report on and assessment of the human resources...
TRANSCRIPT

Report on and assessment of the human resources
management system, including activities undertaken to
strengthen the system and recommendations for use in
other regions
USAID/Peru/Health Policy
Contract No. GHS-I-10-07-00003-00
December 15, 2013
Prepared for:
Armando Cotrina, COR
USAID/Peru Health Office
Av. Encalada s/n
Lima - Peru
Submitted by:
Abt Associates Inc.
4550 Montgomery
Avenue
Suite 800 North
Bethesda, MD 20814

This document has been drafted by the USAID|PERU|Health Policy Project, financed by the
United States Agency for International Development (USAID) under contract #GHS-I-10-07-
00003-00.
The author’s views expressed in this publication do not necessarily reflect the views of the
United States Agency for International Development or the United States government.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Table of Contents ▌pg. i
Table of Contents
Acronyms ....................................................................................................................................... iv
Executive Summary ...................................................................................................................... vi
Introduction .................................................................................................................................... 1
1. Legal and conceptual framework for the development of Human Resources
Management System in health institutions .................................................................................. 3
1.1 SERVIR and Civil Service Reform ............................................................................. 3
1.1.1 Background of the civil service in Peru[2] .................................................... 3
1.1.2 The Civil Service Law ................................................................................... 4
1.2 Ministry of Health: Proposal on Human Resources Management System for Health
Institutions.............................................................................................................................. 6
1.2.1 HHR policy and strategic planning ................................................................ 7
1.2.2 Work organization ......................................................................................... 8
1.2.3 Employment management ............................................................................. 9
1.2.4 Performance management ........................................................................... 10
1.2.5 Development and training management ...................................................... 10
1.2.6 Compensation management ......................................................................... 11
1.2.7 Managing human and social relations ......................................................... 11
2. Assessment of the Human Resources Management System ........................................... 13
2.1 Performance Evaluation of the Entire HRMS in Health Institutions ......................... 13
2.1.1 Tools and methodologies to assess HRMS implementation ........................ 13
2.1.2 Human Resources Management System in SMT-RHD .............................. 15
2.1.3 Human Resources Management System in other regions ........................... 18
2.2 HHR Policy and Strategic Planning: Progress........................................................... 22
2.2.1 Results of the assessment in San Martin Regional Health Directorate ........ 22
2.2.2 Results of the assessment in other regions .................................................. 28
2.3 Work Organization: Progress .................................................................................... 31
2.3.1 Results of the assessment in San Martin Regional Health Directorate ........ 31
2.3.2 Results of the assessment in other regions .................................................. 34
2.4 Employment Management: Progress ......................................................................... 36

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Table of Contents ▌pg. ii
2.4.1 Results of the assessment in San Martin Regional Health Directorate ........ 37
2.4.2 Results of the assessment in other regions .................................................. 40
2.5 Performance Management: Progress ......................................................................... 44
2.5.1 Results of the assessment in San Martin Regional Health Directorate ........ 44
2.5.2 Results of the assessment in other regions .................................................. 47
2.6 Development and Training Management: Progress .................................................. 50
2.6.1 Results of the assessment in San Martin Regional Health Directorate ........ 50
2.6.2 Results of the assessment in other regions .................................................. 53
2.7 Compensation Management: Progress ...................................................................... 56
2.7.1 Results of the assessment in SMT-RHD ..................................................... 56
2.7.2 Results of the assessment in other regions .................................................. 60
2.8 Managing Human and Labor Relations: Progress ..................................................... 62
2.8.1 Results of the assessment in San Martin Regional Health Directorate ........ 62
2.8.2 Results of the assessment in other regions .................................................. 65
3. Activities undertaken to strengthen the HRMS in health institutions .......................... 69
3.1 Activities undertaken to estimate staffing needs ....................................................... 69
3.2 Activities undertaken to define job profiles............................................................... 75
3.3 Activities undertaken to define managerial competencies ........................................ 80
3.4 Activities undertaken to design salary scales ............................................................ 82
3.5 Activities undertaken to develop competencies at micronetwork level..................... 84
3.6 Activities undertaken to assess management performance........................................ 86
3.6.1 Performance evaluation method .................................................................. 87
3.6.2 Performance evaluation implementation ..................................................... 88
3.6.3 Competencies evaluation definition and criteria ......................................... 89
3.6.4 Analysis of results obtained in the evaluation of goals attained and
competencies ............................................................................................................. 89
3.7 Activities undertaken to improve recruit and selection processes ............................. 90
4. Conclusions ....................................................................................................................... 100
5. Recommendations to implement the HRMS at regional level ..................................... 102
6. References ......................................................................................................................... 103

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Table of Contents ▌pg. iii
7. Annex ................................................................................................................................ 104
7.1 Questionnaire to assess the implementation of the HRMS in health institutions .... 104
7.2 Qualitative assessment of HRMS conducted by PARSALUD II in 4 Regions ....... 138
7.3 SMT-RHD: HHR regional policies ......................................................................... 140
7.4 National agenda for research in HHR ...................................................................... 141
7.5 ASEGURA software for HHR requirements calculations ....................................... 143
7.6 Using the spreadsheet to facilitate calculations ....................................................... 144
7.7 Survey to determine the available working time in the first-level-of-care .............. 155
7.8 Detailed table of "available working time" for health facilities .............................. 159
7.9 Available working time to provide PEAS in first-level-of-care health facilities..... 160
7.10 Ministry of health: General competencies for the health sector .................... 161
7.11 CONEAU: Managerial competencies for health professionals ..................... 163
7.12 Human resources management competencies ............................................... 164
7.13 Transversal managerial competencies ........................................................... 167

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Acronyms ▌pg. iv
Acronyms
AETA Asignación Extraordinaria por Trabajo Asistencial / Extraordinary Assignment
for Health Care Work
CAFAE Comité de Administración del Fondo de Asistencia y Estímulo / Management
Committees for the Stimulus and Assistance Fund
CAS Contrato administrativo de servicios / Administrative services contract
CAP Cuadro de asignación de personal / Staffing Table
CDC Competencies Development Centers
CGP Civil service managers
CLAS Comités Locales de Administración de Salud / Health Administration Local
Committees
CONEAU Consejo de evaluación, acreditación y certificación de la calidad de la
educación superior universitaria / Council for the Quality of Professional
Education
CTS Compensación por Tiempo de Servicios / Compensation for time of service
DGGDRH Department of Human Resources Development Management
DIRESA Dirección Regional de Salud / Region Health Directorate
DL Legislative Decree
HP Health Policy
HR Human resources
HHR Health human resources
HRMS Human Resources Management System
ILO International Labour Organization
JNE National Jury of Elections
LMEP Ley marco del empleo público / Framework law for public employment
MAPRO Manual de procesos / Procedures Manual
MOF Manual of Organizations and Functions
MoF Ministry of Finance
MoH Ministry of Health
PAHO Pan American Health Organization
PAP Presupuesto analítico de personal / Staff budget
PARSALUD II Programa de Apoyo a la Reforma del Sector Salud / Program for Health
Reform Support
PCM Presidency of the Council of Ministers
PDP Personal Development Plan
PEAS Plan esencial de aseguramiento universal / Essential package
PLAME Planilla mensual de pagos / Monthly payroll
RG Regional governments

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Acronyms ▌pg. v
RHD Regional health directorate
RIT Reglamento interno de trabajo / Internal rules
RNSDD Registro Nacional de Sanciones de Destitución y Despido / National Registry
of Sanctions and Dismissals
ROF Regulation of Organization and Functions
SERUMS Servicio Rural y Urbano Marginal en Salud / Civil Health Service in Rural and
Marginal Urban Areas
SERVIR National Civil Service Authority
SMT-RHD San Martin Regional Health Directorate
TA Technical Assistance
UE Unidades ejecutoras de presupuesto / Budget spending units
UHI Universal health insurance
UNDP United Nations Development Programme
USAID United States Agency for International Development
WHO World Health Organization
WISN Workload Indicators of Staffing Need

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Executive Summary ▌pg. vi
Executive Summary
In June 2008, the National Civil Service Authority (SERVIR) was created as the leading agency in
managing the Human Resources Management System for public institutions. Complementarily,
the Ministry of Health defined a basic structure for this system to be implemented in health
institutions. This structure contains seven components or sub-systems with 29 processes.
Based on this structure, the Health Policy (HP) project designed a tool to assess the level of
implementation for all 29 processes at the regional level. This assessment instrument was applied
to Cajamarca and San Martin regional health directorates, and as results collected by the
Program to Support Health Reform (PARSALUD II) in 4 additional regions.
Evidence from these six regions confirms that human resource offices only perform administrative
activities related to monitoring staff attendance; recruiting, selection and hiring; managing
payrolls; and relations with unions. Almost no progress was seen in the performance evaluation
and planning components, while some modest progress was observed in processes related to
organization of work; capacity development; and management of human and social relations. The
few processes that are developing display technical shortcomings. The challenge is to make
these offices move away from personnel administration towards a more comprehensive human
resource management approach.
The poor performance of human resource offices is mainly due to the fact that these offices are
staffed with non-professional personnel who are not trained in human resource management.
Additionally, offices are not able to take on new responsibilities under the regulatory framework of
the human resources management system. Another difficulty related to the management of
human resources is the variety of personnel policies, many of which are duplicates of or are in
conflict with other policies. This confusion over policies prevents processes from being carried out
according to norms; causes frequent staff turnover; contributes to a lack of clarity in team member
roles and the lack of a responsible part for managing processes; engenders the existence of
various remunerative norms that provoke dissatisfaction and inequity; and impedes the creation of
reliable human resources information to formulate sound decisions. Additionally, not all processes
are managed by a single organizational unit.
A key factor in this situation is that the health authorities do not give much importance to human
resource management. In some cases, authorities have designated untrained employees as
heads of human resources offices. In another case, authorities have hired a lawyer to manage the
office to have a legal advisor to manage institutional relationships with unions.
For the health sector, the lack of a proper human resource planning process generates that
specific human resource needs to meet the population’s health needs are unknown. The lack of
job profiles favours selection processes that are based on subjective criteria rather than the needs
of the position. Recruitment and selection processes are carried out without taking into account
key regulatory aspects such as adequate dissemination for competitive recruitment; and objective
assessment of the candidates. The lack of objective performance assessments based on job
profiles generates that staff do not know if what they are doing is right. Lack of performance
incentives generates a lack of motivation. The lack of a fair and equitable salary scale not only
generates dissatisfaction but also results in a shortage of human resources where they are
needed most.
To tackle these problems, USAID has contributed to the design and validation of tools aimed at
the implementation of key processes for managing health human resources. The tools designed
include the following:
Methodology and tools to define human resource requirements at the first level of care.
Methodology and tools for the design of job profiles.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Executive Summary ▌pg. vii
Methodology for the design of labor competencies and performance standards.
Methodology and tools for designing salary scales for staff recruitment at the first level of
care.
Methodology and tools for competency development for health personnel responsible for the
growth and development of children under five years through the implementation of
competency development centers at the first level of care.
Methodology and flowcharts for recruitment, selection and hiring processes based on job
profiles.
Methodology and tools for evaluating the performance of health network managers.
Implementing these tools at the regional level depends fundamentally on whether regional
authorities understand the link between improvement in health indicators and the performance of
health human resources. Improving organizational performance depends on how many human
resources are required for the achievement of regional health goals and the individual
performance of each health worker.
To improve individual performance, it is necessary to define what is expected of each health
worker; measure the performance gap; implement incentive mechanisms for good performance or
capacity building programs; and establish an appropriate working environment.
This report presents detailed information about the results of the human resources management
system assessment as well as an explanation of the tools that were designed and implemented to
strengthen the system.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Introduction ▌pg. 1
Introduction
The enactment of Legislative Decree (DL) 1023 in June 2008 created the National Civil Service
Authority (Autoridad Nacional del Servicio Civil - SERVIR) as the governing body of the Human
Resources Management System (HRMS). The Presidency of the Council of Ministers
(Presidencia del Consejo de Ministros – PCM) confers SERVIR with the legal power and national
authority to improve public administration by strengthening the civil service at national scope.
The HRMS provides, develops and implements government policies related to the civil service,
including the rules, principles, resources, methods, procedures and techniques used by all public
sector entities in the management of human resources (HR).
The HRMS is composed of:
a) SERVIR, which formulates civil service national policy, governs the system and resolves
disputes.
b) State-level human resources offices, or those acting in their place, which are responsible for
implementing the rules, principles, methods, procedures and techniques of the system as part
of the decentralization process.
According to DL 1023, the system comprises the following processes:
Planning of HR policies
Work organization
Employment management
Performance management
Compensation management
Development management and training
Managing relationships
Resolution of disputes
In addition, Article Six of Law No. 30057[1], the Civil Service Law passed in July 2013,
establishes the following functions for the HR office in public institutions:
a) Executes and implements arrangements, guidelines and management tools provided by
SERVIR and the respective public institution.
b) Develops guidelines and policies for the development of the personnel management plan and
the optimal functioning of the HRMS, including the application of indicators.
c) Supervises, develops and implements continuous improvement initiatives in the processes
that comprise the HRMS.
d) Conducts research as well as quantitative and qualitative analysis of staff provision, according
to institutional needs.
e) Manages job profiles.
f) Manages and updates, in the scope of its competence, the National Registry of Civil Service
Personnel (Registro Nacional de Personas del Servicio Civil) and the National Registry of
Dismissal and Sanctions (Registro Nacional de Sanciones de Destitución y Despido –
RNSDD).
g) Other functions that are established through regulations by the governing body of the system.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Introduction ▌pg. 2
Through this framework, the Ministry of Health (MoH) proposes a scheme to support health
institutions in the implementation of a system for health human resources (HHR).
This report presents the current operating status of the HRMS in six regional health directorates;
activities that have been developed to strengthen HRMS implementation in health institutions; and
recommendations to improve implementation and replicate successes in other regions.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 3
1. Legal and conceptual framework for the development of Human
Resources Management System in health institutions
This chapter delineates the legal framework governing HRMS implementation in public institutions
and the HRMS structure, which was designed by the MoH for health institutions nationwide.
1.1 SERVIR and Civil Service Reform
1.1.1 Background of the civil service in Peru[2]
The civil service in Peru has been characterized as very complex with large deficits in planning
and organization capacity. Most especially, however, the civil service has been criticized for
lacking a clear authority to conduct the processes required to satisfy workers’ needs and improve
performance.
Most of the obstacles toward achieving a just and equitable civil service are related to the
coexistence of different working regimes, distortions in remunerative schemes, temporary
contracts, the lack of a governing body, and most especially the lack of a national civil service
policy.
There have been various reform processes over the past 20 years, including the following:
a) In 1990, the reform process was characterized by downsizing and the redefinition of the
state’s role in HR issues. The following initiatives illustrate this process: reducing staff
through incentives to resign; closing entry into the civil service; creating a private activity
labor regime (DL 728); contracting "non-personnel services" to prevent the entry of
permanent staff; hiring senior officials from UNDP and the Management Support Fund;
and creating alternative mechanisms to increase worker incomes such as the
Management Committees for the Stimulus and Assistance Fund (Comités de
Administración del Fondo de Asistencia y Estímulo - CAFAE).
b) In 1995, the reform process concentrated on modernizing the state and encouraging the
flexibility of administrative systems. However, the process lacked political support, and
progress was limited to the enactment of the following laws: Law of State Procurements
(Ley de Contrataciones del Estado); Diplomatic Service Law; and the law that prohibits
recruitment and employment in case of kinship.
c) In 2000, the reform process sought to overcome citizens’ distrust of public institutions
through the creation of spaces for dialogue. A new process of decentralization was
initiated in 2002, and the “Framework Law for Public Employment (Ley Marco del Empleo
Público - LMEP) was enacted in 2004.
d) In 2008, the current civil service reform process started. At the outset, there were 500 civil
service regulations, more than 102 salary scales in 82 public institutions, over 400 rules to
regulate payment of public employees, and more than 198 remunerative and non-
remunerative types of payments. The Peruvian state employed approximately 1,300,000
public servants, and each year 42,000 new employees were being hired without a clear
purpose or need. SERVIR was created at this time1 as the administrative governing body
for HRM and responsible for civil service development. Several of the laws related to civil
service reform[2] are shown in the following table:
1 DL 1023

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 4
Table 1: Problems that are trying to be solved by new civil service laws.
Problem Proposal Law
Lack of governing body in HRM Creation and implementation of SERVIR DL 1023
Lack of formal recruitment for highly
qualified professionals
Creation and regulation of the Public Managers
Corps
DL 1024
Lack of a performance assessment
system
Permanent evaluation:
To train underperforming workers
To recognize and reward efficient workers
To have qualified staff
DLDL 1025
Lack of training programs and policies Approval of training procedures and a training
fund
DL 1025
Limitations in rationalizing staff
especially in regions and
municipalities
Establishment of a special regime that allows local
and regional governments to implement
comprehensive modernization processes
DL 1026
SOURCE: SERVIR
These regulations have been integrated into one law, which will regulate incorporation, retention,
promotion and termination of civil servants.
1.1.2 The Civil Service Law
After several attempts to improve civil service in Perú, Law No. 30057[1], the Civil Service Law,
was enacted on July 4, 2013 to establish a unique regime for individuals who are employed by the
government and are responsible for its management, the exercise of its authority, and the
provision of services.
According to the rule, the guiding principles of the civil service according to the law are: general
interest; effectiveness and efficiency; equal opportunity; merit; budgetary provision; legal and
regulatory expertise; transparency; management accountability; probity and public ethics;
flexibility; and protection against the arbitrary end of the civil service.
Civil servants in public entities will be classified by the following groups when the law is
implemented:
a) Public Official: Political representative or political office representative who exercises
government functions in state organizations. Directs a unit and approves policies and
standards.
Public officials are classified as:
Public official from a direct and universal election (president, vice president,
congressmen, regional councilors, mayors, aldermen)
Public official whose designation and removal is regulated (ombudsman;
comptroller general of the republic; public prosecutor; chairman of the supreme
court; president of the National Jury of Elections (JNE); and rectors and vice
rectors of public universities, among others)
Public official whose designation and removal is based on trust (ministers; vice
ministers; general manager of regional government; and municipal manager).
They must have higher education or experience and meet the job profile
requirements.
b) Public Directors: Civil servant who runs a body, program or special project. Admission is
by open competition based on merit and fulfillment of the respective job profile. Public
directors can remain in their position for three years renewable up to two terms depending

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 5
on the fulfillment of annual goals. Their performance evaluations are based on
compliance with goals. Only 20% of public directors can have the status of “trusted
servants”2 .
c) Career civil servant: Civil servant with functions directly related to compliance of key
substantive functions. This is a unique and integrated system, which does not include
officers; public officials; trusted officials; or complementary activities civil servants. These
positions are not filled on a temporary basis. Hiring is done by open or public competition
based on merit, fulfilling the respective job profile.
d) Complementary activities civil servant: Civil servant with functions indirectly related to
compliance of key substantive functions. Hiring is done by open competition based on
merit, fulfilling the respective job profile. They can be hired through a contract for an
indefinite period or a fixed-term contract.
This law also reaffirms the organization of the civil service through the Administrative System of
Human Resource Management, which includes SERVIR, the HR offices of public institutions and
the Civil Service Tribunal.
HR offices or those serving in their stead are responsible for the HRM and have the following
functions:
a) Implements HR management guidelines provided by SERVIR and its unit.
b) Designs guidelines and policies for the development of a “people management plan” and
the optimal functioning of the HRMS, including the application of indicators.
c) Supervises, develops and implements continuous improvement initiatives in the HRMS.
d) Analyzes quantitative and qualitative staffing according to institutional needs.
e) Manages job profiles.
f) Maintains the National Registry of Civil Service Personnel and the National Registry of
Sanctions and Dismissals (RNSDD).
Major criticisms of the law originate from the workers union, which believes:
1. The law creates a new labor regime in the state.
2. The law did not collect the opinions of workers, who are directly involved.
3. The law restricts union rights and eliminates collective negotiation as well as the right to
strike and join a union.
4. Assessments would bring mass dismissals of workers, affecting labor stability.
5. It is unknown whether civil service salaries will be better.
6. The ability to relax the rules facilitates dismissal.
7. The law eliminates special assignments and subsidies.
Since passage of the law, the workers union has organized strikes
and mobilizations against implementation of the law, arguing that the
2 The law defines "trusted servant" (cargo de confianza) as a civil servant who is part of the direct and
immediate environment of public officials or public directors, and whose tenure in the civil service is
subject to the confidence of the person who supervises him. The number of trusted servants in no one
case should be greater than 5% of total posts provided by the institution, with a minimum of two and a
maximum of 50, with the head of the unit determining the location of trusted servants.
"There is a great fear that the law
can generate massive layoffs, but
we have repeatedly clarified that
this reform cannot be compared
with that made in the nineties.”
Nancy Laos, Minister of Labor,
July 31st, 2013.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 6
law eliminates work stability. The Minister of Labor has appeased labor unions by proposing a
series of "locks" to ensure stability required for state workers.
Encouragingly, a survey conducted between June 7-8, 2013[3] by a renowned polling company
produced the following results:
84% of the population agrees with meritocracy as the core of the reform, and 88%
supported annual evaluations of public servants.
74% approve the termination of personnel who has received negative performance
evaluations for two consecutive years.
36% have heard of this reform. Among this group, 56% approve of it. Support increases
to 78% after the components of the reform are fully explained.
According to the law, the new labor regime is meritocratic: hiring is carried out by publicized,
competitive examination, and job retention and promotion are secured through evaluations.
Perhaps the greatest error in rollout of the law was the lack of discussion to explain the scope of
the new law.
Regarding collective negotiation, the law states the following: “Collective rights of civil servants
are specified in Convention 151 of the International Labour Organization (ILO) and the
Constitution of Peru”. The law also stipulates that the right to strike is exercised after the failure of
any mechanisms for negotiation, and if workers decide to use this right, they must give 15 days of
advance notice to allow time for hiring temporary staff to ensure the provision of minimum
services.
The law does not explicitly mention dismissal as a result of evaluations. The law says that a
worker who receives a negative review, specifically "performance under observation", should be
trained; if the result of a second evaluation is again "performance under observation", the rating
will become “unsatisfactory”. However, the law does not state what will happen with employees
who receive “disapproving”.
There is currently no information on the contents of the law’s regulations. Meanwhile, union
protests continue.
1.2 Ministry of Health: Proposal on Human Resources Management
System for Health Institutions
Under the legal framework established by SERVIR and according to the Civil Service Law, public
institutions must implement their HRMS. To facilitate its implementation, the MoH has developed
a proposal for the structure of HRMS which defines subsystems, processes and functions.
The expected results of HRMS implementation in health institutions are:
a) Adequate health workers properly situated and properly performing their duties.
b) Attract and retain competent staff.
The following inputs are necessary to implement HRMS in health institutions:
a) Health policies and strategies to align staff performance.
b) Models of health care, management and health services organization to define
competency profiles, HR allocation, and HR compensation, among others.
c) Health service portfolios to define individual goals.
d) Civil Service Law as a legal framework for HRMS implementation.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 7
e) Regulation of organization and functions (ROF) to define job profiles, recruitment,
assessment, etc.
The following graph displays this structure:
Graphic 1: HRMS in health institutions: MoH proposed structure.
II. Work
Organization
Job profiles
Identification
of labor
competencies
Job Rating
III. Employment
Management
Recruitment,
selection,
incorporation
and induction
Staff mobidity
Disciplinary
process
Staff retirement
and retirement
VI. Development
Management
Career progression
Capacity building
Teaching &Service
Regulation
I. HHR Policy and Strategic PlanningHR needs, Strategies to cover HR gap
VII. Managing humanand social relationshipsOrganizational Climate and Culture; Labor relation; Workplace health, safety and
welfare.
V. Compensation
Management
Salary scales
Payroll
Benefits, bonuses,
pensions
Incentives
Health Policy
Strategies
HealthcareModel
Management Model
OrganizationalModel
Healthserviceportfolio
Civil,ServiceLaw
ROF
IV. Performance
Management
Performance
planning
Supervision
Performance
evaluation
Feedback
Plans for
Individual
performance
improvement
Having
adequate
workers,
placed in
appropriate
places, doing
well what they
have to do.
Attract and
retain
competent staff
The following subsections explain the operational definitions of each process within the HRMS for
health institutions.
1.2.1 HHR policy and strategic planning
This subsystem is primarily responsible for HRM alignment to national and regional policies;
national health strategies; and the comprehensive care model. It also enables coordination
among all HRM processes to ensure suitable and competent workers where they are needed.
The processes involved in this subsystem are:
HHR policies and strategies. This process consists of developing HRM policies and strategies
that will attract and retain competent staff.
Operational research development. It is necessary to have evidence in order to define policies
and strategies for HR management and development that are relevant and cost-effective. This
process seeks to promote research studies focused on factors that will attract and retain
competent staff as well as research to support HR policy design.
HHR information management. To ensure proper management, it is necessary to have reliable
and update-to-date HHR information at both the institutional and sectoral levels. HR observatories
are an excellent mechanism to maintain HHR quantitative information, and information system
records or specific databases, including staff competencies, performance evaluations, and
incentives, complement quantitative information. All information must be updated to allow
informed HRM decisions.
HHR management control. This process is aimed at supporting health managers at different
levels, as well as those responsible for other subsystems, in monitoring HRM indicators,

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 8
analyzing results and defining necessary corrective measures. It also includes annual evaluations
of HRMS processes and manager performance.
HHR strategic planning. This process includes all actions related to quantitative and qualitative
HHR requirements and needs at all levels in the short, medium and long term at both institutional
and sectoral levels. This process also addresses necessary actions to fill the HHR gap. HHR
planning should be closely linked and coordinated with national and regional health policies;
institutional strategies; and health provision approaches (e.g. the family health care model).
Challenges to the planning process include high internal and external migration of health workers
as well as high staff turnover.
HHR financing. This process includes the necessary actions to ensure a sufficient budget to
provide adequate HHR for proper health facility operation.
1.2.2 Work organization
This subsystem exists to optimize HHR working capacity by specifying the content of functions,
activities and tasks, as well as the staff qualifications to achieve them.
The main goal of this subsystem is to establish a set of policies and standards regarding work
specialization that forms the "job"; the job profile includes a work description, including objectives,
relationships, roles, responsibilities and working conditions; and the position requirements,
including educational background, experience and competencies. As an additional part of the job
profile, competency profiles articulate staff abilities in regard to institutional objectives, goals and
organizational culture.
The processes involved in this subsystem are:
Job profile design. Based on the "general functions" established in the institutional ROF, each
organizational unit designs its positions and the specific functions of each position. The functions
of each position are outlined in the Manual of Organization and Functions (MOF). Based on the
MOF, each unit defines its "job profile", which has two major components:
Job description: Defines the characteristics of the job, including the job title; location within the
organization; relationships with other positions, including supervisory, managerial, and
collaborative roles; purpose; functions to be performed; and working conditions (e.g physical
such as equipment; normative, as the regulatory framework to be used) for good job
performance.
Job analysis: This refers to the characteristics of ideal job candidate in relation to the job
requirements. This section establishes required academic training, experience, knowledge
and skills.
Identification of labor competencies. This process identifies specific and general competencies
for each position.
Job rating. This process analyzes and compares the contents of jobs to define their relative
importance within the organization; place them in hierarchical order as the basis of the
remuneration system; and aid in the development of career plans within health institutions. Job
design alone is not enough to trigger HRM processes and it is also necessary to rank and value
jobs in relation to their importance within the organization. The position must be assessed and not
the person who occupies it.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 9
1.2.3 Employment management
Employment management seeks to establish a set of policies and standards to optimize inflows,
movement and exit of staff in health care organizations. These policies and standards should be
based on job profiles and competencies established by the employer and should foster the
achievement of sectoral health objectives.
The processes involved in this subsystem are:
Recruitment. This process allows health care organizations, based on HHR needs identified in
the planning process, to attract candidates to participate in selection processes. The recruitment
process uses internal (within the organization) or external sources.
Selection. In this process, the institution examines whether candidates meet the job
requirements, which are described in the job profile, and then selects the candidate who has the
necessary skills for successful performance. This process also involves the formation of selection
committees and defines the criteria, standards, procedures and tools for evaluating candidates in
the selection process.
Incorporation. This process formalizes the entry of the selected candidate into health
organizations and establishes the characteristics, conditions, restrictions and penalties related to
employment. This process includes compliance with standards for each of the modalities of
incorporation (stable or contracted) and the definition of the duties and rights of HHR.
Induction. This is a general orientation process prior to the start of work activity. This process
provides basic information about the institution, including norms, policies and organizational
characteristics; explains the nature of the position; and indicates requisite functions and roles. In
addition, the new employee receives relevant information to help achieve satisfactory
performance.
Staff mobility. This process defines workplace assignment changes that HHR can perform both
inside and outside health institutions. These changes balance the needs identified in the target
unit and the availability of the worker (in the origin institutional source) as well as the worker's own
need, under current regulations. The regulation defines the types of workplace assignment
change, displacement criteria, and administrative procedures to be followed for each type of
mobility.
Management of personnel files, control of attendance. This process consists of conservation,
renovation, veracity and legality of the documents maintained by institution staff, as well as
compliance with rules for the submission of affidavits. It also includes the management and
control of the working day, permissions, holidays, leave, etc.
Administration of disciplinary process. In this process, the institution determines the level of
staff responsibility in certain administrative acts, including compliance with disciplinary procedures
in accordance with applicable regulations; the classification of fault; the design of internal rules
(reglamento interno de trabajo - RIT); and the registration and updating of the RNSDD.
Staff termination and retirement. In this process, the institution regulates the term of
employment between staff and the institution. In compliance with labor rights and under current
regulations, disengagement may be voluntary or involuntary. There are currently several forms of
disengagement: resignation, removal, dismissal, and termination, among others. This process
includes the enforcement of laws on the causes for dismissal; termination of employment
procedures and requirements; and standards and criteria for the termination of employment.
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 10
1.2.4 Performance management
The performance management subsystem aligns the strategy of the institution with the individual
objectives of HHR to continuously improve staff performance and hence institutional performance.
Performance evaluation is part of performance management, which allows each member of the
institution to know at all times specific employee expectations in terms of quantitative and
qualitative attributes for a given period. The aim of the evaluation is to establish strategies for
solving performance problems motivate employees and encourage personal development.
The performance management subsystem defines and measures competency standards and
performance targets to be achieved by health personnel in order to promote and maintain the
highest possible level of performance based on recognition of merit, ability and equal
opportunities.
Performance management is mainly aimed at establishing a set of policies and rules regarding
standards of competence and performance goals of health workers.Achievement of these goals is
linked to various incentive and personal development mechanisms, which promote continuous
improvement processes in HHR and, consequently, in health institutions.
The processes involved in this subsystem are:
Performance planning. This consists of defining competencies, standards and individual
performance goals to be achieved in line with institutional priorities, strategies and objectives.
This process also includes the definition of the methodology for performance evaluation as well as
the design of the necessary assessment tools for an objective measurement of staff competence
and compliance with established performance goals.
Supervision. This consists of continuous and systematic support to health workers to improve
their performance based on the observation that immediate supervisors do to promote continuous
improvement of skills. This process is also driven by leaders.
Performance evaluation. This consists of an objective and transparent measurement of health
staff skills and institutional goals obtained during a defined time period and following a predefined
methodology. Results should be compared to competency standards and goals established in the
performance planning process.
Feedback and design of plans for individual performance improvement. In this process,
plans are designed for individual performance improvement based on results from the
performance evaluation. Leaders define performance objectives for each employee in the
following year.
1.2.5 Development and training management
The development and training management subsystem defines practices to encourage
professional and job development opportunities by providing learning opportunities as well as
career path planning within the organization.
The processes involved in this subsystem are:
Labor advancement (promotion and career path). This process is responsible for the policies
and procedures governing HHR promotion and occupational group change within an institution. It
also manages the assumption of duties and responsibilities of greater difficulty or complexity in
comparison to the previous level. The labor process includes both horizontal progression, which is
a progression in degree, category, or step that can be established without shifting the workplace
or occupational group to which the worker belongs; and vertical progression, which is promotion
within the structure of the organization to a higher level.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 11
Capacity building. This process is responsible for providing tools and resources to facilitate
individual and collective learning and further develop staff labor competencies. The term "labor
competency" refers to the knowledge and skills demonstrated at work and reflect the worker's
contribution to the objectives of the organization.
Regulation of the teaching - service process. This process involves a set of actions needed to
articulate HHR training and education activities within health services. The teaching and service
provision relationship refers to the simultaneous occurrence of health service provision and
specialized educational opportunities for health personnel in health facilities. The dual nature of
these training areas requires the regulation and enforcement of standards to ensure the quality of
both health and education services.
1.2.6 Compensation management
Compensation management relates to remuneration provided by the organization in return for
work done.
Compensation can take several different forms: pay or base salary, which is a fixed amount that is
paid hourly or monthly; monetary and non-monetary incentives related to performance
recognition; and benefits, which are established by law and serve as additional payments
awarded by the institution.
The processes involved in this subsystem are:
Design of salary scales. This process defines salary scales based on job profile and job
classification by levels.
Management of payroll and salaries. This process manages compliance with the rules and
procedures which establish and maintain fair and equitable salary structures in the organization.
In this process, the organization defines the remunerative and non-remunerative compensation as
well as electronic payroll management: monthly payroll (Planilla Mensual de Pagos - PLAME);
registration of labor information (Registro de información laboral – T Registro); and social benefits
settlement, such as compensation for time of service (Compensación por Tiempo de Servicios -
CTS), gratuities and bonuses. This process also involves the regular registration of income, both
on the dependent category (fifth category) and the independent category (fourth category).
Administration of benefits and bonuses. This process administers extra-pay benefits including
holidays, life insurance, subsidized transportation, subsidized food and health insurance.
Incentive management. This process enforces the rules and instruments that are established
and applied by the institution to recognize worker achievements. This recognition has no
permanent wage effects and can be monetary and non-monetary.
Pension management. This process manages the recognition and granting of pensions; survival
verification; and the application of legislation for pension payment.
1.2.7 Managing human and social relations
This subsystem seeks to regulate and harmonize interactions between individuals, focusing on
the collective dimension. It includes policies and practices related to organizational climate; labor
relations; social welfare; and safety at work.
This subsystem supports all of the subsystems mentioned above and guarantees conditions
conducive to satisfactory productivity and performance.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Legal and conceptual framework for HRMS ▌pg. 12
The processes involved in this subsystem are:
Management of the organizational climate and culture. This process is aimed at maintaining
or improving the perception of collective satisfaction. Organizational climate is defined as the set
of qualities, attributes or relatively permanent properties of a particular work environment, which
are perceived, felt or experienced by workers who make up the organization. The organizational
climate influences individual behavior.
Management of labor relations. This process governs relations between the head of an
organization and social partners, including unions and associations, which represent workers or
group of workers. This process also involves collective negotiation of wages and working
conditions to appropriately manage conflicts.
Workplace health, safety and welfare. This process includes two groups of activities:
Social welfare: This activity affects the quality of life of staff and their extended family and
fosters a peaceful and enjoyable workplace experience. Social welfare programs include the
promotion of sports activities; event celebrations; cafe or restaurant services; educational
support; financial services; daycare; and care for elderly people, among others.
Health and safety at work: This activity refers to a set of rules; procedures; and technical,
educational, medical and psychological measures to protect employees’ physical and mental
integrity. These measures prevent health risks inherent to job tasks and the physical working
environment. This activity also seeks to diagnose and prevent occupational diseases based
on the study of two variables: man and his work environment.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 13
2. Assessment of the Human Resources Management System
In 2012, the Program for Health Reform Support (Programa de Apoyo a la Reforma del Sector
Salud – PARSALUD II) led the development of a technical report entitled "Developing a Health
Model for Decentralized Regional HRMS: Ayacucho, Cajamarca, Cusco, Huanuco and Ucayali
and their Respective Action Plans"[4]. This document includes a diagnosis of HRMS performance
at various levels of management, including the Regional Health Directorate (RHD), networks,
micro-networks and hospitals. Both PARSALUD II and the project developed the HRMS
diagnosis, which was based on the HRMS structure as defined by the MoH. To gather the
information, PARSALUD II designed a survey for examining each of the subsystems defined by
the MOH.
The project reviewed PARSALUD II’s survey and incorporated the latest developments in the
HRMS structure. The project also worked with the MoH to expand the survey to examine all
processes involved in the HRMS.
In this chapter, the methodology developed by the project to gather information in San Martin
Regional Health Directorate (SMT-RHD) will be presented. In addition, the results of the survey
conducted in SMT-RHD for each of the HRMS processes will also be presented.
Based on the PARSALUD II technical report, a comparative chart was compiled to display each
subsystem’s operations in regions where PARSALUD II works.
Since the instruments used by PARSALUD II and the project are different, the results are not
comparable. Given this, the project gathered information from Cajamarca using the instruments
applied in San Martin to compare results obtained. This comparison is presented in a table
showing the performance of HRMS in these two regions.
2.1 Performance Evaluation of the Entire HRMS in Health Institutions
2.1.1 Tools and methodologies to assess HRMS implementation
In order to gather the necessary information to determine the level of HRMS implementation, the
project employed the following tools, which were developed by the USAID Peru Health Policy
Project:
a) A list of questions for each of the processes in each HRMS subsystem3.
The questionnaire consists of several closed questions whose answers are YES or NO. The
following are several examples:
3 See the questionaire in Annex 7.1

