiencing different social, emotional and practical factors within their home which might impact the motivation to use technology especially when compared to clinical settings [48].
Clear tasks and skills that are required from the patient can enhance motivation.
Collaborative goal-setting can strengthen engagement of the patients and enhance sense of control and expectation of success.
The notion of data being stored and shared can be worrying to some PD patients. [49].
As the disease progresses PD patients show two typical personality traits characterized by low novelty seeking behaviour and by high levels of harm avoidance. These two traits are related to cognition and emotion [50].
Computer operation:
Computer use habits:
The two most important computer uses for PD patients are communication, information and social participation.
The three more important contributions of the computer are 1) interpersonal interactions and relationships, educational attainment and emotional wellbeing.
Age differences have been found with younger PD patients to be more experienced in their use of technology and their readiness to adopted new technologies [4].
Computer use difficulties:
The majority of the users experience serious interaction challenges.
Their main difficulties are related to the use of the cursor: moving the cursor on the screen, double clicking with the cursor, using two keys at the same time and clicking with the cursor [4].
Computer working environment:
They majority uses a stationary computer, with the computer being located mostly on a desk [4].
Needs, missing functions and demands for improvement:
Most of the PD patients were positive in using EEG but with conditions, such as to try them first and to be easy with a training provided.
D5.1 – V0.4
Page 18
Novel technologies are often interpreted by elderly as being too complicated or too modern for them to feel comfortable using [4].
Use of Assistive Devices (AD):
PD patients were found to have less acquaintance with alternative peripherals [51].
They appear to have lack of information of what kind of AD are available or how to optimize computer use.
With regard to their computer attitude, PD patients often express that they should cope with ordinary devices and adjust their own behaviour to better match “standard” ways of how computers are used [52].
Since PD symptoms vary, one assistive solution or a standard set-up will no fit all or suffice over time 53].
2.1.3 NMD user profile
NMD is a very broad term that encompasses many disorders and ailments, which are characterized by gradually reduced mobility. They all impair the functioning of the muscles either directly being pathologies of the muscle or indirectly being pathologies of nerves or neuromuscular junctions.
In the following NMD user profile we will focus on Duchenne Muscular Dystrophy (DMD), Spinal Muscular Atrophy (SMA), Amyotrophic Lateral Sclerosis (ALS) and Arthrogryposis, as these are the most common diseases among our group of patients. The user profiles of NMD describe areas such as disease range, physical symptoms, cognitive functioning, and quality of life for each of the four neuromuscular disorders and ends with a description of computer operation and assistive device use for all of them together.
2.1.3.1 Duchenne Muscular Dystrophy
Range:
DMA affects 1/4200 live-born boys.
Survival of the DMA patients into the early 30 is becoming more common [54].
Physical disabilities:
The muscles are affected at birth and there is a progressive muscle weakness.
Upper extremity function declines in the mid-teens and boys loose ability to feed and take care of themselves.
These boys begin to use wheelchairs full time between 8 to 12 years of age.
Other physical symptoms include cardiac and respiratory problems [55].
Touch and other senses, control over muscles of the bladder and bowel and sexual functions are intact.
Fatigue and pain are a common symptoms. Symptoms of fatigue in DMD boys are found to be approximately 40.5% and pain around 73.4%.
Cognitive, learning and neurobehavioral functioning:
D5.1 – V0.4
Page 19
A substantial number of the DMD population has a cognitive impairment.
Cognitive skills do not deteriorate over time.
Cognitive deficits documented in older children and adults mainly pertain to verbal skills.
Vision-spatial skills, long term memory and abstract reasoning skills are not affected.
NMD patients have being characterized as being easily frustrated, easily distracted, have poor attention span and immature [56].
Learning issues:
One third has a learning disability, although few have a serious mental retardation
Learning problems in NMD occur in three general areas: attention focusing, verbal learning, memory, and emotional interaction [57].
May have difficulty in understating complex-multi-stepped tasks and their frustration may interfere with learning [55].
Most boys tend to be creative and artistic [56].
Emotional functioning:
The majority of boys tends to cope well with their medical condition and to be emotionally adjusted.
Affective disorders tend to be twice than among healthy children [57].
Quality of life:
Quality of life in adults with various muscle diseases is significantly affected by disease severity, pain fatigue and mood [58].
NMD patients can face problems in the social domain, such as getting involved in an intimate relationship, work and leisure activities and mobility and transportation [59].
2.1.3.2 Spinal Muscle Atrophy
Range:
SMA causes progressive muscular weakness and atrophy, with males being mostly affected.
It has been estimated that 1 in 6,000 babies born will be diagnosed with SMA [60, 61].
Physical disabilities:
D5.1 – V0.4
Page 20
SMA is classified intro three main phenotypes, based on the age of onset and severity of disease [62, 63]: SMA Type I is the most severe form and represents approximately 60 % of
incident SMA cases. Children with it never sit or stand and rarely survive past 2 years of age.
SMA Type II accounts for approximately 30 % of SMA cases, usually evident by 18 months of age. Many survive into adulthood, but life expectancy is shortened compared to the general population.
Approximately 10 % of SMA cases are classified as SMA Type III. SMA symptoms tend to be milder compared with Types I and II, appearing anytime between 18 months of age and adulthood. These patients have a normal lifespan.
Type IV, the mildest form, is rare. Individuals with this form do not exhibit muscle weakness until adulthood.
Cognitive functioning:
SMA patients are characterized by a general intelligence in the normal range.
Due to immobility, the domain of thinking and learning becomes the main area of creativity [64].
Psychosocial functioning:
Psychosocial impact of living with DMA has been indicated in 10 thematic areas: 1) confronting premature death; 2) making difficult treatment choices; 3) fearing the loss of functional ability; 4) coming to terms with lost expectations; 5) loss of sleep and stress; 6) social discomfiture and stigma; 7) limitations on social activities; 8) struggle to achieve independence; 9) uncertainty and helplessness; and 10) family finances [63].
Strategies to successful living with SMA include 4 themes: establishing a network of strong relationships; normalizing (i.e. living independently, engaging in leisure activities) and mainstreaming (i.e. maintaining an employment and being productive societal member) within society; adopting a creative and innovative approach to managing the symptoms; maintaining an optimistic life view [62].
Quality of life:
Higher rates of stress and strain and lower rates of social support have been reported, compared to healthy children, which affect the quality of life [63].
2.1.3.3 Amyotrophic Lateral Sclerosis
Range:
The annual incidence of ALS is approximately 1.5 to 2.7/100,000/y and the prevalence is 3 to 5/100,000.
The average age at onset of ALS is 55 to 65 years, though the range is very large [18].
D5.1 – V0.4
Page 21
Symptom onset can occur from the late teens through the tenth decade of life. Incidence in the younger age groups is very low.
AMS more commonly strikes men than women, with a male predominance of approximately 1.5:1.
Overall, the average survival after diagnosis is approximately 3 to 5 years. About 10% survive longer than 10 years [65].
Physical Disabilities:
The degeneration of neurons leads to weakness, the overriding symptom of the disease, with a variety of symptoms and signs such as muscle atrophy, fasciculation, spasticity and increased reflex activity. Other symptoms of include progressive dysarthria that can limit communication and respiratory failure [18].
Neural degeneration may progress, such that patients arrive at the complete locked-in state. Most patients will use a motorized wheelchair at some point in the disease [65, 66].
Cognitive and behavioural functioning:
Up to half of ALS patients have cognitive or behavioural deficits. Cognitive deficits can appear in verbal fluency, attention, visual and verbal memory and learning [66].
It was found that 40% of patients with ALS have mild cognitive changes [65].
ALS patients have been rated as significantly lower than other medical patients in the Openness trait (the characteristic of being attentive of various areas of experience, including fantasy, intellective and feeling states).
ALS patients are described by their doctors as being “nicer” than the average patient and they appear to comply with their medical treatment [67].
Quality of life
The QoL domains most often named are family friends/social life, health and profession. Other domains mentioned are finances, entertainment and spiritual life [68].
Brain-computer interface
People with ALS usually express strong interest in the BCIs
Patients require a BCI system to be multifunctional, accurate and robust against false-positives.
Perception of success on BCIs is very important for the system acceptance and use. Performing well tends to increase the interest while performing unsatisfactorily can decrease the desire to use the device [66].
Analysis of the relationship between physical impairment and level of success in BCI concluded that brain regulation for communication was possible in all stages for paralysis except those in a complete locked-in state [69].
D5.1 – V0.4
Page 22
2.1.3.4 Arthrogryposis
Physical disabilities
Arthrogryposis is a descriptive diagnosis used to denote more than 300 individual diseases with varying etiologies.
It is present in affected children from birth and occurs in about 1 in 10,000 live births.
It is characterized by malformed or stiff joints, muscles, and tendons that result in arms, legs, hands, and/or feet having limited or no mobility. Scoliosis (a curvature of the spine) may be present in some children as well [70, 71].
Cognitive functioning:
The cognitive function of children with the condition is not affected. In fact, they are often extremely bright and communicative.
2.1.4 NMD computer operation
Computer use:
Gender differences were found, with girls to use the internet more often for mailing, information about health/diet and school, and boys use it more often for playing games and sport information [72].
The ability to use a computer independently can provide NMD a sense of being normal having a regular life and it can provide privacy.
People with NMD often worry that they might lose their minds, so the use of computer validates their ability to think, respond and function well.
NMD patients are susceptible to tiredness when using computers, as they have limited energy resources [3].
Computer use habits:
They are described as frequent compute users
They most frequently use a laptop
The three most important computer uses were: social participation, communication and recreation
The thee most important computer applications were: internet browser, e-mail, word processor
The three most important aspects of computer contribution in their life were: 1) interpersonal interactions and relationships, 2) educational attainment 3) work and employment status/potential [4].
D5.1 – V0.4
Page 23
Difficulties in computer operations:
Computer difficulties pertain to identifying the cursor on the screen, using the keyboard, identifying the letters on the keyboard, using two keys at the same time, selecting and dragging and resizing windows.
Participants reported difficulties in using the keyboard.
NMD diseases can be progressive, and eventually, progressively, the use of computer becomes even more challenging, as the patient becomes easily tired, has many involuntary twitches that slow down the use of computer and create frustration and tiredness, so eventually, as the disease progresses, many patients just give up using the computer or use it less and less [4].
Current working environment:
Both stationary and a portable computers are used.
The computer is mostly located on a desk or rarely on an arm or on bed or on ones legs.
They operate the computer at their home and they usually sit on either a motorized wheel chair or a wheelchair, while operating the computer [4].
Needs, missing functions and demands for improvement:
With regard to computer applications, playing games and reading magazines and newspapers were mentioned.
Their attitude toward BCI were positive but conditional (if it was easy and had proper training).
Their attitude toward AD based on gaze were positive but conditional; problems with focus were mentioned.
Generally they have a positive attitude towards wearing an EEG recording device and/or special glasses on their head, but conditional (if it was needed or if it was comfortable/easy to use). Some negative answers include concerns about pressure on the head by the AD, fear of radiation, and sensitivity to touch on the head, problems with focus and respirator [4].
D5.1 – V0.4
Page 24
2.2 Personas
In order to create personas for each of the three target groups, a list of variables that seem to be the most relevant for the MAMEM scope was made. These variables (i.e., demographic, behavioural) were derived from the user profiles. Next, for each group, we mapped participants’ responses to the questionnaires, presented in the Deliverable D6.2 and summarised in the user profiles, against the selected set of variables. The overall goal of the variable mapping was to find a major pattern for each variable that will form the basis for the personas. The sets of variables have been grouped to four groups for all three groups: demographic, medical, computer use and goals and attitudes. Lastly, in order to complete the personas, we added extra details based on the user data (i.e., occupation, marital status) (D6.2).
Table 1 provides detailed information about the chosen variables for SCI and how SCI patients were mapped against them. Table 2 and 3 shows the same information for PD and NMD respectively. It is worth mentioning, that inclusion and exclusion criteria for the MAMEM pilot trials were taken into account for the variable mapping and consequently for the personas creation. Hence, according to the inclusion criteria, the SCI audience will be included by individuals suffering from complete or incomplete SCI (level A, B and C), from C5 level and above. What is more, according to the exclusion criteria, participants with any psychiatric (e.g., major depression) or cognitive conditions that might interfere with understanding the instruction or with cooperation will be removed. Thus, the variables of cognitive and emotion functioning were not taken into primary consideration for the personas creation.
In the following subsections, we present two set of personas for each group to represent a wide range of end-users.
D5.1 – V0.4
Page 25
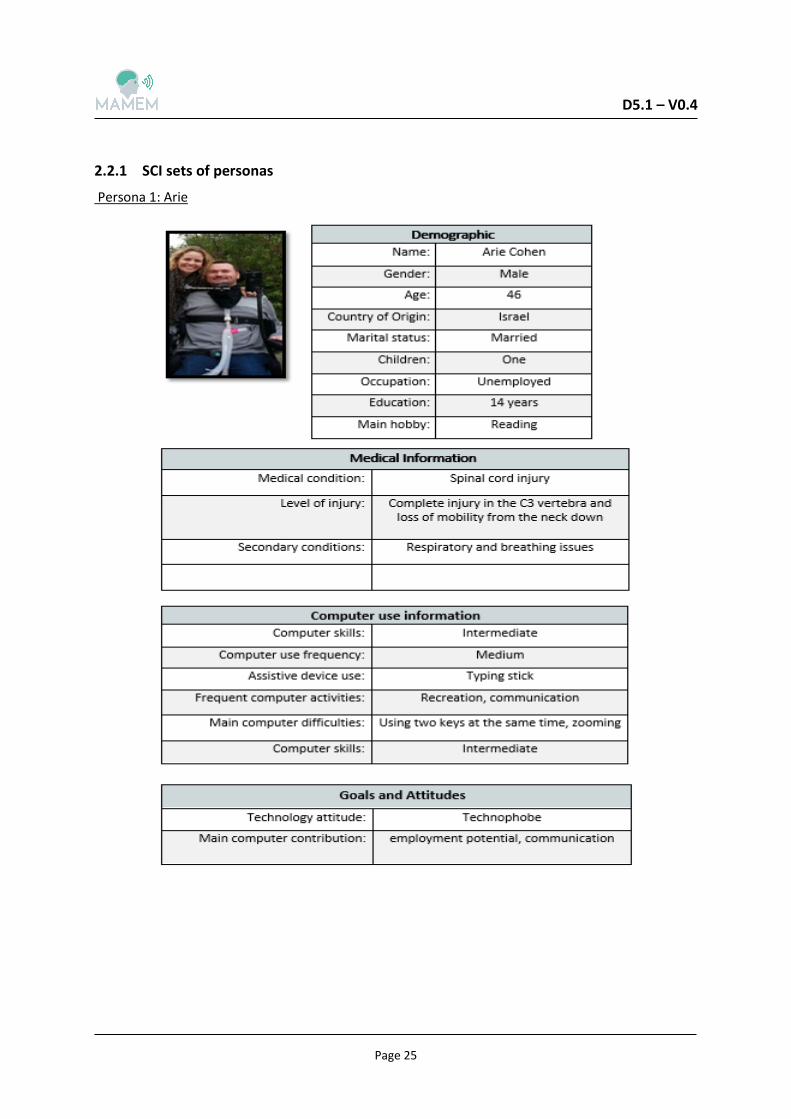
2.2.1 SCI sets of personas
Persona 1: Arie
D5.1 – V0.4
Page 26
Arie is 46 years old and he lives with his wife in Tel Aviv, Israel. His life changed after a military training accident that caused him a SCI. Now he has a complete tetraplegia at C3. After completing his rehabilitation, he finally managed to sit and to move using a motorized wheel chair. This was one of the biggest accomplishments for Arie, since he struggled a lot to make it happen. He is also mechanically ventilated, 24/7.
Arie requires a complete assistance with almost all daily activities. Due to the fact that his wife works full-time, he has a professional caregiver to take care of him most of the day. He is unemployed at the moment, but he receives a financial support from the Ministry of Defence. Although he has several friends that meets frequently, he feels most of the time bored and he really misses doing something productive.
His feelings of monotony exacerbated when his son, Timothy, left the house recently. Timothy is 23 years old and he has recently moved to the U.S. to study; thus they do not see each other very often anymore. Arie is very unhappy because of this and he misses him a lot.
Arie discussed about his feelings with his wife, who insisted that it is time to find an assistive device to help him operate the computer better, in order to be better able to search for a job and to communicate with their son more frequently. Arie does not like changes and he is very cautious when trying new things; that is why he was reluctant to use an assistive device all this time. However, after he started using a typing stick, his computer use has increased. He uses image applications to edit photos and send them to his son through social media networks. He also uses internet browser to search for job vacancies and sends job applications through mail.
Although, the typing stick is useful, Arie still faces many difficulties with his computer operation. This difficulties are related to both the type of the assistive device and his medical condition. Specifically, he has troubles using two keys at the same time and zooming. In addition his medical condition has an impact on the endurance and effectiveness of computer use. As a consequence, he do not use his computer as often as he would desire. Although, he would like an assistive device that would provide him conform and ease of use, he lacks the motivation to search for a more suitable one and learn how to use and master it.
D5.1 – V0.4
Page 27
Persona 2: Sarah
D5.1 – V0.4
Page 28
Sarah is a 29 years old and she lives in Tel Aviv, Israel. Nine years ago, she had a car accident that left her with a SCI at C4; she has partial finger mobility and she uses a motorized wheelchair. Sarah leaves with her mother, who is also her main caregiver. They have a very good relationship, since her mother was always very caring and supported her a lot after her injury.
At the moment, Sarah is a psychology student at Tel Aviv University. She is a very good student and se is very motivated to finish her master’s degree soon. She travels to the university twice per week to attend the lectures and meet with her fellow students. Her future goal is to work as a researcher in this field.
In her spare time, Sarah likes writing psychology articles and she often uploads those that she likes the most in a blog that she created for this purpose. In addition, she enjoys listening to music, especially when she has mood swings; her favourite band is Nirvana and Beatles.
She has an extensive computer experience, even before the accident, and she uses her laptop daily. Sarah’s main computer activities are related to her studies; this is, reading and writing articles. She most often uses internet browser and word processor.
Although a daily computer use is vital to her, most of the times she has to stop the operation after some time, due to pain and fatigue efforts. This frustrates her a lot because she cannot finish as quickly as she would desire. After trying different assistive devices, she concluded that using a mouth stick to point on the screen and a keyboard to type is the most optimal solution. However, this solution is likewise problematic, since it still slows down her computer operation significantly.
For this reason, she is currently looking for an assistive device, which will help her to improve her computer use. She was always an adventurous person and she would like to be trained and use high tech gadgets and devices that would help her to successfully finish her studies and work as a researcher afterwards.