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 14
1. Does your institution have human resources management and development policies? ( ) YES ( ) NO
If the answer is yes, please answer the following questions. Otherwise, skip to the next section. 2. Are the human resources management and development approved?
( ) YES ( ) NO
……
Do you have the specifics of at least 60% of job the profiles for the following levels written down?
Question N°
Level 60% of job profiles
YES NO
1 Regional Health Directorate
2 Network
3 Operational Office
4 Micro-network
……
There are also open questions that allow qualitative information or more specific information,
including the following examples:
According to the current ROF, which governing bodies are involved in estimating human resource
requirements and design staffing plans in your institution?
Level Is involved? In case of participating
YES NO Name of the responsible body Specific function
RHD
Network
Micro-network
In relation to the selection process conducted during the past year, provide the following information:
Month # Days to publicize the
vacancy
Results of selection process
Achieved Invalid Process with
objections
……
b) A spreadsheet to record the answers of every closed question.
The spreadsheet immediately allows the aggregation of results into tables and graphs for
easy analysis. Additionally, each question has been weighted according to its strategic
importance in proper HRMS functioning.
The project used the following ratings to analyze the results:
High development: > 80% complete
Moderate development: 40% - 80% complete

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 15
Little Development: <40% complete
The processes considered in the analysis were identified by the MoH as important to include.
Table 2: Key processes for each HRMS subsystem in health institutions.
Subsystem Key Processes
HHR policy and strategic planning Policies and strategies for HHR management and development
Development of operational research
HHR information management
HHR management control
HHR strategic planning
HHR financing
Work organization Design of job profiles
Identification of labor competencies
Job rating
Employment management Recruitment, selection, incorporation and induction
Staff mobility
Management of personnel files, control of attendance
Administration of disciplinary process
Staff termination and retirement
Development and training management Labor advancement (promotion and career path)
Capacity building
Regulation of the teaching-service process
Performance management Performance planning
Supervision
Performance evaluation
Feedback and design of plans for individual performance
improvement
Compensation management Design of salary scales
Management of payroll and salaries
Administration of benefits and bonuses
Incentive management
Pension management
Managing human and social relations Management of the organizational climate and culture
Management of labor relations
Workplace health, safety and welfare
To gather information on the implementation of the HRMS in SMT-RHD, the director of the HR
Management Directorate developed a workshop for responsible parties of HRM processes at
different organizational levels.
Working groups were formed to analyze each subsystem. The project made a conceptual
presentation of the processes in each subsystem for each working group to facilitate
understanding of survey questions.
2.1.2 Human Resources Management System in SMT-RHD
The new organizational structure of SMT-RHD[5] has considered the functioning of two normative
units, which must maintain close coordination, to lead HRMS implementation:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 16
Human Resource Management and Development Directorate (HRM Directorate) - This body
executes exclusive regulatory functions in HHR management and is primarily responsible for
the following subsystems: policy and planning; work organization; performance management;
development and training management; and some processes related to compensation and
labor relations management.
Operations Directorate – This body manages regulatory functions for all administrative
systems, including personnel administration. It is primarily responsible for the job
management subsystem and some processes of compensation and labor relations
management.
The implementing units of HRMS are:
Health networks, which are responsible for implementing the processes regulated by the
HRM Directorate.
Operations Offices, which are responsible for implementing the processes regulated by the
Operations Directorate.
These inter-relationships are presented in the following graph:
Graphic 2: Staff of the Human Resources Management and Development Directorate:
Number of workers by labor regimen, San Martin 2013.
HRMS Governing at regional level
Responsible for HR development processes
Responsible for personnel administration processes
No
Regional Health Directorate
Office of Sectoral Legal
Consulting
Office of Planning and
Health
Intelligence
Comprehensive Health Direction
Department of Regulation and Control in Health Sector
Directorate of Human Resource Development
Operations Management -Health
Operations Offices (05)
Health Networks
Management (10)
Hospitals and Regional Services
Administrative Management Unit
Budget Management Unit
Referential Hospital Tarapoto
Referential Laboratory
Blood Bank
Regional Management of Social Development
REGIONALGENERAL MANAGEMENT
Regional Office of Planning and Busget
Regional Office of Legal Consulting
Regional Office of Regional Defense ad Disaster Risk Management
Regional Office of Administration
Persons Management Office
Accounting and Treasury Office
Logistics Office
Estate Control Office
Office of information Technology
Normative Units Implementing Units
SOURCE: SMT technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 17
The new ROF is currently under implementation so the region’s units are not fully deploying their
functions. As of July 2013, the HRM Directorate only has five employees, including four
professionals and one technician; two of the professionals have permanent positions, while the
other staff members were hired through an administrative services contract (Contrato
Administrativo de Servicios – CAS)[6]. The quantity and composition of staff members is
insufficient to lead, regulate, monitor and control the implementation of HRM processes.
Table 3: HRM Directorate staff: Number of workers by labor regimen, San Martin 2013.
Occupational group Total 276
Regimen
728
Regimen CAS
Full-time
independ
ent
contracto
r
Other
Professional 4 2 0 2 0 0
Administrative Technician 1 0 0 1 0 0
Administrative Assistant 0 0 0 0 0 0
TOTAL 5 2 0 3 0 0
SOURCE: SMT technical report
Listed below are results from the diagnostic tools.
Graphic 3: Results for each subsystem, San Martin 2013.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Sub-System: HHR Policy and Strategic Planning
Sub-System: Work Organization
Sub-system: Employment Management
Sub-System: Development and
Training Management
Sub-System: Performance Management
Sub-System: Compensation Management
Sub-System: Managing human and social
relations
San Martin: HRMS in Health Institutions
SOURCE: SMT technical report[7]

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 18
Table 4: Results for each subsystem, San Martin 2013.
Human Resource Management System % complete Result
Subsystem: HHR policy and strategic planning 65.0% Moderate development
Subsystem: Work organization 32.0% Low development
Subsystem: Employment management 37.5% Low development
Subsystem: Development and training management 62.2% Moderate development
Subsystem: Performance management 14.0% Low development
Subsystem: Compensation management 57.7% Moderate development
Subsystem: Managing human and social relations 64.3% Moderate development
HUMAN RESOURCE MANAGEMENT SYSTEM 47.5% Moderate development
SOURCE: SMT technical report
Table 4 shows that SMT-RHD has, on average, achieved a 48% progress rate in HRMS
implementation.
The subsystems that are more developed include HHR policy and strategic planning; managing
human and social relations; and development and training management. On the opposite end, the
performance management subsystem is the least developed.
2.1.3 Human Resources Management System in other regions
Graphic 4: Results for each subsystem, Cajamarca 2013.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Sub-System: HHR Policy and Strategic Planning
Sub-System: Work Organization
Sub-system: Employment Management
Sub-System: Development and
Training Management
Sub-System: Performance Management
Sub-System: Compensation Management
Sub-System: Managing human and social
relations
Cajamarca HRMS
SOURCE: Cajamarca technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 19
Table 5: Results for each subsystem, Cajamarca 2013.
Human Resources Management System % completed Result
HHR policy and strategic planning 48.0% Moderate development
Work organization 10.0% Little development
Employment management 35.0% Little development
Development and training management 29.6% Little development
Performance management 1.8% Little development
Compensation management 57.7% Moderate development
Managing human and social relations 21.4% Little development
Human Resources Management System 29.1% Little development
SOURCE: Cajamarca technical report
Table 5 shows that Cajamarca has not reached optimal levels for proper HRM. The weaker
subsystems include performance management; work organization; and management of human
relations. These weaknesses are concerning since these subsystems are integral to achieving the
objectives, goals and outcomes of the health care model in the region.
Regional management documents are outdated and are not aligned with the decentralization
process, much less with the current care model. Given this situation, processes within the HR
policy and strategic planning subsystem have not been developed.
Comparative chart
The project created a table of results obtained by PARSALUD II from Ucayali, Cusco, Ucayali,
Cajamarca and Huánuco to compare RHD performance on HRMS implementation. Other results
from Cajamarca and San Martin, which were obtained by applying diagnostic tools designed by
the project, are also included to make additional comparisons.
Analysis of some processes has not been considered in the PARSALUD II evaluation because
the information is too qualitative.
To elaborate this matrix, the project examined information from the PARSALUD II technical
report4 to compare the results and formulated the following conclusions:
All PARSALUD II RHDs, with the exception of Ucayali which shows little development in all
subsystems, show the same results in each of the subsystems.
PARSALUD II survey does not cover all processes in its analysis.
The project’s survey explores in greater detail HRMS processes. Comparing Cajamarca
results from both surveys, differences in application, analysis and results are apparent.
By comparing San Martin and Cajamarca performance with the application of HP project
survey, better results are apparent in San Martin in all the subsystems.
4 See the results of qualitative assessmemnt in PARSALUD regions in Annex 7.2

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 20
Table 6: Comparative table of HRMS level of implementation in six regions.
N.c.= Not considered in PARSALUD II assessment; N.i.= No information
HRMS Ucayali * Cusco * Huanuco
*
Cajamarc
a*
Ayacuc
ho * San Martín **
Cajamarca
**
HHR policy and strategic planning
65% Moderate 48%
Modera
te
Policies and strategies for HHR
management and development N.c. N.c. N.c. N.c. N.c. 73% Moderate 0% Little
Development of operational
research N.c. N.c. N.c. N.c. N.c. 0% Little 0% Little
HHR information management Little Little Little Little Little 76% Moderate 90% High
HHR management control
N.c. N.c. N.c. N.c. N.c. 0% Little 50%
Moderat
e
HHR strategic planning Little Little Little Little Little 82% High 57%
Moderat
e
HHR financing
N.c. N.c. N.c. N.c. N.c.
100
% High 86% High
Work organization 32% Little 10% Little
Design of job profiles Little Moderate Moderate Moderate
Moderat
e 38% Little 18% Little
Identification of labor competencies Little Moderate Moderate Moderate
Moderat
e 38% Little 0% Little
Job rating N.c. N.c. N.c. N.c. N.c. 10% Little 0% Little
Employment management 37% Little 36% Little
Recruitment, selection,
incorporation and induction Little High High High High 38% Little 38% Little
Staff mobility N.i. N.i. N.i. N.i. N.i. 0% Little 0% Little
Management of staff files and
attendance control N.c. N.c. N.c. N.c. N.c. 40% Moderate 25% Little
Administration of disciplinary
process
N.c. N.c. N.c. N.c. N.c. 43% Moderate 43%
Moderat
e
Staff termination and retirement Little Little Little Little Little 0% Little 67%
Moderat
e
Development and training
management 60% Medium 30% Little
Labor advancement (promotion and
career path) Little Moderate Moderate Moderate
Moderat
e 76% Moderate 19% Little
Capacity building Little Little Little Little Little 58% Moderate 40% Little
Regulation of the teaching & service
process
N.c. N.c. N.c. N.c. N.c. 35% Little 30% Little
Performance management 14% Little 2% Little
Performance planning Little Little Little Little Little 16% Little 12% Little
Supervision Little Little Little Little Little 0% Little 0% Little
Performance evaluation Little Little Little Little Little 22% Little 0% Little
Feedback and design of plans for
individual performance improvement
N.c. N.c. N.c. N.c. N.c. 0% Little 0% Little

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of the Human Resources Management System ▌pg. 21
HRMS Ucayali * Cusco * Huanuco
*
Cajamarc
a*
Ayacuc
ho * San Martín **
Cajamarca
**
Compensation management 61% Moderate 58%
Modera
te
Design of salary scales Little Little Little Little Little 63% Moderate 41%
Moderat
e
Management of payroll and salaries Little Little Little Little Little
100
% High
100
% High
Administration of benefits and
bonuses Little Little Little Little Little
100
% High
100
% High
Incentive management Little Little Little Little Little 44% Moderate 56%
Moderat
e
Pension management Little Little Little Little Little
100
% High
100
% High
Managing human and social
relations 70% Moderate 21% Little
Workplace health, safety and
welfare Little Little Little Little Little 63% Moderate 34% Little
Management of labor relations N.i. Moderate Moderate Moderate
Moderat
e
100
% High 22% Little
Management of the organizational
climate and culture Little Little Little Little Little 69% Moderate 29% Little
HUMAN RESOURCES
MANAGEMENT SYSTEM
48% Moderate 29% Little
SOURCE: (*) PARSALUD II technical report. (**) HP project assessment.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 22
2.2 HHR Policy and Strategic Planning: Progress
2.2.1 Results of the assessment in San Martin Regional Health Directorate
The following graph shows the results of five of the processes that are within this subsystem.
On average, implementation of this subsystem is 65% completed, which indicates “moderate
development”.
It has been noted that some processes are not working, including development of operational
research and HHR management control.
According to what was reported, HHR financing is functioning adequately.
Graphic 5: San Martin HHR policy and strategic planning: Results by key processes.
0%10%20%30%40%50%60%70%80%90%
100%
Policies and Strategies for
HHR Management …
Development of
operational research
HHR information management
HHR
Management Control
HHR Strategic Planning
HHR Financing
San Martin: HHR Policy and Strategic Planning
SOURCE: SMT technical report
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 23
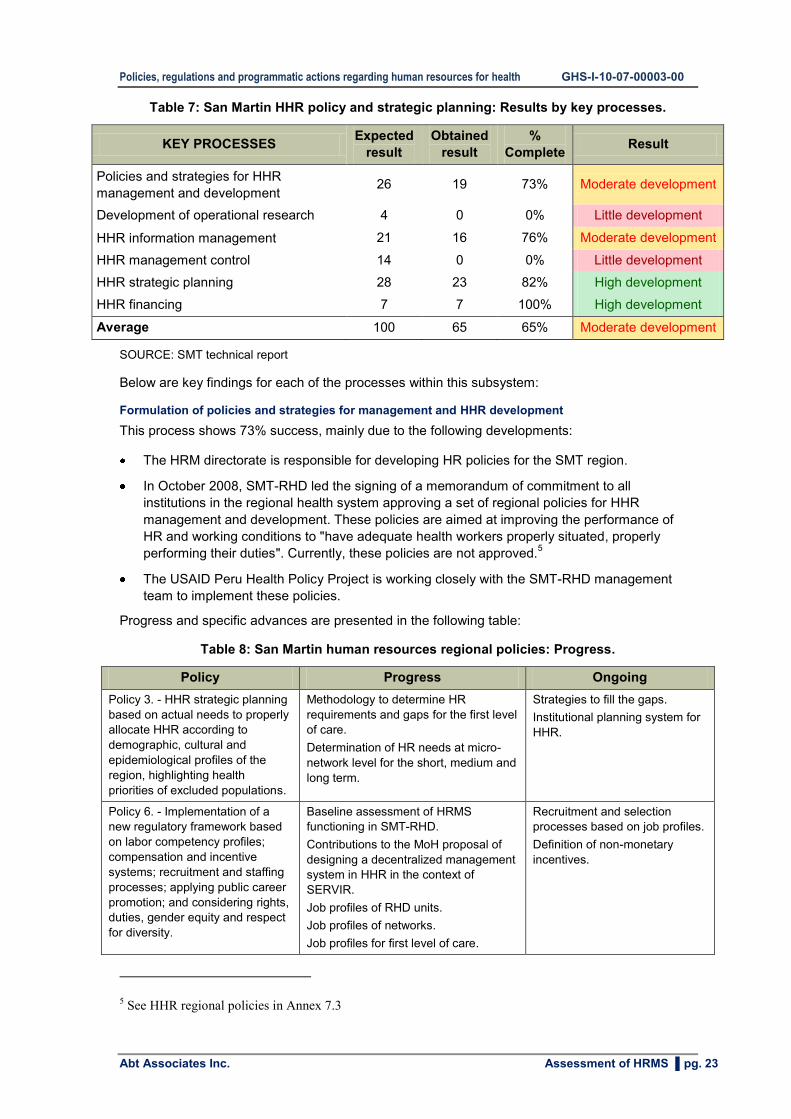
Table 7: San Martin HHR policy and strategic planning: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Policies and strategies for HHR
management and development 26 19 73% Moderate development
Development of operational research 4 0 0% Little development
HHR information management 21 16 76% Moderate development
HHR management control 14 0 0% Little development
HHR strategic planning 28 23 82% High development
HHR financing 7 7 100% High development
Average 100 65 65% Moderate development
SOURCE: SMT technical report
Below are key findings for each of the processes within this subsystem:
Formulation of policies and strategies for management and HHR development
This process shows 73% success, mainly due to the following developments:
The HRM directorate is responsible for developing HR policies for the SMT region.
In October 2008, SMT-RHD led the signing of a memorandum of commitment to all
institutions in the regional health system approving a set of regional policies for HHR
management and development. These policies are aimed at improving the performance of
HR and working conditions to "have adequate health workers properly situated, properly
performing their duties". Currently, these policies are not approved.5
The USAID Peru Health Policy Project is working closely with the SMT-RHD management
team to implement these policies.
Progress and specific advances are presented in the following table:
Table 8: San Martin human resources regional policies: Progress.
Policy Progress Ongoing
Policy 3. - HHR strategic planning
based on actual needs to properly
allocate HHR according to
demographic, cultural and
epidemiological profiles of the
region, highlighting health
priorities of excluded populations.
Methodology to determine HR
requirements and gaps for the first level
of care.
Determination of HR needs at micro-
network level for the short, medium and
long term.
Strategies to fill the gaps.
Institutional planning system for
HHR.
Policy 6. - Implementation of a
new regulatory framework based
on labor competency profiles;
compensation and incentive
systems; recruitment and staffing
processes; applying public career
promotion; and considering rights,
duties, gender equity and respect
for diversity.
Baseline assessment of HRMS
functioning in SMT-RHD.
Contributions to the MoH proposal of
designing a decentralized management
system in HHR in the context of
SERVIR.
Job profiles of RHD units.
Job profiles of networks.
Job profiles for first level of care.
Recruitment and selection
processes based on job profiles.
Definition of non-monetary
incentives.
5 See HHR regional policies in Annex 7.3

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 24
Policy Progress Ongoing
Salary scale for staff employed in first-
level-of-care facilities.
Policy 2. - Managing training
processes linked to institutional
development projects using the
“Continuing Education in Health”
(Educación Permanente en Salud
– EPS) and competencies
approach to strengthen job
performance, characterized by
respect for rights, gender equity
and cultural relevance of the
population.
Definition of RHD management
competencies to assume functions
transferred in the decentralization
process.
Definition of managerial competencies
for networks.
Proposal for job performance
evaluation of network management
teams based on job competencies.
Implement a job performance
evaluation system of network
management teams based on
individual goals and job
competencies.
SOURCE: SMT technical report
Despite advances in the design and implementation of regional HR policies, problems that have
been encountered in this process are outlined in the following table:
Table 9: Constraints in the formulation of policies and strategies for HHR management and
development. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
HR policies have not been
approved.
Designed policies have nothing
explicitly related to health and
safety at work.
There are aspects of designed
policies which are not yet
implemented, including skills
development; motivation and
incentives; and workplace
health, safety and welfare.
Changes in regional authorities
slow the approval process.
This aspect was not prioritized
at the outset due to lack of
information and awareness
regarding its importance.
Lack of a policy framework and
competent teams to design
policy implementation
strategies.
Lack of a regulatory
framework for HHR
actions in RHD.
Administrative
sanctions for failure to
comply.
Review and update
policies to bring into
alignment with Civil
Service Law.
SOURCE: SMT technical report
The Civil Service Law includes the following statement to describe one function of the HR office or
corresponding body:
"Develop guidelines and policies for the development of a personnel management plan and the
optimal functioning of the HRM, including the application of performance indicators."
Development of operational research
Unfortunately, this process has not progressed, despite the existence of a national research
agenda for HHR problems for 2011-2014, which was approved on March 18, 2011 by ministerial
resolution.6
Problems encountered during this process are included in the table below.
6 See the national agenda for HHR research in Annex 7.4

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 25
Table 10: Constraints in the development of operational research. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
Neither HRH
investigations nor a
diagnostic assessment
of the HRH situation in
the region have been
carried out.
The lack of research and
diagnostics is mainly due to
the lack of a responsible party
to promote this work. The
diagnosis is not taken into
account when making
decisions.
Authorities do not give due
importance to this process.
HRM directorate has little
capacity for HRM: staff must
assume multiple roles and
cannot specialize in research
issues.
Due to the lack of research, there
is no evidence to support the need
for policies and strategies to
improve HRM and staff
performance.
Based on HRMS
diagnosis, identify
research topics to
be co-financed with
the central level.
SOURCE: SMT technical report
HHR information management
Progress in this process is 76%, which is deemed “moderate development”.
According to current ROF, the HRM directorate is responsible for maintaining HR information. To
accomplish this, the institution employs official reporting systems to record information on HR
employment.
Key informants report that they use the information from these systems to make decisions.
The weaknesses identified in this process are included in the following table.
Table 11: Constraints in HHR information management. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
Current information
systems do not register
non-remunerative items;
staff attendance,
tardiness and absences;
public tenders; current
allocation of each
worker; or personnel
files.
They use MEF reporting
applications (payroll system,
SIGA), but this data is
insufficient for decision
making and comprehensive
analysis.
This is because the RHD
does not define the type of
information they need for
relevant and timely decisions.
Insufficient information is
recorded to make decisions.
By not knowing the allocation of
workers, health networks are
hiring staff where they are not
needed. Operational units do
not report to the RHD about
public tenders they perform.
Define HRM issues to
monitor at all levels.
Develop reporting
systems; flow charts;
and collation and
analysis of required
information.
SOURCE: SMT technical report
HHR management control
No progress has been achieved in this process.
According to the current ROF, there is no party responsible for this process although it is noted as an important function of HR offices in the Civil Service Law.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 26
"Develop guidelines and policies for the development of people management plan and the optimal HRM functioning, including the application of performance indicators."
The weaknesses identified in this process are included in the table below.
Table 12: Constraints in HHR management control. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
A responsible party has
not been defined to
manage this key
function, which is
explicitly mentioned in
the Civil Service Law.
Indicators for HRM have
not been defined.
RHD does not perceive
the need to monitor HRM
indicators.
Due importance is not
given to this process.
Insufficient staff to
implement HRM
processes, and current
staff must execute
multiple roles and cannot
specialize.
RHD and operational units
do not measure progress
in HRMS implementation
in order to improve them.
Form an ad hoc
committee to define
indicators and
procedures for
collecting, recording,
measuring and
periodically analyzing
results.
Strengthen capacities of
the committee to monitor
indicators.
SOURCE: SMT technical report
The HP project survey tool defines a set of HRM indicators that can be reviewed to establish a
HRMS monitoring plan in SMT-RHD.
PROPOSED INDICATORS OF HUMAN RESOURCE MANAGEMENT
% of micro-networks that have HR needs estimation
% of units that have job profiles7
% of contracts signed after a meritocratic selection process
% of vacancies that have been published on the website of the Ministry of Labor
% of recruitment and selection processes that have been made based on job profiles
% of training conducted on the basis of a performance gap
% of workers who have agreed output targets
% of workers who have been assessed by competencies
% of workers who have been hired in remote areas, based on an attractive pay scale
HHR strategic planning
Progress in this process is 82%, which is deemed “high development”.
This high level of achievement is based on the following actions:
According to the current ROF, the HRM directorate is responsible for this process.
Last year, the RHD made calculations of HHR requirements and needs at the first level of
care.
7 The standard suggested to be fulfilled is at least 80%.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 27
To estimate HHR needs, SMT-RHD considered population growth; an increase in functions;
expected increase in production; effective demand projections; and health service use
projections.
To make accurate calculations, SMT-RHD used a spreadsheet prepared by the project and
an application designed by the MoH. The MoH application includes the same criteria as the
project spreadsheet.
According to key informants, these results are used for hiring purposes to justify the need for
an increased budget and request more Civil Health Service in Rural and Marginal Urban
Areas (Servicio Rural y Urbano Marginal en Salud - SERUMS) positions.
SMT-RHD has a staffing plan for the medium term. Unfortunately, recent staff turnover in the
RHD management team has delayed the plan’s revision by the new team. Additionally, the
HRM directorate has insufficient staff to perform all assigned tasks.
The weaknesses identified in this process are included in the table below.
Table 13: Constraints in HHR strategic planning. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
In spite of having a
party responsible for
estimating HR needs
and an application to
calculate needs, there
is no updated
information on current
staffing.
The MoH has provided an
application to facilitate
accurate calculations.
Micro-networks do not
regularly report information on
staff allocation and levels
because they are not required
to do so. Additionally, there is
no mechanism to allow this
information to flow from the
bottom up, at least quarterly.
HR gaps cannot be
estimated due to
unreliable information on
current staffing.
High risk of overstaffing
or misallocation.
Develop a staff
information mechanism
to periodically flow from
the bottom up to identify
needs; this mechanism
could be included in the
MOF that is being
designed.
SOURCE: SMT technical report
According to the Civil Service Law, all HRM offices in the public sector must execute the following
function:
"Study and analyze the quantitative and qualitative staffing of public institutions according to institutional needs."
HHR financing
Progress in this process is 100%, which is deemed “high development”.
This level of achievement is due to the following actions:
There is a body responsible for managing this process.
According to key informants, last year the SMT-RHD estimated HHR funding needs and
generated calculations based on the number of unfilled positions of contracted staff under
CAS mode; HR needs evaluation; implementing units’ requirements; and the historical
budget.
The SMT-RHD designed proposals to finance hospitals and SERUMS staff.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 28
2.2.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 14: HHR policy and strategic planning: Performance in four regions at different
levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD No HRM plan, so
HRM is reactive.
HRM office activities
are focused on a
short-term
administrative
aspects instead of
integrated HRM .
Personnel files are
incomplete.
RHD has an HR
management plan
but has insufficient
information.
RHD has developed
HHR gap analysis
based on the MoH’s
Health Information
System (HIS) but
did not consider
qualitative
information.
HRM office
activities are
focused on short-
term administrative
aspects instead of
integrated HRM.
Poor allocation of
computing
resources. No
systematic updating
of information in
personnel files.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on short-
term administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HRM.
Personnel files are
incomplete.
Network No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan, so
HRM is reactive.
Poor allocation of
computing
resources.
No systematic
updating of
information in
personnel files.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on short-
term administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
Micro-
network
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete. There is
a notable shortage
of HR in the HRM
office.
No HRM plan, so
HRM is reactive.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on short-
term administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 29
Institution Ucayali Cusco Huánuco Ayacucho
Hospital Has an incomplete
HRM plan.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan.
Poor allocation of
computing
resources.
No systematic
updating of
information in
personnel files.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on short-
term administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
No HRM plan, so
HRM is reactive.
HRM office activities
are focused on
short-term
administrative
aspects instead of
integrated HR
management.
Personnel files are
incomplete.
SOURCE: PARSALUD II technical report
PARSALUD II qualitative information shows poor development in the HHR policy and planning
subsystem, especially in the capacity to determine HHR requirements and manage HHR
information.
Regarding Cajamarca RHD, the project will present the results of the assessment using HP
project methodology and instruments.
Graphic 6: Cajamarca HHR policy and strategic planning: Results by key processes.
0%10%20%30%40%50%60%70%80%90%
100%
Policies and Strategies for HHR Management and
Development
Development of operational
research
HHR information management
HHR Management Control
HHR Strategic Planning
HHR Financing
Cajamarca: HHR Policy and Strategic Planning
SOURCE: PARSALUD II technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 30
Table 15: Cajamarca HHR policy and strategic planning: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Policies and strategies for HHR
management and development 26 0 0% Little development
Development of operational research 4 0 0% Little development
HHR information management 21 19 90% High development
HHR management control 14 7 50% Moderate development
HHR strategic planning 28 16 57% Moderate development
HHR financing 7 6 86% High development
Average 100 48 48% Moderate development
SOURCE: Cajamarca technical report
The table below presents the findings for each of the processes in this sSubsystem.
Table 16: Constraints in HHR policy and strategic planning. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Policies and
strategies for
HHR
management and
development
Lack of HRM policies and
strategies.
Some authorities do
not know the scope of
HR planning while
others show a lack of
interest. In addition,
the MoH does not
provide TA to help
regions develop
HRM.
Personnel
disorganized.
Lack of interest
and institutional
commitment to the
objectives.
Formulate a
comprehensive proposal
for HRM with TA from the
MoH.
Development of
operational
research
Operational research is
conducted in an isolated
manner with little
monitoring of RHD.
There is no research
unit in the Cajamarca
RHD to promote and
monitor the
development of
research.
Lack of research
hinders progress
of health sector
development in
Cajamarca.
Create a research unit
with competent staff.
HHR information
management
Cajamarca has a matrix
that identifies the
allocation of health
personnel in each
service.
There is a
responsible party in
each health network
to monitor the
availability of staff in
health facilities.
The availability of
information about
the location of HR
facilitates the
identification of
HHR gaps.
Specify in detail some
aspects of the actual and
current location of staff,
as well as the temporary
movement to other
facilities.
HHR
management
control
Absent or weak HRM
control.
HR offices in health
networks have little
support from RHD
and do not have
access to training.
These offices do not
exercise their
authority in HRM.
Staff do not fulfill
their duties and
are sometimes
absent or
unavailable.
HR offices must exercise
greater control, authority
and respect for the rules
of HHR control.
HHR strategic
planning
Lack of HHR strategic
planning.
Recently, some HHR
plans are being
implemented.
Cajamarca RHD has
Unavailability of
appropriate staff
in the right place.
Implementation and
strengthening of an
adequate HHR strategic
plan.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 31
Key Process Problem Constraint Consequences Proposal for
improvement
defined HR gaps.
There is a plan of
action to close HHR
gaps, among other
issues related to HR
planning.
HHR financing Cajamarca RHD has
sufficient budget to
ensure staff salaries, but
there are old debts to be
paid from the arbitrary
and non-technical
distribution of staff
bonuses and incentives
granted by the state.
No constraints
reported.
Personnel receive
remuneration
according to work
assignment.
Continuous monitoring of
budget availability, and
design of a proper
financial plan to include
budget needs of both
stable and hired staff.
SOURCE: Cajamarca technical report
2.3 Work Organization: Progress
2.3.1 Results of the assessment in San Martin Regional Health Directorate
The following graph shows the results of three processes included in this subsystem.
On average, this entire subsystem has only achieved a 32% progress rate, which is deemed “little
development”.
In general, all processes have increased but with "little development".
According to key informants, processes exhibiting slight improvements are associated with job
profiles definitions and competencies design.
Graphic 7: San Martin work organization: Results by key processes.
0%
20%
40%
60%
80%
100%
Design of jobs
profiles
Identification of
labor competencies
Job rating
San Martin: Work Organization
SOURCE: SMT technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 32
Table 17: San Martin work organization: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Design of job profiles 56 21 38% Little development
Identification of labor competencies 24 9 38% Little development
Job rating 20 2 10% Little development
Average 100 32 32% Little development
SOURCE: SMT technical report
More specific findings on each of the processes are listed below.
Design of job profiles
This process shows a 38% achievement rate due to the following developments, among others:
Technical team members have utilized the following documents: Staffing Table 2013 (Cuadro
de Asignación de Personal – CAP); MOF 2006; and Staff Budget 2012 (Presupuesto Analítico
de Personal – PAP).
According to CAP 2013, the number of stable staff is less than the number authorized in the
CAP. However, the total number of workers, both stable and hired, exceeds the quantity
allocated in the CAP. Therefore, contracted staff exceeds the authorized number.
Job profiles have been created for 60% of the positions in SMT-RHD organizational units.
To design the specific functions of each position, the SMT technical team referenced the opinion
of experts and general functions established in the ROF. To define the position requirements, the
team considered the regional labor market situation, the complexity of the functions and the
importance of the position. However, designed job profiles have not yet been officially approved.
Despite advances in this process, problems have been encountered and are summarized in the
table below.
Table 18: Constraints in the design of job profiles. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
SMT-RHD has not
assigned the task of job
profile design to a
specific group in the
institution. The ROF also
does not specify a
responsible party for this
task.
The design of job
profiles is not based on
the Procedures Manual
(Manual de procesos –
MAPRO) because SMT-
RHD does have not one.
There is an institutional
MOF from 2006 that
does not correspond to
the current
organizational structure;
Since stripping the National
Institute of Public
Administration (INAP) of its
role as HRMS policy maker,
there has been a loss of
interest in following HRMS
regulations. With the entrance
of SERVIR, regulations are
being reviewed and important
tasks are being identified,
including job profile design.
Lack of awareness of the
importance in managing
MAPRO, which identifies all
procedures for operational
management of the
organization. These
procedures present the
functional tasks for specific
The lack of job profiles
and unclear technical job
requirements negatively
affects the recruitment
process.
Remuneration is linked to
the person and not to the
specific profile.
The disuse of MAPRO
results in overlapping
functions, shared
responsibilities and
duplicate subordinated
functions.
Due to the outdated MOF,
workers have no effective
responsibility for the tasks
performed.
Assign this process to
an appropriate party.
Appoint a committee to
develop and
institutionalize
MAPRO.
Appoint a commission
to assume
development of a MOF
aligned to ROF and
CAP.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 33
Problem Constraints Consequences Proposal for
improvement
specific roles are
outdated.
positions.
A new ROF necessitates
amending other documents,
including MOF, CAP, PAP,
MAPRO, and job profiles.
SOURCE: SMT technical report
The Civil Service Law explicitly states the HR office or corresponding body should perform the
following function[1]:
"Manage Job Profiles."
Identification of labor competencies
This process has reached a 38% achievement rate, due largely to SMT-RHD progress since
January 2013 in designing competency profiles for the first level of care as well as for managerial
and administrative positions. In designing the profiles, the technical team is referencing the
Competencies Dictionary and MoH-designed competencies and consulting with experts.
Despite advances in this process, problems have been encountered and are summarized in the
table below.
Table 19: Constraints in the identification of labor competencies. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
There is no party
responsible for defining
the competency profile
since the current ROF
does not consider the
subject.
HRM based on
competencies is not well
developed in the public
sector, which could
contribute to
implementation failure in
the regional governments.
Weakly designed job
profiles without including
competencies would result
in hiring people without
identifying their skills.
Hire an external consultant
to apply competency
profiles in HRMS
processes.
SOURCE: SMT technical report
Job rating
This process has achieved a 10% progress rate due mostly to the development of job profile assessment processes at the micro-network level.
Despite advances in this process, problems have been encountered and are summarized in the
table below.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 34
Table 20: Constraints in job rating. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
In the current ROF, there
is no party responsible for
assessing job profiles.
Lack of awareness as to
the importance of
evaluating job positions to
design equitable salary
scales and career plans.
Compensation could not be
assigned in a fair and
equitable manner.
Demotivated staff could
weaken institutional
achievements.
Assign a person or
appoint a committee to
be responsible for
assessing job profiles
and rating.
SOURCE: SMT technical report
2.3.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 21: Work organization: Performance in four regions at different levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD Has updated
management
records but poorly
defined in some
cases.
Possesses all
management
records but with
incomplete
information.
Has designed CAS
job profiles.
RHD refers to
having designed
competencies, but
they only define
knowledge which is
part of a
competency.
Has management
documents
developed in 2006.
Has management
documents
developed in 2006.
Network Networks either do
not possess
management
documents or they
are outdated.
Functions and
responsibilities are
not uniform among
networks.
Possesses all
management
documents but with
incomplete
information.
Have developed
models to design
MOF at network
level.
They use Cusco
RHD job profiles to
hire network staff.
All networks have
management
documents, but they
are outdated.
Functions and
responsibilities are
not uniform among
networks.
All networks have
management
documents, but they
are outdated.
Functions and
responsibilities are
not uniform among
networks.
Micro-
network
Micro-networks
either do not
possess
management
documents or have
outdated versions.
Functions and
responsibilities are
not uniform among
micro-networks.
Micro–networks
either do not
possess
management
documents or have
outdated versions.
Functions and
responsibilities are
not uniform among
micro-networks.
Micro–networks
either do not
possess
management
documents or have
outdated versions.
Functions and
responsibilities are
not uniform among
micro-networks.
Micro–networks
either do not
possess
management
documents or have
outdated versions.
Functions and
responsibilities are
not uniform among
micro-networks.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 35
Institution Ucayali Cusco Huánuco Ayacucho
Hospital Hospitals either do
not possess
management
documents or have
outdated versions.
Not all hospitals
have the entire
range of
management
documents, but if
they do, these
documents do not
contain complete
information.
The majority uses
Cusco RHD hired
staff job profiles.
All have
management
documents.
All have
management
documents.
SOURCE: PARSALUD II technical report
PARSALUD II qualitative information shows poor development in the design of job profiles.
Additionally, all regions have outdated management documents.
Regarding Cajamarca RHD, the results of the project’s assessment using HP project
methodology and instruments are below.
Graphic 8: Cajamarca work organization: Results by key processes.
0%
20%
40%
60%
80%
100%
Design of jobs
profiles
Identification
of labor
competencies
Job rating
Cajamarca: Work Organization
SOURCE: Cajamarca technical report
Table 22: Cajamarca work organization: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Design of job profiles 56 10 18% Little development
Identification of labor competencies 24 0 0% Little development
Job rating 20 0 0% Little development
Average 100 10 10% Little development
SOURCE: Cajamarca technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 36
Findings for each of the processes in this subsystem are presented in the table below.
Table 23: Constraints in work organization. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Design of job
profiles
There is no
responsible party to
assume job profile
design in the
institution, but they
have the following
management
documents: CAP
2013, MOF 2009
and PAP 2013.
No specialist has
been identified who
can assume this
role within the
institution. It is also
likely that the
institution does not
have the budget to
hire an external
specialist.
Recruitment does
not meet job
technical
requirements.
Due to the lack of
job profiles,
remuneration is
often linked to a
person and not to
the specific job
profile.
Assign a
responsible party to
develop job profiles
for the Cajamarca
RHD and
decentralized
bodies.
Identification of
labor
competencies
Have not been
developed nor
implemented.
Lack of competent
team.
Assign a
responsible party to
develop labor
competencies for
the Cajamarca RHD
and decentralized
bodies.
Job rating Have not been
developed nor
implemented.
Lack of competent
team.
Assign a
responsible party to
rate posts for the
Cajamarca RHD
and decentralized
bodies.
SOURCE: Cajamarca technical report
While this is the most important subsystem, it is also the least developed. Staff has not developed
the technical skills needed to perform this function. Management documents are outdated, and
functions are not defined in the current HRM framework.
2.4 Employment Management: Progress
The following graph presents the results of the five processes that are involved in this subsystem.
On average, the subsystem only achieved a 37% progress rate, which is deemed “little
development”.
In general, most processes have made some progress. According to information provided by key
informants, however, there are processes that have achieved no development, including staff
mobility as well as staff termination and retirement.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 37
2.4.1 Results of the assessment in San Martin Regional Health Directorate
Graphic 9: San Martin employment management: Results by key processes.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Recruitment,
Selection, Incorporation and
Induction
Staff mobility
Management of staff files and
attendance control
Administration of
disciplinary process
Staff termination and retirement
San Martin: Employment Management
SOURCE: SMT Technical Report
Table 24: San Martin employment management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Recruitment, selection, incorporation
and induction 60 23 38% Little development
Staff mobility 3 0 0% Little development
Management of staff files, attendance
control 20 8 40%
Moderate
development
Administration of disciplinary process 14 6 43%
Moderate
development
Staff termination and retirement 3 0 0% Little development
Average 100 37 37% Little development
SOURCE: SMT Technical Report
Finding for each process in this subsystem are presented below.
Recruitment, selection, incorporation and induction
This process shows achieved a 38% progress rate due to the following developments, among others:
There is a responsible party for managing staff recruitment, selection, incorporation and
induction. However, in some cases there is no one responsible for the development of each
process.
Key informants said that evaluation instruments in the most recent selection process were
only used to fulfill the minimum requirements of current regulations. These evaluation tools