D5.1 – V0.4
Page 29
2.2.2 PD set of personas
Persona 1: Giorgos
D5.1 – V0.4
Page 30
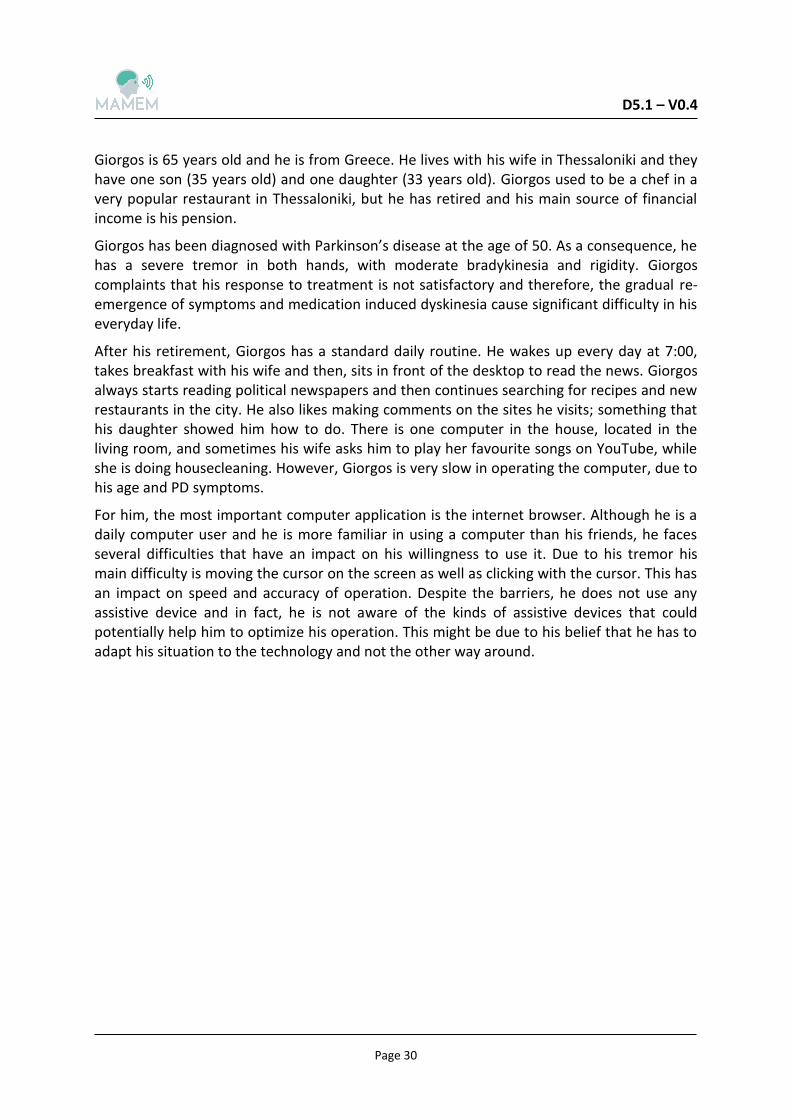
Giorgos is 65 years old and he is from Greece. He lives with his wife in Thessaloniki and they have one son (35 years old) and one daughter (33 years old). Giorgos used to be a chef in a very popular restaurant in Thessaloniki, but he has retired and his main source of financial income is his pension.
Giorgos has been diagnosed with Parkinson’s disease at the age of 50. As a consequence, he has a severe tremor in both hands, with moderate bradykinesia and rigidity. Giorgos complaints that his response to treatment is not satisfactory and therefore, the gradual re-emergence of symptoms and medication induced dyskinesia cause significant difficulty in his everyday life.
After his retirement, Giorgos has a standard daily routine. He wakes up every day at 7:00, takes breakfast with his wife and then, sits in front of the desktop to read the news. Giorgos always starts reading political newspapers and then continues searching for recipes and new restaurants in the city. He also likes making comments on the sites he visits; something that his daughter showed him how to do. There is one computer in the house, located in the living room, and sometimes his wife asks him to play her favourite songs on YouTube, while she is doing housecleaning. However, Giorgos is very slow in operating the computer, due to his age and PD symptoms.
For him, the most important computer application is the internet browser. Although he is a daily computer user and he is more familiar in using a computer than his friends, he faces several difficulties that have an impact on his willingness to use it. Due to his tremor his main difficulty is moving the cursor on the screen as well as clicking with the cursor. This has an impact on speed and accuracy of operation. Despite the barriers, he does not use any assistive device and in fact, he is not aware of the kinds of assistive devices that could potentially help him to optimize his operation. This might be due to his belief that he has to adapt his situation to the technology and not the other way around.
D5.1 – V0.4
Page 31
Persona 2: Eleni
D5.1 – V0.4
Page 32
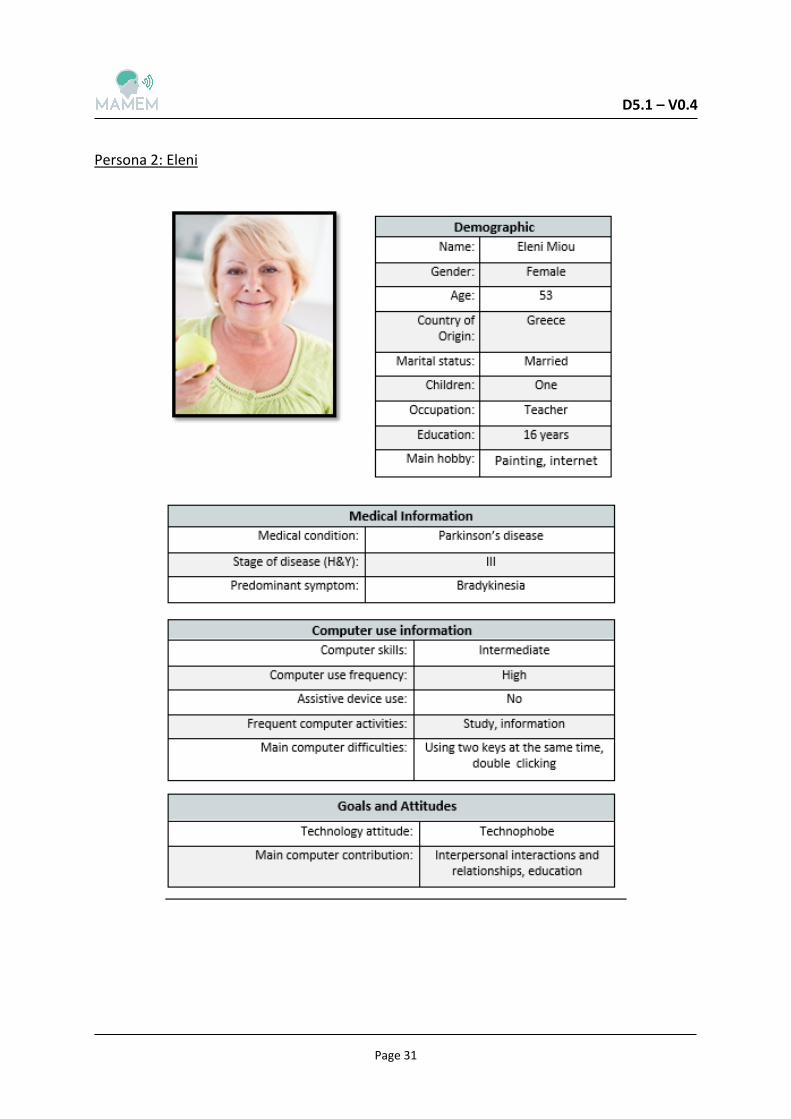
Eleni is a 53 year-old teacher from Thessaloniki. She has two children, one daughter who lives in the same block, and one son who lives in the UK. The last years were very difficult for her, because her husband passed away and she has been diagnosed with Parkinson’s disease.
Eleni finds her peace of mind in painting. She is very good in many artistic activities, but the last years she is slow in motor initiation and she cannot do two things at the same time. She also experiences severe stiffness in her muscles and she cannot move her hands from time to time. The doctors informed her that this is a parkinsonian symptom, called bradykinesia. Likely, due to levodopa medication, these symptoms are decreased and she can go back to painting again. However, the medication is not always effective and during its off periods, she experiences involuntary movements.
However, Eleni does not give up easily, and she is determined to know more about her disease and find new ways to cope with her symptoms and daily life. Her computer is the main source of information. She frequently searches for medical information about PD. Specifically, she uses the browser to educate herself about PD characteristics, evolution, medication, treatment alternatives, and physical therapy and future perspectives. What is more, she recently joined an online course for painting to improve her skills. This also increased her social interaction, as she often communicates with her teachers of the online course, as well as the other registered members, through mails.
Although Eleni uses the computer frequently, she phases some barriers during its operation. She has problems using two keys at the same time and double click with the cursor. Thus, she does not feel that she is effective and her satisfaction is low. She would like to use an assistive device and she recently started searching on the web how other people with PD overcame the barriers and optimized their computer use. Although she is motivated to find more information, she lacks the trigger to motivate her further and actually buy one.
D5.1 – V0.4
Page 33
2.2.3 NMD sets of personas
Persona 1: Nikos

D5.1 – V0.4
Page 34
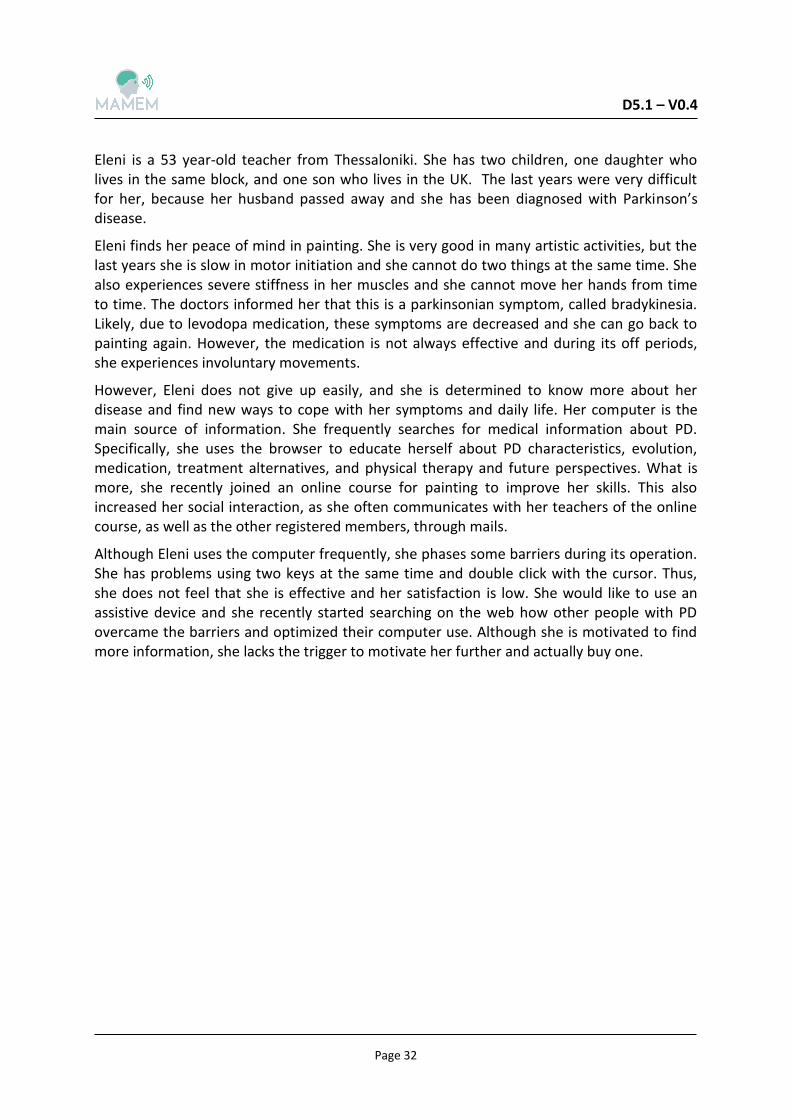
Nikos is a 25 years old and he lives with his parents and sister in Athens. From very early in life he has been diagnosed with spinal muscular atrophy; a disease that causes a progressive muscular weakness and atrophy. As a result, he is unable to take care of himself and he has respiratory problems. He has a very supportive family, and he is very close to his mother, who also is his main caregiver.
Nikos has two passions in his life; sports and writing. Thus, he found a way to combine them;
he obtained a degree in journalism from the University of Athens and he became a sports
journalist. At the moment, he works part time in two sports magazines and his task includes
writing articles related to various sports.
Due to the nature of his work, Nikos uses his computer daily, in order to find information
about sports players, to watch games and to prepare his articles. In addition, he follows his
favourite players on twitter and has frequent online discussions with his friends and
colleagues, mainly about sports.
He types a lot every day using a virtual keyboard and he uses the mouse to point on the
screen. However, he gets tired easily when using a computer and he has to stop his online
activities. He would like to try new assistive devices that would offer him comfort and to also
increase his computer satisfaction.
D5.1 – V0.4
Page 35
Persona 2: Alex
D5.1 – V0.4
Page 36
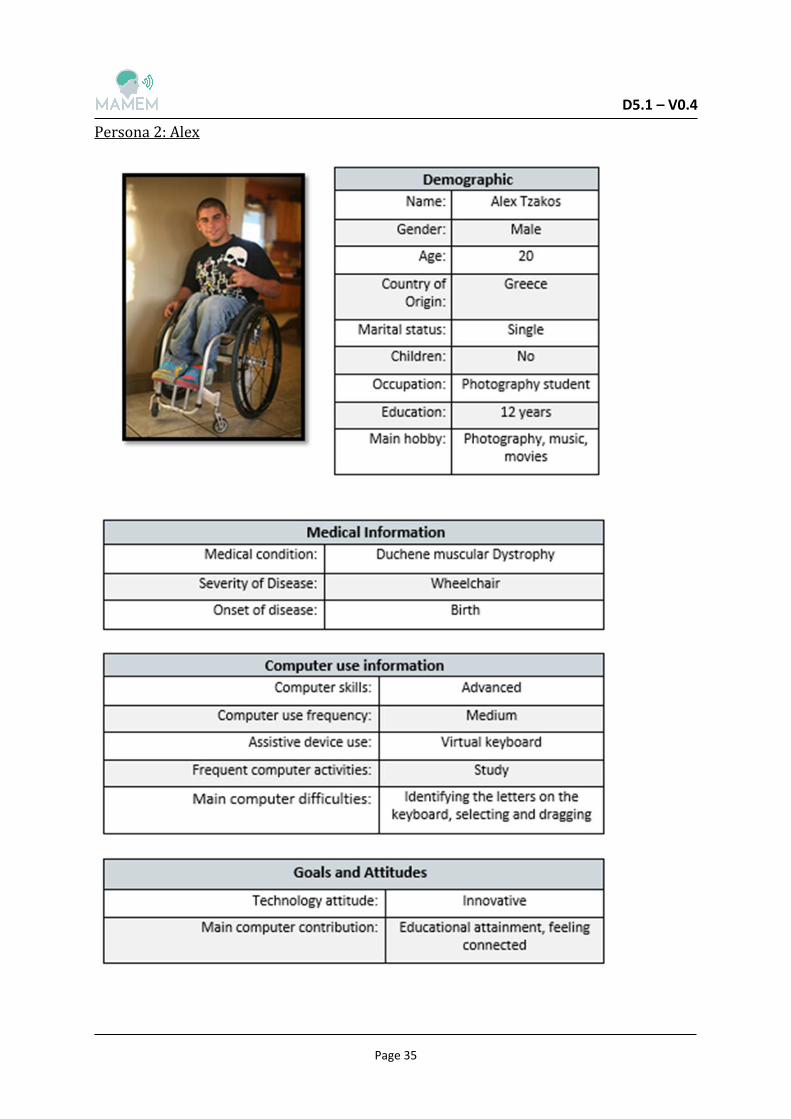
Alex is a 20 year-old photography student. His main hobby is capture the moments with his camera and then transfer them to his laptop. He also enjoys editing them and make them look more artistic. The best pictures are uploaded in his Instagram and Facebook page.
Alex is also a Duchene patient. He has severely disabilities and he needs his mother’s help in all aspects of his daily life. Sometimes he feels frustrated by his lack of privacy and independence. However, his disease never prevented him to make dreams about his future. He wants to become a well-known photographer.
For this reason he follows online courses on photography. Therefore, he tries to use his computer daily in order to attend the online lectures. However, this is not always possible, because he suffers from pains, which make him feel exhausted during the day. In addition to his medical condition, he faces some difficulties in using his computer. The most significant barriers for him are to identify the letters on the keyboard and select and drag with the mouse. He has used several assistive devices, such as a pointer and virtual keyboard, which improved his computer operation, but his satisfaction is still somewhat low. He likes to feel connected with the others through the photos that he shares online, and to improve his skills in photography and this desire motivates him to be open to innovative assistive devices that could make his computer operation more effective. Through forums, he discusses with other people, similar to him, about new assistive devices and he is convinced that there must be something that could help him to use a computer without feeling exhausted afterwards.
D5.1 – V0.4
Page 37
3
In this Chapter we will discuss about persuasive technology as well as theories underpinning persuasive technology (3.1) and persuasive design (3.2). It should be clear that the intention is not to present a complete overview on the existing literature; rather to explore theories in the health-related context, which can form the basis for selecting persuasive strategies for the MAMEM system.
3.1 Persuasive technology
Fogg (2003) defines persuasive technology as “the class of technologies or interactive computing systems that are intentionally designed to change a person’s attitude or behaviour” *73+. Social and behavioural sciences offer several theories containing relevant persuasive principles. In the following paragraphs, various theories and mechanisms underpinning persuasive technology will be presented and principles of persuasive design will be discussed.
3.1.1 Self-determination theory
Self-Determination Theory (SDT) is concerned with the degree to which an individual’s behaviour is self-determined [74]. This refers to whether the resulted behaviour is a product of an individual’s free choice or it is imposed to him/her. This is important, because the degree of one’s self-determination to produce a behaviour is associated with the quality of his/her motivation. This degree is dependent on how well meets the expectations of the internal psychological needs of a person. According to SDT three psychological needs must be satisfied for optimal functioning and personal development:
Competence is the ability of an individual to achieve challenging tasks and having the feeling that he/she is capable to attain a goal. Perceived competence can be escalated by social context events, like positive feedback or rewards, To the contrary, negative feedback can reduce it.
Autonomy refers to the feeling of an individual to be in control. This can be achieved either by taking his own decisions or by consciously deciding to let the opinion of others lead him in taking decisions. Autonomy must go together with competence so as people to view their behaviour as self-determined by intrinsic motivation.
Relatedness is the need of a person to feel connected to others around him/her. Individuals need interpersonal relations and social support, because this generates a safe and secure feeling.
The more certain behaviour satisfies each of these needs, the more self-determined the behaviour is and the more a person will be motivated to demonstrate (and keep on producing) the behaviour. A high quality of motivation (highly self-determined) will increase the likelihood of long-term motivation and long-lasting behaviour change.
D5.1 – V0.4
Page 38
3.1.2 Self-regulation theory (goal setting)
Self-regulation pertains to the capacity of a person to impinge on and change his/her responses. Specifically, it describes the process that people use to inhibit unwanted urges by gaining control over the impulsive response. This is required when short-term objectives contradict longer-term ones, for example enjoying food and staying fit [75]. These two aims are thought to be set by different mental systems: the impulsive system, which functions automatically and without effort and the reflective system, which works slower since it is charge of higher order mental operations [76]. For self-regulation, different ingredients are essential [75]:
Standards or goals: what does one want to accomplish or reach?
Monitoring: reaching a standard or goal requires a feedback-loop [77]. A person’s self-regulation can be based on the comparison to the self (or the relevant aspect of the self) to the standard.
Willpower, or self-regulatory strength: self-regulation as well as effortful choice and active initiative, are based on a limited resource that is consumed during such activities. Ego depletion refers to a state in which the self does not have all the resources it usually has. Ego depletion renders the self temporarily less able and less willing to function normally or optimally.
Motivation: caring about reaching the standard or goal. Motivation may be especially effective in compensating for decreased willpower (when willpower is not entirely depleted).