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 38
included curriculum evaluation; personal interview; and knowledge and psychological test
scores.
Despite advances in this process, problems have been encountered and are summarized in the following table.
Table 25: Constraints in recruitment, selection, incorporation and induction. San Martin,
2013.
Problem Constraints Consequences Proposal for
improvement
Despite having a
responsible party for
managing recruitment,
selection, incorporation
and induction of staff,
CAS hiring processes
conducted last year lack
the use of job profiles,
terms of reference,
functions worksheets,
and budgetary
certification8.
Affidavits from hired
candidates are not
verified during the
recruitment and
selection process.
Hired staff does not
receive appropriate
instruction because
there is no responsible
party to inform them of
policies, rules, roles,
goals, vision, mission
and institutional values.
Lack of administrative
procedures in personnel
administration.
There are no visible leaders
to take responsibility for
executing these processes.
The local labor market is tight,
and there is a poor
understanding of these
processes.
Salary scale is not
competitive to attract skilled
personnel with HRM
knowledge.
Frequent personnel turnover
results in the accumulation of
records pending verification
and interferes with daily
tasks.
Lack of awareness regarding
the importance of the
induction process as a tool for
strengthening organizational
learning.
Absence of qualified
personnel and sound
knowledge of HRM
procedures generate
mediocre management
results, and an error prone
environment that has high
civil and criminal liability.
The working environment
deteriorates as a result of
staff who do not fit the job
profile, standards or
requirements; this can
cause a rise in unmet
demands.
The cost to the state to
recruit unqualified
personnel is high because
turnover is more likely.
This creates further costs
in time and money to carry
out a new recruitment and
selection process.
Design a directive to
establish procedures and
responsibilities for the
different processes of
recruitment. This directive
must be supported by the
correct contract file that
includes the standardized
job profile of the post to be
hired, as well as the budget
certification to guarantee
remunerative payment
without neglecting
transparency and
information dissemination
established by current
regulations.
Designate a responsible
party to develop an
induction program with the
person responsible for
institutional image
management.
SOURCE: SMT technical report
The Civil Service Law explicitly states the following as a function of HR offices or the
corresponding body[1]:
“The selection process is a mechanism to join a group of public managers, career civil servants,
and public servants from complementary activities. It selects the best people for the job on the
basis of merit, competence and transparency, ensuring equal access to public service."
Staff mobility
This process has achieved little to no progress.
8 It means "ensure availability of budgetary provision to compromise expenditure for the respective
fiscal year".

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 39
The problems encountered in this process are presented in the table below.
Table 26: Constraints in staff mobility. San Martín, 2013.
Problem Constraints Consequences Proposal for improvement
Staff shifting is made
according to personal
needs rather than
institutional
Lack of knowledge of
rules governing staff
mobility.
Shifting of staff does not
satisfy the needs of the
original or destination
position.
Develop and approve internal
job regulation (Reglamento
Interno de Trabajo – RIT) to
clarify and specify all the
necessary tasks to implement
institutional policies and
procedures.
SOURCE: SMT technical report
Management of staff files and attendance control
This process has achieved a 40% progress rate mostly due to SMT-RHD selection of a person responsible for updating information regarding staff files and a person responsible for attendance control records.
Despite advances in this process, problems have been encountered and are summarized in the table below.
Table 27: Constraints in management of staff files, attendance control. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
The filing of staff information
is not done through a digital
recording system which would
facilitate and expedite the
organization of information on
recruited staff.
A digital attendance control
system is in use, but
physicians do not record
attendance in the way agreed
to by the medical union.
Physicians also disregard the
rules requiring a public
servant to record attendance
in order to maintain payment
of their salaries.
Failure to implement
software for the digital
recording system may
stem from insufficient
budget or poor familiarity
with modern devices.
In health institutions, it is
critical to establish
physician attendance
controls. Physicians are
the only workers exempt
from signing attendance
control records
according to an
administrative
resolution.
Failure to evaluate staff
in a timely manner can
interfere with efficient
decision making.
Implementation of a
comprehensive
administrative system of
personnel control and
records, which includes all
personnel administration
processes.
SOURCE: SMT Technical Report
Administration of disciplinary process
This process has achieved a 43% progress rate due to SMT-RHD designation of a responsible party to manage disciplinary proceedings. The SMT-RHD has also created a permanent commission to manage administrative processes; the commission’s decisions are inherently supported by a resolution.
Despite advances in this process, problems have been encountered and are summarized in the table below.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 40
Table 28: Constraints in administration of disciplinary process. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
SMT-RHD has neither
developed nor approved
RIT, which identifies the
rights and obligations of
the public servant.
They do not maintain an
updated record to report
dismissals and dismissal
sanctions to the National
Registry of Sanctions
(RNSDD).
Lack of knowledge
regarding regulations or
insufficient staff to develop
regulations and internal
policies.
Lack of knowledge
regarding current
regulations administered by
SERVIR to develop an
updated record of the
RNSDD.
Disoriented personnel
unable to exercise their
rights and duties as well as
a weak governing body to
apply normative standards.
Failure to maintain updated
records for SERVIR would
result in state entities hiring
unfit personnel. In the case
of health professionals, this
[the hiring of unfit
personnel] could cause
irreparable damage: poor
decision making could
negatively affect public
health.
Develop internal
regulations by hiring a
consultant or assigning a
manager to lead the
development of
management regulations.
Designate a responsible
individual or party to
manage registration,
dismissals and dismissal
sanctions for prompt
reporting to SERVIR.
SOURCE: SMT technical report
Staff termination and retirement
This process has achieved little to no progress.
The problems encountered are listed in the following table.
Table 29: Constraints in staff termination and retirement. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
There is no responsible
party to manage the
process of
disengagement in order
to effectively manage
staff termination in a
timely manner.
Lack of knowledge
regarding HRM processes
and lack of verification of
data that generates
unjustified regular expenses
(payments to dead
workers).
Inappropriate payment of
remunerative obligations,
which could possibly
generate administrative,
civil and criminal penalties.
Implement a
comprehensive
administrative staff system
with detailed information
on all types of
disengagement according
to labor rules and
contracts. Alternatively, a
responsible party should
be assigned for the sole
purpose of managing all
types of employment
termination.
SOURCE: SMT technical report
2.4.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 41
Table 30: Employment Management: Performance in four regions at different levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD RHD publicizes
CAS vacancies to
recruit but does not
record information
about the
recruitment
processes.
Incomplete use of
selection tools.
There is no system
to register the real
destination of HR.
Lack of a
permanent
selection
committee.
RHD utilizes job
profiles in selection
process and has a
permanent
selection
committee.
RHD does not
systematize CAS
selection
processes.
There is no system
to register the real
destination of HR.
RHD publicizes CAS
vacancies to recruit
but does not record
information about the
recruitment
processes.
Incomplete use of
selection tools.
There is no system
to register the real
destination of HR.
Lack of a permanent
selection committee.
RHD publicizes CAS
vacancies to recruit but
does not record
information about the
recruitment processes.
Incomplete use of
selection tools.
There is no system to
register the real
destination of HR.
Lack of a permanent
selection committee.
Network Networks publicize
CAS vacancies to
recruit but do not
record information
about the
recruitment
processes.
Incomplete use of
selection tools.
There is no system
to register the real
destination of HR.
Lack of a
permanent
selection
committee.
Networks publicize
CAS vacancies to
recruit.
Utilize job profiles
in selection
process.
Have a permanent
selection
committee.
Insufficiently
systematized CAS
selection
processes.
There is no system
to register the real
destination of HR.
Networks publicize
CAS vacancies to
recruit.
Use of selection
tools as well as
recording and
storage of
examinations do not
occur uniformly
among networks.
All networks lack
permanent selection
committees.
All networks provide
induction programs
for new staff.
Networks publicize CAS
vacancies to recruit.
Use of selection tools as
well as recording and
storage of examinations
do not occur uniformly
among networks.
Lack of permanent
selection committees.
Always conduct
induction programs.
Micro-
network
Micro-networks do
not publicize CAS
vacancies.
Micro-networks do
not publicize CAS
vacancies.
Micro-networks do
not publicize CAS
vacancies.
Micro-networks do not
publicize CAS
vacancies.
Hospital Hospitals do not
publicize CAS
vacancies.
Selection tool
usage is not
standardized.
Formation of
permanent
selection
committees is not
uniform.
Hospitals use job
profiles in selection
processes.
They have a
permanent
selection
committee.
There is no system
to register the real
destination of HR.
All entities publicize
CAS vacancies.
There are no
permanent selection
committees.
There is no
uniformity in the use
of criteria and
selection
instruments.
Always provide
induction programs.
All entities publicize
CAS vacancies.
There are no permanent
selection committees.
Always conduct
induction programs.
SOURCE: PARSALUD II technical report
PARSALUD II qualitative information shows incomplete development of recruitment and selection
processes.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 42
Regarding Cajamarca RHD, the project will present the results of the assessment using HP
project methodology and instruments.
Graphic 10: Cajamarca employment management: Results by key processes.
0%10%20%30%40%50%60%70%80%90%
100%
Recruitment,
Selection, Incorporation and Induction
Staff mobility
Management of
staff files and attendance
control
Administration of disciplinary
process
Staff termination and retirement
Cajamarca: Employment Management
SOURCE: Cajamarca technical report
Table 31: Cajamarca employment management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete
Level of
developme
nt
Recruitment, selection, incorporation
and induction 60 23 38% Little
Staff mobility 3 0 0% Little
Management of staff files and
attendance control 20 5 25% Little
Administration of disciplinary process 14 6 43% Moderate
Staff termination and retirement 3 2 67% Moderate
Average 100 36 36% Little
SOURCE: Cajamarca technical report
The findings for each of the processes in this subsystem are included in the following table.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 43
Table 32: Constraints in employment management. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Recruitment,
selection,
incorporation and
induction
Cajamarca RHD
has a permanent
selection
committee.
Lack of
knowledge
regarding
implementation of
the recruitment
process required
by law.
To reduce time in
selection process,
Cajamarca RHD
eliminates some
important procedures.
Contract inadequate
staff due to
inappropriate
recruitment; staff
selection does not
fit the job profile.
Standardize the
recruitment and
selection processes
to include
standardized job
profiles based on
current regulations.
Staff mobility There is an
evaluation
committee for
mobilization
(displacement) of
staff within the
organization, but
there is no control
or monitoring of
other staff,
especially health
facility staff.
Lack of interest
among health
networks in managing
mobility of health
facility staff based on
current regulations.
There is no real
information about
personnel
allocation.
Frequent absence
of staff in health
facilities.
Implement a staff
attendance and
mobility control
system.
Management of
staff files and
attendance control
Poor management
of health
personnel files
and records.
Poor management
of attendance
records.
Poor definition of
functions for
personnel file control.
Lack of staff
commitment to
register attendance.
There is no
responsible party to
monitor attendance
and retention in
health facilities and
networks.
Staff files with
incorrect
information.
Frequent absence
of staff in health
facilities.
Form a party
responsible for
managing files and
records.
Implement an
attendance control
system in health
facilities.
Administration of
disciplinary
process
Disciplinary
process
commissions
unfamiliar with
rights and
obligations of
public servants.
Disciplinary
process
unnecessarily
extended.
Lack of trained
personnel to manage
processes and
current regulations on
disciplinary process.
Statute of limitations
on faults.
Commissions must
be properly staffed
with qualified
personnel who are
familiar with labor
regulations and
administrative
procedures.
Staff termination
and retirement
Current processes
are incomplete
and not based on
current
regulations.
Lack of knowledge
regarding the legal
basis of personnel
administration
processes.
Staff termination
and retirement
without technical
and legal support.
Designate a
responsible party to
manage all types of
employment
terminations.
SOURCE: Cajamarca technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 44
2.5 Performance Management: Progress
The following graph shows results of the four processes that are involved in this subsystem.
On average, this entire subsystem only achieved a 14% progress rate, which is deemed “little
development”.
The supervision process as well as the feedback and design of plans for individual performance
improvement process achieved little to no development.
According to key informants, the performance evaluation process is the most developed within the
performance management subsystem despite having a progress rate of 22%.
2.5.1 Results of the assessment in San Martin Regional Health Directorate
Graphic 11: San Martin performance management: Results by key processes.
0%
50%
100%Performance Planning
Supervision
Performance Evaluation
Feedback and design of
plans for individual performance improvement
San Martin: Performance Management
SOURCE: SMT technical report
Table 33: San Martin performance management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Performance planning 25 4 16% Little development
Supervision 16 0 0% Little development
Performance evaluation 45 10 22% Little development
Feedback and design of plans for
individual performance improvement 14 0 0% Little development
Average 100 14 14% Little development
SOURCE: SMT technical report
Findings for each of the processes in this subsystem are listed below.
Performance planning
This process has achieved a 16% progress rate due to the following developments, among others:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 45
There is a responsible party for the planning, organization and implementation of a
performance evaluation process for the institution.
The current ROF indicates that this function is the responsibility of the HRM directorate in the
SMT-RHD.
The SMT-RHD plans to implement staff performance this year to replace subjective
assessment, which does not reflect the true performance and expected results of each
worker.
Despite advances in this process, problems have been encountered and are summarized in the
table below.
Table 34: Constraints in performance planning. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
Although there is a body
responsible for planning,
organizing, implementing
and evaluating staff
performance evaluations,
there is no methodology
or evaluation plan. In spite
of this, the SMT-RHD
conducted staff
performance evaluations.
There is no methodology
for establishing individual
performance goals.
Evaluations are conducted
only to meet administrative
requirements in order to
avoid sanctions from the
government comptroller.
Lack of knowledge in
managing staff performance
evaluations.
Staff is evaluated but
without considering the
attainment of
institutional goals.
Retain institutional staff
with apparently good
performance while in
reality staff may not be
achieving performance
goals.
Develop methodologies and
management tools to
measure job performance in
order to contribute to the
achievement of institutional
goals.
Develop a policy that
defines the standards of job
competence at the
individual level within the
framework of RHD policies
and including identification
of performance goals for
each unit.
SOURCE: SMT technical report
The Civil Service Law explicitly states the following as a function of the HR office or
corresponding body[1]:
“Be responsible for assessments to be made by the organization and in the manner established by SERVIR ".
"Public managers, career civil servants and related-activity public servants are subject to performance
evaluation."
Supervision
This process has achieved a 0% progress rating, which is deemed “poor development”.
The problems encountered are summarized in the following table.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 46
Table 35: Constraints in supervision. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
There is no responsible
party to manage, monitor,
coach or mentor. In the
current ROF, this process is
not defined.
There are no methods or
instruments to provide TA
to staff.
RHD does not develop
coaching, supervision or
mentoring activities.
Managers do not realize the
importance of standardizing
and developing tools and
methodologies to
accompany staff
performance.
Errors and wasted time,
which affects achievement
of individual goals.
Confused and
demotivated staff feels
uncommitted and
uninvolved in their jobs
and duties, which
prevents attainment of
institutional goals.
Designate a responsible
party to develop
methodology and
management tools to
guide staff performance.
SOURCE: SMT technical report
Performance evaluation
This process has achieved a 22% progress rate due to the following developments, among others:
There is a responsible party for planning, organizing and implementing staff performance
evaluations for SMT-RHD organizational units and its decentralized bodies.
The current ROF indicates that this function is the responsibility of the HRM directorate.
Last year, the SMT-RHD conducted a performance evaluation but only for staff hired in CAS
mode. Results were used to dismiss contract workers with poor scores.
Despite advances in this process, problems have been encountered and are summarized in the
following table.
Table 36: Constraints in performance evaluation. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
There is a responsible
party according to the
current ROF, but there is
no person in charge of
organizing and monitoring
the staff performance
evaluation process.
Methodology and
management tools to
define the staff
performance evaluation
process have not been
developed or approved.
A non-technical staff
performance evaluation for
CAS staff took place,
reflecting only the
fulfillment of routine
administrative obligations.
RHD has not identified a
specialist within the
current staff who can
assume this role.
The institution does not
have the budget to hire an
external specialist.
Subjective evaluation that
does not reflect the
performance
achievements of each
worker.
SMT-RHD will assume
administrative
responsibility for the
failure to implement the
mandatory provisions of
the Civil Service Law
regarding a
comprehensive,
systematic, continuous,
demonstrable and
objective assessment
process.
Designate a party
responsible for organizing
and monitoring an objective
staff performance
evaluation process.
Develop methodology and
management tools to
develop a performance
evaluation in line with
institutional goals.
SOURCE: SMT technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 47
Feedback and design of plans for individual performance improvement
This process has achieved a 0% progress rate.
The problems encountered are summarized in the following table.
Table 37: Constraints in feedback and design of plans for individual performance
improvement. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
There is no party with
direct responsibility for
processing feedback
and designing plans to
improve individual staff
performance; the current
ROF also does not
specify a party for these
duties.
Through performance
feedback, heads of
organizational units perform
appropriate actions to
improve staff performance.
HHR with poor
performance, making the
same mistakes indefinitely.
Designate a responsible
party to manage the
feedback process and
design plans to improve
individual staff performance
for all SMT-RHD
organizational units and its
decentralized bodies.
SOURCE: SMT technical report
2.5.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 38: Performance management: Results in four regions at different levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD RHD conducts
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
RHD does not
conduct
performance
evaluations.
RHD conducts
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
RHD conducts
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
Network RHD conducts
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
RHD conducts
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
All the networks,
except Leoncio
Prado, conduct
performance
evaluations using
the instrument
provided by the MoH
but does not put the
results to practical
use.
Only Puquio and
Huamaga networks
conduct
performance
evaluations using
the instrument
provided by the
MoH.
However, these
networks do not put
results to practical
use.
Micro-
network
Micro-networks do
not conduct
performance
evaluations.
Micro-networks do
not conduct
performance
evaluations.
Micro-networks do
not conduct
performance
evaluations.
Micro-networks do
not conduct
performance
evaluations.
Hospital Hospitals rarely
conduct
performance
Hospitals conduct
performance
evaluations for staff
Hospitals conduct
performance
evaluations for staff
Hospitals do not
conduct
performance