3.1.3 Dual processes
According to Dual process models, a behaviour can be described through two routes: an effortful rational route and an effortless automatic route. Such models also explain under which conditions the two routes are most likely to be activated. Recent formulations of the dual processes are the Reflective-Impulsive Model [78] and the System1-System2 approach [79]. In line with the dual process models, research has demonstrated that human behaviour is not only dictated by explicit, conscious processes, but also by implicit, non-conscious processes. In recent years, various behaviour change techniques (BCT) have been developed that targeted these automatic processes, in order to attain change behaviour [80].
3.1.4 Social Cognitive Learning Theory
Bandura's Social Cognitive Theory (SCT) is an interpersonal theory that covers determinants of behaviour as well as the process of behaviour change [81, 82]. In more details, it differentiates between two behavioural expectations, outcome expectations and efficacy expectations:
Outcome expectations touch on beliefs that a specific behaviour will produce a certain outcome. For example, being more physically active will improve a person’s physical health.
Efficacy expectations refer to the belief that one is capable of showing a certain behaviour. It reflects the self-confidence of an individual that he/she is able to
D5.1 – V0.4
Page 39
perform something and not about his actual capability. E.g. a person could still believe that he is not able to bike 100kms even though he is indeed capable of doing so.
3.1.5 Theories on emotions
Theories have distinguished among affect, emotion, and mood. Although these terms have been often used interchangeably, many researchers came to an understanding that each term is a representation of a different phenomenon. This distinction is essential because they may have different causes and consequences, they may unlike in the way they interact with behaviour and its determinants, and consequently in how they can be addressed to produce behaviour change. Moods are diffuse feeling states, as a consequence of a series of events, and typically it is difficult to recognise what causes this state [83]. Moods are relatively low intensity feelings which do not interfere with ongoing activities [84]. On the other hand, emotions are briefer than moods, powerful and the specific event that generated them is easily identified and well-defined [85]. Emotions request attention, and interfere with cognitive processes and behaviours [84]. Ekman has distinguished six basic emotions, which are universal among the cultures: fear, disgust, anger, surprise, happiness, and sadness, and later, he also included embarrassment, excitement, contempt, shame, pride, satisfaction, and amusement [86]. Finally, the term affective attitude (or “affect”) refers to judgment about the pleasantness or unpleasantness of the execution certain behaviour [87, 88]. Within affective attitudes a further distinction has been made between anticipated affect and anticipatory affect. The first reflects the affect one anticipates to experience after engaging (or not engaging) in behaviour. Anticipatory affect pertains to the affect one anticipates to experience while engaging in certain behaviour.
3.1.6 Theory of Planned Behaviour
The Theory of Reasoned Action (TRA) claimed that the intention to perform a behaviour is determined by the attitude towards that behaviour and the subjective norm regarding that behaviour [89]. Later, the Theory of Planned Behaviour (TPB) was formulated in which a third determinant was added, namely perceived behavioural control [90].This determinant was similar to the concept of self-efficacy [82]. In recent times the theory was reformulated, by specifying that behaviour is determined by intention, to the extent that people have actual control over their behaviour [91]. Determinants of the actual control are considered environmental factors and skills to deal with these factors. Intention is determined by attitude, subjective norm, and perceived behavioural control, which in turn are all determined by salient beliefs: behavioural beliefs, normative beliefs and control beliefs. Attitudes are based on the expected positive and negative consequences of a behaviour. A subjective norm is the person’s perception that most significant others think whether he should or should not perform the behaviour in question. Lastly, perceived behavioural control echoes the notion of how much an individual is able to influence a behaviour. These three factors provide insights into what influences the behaviour, and thus which determinants should be altered.
D5.1 – V0.4
Page 40
3.1.7 Principles of social influence
Robert Cialdini (1998) has developed six principles that underpin the majority of successful social influence strategies. He refers to these principles as the six universal principles or rules of social influence [92]:
• Reciprocity: People by their nature feel obliged to return a favour and to pay back others. Thus, when a persuasive request is made by a person the receiver feels indebted to, the receiver is more inclined to adhere to the request.
• Commitment and consistency: People by their nature strive to be consistent with previous or reported behaviours to avoid cognitive dissonance.
• Consensus: We often observe the behaviours of others to help us make decisions. This is because “a large majority of individuals are imitators rather than initiators and therefore make decisions only after observing the behaviours and consequences on those around them”.
• Authority: People defer to experts. Therefore, individuals are more likely to comply with a request when it is made by a person or people they perceived as possessing high levels of knowledge, wisdom or power.
• Liking: People can be easily influenced or persuaded by someone they like. Factors, such as similarity, praise and attractiveness can reliably increase the effectiveness of the liking strategy.
• Scarcity: People tend to place more value on things that are in short supply. This is due to the popular belief that less available options are of higher quality.
3.1.8 Social influence theories
Persuasive technologies based on social psychology theories would require the user to be able to compare their selves with other people. Fogg describes four social psychology theories that can be applied to persuasive technologies [73]:
• Social facilitation: People are more likely to perform a well-learned target behaviour if they know they are being observed via computing technology, or if they can discern via technology that others are performing the behaviour along with them.
• Social comparison: People will have a greater motivation to perform a target behaviour if they are given information, via computing technology, about how their performance compares with the performance of others, especially others who are similar to themselves.
• Social learning: A person will be more motivated to perform a target behaviour if he or she can use computing technology to observe others performing the behaviour and being rewarded for it.
• Conformity: People tend to alter attitudes and behaviours to match the expectations, attitudes and behaviours of others, and more precisely of their “in-group” (i.e. a social group to which someone psychologically identifies as being a member).
D5.1 – V0.4
Page 41
3.2 Persuasive design
Persuasive technology employs principles of persuasive design. It is considered an attempt to consciously deal with the issue of persuasion, based on understanding the persuasive dimension underlying the dialogue between objects and users [93].
In the following subsections we will describe the three main methodologies for the development of persuasive systems, which are the Functional Triad (3.2.1), the Persuasive Systems Design model (3.2.2) and Design with Intent (3.2.3).
3.2.1 Functional Triad
According to Fogg , the functional triad is a framework that illustrates the three roles computing technology can play: tools, media and social actor [73]. As tools, persuasive technologies make users’ activities easier or more efficient to do, e.g. by performing calculations or providing guidance which lead users through processes in a step-by-step manner. As media, persuasive technologies provide interactive and engaging experiences. Finally, as social actors, persuasive technologies attempt to mimic a living entity e.g. by providing feedback or social support.
Fogg has identified seven types of persuasive technology tools:
Reduction (‘sequencing’): simplifying a behaviour or activity, by reducing it to a few simple steps. Reduction increase a person’s self-efficacy, or a person’s belief in his/her ability to perform a specific behaviour. This provides positive experiences to users, who might also perform it more frequently.
Tunneling: guiding users through a predetermined sequence of actions or events, step by step. For users, tunneling makes it easier to go through a process, and its use provides opportunities to persuade along the way. Lastly, it is also effective because people value consistency.
Tailoring: providing information relevant to the user’s needs, interest, use context or other relevant factors relevant to the individual. Tailored information is more persuasive than generic information in changing attitudes and/or behaviours.
Suggestion: offering hints, instructions or options for users at the most opportune moment, The six principles of opportune moment are when people are in good mood, when they find their current world view no longer makes sense, when they can take action on immediately, when they feel indebted because of a favour they have received, a mistake they made, or a request they recently denied. (‘Kairos’).
Self-monitoring: enabling users monitor themselves to modify their attitudes or behaviours to achieve a predetermined goal. Ideally, self-monitoring technologies work in real-time, offering users an ongoing data and feedback about their progress.
Surveillance (‘observation’): allowing one party to monitor the behaviour of another to modify behaviour in a specific way. To effectively change behaviours, individuals must be aware of the fact that they are observed.
Conditioning (‘shaping’): encouraging or discouraging behaviour with the use of rewarding or punishing them. Depending on the consequences of a behaviour, the instances will either increase or decrease and self-efficacy will be strengthened. To
D5.1 – V0.4
Page 42
be effective, reinforcements should immediately follow the performance of a target behaviour.
Technology as a medium can be used to persuade users to change behaviour through simulations. Computer simulations can create experiences that mimic experiences in the real world or they can create hypothetical worlds that are experienced as “real”. There are three classes of simulations that are relevant to persuasive technologies, based on what the user actually experiences:
Simulated cause-and-effect scenarios: enabling users to observe immediately the link between cause and effect, in order to gain insight into the likely consequences of their attitudes or behaviours in vivid and credible ways.
Simulated environments: creating situations that reward and motivate people for a target behaviour; allow users to practice a target behaviour; control exposure to new or frightening situations and facilitating role-playing, adopting another person’s perspective.
Simulated objects: object simulations that fit into the context of a person’s everyday life and are less dependent on imagination or suspension of disbelief. This approach enables users to experience the impact of certain behaviours in the context of real life and motivate behaviour or attitude change.
Technology as a social actor intends to provide social cues that elicit social responses from their human users, i.e., animated characters having facial expressions that convey emotions. When perceived as social actors, technology can leverage principles of social influence to motivate and persuade. Fogg proposes five primary types of social cues causing people to make inferences about social presence [73]:
Physical cues: computer products can convey physical cues through eyes a mouth movement and other physical characteristics. However, more attractive a technology is (interface or hardware) has a greater persuasive power than unattractive technology.
Psychological cues: leading people to infer that a product has emotions, preferences, motivations and personality, e.g. in text messages conveying empathy, onscreen icons portraying emotions or cues portraying personality. In that regard, similarity is a powerful persuasion principle: people we think are similar to us can motivate and persuade us more easily than people who are not similar to us in some way. In general, the greater the similarity, the greater the potential to persuade.
Language: persuading people by offering praise via words, images, symbols or sounds or by speaking to them directly.
Social dynamics: using ‘unwritten rules’ for interacting with each other, e.g. reciprocity.
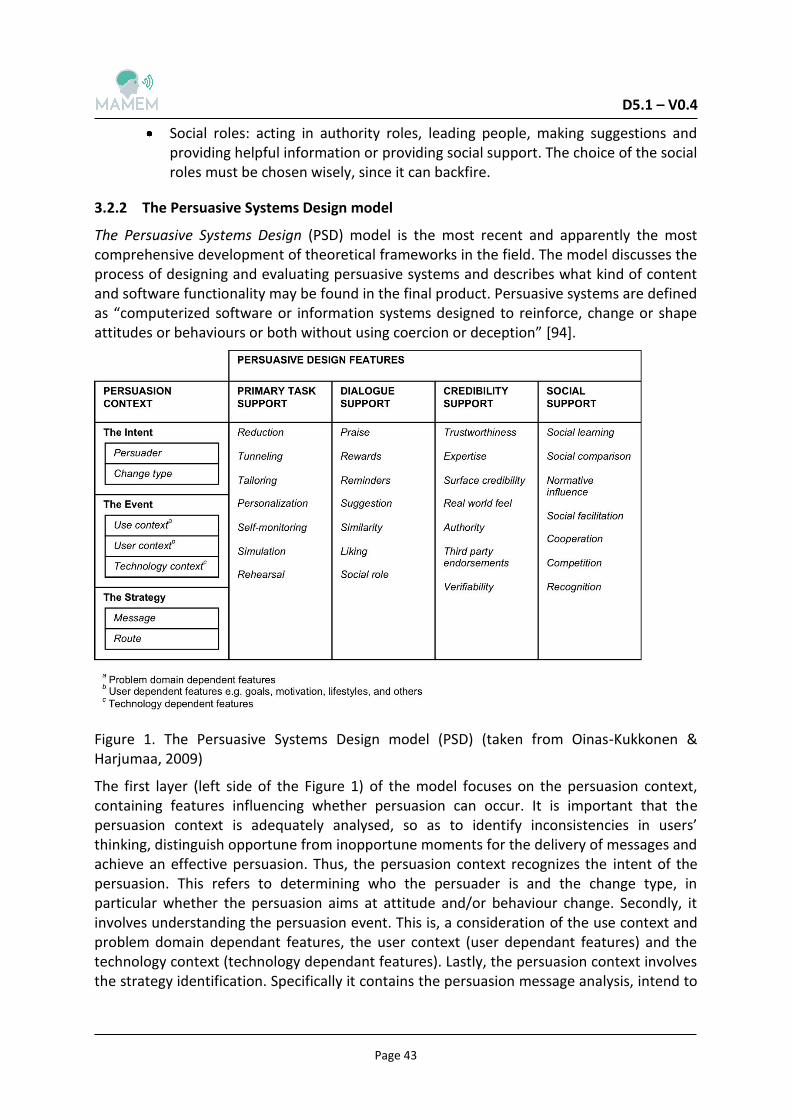
D5.1 – V0.4
Page 43
Social roles: acting in authority roles, leading people, making suggestions and providing helpful information or providing social support. The choice of the social roles must be chosen wisely, since it can backfire.
3.2.2 The Persuasive Systems Design model
The Persuasive Systems Design (PSD) model is the most recent and apparently the most comprehensive development of theoretical frameworks in the field. The model discusses the process of designing and evaluating persuasive systems and describes what kind of content and software functionality may be found in the final product. Persuasive systems are defined as “computerized software or information systems designed to reinforce, change or shape attitudes or behaviours or both without using coercion or deception” [94].
Figure 1. The Persuasive Systems Design model (PSD) (taken from Oinas-Kukkonen & Harjumaa, 2009)
The first layer (left side of the Figure 1) of the model focuses on the persuasion context, containing features influencing whether persuasion can occur. It is important that the persuasion context is adequately analysed, so as to identify inconsistencies in users’ thinking, distinguish opportune from inopportune moments for the delivery of messages and achieve an effective persuasion. Thus, the persuasion context recognizes the intent of the persuasion. This refers to determining who the persuader is and the change type, in particular whether the persuasion aims at attitude and/or behaviour change. Secondly, it involves understanding the persuasion event. This is, a consideration of the use context and problem domain dependant features, the user context (user dependant features) and the technology context (technology dependant features). Lastly, the persuasion context involves the strategy identification. Specifically it contains the persuasion message analysis, intend to
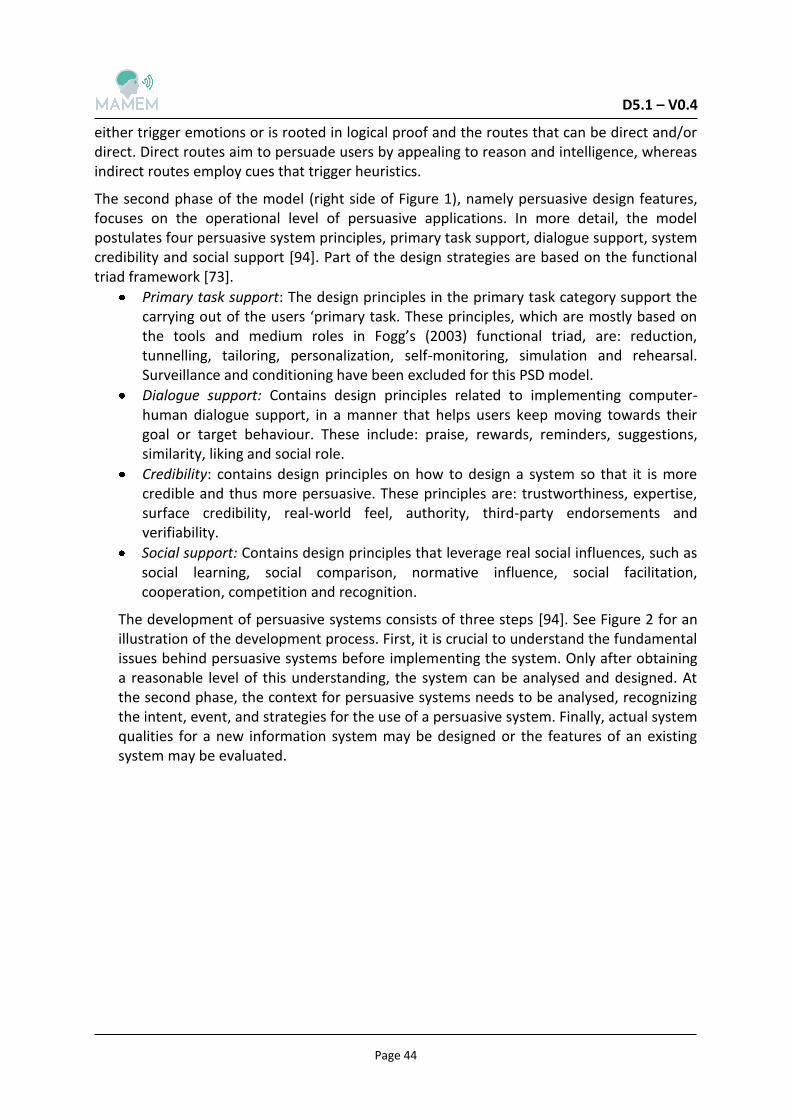
D5.1 – V0.4
Page 44
either trigger emotions or is rooted in logical proof and the routes that can be direct and/or direct. Direct routes aim to persuade users by appealing to reason and intelligence, whereas indirect routes employ cues that trigger heuristics.
The second phase of the model (right side of Figure 1), namely persuasive design features, focuses on the operational level of persuasive applications. In more detail, the model postulates four persuasive system principles, primary task support, dialogue support, system credibility and social support [94]. Part of the design strategies are based on the functional triad framework [73].
Primary task support: The design principles in the primary task category support the carrying out of the users ‘primary task. These principles, which are mostly based on the tools and medium roles in Fogg’s (2003) functional triad, are: reduction, tunnelling, tailoring, personalization, self-monitoring, simulation and rehearsal. Surveillance and conditioning have been excluded for this PSD model.
Dialogue support: Contains design principles related to implementing computer-human dialogue support, in a manner that helps users keep moving towards their goal or target behaviour. These include: praise, rewards, reminders, suggestions, similarity, liking and social role.
Credibility: contains design principles on how to design a system so that it is more credible and thus more persuasive. These principles are: trustworthiness, expertise, surface credibility, real-world feel, authority, third-party endorsements and verifiability.
Social support: Contains design principles that leverage real social influences, such as social learning, social comparison, normative influence, social facilitation, cooperation, competition and recognition.
The development of persuasive systems consists of three steps [94]. See Figure 2 for an illustration of the development process. First, it is crucial to understand the fundamental issues behind persuasive systems before implementing the system. Only after obtaining a reasonable level of this understanding, the system can be analysed and designed. At the second phase, the context for persuasive systems needs to be analysed, recognizing the intent, event, and strategies for the use of a persuasive system. Finally, actual system qualities for a new information system may be designed or the features of an existing system may be evaluated.
D5.1 – V0.4
Page 45
Figure 2. Phases in Persuasive Systems Development (taken from Oinas-Kukkonen2009)
3.2.3 Design with Intent
Lockton et al., 2010 developed a collection of design patterns for discovering the interactions between design and people’s behaviour, both in digital and physical settings [95]. The toolkit is named “Design With Intent” and includes 101 principles that are structured under eight different “lenses”. These strategic designs rely on deep psychological principles and intent to influence or result in certain user behaviour. This collection was created based on the notion that all design inevitably affect behaviour. As Lockton (2010) said: “Whether we mean to do it or not, it's going to happen, so we might as well get good at it — and understand when it's being done to us.”
“Design With Intent” toolkit contains the following eight lenses:
Architectural: drawing on techniques used to influence user behaviour in architecture, urban planning and related disciplines;
Error-proofing: treating deviations from the target behaviour as ‘errors’ which design can help avoid, either by making it easier for users to work without making errors, or by making errors impossible in the first place
Interaction: brings together some of the most common design elements of interfaces where users' interactions with the system affect how their behaviour is influenced;
Ludic: includes a number of techniques for influencing user behaviour that can be derived from games and other ‘playful’ interactions;
Perceptual: Ways how users’ perceptions of patterns and meaning can influence their behaviour;
Cognitive: Principles drawing on research in behavioural economics and cognitive psychology looking at how people make decisions, and how this is affected by “heuristics” and “biases”;
Machiavellian: Design patterns “forcing” the user to change behaviour such as lock-ins or planned obsolescence;

D5.1 – V0.4
Page 46
Security: It represents a ‘security’ worldview i.e. that undesired user behaviour is something to deter and/or prevent.
D5.1 – V0.4
Page 47
4
In view of developing a MAMEM prototype, a selection of persuasive design strategies and techniques should be made as inventoried in the previous chapter. The main criterion for this selection is to choose those techniques that are more likely to persuade the target groups to use the MAMEM system for managing, authoring and sharing multimedia context.
The core goal of this task is to influence user motivation, and make patients willing to use the technology and keep on using it. The pilot trials are divided in two phases: phase I refers to patients testing the platform in a controlled environment (patient centres) to address its feasibility and usability; and phase II, during which, participants are encouraged to use the MAMEM system in their home environments for a fixed period, in order to assess the impact of their multimedia authoring in a less control setting. Hence, the overall desired outcome for the three target groups (SCI, PD, and NMD) is twofold:
User acceptance and training engagement of the MAMEM system; Keep using MAMEM to increase social participation in: a) Social network activities, b)
Digital productivity.
The next subsection describe the development of the persuasive strategies to realize the first objective (4.1) while the following subsections refer to the selection of persuasive strategies to accomplish the second objective (4.2, 4.3 and 4.4).
4.1 Developing persuasive strategies for Phase I: user acceptance and training
Phase I of the clinical trials will include training with EEG element, training with gaze element and training with both elements. It is divided in two parts: the first part includes the introduction to the platform, putting it on the participants and training them with basic tasks, such as cursor, windows and keyboard basic operations. The second part of the training refers to multimedia managing, authoring and sharing using dictated tasks like writing a mail and photo editing. To come to a selection of the techniques to be incorporated in the system during the first phase, we applied Intervention mapping (IM), a framework for developing and implementing health interventions [96].In the next subsections, we discuss the IM framework in more detail.
4.1.1 Intervention Mapping framework
Intervention mapping (IM) is a framework for the development of theory and evidence based health promotion programmes. It provides guidelines and tools for the selection of theoretical foundations and underpinnings of health promoting programmes, for the application of theory and for the translation of theory in actual programme materials and activities. Past projects demonstrated that IM allows intervention developers to successfully identify 1) behavioural and environmental determinants affecting target health problems 2) the most appropriate methods and strategies to address the identified determinants.
The IM framework guides the developer through iterative steps, as shown in the Figure 3 below.
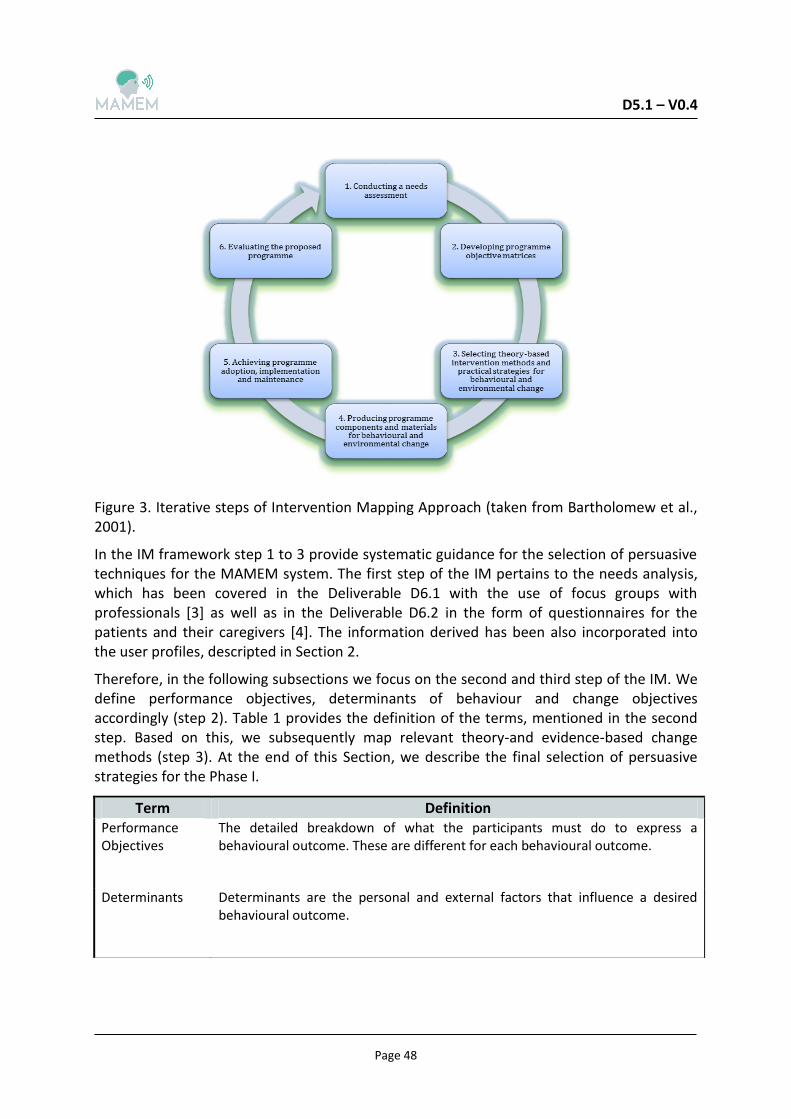
D5.1 – V0.4
Page 48
Figure 3. Iterative steps of Intervention Mapping Approach (taken from Bartholomew et al., 2001).
In the IM framework step 1 to 3 provide systematic guidance for the selection of persuasive techniques for the MAMEM system. The first step of the IM pertains to the needs analysis, which has been covered in the Deliverable D6.1 with the use of focus groups with professionals [3] as well as in the Deliverable D6.2 in the form of questionnaires for the patients and their caregivers [4]. The information derived has been also incorporated into the user profiles, descripted in Section 2.
Therefore, in the following subsections we focus on the second and third step of the IM. We define performance objectives, determinants of behaviour and change objectives accordingly (step 2). Table 1 provides the definition of the terms, mentioned in the second step. Based on this, we subsequently map relevant theory-and evidence-based change methods (step 3). At the end of this Section, we describe the final selection of persuasive strategies for the Phase I.
Term Definition Performance Objectives
The detailed breakdown of what the participants must do to express a behavioural outcome. These are different for each behavioural outcome.
Determinants Determinants are the personal and external factors that influence a desired behavioural outcome.
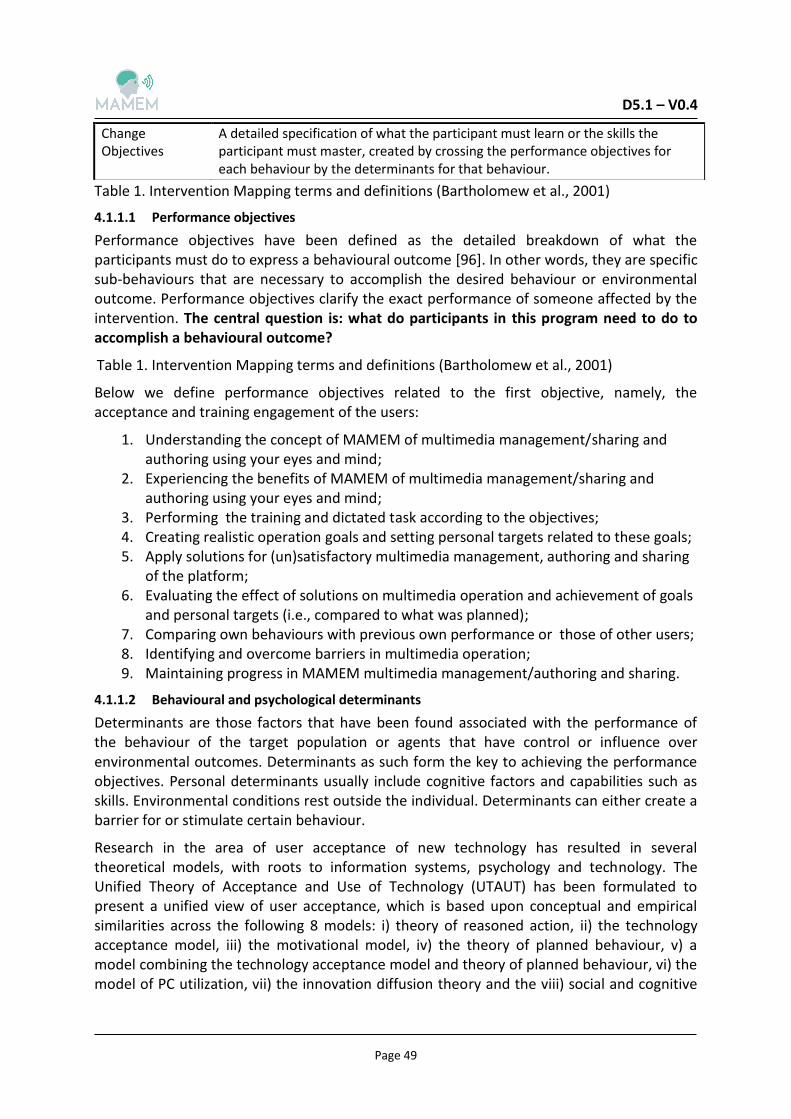
D5.1 – V0.4
Page 49
Table 1. Intervention Mapping terms and definitions (Bartholomew et al., 2001)
4.1.1.1 Performance objectives
Performance objectives have been defined as the detailed breakdown of what the participants must do to express a behavioural outcome [96]. In other words, they are specific sub-behaviours that are necessary to accomplish the desired behaviour or environmental outcome. Performance objectives clarify the exact performance of someone affected by the intervention. The central question is: what do participants in this program need to do to accomplish a behavioural outcome?
Below we define performance objectives related to the first objective, namely, the acceptance and training engagement of the users:
1. Understanding the concept of MAMEM of multimedia management/sharing and authoring using your eyes and mind;
2. Experiencing the benefits of MAMEM of multimedia management/sharing and authoring using your eyes and mind;
3. Performing the training and dictated task according to the objectives; 4. Creating realistic operation goals and setting personal targets related to these goals; 5. Apply solutions for (un)satisfactory multimedia management, authoring and sharing
of the platform; 6. Evaluating the effect of solutions on multimedia operation and achievement of goals
and personal targets (i.e., compared to what was planned); 7. Comparing own behaviours with previous own performance or those of other users; 8. Identifying and overcome barriers in multimedia operation; 9. Maintaining progress in MAMEM multimedia management/authoring and sharing.
4.1.1.2 Behavioural and psychological determinants
Determinants are those factors that have been found associated with the performance of the behaviour of the target population or agents that have control or influence over environmental outcomes. Determinants as such form the key to achieving the performance objectives. Personal determinants usually include cognitive factors and capabilities such as skills. Environmental conditions rest outside the individual. Determinants can either create a barrier for or stimulate certain behaviour.
Research in the area of user acceptance of new technology has resulted in several theoretical models, with roots to information systems, psychology and technology. The Unified Theory of Acceptance and Use of Technology (UTAUT) has been formulated to present a unified view of user acceptance, which is based upon conceptual and empirical similarities across the following 8 models: i) theory of reasoned action, ii) the technology acceptance model, iii) the motivational model, iv) the theory of planned behaviour, v) a model combining the technology acceptance model and theory of planned behaviour, vi) the model of PC utilization, vii) the innovation diffusion theory and the viii) social and cognitive
Change Objectives
A detailed specification of what the participant must learn or the skills the participant must master, created by crossing the performance objectives for each behaviour by the determinants for that behaviour.
Table 1. Intervention Mapping terms and definitions (Bartholomew et al., 2001)
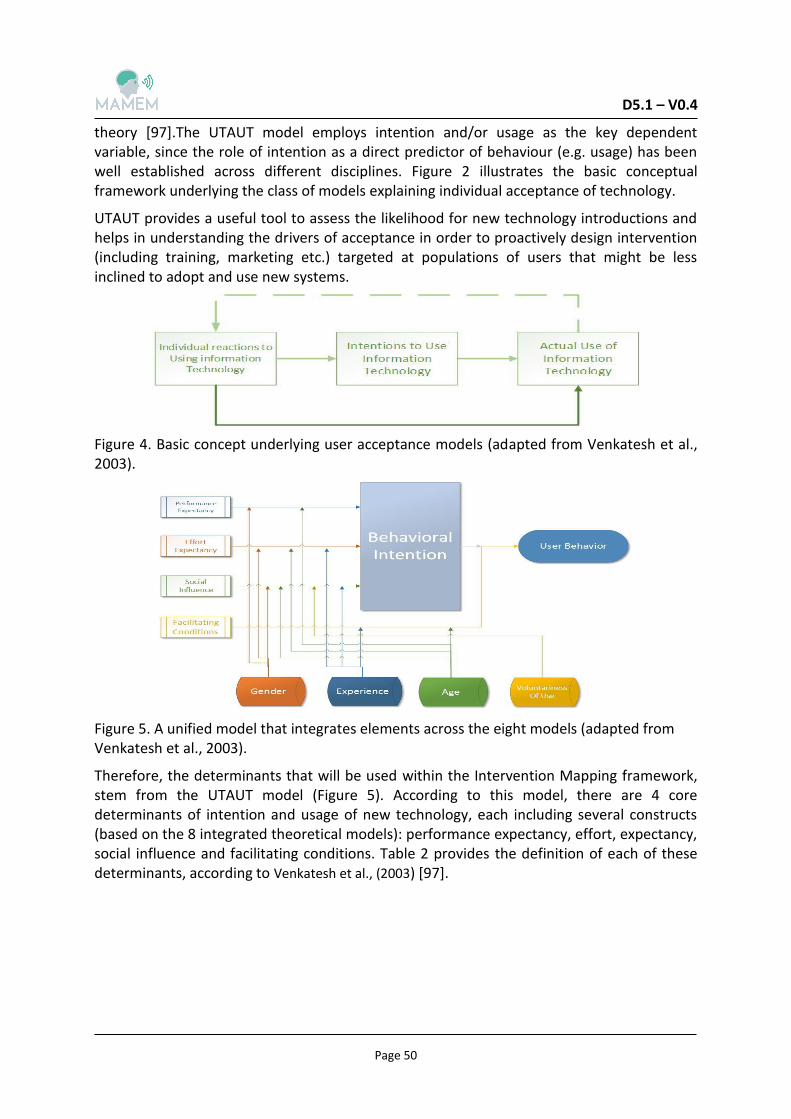
D5.1 – V0.4
Page 50
theory [97].The UTAUT model employs intention and/or usage as the key dependent variable, since the role of intention as a direct predictor of behaviour (e.g. usage) has been well established across different disciplines. Figure 2 illustrates the basic conceptual framework underlying the class of models explaining individual acceptance of technology.
UTAUT provides a useful tool to assess the likelihood for new technology introductions and helps in understanding the drivers of acceptance in order to proactively design intervention (including training, marketing etc.) targeted at populations of users that might be less inclined to adopt and use new systems.
Figure 4. Basic concept underlying user acceptance models (adapted from Venkatesh et al., 2003).
Figure 5. A unified model that integrates elements across the eight models (adapted from Venkatesh et al., 2003).
Therefore, the determinants that will be used within the Intervention Mapping framework, stem from the UTAUT model (Figure 5). According to this model, there are 4 core determinants of intention and usage of new technology, each including several constructs (based on the 8 integrated theoretical models): performance expectancy, effort, expectancy, social influence and facilitating conditions. Table 2 provides the definition of each of these determinants, according to Venkatesh et al., (2003) [97].
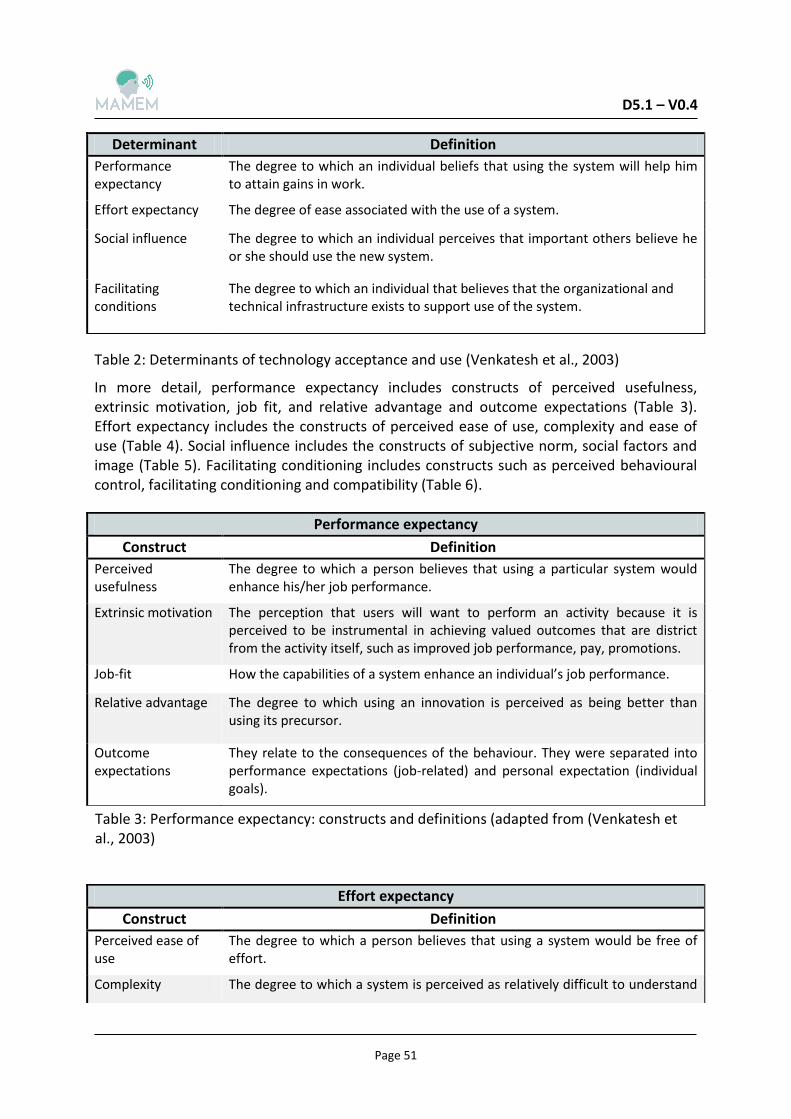
D5.1 – V0.4
Page 51
In more detail, performance expectancy includes constructs of perceived usefulness, extrinsic motivation, job fit, and relative advantage and outcome expectations (Table 3). Effort expectancy includes the constructs of perceived ease of use, complexity and ease of use (Table 4). Social influence includes the constructs of subjective norm, social factors and image (Table 5). Facilitating conditioning includes constructs such as perceived behavioural control, facilitating conditioning and compatibility (Table 6).
Determinant Definition
Performance expectancy
The degree to which an individual beliefs that using the system will help him to attain gains in work.
Effort expectancy The degree of ease associated with the use of a system.
Social influence The degree to which an individual perceives that important others believe he or she should use the new system.
Facilitating conditions
The degree to which an individual that believes that the organizational and technical infrastructure exists to support use of the system.
Table 2: Determinants of technology acceptance and use (Venkatesh et al., 2003)
Performance expectancy
Construct Definition
Perceived usefulness
The degree to which a person believes that using a particular system would enhance his/her job performance.