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 48
Institution Ucayali Cusco Huánuco Ayacucho
evaluations. When
they do, they utilize
MoH instruments but
do not put the
results to practical
use.
hired on the 276
legal regime and
CAS. Administrative
and health care staff
are evaluated
utilizing MoH
instruments but do
not put the results to
practical use.
hired on the 276
legal regime and
CAS. Administrative
and health care staff
are evaluated
utilizing MOH
instruments but do
not put the results to
practical use.
evaluations.
SOURCE: PARSALUD II technical report
PARSALUD II qualitative information shows that RHD, networks and hospitals develop
performance evaluation; however, these evaluations are subjective and are not linked to
individual goals. Additionally, evaluation results are not used to improve performance, and there is
no feedback to employees.
Regarding Cajamarca RHD, the project presents the results of the assessment using HP project
methodology and instruments below.
Graphic 12: Cajamarca performance management: Results by key processes.
0%
20%
40%
60%
80%
100%Performance Planning
Supervision
Performance
Evaluation
Feedback and design of plans for individual
performance improvement
Cajamarca: Performance Management
Table 39: Cajamarca performance management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Performance planning 25 3 12% Little development
Supervision 16 0 0% Little development
Performance evaluation 45 0 0% Little development
Feedback and design of plans for
individual performance improvement 14 0 0% Little development
Average 100 3 3% Little development
SOURCE: Cajamarca Technical Report
Findings from each of the processes in this subsystem are presented below.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 49
Table 40: Constraints in performance management. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Performance
planning
There is no
responsible party
for objectively
managing, planning,
organizing,
implementing,
monitoring and
evaluating staff
performance using
a comprehensive,
systematic and
continuous
assessment.
Lack of knowledge
regarding the
importance of design
tools and instruments
for an objective
performance
evaluation.
Subjective
performance
assessment.
Designate a party
responsible for
planning
performance
evaluations at all
levels.
Supervision Has not been
developed nor
implemented.
Lack of knowledge
regarding the
importance of guiding
staff in the
performance of its
duties and functions.
Staff making the
same mistakes,
repeatedly, without
technical assistance
to correct them.
Train managers in
strategies to guide
staff to improve
performance,
through coaching,
mentoring and
supervision.
Performance
evaluation
A management tool
has not been
developed or
approved to define
the methodology to
develop the staff
performance
evaluation process.
Lack of knowledge
regarding the
importance of
developing
methodologies and
management tools to
objectively organize
and implement staff
performance
evaluations.
Health staff
performance
evaluation processes
have been executed
at the health facility
level but only to meet
an administrative
need.
Health facility staff
with apparently
good performance
ratings but
demonstrates
minimum
achievement in
institutional and
individual goals.
Designate a party
responsible for
organizing and
monitoring the staff
performance
evaluation process.
Develop a
management tool to
measure the
effectiveness and
efficiency of
administrative and
health care staff for
Cajamarca RHD
units.
Feedback and
design of plans
for individual
performance
improvement
Has not been
developed nor
implemented.
Lack of knowledge
regarding the
importance of
providing feedback
after a performance
evaluation process.
Workers without
plans to help them
improve
performance
Train managers to
provide feedback to
their workers and
design individual
plans to improve
performance.
SOURCE: Cajamarca technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 50
2.6 Development and Training Management: Progress
2.6.1 Results of the assessment in San Martin Regional Health Directorate
The following graph shows results of the three processes in this subsystem.
On average, this subsystem has achieved a 60% progress rate, deemed “medium development”.
The teaching-service process has progressed the least.
According to information provided by participants, the process with the greatest level of progress
is labor advancement.
Graphic 13: San Martin development and training management: Results by key processes.
0%
20%
40%
60%
80%
100%
Labor advancement (Promotion and
Career Path)
Capacity BuildingRegulation of the
Teaching & Service process
San Martin: Development and Training Management
SOURCE: SMT technical report
Table 41: San Martin development and training management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Labor advancement (promotion and
career path) 35 27 76% Moderate development
Capacity building 47 27 58% Moderate development
Regulation of the teaching & service
process 19 7 35% Little development
Average 100 60 60% Moderate development
SOURCE: SMT technical report
Findings for each of the processes in this subsystem are listed below.
Labor advancement (promotion and career path)
This process has achieved a 76% progress rate (Development Environment) due to the following
reasons:
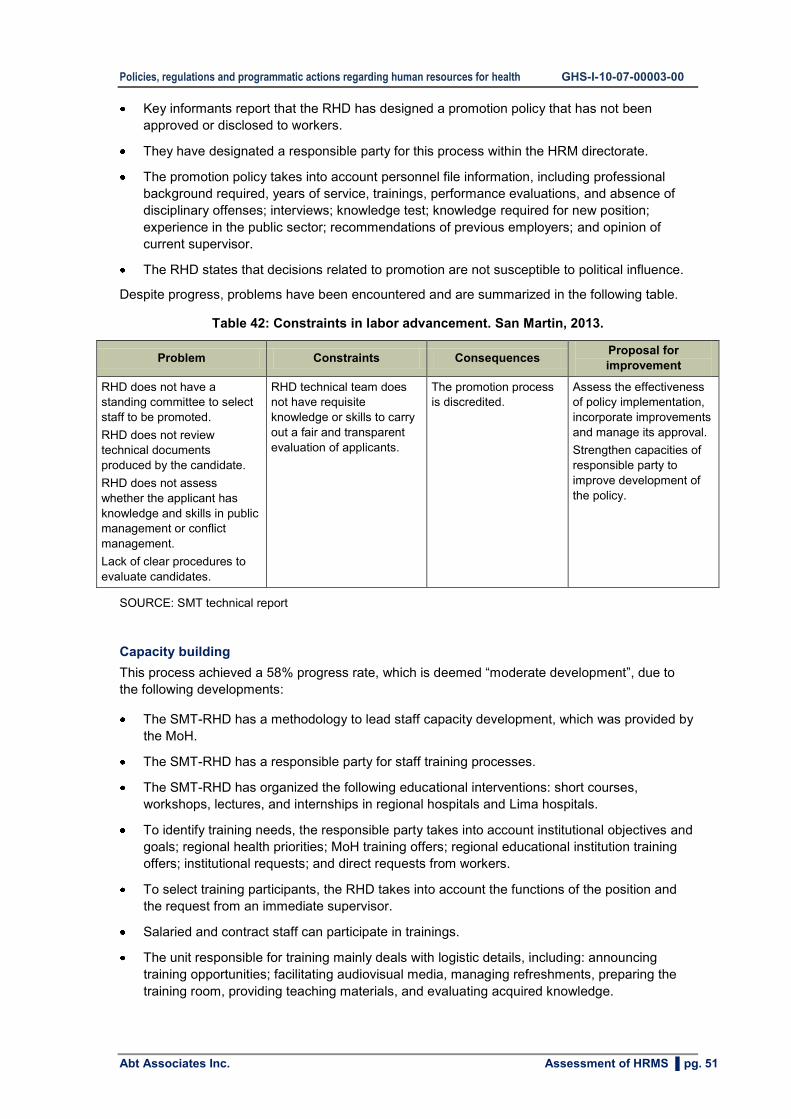
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 51
Key informants report that the RHD has designed a promotion policy that has not been
approved or disclosed to workers.
They have designated a responsible party for this process within the HRM directorate.
The promotion policy takes into account personnel file information, including professional
background required, years of service, trainings, performance evaluations, and absence of
disciplinary offenses; interviews; knowledge test; knowledge required for new position;
experience in the public sector; recommendations of previous employers; and opinion of
current supervisor.
The RHD states that decisions related to promotion are not susceptible to political influence.
Despite progress, problems have been encountered and are summarized in the following table.
Table 42: Constraints in labor advancement. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
RHD does not have a
standing committee to select
staff to be promoted.
RHD does not review
technical documents
produced by the candidate.
RHD does not assess
whether the applicant has
knowledge and skills in public
management or conflict
management.
Lack of clear procedures to
evaluate candidates.
RHD technical team does
not have requisite
knowledge or skills to carry
out a fair and transparent
evaluation of applicants.
The promotion process
is discredited.
Assess the effectiveness
of policy implementation,
incorporate improvements
and manage its approval.
Strengthen capacities of
responsible party to
improve development of
the policy.
SOURCE: SMT technical report
Capacity building
This process achieved a 58% progress rate, which is deemed “moderate development”, due to
the following developments:
The SMT-RHD has a methodology to lead staff capacity development, which was provided by
the MoH.
The SMT-RHD has a responsible party for staff training processes.
The SMT-RHD has organized the following educational interventions: short courses,
workshops, lectures, and internships in regional hospitals and Lima hospitals.
To identify training needs, the responsible party takes into account institutional objectives and
goals; regional health priorities; MoH training offers; regional educational institution training
offers; institutional requests; and direct requests from workers.
To select training participants, the RHD takes into account the functions of the position and
the request from an immediate supervisor.
Salaried and contract staff can participate in trainings.
The unit responsible for training mainly deals with logistic details, including: announcing
training opportunities; facilitating audiovisual media, managing refreshments, preparing the
training room, providing teaching materials, and evaluating acquired knowledge.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 52
Despite these advances, problems occurred and are summarized in the following table.
Table 43: Constraints in capacity building. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
SMT-RHD does not have a
regional policy for training
activities.
SMT-RHD does not know
how much is invested in
training.
Each unit develops its own
training activities and does
not report to the RHD training
unit.
Training activities do not take
place in locations similar to
the workplace.
First-level-of-care staff does
not perform internships at
first-level-of-care facilities.
RHD does not coordinate the
development of training
activities with universities.
When identifying staff training
needs and selecting staff to
train, RHD does not take into
account the results of
knowledge and performance
evaluations, or the previous
training record of the worker
(to avoid duplication).
There are no objective criteria
to select participants. The
responsible party is not
developing essential
functions, including
identifying staff training
needs; TA to network
regarding training
management; controlling
training attendance;
assessing teacher
performance; evaluating skills
according to each position;
evaluating training impact;
and evaluating training
funding.
The understaffed HR unit
manages multiple
activities, which do not
allow it to develop a
regional training policy
and strategies.
Each unit manages its
training financing.
There are no training
venues in first-level-of-
care facilities.
Logistics absorb time and
attention of training unit.
No performance
evaluations are conducted
to identify training needs.
Poor ability to manage
training activities.
Staff performance is not as
expected.
Trained workers are not
always the most in need.
RHD training unit is not
recognized as a TA unit in
training management.
RHD does not know the total
investment made in training
activities, although it
considers that the investment
made does not significantly
improve the quality of care.
Strengthen capacities
in training
management at all
levels.
Design standards,
guidelines and tools to
improve training
activities.
Design training
programs and
internships in places
similar to the working
environment of
trainees.
Develop strategies to
create internship
opportunities in first-
level-of-care facilities
to train first-level-of-
care workers.
Establish a
mechanism to
centralize information
regarding training
activities and
associated financing.
SOURCE: SMT technical report
Regulation of teaching - service process
This process achieved a 35% progress rate, deemed ”little development”, mainly because the
RHD has signed agreements with training institutions for undergraduate and graduate students in
medicine; undergraduate students in nursing and midwifery; and students in technical institutes.
The problems encountered are included in the following table.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 53
Table 44: Constraints in regulation of teaching - service process. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
SMT-RHD does not have
criteria to qualify "teaching
hospitals". Teaching
hospitals are not
accredited.
SMT-RHD does not have
a Pre-degree Regional
Committee (Comité
Regional de Pregrado en
Salud - COREPRES)
officially established and
running.
RHD does not keep
records of all students
who were trained in health
institutions in the region.
There is no responsible
party to manage
agreements with training
institutions.
No regional rules related
to the operation of
teaching hospitals.
Do not know in detail the
national regulations of
COREPRES.
RHD does not understand
the need for or importance
of this information.
Patients' rights are not
respected in teaching
hospitals.
The quality of training is not
satisfactory and not in line
with national regulations.
Training institutions do not
meet the commitments set out
in the agreements, which are
also outdated.
Training institutions use
health facilities to train their
students, but health
institutions receive nothing in
return. For example, RHD
employees could participate
in courses offered by
universities but are currently
not able to.
Revise the existing
legislation regarding
COREPRES and
teaching hospitals.
Revise existing
agreements and design
an advantageous
proposal for RHD.
Designate a responsible
party to manage
agreements.
Schedule an internship
at the MoH to train party
responsible for
agreements in all related
regulations.
SOURCE: SMT technical report
2.6.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 45: Development and training management: Performance in four regions at different
levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD RHD performs
promotion processes
for stable staff
(administrative and
care staff).
Training activities are
guided by the range of
courses and not by
specific need or
demand. Courses are
primarily in public
health rather than
public management.
Develop promotion
processes for stable
staff based on
document review.
Training activities are
arbitrarily oriented
rather than guided by
needs.
Trainings focus on
professional staff.
Main topic in trainings
is public health.
There are restrictions
in training contract
staff.
Develop promotion
processes for all
stable staff.
Trainings are
conducted based on
supply, not demand.
RHD prioritizes public
health issues and
public management.
RHD designs and
implements its own
training courses.
No promotion
process.
Training programs
are based on supply.
RHD designs and
implements its own
training courses.
Network Some networks do
promotion processes
for stable staff, mainly
care staff.
Trainings focus on
public health issues.
Training activities are
Perform promotion
processes for stable
staff based on
document review.
Trainings are
conducted based on
supply rather than
Huánuco network is
the only one that has
performed promotions
for stable staff.
All networks train
both stable and
contract staff.
Only Huanta network
performs promotion
process.
Trainings are carried
out for both stable
and contract staff.
Trainings only

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 54
Institution Ucayali Cusco Huánuco Ayacucho
guided by a supply
approach.
Trainees do not apply
what they have
learned.
One network stated
restrictions in training
hired staff.
demand.
Trainings focus on
professional staff and
public health issues.
There are restrictions
to train hired staff.
All networks prioritize
public health issues in
trainings.
Only Huánuco and
Leoncio Prado
networks include
governance issues in
trainings.
prioritize public health
issues.
Each network is
responsible for
designing and
implementing training
activities.
Micro-
network
Micro-networks do not
execute promotion
and training
processes.
Micro-networks do
not execute
promotion and
training processes.
Micro-networks do
not execute
promotion and
training processes.
Micro-networks do
not execute
promotion and
training processes.
Hospital Hospitals perform
promotion processes
for stable staff focused
on care staff.
Training is led by
supply rather than
demand.
One hospital uses
training plan
guidelines.
Some hospitals
restrict trainings to
hired staff.
Hospitals perform
promotion processes
for permanent staff, in
some cases through
a systematic process
but usually based on
document review.
Training is led by
supply rather than
demand.
Trainings focus on
professional staff and
on general public
health issues instead
of institutional
governance.
No restrictions in
training hired
personnel.
All hospitals develop
promotion processes,
primarily for stable
staff who perform
clinical work.
Hospitals train both
stable and hired staff.
All hospitals provide
training in public
health topics but not
in governance.
Each hospital is
responsible for
designing and
implementing training
activities.
Contracted staff
finances their own
training.
Hospitals do not
conduct promotions
or training processes.
Each hospital is
responsible for
designing and
implementing training
activities.
SOURCE: PARSALUD II technical report
The results of the HRMS performance evaluation conducted by the management team of
Cajamarca RHD are shown below.
More specifically, the following graph shows results from the three processes in this subsystem.
On average, the entire subsystem has achieved a 31% progress rate, which is deemed “little
development”.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 55
Graphic 14: Cajamarca development and training management: Results by key processes.
SOURCE: Cajamarca technical report
Table 46: Cajamarca development and training management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Labor advancement (promotion and
career path) 35 7 19% Little development
Capacity building 47 19 40% Little development
Regulation of the teaching & service
process 19 6 30% Little development
Average 100 31 31% Little development
SOURCE: Cajamarca technical report
Findings for each of the processes in this subsystem are included in the table below.
Table 47: Constraints in development and training management. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Labor
advancement
(promotion and
career path)
RHD does not
have regional
policies to
promote staff.
RHD managers do
not show interest in
promoting staff
advancement and
progression.
MoH does not have
adequate public
policies to promote
staff; as a result,
regions have not
received the proper
TA and guidance in
this issue.
Health personnel
unmotivated with
lack of institutional
commitment.
Design a proposal
for a regional policy
to promote HHR.
Capacity building Lack of a single
regional plan to
Weak RHD
stewardship to lead
Health personnel
unmotivated,
Design a regional
training proposal

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 56
Key Process Problem Constraint Consequences Proposal for
improvement
train and build
health staff
capacity.
and manage
training activities.
RHD units do not
coordinate their
training activities.
Weak institutional
commitment to joint
work, which would
include agreed
targets and
complementary
activities.
without minimum
competencies.
Poor health care
services, both in
quantity and quality.
Population
unsatisfied with
health service
provision.
with appropriate
methodologies and
institutional training
objectives that are
mandatory for all
units.
Regulation of the
teaching - service
process
Poor capacity to
manage these
activities.
Weak regulatory
processes for
teaching in health
services.
Lack of a party
responsible for
managing teaching-
service process.
Graduates of health
training institutions
do not meet the
minimum
requirements to
work in health
services nor do they
have the necessary
skills to work in rural
areas of Cajamarca.
Generate capacities
of the party
responsible for
managing the
teaching - service
process.
Design a plan to
monitor signed
agreements
between the RHD
and universities.
SOURCE: Cajamarca technical report
2.7 Compensation Management: Progress
2.7.1 Results of the assessment in SMT-RHD
The graph below presents results from the five processes in this subsystem.
On average, the subsystem achieved a 67% progress rate, which is deemed “moderate
development”.
Processes related to the payment of salaries, bonuses and pensions are fully developed with a
100% progress rate. The directorate of operations and the operation offices are responsible for
these processes.
On the other hand, SMT-RHD has achieved ”moderate development” in the management of
incentives and the design of a pay scale; the HRM directorate is responsible for implementing
these processes.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 57
Graphic 15: San Martin compensation management: Results by key processes.
0%
20%
40%
60%
80%
100%
Design of Salary
Scales
Management of
Payroll and Salaries
Administration of benefits and
bonuses
Incentive
Management
Pensions
Management
San Martin: Compensation Management
SOURCE: SMT technical report
Table 48: San Martin compensation management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Design of salary scales 56 35 63% Moderate development
Management of payroll and salaries 4 4 100% High development
Administration of benefits and bonuses 2 2 100% High development
Incentive management 32 14 44% Moderate development
Pension management 6 6 100% High development
Average 100 61 61% Moderate development
SOURCE: SMT technical report
Findings for each of the processes in this subsystem are summarized below.
Design of salary scales
This process has achieved a 63% progress rate, which is deemed “moderate development”, due
to the following developments, among others:
Utilizing HP project TA, SMT-RHD designed and approved a salary scale to hire staff working
in first-level-of-care facilities. This approval resolution defines mechanisms for implementation
and maintenance.
The approved salary scale incorporates the following criteria: level of development (rurality)
and poverty in health facility location; distance from Tarapoto to health facility; furthest village
still within its jurisdiction.
Rioja network used the approved pay scale to hire physicians. This network is also in the
process of implementing the new scale for new contract hires.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 58
Despite these advances, problems have been encountered and are summarized in the table
below.
Table 49: Constraints in the design of salary scales. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
Absence of a responsible
party to lead the design of
salary scales for all RHD
staff.
SMT-RHD does not have
pay scales for managers,
professionals and
technicians from
administrative areas.
Each budgetary execution
unit autonomously defines
hired staff salaries without
referencing RHD regulation
and control.
Low wages in remote and
underdeveloped areas
affect recruitment and
retention of health
personnel.
Technical team members
trained in the design of
salary scales have been
moved to other positions.
SMT-RHD has not yet
analyzed the budget to
approve implementation of
the pay scale next year.
Salary scale directive
includes a variable
remunerative component
linked to performance but
has not yet defined its
implementation.
The pay scale does not
consider position hierarchy
or length of service as
criteria.
SMT-RHD pay scale does
not have a corresponding
policy to promote hiring staff
as part of a career plan
framework.
SMT-RHD has not identified the
importance of monitoring the
existing pay scale nor are they
exploring the need for other
scales.
The new technical team does
not know how to apply the
methodology to estimate other
pay scales.
Mechanisms to implement the
pay scale in all networks have
not been defined.
SMT-RHD management team
has not allocated time to plan
implementation of the scale.
Hired staff is unsatisfied
and perceives that the
wage assignment is not
fair and equitable.
Current wages do not
attract and retain health
personnel where needed.
Health professional
positions go permanently
unfilled in remote areas
because of low wages.
Designate and train a
responsible party to
manage all aspects of
the pay scale.
Design other pay scales
where required.
SOURCE: SMT technical report
Management of payroll and salaries
This process has achieved a 100% progress rate, deemed “high development”, due to
the following developments, among others:
The SMT-RHD has an exclusive division responsible for managing payroll.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 59
Payrolls and pensions are kept up-to-date. This is mainly because there are mandatory
national regulations, as well as software which need to be regularly updated so that staff can
receive timely payment of their salaries.
Administration of benefits and bonuses
This process has also achieved a 100% progress rate, which is deemed “high development”.
Like the previous process, the registration of benefits and bonuses is mandatory and is monitored
by the Ministry of Economy and Finance (MoF).
Operations offices are responsible for this process.
Additional bonuses in the form of AETA (Extraordinary Assignment for Health Care Work) are
distributed among professionals and technicians working in health care. Each type of professional
group and technicians receives 22 AETAs.
Bonuses to officers and managers are provided through CAFAE. Technicians in administrative
positions receive bonuses through SUB-CAFAE.
Incentive management
This process has achieved a 44% progress rate, which is deemed “moderate development”, due
to the following developments, among others:
While operations offices are responsible for managing monetary incentives, the SMT-RHD
has not assigned a responsible party to define non-monetary incentives.
Key informants report that the RHD has approved institutional regulations for the
implementation of monetary and non-monetary incentives.
The SMT-RHD has assigned monetary incentives to work teams and not to individuals.
Despite the lack of a responsible party to manage non-monetary incentives, SMT-RHD has
granted several, including public recognition of achievement of corporate goals; secretaries
receiving training courses; days off; baskets of food; uniforms; and organization of internal
sports championships.
Despite these advances, problems have been encountered and are included in the following
table.
Table 50: Constraints in incentive management. San Martin, 2013.
Problem Constraints Consequences Proposal for improvement
SMT-RHD has not
designated a
responsible party to
manage non-monetary
incentives.
Last year, SMT-RHD did
not provide incentives to
individuals and did not
take into account the
results of performance
evaluations. Moreover,
workers are not all able
to receive incentives.
HRM directorate is
understaffed.
SMT-RHD does not have
mechanisms to measure
and evaluate individual
results.
SMT-RHD does not know
what kind of incentives are
desirable to staff.
Poor staff motivation
and commitment in
achieving institutional
goals.
Designate and train a responsible
party to develop incentive
programs.
Conduct operational research to
identify the type of incentives that
staff wants, at all levels, whether
health care staff or administrative
personnel.
Implement a performance
evaluation system with individual
goals.
SOURCE: SMT technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 60
Pension management
This process has achieved a 100% progress rate, which is deemed “high development”.
Like previous processes, the registration of pensions is also mandatory and is monitored by the
MEF.
Operations offices are responsible for administering pensions. There is an approved regulation for
handling them, and pensions are awarded according to the current regulation.
2.7.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 51: Compensation management: Performance in four regions at different levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD RHD does not have
a pay scale for hired
staff; wages are set
on a case-by-case
basis.
RHD does not have
a pay scale for hired
staff.
RHD does not have
a pay scale for hired
staff; wages are set
on a case-by-case
basis.
RHD does not have a pay
scale for hired staff;
wages are set on a case-
by-case basis.
Network One network has a
pay scale for hired
staff based on stable
staff salaries.
Some networks
have a pay scale for
hired staff.
RHD does not have
a pay scale for hired
staff; wages are set
on a case-by-case
basis.
Only the San Miguel
network has designed a
pay scale for hired staff
based on the stable staff
remuneration structure.
Micro-
network
Micro-networks do
not have pay scale
for hired staff; wages
are set on a case-
by-case basis.
Micro-networks are
not involved in
remunerative issues.
Wages and salaries
of micro-networks
are defined by
network or RHD.
Micro-networks are
not involved in
remunerative issues.
Wages and salaries
of micro-networks
are defined by
network or RHD.
Micro-networks are not
involved in remunerative
issues. Wages and
salaries of micro-networks
are defined by network or
RHD.
Hospital Hospitals do not
have a pay scale for
hired staff; wages
are set on a case-
by-case basis.
Hospitals do not
have a pay scale for
hired staff; wages
are set on a case-
by-case basis.
Only Tingo Maria
hospital has created
pay scales for hired
staff based on the
remuneration
received by
permanent staff.
Hospitals do not have a
pay scale for hired staff;
wages are set on a case-
by-case basis.
SOURCE: PARSALUD II technical report
In general, PARSALUD regions do not have specific pay scales for hired staff. Every
remuneration concept is linked to an official that manages each one of them (pensions, benefits,
bonuses and monetary incentives). Every remuneration concept must be updated on a permanent
basis because staff payment depends on the timeliness and accuracy of this information.
The results from the HRMS performance evaluation conducted by the Cajamarca RHD
management team are shown below.
More specifically, the following graph shows the results from the five processes in this subsystem.
On average, the subsystem achieved a 53% progress rate with some processes achieving a
100% progress rate.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 61
Graphic 15: Cajamarca compensation management: Results by key processes.
0%
20%
40%
60%
80%
100%
Design of Salary
Scales
Management of Payroll and
Salaries
Administration of benefits and
bonuses
Incentive
Management
Pensions Management
Cajamarca: Compensation Management
SOURCE: Cajamarca technical report
Table 52: Cajamarca compensation management: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Design of salary scales 56 23 41% Moderate development
Management of payroll and salaries 4 4 100% High development
Administration of benefits and
bonuses 2 2 100% High development
Incentive management 32 18 56% Moderate development
Pension management 6 6 100% High development
Average 100 53 53% Moderate development
SOURCE: Cajamarca technical report
Findings for each of the processes in this subsystem are summarized in the following table.
Table 53: Constraints in compensation management. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Design of salary
scales
Regional authorities
have not
established an
appropriate regional
salary structure.
The decentralization
of functions from
the MoH to regional
authorities has not
been accompanied
by a transfer of
knowledge and
skills.
Cajamarca RHD has
kept the wage
structure defined by
the MoH for several
years.
Set a salary scale
according to local
conditions and
needs.
Management of
payroll and
salaries
No significant
problems were
reported.
Payroll payment is
guaranteed for
stable staff in
Wages are paid on
time in the face of
strong administrative
Monitor all
procedures.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 62
Key Process Problem Constraint Consequences Proposal for
improvement
institutional budgets
(the so called
ordinary resources.)
sanctions.
Administration
of benefits and
bonuses
No significant
problems were
reported.
Benefits are
guaranteed for
stable staff in
institutional budgets
(the so called
ordinary resources).
Benefits are paid on
time in the face of
strong administrative
sanctions.
Monitor all
procedures.
Incentive
management
There is no
incentive policy.
Cajamarca RHD is
not authorized to
use institutional
budget to grant
incentives.
Decentralization
process was not
accompanied by
adequate budgetary
support.
Lack of incentives
inhibits staff
commitment to
achieve institutional
goals.
Design an
incentive policy for
health staff,
according to local
realities and staff
needs.
Pursue research
to target
incentives that
can motivate staff
to perform well.
Pension
management
No significant
problems were
reported.
Pensions are
guaranteed for
stable staff in
institutional budgets
(the so called
ordinary resources).
Pensions are paid on
time in the face of
strong administrative
sanctions.
Monitor all
procedures.
SOURCE: Cajamarca technical report
2.8 Managing Human and Labor Relations: Progress
2.8.1 Results of the assessment in San Martin Regional Health Directorate
The following graph shows results from the three processes in this subsystem. On average, this
subsystem achieved a 70% progress rate, which is deemed “moderate development”. The
management labor relations process has achieved more progress than other processes.
Graphic 15: San Martin managing human and social relations: Results by key processes.
0%
20%
40%
60%
80%
100%
Management of the Organizational
Climate and Culture
Management of labor relations
Workplace health, safety and welfare
San Martin: Managing human and social relations
SOURCE: SMT technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 63
Table 54: San Martin managing human and social relations: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Management of the organizational
climate and culture 32 20 63%
Moderate
development
Management of labor relations 9 9 100% High development
Workplace health, safety and welfare 59 41 69% Moderate
development
Average 100 70 70% Moderate
development
SOURCE: SMT technical report
Findings from each of the processes in this subsystem are summarized below.
Management of the organizational climate and culture
This process achieved a 63% progress rate, which is deemed “moderate development” due to the
following developments:
The SMT-RHD has designated a responsible party to manage organizational climate and
culture in the HRM directorate.
The SMT-RHD has methodology and tools to assess organizational climate; with these tools,
they have assessed the organizational climate this year.
The assessment of the organizational climate has received support from the highest levels
within the institution and at least 90% of workers.
Despite these advances, problems have been encountered and are summarized in the following
table.
Table 55: Constraints in the management of the organizational climate and culture. San
Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
The results of organizational
climate assessment9 have not
yet been analyzed.
No plans have been made to
improve the working
environment.
No immediate action was taken
within 30 days of the
assessment.
The team responsible has not
defined whether the results will
SMT-RHD has done only
one phase of the
organizational climate
management, which is the
assessment.
The team in charge has not
yet organized meetings to
discuss the results.
The delay in analysis
could magnify existing
problems, and
dissatisfaction could
grow.
Arrange meetings to
discuss the results and
propose plans to improve
the organizational climate.
9 The assessment of organizational climate is a snapshot that measures employe perception of
organizational factors; rules; procedures; standards of productivity; management style; communication;
interpersonal relationships; motivators; and leadership. These factors characterize the organization and
influence employee behavior.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 64
Problem Constraints Consequences Proposal for
improvement
be used to review and improve
policies and practices of HRM.
SOURCE: SMT technical report
Management of labor relations
This process has achieved a 100% progress rate, which is deemed “high development”.
The project isolated the following positive developments in this process:
The HRM directorate is responsible for managing this process.
Over 75% of staff is unionized.
Doctor, nurse and midwife unions meet monthly to discuss issues related to the health staff
on duty and job stability.
Administrative and technical staff unions meet at the request of the union leadership to
discuss problems about health staff on duty and job stability.
Key informants describe the relationship between trade unions and RHD authorities as
"good".
The latest negotiation between the union and the authorities has left both parties satisfied,
and both sides are fulfilling all agreements and commitments.
In 2012, the medical strike lasted 72 days.
Relations among RHD members, networks and health facilities are generally good. However,
relations within operations offices are rated as "poor" due to a lack of communication.
The most common causes of labor disputes include salaries, union struggles and internal
rivalries.
Mechanisms used to solve conflicts include negotiating with unions, direct negotiations with
the aggrieved, and negotiations with the immediate boss.
Workplace health, safety and welfare
This process has achieved a 60% progress rate, which is deemed “high development”, due to the
following advances:
The HRM directorate is responsible for managing this process.
There are social welfare programs but only in hospitals and mostly for the elderly. Hospitals
plan and organize social welfare activities.
This year, the RHD is organizing the regional olympics as a social welfare activity.
Hospitals have planned social welfare activities including the celebration of national and
regional public holidays; staff birthday celebrations; the institution’s anniversary celebration;
and the organization of sports competitions.
The control and regulation directorate is responsible for health and safety at work.
There are approved rules, policies and programs to manage health and safety at work.
The SMT-RHD plans activities for health and safety at work.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 65
The scheduled activities on health and safety at work include fumigation of workplaces;
provision of protective equipment for epidemics; occupational disease screening campaigns;
vaccination campaigns; and an infrastructure assessment by Civil Defense.
Despite these advances, problems have been encountered and are summarized in the following
table.
Table 56: Constraints in workplace health, safety and welfare. San Martin, 2013.
Problem Constraints Consequences Proposal for
improvement
The SMT-RHD has not
scheduled other social
welfare activities aside
from the olympics.
Workers do not have a
cafeteria or restaurant;
cash loan services;
financial support for
trainings; a nursery; an
elderly club; travel
arrangements.
Workers do not have
health insurance in case
of accident or illness.
The HRM directorate has
limited staff to perform these
tasks.
RHD has not conducted a
study to identify employee
needs.
RHD has not evaluated the
institutions’ ability to provide
for these needs.
The responsible team is not
familiar with the Health and
Safety at Work Law.
Welfare activities should
generate greater
companionship to reduce
internal conflicts and
improve relationships.
The institution could be
penalized for not applying
health and safety
measures.
Conduct a study to identify
workers’ needs in order to
improve work performance.
The team responsible
should review the Health
and Safety at Work Law
enacted by the Ministry of
Labor and then implement
its provision.
SOURCE: SMT technical report
2.8.2 Results of the assessment in other regions
The following table shows the consolidated results from the evaluation prepared by PARSALUD
II.
Table 57: Managing human and social relations: Performance in four regions at different
levels.
Institution Ucayali Cusco Huánuco Ayacucho
RHD Human relations are
good despite the
absence of labor
climate studies.
The most frequent
cause of conflict is
remuneration.
The RHD does not
conduct staff welfare
programs or health
and safety at work
activities.
Human relations are
good despite the
absence of labor
climate studies.
The cause of
conflicts is
remuneration.
The RHD does not
conduct
occupational safety
programs.
Human relations are
bad due to internal
rivalry between
health care staff and
administrative staff;
remunerative
differences are also
a problem.
There have been
isolated technical
initiatives to assess
the work
environment, but
with little application
of the results.
Programs for
welfare, health and
safety at work focus
both on providing
protective equipment
for diseases and
There is no
information on
human relations.
The most frequent
causes of conflicts
are internal rivalries
and remuneration.
No welfare and
safety at work
programs.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 66
Institution Ucayali Cusco Huánuco Ayacucho
accidents as well as
holiday celebrations.
Network Human relations are
good despite the
absence of labor
climate studies.
The most frequent
cause of conflict is
remuneration.
Networks do not
conduct staff welfare
programs or health
and safety at work
activities.
Human relations in
some networks are
good and in others
bad.
The most frequent
cause of labor
disputes is
remuneration.
Conflict resolution is
managed by the
union.
Human relations are
good except in the
Leoncio Prado
Network, where they
are bad.
None of the
networks provide
welfare and safety at
work programs.
Human relations are
classified as bad.
The most frequent
causes of labor
disputes include
salaries, internal
rivalries and conflicts
generated by
unions.
No records exist
regarding
information on
welfare and safety at
work programs.
Micro-
network
Human relations are
good despite the
absence of labor
climate studies.
The most frequent
cause of conflict is
remuneration.
Micro-networks do
not keep records of
welfare and safety at
work programs.
No information on
the analysis of social
and human relations
or welfare and safety
at work programs.
No information on
the analysis of social
and human relations
or welfare and safety
at work programs.
No information on
the analysis of social
and human relations
or welfare and safety
at work programs.
Hospital Human relations are
generally good to
very good despite
the absence of labor
climate studies,
The most frequent
cause of conflict is
remuneration.
Only one hospital
keeps a record of
welfare and safety at
work programs.
Human relations are
in some cases good
and in other cases
bad.
The most frequent
cause of labor
disputes is
remuneration.
Conflict resolution is
managed by the
union.
Some hospitals run
occupational safety
programs.
Staff at all hospitals
believes that human
relations are bad.
The most frequent
causes of conflict
are compensation
and internal rivalries.
Only Hermilio
Valdizán hospital
provides social
welfare programs,
as well as sterile and
safe equipment for
customer service.
Human relations in
general are
evaluated as good,
despite the absence
of labor climate
studies.
Welfare programs
are aimed at the
supply of sterile and
safe equipment for
customer service.
SOURCE: PARSALUD II technical report
In general, PARSALUD regions do not have specific activities to assure health and safety at work.
Results from the HRMS performance evaluation conducted by the Cajamarca RHD management
team are presented below.
The following graph shows results from the five processes in this subsystem. On average, the
subsystem achieved a 30% progress rate.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 67
Graphic 16: Cajamarca managing human and social relations: Results by key processes.
0%
20%
40%
60%
80%
100%
Management of the Organizational
Climate and
Culture
Management of labor relations
Workplace health, safety and welfare
Cajamarca: Managing human and social relations
SOURCE: Cajamarca technical report
Table 58: Cajamarca managing human and social relations: Results by key processes.
KEY PROCESSES Expected
result
Obtained
result
%
Complete Result
Management of the organizational
climate and culture 32 11 34% Little development
Management of labor relations 9 2 22% Little development
Workplace health, safety and welfare 59 17 29% Little development
Average 100 30 30% Little development
SOURCE: Cajamarca technical report
The findings for each of the processes in this subsystem are included in the following table.
Table 59: Constraints in managing human and social relations. Cajamarca, 2013.
Key Process Problem Constraint Consequences Proposal for
improvement
Management of
the
organizational
climate and
culture
Cajamarca RHD
has made little
progress in
organizational
climate
management.
This is evident on a
daily basis: a large
number of
employees are
unhappy and lack
commitment to
institutional goals.
Managers show
little interest in
improving
organizational
climate among
workers.
Weak health
outcomes; poor
achievement of
institutional goals
and objectives; and
population
dissatisfied with
health care
services.
Strengthen HR in
the institution.
Implement an
organizational
climate study to
establish a baseline
and develop
mechanisms to
solve problems.
Management of
labor relations
Management of
labor relations is
Little interest in
strengthening labor
Staff weakly
committed to
Design and
implement an