Extrinsic motivation The perception that users will want to perform an activity because it is perceived to be instrumental in achieving valued outcomes that are district from the activity itself, such as improved job performance, pay, promotions.
Job-fit How the capabilities of a system enhance an individual’s job performance.
Relative advantage The degree to which using an innovation is perceived as being better than using its precursor.
Outcome expectations
They relate to the consequences of the behaviour. They were separated into performance expectations (job-related) and personal expectation (individual goals).
Table 3: Performance expectancy: constructs and definitions (adapted from (Venkatesh et al., 2003)
Effort expectancy
Construct Definition
Perceived ease of use
The degree to which a person believes that using a system would be free of effort.
Complexity The degree to which a system is perceived as relatively difficult to understand
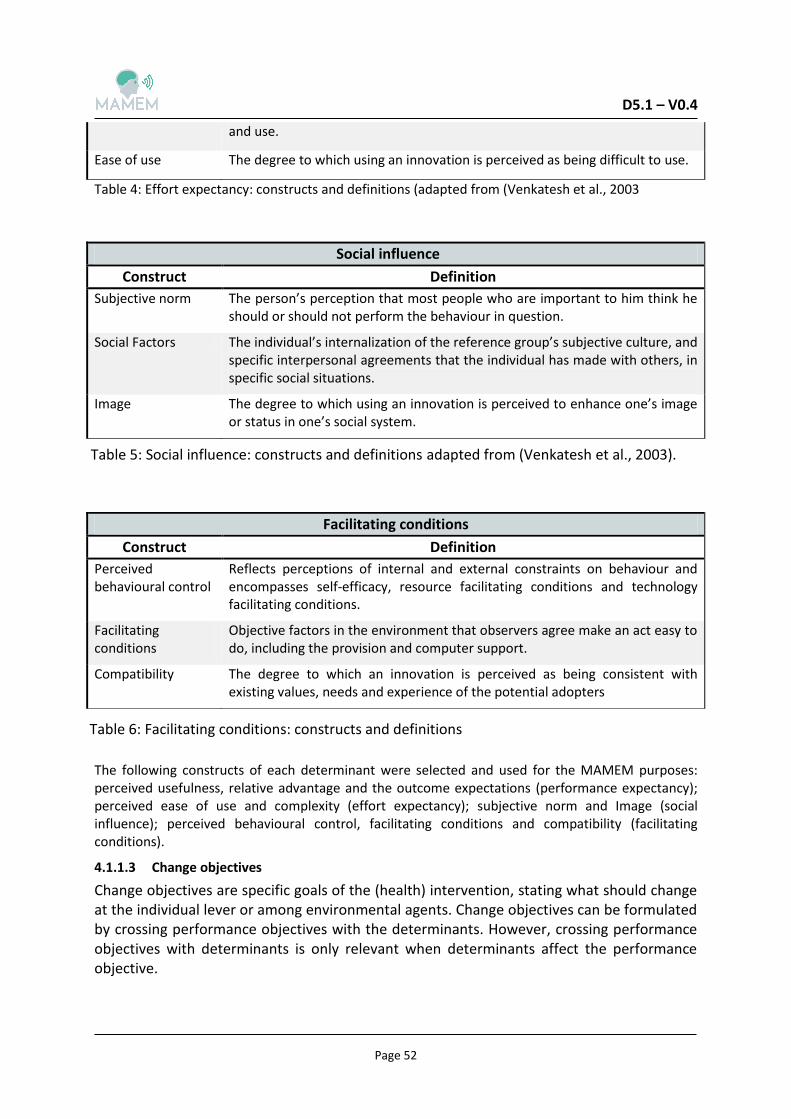
D5.1 – V0.4
Page 52
Table 4: Effort expectancy: constructs and definitions (adapted from (Venkatesh et al., 2003
The following constructs of each determinant were selected and used for the MAMEM purposes: perceived usefulness, relative advantage and the outcome expectations (performance expectancy); perceived ease of use and complexity (effort expectancy); subjective norm and Image (social influence); perceived behavioural control, facilitating conditions and compatibility (facilitating conditions).
4.1.1.3 Change objectives
Change objectives are specific goals of the (health) intervention, stating what should change at the individual lever or among environmental agents. Change objectives can be formulated by crossing performance objectives with the determinants. However, crossing performance objectives with determinants is only relevant when determinants affect the performance objective.
and use.
Ease of use The degree to which using an innovation is perceived as being difficult to use.
Social influence
Construct Definition
Subjective norm The person’s perception that most people who are important to him think he should or should not perform the behaviour in question.
Social Factors The individual’s internalization of the reference group’s subjective culture, and specific interpersonal agreements that the individual has made with others, in specific social situations.
Image The degree to which using an innovation is perceived to enhance one’s image or status in one’s social system.
Table 5: Social influence: constructs and definitions adapted from (Venkatesh et al., 2003).
Facilitating conditions
Construct Definition
Perceived behavioural control
Reflects perceptions of internal and external constraints on behaviour and encompasses self-efficacy, resource facilitating conditions and technology facilitating conditions.
Facilitating conditions
Objective factors in the environment that observers agree make an act easy to do, including the provision and computer support.
Compatibility The degree to which an innovation is perceived as being consistent with existing values, needs and experience of the potential adopters
Table 6: Facilitating conditions: constructs and definitions
D5.1 – V0.4
Page 53
Appendix 2 lists the behaviour change objectives, derived from performance objectives and determinants.
4.1.2 Selected persuasion strategies
After the creation of the behaviour change matrix, the next step was the mapping of strategies for each change objective/determinant. The mapping involves selecting strategies that have been proven effective to realize the defined change objectives and describing how they are practically applied. Based on this, a plethora of persuasive strategies was selected for the MAMEM system.
In total, 7 change objectives were selected as candidates for the MAMEM prototype:
1. Feel that it is easy to become skilful at using the system 2. Feel that the training is fun 3. Know how to state clear goals and tasks 4. Compare performance level with what other users do 5. Demonstrate ability to monitor own operation activity (i.e. training tasks) 6. Ask for positive reinforcement on system operation successes 7. Be able to identify barriers in own performance and demonstrate how to overcome
them Since each change objective is related to one or more behaviour change theories, multiple persuasive technologies might be appropriate. For each change objective selected, several persuasive strategies were chosen and are described in the table 7. Tailoring and tunnelling are the most common persuasive strategies and tools selected. By combining different persuasive technologies (e.g. monitoring progress and rewarding user with positive feedback) we believe that we would enlarge the persuasive impact of the system and successfully motivate our target groups to operate multimedia management, authoring and sharing using the MAMEM system.
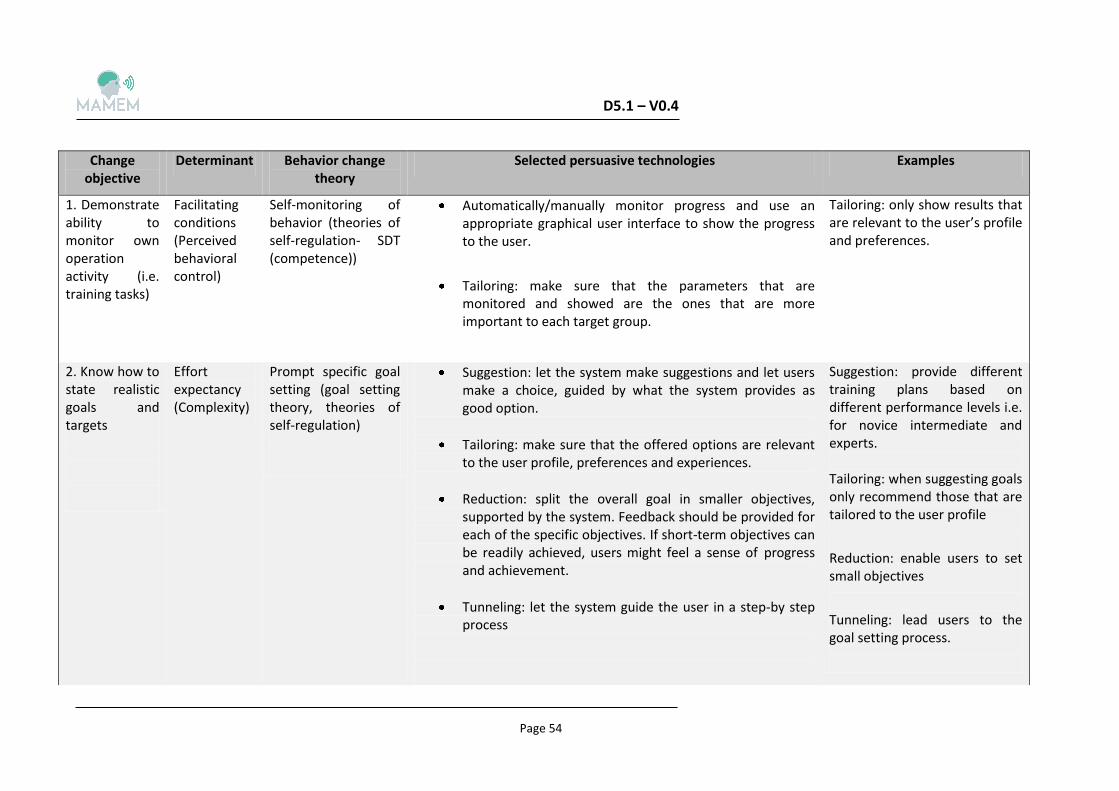
D5.1 – V0.4
Page 54
Change objective
Determinant Behavior change theory
Selected persuasive technologies Examples
1. Demonstrate ability to monitor own operation activity (i.e. training tasks)
Facilitating conditions (Perceived behavioral control)
Self-monitoring of behavior (theories of self-regulation- SDT (competence))
Automatically/manually monitor progress and use an appropriate graphical user interface to show the progress to the user.
Tailoring: make sure that the parameters that are monitored and showed are the ones that are more important to each target group.
Tailoring: only show results that are relevant to the user’s profile and preferences.
2. Know how to state realistic goals and targets
Effort expectancy (Complexity)
Prompt specific goal setting (goal setting theory, theories of self-regulation)
Suggestion: let the system make suggestions and let users make a choice, guided by what the system provides as good option.
Tailoring: make sure that the offered options are relevant to the user profile, preferences and experiences.
Reduction: split the overall goal in smaller objectives, supported by the system. Feedback should be provided for each of the specific objectives. If short-term objectives can be readily achieved, users might feel a sense of progress and achievement.
Tunneling: let the system guide the user in a step-by step process
Suggestion: provide different training plans based on different performance levels i.e. for novice intermediate and experts. Tailoring: when suggesting goals only recommend those that are tailored to the user profile
Reduction: enable users to set small objectives
Tunneling: lead users to the goal setting process.
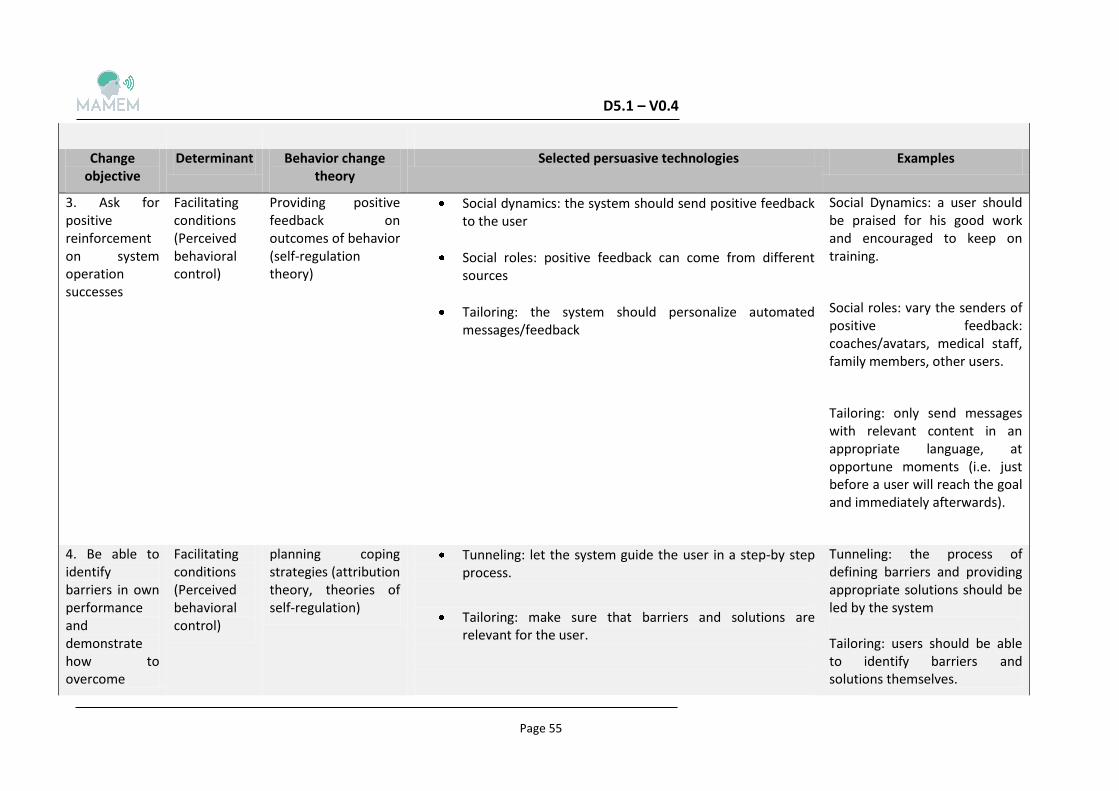
D5.1 – V0.4
Page 55
Change objective
Determinant Behavior change theory
Selected persuasive technologies Examples
3. Ask for positive reinforcement on system operation successes
Facilitating conditions (Perceived behavioral control)
Providing positive feedback on outcomes of behavior (self-regulation theory)
Social dynamics: the system should send positive feedback to the user
Social roles: positive feedback can come from different sources
Tailoring: the system should personalize automated messages/feedback
Social Dynamics: a user should be praised for his good work and encouraged to keep on training.
Social roles: vary the senders of positive feedback: coaches/avatars, medical staff, family members, other users.
Tailoring: only send messages with relevant content in an appropriate language, at opportune moments (i.e. just before a user will reach the goal and immediately afterwards).
4. Be able to identify barriers in own performance and demonstrate how to overcome
Facilitating conditions (Perceived behavioral control)
planning coping strategies (attribution theory, theories of self-regulation)
Tunneling: let the system guide the user in a step-by step process.
Tailoring: make sure that barriers and solutions are relevant for the user.
Tunneling: the process of defining barriers and providing appropriate solutions should be led by the system Tailoring: users should be able to identify barriers and solutions themselves.
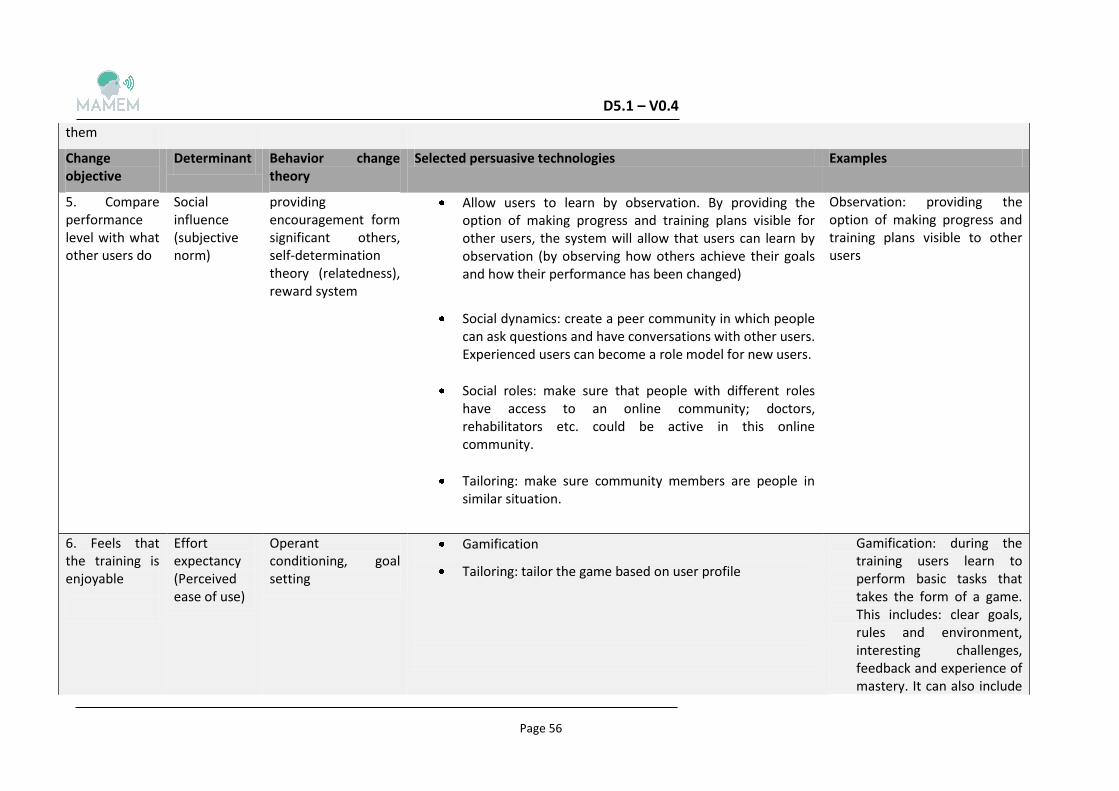
D5.1 – V0.4
Page 56
them
Change objective
Determinant Behavior change theory
Selected persuasive technologies Examples
5. Compare performance level with what other users do
Social influence (subjective norm)
providing encouragement form significant others, self-determination theory (relatedness), reward system
Allow users to learn by observation. By providing the option of making progress and training plans visible for other users, the system will allow that users can learn by observation (by observing how others achieve their goals and how their performance has been changed)
Social dynamics: create a peer community in which people can ask questions and have conversations with other users. Experienced users can become a role model for new users.
Social roles: make sure that people with different roles have access to an online community; doctors, rehabilitators etc. could be active in this online community.
Tailoring: make sure community members are people in similar situation.
Observation: providing the option of making progress and training plans visible to other users
6. Feels that the training is enjoyable
Effort expectancy (Perceived ease of use)
Operant conditioning, goal setting
Gamification
Tailoring: tailor the game based on user profile
Gamification: during the training users learn to perform basic tasks that takes the form of a game. This includes: clear goals, rules and environment, interesting challenges, feedback and experience of mastery. It can also include
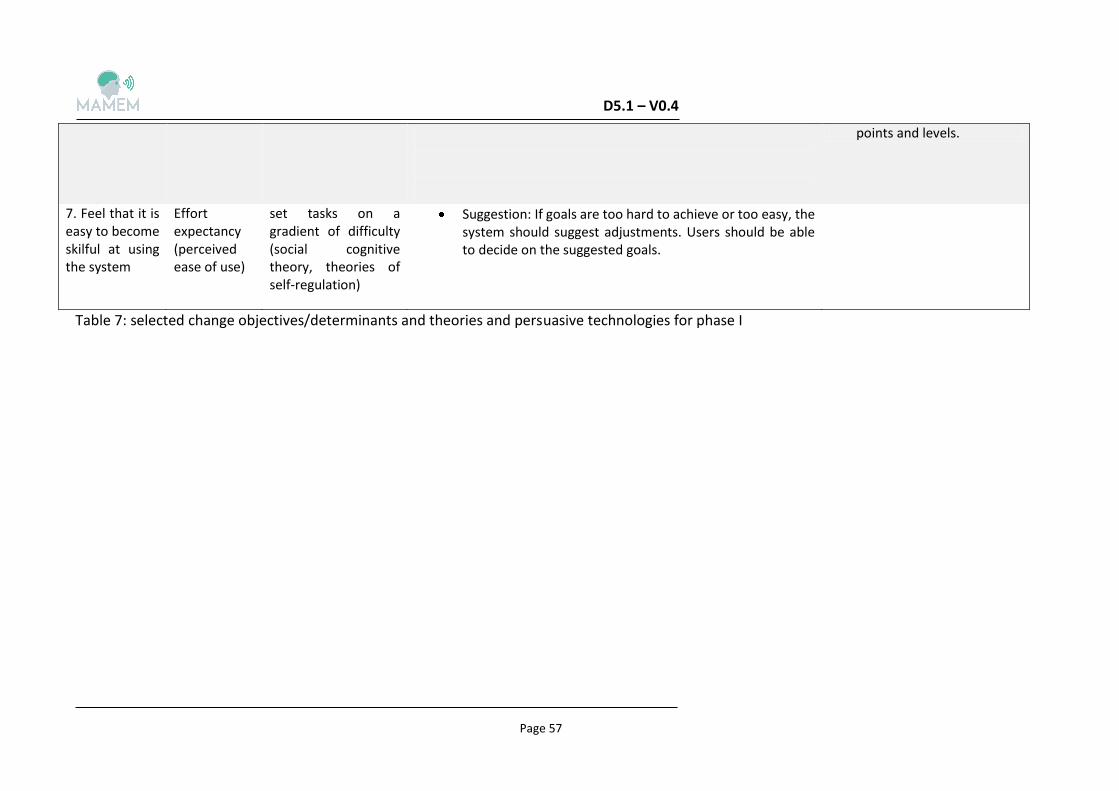
D5.1 – V0.4
Page 57
points and levels.
7. Feel that it is easy to become skilful at using the system
Effort expectancy (perceived ease of use)
set tasks on a gradient of difficulty (social cognitive theory, theories of self-regulation)
Suggestion: If goals are too hard to achieve or too easy, the system should suggest adjustments. Users should be able to decide on the suggested goals.
Table 7: selected change objectives/determinants and theories and persuasive technologies for phase I
D5.1 – V0.4
Page 58
4.2 Developing persuasive strategies for Phase II: Social inclusion
In the second phase of the clinical trials of MAMEM, the participants will go over the same protocol as in the first phase, but this time in their home environments. The platform will be given to them for a fixed period in which they will be encouraged to use it. The core objective is to assess the impact of the MAMEM system on multimedia management, authoring and sharing in less controlled settings. In this phase, social network activities (i.e. social media activities) and digital productivity (i.e. online courses taken) are of primary importance.
Since the overall aim of the MAMEM project is to increase users’ potential in social inclusion, strategies are needed, as motivators, for the users to continue using the system and stimulate their online social participation. The desired outcome of the second phase is different from that of the first phase and therefore, the IM framework is not applicable; here, the overall goal is broader and it is pointless to predefine objectives and determinants of behaviour of potential online activities. All in all, a different persuasive approach needs to be designed.
In the following subsections, we refer to some theories of social psychology to be used as the foundations of the strategies to motivate user’s online social participation and contributions (4.2.1). Next we describe the selected persuasive strategy of hierarchical memberships (4.3) and lastly, present our proposed motivation strategy to accomplish the goal of social inclusion for MAMEM (4.4).
4.2.1 Reciprocation theory
Reciprocation is a basic norm of human society. In states that appropriate rewards are necessary, when individuals are invited to do something for someone else [92]. Since MAMEM’s goal is individuals to keep using the system, users should benefit from their participation. One overly used technique is to match rewards with the participation level. Simply put, the amount of reward a user gets should be contingent on his/her activity level. At this point, two crucial questions are important: how to precisely measure users’ participation and activity and what the reward should be. If the rewards are perceived as unimportant, it can affect users’ motivation to continue using the system.
4.2.2 Consistency
According to the consistency theory, making initial public commitments increase the probability that subsequent actions will be consistent with such commitments [98]. Forming this theory for MAMEM, users could be encouraged to make an initial commitment of their online social participation. Thereinafter, they will be reminded of the commitment whenever they do not act in accordance to this commitment. Based on the theory, the user, in an effort to reduce his/her cognitive dissonance, will adjust his/her behaviour accordingly. The central issue here is how to persuade the user to make a public commitment.
D5.1 – V0.4
Page 59
4.2.3 Social validation
According to social validation theory, people often choose what to do in a situation by observing the actions of others. If a large percentage of people are in favour of a certain idea, many others would tend to follow their way [92]. Moreover, people who share some short of similarity, can influence the behaviour one another. Therefore, it is likely to persuade users to increase their online participation, by making known that many others, just like them, performed the same and got rewarded for this.
4.2.4 Theories of discrete emotions
Discrete emotions are universal emotions such as fear, anger, sadness and joy. They have been defined as “those emotions that have unique appraisals patterns, motivational functions and behavioural associations” [99]. For MAMEM, the theory of fear will be primarily used. According to the theory of fear, a person can feel fear when he/she find himself/herself in a situation of perceived threat, directed either to the self or his/her properties. This fear of loss increases the appeal of incoming messages, particularly those enclosing reassuring information [99]. An interpretation of the theory to our motivation strategy could involve provoking fear to the users; for example by threating that they may lose some of their privileges. Afterwards, they are presented with the information about how to prevail this issue. As a consequence, the persuasiveness of the information is enhanced and a user becomes more active.
4.3 Selected persuasive strategy: hierarchical memberships
The core motivation strategy here is to introduce of a set of hierarchical memberships into the system. Users can be given different memberships based on to their levels of online activity. The more active a user is, the higher his/her membership level is. The three issues that are explored in the below subsections pertain to the selection of measuring activity indicators (4.3.1), the membership decision (4.3.2) and the selected rewards for each group (4.3.3). Lastly, subsection 4.4 describes a detailed example of how the selected persuasive strategy could be applied to the MAMEM system.
4.3.1 Selection of measuring activity indicators
In accordance with the questionnaire analysis, described in the Deliverable D6.2 [4], we expect the users to engage in the following four social activities that have been rated as the most important aspects of computer use categories for all patient groups:
1. Social participation
2. Educational attainment
3. Work/employment potential
4. Recreation and information
Furthermore, each of these four categories contain various social indicators. For example, the interpersonal relationship category includes, among other, increase of online friends and amount of messages sent. A very important aspect here, is that the amount of indicators (shown to the users) should not be a large and should also be concrete and easy for the users to understand (so as to know how to match their activity in accordance with them).

D5.1 – V0.4
Page 60
Since these will be the target behaviours for each of the four categories careful consideration is needed in their selection.
Another essential issue is that users of each of the three target groups have different needs and preferences for social inclusion that have to be taken into account. The feedback from questionnaires has pointed out that the three most important computer categories among the group of patients were:
a) SCI patients: productive activities and recreation, social participation, study/recreation and information
b) PD patients: communication, information, social participation
c) NMD patients: social participation, communication and recreation
Although some of the indicators can be chosen to apply to all three groups (such as ‘log on the system frequently’ and ‘stay online’) other indicators should be tailored to each of the three groups. This means that the indicators should reflect the most significant social indicators related to computer activities, which are important to the patient groups.
As a result, the core idea is that each group will be presented with different indicators to accomplish, according to groups’ preferences for online activities. For example, frequency of SNS use (e.g., Facebook, Twitter) could be a more relevant social indicator for NMD patients, while for PD patients, frequency of mail and skype use would have a higher importance. Based on this, our approach is the following: first, maintain separate numeric values for each user to represent his/her performance on each of the selected indicators per category. For example, a value “V1” may account for users’ frequency of social media use per time unit (e.g. one week), in the first category.
Moreover, these indicators can have the same or different weight. Since, the importance of the selected indicators for social inclusion can be different, different weights (i.e., W1, W2, W3) could be introduced per indicator. The weights could be again tailored per group; the activities that are more relevant to each group could be assigned with a higher value.
Although in most cases users’ activity can be measured accurately, there is a detail that deserves mentioning. We hope that users engage in all categories. In other words, they should not keep doing one of them and skip others. Therefore, we can put a ceiling value (Ci) for each criterion. If a user’s performance value of a certain activity is greater than the ceiling value of that activity, the weight for the excess part (Wi_excess) would be much less than the original one (Wi). The intent of introducing the ceiling values is to stimulate users to be active in four categories, with the same effort. It ensures that the users who always do one thing and ignore others would not get a high-level membership.
All in all, the four categories with the assigned (tailored) indicators that could measure the users’ social inclusion, with their assigned weights and celling value to determine their membership level.
D5.1 – V0.4
Page 61
4.3.2 Users’ membership decision
First of all, we should decide how many membership levels we should introduce to the system. If the number of the membership levels is too small the users’ activity would not be differentiated well. On the other hand, too many membership levels could be confusing for the users. Generally the number of the memberships should not be greater than six and not less than three. For the MAMEM we selected to rank the users in the system into three levels depending on the overall evaluation of their online activity: gold (first level) silver (middle level) and bronze (bottom level).
In general, becoming a gold member should be relatively more difficult, because gold users, representing the highest level of participation, are not easy to be stimulated further. According to the theory of discrete emotions, their only motivation is to try trying to maintain their memberships. It is intended to be relatively easier for users to be classified in the silver member category, because these users have the change chance to upgrade their membership and at the same time have the fear about being degraded. Both of two possibilities could become their motivation to increase their participation. In addition, according to the social validation theory, the fact that it will be visible for users to see participants who managed to be in the first two levels could bring a pressure and stimulation for the users in the bronze category (bottom).
4.3.3 Users’ rewards decision
When users have managed to upgrade their membership, it is really important to have them realize that the system offers some kind of reward for their active participation. Otherwise users would feel there is no meaningful reason to achieve a high membership level and their participation might decline.
What should be the reward for active users? To start with, the membership itself is a kind of reward if it becomes public. Since there is a limited numbers of MAMEM platforms to be distributed, they will be given to the users in a rotational process. Thus, the simultaneous and “live” comparison and visualization of the participants is impossible. However, users’ membership serves as kind of recognition when it becomes public and available for visualization by all users. Gold members would gain a high status and silver members would gain some social credits as well. Therefore, it should be highlighted to the users that the levels of their progress as well as membership they reached, would be visible on the interface to the subsequent users.
However, offering only this reward is not enough since not all users are motivated by status and social comparison. A basic rue rule of thumb is that the reward should deserve or outweigh the users ‘effort to upgrade their memberships. Consequently, a more “materialistic” reward could be introduced, such as providing better services for active users. The definition of better services should be what users really need in the system. Previous research rewarded users by altering media items such as sounds, background skin, or user avatar according to user’s performance.
However, users of the three groups have different needs, difficulties and requirements; that is why rewards have to be tailored to the group. Based on their status, we can reward the groups with some extra functionality which is highly attractive enough to them.

D5.1 – V0.4
Page 62
4.4 The motivation interface of MAMEM
The MAMEM system will introduce three memberships into the system: gold, silver and bronze. A user will be grouped into these three levels according to his/her activity, related to the selected social indicator. A graphical user interface shows the user’s membership. On the default panel when the user enters the program, a symbolic membership card is displayed, which clearly shows the user’s current membership level. If the user clicks on the card, a new window would pop up and show the user’s participation during the previous period of time (e.g. days, weeks). The window will describe the proportion of the user’s activity in each of selected indicators (of the four broad categories) instead of the absolute value. This information explains visually why the user is in the current membership class. In addition, user while receive a message with a notification, when +++
In the MAMEM system, the users’ membership will be public among the participants. There will be a visualization panel that shows the hierarchical representation of all (previous) users’ nicknames together with their memberships. This representation supposed to trigger social comparison and thus stimulate the user to increase participation.
Based on their status we reward the active users with some useful extra functionality, tailored to the group. The rewards will increase as the user moves to a higher level.
Lastly, users will receive messages, which evaluate their progress, warning them when they are about to downgrade or upgrade their membership.
D5.1 – V0.4
Page 63
In the document we completed two tasks. The first task was related to an attempt to learn about the MAMEM real users’ characteristics, which will help to drive the design process in the next steps. Thus, user profiles and Personas were created, which include information, relevant to the MAMEM purpose.
It was shown, that the three patient groups share many similarities such as perceptions about computer contributions and interaction behaviour; however, they have some differences in other domains that can affect their interaction with MAMEM (i.e., some demographic, such as age and physical symptoms). These similarities and differences must be taken into account in the future steps towards creating the MAMEM prototype.
In addition, the second task involved the design of persuasive principles to motivate users towards the use of MAMEM. This design followed the pilot trials protocol which is divided into two phases; therefore, the persuasive strategies were designed for each phase. For the first phase, which is the user acceptance and training engagement, various persuasive theories were selected and proposals on how they could be applied were made. For the design of the persuasive strategies, the needs and requirements of each of the target groups were taken into consideration. Thus, tailoring was the persuasive technique most frequently used. With regard, to the second phase, which refers to the increase of users ‘social inclusion through online social activities, a persuasive strategy called hierarchic memberships, was designed, taking into account the particularities of the groups throughout the design process.
The next step is to validate the selected strategies through experiments with users with similar characteristics with our target groups, to incorporate the updated strategies into the MAMEM prototype.
D5.1 – V0.4
Page 64
[1] Liu, Y., Osvalder, A. L., & Karlsson, M. (2010). Considering the importance of user profiles in interface design (pp. 61-80). INTECH Open Access Publisher.
[2] Henry, S. L. (2007). Just ask: integrating accessibility throughout design. Lulu. com.
[3] D6.1 - Clinical requirements for the MAMEM platform for each of the patient cohort, MAMEM Consortium, August 2015. url: http://www.mamem.eu/wp-
content/uploads/2015/09/D6.1_Clinical_requirements_Final.pdf
[4] D6.2 - Definition of pilot trials with the participation of patients, MAMEM Consortium, November 2015. url: http://www.mamem.eu/wp-
content/uploads/2015/11/D6.2_ClinicalRequirements_PilotTrialsDefinition_Final.pdf
[5] Van den Berg, M. E. L., Castellote, J. M., Mahillo-Fernandez, I., & de Pedro-Cuesta, J. (2010). Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology, 34(3), 184-192.
[6] J. Kemp, B., & Stuart Krause, J. (1999). Depression and life satisfaction among people ageing with post-polio and spinal cord injury. Disability and Rehabilitation, 21(5-6), 241-249.
[7] Rupp, R. (2014). Challenges in clinical applications of brain computer interfaces in individuals with spinal cord injury. Frontiers in neuroengineering, 7.
[8] Maynard, F. M., Karunas, R. S., & Waring 3rd, W. P. (1990). Epidemiology of spasticity following traumatic spinal cord injury. Archives of physical medicine and rehabilitation, 71(8), 566-569.
[9] Siddall, P. J., & Loeser, J. D. (2001). Pain following spinal cord injury. Spinal cord, 39(2).
[10] Diner, B. C., Holcomb, P. J., & Dykman, R. A. (1985). P 300 in major depressive disorder. Psychiatry Research, 15(3), 175-184.
[11] Krassioukov, A. V., Karlsson, A. K., Wecht, J. M., & Wuermser, L. A. (2007). Assessment of autonomic dysfunction following spinal cord injury: rationale for additions to International Standards for Neurological Assessment. Journal of rehabilitation research and development, 44(1), 103
[12] Martz, E., Livneh, H., Priebe, M., Wuermser, L. A., &Ottomanelli, L. (2005). Predictors of psychosocial adaptation among people with spinal cord injury or disorder. Archives of Physical Medicine and Rehabilitation, 86(6), 1182-1192.
[13] J. Kemp, B., & Stuart Krause, J. (1999). Depression and life satisfaction among people ageing with post-polio and spinal cord injury. Disability and Rehabilitation, 21(5-6), 241-249.
[14] Bonanno, G. A., Kennedy, P., Galatzer-Levy, I. R., Lude, P., &Elfström, M. L. (2012). Trajectories of resilience, depression, and anxiety following spinal cord injury. Rehabilitation Psychology, 57(3), 236.
D5.1 – V0.4
Page 65
[15] Hampton, N. Z. (2004). Subjective Well-Being Among People with Spinal Cord Injuries The Role of Self-Efficacy, Perceived Social Support, and Perceived Health. Rehabilitation Counseling Bulletin, 48(1), 31-37
[16] Dowler, R. N., Harrington, D. L., Haaland, K. Y., Swanda, R. M., Fee, F., & Fiedler, K. (1997). Profiles of cognitive functioning in chronic spinal cord injury and the role of moderating variables. Journal of the International Neuropsychological Society, 3(05), 464-472.
[17] Kerstin, W., Gabriele, B., & Richard, L. (2006). What promotes physical activity after spinal cord injury? An interview study from a patient perspective. Disability and rehabilitation, 28(8), 481-488.
[18] Goodman, N., Jette, A. M., Houlihan, B., & Williams, S. (2008). Computer and internet use by persons after traumatic spinal cord injury. Archives of physical medicine and rehabilitation, 89(8), 1492-1498.
[19] Houlihan, B. V., Drainoni, M. L., Warner, G., Nesathurai, S., Wierbicky, J., & Williams, S. (2003). The impact of Internet access for people with spinal cord injuries: a descriptive analysis of a pilot study. Disability & Rehabilitation, 25(8), 422-431
[20] Miller, S. M. (2008). The effect of frequency and type of internet use on perceived social support and sense of well-being in individuals with spinal cord injury. Rehabilitation Counseling Bulletin, 51(3), 148-158.
[21] Caltenco, H. A., Breidegard, B., Jönsson, B., &AndreasenStruijk, L. N. (2012). Understanding computer users with tetraplegia: Survey of assistive technology users. International Journal of Human-Computer Interaction, 28(4), 258-268
[22] Pfurtscheller, G., Linortner, P., Winkler, R., Korisek, G., & Müller-Putz, G. (2009). Discrimination of motor imagery-induced EEG patterns in patients with complete spinal cord injury. Computational intelligence and neuroscience, 2009
[23] Onose, G., Grozea, C., Anghelescu, A., Daia, C., Sinescu, C. J., Ciurea, A. V., ...&Popescu, C. (2012). On the feasibility of using motor imagery EEG-based brain–computer interface in chronic tetraplegics for assistive robotic arm control: a clinical test and long-term post-trial follow-up. Spinal Cord, 50(8), 599-608.
[24] Gourab, K., &Schmit, B. D. (2010). Changes in movement-related β-band EEG signals in human spinal cord injury. Clinical Neurophysiology, 121(12), 2017-2023.
[25] Wooten, G. F., Currie, L. J., Bovbjerg, V. E., Lee, J. K., &Patrie, J. (2004). Are men at greater risk for Parkinson’s disease than women?.Journal of Neurology, Neurosurgery & Psychiatry, 75(4), 637-639.)
[26] Fahn, S., Jankovic, J., & Hallett, M. (2011). Principles and practice of movement disorders. Elsevier Health Sciences.
[27] Jankovic, J. (2008). Parkinson’s disease: clinical features and diagnosis. Journal of Neurology, Neurosurgery & Psychiatry, 79(4), 368-376.
[28] Wu, T., Hallett, M., & Chan, P. (2015). Motor automaticity in Parkinson's disease. Neurobiology of disease, 82, 226-234.