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Assessment of HRMS ▌pg. 68
Key Process Problem Constraint Consequences Proposal for
improvement
weak. relations. Sporadic
activities without
clear objectives.
achieving
institutional goals
and objectives.
institutional plan for
improving labor
relations. RHD
authorities must be
present and monitor
this plan.
Workplace
health, safety
and welfare
Processes to
ensure staff welfare
and safety at work
are
underdeveloped.
Authorities show
little interest in this
subject.
Occupational
diseases and
frequent absences
due to occupational
diseases.
Design and
implement an
institutional plan for
welfare and safety
at work with the
participation of all
appropriate offices
and organizational
units.
SOURCE: Cajamarca technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 69
3. Activities undertaken to strengthen the HRMS in health
institutions
3.1 Activities undertaken to estimate staffing needs
To implement universal health insurance (UHI) at the national level, it necessary to assure the
availability and proper allocation of HHR with the necessary competencies to provide quality
health care services. The first step in this process is estimating the HHR requirements needed
to provide the UHI “essential package” (Plan Esencial de Aseguramiento Universal - PEAS) and
cover the HHR gap to assure quality care under UHI.
One of the main problems at the national level is the scarcity of health professionals at the first
level of care. To rectify this issue, one of the HP project’s main activities was designing a
proposal to estimate HHR requirements at the micro-network level.
The MoH and HP project designed and validated methodology for one region, and this
experience was scaled up to the national level. The HP project and MoH supported the
following activities:
Bibliographic review of methods to identify HHR needs. The project decided to use tools
proposed by WISN (Workload Indicators of Staffing Need)[8] as its main reference.
Human resources software review which are applying at the regional level. The project
specifically reviewed software that manages the centralized registry of payrolls and public
sector HR data, which is administered by the Ministry of Finance (MoF); more specifically,
the project looked at the level of reliability, data timeliness, and the level of analysis at the
point of data entry. HP project regions keep updated information through software that
registers HHR data except staff recruited for Health Administration Local Committees
(CLAS - Comités Locales de Administración de Salud); CAS hired staff; displacements; and
actual HR allocation. All regions must report using MoF software, but they do not analyze
the data.
Bibliographic review of approaches in estimating HR requirements for the first level of care.
The project analyzed three main approaches[9, 10]:
- Needs-based: converts projected service needs to personnel requirements using
productivity norms and professional judgment.
- Utilization-based (or demand-based): estimates future requirements based on current
level of service utilization.
- Health workforce to population ratio: specifies desired worker-to-population ratio.
To meet the health needs and services determined by PEAS and to address population
health needs using a mix of HHR, the project selected the needs-based approach.
The methodology used within this approach is based on a a bottom-up process: data is
collected from each health facility and is consolidated by the micro-network; data from all
micro-networks is consolidated at the network level and then further consolidated at the
RHD level.
Established a formula to calculate HR requirements. This calculation must be done for each
type of HHR.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 70
Formula:
HHR requirement
=
Total quantity of time (hours) required to produce PEAS procedures
Standard of available working time per health worker per year x
dispersion index
Calculated the numerator. The project reviewed and validated ASEGURA10
software, which
determines the number of hours required to provide each PEAS procedure linked with a
specific health staff category and a specific unit time (activity standard or activity time)11
at
the national level12
. In order to validate ASEGURA usefulness in HR calculations at the
regional and network level, the HP project and the MoH organized a workshop with Callao
RHD and Lima Ciudad RHD. The main conclusion from the workshop was the need to
make adjustments in ASEGURA, which was designed to perform financial analysis at the
national level. In order to define the total number of procedures necessary to provide PEAS
at the regional and local level for a given population, ASEGURA needs to be flexible when
considering local incidence of priority diseases; determining the type of procedures actually
performed by health staff within networks according to PEAS procedures and the actual
operational capacity of health facilities; considering the regional and local population
structure which is different from the structure at the national level; and considering current
health care norms to calculate activity standards.
In order to make calculations and include adjustments in ASEGURA, the project designed a
spreadsheet13
. Another option considered was the design of an HR module within
ASEGURA, but at that moment ASEGURA was being reviewed and updated.
The spreadsheet has the following advantages:
o It is based on the probability of occurrence of cases (for healthy and ill conditions)
by age group for a given population.
o For each case, the spreadsheet defines all the procedures involved based on
current health care standards.
o For each procedure, it establishes the HHR types involved and the time spent by
each HR type to perform a procedure based on current health care standards.
o It considers the effective time that will be available to provide health care (that is
discounting administrative, training, vacations time, among other issues).
o Allows adjustment according to current and potential health portfolio in the short
and medium term.
o Allows calculation of the HR requirements adjusted for the conditions of the district
in which the health facility is located.
o It considers the current HR allocation in each health facility to determine the gap
that must be covered.
10 Software designed by Partherships for Health Reform plus (PHRplus) project to estimate PEAS cost
at the national level.
11 How much time on average a case should take each staff category, while working to acceptable
professional standards. (WISN, page 5.)
12 See ASEGURA software in Annex 7.5.
13 See procedures to use spreadsheet in Annex 7.6.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 71
o Facilitates the design of charts and graphs, which allow for better analysis of HR
allocation within the micro-network.
Calculated the denominator. The project used the WISN method as a technical reference
point: WISN is based on actual work and is useful for calculating both current and future
HHR requirements. More specifically, it is based on working time, components of work and
activity standards. For our purposes, the project identified indicators related to time spent at
work and other components, including time to directly provide services, vacations, sick
leave, holidays, training, local travel, and administrative burden. On this basis the project
gathered the relevant information in the field. The project provided technical assistance to
the MoH team to design and develop the research project using these indicators. The
research was executed in Ayacucho RHD to determine the time available to solely perform
PEAS procedures. This research project was financed by the MoH. Additionally, the HP
project, along with technical teams from Ucayali and San Martin RHD, conducted interviews
to determine the available working time to provide PEAS at the first level of care14
.
Research results were, in some cases, absolutely unacceptable: in several networks, health
workers spend more than 50% of their time doing activities other than providing health care
services. One conclusion from this research study is that there is a need to define “activity
standard”: how much time on average a case should take each staff category while working
to acceptable professional standards and standards related to distribution of health
providers’ time. It is not acceptable that health workers, who are hired to provide health care
services, spend more than 80% of their time doing other activities. If RHDs do not properly
organize and control staff time distribution, they will always have HR gaps.
Given these results, the SMT-RHD defined standards for the available working time for
each type of health facility at the first level of care15
.
The MoH analyzed results obtained in Ayacucho, San Martin and Ucayali, and determined a
national standard for the available working time needed to provide PEAS.
Table 60: Ministry of Health: Percentage distribution of the workload, by occupational
group for the first level of care.
Occupational group Workload
To provide
PEAS Other
activities Total
Physician 82% 18% 100%
Dentist 94% 6% 100%
Nurse 74% 26% 100%
Psychologist 73% 27% 100%
Midwife 72% 28% 100%
Medical technologist - radiology 94% 6% 100%
Medical technologist - laboratory 94% 6% 100%
Nutritionist 90% 10% 100%
14 See the survey in Annex 7.7.
15 See a detailed table in Annex 7.8 and a summary table in Annex 7.9.
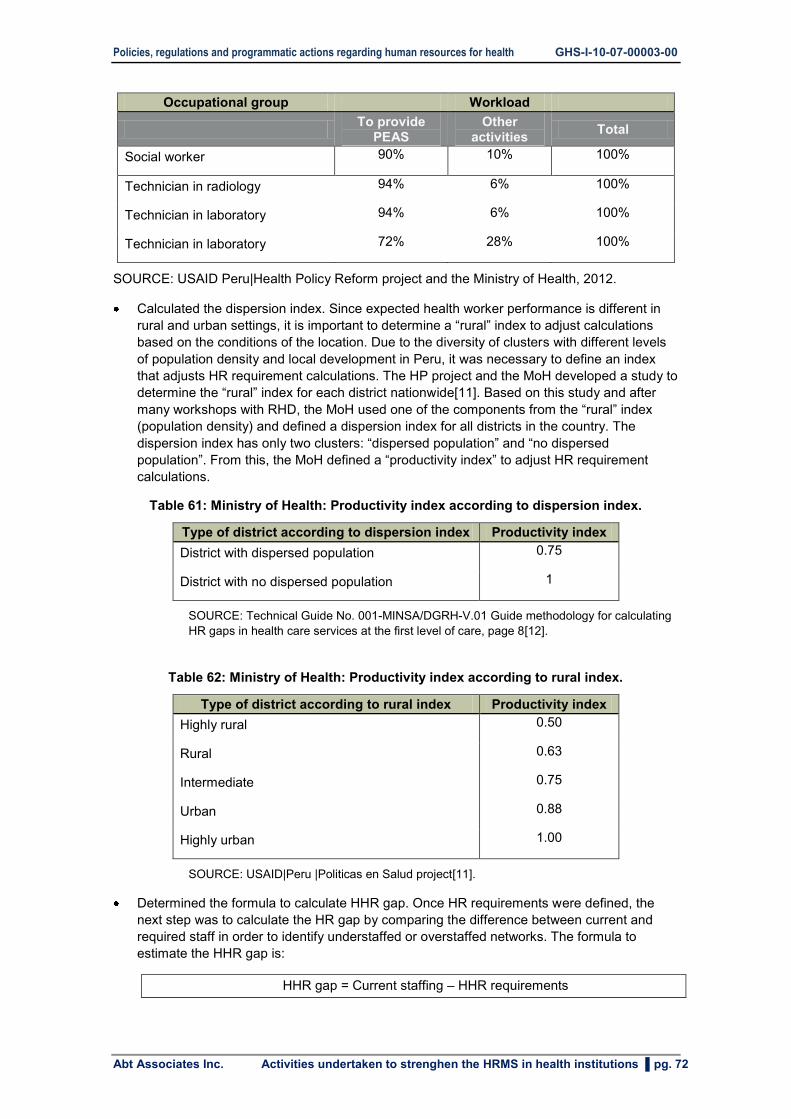
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 72
Occupational group Workload
To provide
PEAS Other
activities Total
Social worker 90% 10% 100%
Technician in radiology 94% 6% 100%
Technician in laboratory 94% 6% 100%
Technician in laboratory 72% 28% 100%
SOURCE: USAID Peru|Health Policy Reform project and the Ministry of Health, 2012.
Calculated the dispersion index. Since expected health worker performance is different in
rural and urban settings, it is important to determine a “rural” index to adjust calculations
based on the conditions of the location. Due to the diversity of clusters with different levels
of population density and local development in Peru, it was necessary to define an index
that adjusts HR requirement calculations. The HP project and the MoH developed a study to
determine the “rural” index for each district nationwide[11]. Based on this study and after
many workshops with RHD, the MoH used one of the components from the “rural” index
(population density) and defined a dispersion index for all districts in the country. The
dispersion index has only two clusters: “dispersed population” and “no dispersed
population”. From this, the MoH defined a “productivity index” to adjust HR requirement
calculations.
Table 61: Ministry of Health: Productivity index according to dispersion index.
Type of district according to dispersion index Productivity index
District with dispersed population 0.75
District with no dispersed population 1
SOURCE: Technical Guide No. 001-MINSA/DGRH-V.01 Guide methodology for calculating
HR gaps in health care services at the first level of care, page 8[12].
Table 62: Ministry of Health: Productivity index according to rural index.
Type of district according to rural index Productivity index
Highly rural 0.50
Rural 0.63
Intermediate 0.75
Urban 0.88
Highly urban 1.00
SOURCE: USAID|Peru |Politicas en Salud project[11].
Determined the formula to calculate HHR gap. Once HR requirements were defined, the
next step was to calculate the HR gap by comparing the difference between current and
required staff in order to identify understaffed or overstaffed networks. The formula to
estimate the HHR gap is:
HHR gap = Current staffing – HHR requirements

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 73
Current staffing. Aside from determining HHR requirements, it is necessary to determine
current staffing by network in order to calculate the gap. The main difficulties in estimating
the HHR gap were related to staff turnover as well as the lack of reliable information
regarding the actual location of health staff. It took more than six months to collect current
staff information in Ayacucho, Ucayali and the SMT-RHD; once consolidated, this
information proved to be completely outdated.
The SMT-RHD decided to organize a workshop with all the micro-networks; each micro-
network prepared the required information, which was consolidated during the course of the
workshop. While productive, organizing a workshop whenever RHDs need this type of
information is expensive and inefficient. A mechanism is needed to oblige all micro-
networks periodically send information about the current staffing at each facility to its
respective network; networks would then send this information to the RHD for regional
consolidation and analysis. The micro-network is the only source of this kind of information;
without this information, any estimation is completely arbitrary.
The following table displays an example of the results which could be obtained automatically
with the application of the spreadsheet to calculate HR staffing needs.
Table 63: Huallaga network: HHR staffing needs, SMT-RHD, 2012.
Physician Dentist Nurse Psychologist Midwife Biologist
Lab
Tech Technician
Sacanche micro-network
(7,782 inhabitants)
HHR requirements (A) 2.67 0.40 11.22 0.26 3.23 0.17 0.30 2.15
Current staffing (B) 4.00 1.00 5.00 1.00 4.00 0.00 1.00 10.00
HHR gap (B - A) 1.33 0.60 -6.22 0.74 0.77 -0.17 0.70 7.85
Workload ratio (B/A) 1.50 2.49 0.45 3.87 1.24 0.00 3.30 4.65
Health workforce to
population ratio
(B/hab*10000) 5.07 1.27 6.34 1.27 5.07 0.00 1.27 12.69
Saposoa micro-network
(19,875 inhabitants)
HHR requirements (A) 9.54 3.66 30.09 2.49 9.46 1.97 3.29 17.97
Current staffing (B) 10.00 1.00 10.00 1.00 11.00 0.00 2.00 44.00
HHR gap (B - A) 0.46 -2.66 -20.09 -1.49 1.54 -1.97 -1.29 26.03
Workload ratio (B/A) 1.05 0.27 0.33 0.40 1.16 0.00 0.61 2.45
Health workforce to
population ratio
(B/hab*10000) 5.03 0.50 5.03 0.50 5.53 0.00 1.01 22.14
HUALLAGA NETWORK
(27,757 inhabitants)
HHR requirements (A) 12.21 4.06 41.30 2.74 12.69 2.14 3.60 20.12
Current staffing (B) 14.00 2.00 15.00 2.00 15.00 0.00 3.00 54.00
HHR gap (B - A) 1.79 -2.06 -26.30 -0.74 2.31 -2.14 -0.60 33.88
Workload ratio (B/A) 1.15 0.49 0.36 0.73 1.18 - 0.83 2.68
Health workforce to
population ratio
(B/hab*10000) 5.04 0.72 5.40 0.72 5.40 0.00 1.08 19.45

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 74
SOURCE: SMT-RHD technical report on HHR gap[13].
Analyzed results. The analysis is based on three calculations using two variables: HHR
requirements obtained through ASEGURA plus adjustments for location conditions; and
current staffing obtained directly from micro-networks until a comprehensive HHR
information system is implemented.
o HHR gap: Comparing the difference between current and required staffing levels to
identify which locations are understaffed or overstaffed. In the table above, the
negative numbers in red indicate understaffed positions. For example, in Huallaga
network there is a severe shortage of nurses, especially in the Saposoa micro-
network. This information could prove useful if Huallaga network has additional
funds to hire health workers: the priority would be to hire nurses in Saposoa micro-
network instead of technicians, which is a currently overstaffed position.
o Workload ratio (the WISN ratio)[8]: Dividing current staffing by HR requirements as
a proxy measure to assess the pressure that health workers experience in their
daily work. Values over “1” indicate overstaffed; values below “1” indicate
understaffed. For example, if a heath facility has four physicians and needs only
two, the workload ratio is two; this means that two doctors are working for every
one that is needed. Conversely, if a heath facility has two physicians and needs
four, the workload ratio is 0.5, which means that one doctor has the workload of two
doctors. In Huallaga network, nurses have the lowest workload ratio, which means
that they have the highest actual workload and feel the most pressure of all
workers.
o The availability of HHR measured by the ratio of professionals per 10,000
inhabitants: Dividing the current staffing by the total population. According to the
Pan American Health Organization (PAHO), there are usually 10 physicians, 10
nurses, and five midwives per 10,000 inhabitants in developing countries. To
compare, Huallaga network has five physicians and five nurses per 10,000
inhabitants; this is 50% less than the average. There are 5.4 midwives per 10,000,
which is slightly more than the average. Accordingly, there would be no need to hire
additional midwives in this network.
The HHR shortage is severe in remote and rural areas mainly due to low wages and poor
working conditions, as well as low connectivity in most of the micro-networks which
prevents regular professional development.
Defined strategies to cover the gap. With these results, the project discussed a set of
strategies to gradually bridge the gap:
o Improve working conditions, especially in remote and rural areas.
o Establish mechanisms to monitor the appropriate use of staff time.
o Distribution of tasks or “task shifting”.
o Improve equipment to shorten working time.
o Define health facility opening hours according to population needs to increase
productivity.
The project worked with Ayacucho RHD to implement task shifting at the network level.
Preliminary results from task shifting show that at the operational level, where the scarcity of
physicians is high, nurses and midwives are performing some medical procedures. In
Ayacucho, nurses and midwives are teaming up to share tasks that have traditionally
belonged to only one of them. Task shifting resulted in a decrease in the average number of
working hours for doctors and nurses, as well as an increase the average number of
working hours for midwives. After task shifting, the overall gap of health staff changed.
Some networks have a gap in midwives instead of being overstaffed, and fewer networks

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 75
are overstaffed in general. This is evidence that the redistribution of tasks as a result of task
shifting allows the efficient use of scarce resources such as doctors and nurses.
Based on this methodology, the MoH designed an application to perform these calculations,
and the project provided TA to support application in Ayacucho. Additionally, the HP project
worked with the MoH to design the “Methodology Guide to Calculate HHR Gaps for the
First-Level-of-Care”, which is being approved through a ministerial resolution for national-
level implementation.
3.2 Activities undertaken to define job profiles
The National Civil Service Authority (SERVIR), which directs the HRMS, states that the
classification and organization of employment positions is the starting point for the
implementation of a HRMS. To promote this idea, SERVIR developed a technical paper entitled
"A Methodological Guide for the Development of Job Profiles” to facilitate the correct
construction of job profiles by human resource managers[14].
Within this framework, job profiles serve as a tool of HR management in providing structured
information regarding the location of a position within an organizational structure, the position’s
purpose and its main functions. A job profile also includes the requirements and demands of the
job to clarify expectations and performance standards.
Based on the importance of the job profile, SERVIR and the HP project developed two macro-
regional workshops to disseminate methodology for designing profiles.
The methodology, in line with the conceptual framework established by SERVIR, identified a
number of procedures to be accomplished before the design of a job profile[15]:
Review of institutional policy documents (ROF, MOF, CAP)
Define the criterion that determines positions and their functions based on one of the
following three approaches: systems approach, process approach, or function focused.
Development of a matrix to define functions for each of the positions.
Preliminary Job profile design
- Determining functions within the matrix of job functions.
- Assessing job functions.
- Identifying essential job functions.
- Identifying position requirements.
- Identifying skills and competencies required for the position.
The Ayacucho RHD technical team, with technical assistance from the HP project, developed
job profiles for the Ayacucho Executive Office of Management and Human Resource
Development; these job profiles are listed below and detailed in the HP project technical paper,
entitled "Staff Jobs Profiles for the Executive Office of Management and Human Resource
Development”[16].

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 76
Table 64: Job profiles for the Ayacucho RHD.
Organizational Unit Proposed Positions
Executive Office of
Management and Human
Resource Development
Executive director for HRM and development in health
Head of the HR planning unit
Head of employment management unit
Head of job design and performance management unit
Head of pensions and other benefits unit
Responsible for social welfare and incentives
Responsible for payroll and salary scale
Head of occupational health and organizational climate unit
Responsible for personnel data and record keeping
Responsible for attendance control
Responsible for SERUMS
SOURCE: USAID Peru Health Policy project and Ayacucho RHD.
The HP project continues to support and provide technical assistance to the Ayacucho RHD in
designing job profiles for staff who provide primary health care services. More specifically, the
project is working to identify and systematize technical information that has been validated by
representatives of networks and micro-networks.
The methodology developed by the HP project for job profile development dictates that defining
"health professional” positions is a first step in the process and should be guided by Law No
23536 and its regulations (DS No 0019 - 83-PCM). Based on this, health professionals include
the following groups: surgeons, dental surgeons, obstetricians, nurses, biologists,
psychologists, social workers, and pharmacists. The HP project also considers nursing
technicians to be important components of the health team. Having specified professional
health groups, the following three points are important in the development of job profiles and are
included in the HP project document entitled "First-Level-of-Care Job Profiles"[17]:
Point 1: Finding information on the functions of each occupational group by category within
each first level of care including I-2, I-3, and I-4.
Point 2: Confirmation of job functions through expert judgment (regional workshop).
Point 3: Job profile description for first-level-of-care staff.
The Ayacucho RHD technical team designed job profiles for the following first-level-of-care
personnel:
Table 65: First-level-of-care personnel job profiles for the Ayacucho RHD.
Health Facility
Categories Proposed Positions
I-2
Medical care I-2
Nursing care I-2
Obstetrical care I-2
Nursing technician I-2
I-3 Medical care I-3
Nursing care I-3

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 77
Obstetrical care I-3
Nursing technician I-3
Responsible del Pharmacy Services I-3
Responsible for Nutritional Services I-3
Responsible for Social Services I-3
I-4 Medical care I-4
Nursing care I-4
Obstetrical care I-4
Nursing technician I-4
Dental surgeon (primary care)
Psychological care (primary care)
Laboratory supervisor (primary care)
Responsible for Pharmacy Services I-4
Responsible for Nutritional ServicesI-4
Responsible for Social Services I-4
SOURCE: USAID Peru Health Policy project and Ayacucho RHD.
In addition, the HP project provided TA to the SMT-RHD in the analysis of a new organizational
structure and, more specifically, in the definition of specific functions; job descriptions and
analysis; and job profiles.
Taking into account SMT-RHD priorities, the following tables summarize organizational units
and corresponding job profiles[15]:
Table 66: Regional Health Directorate of San Martin.
Organizational Unit Proposed Positions
DIRECTORATE OF HUMAN RESOURCES
DEVELOPMENT
Director
Institutional organizational development specialist
RRHH sector management specialist
Work management specialist
Performance development and evaluation specialist
DIRECTORATE OF OPERATIONS Director
Unit chief
Budget management specialist
Administrative support specialist (decentralized operations)
Logistics management and control specialist
Internal administrative management specialist
OFFICE OF STRATEGIC SECTOR
PLANNING Office chief
Budget and finance specialist
Planning specialist
Project investment specialist
Organization and quality assurance specialist

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 78
Organizational Unit Proposed Positions
OFFICE OF HEALTH INTELLIGENCE
Epidemic Control, Emergency,
Disaster Prevention Unit
Information Research and Analysis
Management Unit
Office chief
Unit chief
Epidemiological surveillance specialist
Epidemics, emergencies and disaster specialist in
charge
Unit chief
Investigation specialist
Information management specialist
Communications specialist
Documentation specialist
OFFICE OF LEGAL COUNSEL
Office chief
Regulation and supervision specialist
Judicial processes and administration specialist
DIRECTORATE OF HEALTH SECTOR
REGULATION AND AUDIT
Health Sector Regulatory Unit
Health Sector Audit Unit
Director
Unit chief
Environmental health specialist
Unit chief
Public and private services inspector specialist
Pharmaceutical establishments inspector specialist
Basic sanitation inspector specialist
Food hygiene inspector specialist
Ecology and environmental protection inspector
specialist
DIRECTORATE OF COMPREHENSIVE
HEALTH
Individual and Family Health Unit
Public Health and Environment Unit
Drug and Health Services
Management Unit
Director
Coordinator of comprehensive health
Individual and family health unit chief
Youth and adult life stage specialist
Senior adult life stage specialist
Public health and environment unit chief
Health promotion specialist
Technical unit chief
Organizational and services management specialist
SOURCE: USAID Peru Health Policy project and SMT-RHD.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 79
Table 67: Office of Operations - Health (OOH).
Organizational Unit Proposed Positions
OFFICE OF OPERATIONS Office chief
ADMINISTRATIVE MANAGEMENT
UNIT
Unit chief
Personnel manager
Accounting manager
Treasurer
BUDGET MANAGEMENT UNIT
Unit chief
Budget management unit chief
SOURCE: USAID Peru Health Policy project and SMT-RHD.
Table 68: Health Network.
Organizational Unit Proposed Positions
Health Network Director
OFFICE OF HEALTH PLANNING
AND INTELLIGENCE
Office chief
Planning specialist
Epidemiology specialist
OFFICE OF SANITARY
MANAGEMENT
Office chief
Organization and health services management specialist
Human resource management specialist
DIRECTORATE OF INDIVIDUAL
HEALTH Director
Immunization and child specialist
Food and nutrition specialist
DIRECTORATE OF COLLECTIVE
HEALTH MANAGEMENT Director
Health promotion and community participation specialist
Occupational health specialist
OFFICE OF ADMINISTRATIVE
LIAISON MANAGEMENT Office chief
Personnel administration assistant
Logistics and control assistant
SOURCE: USAID Peru Health Policy project and SMT- RHD.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 80
Table 69: Job profiles for the health micro-network: First-level-of-care staff.
Organizational Unit Proposed Positions
Micro-network Medical care I-2
Nursing care I-2
Obstetrical care I-2
Nursing technician I-2
Medical care I-3
Nursing care I-3
Obstetrical care I-3
Nursing technician I-3
Medical care I-4
Nursing care I-4
Obstetrical care I-4
Nursing technician I-4
Dental surgeon (primary care)
Psychological care (primary care)
Laboratory supervisor (primary care)
SOURCE: USAID Peru Health Policy project and SMT-RHD.
The HP project’s TA was instrumental in the development of job profiles at the regional health
directorate level and has contributed to the improvement of the HRMS in the following ways:
- Regarding the recruitment and selection process, job profiles provide information that can help define the types of media and notices necessary to attract the largest number of candidates.
- Job profiles facilitate the induction process of orientating a new employee within the organizational structure; clarifying relationships with other positions and organizational units; and outlining objectives and duties.
- Training processes are better oriented for the development of Personal Development Plan (PDP).
- In the performance evaluation process, updated job profiles are helpful in defining personal skills or competencies to be monitored through performance evaluations.
- Job profiles also support decision making regarding displacement decisions, designation, rotation, temporary assignments and staffing redeployment.
In recent years, SERVIR has been developing actions within the most urgent aspects identified
to initiate civil service reform as a mandatory by the human resources office, or in lieu thereof,
as stated in Article 6 of Law No 30057.
During the course of the year, there have been a series of regulatory changes regarding HRM in
health institutions nationwide. Specifically, it is now mandatory for health care institutions to
possess updated job profiles in compliance with administrative regulations and requirements.
HP project participation in organizing and structuring Ayacucho HRD and SMT-HRD job profiles
has provided both a valuable experience and a considerable advantage for both regions as
other regions work towards adapting to current regulations for HRM in health institutions.
3.3 Activities undertaken to define managerial competencies
According to the ILO[18], job competencies are divided into general and specific competencies.
General competencies can be described as corporative, generic, organizational, core, and

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 81
value-based; all members of an organization must possess these competencies. Specific
competencies can be described as technical or functional aspects; each worker in an
organization performs a set of functions and must demonstrate competency in the proper
performance of those functions. The capabilities linked to the employee's functions are "specific
competencies".
USAID projects provided TA to the MoH in the conceptual and methodological framework to
define general competencies. Using this framework, the MoH defined the following general
competencies for the health sector16
:
1. Ethical commitment
2. Respect for life, people and environment
3. Communication based on cultural diversity
4. Teamwork
5. Ability to organize and plan
These general competencies must be a part of the job profiles for each posotion in all public
health organizations. Accordingly, the HP project provided TA to help design job profiles in the
Ayacucho RHD and the SMT-RHD, and these competencies have been included in all job
profiles.
The Council for the Quality of Professional Education (Consejo de evaluación, acreditación, y
certificación de la calidad de la educación superior universitaria – CONEAU) is in the process of
defining managerial competencies for all health professions. CONEAU is responsible for
working with professional associations and training institutions in the definition of professional
competencies. There is consensus among health professional associations that all health
professionals perform healthcare, training, management and research actions, focusing on their
daily activities in one of them. In April 2013, CONEAU officially formed a special committee
responsible for designing managerial competencies, which will be used in the mandatory
professional certification process. In 201217
, CONEAU designed a proposal related to
managerial competencies and in 2013 CONEAU submitted the proposal to the special
committee for review, but this committee has yet to convene.
As part of the decentralization process, a new set of functions was transferred from the MoH to
regional health directorates. To support this change, the HP project provided assistance to the
SMT-RHD in the definition of specific managerial competencies for each of the new functions
through the creation of a competencies dictionary18
. This dictionary has been used in the
definition of specific managerial competencies in Ayacucho and SMT.
The Ayacucho RHD asked the HP project for TA in the design of HR job profiles. Using the
SMT-RHD managerial competencies dictionary, the Ayacucho management team identified
specific competencies necessary for HR management19
and then assigned specific
competencies to appropriate job profiles.
To define job profiles and develop performance evaluations for managers at the SMT-RHD
network level, the HP project supported technical teams at the network level in defining two
types of managerial competencies: transversal, which are common to all management
positions, and specific, which are related to the specific functions of the position. For specific
managerial competencies, the HP project utilized the managerial competencies dictionary,
which contains 86 specific competencies. Managers at the network level used this dictionary to
prioritize three competencies that are specific to each position and included them in respective
16 See MoH general competencies in Annex 7.10. 17 See CONEAU managerial competencies in Annex 7.11. 18 See Managerial competencies dictionary in Annex 7.12. 19 See HRM competencies in Annex 7.13.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 82
job profiles. For transversal competencies, the HP project provided a list of 14 competencies20
determined by a bibliographic search of the most common managerial competencies. Based on
this list, network managers defined four competencies to be included in job profiles for all
managerial positions and in performance assessments for network managers.
The four transversal managerial competencies include:
1. Maintain a satisfactory organizational climate
2. Lead, mobilize and inspire teams
3. Maintain good interpersonal relationships
4. Use resources with a high sense of responsibility
3.4 Activities undertaken to design salary scales
One problem in the health sector is the shortage of human resources, especially at first-level-of-
care facilities. One cause of this problem is the inability to attract and retain qualified staff,
mainly in health facilities located in remote and excluded areas; unfortunately, these areas also
have a greater need for health care services. More broadly, while the level of development and
connectivity plays roles in attracting and retaining health care professionals, wages are even
more strongly linked to hiring and retention.
Given this, RHDs should set fair and equitable salaries for hiring staff, especially since more
than 50% of the health workforce is contracted by a variety of regimes.
Graph 17: Health professionals by labor condition, MoH and regional governments, 2012.
SOURCE: MoH – HHR Observatory
The main problem in setting a regional salary scale for health staff is the lack of governance
from RHDs due to the existence of “budget spending units” (unidades ejecutoras de
presupuesto – UE). These units have the authority to define the number of staff hired and
respective salaries without considering technical criteria. This autonomy generates internal
20 See Transversal managerial competencies in Annex 7.14.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 83
inequality, dissatisfaction and demotivation among health workers since two or more health
professionals doing the same job receive different wages. Additionally, local governments as
well as public and private donors can hire health personnel and offer a different salary: this
means that professionals working in the same health facility performing the same functions earn
different wages.
To define a fair and equitable salary scale in hiring health personnel at first-level-of-care
facilities, the HP project worked with Ayacucho, Ucayali and SMT RHDs to define methodology
and tools to set salary scales according to specific characteristics and regional needs[19].
In February 2012, two directives were approved in Ayacucho: a regional directive approving
salaries for first-level-of-care personnel hired by CAS and a second-level-of–care personnel
hired by CAS21
. In Ayacucho, the wage scale is being implemented in all UE. The RHD team
used the methodology to design salary scales for hospitals and RHD workers; they also used
the wage scale to establish the 2013 budget.
In Ucayali, the HP project provided TA to define criteria and respective weights in order to value
job positions and define a salary scale for each micro-network. The salary scale was applied in
the recruitment and selection process in some networks, but there was no regional resolution to
approve its use in all networks.
In SMT, the project presented its experiences from Ucayali and Ayacucho in the design of pay
scales for the first level of care. Regional authorities were interested in this methodology
because it allows them to consider different contexts and factors. Using this background
information, the management team defined four factors to be considered in the SMT pay scale
as well as the relative weight and importance of each factor. The team also defined the
following characteristics: separate pay scales for medical and non-medical health professionals
and technicians; and a pay scale for each health facility.
With these guidelines, the project designed SMT-RHD pay scales that were then approved through directorial resolution. Factors and their respective weights are shown in the table below.
Table 69: Criteria and weights
Level of
development
Accessibility: Distance from
Tarapoto Level of poverty
Time spent to get to remote
communities
A. Most rural 50 A. More than 8 hrs 65 A. Quintile I
and II
30 A. More than 6 hrs 36
B. Rural 40 B. 2 to 8 hrs 55 B. Quintile III 25 B. 3 to 6 hrs 30
C. Intermediate 35 C. 15 minutes to 2 hrs 40 C. Quintile IV 20 C. 30 minutes to 3 hrs 25
D. Urban 30 D. Less than 15 minutes 35 D. Quintile V 15 D. Less than 30
minutes
20
21 Regional Directive N. 001-2012-GRA/GG-GRDS-RHD-DEGRRHH and Regional Directive N.
002-2012-GRA/GG-GRDS-RHD-DEGRRHH.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 84
3.5 Activities undertaken to develop competencies at micronetwork
level
One of the challenges faced by all RHDs is reducing maternal mortality and child malnutrition.
Achieving this depends not only on the availability of equipment but also on the availability of
competent health workers to provide quality health care. Accordingly, it is important to identify
and confront issues related to HHR management and development, including the following[20]:
Limited development of competencies among health workforce.
High turnover of trained staff.
Reduced or inexistent access to training activities for health personnel in remote areas
Poor coordination between RHDs and training institutions resulting in health professionals
who are not responsive to regional health needs Training programs conducted in settings
which are different from actual work environments
Performance evaluations are not competency-based
Health personnel are poorly motivated and not committed to the goals and strategies of
their respective institutions
To manage these issues, USAID provided TA to regional governments to implement regional
HHR policies and improve health worker competencies related to the provision of quality health
services to mothers and children. As part of this TA, Huanuco, Pasco and Junin RHDs
cooperated in the development of a conceptual, methodological and instrumental framework for
a "Competencies Development System", which includes the implementation of competencies
development centers (CDC). Huanuco RHD was the only institution that implemented all
aspects of the system, including the opening of three CDCs in Amarilis, Margos and Acomayo.
The objective of a CDC is to generate and strengthen labor competencies among RHD health
workers at the network and micro-network level with the involvement of local government,
training institutions and professional associations. These centers are part of an in-service
training strategy to foster the development of competencies in locations similar to actual
workplace settings.
Stages of CDC implementation are shown in the graph below.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 85
Graphic 18: Stages in CDC implementation
Design and approval of job competencies,
performance standards
and evaluation tools
Identifying potential
internship sites
Qualification of micro-networks
as CDC
Training program design
Certification of workers trained
Continous supervision of
certified workers
Training program
development
Implementation of competencies
development centerCDC
Supervision of workers trained in their workplace
E
V
A
L
U
A
C
I
O
N
Source: USAID Health Policy Initiative. Mejorando Las Competencias Laborales en el Ámbito Local. 2009:
31.
USAID TA achieved the following results in 2009[21]:
CDCs institutionalized in Huanuco, Junin and Pasco regions with the assistance of the
regional government’s social development management department as well as RHDs and
local governments.
Labor competencies designed, validated and approved for antenatal care; growth and
development monitoring (control de crecimiento y desarrollo – CRED); training nutritional
sessions; care of women in labor and immediate postpartum; and vertical birth.
Non-monetary incentives granted by local governments and civil society to reward
competent HHR from San Luis de Shuaro and Pichanaki micro-networks in Junin RHD.
Official recognition of competency evaluation committees in Huanuco, Cusco, Junin and
Ucayali.
Official recognition of CDC qualification committees in Huanuco, Cusco, Junin and Ucayali.
Official recognition of CDC tutors.
Evaluation of the following competencies: CRED in Huanuco, Junin and Pasco;
demonstration sessions for the preparation of food with local products in Junin; and
antenatal care in Pasco and Junin.
Official recognition of CDCs in Huanuco for CRED; Junin for antenatal care and nutritional
demonstration sessions; Ayacucho for antenatal care; Cusco for vertical birth; Pasco for
antenatal care; and Ucayali for antenatal care.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 86
92 health workers were trained at a CDC through an internship.
Six health workers trained at a CDC have received supervisory visits.
Achievements in Huanuco in this short time frame were mainly due to USAID TA; strong support
from the regional government’s social development manager; the involvement of the University
of Huanuco’s School of Nursing; and most especially the commitment of networks’ technical
team.
A year into CDC implementation in Huanuco, regional and RHD authorities changed, and CDCs
were left without technical and political support. However, two CDCs in Amarilis and Acomayo
are still operating today.
The HP project visited these two centers to interview health authorities and tutors to determine
how the centers have managed to continue operating. The visit yielded the following findings:
All tutors were recognized as certified and competent in CRED through regional resolutions.
Many tutors were also employed as teachers in regional universities, and the health facility
was incorporated into the university as a teaching center.
Mothers attending these health facilities, easily recognized if they are attended by a trained
in the CDC, of another who was not involved in the internship at the CDC, and not allowed
to be attended by untrained personnel. This causes the staff has not been trained ask to
participate in the internship at the CDC.
Health workers from other health networks claimed to be trained at the CDC.
The local government supports the maintenance of equipment and materials for early
stimulation.
This program will be implemented in SMT health networks.
3.6 Activities undertaken to assess management performance
A performance assessment consists of identifying, measuring and managing human
performance in organizations. Identification is based on jobs analyses and intends to determine
which work areas should be studied when their performance is being measured. Measurement
is the core of an evaluation system and seeks to determine how performance compares with
certain objective parameters. Management is the focal point of any assessment system and to
realize the full human potential of an organization it should be orientated towards the future
rather than focus on examining past activity[22].
The regulatory framework defines performance evaluation as a mandatory, comprehensive,
systematic, continuous and demonstrable set of staff activities, skills and performance
measures to meeting goals and objectives. Senior management and human resources, or the
latter’s designees, are responsible for ensuring assessments are carried out in the time and
manner established by SERVIR.
All evaluation processes are subject to the following minimum requirements:
Performance factors measured should be related to job functions, which are clearly defined
in the job profiles of the organization.
Performance is based on factors related to measurable and verifiable targets.
Prior to the evaluation, the worker must be aware of the procedures, factors or goals which
are evaluated.
Evaluations are conducted on an annual basis.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 87
A worker who does not participate in the evaluation process on his own accord, for justified
reasons such as illness, receives a disapproving score, since the performance evaluation is
mandatory for all employees.
All performance evaluations must conform to institutional characteristics, and services provided
correspond to the position types in an organization.
SERVIR considers the following two types of evaluation as complementary. The first type of
evaluation is a measurement of competence that identifies the gap between optimal skills and
current skills to identify training needs. The second type of evaluation aims to measure goal
achievement and identify staff contribution towards achieving organizational goals as well as
areas where adjustments are required to improve performance.
Due to the approval in previous months of new regulations for the civil service and the
administration of performance evaluation, the HP Project has conducted workshops with the
SMT-RHD management team to develop a management tool that allows them to identify
training needs. Additionally, the management tool would also verify and qualify achievements
according to individual institutional goals programmed into the duties’ performance required by
each position. The objective is to provide the SMT-RHD with a tool to measure the evolution of
employee work performance in order to continuously improve institutional management.
3.6.1 Performance evaluation method
The evaluation method developed and proposed by the HP Project ensures that criteria and
practices allow distinguishing performance differences that exist between people in the service
of SMT-RHD. The performance evaluation consists of two parts:
a. Results Evaluation – This component measures the performance of position functions
and/or processes. These functions, including essential and general functions, as well as
position processes, are clearly defined in position profiles for each organizational unit of
the SMT-RHD.
b. Competency Assessment – This component measures general work competencies
which have been identified and approved for all health sector staff and are contained
within the MoH publication "Work Competencies for Improving the Performance of
Health Human Resources".
The following graphs demonstrate the two components of a performance evaluation.
Graphic 19: Results Evaluation

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 88
Graphic 20: Competency Evaluation
3.6.2 Performance evaluation implementation
The implementation of performance evaluations for SMT-RHD staff contains two components:
a) Competency measurements to examine position abilities, skills and attitudes takes
place through a 360° evaluation in which the criteria and parameters for each evaluator,
including self, supervisor, subordinate, peer and client, are required to measure the
competencies established by position type, as shown in the graph below.
b) Completion of essential job functions. To achieve strategic and institutional objectives,
in which essential functions need to be identified, processed, displayed and valued on
levels established by SMT-RHD organizational unit leaders.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 89
Graphic 21: 360° Competency Assessment
3.6.3 Competencies evaluation definition and criteria
The following general competencies were selected by the SMT-RHD technical team while the
definitions and evaluation criteria were established by the MoH[23].
ETHICAL
COMMITMENT
The health worker demonstrates responsible attitudes
and service actions in response to service needs
based on principles and values, the common good,
human dignity and the right to health.
Works for the common good, with honesty and
confidentiality.
Completes his/her work quickly and with quality.
ORGANIZATION
AND PLANNING
CAPACITY
The health worker organizes his/her goals, objectives,
resources, roles, activities and tasks to achieve better
health and social transformation results working within
health guidelines and policies.
Identifies, organizes his/her goals, objectives,
functions, activities, tasks and options through
an established plan.
Works in a planned manner to achieve strategic
results, in a set time frame, building towards
future progress.
TEAMWORK The health worker cooperates and collaborates;
integrating into trans disciplinary teams to achieve
organizational objectives and quality care services in
community health.
Participates in obtaining common goals,
respecting different opinions and avoiding
competition.
Supports team members principally by sharing
information, knowledge and resources.
3.6.4 Analysis of results obtained in the evaluation of goals attained and
competencies
Once the performance evaluation is completed, the SMT-RHD Directorate of Human Resources
processes the information in a format entitled "Analysis of Results Obtained", as shown below,
to determine the gap between expected and observed results. The “Problem Statement”
section highlights factors which caused the gap, analyzes the problem and identifies causes.
The format also shows proposed corrective actions in the short- and medium-term for each
evaluated category.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 90
Graphic 22: Analysis of the results obtained
3.7 Activities undertaken to improve recruit and selection processes
The recruitment and staff selection sub-processes are defined in the employment management
system and framed by the HRM system. These processes are intended to include highly
competent persons within varying organization work areas through transparent and efficient
processes, where merit, suitability and non-discrimination are central elements of its execution.
At present there are irregularities in the implementation of HRM processes (selection, training,
evaluation, mobility, separation, compensation and incentives) depending on labor
arrangements. For example, in most public sector institutions there is no application of merit
and performance principles for either recently hired or long term staff or towards service
retention and no monitoring mechanisms both selection and design processes of job profiles.
Selection tends to be based on the characteristics of the person to be chosen rather than those
required for the position.
Following the analysis for estimating health human resource gaps at all SMT-RHD networks and
micro-networks, the project performed in January 2013, a baseline evaluation of staff
recruitment and selection processes. The analysis took as observation samples the budget
execution units at San Martin (U.E. 400) and Alto Mayo (U.E. 401), both of them in San Martin
RHD. The purpose of the study was to describe the recruitment process in force, so as to allow
the identification of improvement options in the context of the modernization of the human
resource management system.
Tools used in the baseline evaluation were: questionnaires (items research), interview guides
and check lists. Steps from the recruitment and selection process that were evaluated are:
preparatory stage, recruitment stage, selection stage, contract signing stage. The organic units
which participated in this evaluation are mentioned in table 64:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 91
Table 70: Base Evaluation: Participants
U.E 400 U.E 401 SMT-RHD
Office of Resource
Administration
Office of Human
Resources
Office of Planning
Office of Resource
Administration
Office of Human Resources
Office of Planning
Directorate of the Office of
Administration
Executive Office of Institutional
Development and Quality
Office of Strategic Planning
SOURCE: USAID|Peru|Health Policy project
Results of assessment are shown in the table 71 below:
Table 71: Results of baseline evaluation of recruitment and selection processes at San
Martin RHD. January, 2013
Issues assessed U.E. 400 U.E. 401 Comment / recommendation
Preparatory Stage
No workers in the area of human resources 5 3 HRM unit understaffed and under
qualified
Incumbent officer for recruitment and selection No No Appointment of the incumbent
Job profiles availability No No Development and standardization of
job profiles
Competitive salary scale definition and
implementation
Scale defined but
not implemented
Scale defined but
not implemented
Implementation plan needs to be
defined and deployed
Estimation of human resources gaps Yes Yes Link recruitment process to gaps
identified
Triggers to staff recruitment process
Memo/Micro-
Networks
Reports/Networks
and Micro-networks
Define and standardize forms and
define formal parties
Recruitment Stage
Use of institutional web page Sometimes No Publication is mandatory
Ministry of Labor Portal (website) No No Publication is mandatory
Other recruitment methods Hospitals murals Hospitals murals Utilize any method that attracts the
largest pool of candidates
Publication duration 5 days 3 days Use time frame indicated in current
regulations
Selection Stage
Selection committee nomination Yes Yes Recommended composition: at least
one representative of HR area and
one from the user area
No of committee members 8 5 Standardized criteria
Evaluation of CV and personal interview Yes Yes Required by law
Other evaluations Psychological
plus knowledge
evaluation
Psychological
Evaluation
Structured evaluation instruments
should be utilized
Publication of evaluation results on institution
website
No No Publication is mandatory
SOURCE: USAID|Peru|Health Policy project

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 92
The assessment performed in San Martin RHD revealed that the highest percentage of health
workers in health facilities and micro-networks were hired under CAS modality.
With that information in mind San Martin RHD requested the project advance a proposal to set
policies and procedures for the recruitment and selection of staff. Within this proposal also had
to be defined powers, responsibilities, obligations and terms of the organizational units involved
in the process, according to regulations and the reality and potential of the region. Particularly,
SERVIR regulation for the recruitment procedure were taken into consideration (see graphic
66).
Graphic 23: Macro process: administrative services contracting - CAS
During 2013, the project conducted workshops with the technical team of San Martin RHD to
build the recruitment process proposal. As a consequence San Martin RHD Director and his
management team approved the general process flowchart for recruitment. This process is
described below (Graphic 24).
Preparation Stage: This stage starts the recruitment process, and includes the approval of
recruitment requirements to be part of the job announcement. The administrative
management unit (UGA) is the body responsible for administrative services contracts within
health office operations, hereinafter OOS.
Process initialization:
a. The user area sends the administrative service requirement to the immediate supervisor
in their organization. In San Martin RHD, through the Directorate of Health Management,
where an assessment has to be made as related to estimates of human resource
requirements.
b. All networks forward to their Health Operations Office their approved human resource
requirements, within a schedule timetable. OOS budget execution unit evaluates networks
requirements based on budget availability.
c. Budget execution unit forwards the requirement along with their certified budget proposal
to the health network.
d. The health network forwards the requirement to San Martin RHD-Directorate of Human
Resources Development. This instance assesses the requirement according to stated
regional health priorities.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 93
e. Directorate of Human Resources Development responds to the health network to
authorize and commence the recruitment process through the Directorate of Health
Management.
The Directorate of Health Management cannot start the recruitment process unless it has the
following documents: institutional requirement, terms of reference and budget certification by
budget execution unit. It may be necessary to develop or adjust the job profile of the desired
personnel to be hired. However, if there is already a job profile, it has to be reviewed and
updated according to the functions and competencies required.
For facilitating this process, the project defined a methodology for defining job profiles, providing
a framework for developing job profiles in health provision and health management
positions[15].

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 94
Graphic 24: Preparation Stage flowchart

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 95
Recruitment Stage. During this stage, dissemination is started in order to inform vacancies
available, according to institutional needs. Dissemination must comply with current regulations
for recruitment procedures. In the case of San Martin RHD, health networks are entitled to
utilize additional dissemination media for attaining recruitment objectives. Minimum media to be
used are:
a. National Employment Service of the Ministry of Labor www.empleosperu.gob.pe/
b. National Internet Portal http://www.peru.gob.pe/
c. Institution web portal http://www.diressanmartin.gob.pe/web/
This process is described below (Graphic 25).
The MoH web portal as supplementary dissemination media
This tool is currently unavailable for informing on vacancies availability. However, it has been
considered by the project as a valuable tool based on the following facts:
a. It facilitates of the tracking and monitoring of jobs demands nationwide, since it can
concentrate institutional, local and regional offers in each region
b. It could serve as a specialized broadcasting tool nationwide within the health sector.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 96
Graphic 25: Recruitment Stage

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 97
Selection Stage. This stage comprises the objective assessment of applicants who meet the
conditions required by the area user. Assessments required by law are curriculum evaluation
and interviews. In San Martin RHD, additional mechanisms are used by health networks, such
as psychological evaluations, knowledge assessments, etc. to suit the characteristics of the
vacancy service area.
a) Curriculum Evaluation: It involves the analysis, review and compliance checking with
the minimum position requirements in terms of education, training and/or expertise,
experience and skills (mandatory).
b) Personal Interview: This technique allows the evaluator to meet and evaluate the
applicant during the recruitment process (mandatory). Personal interview includes the
following elements:
- Presentation and development: Appropriate personal bearing and ease of
communication in conveying ideas.
- Attitude and qualities: Applicant behavior and expression, both verbal and nonverbal,
manifested during the conduct of the interview.
- Knowledge and analytical skills: Ability to respond to hypothetical and diverse workplace
scenarios related to the job as well as actual work situations.
This process is described below (Graphic 26).

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strenghen the HRMS in health institutions ▌pg. 98
Graphic 26: Selection Stage

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strengthen HRMS ▌pg. 99
To create the final technical document proposal for SMT-RHD hiring, the HP project must have all job profiles including competencies of staff to be hired for SMT-RHD.
The HP Project’s technical paper[24] proposes processes and activities to conduct recruitments is
based on existing national and regional norms corresponding to its scope.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strengthen HRMS ▌pg. 100
4. Conclusions
Based on the results of HRMS assessment in six RHDs, the following can be concluded:
1. In general, there is poor development in the implementation of HRMS processes at the regional
level; only SMT-RHD shows moderate development at 48% towards goals.
2. The performance management component shows the lowest level of development in all assessed
RHDs, including SMT-RHD. The employment management component shows a high level of
development in four RHDs.
3. These results are due to a clear lack of delineation of regulatory functions in RHDs regarding
HRM, which must be explicitly stated in the manual of operations and functions (MOF). RHDs
have not designated responsible parties for many of the HRM processes. HRMS components are
not in the same organizational unit which makes it difficult to implement as a whole system with
components and processes interrelated and interdependent, under a single person. Additionally,
in many RHDs the heads of HR offices are non-professional staff members and have not been
trained in HRM. The number of personnel working in HR offices is insufficient to perform all HRM
processes well.
4. Processes that have reached more than 50% implementation are mostly related to compliance
with the requirements of higher authorities such as the MEF, which requires regular information
reporting.
5. Regarding the planning component, there is an absence of operational research to support
formulation of HHR policies and strategies as well as monitoring and control of HRM indicators.
There have been significant advances in the design of HR policies, which must be reviewed and
updated. A national guideline to estimate HHR needs for the first level of care was designed and
validated; it is currently being approved by MoH. This guideline incorporates tools and
methodologies which were validated and applied by the HP project in Ucayali, Ayacucho and San
Martin.
6. For the work organization component, all RHDs show some progress in relation to the design of
managerial documents such as ROF, MOF, CAP and PAP. However, there have been few
advances in the development of procedure manuals for relevant processes. SERVIR, which is the
national authority for HRMS, has defined a methodology for the design of job profiles, and it has
been validated and applied by the HP project in Ayacucho and San Martin.
7. In the employment management component, the processes performed to date have not met all
the regulatory requirements for conducting a recruitment process. For example, most of the
contract files do not include standardized job profiles or the respective budget certification which
specifies and guarantees remunerative payment. Additionally, dissemination required by current
regulations is not being executed. Staff recruited as a result of this process does not receive the
appropriate induction because there is no responsible party to inform them of policy, rules, roles,
goals, vision, mission and values of the institution. This situation places new staff in institutional
limbo, creating conditions where personnel do not identify with institutional goals.
8. In the performance management component, despite having an organizational unit responsible
for the process, there is no designated person to manage this process. Additionally, a
management tool has not been developed or approved defining the methodology to evaluate the
performance of institution staff.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Activities undertaken to strengthen HRMS ▌pg. 101
9. The development management component demonstrates a poor level of implementation. Despite
having a promotion policy for stable staff, it is not being implemented. This policy needs to be
revised and improved to serve as a reference for more transparent and meritocratic processes.
Regarding capacity building, some regions have restrictions in training hired staff; in these
regions, training activities focus on professional staff.
10. Regarding the compensation management component, only SMT-RHD and Ayacucho have
salary scales for all first-level-of-care facilities. The scales are approved but have not yet been
implemented at the regional level in the case of SMT-RHD.
11. For the management of human and social relations component, there have been advances in
management of labor relations but slightly less progress in developing processes related to
organizational climate and culture as well as workplace health, safety and welfare.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Recommendations to implemente the HRMS at regional level ▌pg. 102
5. Recommendations to implement the HRMS at regional level
1. Diagnose the level of implementation of HRMS at different levels of management. Based on the
results, define critical processes to further develop improvement processes. It is important to
define whether the deficiency in the implementation of critical processes is due to deficiencies in
staff skills or lack of a standard.
2. Establish an organizational structure for HR offices that allows implementing all HRMS processes
by assigning each process to a particular party who is responsible for a defined position in the
new structure.
3. Define job profiles for the head of the HR office and all units established by the new structure.
4. Build the capacity of the HR office´s technical team through a specific program in management of
HRM tools and standards, according to the job profile defined, ensuring permanence of trained
personnel.
5. Strengthen HR offices at the regional and network level with competent and sufficient staff to
implement key HRMS processes and fulfill basic functions of the HR office.
6. Identify indicators for monitoring the implementation of HRMS at the RHD level.
7. Design, adapt or adopt documents or technical tools to improve the management of a given HRM
process. The HP project has designed and validated a HRM toolkit which can be used or adapted
according to the specific environment.
8. Design, adapt or adopt rules or policies when the proper functioning of a process requires the
approval of a regional standard.
9. Establish a workshop among the regional bodies that are involved with HRMS implementation.
Employ regional government HR Offices and the RHD HR Office to analyze the results obtained
in evaluating HRMS, and define improvement plans for the proper functioning of these processes
in accordance with SERVIR provisions.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. References ▌pg. 103
6. References
1. Ley del Servicio Civil, in Ley 30057 2013, Congreso de la República: Perú.
2. SERVIR, El Servicio Civil Peruano; Antecedentes, Marco Normativo Actual y Desafíos Para
La Reforma. 2012, Autoridad Nacional del Servicio Civil: Lima.
3. Ipsos, Evaluación de la Reforma del Servicio Civil. 2013: Lima.
4. Villanueva, C., Elaborar un modelo de gestión descentralizado de recursos humanos en
salud para las regiones: Ayacucho, Cajamarca, Cusco, Huánuco y Ucayali y los planes de
intervención respectivos. 2012, MINSA: Perú.
5. GORESAM, Ordenanza Regional N° 003-2013-GRSM/CR, in OR 003-2013-GRSM/CR.
2013: Región San Martín.
6. Nivel de implementación del sistema de gestión de recursos humanos de la DIRES San
Martín. 2013, Dirección de Desarrollo de RR.HH. de la DIRESA San Martín.
7. Informe de sistemas de gestión de RR.HH. de la DIRESA Cajamarca.
8. Workload Indicators of Staffing Need (Software Manual). 2010, World Health Organization:
Ginebra.
9. Dreesch, N., An approach to estimating human resource requirements to achieve the
Millenium Development Goals. 2013, Oxford University England.
10. An overview of human resources for health (HRH) Projection Models. 2008, USAID: North
Carolina.
11. Alvarez, C., Cálculo de índice de ruralidad para todos los distritos del Perú. 2012: Lima.
12. Guía de metodología de cálculo de las brechas de recursos humanos en salud para los
servicios asistenciales del primer nivel de atención, in Guía Técnica N° 001-MINSA/DGRH-
V.01, MINSA: Lima.
13. Cálculo de brecha de recursos humanos y propuesta de asignación de dotación del equipo
básico para el primer nivel de atención. 2013, Dirección Regional de Salud de San Martín:
Lima.
14. SERVIR, Guía metodológica para la elaboración de perfiles de puestos en las entidades
públicas. 2012: Lima.
15. Perfiles de puestos de la DIRESA San Martín y sus órganos desconcentrados. 2013, HP: San
Martín.
16. Perfiles de puestos para el personal de la dirección ejecutiva de gestión y desarrollo de
recursos humanos. 2012, HP: Ayacucho.
17. Perfiles de puestos para el personal asistencial del primer nivel de atención, HP: DIRESA
Ayacucho.
18. OIT, Diseñar un modelo integtral y dinámico de gestión de recursos humanos por
competencias. 2006, Centro Internacional de Formación de la OIT: Turín.
19. Chiavenato, I., Gestión del Talento Humano. Mc Graw-Hill ed. 2009, México D.F.
20. USAID, Mejorando las competencias laborales en el ámbito local. 2009, USAID | Iniciativa
de Políticas en Salud Lima.
21. USAID, Desarrollo de recursos humanos en salud; Sistema de Desarrollo de Competencias.
2009, USAID | Iniciativa de Políticas en Salud: Lima.
22. WHO, Working together for health - The World Health Report 2006. 2006, World Health
Organization: Ginebra.
23. MINSA, Competencias laborales para la mejora del desempeño de los recursos humanos en
salud. 2011, MINSA - Dirección General de Gestión del Desarrollo de Recursos Humanos:
Lima.
24. Directiva que regula el procedimiento de contratación del personal bajo el régimen especial
laboral de contrato administrativo de servicios - CAS de la Dirección Regional de Salud de
San Martín - Propuesta, HP project.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 104
7. Annex
7.1 Questionnaire to assess the implementation of the HRMS in health
institutions
SISTEMA DE GESTIÓN DE RECURSOS HUMANOS EN INSTITUCIONES DE SALUD
La finalidad de este instrumento es conocer cuál es el nivel de avance en la implementación de los procesos de
la gestión de recursos humanos. Para ello, sírvase responder las preguntas que se formulan a continuación.
Esperamos que las respuestas se acerquen lo más posible con la realidad de su institución, de tal forma que se
puedan identificar las áreas que son necesarias fortalecer.
El instrumento consta de preguntas cerradas donde usted puede marcar la o las alternativas que más se
acerquen a la realidad de su institución. También hay preguntas abiertas donde se espera que pueda ampliar la
información proporcionada en las preguntas cerradas.
Se agradece de antemano su colaboración.
A continuación, sírvase llenar la siguiente información
GESTIÓN Y DESARROLLO DE RECURSOS HUMANOS
Nombre de la institución:
_____________________________________________________________________________
1. En su institución ¿Existe una instancia responsable de la gestión y desarrollo de recursos humanos en
salud? ( ) SI ( ) NO
¿Cuál es el nombre de la unidad responsable de la gestión de recursos humanos en su institución? _______________________________________________________________________________
2. ¿Cuál es la ubicación de la unidad de recursos humanos en su institución? ( ) Órgano de Asesoría ( ) Órgano de Línea ( ) Órgano de Apoyo ( ) No existe, se encuentra dentro de otra
Unidad
3. ¿Cuántas personas trabajan en esta unidad?
Grupo ocupacional
TOTAL
Número de personas por régimen laboral
Régimen 276
Régimen 728
CAS Locador a
tiempo completo
Otro
Profesionales
Técnicos
Otros
TOTAL
POLÍTICA Y PLANIFICACION ESTRATÉGICA DE RECURSOS HUMANOS EN SALUD Cuestionario Formulación de Políticas y estrategias de Gestión y Desarrollo de Recursos Humanos

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 105
1. En su institución ¿Existe una instancia responsable de la formulación y evaluación de políticas de recursos humanos en salud?
( ) SI ( ) NO De acuerdo con su ROF vigente, ¿Cuáles son las instancias que participan en el diseño y evaluación de las políticas de recursos humanos en su institución?
Nivel
¿Participa? En caso de que participe
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
2. ¿Cuenta con Políticas de Gestión y Desarrollo de Recursos Humanos?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas. En caso contrario, pasar a la siguiente Sección.
3. ¿Las Políticas de Gestión y Desarrollo de Recursos Humanos están aprobadas? ( ) SI ( ) NO
¿Cuándo han sido aprobadas? ______________________________________
El diseño de las Políticas de Recursos Humanos ha tomado en cuenta los siguientes procesos: (Si es posible, pedir las políticas y revisar)
N° Pregunta SI NO
4. Planificación de Recursos Humanos
5. Desarrollo de competencias
6. Evaluación del desempeño
7. Motivación e Incentivos
8. Salud y Seguridad en el Trabajo
9. Selección en base al mérito
10. Perfiles de puestos y competencias
11. Agentes comunitarios en salud
Otros; Especificar:
Otros; Especificar:
12. ¿Las políticas aprobadas han tenido algún nivel de implementación?
( ) SI ( ) NO
Si la respuesta a la pegunta anterior ha sido afirmativa, ¿Qué aspectos de la política han sido implementadas?
N° Pregunta SI NO
13. Planificación de Recursos Humanos
14. Desarrollo de competencias
15. Evaluación del desempeño
16. Motivación e Incentivos
17. Salud y Seguridad en el Trabajo
18. Selección en base al mérito
19. Perfiles de puestos y competencias
20. Políticas de Remuneraciones
Otros; Especificar:
Otros; Especificar:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 106
Desarrollo de investigaciones operativas 21. ¿Han desarrollado algún tipo de investigación relacionada con la gestión de recursos humanos?
( ) SI ( ) NO
Si la respuesta a la pegunta anterior ha sido afirmativa, ¿Qué investigaciones han desarrollado? _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
22. ¿Cuentan con un diagnóstico situacional de los recursos humanos en su Región? ( ) SI ( ) NO
Organización y administración de la información en recursos humanos en salud 23. En su institución ¿Existe una instancia responsable de mantener actualizada la información relacionada con
los recursos humanos en salud? ( ) SI ( ) NO
De acuerdo con su ROF vigente, ¿Cuáles son las instancias que participan en la gestión de la información de recursos humanos en su institución?
Nivel
¿Participa? En caso de que participe
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
24. ¿Cuenta con algún sistema de información sobre recursos humanos?
( ) SI ( ) NO
Si la respuesta a la pegunta anterior ha sido afirmativa, marcar con una “X” el tipo de información que se registra en cada aplicativo, software o base de datos de recursos humanos que utilizan en su institución.
Información de RRHH que se registra
Nombre del aplicativo / software / base de datos
Planillas
SIGA …….. …….. ……..
25. Nombre completo de todos los trabajadores
26. Número de plazas ocupadas
27. Número de plazas previstas
28. Número de plazas previstas y presupuestadas sin ocupar
29. Conceptos remunerativos
30. Conceptos no remunerativos
31. Gastos en planilla
32. Asistencia/Tardanzas/Faltas
33. Personas por regímenes laborales
34. Personas por unidad orgánica
35. Personas por grupo ocupacional
36. Concursos públicos realizados
37. Ubicación actual del trabajador
38. Legajo de servidores
39. Servidores por especialidad
40. Tipo de desplazamientos
Otro: ___________________________________
Otro: ___________________________________
Otro: ___________________________________

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 107
41. Los aplicativos que utilizan ¿le ayudan a tomar las decisiones que necesita? ( ) SI ( ) NO
Control en la Gestión de recursos humanos en salud 42. En su institución ¿Existe una instancia responsable del monitoreo de indicadores de gestión de recursos
humanos en salud? ( ) SI ( ) NO
De acuerdo con su ROF vigente, ¿Cuáles son las instancias que participan en el monitoreo de indicadores de gestión de recursos humanos en su institución?
Nivel
¿Participa? En caso de que participe
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
43. ¿En el último año han definido los indicadores de gestión de recursos humanos en su institución?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas. ¿Qué indicadores de gestión de recursos humanos han definido? (puede marcar más de 1)
N° Pregunta SI NO
44. % de MR que cuentan con la estimación de necesidades de RRHH
45. % de instancias que cuentan con el 80% de perfiles de puestos
46. % de contratos suscritos después de un proceso de selección meritocrático
47. % de convocatorias que han sido publicadas en la web del MINTRA
48. % de procesos de reclutamiento y selección que se han realizado en base a perfiles
49. % de capacitaciones realizadas en base a la brecha en el desempeño
50. % de trabajadores que cuentan con metas de producción concertadas
51. % de trabajadores que han sido evaluados por competencias
52. % de trabajadores que han sido contratados en zonas alejadas, en base a una escala salarial atractiva.
Otros; Especificar:
Otros; Especificar:
53. ¿Han realizado la medición de los indicadores de monitoreo de la gestión de recursos humanos en su
institución. ( ) SI ( ) NO
Planificación estratégica de Recursos Humanos 54. En su institución ¿Existe una instancia responsable de la planificación de recursos humanos en salud?
( ) SI ( ) NO De acuerdo con su ROF vigente, ¿Cuáles son las instancias que participan en la estimación de requerimientos de recursos humanos y en el diseño de los planes de dotación en su institución?
Nivel
¿Participa? En caso de que participe
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 108
En la MR
55. ¿En el último año han realizado estimaciones de requerimientos y necesidades de recursos humanos en su
institución? ( ) SI ( ) NO
Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
¿Qué criterio han usado para definir los requerimientos de recursos humanos? (puede marcar más de 1)
N° Pregunta SI NO
56. Plazas del CAP no cubierto
57. Crecimiento vegetativo de la población
58. Aumento de funciones
59. Aumento de la producción
60. Proyecciones de demanda
61. Proyecciones de uso de servicios
62. Ratio de la OMS
Otros; Especificar:
Otros; Especificar:
63. ¿Cuentan con algún aplicativo para las estimaciones de requerimientos de recursos humanos?
( ) SI ( ) NO
64. ¿Han podido contar de manera inmediata, con información actualizada acerca de la dotación actual de recursos humanos y su situación laboral?
( ) SI ( ) NO Si la respuesta es NO, indique ¿Por qué? __________________________________________ _________________________________________________________________________
65. ¿Han utilizado el estudio de brechas o de necesidades de recursos humanos para tomar alguna decisión? ( ) SI ( ) NO
Si la respuesta es afirmativa, ¿En qué han utilizado esta información de necesidades de recursos humanos?
N° Pregunta SI NO
66. Para las nuevas contrataciones
67. Para sustentar más presupuesto
68. Para redistribuir personal
69. Para solicitar mas SERUMS
Otros; Especificar:
Otros; Especificar:
70. ¿En base a esta información, han elaborado su Plan de dotación para el corto, mediano y largo plazo?
( ) SI ( ) NO Si la respuesta es NO, indique ¿Por qué? __________________________________________
Financiamiento de Recursos Humanos 71. En su institución ¿Existe una instancia responsable de estimar las necesidades de financiamiento de
recursos humanos en salud para la Región? ( ) SI ( ) NO