D5.1 – V0.4
Page 66
[29] Williams, D. R., & Litvan, I. (2013). Parkinsonian syndromes. Continuum (Minneapolis, Minn.), 19(5 Movement Disorders), 1189-1212
[30] Doherty, K. M., van de Warrenburg, B. P., Peralta, M. C., Silveira-Moriyama, L., Azulay, J. P., Gershanik, O. S., & Bloem, B. R. (2011). Postural deformities in Parkinson's disease. The Lancet Neurology, 10(6), 538-549.
[31] Schoneburg, B., Mancini, M., Horak, F., & Nutt, J. G. (2013). Framework for understanding balance dysfunction in Parkinson's disease. Movement disorders, 28(11), 1474-1482.
[32] Cunningham, L. M., Nugent, C. D., Finlay, D. D., Moore, G., & Craig, D. (2009). A Review of Assistive Technologies for People with Parkinson's Disease. Technology and Health Care, 17(3), 269-279
[33] Pinkhardt, E. H., Jürgens, R., Lulé, D., Heimrath, J., Ludolph, A. C., Becker, W., & Kassubek, J. (2012). Eye movement impairments in Parkinson's disease: possible role of extradopaminergic mechanisms. BMC neurology, 12(1), 1.
[34] Nowacka, B., Lubioski, W., Honczarenko, K., Potemkowski, A., & Safranow, K. (2014). Ophthalmological features of Parkinson disease. Medical science monitor: international medical journal of experimental and clinical research, 20, 2243.
[35] Todorova, A., Jenner, P., & Chaudhuri, K. R. (2014). Non-motor Parkinson's: integral to motor Parkinson's, yet often neglected. Practical neurology, practneurol-2013.
[36] Dissanayaka, N. N., White, E., O'Sullivan, J. D., Marsh, R., Pachana, N. A., & Byrne, G. J. (2014). The Clinical Spectrum of Anxiety in Parkinson's Disease. Movement Disorders,29(8), 967-975.
[37] Goldman, J. G., Williams‐Gray, C., Barker, R. A., Duda, J. E., & Galvin, J. E. (2014). The Spectrum of Cognitive Impairment in Lewy Body Diseases. Movement Disorders, 29(5), 608-621
[38] Aarsland, D., Påhlhagen, S., Ballard, C. G., Ehrt, U., & Svenningsson, P. (2012). Depression in Parkinson disease—epidemiology, mechanisms and management. Nature Reviews Neurology, 8(1), 35-47.
[39] Pagonabarraga, J., Kulisevsky, J., Strafella, A. P., &Krack, P. (2015). Apathy in Parkinson's Disease: Clinical Features, Neural Substrates, Diagnosis, and Treatment. The Lancet Neurology, 14(5), 518-531.
[40] Franssen, M., Winward, C., Collett, J., Wade, D., & Dawes, H. (2014). Interventions for Fatigue in Parkinson's Disease: A Systematic Review and Meta‐analysis. Movement Disorders, 29(13), 1675-1678.
[41] Chaudhuri, K. R., Rizos, A., & Sethi, K. D. (2013). Motor and nonmotor complications in Parkinson’s disease: an argument for continuous drug delivery?. Journal of neural transmission, 120(9), 1305-1320.
[42] Aquino, C. C., & Fox, S. H. (2015). Clinical spectrum of levodopa‐induced complications. Movement Disorders, 30(1), 80-89.
D5.1 – V0.4
Page 67
[43] Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., ... &Aarsland, D. (2012). Diagnostic Criteria for Mild Cognitive Impairment in Parkinson's Disease: Movement Disorder Society Task Force guidelines. Movement Disorders, 27(3), 349-356.
[44] Muslimovid, D. (2009). Cognitive sequelae of Parkinson’s disease: nature, course, risk factors and functional impact.
[45] Katsarou, Z., Bostantjopoulou, S., Peto, V., Alevriadou, A., &Kiosseoglou, G. (2001). Quality of Life in Parkinson's Disease: Greek Translation and Validation of the Parkinson's Disease Questionnaire (PDQ-39). Quality of Life Research, 10(2), 159-163
[46] Knipe, M. D. W., Wickremaratchi, M. M., Wyatt‐Haines, E., Morris, H. R., & Ben‐Shlomo, Y. (2011). Quality of Life in Young‐Compared with Late‐Onset Parkinson's Disease. Movement Disorders, 26(11).
[47] McNaney, R., Balaam, M., Holden, A., Schofield, G., Jackson, D., Webster, M., ...& Olivier, P. (2015, April). Designing for and with People with Parkinson's: A Focus on Exergaming. In Proceedings of the 33rd annual ACM conference on Human Factors in Computing Systems (pp. 501-510). ACM.
[48] Alankus, G., & Kelleher, C. (2012, May). Reducing compensatory motions in video games for stroke rehabilitation. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (pp. 2049-2058). ACM.
[49] Marin, R. S., &Wilkosz, P. A. (2005). Disorders of Diminished Motivation. The Journal of head trauma rehabilitation, 20(4), 377-388
[50] Koerts, J., Tucha, L., Lange, K. W., & Tucha, O. (2013). The influence of cognitive reserve on cognition in Parkinson’s disease. Journal of Neural Transmission, 120(4), 593-596.
[51] Begnum, M. E. N. (2010). Challenges for Norwegian PC-Users with Parkinson’s Disease–A Survey. In Computers Helping People with Special Needs (pp. 292-299). Springer Berlin Heidelberg.
[52] Hartikainen, M., &Ovaska, S. (2015, October). People with Parkinson's Disease Using Computers. In Proceedings of the 17th International ACM SIGACCESS Conference on Computers & Accessibility (pp. 407-408). ACM
[53] Cunningham, L. M., Nugent, C. D., Finlay, D. D., Moore, G., & Craig, D. (2009). A Review of Assistive Technologies for People with Parkinson's Disease. Technology and Health Care, 17(3), 269-279
[54] van Essen, A. J., Busch, H. F. M., te Meerman, G. J., & Leo, P. (1992). Birth and population prevalence of Duchenne muscular dystrophy in The Netherlands. Human genetics, 88(3), 258-266.
[55] Biggar, W. D. (2006). Duchenne Muscular Dystrophy. Pediatrics in Review, 27(3), 83.
[56] Cyrulnik, S. E., Fee, R. J., Batchelder, A., Kiefel, J., Goldstein, E., &Hinton, V. J. (2008). Cognitive and Adaptive Deficits in Young Children with Duchenne Muscular
D5.1 – V0.4
Page 68
Dystrophy (DMD). Journal of the International Neuropsychological Society, 14(05), 853-861.
[57] Banihani, R., Smile, S., Yoon, G., Dupuis, A., Mosleh, M., Snider, A., & McAdam, L. (2015). Cognitive and Neurobehavioral Profile in Boys with Duchenne Muscular Dystrophy. Journal of child neurology, 30(11), 1472-1482.
[58] Pangalila, R. F., van den Bos, G. A., Bartels, B., Bergen, M., Stam, H. J., &Roebroeck, M. E. (2015). Prevalence of Fatigue, Pain, and Affective Disorders in Adults with Duchenne Muscular Dystrophy and their Associations with Quality of Life. Archives of physical medicine and rehabilitation, 96(7), 1242-1247.
[59] Pangalila, R. F., van den Bos, G. A., Bartels, B., Bergen, M. P., Kampelmacher, M. J., Stam, H. J., &Roebroeck, M. E. (2015). Quality of Life of Adult Men with Duchenne Muscular Dystrophy in the Netherlands: Implications for Care. Journal of rehabilitation medicine, 47(2), 161-166.
[60] Ogino, S., Leonard, D. G., Rennert, H., Ewens, W. J., & Wilson, R. B. (2002). Genetic risk assessment in carrier testing for spinal muscular atrophy. American journal of medical genetics, 110(4), 301-307
[61] Prior, T. W., Snyder, P. J., Rink, B. D., Pearl, D. K., Pyatt, R. E., Mihal, D. C., ... & Noonan, C. (2010). Newborn and carrier screening for spinal muscular atrophy. American Journal of Medical Genetics Part A, 152(7), 1608-1616.
[62] Lamb, C., &Peden, A. (2008). Understanding the Experience of Living with Spinal Muscular Atrophy: A Qualitative Description. Journal of Neuroscience Nursing, 40(4), 250-256.
[63] Qian, Y., McGraw, S., Henne, J., Jarecki, J., Hobby, K., &Yeh, W. S. (2015). Understanding the Experiences and Needs of Individuals with Spinal Muscular Atrophy and their Parents: a Qualitative Study. BMC neurology, 15(1), 1.
[64] Von Gontard, A., Zerres, K., Backes, M., Laufersweiler-Plass, C., Wendland, C., Melchers, P., ...&Rudnik-Schöneborn, S. (2002). Intelligence and Cognitive Function in Children and Adolescents with Spinal Muscular Atrophy. Neuromuscular Disorders, 12(2), 130-136.
[65] Salameh, J. S., Brown Jr, R. H., & Berry, J. D. (2015, August). Amyotrophic Lateral Sclerosis: Review. In Seminars in neurology (Vol. 35, No. 4, pp. 469-476).
[66] Geronimo, A., Stephens, H. E., Schiff, S. J., & Simmons, Z. (2015). Acceptance of Brain-Computer Interfaces in Amyotrophic Lateral Sclerosis. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, 16(3-4), 258-264.
[67] Grossman, A. B., Levin, B. E., & Bradley, W. G. (2006). Premorbid personality characteristics of patients with ALS. Amyotrophic Lateral Sclerosis, 7(1), 27-31.
[68] Neudert, C., Wasner, M., &Borasio, G. D. (2004). Individual Quality of Life is not Correlated with Health-Related Quality of Life or Physical Function in Patients with Amyotrophic Lateral Sclerosis. Journal of palliative medicine, 7(4), 551-557.
D5.1 – V0.4
Page 69
[69] Kübler, A., &Birbaumer, N. (2008). Brain–Computer Interfaces and Communication in Paralysis: Extinction of Goal Directed Thinking in Completely ParalysedPatients?.Clinical neurophysiology, 119(11), 2658-2666.
[70] Bamshad, M., Van Heest, A. E., & Pleasure, D. (2009). Arthrogryposis: a Review and Update. J Bone Joint Surg Am, 91(Supplement 4), 40-46.
[71] Kowalczyk, B., &Feluś, J. (2016). Arthrogryposis: an Update on Clinical Aspects, Etiology, and Treatment Strategies. Archives of Medical Science: AMS, 12(1), 10.
[72] Lathouwers, K., de Moor, J., &Didden, R. (2009). Access to and Use of Internet by Adolescents who Have a Physical Disability: A Comparative Study. Research in developmental disabilities, 30(4), 702-711
[73] Fogg, B.J. (2003). Persuasive Technology: Using Computers to Change What We Think and Do. Morgan Kaufmann Publishers: San Francisco.
[74] Deci, E. L., & Ryan, R. M. (2000). The" what" and" why" of goal pursuits: Human needs and the self-determination of behavior. Psychological inquiry, 11(4), 227-268.
[75] Baumeister, R. F., & Vohs, K. D. (2007). Self‐Regulation, ego depletion, and motivation. Social and Personality Psychology Compass, 1(1), 115-128.
[76] Friese, M., & Hofmann, W. (2009). Control me or I will control you: Impulses, trait self-control, and the guidance of behavior. Journal of Research in Personality, 43(5), 795-805.
[77] Carver, C. S., & Scheier, M. F. (1982). Control theory: A useful conceptual framework for personality–social, clinical, and health psychology. Psychological bulletin, 92(1), 111.
[78] Strack, F., & Deutsch, R. (2004). Reflective and impulsive determinants of social behavior. Personality and social psychology review, 8(3), 220-247.
[79] Kahneman, D. (2003). A perspective on judgment and choice: mapping bounded rationality. American psychologist, 58(9), 697.
[80] Sheeran, P., Gollwitzer, P. M., & Bargh, J. A. (2013). Nonconscious processes and health. Health Psychology, 32(5), 460.
[81] Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Prentice-Hall, Inc.
[82] Bandura, A. (1997). Self-efficacy: the exercise of control. New York: Freeman.
[83] Schwarz, N. (1990). Feelings as information: informational and motivational functions of affective states. Guilford Press.
[84] Forgas, J.P. (1992). Affect in social judgments and decisions: A multi-process model. In: Zanna, M.P. (Eds), Advances in experimental social psychology (Vol 27, pp. 227-275). San Diego: Academic
[85] Beedie, C., Terry, P., & Lane, A. (2005). Distinctions between emotion and mood. Cognition & Emotion, 19(6), 847-878.
D5.1 – V0.4
Page 70
[86] Ekman, P. (1999). Basic emotions. In Dalgleish, T., & Power, M. J. Handbook of cognition and emotion. Sussex UK: John Wiley & Sons.
[87] Crites, S. L., Fabrigar, L. R., & Petty, R. E. (1994). Measuring the affective and cognitive properties of attitudes: Conceptual and methodological issues. Personality and Social Psychology Bulletin, 20(6), 619-634.
[88] Trafimow, D., & Sheeran, P. (1998). Some tests of the distinction between cognitive and affective beliefs. Journal of experimental social psychology, 34(4), 378-397.
[89] Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention and behavior: An introduction to theory and research.
[90] Ajzen, I., & Madden, T. J. (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of experimental social psychology, 22(5), 453-474.
[91] Fishbein, M., & Ajzen, I. (2011). Predicting and changing behavior: The reasoned action approach. Taylor & Francis.
[92] Cialdini, R. B., & Trost, M. R. (1998). Social influence: Social norms, conformity and compliance.
[93] Redström, J. (2006). Persuasive design: Fringes and foundations. In Persuasive Technology (pp. 112-122). Springer Berlin Heidelberg.
[94] Oinas-Kukkonen, H., & Harjumaa, M. (2009). Persuasive systems design: Key issues, process model, and system features. Communications of the Association for Information Systems, 24(1), 28.
[95] Lockton, D., Harrison, D., & Stanton, N. A. (2010). The Design with Intent Method: A design tool for influencing user behaviour. Applied ergonomics, 41(3), 382-392.
[96] ldredge, L. K. B., Parcel, G. S., Kok, G., & Gottlieb, N. H. (2011). Planning health promotion programs: an intervention mapping approach. John Wiley & Sons.
[97] Venkatesh, V., Morris, M. G., Davis, G. B., & Davis, F. D. (2003). User acceptance of information technology: Toward a unified view. MIS quarterly, 425-478.
[98] Dillard, J., & Harmon-Jones, C. (2002). A Cognitive Dissonance Theory Perspective on Persuasion. The Persuasion Handbook: Developments in Theory and Practice, 99.
[99] Nabi, R. L. (2002). Discrete emotions and persuasion. The persuasion handbook: Developments in theory and practice, 289-308.