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 109
De acuerdo con su ROF vigente, ¿Cuáles son las instancias que participan en la estimación de las necesidades de financiamiento de recursos humanos en salud para la Región?
Nivel
¿Participa? En caso de que participe
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
72. ¿En el último año han realizado estimaciones de necesidades de financiamiento para los recursos humanos
en salud para la Región? ( ) SI ( ) NO
Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
¿Qué criterio han usado para definir los requerimientos de financiamiento de recursos humanos? (puede marcar más de 1)
N° Pregunta SI NO
73. Plazas del CAP no cubierto
74. Estudio de necesidades de RRHH
75. Requerimientos de las unidades ejecutoras
76. Presupuesto histórico
Otros; Especificar:
Otros; Especificar:
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DEL SUB SISTEMA DE POLÍTICA Y PLANIFICACIÓN ESTRATÉGICA DE RECURSOS HUMANOS:
ORGANIZACIÓN DEL TRABAJO
Cuestionario
Diseño de perfiles de puestos de trabajo 1. ¿Existe una instancia responsable del diseño de los perfiles de puestos en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente, ¿Quién o quiénes son las instancias que participan en el diseño de las competencias?
Nivel
¿Existe responsable?
En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 110
Nivel
¿Existe responsable?
En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En la Red
En la MR
Para el diseño de perfiles de puestos, deben tomarse como referencia los documentos de gestión en materia de recursos humanos, al respecto, llene el siguiente cuadro:
N° Documento
¿Existe al menos en el 80% de las
unidades orgánicas?
En caso de que exista, responda lo que ocurre en la mayoría de los casos
SI NO Año de
aprobación Año de última modificación
# de modificaciones en los últimos 3 años
2. 1 CAP
3. 2 MOF
4. 3 MAPRO
5. 4 PAP
En relación al CAP, marque lo que corresponda para su institución:
( ) El número de personas nombradas trabajando es exactamente igual al número de personas consignadas en el CAP
( ) El número de personas nombradas trabajando es mayor al número de personas consignadas en el CAP
( ) El número de personas nombradas trabajando es menor al número de personas consignadas en el CAP
( ) El número de personas trabajando (nombradas y contratadas) es exactamente igual al número de personas consignadas en el CAP
( ) El número de personas trabajando (nombradas y contratadas) es mayor al número de personas consignadas en el CAP
( ) El número de personas trabajando (nombradas y contratadas) es menor al número de personas consignadas en el CAP
Para el documento CAP más avanzado y completo, marque el contenido
N° Pregunta SI NO
6. Puestos ocupados
7. Puestos previstos
8. Cargos de confianza
9. Puestos por grupo ocupacional
10. Puestos del personal CAS
Otros; Especificar:
Para el documento MOF más avanzado y completo, marque el contenido
N° Pregunta SI NO
11. Funciones específicas del puesto
12. Conocimientos requeridos
13. Experiencia previa
Otros; Especificar:
Para el documento MAPRO más avanzado y completo, marque el contenido
N° Pregunta SI NO
14. Procesos desarrollados
15. Responsables de cada proceso

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 111
N° Pregunta SI NO
16. Metas por procesos
17. Metas por persona
Otros; Especificar:
Para el documento PAP más avanzado y completo, marque el contenido
N° Pregunta SI NO
18. Monto de Ingresos por servidor
19. Clasificación de conceptos remunerativos
20. Clasificación conceptos no remunerativos
21. Frecuencia de otorgamiento de conceptos salariales
Otros; Especificar:
22. ¿En el último año han diseñado perfiles de puestos en alguna unidad orgánica?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas. En caso contrario, pase a la siguiente sección. ¿Cuentan con al menos el 60% de perfiles para los puesto de los siguientes niveles?
N° Nivel 60% de perfiles
SI NO
23. DIRESA
24. Red
25. Oficina de Operaciones
26. MR
¿Qué han tomado como referencia para definir las funciones específicas de los puestos?
N° Pregunta SI NO
27. Las funciones vigentes del MOF
28. Las funciones descritas en los TDR
29. Opinión de expertos
30. Perfil de competencias
31. Las funciones generales del ROF
32. Un análisis de procesos
Otros; Especificar:
Otros; Especificar:
¿Qué han tomado como referencia para definir los requisitos para los puestos?
N° Pregunta SI NO
33. La situación del mercado laboral regional
34. La situación del mercado laboral nacional
35. La situación laboral de los trabajadores actuales
36. La complejidad de las funciones
37. La importancia del puesto
Otros; Especificar:
Otros; Especificar:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 112
38. ¿Los perfiles de puestos diseñados, tienen algún tipo de aprobación oficial? ( ) SI, ¿Cuál? _______________________ ( ) NO
39. ¿Han utilizado los perfiles de puestos diseñados para tomar algún tipo de decisión?
( ) SI ( ) NO, ¿Por qué? ___________________________________ ¿En qué han utilizado los perfiles de puestos diseñados?
N° Pregunta SI NO
40. Para los procesos de reclutamiento
41. Para los procesos de selección
42. Para los procesos de capacitación
43. Para definir las compensaciones
44. Para la evaluación del desempeño
45. Para los ascensos
Otros; Especificar:
Otros; Especificar:
Identificación de competencias 46. ¿Existe una instancia responsable de definir el perfil de competencias en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente, ¿Quién o quiénes son las instancias que participan en el diseño de las competencias?
Nivel
¿Existe responsable?
En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
47. ¿En el último año han diseñado perfiles de competencias en alguna unidad orgánica?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas. ¿Cuentan con al menos el 60% de perfiles para los puesto de los siguientes niveles?
N° Nivel 60% de perfiles
SI NO
48. Asistencial
49. Gerencial o Directivo
50. Administrativo
¿Qué herramientas han usado para definir las competencias?
N° Pregunta SI NO
51. Diccionario de competencias
52. Las competencias del MINSA
53. Las competencias de los colegios profesionales
54. Las competencias definidas por otras instituciones similares
55. Análisis Funcional
56. Análisis Conductual
57. Consulta a expertos

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 113
N° Pregunta SI NO
Otros; Especificar:
Otros; Especificar:
58. ¿Las competencias definidas, tienen algún tipo de aprobación oficial? ( ) SI, ¿Cuál? ___________________ ( ) NO
59. ¿Han utilizado las competencias diseñadas para tomar algún tipo de decisión?
( ) SI ( ) NO, ¿Por qué? ____________________________________
¿En qué han utilizado las competencias definidas?
N° Pregunta SI NO
60. Como parte de los perfiles de puestos
61. Para la evaluación de candidatos en los procesos de selección
62. Para definir los contenidos de la capacitación
63. Para definir la línea de carrera
64. Para la evaluación del desempeño
65. Para definir las compensaciones
Otros; Especificar:
Valoración de puestos de trabajo 66. ¿Existe una instancia responsable de valorar los puestos de trabajo en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente, ¿Quién o quiénes son las instancias que participan en la valoración de los puestos de trabajo?
Nivel
¿Existe responsable?
En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
67. ¿En el último año han desarrollado algún proceso de valoración de puestos de trabajo?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas. La valoración de puestos realizada, han sido para los puestos en los siguientes niveles:
N° Nivel SI NO
68. DIRESA
69. Red
70. Oficina de Operaciones
71. MR
¿Qué criterios han usado para definir las competencias?
N° Pregunta SI NO
72. El perfil del puesto: Jerarquía, formación, experiencia
73. Presupuesto bajo responsabilidad

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 114
N° Pregunta SI NO
74. Cantidad de personal bajo responsabilidad
75. Ubicación geográfica del puesto
76. Carga de trabajo del puesto
77. Condiciones de desarrollo del lugar donde se ubica el puesto
78. Nivel de pobreza del lugar donde se ubica el puesto
Otros; Especificar:
Otros; Especificar:
79. ¿Han utilizado la valoración del puesto para tomar algún tipo de decisión? ( ) SI ( ) NO, ¿Por qué? ______________________________________
¿En qué han utilizado la valoración del puesto realizada?
N° Pregunta SI NO
80. Para definir la línea de carrera
81. Para definir el salario
82. Para distribuir el personal
83. Para definir los incentivos
Otros; Especificar:
Otros; Especificar:
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DEL SUB SISTEMA DE ORGANIZACIÓN DEL TRABAJO:
GESTIÓN DEL EMPLEO
Cuestionario
Reclutamiento, Selección, Incorporación e Inducción
1. ¿Cuentan con una instancia responsable de administrar los procesos de reclutamiento, selección, incorporación e inducción de personal?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los procesos de reclutamiento, selección, incorporación e inducción de personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 115
2. ¿En el último año han realizado procesos de reclutamiento y selección en su institución? ( ) SI ( ) NO
En el último proceso de contratación ¿Cómo han SUSTENTADO la necesidad de contratación de personal?
N° Pregunta SI NO
3. Existencia de plazas del CAP no cubiertas
4. Incremento en el presupuesto
5. Requerimiento del área usuaria
6. En base a un estudio de brechas
7. Este tipo de decisiones no tiene influencia política
8. Por aumento de la producción
Otros; Especificar:
En la fase preparatoria de los procesos de contratación de CAS realizados el año pasado, han contado con lo siguiente: (puede marcar más de 1)
N° Pregunta SI NO
9. El requerimiento realizado por el área usuaria.
10. Perfil del puesto
11. Términos de Referencia
12. Hoja de funciones
13. Existencia de la disponibilidad en la Certificación Presupuestaria
Otros; Especificar:
En relación al Reclutamiento, en el último concurso de plazas, ¿qué medios de difusión han utilizado?
N° Pregunta SI NO
14. Radio local
15. Televisión local
16. Periódicos locales
17. Mural de la entidad
18. Página web de la institución
19. Servicio Nacional del Empleo del MINTRA
Otros; Especificar:
En relación a los concursos realizados durante el año pasado, llenar la siguiente información
2012 Mes
# días de difusión del concurso
Resultado
Concurso culminado
Concurso desierto
Concurso impugnad
o
Plazas concursadas:
Mes
# Plazas concursadas Tipo y # de plazas asistenciales concursadas
Directivas
Asistenciales
Administrativos
A B C D E
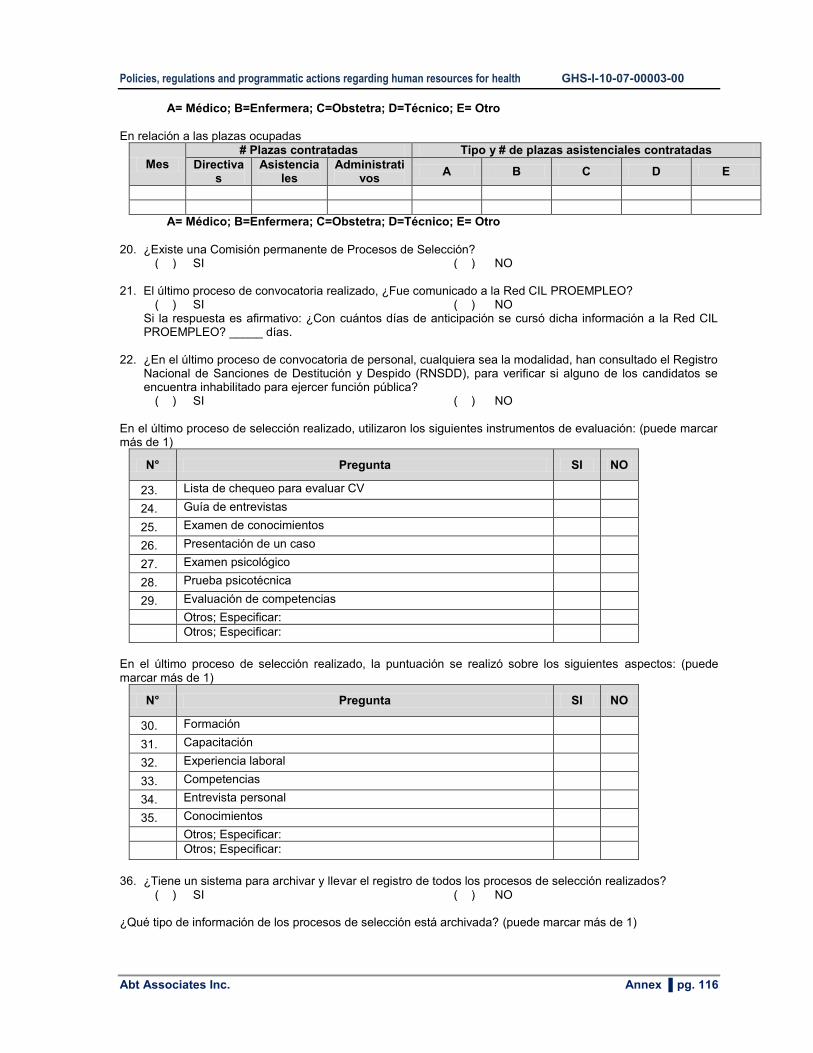
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 116
A= Médico; B=Enfermera; C=Obstetra; D=Técnico; E= Otro
En relación a las plazas ocupadas
Mes
# Plazas contratadas Tipo y # de plazas asistenciales contratadas
Directivas
Asistenciales
Administrativos
A B C D E
A= Médico; B=Enfermera; C=Obstetra; D=Técnico; E= Otro
20. ¿Existe una Comisión permanente de Procesos de Selección?
( ) SI ( ) NO
21. El último proceso de convocatoria realizado, ¿Fue comunicado a la Red CIL PROEMPLEO? ( ) SI ( ) NO
Si la respuesta es afirmativo: ¿Con cuántos días de anticipación se cursó dicha información a la Red CIL PROEMPLEO? _____ días.
22. ¿En el último proceso de convocatoria de personal, cualquiera sea la modalidad, han consultado el Registro Nacional de Sanciones de Destitución y Despido (RNSDD), para verificar si alguno de los candidatos se encuentra inhabilitado para ejercer función pública?
( ) SI ( ) NO
En el último proceso de selección realizado, utilizaron los siguientes instrumentos de evaluación: (puede marcar más de 1)
N° Pregunta SI NO
23. Lista de chequeo para evaluar CV
24. Guía de entrevistas
25. Examen de conocimientos
26. Presentación de un caso
27. Examen psicológico
28. Prueba psicotécnica
29. Evaluación de competencias
Otros; Especificar:
Otros; Especificar:
En el último proceso de selección realizado, la puntuación se realizó sobre los siguientes aspectos: (puede marcar más de 1)
N° Pregunta SI NO
30. Formación
31. Capacitación
32. Experiencia laboral
33. Competencias
34. Entrevista personal
35. Conocimientos
Otros; Especificar:
Otros; Especificar:
36. ¿Tiene un sistema para archivar y llevar el registro de todos los procesos de selección realizados?
( ) SI ( ) NO
¿Qué tipo de información de los procesos de selección está archivada? (puede marcar más de 1)

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 117
N° Pregunta SI NO
37. Bases del concurso
38. Solicitudes recibidas
39. Resultado de las evaluaciones
40. Impugnaciones
41. Actas del Comité de Concurso
Otros; Especificar:
Otros; Especificar:
42. En el último proceso de contratación, ¿Han realizado la inducción al nuevo personal incorporado?
( ) SI ( ) NO En el último proceso de contratación, ¿Quién ha sido la unidad responsable de la inducción al nuevo personal?
( ) Director de la DIRESA ( ) Jefe del Área usuaria ( ) Jefe de la Red ( ) Un trabajador del área usuaria ( ) Jefe de la MR ( ) Otros; Especificar: ____________
En el último proceso de inducción, ¿Qué temas se han abordado?
N° Pregunta SI NO
43. Misión, Visión y Valores de la institución
44. Políticas regionales de salud
45. Políticas y estrategias sanitarias institucionales
46. Reglamento Interno de Trabajo (RIT)
47. Funciones Generales de la unidad orgánica
48. Funciones específicas del puesto
49. Procesos claves que se desarrollan
50. Metas de desempeño esperadas
Otros; Especificar:
51. El último proceso de inducción duró en promedio de 3 días a 1 semana a tiempo completo
( ) SI ( ) NO Desplazamiento o movilidad del personal 52. ¿Cuentan con un responsable de mantener actualizada la información de los desplazamientos del
personal? ( ) SI ( ) NO
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de autorizar el desplazamiento del personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
53. ¿Cuentan con un sistema que permita mantener actualizada la información de los desplazamientos del
personal? ( ) SI ( ) NO
En el 2011 y 2012, ¿cuánto personal ha sido destacado fuera de la institución?
Año # total de personal
# total de personal
# de destaques por grupo ocupacional # destaques
por plaza

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 118
movilizado destacado asistencial
Directivo Asistencial
Administrativo
A B C D E
2011
2012
2013
A= Médico; B=Enfermera; C=Obstetra; D=Técnico; E= Otro
Administración de legajos y declaraciones juradas; control de asistencia y permanencia
54. ¿Cuentan con un responsable de mantener la actualización de la información del legajo?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable del mantenimiento del legajo de personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
55. ¿Cuentan con algún sistema para registrar la información del personal, como por ejemplo un legajo de
personal? ( ) SI ( ) NO
Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
¿Qué información del trabajador contiene el legajo de personal?
N° Pregunta SI NO
56. Datos personales (nombre, edad, sexo, etc.)
57. Régimen laboral al que pertenece
58. Registro de amonestaciones o sanciones
59. Informes de evaluaciones de desempeño
60. Registro de las faltas o tardanzas
61. Capacitaciones recibidas
62. Incentivos recibidos
Otros; Especificar: __________
63. ¿ El año pasado han realizado la actualización de la información del legajo?
( ) SI ( ) NO
¿Cuándo realizaron la última actualización de la información del legajo? ( ) El mes pasado ( ) El año pasado ( ) Hace 6 meses ( ) No se realiza
En relación al Control de Asistencia y permanencia: 64. ¿Cuentan con un responsable del Control de Asistencia y permanencia del personal?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable del Control de Asistencia y permanencia del personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 119
N° Pregunta SI NO
65. ¿Cuentan con un sistema confiable de control de asistencia del personal, que no sea el Cuaderno de asistencia?
Si la respuesta es SI, ¿Cuál?
66. ¿Todos marcan su asistencia? Si la respuesta es NO, ¿Quiénes no marcan y por qué?
67. ¿Tienen alguna Resolución donde se señala el personal que no está obligado a registrar su asistencia?
Si la respuesta es NO, ¿Por qué?
Administración de procesos disciplinarios 68. ¿Cuentan con un responsable de administrar los procesos disciplinarios en su institución?
( ) SI ( ) NO
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los procesos disciplinarios en su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
En relación al Reglamento interno de Trabajo (RIT):
N° Pregunta SI NO
69. ¿Cuentan con un RIT? ¿Cuándo fue diseñado? __________
70. ¿El RIT está aprobado? ¿Cuándo fue aprobado? ______________
71. ¿El RIT es conocido por el personal? ¿Cómo se ha difundido____________________
72. ¿El RIT ha sido entregado al nuevo personal contratado en el último proceso?
Si la respuesta es NO, ¿Por qué?
73. ¿Tiene ejemplares del RIT disponibles en este momento?
Si la respuesta es NO, ¿Por qué?
En relación a los Procesos Disciplinarios:
N° Pregunta SI NO
74. ¿Cuentan con una Comisión de Procesos Administrativos Disciplinarios?
Si la respuesta es NO, ¿Por qué?
75. ¿Han realizado procesos disciplinarios el 2012?
¿Cuántos procesos disciplinarios han desarrollado en el 2012?
76. ¿Todos los fallos formales de la Comisión de procesos administrativos del 2012 cuentan con Resolución?
Si la respuesta es NO, ¿Por qué?
77. ¿Mantienen un registro actualizado de los expedientes de Procesos Administrativo?
Si la respuesta es NO, ¿Por qué?
78.
Mantiene actualizado el Registro Nacional de Sanciones de Destitución y Despido (RNSDD), con el registro oportuno de las sanciones y todos los demás actos relacionados como la modificación, suspensión o anulación, según corresponda
Si la respuesta es NO, ¿Por qué?

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 120
Desvinculación del personal 79. ¿Cuentan con un responsable de administrar los procesos de desvinculación del personal?
( ) SI ( ) NO
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los procesos de desvinculación del personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
80. ¿Cuentan con un sistema que permita mantener actualizada la información de los procesos de
desvinculación del personal por régimen laboral y grupo ocupacional? ( ) SI ( ) NO
En el periodo 2010-2012, ¿cuántos casos de desvinculación por régimen laboral han ocurrido?
Tipos de desvinculación laboral
2010 2011 2012
DL 276
DL 728
CAS DL 276
DL 728
CAS DL 276
DL 728
CAS
Fallecimiento
Renuncia
Despido
Destitución por falta grave
Invalidez permanente
Jubilación
Término del contrato
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DEL SUB SISTEMA DE GESTION DEL EMPLEO:
GESTIÓN DEL DESEMPEÑO Cuestionario
Planificación del desempeño
1. ¿Cuentan con un responsable de planificar, organizar, implementar y evaluar los procesos de evaluación el desempeño del personal de su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de planificar y organizar los procesos de evaluación el desempeño del personal de su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 121
En la MR
En relación a las metas de rendimiento
N° Pregunta SI NO
2. ¿Cuentan con una metodología definida para establecer las metas de rendimiento individual?
3. ¿Cuentan con una metodología definida para establecer las metas de rendimiento grupal?
4. El año pasado y durante el presente año, ¿Han establecido metas de rendimiento de manera concertada, para algún grupo ocupacional?
5. ¿Tienen planificado realizar la estimación de las metas de rendimiento para este año?
En relación a la metodología e instrumentos para evaluar el desempeño del personal
N° Pregunta SI NO
6. ¿Cuentan con una metodología definida para evaluar el desempeño del personal?
7. ¿Cuentan con una metodología aprobada oficialmente para evaluar el desempeño del personal?
8. ¿Cuentan con instrumentos para evaluar de manera objetiva el desempeño del personal?
9. ¿Tienen planificado realizar la evaluación del desempeño del personal durante el presente año?
10. En el último año han elaborado un plan para la evaluación del desempeño del personal de su institución?
( ) SI ( ) NO Acompañamiento
11. ¿Cuentan con un responsable de planificar, organizar, implementar y evaluar los procesos de supervisión, coaching o mentoring en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de planificar y organizar los procesos de supervisión, coaching o mentoring de su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
En relación al acompañamiento del personal:
N° Pregunta SI NO
12. ¿Cuentan con una metodología e instrumentos definidos para que los jefes de unidades puedan realizar el acompañamiento a su personal?
13. La metodología definida para que los jefes de unidades puedan realizar el acompañamiento a su personal, ¿está aprobada?
14. ¿Cuentan con algún mecanismo para registrar los procesos de acompañamiento que realizan los jefes de unidades orgánicas? (Por ejemplo: Informes de supervisión)
15. ¿En el último año los jefes de unidades orgánicas han reportado la ejecución de actividades de
acompañamiento al personal para mejorar su desempeño? ( ) SI ( ) NO
Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 122
N° Pregunta SI NO
16. Los reportes o informes del acompañamiento registran los problemas en el desempeño encontrados
17. Los reportes o informes del acompañamiento registran las medidas correctivas adoptadas
18. Los reportes o informes del acompañamiento registran la fecha de la próxima visita
19. Los reportes o informes del acompañamiento son firmados por el personal visitado
Evaluación del desempeño
20. ¿Cuentan con un responsable de organizar y monitorear los procesos de evaluación de desempeño en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de organizar y monitorear los procesos de evaluación de desempeño en su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
En relación a la evaluación del desempeño:
N° Pregunta SI NO
21. Las unidades orgánicas de su institución programan evaluaciones de desempeño a su personal
22. ¿Cuentan con algún mecanismo para registrar los procesos de evaluación del desempeño que realizan los jefes de unidades orgánicas?
23. ¿En el último año los jefes de unidades orgánicas han realizado procesos de evaluación de desempeño?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
N° Pregunta SI NO
24. Los jefes de unidades orgánicas han usado los perfiles de puestos para diseñar los instrumentos para evaluar el desempeño del personal a su cargo.
25. Los jefes de unidades orgánicas han establecido las metas de rendimiento del personal a su cargo, de manera concertada
26. Los jefes de las unidades orgánicas han definido los estándares de desempeño esperados en el personal a su cargo
27. Los jefes de las unidades orgánicas han definido los indicadores de desempeño en base a las funciones del puesto
28. Los jefes de las unidades orgánicas han definido las preguntas para evaluar conocimientos en base a la información del perfil del puesto
29. Los trabajadores son informados con anticipación sobre la evaluación
30. Los trabajadores son informados sobre los temas a ser evaluados
31. Los trabajadores son informados sobre los instrumentos de evaluación
32. Los trabajadores son informados sobre los mecanismos de impugnación
33. Los trabajadores son informados sobre las consecuencias de la evaluación
34. Han realizado la evaluación de conocimientos específicos para el puesto

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 123
N° Pregunta SI NO
35. Han realizado la evaluación de conocimientos generales para el puesto
36. Han realizado la medición de las metas de producción del personal
37. Han realizado la medición de las competencias específicas del puesto
38. La evaluación del desempeño es realizada por un agente externo a la unidad orgánica (par o superior)
39. La evaluación del desempeño se realiza semestralmente
Las evaluaciones de desempeño se realizan preferentemente a personal:
N° Nivel SI NO
40. Gerencial o Directivo
41. Profesionales asistenciales
42. Técnicos asistenciales
43. Profesionales administrativos
44. Técnicos administrativos
45. Personal nombrado
46. Personal contratado bajo cualquier modalidad
47. ¿Han utilizado los resultados de la evaluación del desempeño para tomar algún tipo de decisión?
( ) SI ( ) NO, ¿Por qué? ______________________________________
¿En qué han utilizado los resultados de la evaluación del desempeño?
N° Pregunta SI NO
48. Para definir los contenidos de la capacitación
49. Para definir la promoción y los ascensos
50. Para definir las compensaciones (incentivos monetarios o no monetarios)
Otros; Especificar:
Otros; Especificar:
Retroalimentación y Diseño de planes de mejora del desempeño individual
51. ¿Cuentan con un responsable de asegurase que el personal evaluado reciba la retroalimentación y diseñe con su jefe los planes de mejora de su desempeño?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de asegurase que el personal evaluado reciba la retroalimentación y diseñe con su jefe los planes de mejora de su desempeño?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
52. ¿Cuentan con algún mecanismo para registrar los procesos de retroalimentación del desempeño que
realizan los jefes de unidades orgánicas? ( ) SI ( ) NO
53. ¿En el último año los jefes de unidades orgánicas han realizado la retroalimentación al personal evaluado?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 124
N° Pregunta SI NO
54. Se entregan los resultados de la evaluación del desempeño al evaluado
55. Se otorga algún tipo de certificación al personal que ha demostrado ser competente en la evaluación del desempeño
56. Como resultado de la medición de las metas de desempeño, se reformulan las metas operativas para la siguiente evaluación.
57. En base a los resultados de la evaluación se formulan planes de mejora con el evaluado
¿Considera que existen problemas para desarrollar los procesos de evaluación de desempeño en su institución?
( ) SI ( ) NO ¿Cuáles son las principales dificultades que existen para desarrollar procesos de evaluación de desempeño basado en metas de rendimiento y en competencias en su institución?
Problemas SI NO
Poco apoyo por parte de la alta dirección
Poco apoyo por parte de los evaluados
Uso casi nulo de los resultados de la evaluación por parte de los jefes inmediatos
Desconocimiento sobre herramientas de diseño y aplicación referidos a la evaluación de desempeño
No se entiende la importancia de la evaluación para mejorar el desempeño
El personal asocia la evaluación con despidos
Las evaluaciones de desempeño tradicionales son subjetivas y desmotivan al personal
El personal no acepta ser evaluado por temor a los resultados
Otro
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DE LA GESTIÓN DEL DESEMPEÑO:
GESTIÓN DEL DESARROLLO Y LA CAPACITACIÓN
Cuestionario
Progresión laboral (Promoción y Carrera) En relación a los ascensos del personal
N° Pregunta SI NO
1. ¿Han diseñado una política de ascensos?
2. ¿Esta política está aprobada? Si la respuesta es SI, ¿Cuándo ha sido
aprobada?_______
3. ¿Esta política es conocida por todos?
4. ¿Cuentan con un responsable de administrar los procesos de promoción y ascenso del personal?

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 125
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los procesos de promoción y ascenso del personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
5. ¿En el último año han realizado procesos de promoción o ascenso al personal de su institución?
( ) SI ( ) NO Solo si la respuesta es afirmativa conteste las siguientes preguntas; caso contrario, pase directamente a la sección “Desarrollo de Capacidades”. La promoción y/o ascensos en los últimos 5 años se han realizado tomando en cuenta lo siguiente.
N° Pregunta SI NO
6. Años de servicio
7. Evaluaciones de desempeño
8. Mediante concurso de mérito
9. Evaluación del legajo
10. Este tipo de decisiones no tienen ninguna influencia política
Otros; Especificar:
Otros; Especificar:
Indicar la cantidad de ascensos ocurridos el 2012, por régimen laboral y grupo ocupacional.
Grupo ocupacional de
origen
Régimen laboral Total
276 728 CAS
Funcionarios
Directivos
Profesionales
Apoyo
Total
11. ¿Existe una comisión permanente para los procesos de selección de personal a promover?
( ) SI ( ) NO Marcar los instrumentos que se utilizan para seleccionar al personal a promover.
N° Pregunta SI NO
12. Entrevistas
13. Exámenes de conocimientos
14. Dinámicas grupales
15. Proyectos/ensayos/documentos de investigación
Otros; Especificar:
Otros; Especificar:
Sobre la difusión del concurso, marcar las que se han utilizado en los últimos 2 años:
N° Pregunta SI NO
16. Son publicados con anticipación
17. Se estipula el cargo y las funciones

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 126
N° Pregunta SI NO
18. Se definen los requisitos para postular
19. Se define el cronograma del concurso
20. Se difunden los resultados
21. Se difunden los ganadores del concurso
22. Se definen las modalidades de impugnación
23. Este tipo de decisiones no tienen ninguna influencia política
Otros; Especificar:
Otros; Especificar:
Marcar los criterios que se evalúan para promover al personal:
N° Pregunta SI NO
24. Conocimientos sobre funciones que realizará
25. Conocimientos sobre gestión pública
26. Liderazgo
27. Comunicación
28. Trabajo en equipo
29. No haber cometido faltas disciplinarias
30. Resultados de evaluación de desempeño
31. Experiencia en el sector público
32. Experiencia en las funciones que realizará
33. Recomendaciones
34. Nivel profesional adquirido
35. Manejo de conflictos
36. Participación en capacitaciones
37. Opinión del jefe inmediato superior
38. Este tipo de decisiones no tienen ninguna influencia política
Otros; Especificar:
Otros; Especificar:
Desarrollo de Capacidades
En relación a las actividades de capacitación
N° Pregunta SI NO
39. ¿Han diseñado una política de capacitación?
40. ¿Esta política está aprobada? Si la respuesta es SI, ¿Cuándo ha sido
aprobada?_______
41. ¿Esta política es conocida por todos?
42. ¿Cuentan con una guía metodológica para el desarrollo de capacidades?
Si la respuesta es SI, ¿esta Guía es la proporcionada por el MINSA? SI___ NO___
43. ¿Cuentan con un responsable de administrar los procesos de capacitación del personal?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los procesos de capacitación del personal?
Nivel ¿Existe? En caso de que exista

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 127
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
44. ¿En el último año han realizado procesos de capacitación al personal de su institución?
( ) SI ( ) NO Solo si la respuesta es afirmativa conteste las siguientes preguntas.
¿Qué tipo de intervenciones educativas han desarrollado en su institución, en el último año?
N° Pregunta SI NO
45. Cursos cortos
46. Charlas
47. Pasantías en sedes del I Nivel
48. Pasantías en Hospitales regionales
49. Pasantías en Hospitales de Lima
50. Diplomados coordinados con una universidad
51. Talleres de capacitación
Otros; Especificar:
Indicar la cantidad de personas que han sido capacitadas el 2012, por régimen laboral y grupo ocupacional.
Grupo ocupacional
Régimen laboral Total
276 728 CAS
Funcionarios
Directivos
Profesionales
Apoyo
Total
Indicar los tres (03) temas que con más frecuencia han sido considerados en la capacitación de cada grupo ocupacional.
Grupo ocupacional
Temas más frecuentes en las actividades de capacitación
Funcionarios
a) b) c)
Directivos
a) b) c)
Profesionales
a) b) c)
Apoyo
a) b) c)
Marcar los criterios que se han tomado en cuenta para identificar las necesidades de capacitación del personal de su institución:
N° Pregunta SI NO
52. Los objetivos/metas de la entidad
53. Las prioridades sanitarias regionales
54. Las oferta de capacitación del MINSA
55. Las ofertas de capacitación de instituciones regionales
56. Resultados evaluaciones de conocimientos
57. Resultados de evaluaciones de desempeño

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 128
N° Pregunta SI NO
58. Lineamientos del Plan de Capacitaciones
59. Sugerencia de otras instancias (redes, DIRESA, etc.)
60. Pedidos específicos de las áreas
61. Pedido directo de los trabajadores
Otros; Especificar:
Marcar los criterios que se utilizan para seleccionar al personal de su institución que participará en una capacitación.
N° Pregunta SI NO
62. El Perfil del puesto
63. Requerimiento de inmediato superior
64. Resultados de evaluaciones de desempeño (brecha de competencias)
65. Lineamientos del Plan de Capacitación
66. Recomendación otra instancia (microrredes, redes, DIRESA, etc.)
67. Ser personal nombrado de la entidad
68. Que no haya recibido capacitación en el mismo tema
69. Este tipo de decisiones no tienen ninguna influencia política
Otros; Especificar:
70. ¿El personal contratado CAS, NO tiene ninguna restricción para recibir capacitaciones? ( ) SI ( ) NO
Marcar los roles y funciones que actualmente cumple la oficina de recursos humanos en los procesos de capacitación al personal de su institución.
N° Pregunta SI NO
71. Identificar las necesidades de capacitación del personal
72. Elaborar el Plan de Capacitación de la DIRES
73. Asesorar a las redes en el diseño de los planes de capacitación
74. Informar sobre oportunidades de capacitación
75. Facilitar los medios audiovisuales
76. Gestionar los refrigerios
77. Facilitar el local o aula de capacitación
78. Entregar materiales de enseñanza
79. Monitorear asistencia a las capacitaciones
80. Monitorear el desempeño de los docentes
81. Evaluar los conocimientos adquiridos
82. Evaluar la aplicación de conocimientos en sus funciones
83. Evaluar el impacto de las capacitaciones
84. Evaluar el financiamiento de las capacitaciones
Otros; Especificar:
Regulación Docencia - Servicio
En relación a las sedes docentes