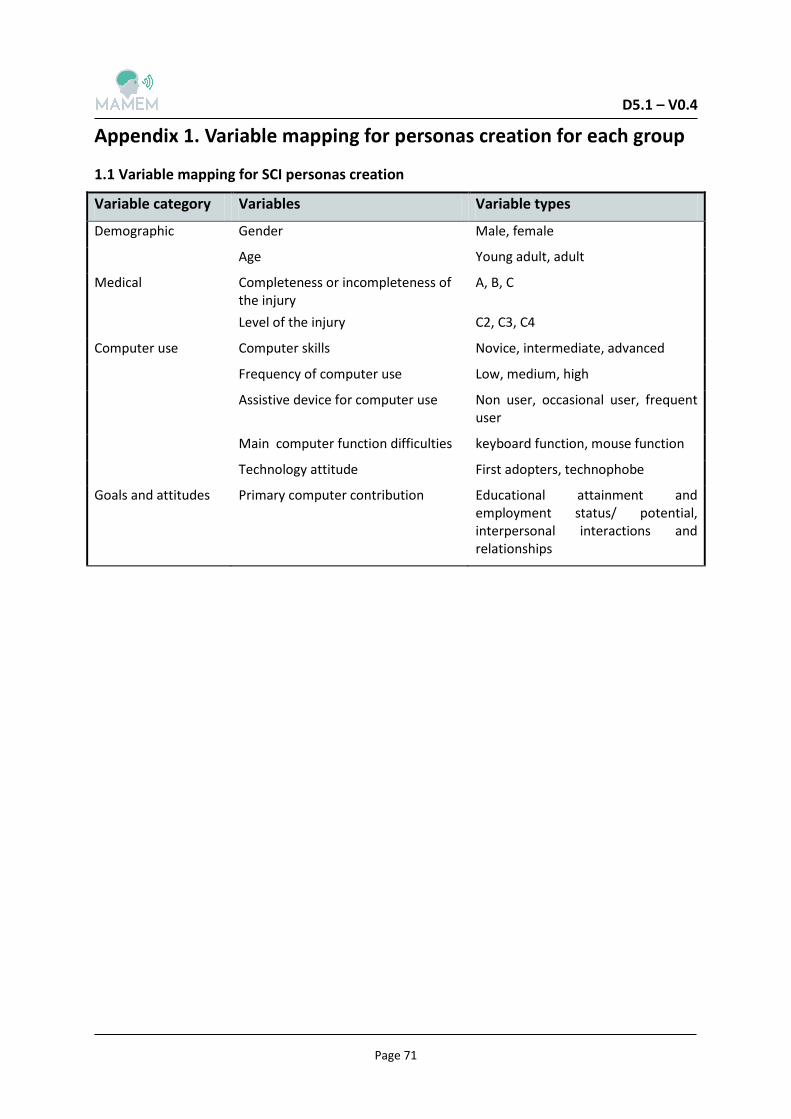
D5.1 – V0.4
Page 71
1.1 Variable mapping for SCI personas creation
Variable category Variables Variable types
Demographic Gender Male, female
Age Young adult, adult
Medical Completeness or incompleteness of the injury
A, B, C
Level of the injury C2, C3, C4
Computer use Computer skills Novice, intermediate, advanced
Frequency of computer use Low, medium, high
Assistive device for computer use Non user, occasional user, frequent user
Main computer function difficulties keyboard function, mouse function
Technology attitude First adopters, technophobe
Goals and attitudes Primary computer contribution Educational attainment and employment status/ potential, interpersonal interactions and relationships
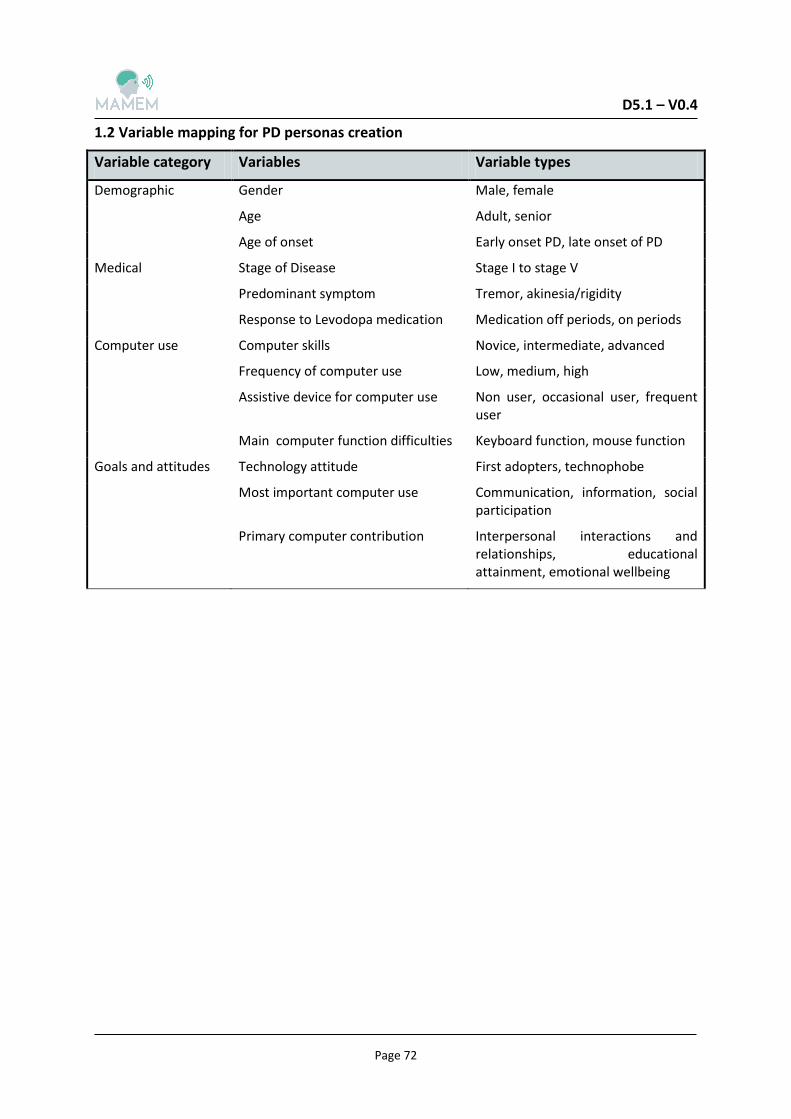
D5.1 – V0.4
Page 72
1.2 Variable mapping for PD personas creation
Variable category Variables Variable types
Demographic Gender Male, female
Age Adult, senior
Age of onset Early onset PD, late onset of PD
Medical Stage of Disease Stage I to stage V
Predominant symptom Tremor, akinesia/rigidity
Response to Levodopa medication Medication off periods, on periods
Computer use Computer skills Novice, intermediate, advanced
Frequency of computer use Low, medium, high
Assistive device for computer use Non user, occasional user, frequent user
Main computer function difficulties Keyboard function, mouse function
Goals and attitudes Technology attitude First adopters, technophobe
Most important computer use Communication, information, social participation
Primary computer contribution Interpersonal interactions and relationships, educational attainment, emotional wellbeing
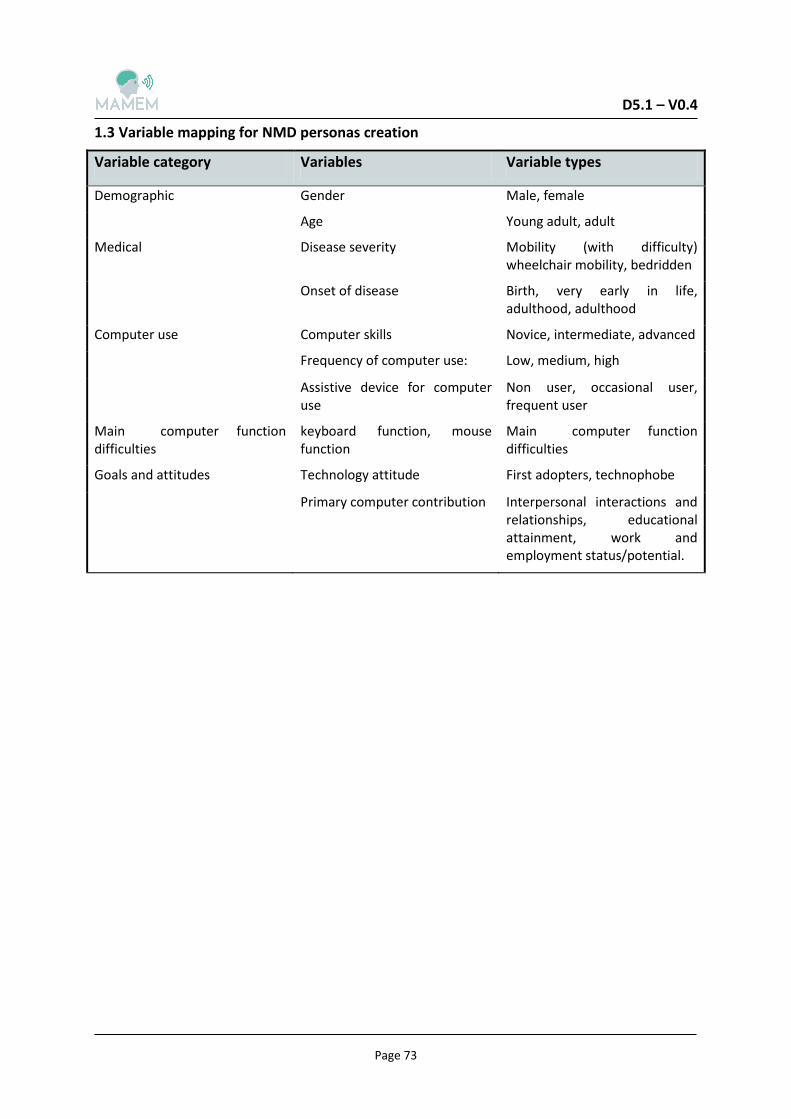
D5.1 – V0.4
Page 73
1.3 Variable mapping for NMD personas creation
Variable category Variables Variable types
Demographic Gender Male, female
Age Young adult, adult
Medical Disease severity Mobility (with difficulty) wheelchair mobility, bedridden
Onset of disease Birth, very early in life, adulthood, adulthood
Computer use Computer skills Novice, intermediate, advanced
Frequency of computer use: Low, medium, high
Assistive device for computer use
Non user, occasional user, frequent user
Main computer function difficulties
keyboard function, mouse function
Main computer function difficulties
Goals and attitudes Technology attitude First adopters, technophobe
Primary computer contribution Interpersonal interactions and relationships, educational attainment, work and employment status/potential.
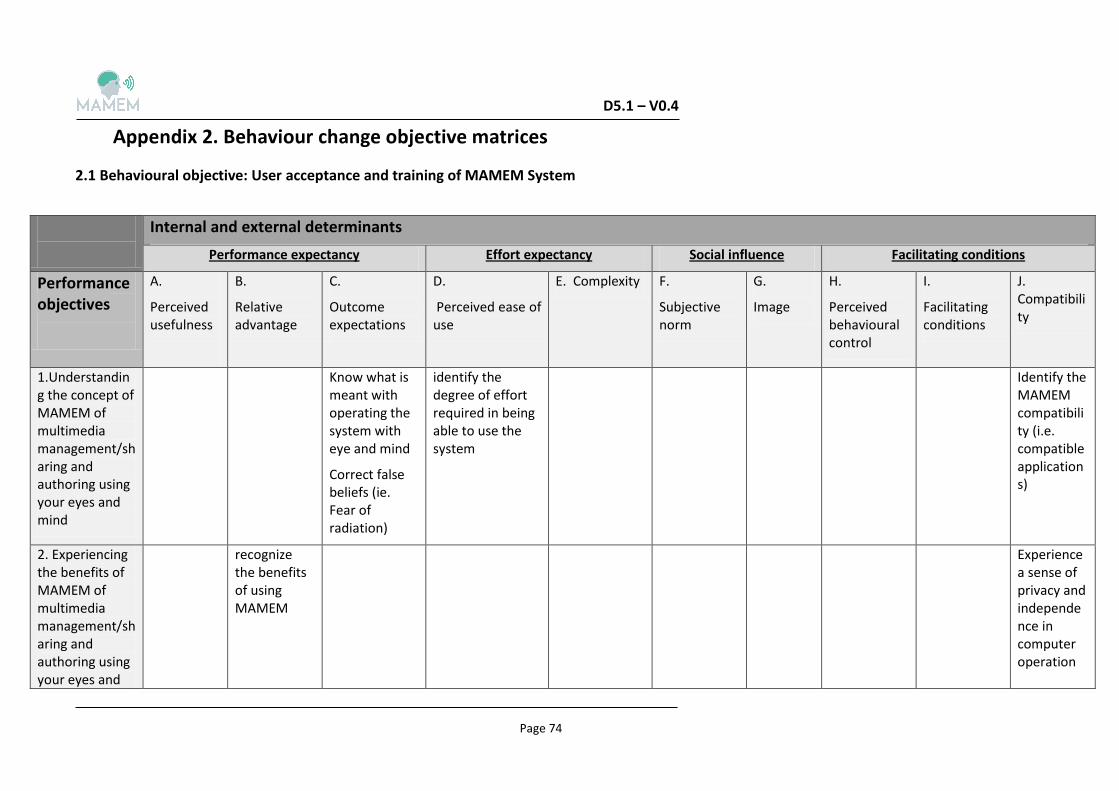
D5.1 – V0.4
Page 74
2.1 Behavioural objective: User acceptance and training of MAMEM System
Internal and external determinants
Performance expectancy Effort expectancy Social influence Facilitating conditions
Performance objectives
A.
Perceived usefulness
B.
Relative advantage
C.
Outcome expectations
D.
Perceived ease of use
E. Complexity F.
Subjective norm
G.
Image
H.
Perceived behavioural control
I.
Facilitating conditions
J. Compatibility
1.Understanding the concept of MAMEM of multimedia management/sharing and authoring using your eyes and mind
Know what is meant with operating the system with eye and mind
Correct false beliefs (ie. Fear of radiation)
identify the degree of effort required in being able to use the system
Identify the MAMEM compatibility (i.e. compatible applications)
2. Experiencing the benefits of MAMEM of multimedia management/sharing and authoring using your eyes and
recognize the benefits of using MAMEM
Experience a sense of privacy and independence in computer operation
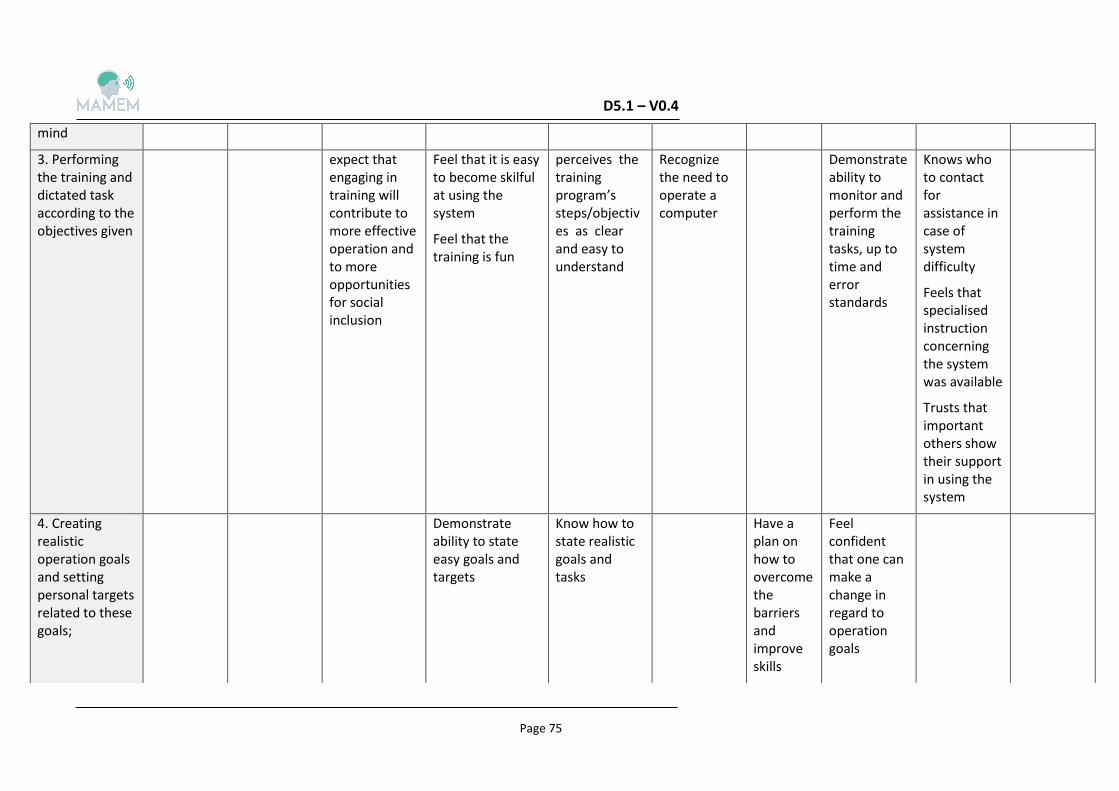
D5.1 – V0.4
Page 75
mind
3. Performing the training and dictated task according to the objectives given
expect that engaging in training will contribute to more effective operation and to more opportunities for social inclusion
Feel that it is easy to become skilful at using the system
Feel that the training is fun
perceives the training program’s steps/objectives as clear and easy to understand
Recognize the need to operate a computer
Demonstrate ability to monitor and perform the training tasks, up to time and error standards
Knows who to contact for assistance in case of system difficulty
Feels that specialised instruction concerning the system was available
Trusts that important others show their support in using the system
4. Creating realistic operation goals and setting personal targets related to these goals;
Demonstrate ability to state easy goals and targets
Know how to state realistic goals and tasks
Have a plan on how to overcome the barriers and improve skills
Feel confident that one can make a change in regard to operation goals
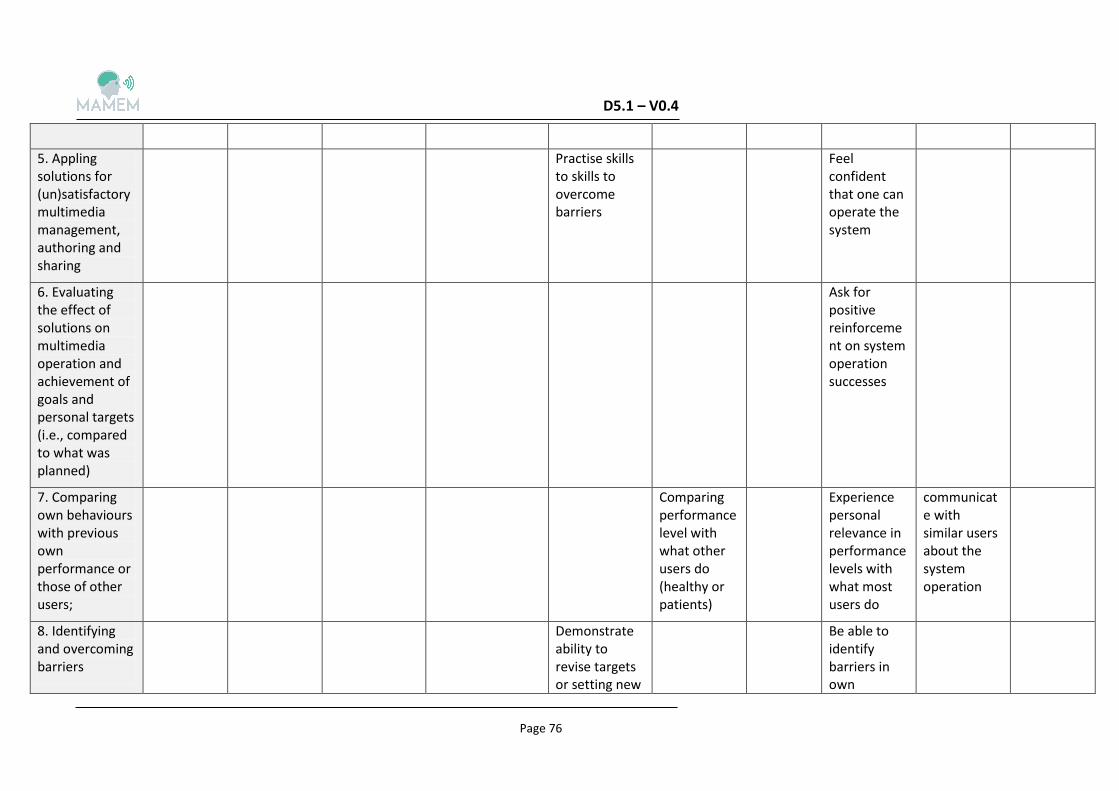
D5.1 – V0.4
Page 76
5. Appling solutions for (un)satisfactory multimedia management, authoring and sharing
Practise skills to skills to overcome barriers
Feel confident that one can operate the system
6. Evaluating the effect of solutions on multimedia operation and achievement of goals and personal targets (i.e., compared to what was planned)
Ask for positive reinforcement on system operation successes
7. Comparing own behaviours with previous own performance or those of other users;
Comparing performance level with what other users do (healthy or patients)
Experience personal relevance in performance levels with what most users do
communicate with similar users about the system operation
8. Identifying and overcoming barriers
Demonstrate ability to revise targets or setting new
Be able to identify barriers in own
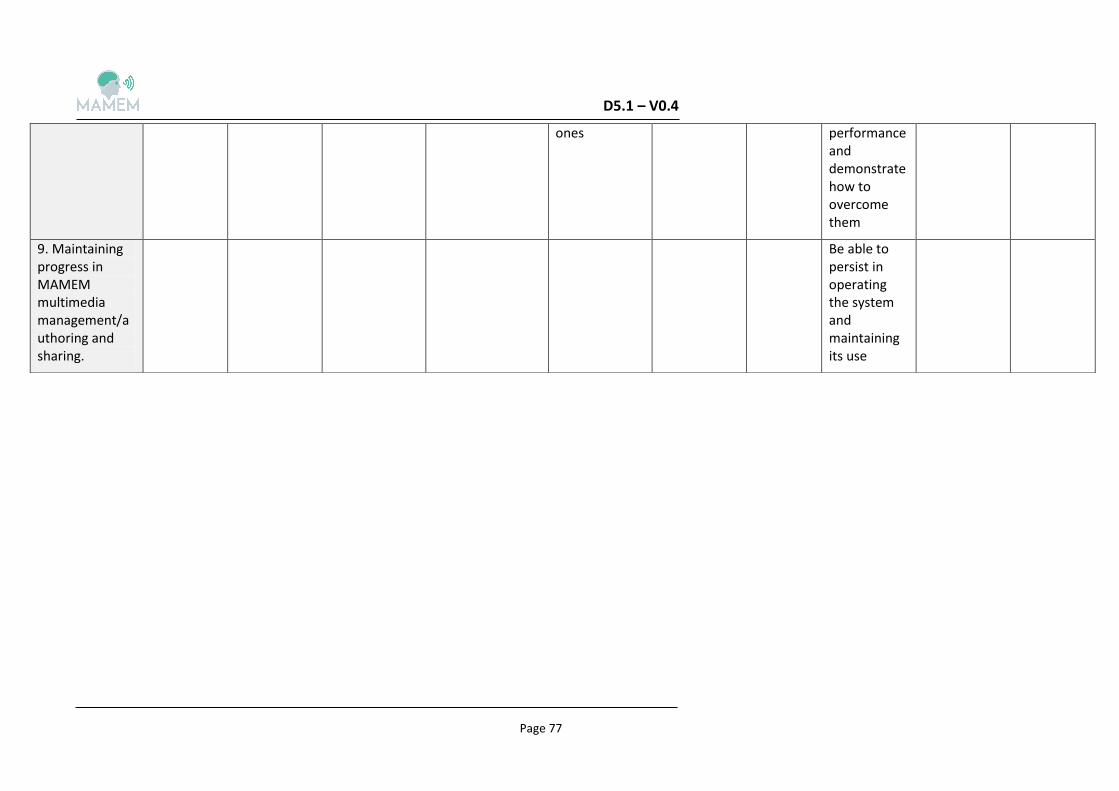
D5.1 – V0.4
Page 77
ones
performance and demonstrate how to overcome them
9. Maintaining progress in MAMEM multimedia management/authoring and sharing.
Be able to persist in operating the system and maintaining its use