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 129
N° Pregunta SI NO
85. ¿Cuentan con criterios para calificar a las sedes docentes?
Si la respuesta es NO, ¿Por qué?
86. ¿Estos criterios están aprobados? Si la respuesta es SI, ¿Cuándo ha sido
aprobada?_______
87. ¿Cuentan con convenios con instituciones formadoras?
Si la respuesta es NO, ¿Por qué?
88. Tienen un Comité Regional de Pregrado (COREPRES) conformado oficialmente?
Si la respuesta es NO, ¿Por qué?
89. El COREPRES se reúne al menos una vez al año?
Si la respuesta es NO, ¿Por qué?
90. ¿Cuentan con un sistema de información o de registro de todos los estudiantes que se forman en su institución?
Si la respuesta es NO, ¿Por qué?
91. ¿Todas las sedes docentes de su ámbito se encuentran acreditadas?
Si la respuesta es NO, ¿Por qué?
92. ¿Cuentan con un responsable de administrar los convenios docencia servicio?
Si la respuesta es NO, ¿Por qué?
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los convenios con las instituciones formadoras?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
93. ¿En el último año han suscrito convenios con instituciones formadoras?
( ) SI ( ) NO Solo si la respuesta es afirmativa conteste las siguientes preguntas.
¿Para qué tipo de formación tienen actualmente convenios vigentes?
N° Pregunta SI NO
94. Pre grado en Medicina
95. Post Grado en Medicina
96. Pre Grado en Enfermería
97. Pre grado en Obstetricia
98. Prácticas de institutos tecnológicos
Otros; Especificar:
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DEL SUB SISTEMA DE GESTION DEL DESARROLLO Y LA CAPACITACIÓN:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 130
GESTIÓN DE LA COMPENSACIÓN
Cuestionario Diseño de estructuras salariales
1. ¿Cuentan con un responsable de diseñar, implementar y monitorear las escalas salariales de su institución? ( ) SI ( ) NO
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de diseñar, implementar y monitorear las escalas salariales de su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
2. En el último año han elaborado alguna escala salarial?
( ) SI ( ) NO
Si la respuesta es afirmativa, responda las siguientes preguntas: 3. ¿La escala salarial está aprobada?
( ) SI ( ) NO Las escalas salariales han sido diseñadas para personal:
N° Nivel SI NO
4. Gerencial o Directivo
5. Profesionales asistenciales
6. Técnicos asistenciales
7. Profesionales administrativos
8. Técnicos administrativos
9. Personal nombrado
10. Personal contratado bajo cualquier modalidad
Las escalas salariales han sido diseñadas para personal que trabaja en:
N° Nivel SI NO
11. DIRESA
12. Redes
13. Microrredes
14. ¿Cuenta con una metodología para diseñar escalas salariales?
( ) SI ( ) NO
15. ¿Cuenta con normas para el cumplimiento y mantenimiento de la escala salarial aprobada? ( ) SI ( ) NO
El diseño de la escala salarial aprobada ha tomado en cuenta lo siguiente:
N° Pregunta SI NO
16. La valoración previa de los puestos de trabajo
17. Los perfiles de puestos
18. Más de 1 criterio
19. La disponibilidad presupuestal
20. Incorpora un componente variable ligado al desempeño

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 131
N° Pregunta SI NO
21. La escala salarial pública
22. Las funciones que realiza el puesto
23. La jerarquía del puesto que ostenta
24. La antigüedad en el puesto
25. La zona geográfica donde se ubica el puesto
26. El grupo ocupacional al que pertenece
Otro
27. ¿Han utilizado la escala salarial aprobada para tomar algún tipo de decisión?
( ) SI ( ) NO, ¿Por qué? ____________________________________
¿En qué han utilizado la escala salarial aprobada?
N° Pregunta SI NO
28. Para los nuevos contratos
29. Acompaña los ascensos del personal
30. Para definir una línea de carrera
Otro
Administración de salarios o Gestión de la Planilla
31. ¿Cuentan con un responsable de administrar los salarios y las planillas del personal en su institución? ( ) SI ( ) NO
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los salarios y las planillas del personal en su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
32. ¿ La planilla de pagos de remuneraciones y pensiones está actualizada)
( ) SI ( ) NO Administración de beneficios y bonificaciones 33. ¿Cuentan con un responsable de administrar los beneficios y bonificaciones del personal de su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar los beneficios y bonificaciones del personal de su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
¿Quiénes reciben AETAS en su institución?
Nivel SI NO Si es “SI” ¿cuántas?
Gerencial o Directivo

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 132
Nivel SI NO Si es “SI” ¿cuántas?
Profesionales asistenciales
Técnicos asistenciales
Profesionales administrativos
Técnicos administrativos
Personal nombrado
Personal contratado bajo cualquier modalidad
Administración de Incentivos 34. ¿Cuentan con un responsable de la administración de los incentivos monetarios?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de la administración de los incentivos monetarios?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
35. ¿Cuentan con un responsable de la administración de los incentivos no monetarios?
( ) SI ( ) NO
36. ¿Cuentan con normas o políticas aprobadas para la aplicación de incentivos? ( ) SI ( ) NO
37. ¿En el último año han otorgado incentivos monetarios?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
N° Pregunta SI NO
38. Los incentivos que se otorgan se hacen de acuerdo a los resultados de la evaluación del desempeño
39. Todos los trabajadores tienen la oportunidad de recibir incentivos monetarios
40. Los incentivos monetarios son individuales
41. Los incentivos monetarios son grupales
42. ¿En el último año han otorgado incentivos no monetarios?
( ) SI ( ) NO Si la respuesta ha sido afirmativa, favor responder las siguientes preguntas.
N° Pregunta SI NO
43. Los incentivos que se otorgan se hacen de acuerdo a los resultados de la evaluación del desempeño
44. Otras instituciones participan en el otorgamiento de incentivos no monetarios
¿Qué tipo de incentivos no monetarios aplican en su institución?
N° Pregunta SI NO
45. Reconocer públicamente los logros que ha conseguido una Red, MR o EESS y cómo ello contribuye a los logros de la DIRES en general.
46. El “trabajador del mes”
47. Un curso de capacitación

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 133
N° Pregunta SI NO
48. Financiar un paseo con la familia
49. Días libres
Otro
Administración de Pensiones 50. ¿Cuentan con un responsable de administrar las pensiones del personal?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de administrar las pensiones del personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
51. ¿Cuentan con una norma o directiva aprobada para administrar las pensiones del personal?
( ) SI ( ) NO
52. ¿Todas las pensiones se otorgan de acuerdo a la norma vigente? ( ) SI ( ) NO
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DE LA GESTIÓN DE LA COMPENSACIÓN:
GESTIÓN DE LAS RELACIONES HUMANAS Y SOCIALES Cuestionario Gestión del Clima Organizacional 1. ¿Cuentan con un responsable de la gestión del clima organizacional de su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de la gestión del clima organizacional de su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
En relación al clima organizacional
N° Pregunta SI NO
2. ¿Cuentan con una metodología definida para medir el clima organizacional?

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 134
N° Pregunta SI NO
3. ¿Cuentan con los instrumentos para medir el clima organizacional?
4. ¿Tienen planificado realizar la medición del clima organizacional para este año?
5. El año pasado han realizado la medición del clima organizacional?
( ) SI ( ) NO Si la respuesta a la pregunta anterior es afirmativa, responda las siguientes preguntas:
N° Pregunta SI NO
6. La medición del clima laboral ha contado con el apoyo de la máxima autoridad de la institución
7. La medición del clima laboral ha contado con la participación de al menos el 80% de los trabajadores
8. Los resultados de la medición han sido analizados con los trabajadores
9. Se han elaborado planes para mejorar el clima laboral
10. Se han tomado acciones inmediatas en un lapso no mayor a 30 días de la medición del clima laboral
11. Los resultados se tienen en cuenta para la revisión y mejora de las políticas y prácticas de la gestión de recursos humanos.
Gestión de las Relaciones Laborales 12. ¿Cuentan con un responsable de la gestión de las relaciones laborales en su institución?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de la gestión de las relaciones laborales en su institución?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
13. ¿Existen servidores que pertenecen a alguna organización sindical?
( ) SI ( ) NO ¿Cuántos trabajadores están sindicalizados?
Menos del 25% del personal
Entre el 26 al 50% del personal
Entre el 51 al 75% del personal
Más del 75% del personal
¿Con cuánta frecuencia se reúnen los sindicatos?
Grupo ocupacional Anual Mensual Trimestral Semestral A pedido
del sindicato
Ante acontecimientos
relevantes
Médicos
Enfermeras
Obstetras
Personal administrativo
Personal Técnico
General
Otros: ____________

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 135
¿Cuáles son los temas que se discuten con más frecuencia con los sindicatos?
Grupo ocupacional Salarios Bienestar
social Movilidad Funciones Ascensos Evaluación
Otro
Médicos
Enfermeras
Obstetras
Personal administrativo
Personal Técnico
General
Otros: __________
¿Cómo califica la relación entre los sindicatos y las autoridades de la institución?
Niveles Muy
buena Buena Mala
Muy mala
Médicos
Enfermeras
Obstetras
Personal administrativo
Personal Técnico
General
Otros: ___________________
14. ¿En el último año se han realizado negociaciones con los sindicatos que han dejado satisfechas a todas las
partes involucradas? ( ) SI ( ) NO
¿Cuántos días de huelga en total han tenido en año pasado?
Grupo ocupacional N° total de días
Médicos
Enfermeras
Obstetras
Personal administrativo
Personal Técnico
General
Otros: __________________________
¿Cómo califica en promedio las relaciones laborales en los diferentes niveles?
Niveles Muy
buena Buena Mala
Muy mala
DIRESA
Redes
Establecimientos de salud
¿Cuáles son las causas más frecuentes de conflictos laborales?
Grupo ocupacional SI NO
Remuneraciones
Luchas sindicales
Rivalidades internas
Otro

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 136
Grupo ocupacional SI NO
Otro
¿Cuáles son los mecanismos de solución de conflictos que mas se han usado en la institución el año pasado?
Grupo ocupacional SI NO
Negociaciones con el sindicato
Negociaciones directas con los agraviados
Negociaciones con los jefes inmediatos superiores
Otro
Otro
Bienestar y Seguridad en el Trabajo 15. ¿Cuentan con un responsable de gerenciar los procesos de bienestar de persona?
( ) SI ( ) NO De acuerdo con el ROF vigente ¿Quién es la instancia responsable de gerenciar los procesos de bienestar de personal?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
16. ¿Existen programas de bienestar social en su institución?
( ) SI ( ) NO 17. ¿Planifican actividades de bienestar social en su institución?
( ) SI ( ) NO 18. ¿Se cumplen las actividades programadas de bienestar social en su institución?
( ) SI ( ) NO Si la respuesta a la pregunta anterior es afirmativa, ¿qué tipo de actividades se programan?
N° Pregunta SI NO
19. Celebraciones de feriados oficiales
20. Celebraciones de feriados regionales
21. Celebraciones de cumpleaños
22. Celebraciones de aniversario de la entidad
23. Organización de campeonatos deportivos
24. Servicio de cafetería o restaurante
25. Servicios de préstamos de dinero
26. Apoyo financiero para capacitaciones
27. Guardería
28. Club de la tercera edad
29. Organización de viajes
30. Organización de hinkanas
31. Organización de paseos con la familia
Otro
Otro
32. ¿Cuentan con un responsable de gerenciar los procesos de salud y seguridad en el trabajo?
( ) SI ( ) NO

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 137
De acuerdo con el ROF vigente ¿Quién es la instancia responsable de gerenciar los procesos de salud y seguridad en el trabajo?
Nivel
¿Existe? En caso de que exista
SI NO Nombre de la unidad
responsable Función específica
En DIRESA
En la Red
En la MR
33. ¿Existen normas o políticas aprobadas de salud y seguridad en el trabajo en su institución?
( ) SI ( ) NO
34. ¿Existen programas de salud y seguridad en el trabajo en su institución? ( ) SI ( ) NO
35. ¿Planifican actividades de salud y seguridad en el trabajo en su institución?
( ) SI ( ) NO 36. ¿Se cumplen las actividades programadas de salud y seguridad en el trabajo en su institución?
( ) SI ( ) NO Si la respuesta a la pregunta anterior es afirmativa, ¿qué tipo de actividades se programan?
N° Pregunta SI NO
37. Fumigación de los lugares de trabajo
38. Provisión de equipamiento protector de enfermedades, epidemias, etc.
39. Otorgamiento de seguros de salud ante accidentes o epidemias
40. Campañas de despistaje de enfermedades ocupacionales
41. Campañas de vacunación
42. Evaluaciones de defensa civil
Otros
Otros
Otros
COMENTARIO ACERCA DE LA ORGANIZACIÓN Y FUNCIONAMIENTO DE LA GESTIÓN DE LAS RELACIONES LABORALES:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 138
7.2 Qualitative assessment of HRMS conducted by PARSALUD II in 4
Regions
PARSALUD: Human Resources Management System in Ucayali RHD
SOURCE: PARSALUD II technical report
PARSALUD: Human Resources Management System in Cusco RHD
SOURCE: PARSALUD II technical report
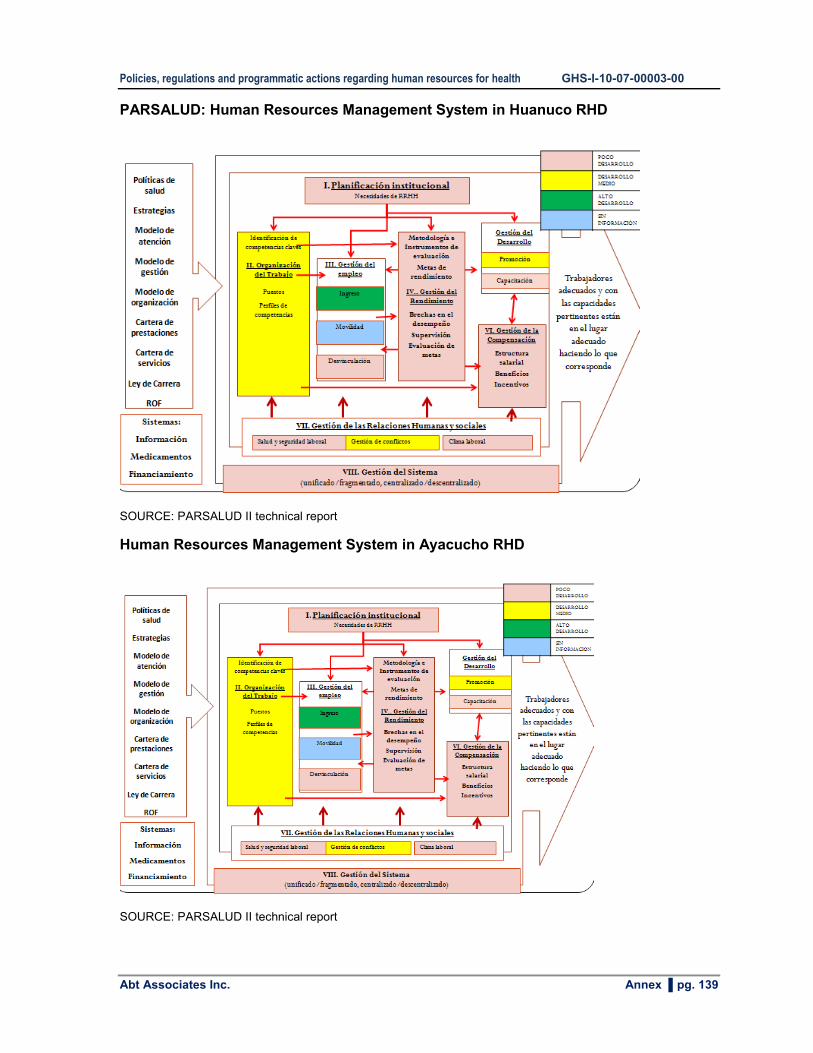
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 139
PARSALUD: Human Resources Management System in Huanuco RHD
SOURCE: PARSALUD II technical report
Human Resources Management System in Ayacucho RHD
SOURCE: PARSALUD II technical report

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 140
PARSALUD: Human Resources Management System in Cajamarca RHD
SOURCE: PARSALUD II technical report
7.3 SMT-RHD: HHR regional policies
Below are 7 formulated policy guidelines, the same that are aligned to the national policy for HHR management and development.
Lineamiento de Política 1.- Formación de los RHUS basado en el Modelo de Atención
Integral de Salud, el perfil epidemiológico y sociocultural de la población, acorde a las
necesidades regionales, locales bajo el marco de la descentralización.
Lineamiento de Política 2.- Gestión de procesos de capacitación articulados a proyectos
de desarrollo institucional, utilizando la Educación Permanente de la Salud y el enfoque de
competencias para fortalecer el desempeño laboral, caracterizado por el respeto a los
derechos, la equidad de género y la pertinencia cultural de la población.
Lineamiento de Política 3.- Planificación estratégica de RHUS, sustentada en la
información de necesidades reales de distribución y ubicación adecuada de RHUS, acorde
al perfil demográfico, sociocultural y epidemiológico de la región, destacando las prioridades
sanitarias de la población más excluida.
Lineamiento de Política 4.- Gestión de RHUS a nivel regional, que asegure servicios de
calidad, generando la participación activa del personal en las innovaciones
organizacionales y la toma de decisiones para conciliar las necesidades de la población,
los requerimientos básicos de los servicios de salud y las necesidades de los RHUS.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 141
Lineamiento de Política 5.- Valoración y reconocimiento del trabajo de los agentes
comunitarios de salud como aliados estratégicos en las acciones preventivo-promocionales
del sistema de salud.
Lineamiento de Política 6.- Aplicación de un nuevo marco normativo laboral consensuado
con los RHUS, en base a perfiles ocupacionales por competencias con un sistema de
compensación e incentivos; y procesos adecuados de reclutamiento, selección del
personal, que aplique la promoción en la carrera pública considerando los derechos y
deberes, la equidad de género, y el respeto a la diversidad.
Lineamiento de Política 7.- Generar condiciones de trabajo, orientadas por relaciones
laborales que promuevan ambientes de trabajo saludables, contribuyan a fortalecer los
valores organizacionales, la calidad de las personas, y el aseguramiento de servicios de
calidad a la población.
7.4 National agenda for research in HHR
Resolución Ministerial 212-2010-MINSA
SE RESUELVE:
Artículo 1º.- Aprobar la Agenda Nacional de investigación para conocer los problemas de
los Recursos Humanos en Salud, para el periodo 2011-2014, que a continuación se
señalan:
1. Articulación de la formación en pregrado de los recursos humanos en salud con las
necesidades de salud del país.
2. Capacidades del docente y estudiante para el uso y aplicación de las tecnologías de
información y comunicación en el proceso de enseñanza aprendizaje en la formación en
pregrado de los recursos humanos en Salud
3. Capacidades pedagógicas, metodología y estilos de aprendizaje durante la formación
del estudiante de pregrado en escenarios comunitarios.
4. Necesidades de las regiones en la formación de recursos humanos en salud en
estudios de postgrado y especialización según niveles de atención.
5. Impacto de las experiencias en la formación y logro de competencias de los recursos
humanos en salud en especialización y postgrado.
6. Evaluación de la formación e investigación en postgrado y segunda especialización en
salud en respuesta a las necesidades y problemas sanitarios del país.
7. Determinación de brechas de recursos humanos por niveles de atención para el
aseguramiento en salud.
8. Análisis de procesos en el marco de la implementación del plan esencial de
aseguramiento en salud con énfasis en el estudio de tiempos y movimientos para la
dotación de recursos humanos.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 142
9. Análisis y formulación de estrategias de financiamiento para la contratación de recursos
humanos en el marco del aseguramiento universal en salud.
10. Perfil de competencias asistenciales y gerenciales, para la atención primaria de salud
con enfoque de interculturalidad del personal existente en el equipo básico de salud.
11. Motivación e incentivos para desarrollar la atención primaria de salud en el primer nivel
de atención.
12. Impacto de los agentes comunitarios en salud y estrategias de integración en atención
primaria de salud.
13. Desarrollo de capacidades en base a competencias que respondan a las necesidades y
objetivos institucionales y sectoriales.
14. Determinantes que influyen en el desarrollo laboral.
15. Ética y valores personales en la gestión de recursos humanos en salud.
16. Evaluación de experiencias exitosas nacionales e internacionales para la retención de
profesionales de salud.
17. Evaluación del impacto económico y sanitario de la migración interna de profesionales
de salud.
18. Dinámica y factores asociados a la movilización interna de los profesionales del sector
salud.
19. Prevalencia e incidencia de la exposición, enfermedades y accidentes ocupacionales.
20. Estado de la implementación de las normas y organización de los servicios para la
gestión de la salud y seguridad del trabajo.
21. Factores de riesgo ergonómicos y psicosociales.
22. Estudio de incentivos laborales.
23. Estudio de ética y funcionamiento.
24. Inequidad entre servidores y funcionarios de la salud.
25. Acceso a cargos públicos, impacto en el clima laboral y prestación de los servicios de
salud.
26. Comparación de la jerarquía organizacional en los establecimientos de salud en relación
a cargos y puestos.
27. Marco legal en materia laboral.
28. Identificar las competencias gerenciales a nivel regional para la gestión de recursos
humanos y la gestión sanitaria regional.
29. Identificar y analizar las políticas/normas nacionales de recursos humanos que deben
actualizarse al nuevo contexto regional.
30. Determinar la situación de las unidades orgánicas o sus equivalentes de gestión de
recursos humanos en las regiones.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 143
7.5 ASEGURA software for HHR requirements calculations
Startup screen
Screen: Time required for various medical procedures by type of HHR – First level of care
(hours)
This screen displays the total number of medical procedures established by PEAS for the
first level of care (132) and respective Current Procedural Terminology (CPT) codes22. The
22 The Current Procedural Terminology (CPT) is a medical code set maintained by the American Medical
Association (AMA) through the CPT editorial panel. The CPT code set (copyright protected by the AMA)

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 144
"N°" column corresponds to the total number of procedures for a given population. The next
set of columns represents each type of HR and the total hours they spend on each
procedure based on activity standards23 set by the MoH. The last row displays the sum of all
hours for each HR type in delivering the PEAS package.
7.6 Using the spreadsheet to facilitate calculations
This annex contains the procedure manual created with the Ayacucho RHD to facilitate
calculations at the micro-network level. The manual was not approved due to RHD authority
turnover.
PROCEDIMIENTO PARA DETERMINAR LA BRECHA DE RECURSOS HUMANOS EN
SALUD PARA EL PRIMER NIVEL DE ATENCION
I. FINALIDAD. La presente directiva tiene la finalidad de contribuir con mejorar la calidad
de atención de los servicios de salud del primer nivel de atención mediante la dotación
adecuada de recursos humanos en salud, distribuidos en lugares adecuados.
II. OBJETIVOS:
a. General. Lograr que los servicios de salud del primer nivel de atención cuenten
con recursos humanos adecuados en cantidad y calidad, que permitan satisfacer
las necesidades de salud de la población ayacuchana.
b. Específicos. La presente directiva permitirá a los jefes de Redes y micro-redes
tomar decisiones relacionadas con:
Establecer la cantidad requerida del personal de salud para atender a la
población que está bajo su responsabilidad y territorio.
Mejorar la ubicación del personal con que ya cuenta en los servicios de salud.
Distribuir y asignar tareas, que permitan aprovechar de manera óptima el tiempo
del personal para producir las atenciones requeridas,
Comparar el esfuerzo y presión laboral a los que está sometido el personal de los
establecimientos, dado que los desequilibrios se pueden manifestar como
sobrecarga o distención laborales.
Distribuir mejor el tiempo disponible del personal para la producción de los
servicios de salud.
describes medical, surgical, and diagnostic services and is designed to communicate uniform information about
medical services and procedures among physicians, coders, patients, accreditation organizations, and payers for
administrative, financial, and analytical purposes.
23 The average amount of time a case should take each staff category to complete in compliance with acceptable
professional standards (WISN, page 5).

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 145
III. ÁMBITO DE APLICACIÓN. Lo establecido en la presente Directiva es de aplicación y
cumplimiento obligatorio de las Unidades Ejecutoras de Salud del ámbito de
competencia de la Dirección Regional de Salud de la Región Ayacucho.
IV. BASE LEGAL
a. Ley Nº 27680.- Aprueba reforma constitucional del Capítulo XIV del Título IV, sobre
descentralización.
b. Ley Nº 27783, Ley de Bases de la Descentralización.
c. Ley Nº 26842, Ley General del Salud.
d. Ley Nº 27867, Ley Orgánica de Gobiernos Regionales.
e. Ley Nº 28411, Ley General del Sistema Nacional de Presupuesto Público, Título III,
“Normas complementarias para la gestión presupuestaria”.
f. D.S. Nº 064-2004-PCM, “Plan Nacional para la superación de la Pobreza”
g. Decreto Legislativo Nº 1057 y su Reglamento aprobado por D.S. Nº 075-2008-PCM,
modificado por D.S. Nº 065-2011-2011-PCM.
h. Ordenanza Regional Nº 059-2005 que aprueba las Políticas Regionales de RRHH.
i. Reglamento de Organización y Funciones de la DIRESA
j. Lineamientos Generales de Política Regional de Gestión y Desarrollo del Potencial
Humano en Salud
V. DISPOSICIONES GENERALES.
a. Principios y valores: El Personal Administrativo de la Dirección Regional de Salud
Ayacucho se rige bajo los Valores y Principios siguientes:
i. Calidad. La Calidad es un enfoque que compromete a todo servidor y a todo nivel
operacional, entendido como satisfacción del usuario, que puede evidenciarse a
través de tres dimensiones: dimensión técnica, dimensión humada y la calidad
del entorno.
ii. Cumplimiento. Es un valor realizable solo si se cumple tres condiciones: que los
objetivos institucionales sean verificables; que las tareas y responsabilidades
sean explicitas; y que los niveles de autoridad sean respetadas.
iii. Seriedad. Basada en el principio de honestidad en nuestras relaciones con el
usuario externo, el usuario interno y los proveedores.
iv. Eficiencia. Enfocada al uso optimo de los recursos.
b. Objetivos institucionales: El personal Administrativo de la Dirección Regional de
Salud Ayacucho desempeña un rol para el logro de los siguientes objetivos
institucionales:
i. Reducir la Desnutrición Infantil.
ii. Evitar la Mortalidad Materna Neonatal.
c. Estrategias institucionales: Son estrategias de la Dirección Regional de Salud
Ayacucho:
i. Estrategia Sanitaria Articulado Nutricional.
ii. Estrategia Sanitaria Materno Neonatal
iii. Estrategia Sanitaria TBC/HIV – Enfermedades Transmisibles.
iv. Estrategia Sanitaria Metaxénicas y Zoonóticas.
v. Estrategia Sanitaria No Transmisibles.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 146
vi. Estrategia Sanitaria Control de Cáncer de Cuello Uterino.
d. Políticas. La presente Directiva se implementa en el marco de los Lineamientos
Generales de Política Regional de Gestión y Desarrollo del Potencial Humano en
Salud. Donde su Política 2 establece: “Planificación estratégica de recursos humanos,
para su distribución equitativa, de acuerdo al MAIS, el perfil demográfico, socio
cultural y epidemiológico de la Región, cautelando las condiciones de trabajo del
personal de salud”. La Dirección Regional de Salud es responsable de la
planificación territorial de los recursos, en coordinación con las unidades
desconcentradas. La elaboración de la presente directiva responde al siguiente marco
conceptual:
e. Marco conceptual:
Planificación de recursos humanos en salud: De acuerdo con la OMS la planificación
de RRHH en Salud consiste en la “Estimación del número de personas y los tipos de
conocimientos, habilidades y actitudes que requieren para alcanzar objetivos
sanitarios predeterminados y una determinada situación de salud”. El Ministerio de
Salud ha definido una propuesta de Sistema de Gestión Descentralizada de RRHH en
Salud, donde un primer subsistema está relacionado con la Planificación de RRHH. El
Objeto del Subsistema de Planificación de Recursos Humanos, involucra la definición
de necesidades, cuantitativas y cualitativas de recursos humanos a corto, medio y
largo plazo; contrastadas con las capacidades internas; así como las acciones que
deben emprenderse para cubrir la brecha identificada. La planificación de recursos
humanos comprende programar las necesidades de recursos humanos de la
organización y establecer los pasos necesarios para satisfacer esas necesidades.
Esta planificación es el primer paso de toda gestión efectiva de los recursos humanos.
El desafío de este subsistema es lidiar con la migración interna y externa de los
trabajadores de salud, así como la alta rotación del personal fundamentalmente la
falta de información. Resulta difícil hacer proyecciones en estos escenarios. La
planificación de los recursos humanos en salud debe estar estrechamente vinculada y
articulada con las políticas y estrategias institucionales, con el modelo de atención de
salud, el modelo de gestión, el modelo de organización de los servicios de salud,
entre otros. En este subsistema se plantean las siguientes interrogantes:
- ¿Hasta qué punto la capacidad de planificar las necesidades de recursos humanos
repercute en el desempeño de los mismos?
- ¿Se encuentran las personas adecuadas en los puestos adecuados?
- ¿Podemos pronosticar las exigencias actuales y futuras de recursos humanos?
- ¿Sabemos cómo y dónde identificar a las personas que poseen las aptitudes
necesarias para satisfacer esas necesidades?
- ¿Podemos vincular la misión y metas organizacionales con la planificación de
recursos humanos?
Los procesos principales que se desarrollan en este subsistema son:
Gestión de la información de recursos humanos: Un aspecto importante e
imprescindible para una adecuada planificación de recursos humanos y para el
cálculo de los requerimientos institucionales de recursos humanos es contar con

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 147
información actualizada y confiable acerca de la cantidad y distribución de recursos
humanos en las diferentes unidades de la institución.
Diseño de políticas y planes para cubrir la brecha de recursos humanos en
salud: Para cubrir la brecha de recursos humanos en salud es necesario realizar un
análisis cuantitativo y cualitativo de necesidades de recursos humanos; un análisis de
la disponibilidad de recursos humanos; la definición de la brecha de recursos
humanos para la definición de estrategias que permitan cubrir la brecha identificada.
Las funciones principales del Subsistema de Planificación de RRHH en salud son:
Mantener actualizada la información de recursos humanos de la institución. Identificar
las necesidades de incorporación de personal en base a los planes y estrategias
institucionales. Diseñar estrategias, planes y políticas destinadas a cubrir las
necesidades de recursos humanos.
f. Enfoques. Se definen varios enfoques para determinar la dotación de RRHH en
Salud. Entre los tres principales más utilizados más utilizados son:
i. Basado en las necesidades de salud. Permite estimar necesidades futuras de RHUS
con base en necesidades de servicios de salud, ajustados por diversos criterios.
Satisface las necesidades de salud. Es lógico, consistente e independiente a la
utilización actual de servicios de salud, pero requiere de normas o estándares de
producción.
ii. Basado en la utilización futura de servicios de salud. Este enfoque proyecta
requerimientos futuros basados en el uso actual de los servicios de salud. Existen
pocos cambios en los ratios de utilización de una población específica. resultan ser
alcanzables financieramente sin embargo es una proyección del status quo cuyo
supuestos, inexactos, pueden ocasionar errores de cálculo por que no toma en
cuenta el nivel de acceso a servicios de salud.
iii. Basado en coeficientes de población. Proporción entre trabajadores de salud y
población. fácil de aplicar y entender, pero no permite explorar interacciones entre:
mezcla, distribución, productividad, resultados.
La selección de un enfoque dependerá de la disponibilidad de información confiable,
del nivel de decisión y del problema o restricción en la gestión de recursos humanos
que se pretende resolver.
g. Metodología. La metodología para la estimación de la dotación de recursos humanos
en salud desde la Micro red está basado en las necesidades de salud, con las
siguientes características:
1. Se basa en la estimación de la probabilidad de ocurrencia de casos, por grupo
etáreo, para una población determinada.
2. Para cada caso y sus respectivas variantes, se definen los procedimientos
asistenciales involucrados, en base a las normas vigentes.
3. Para cada procedimiento se establecen los tipos de RRHH que intervienen y el
tiempo que dedica cada uno de ellos a cada procedimiento, basado en las
normas vigentes.
4. Toma en cuenta el tiempo realmente disponible para la prestación
5. Permite ajustes de acuerdo a la capacidad resolutiva actual y potencial en el
corto plazo

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 148
6. Permite calcular los requerimientos de recursos humanos ajustado en función
al nivel de ruralidad del distrito donde se ubican los establecimientos de salud.
7. Permite introducir la cantidad actual de recursos humanos en el
establecimiento de salud, para determinar la brecha que es necesario cubrir.
8. Permite contar con cuadros finales de análisis que permiten una mejor
asignación de los recursos humanos al interior de la microrred.
La metodología para el análisis de necesidades de recursos humanos en salud
desde la microrred comprende los factores que intervienen entre la disponibilidad
de recursos y la producción de servicios. Los cuales están relacionados con:
a. La productividad de los recursos humanos y su rendimiento
b. El tiempo realmente utilizado en la prestación de servicios de salud
c. La distribución de la carga de trabajo
d. La accesibilidad geográfica para la asignación territorial.
VI. DISPOSICIONES ESPECÍFICAS:
Para realizar los cálculos de dotación de recursos humanos en salud para el primer nivel de
atención, cada microrred contará con un aplicativo en excell. Las hojas de cálculo
destinadas para la estimación tienen tres partes:
(i) La parte superior para introducir los datos;
(ii) La parte intermedia, para el procesamiento automáticamente de los datos
relacionados con:
El listado de los procedimientos asistenciales por tipo de establecimiento de salud.
Las fórmulas que calculan automáticamente la cantidad de procedimientos en un
año, en base a la población asignada.
Las fórmulas que calculan automáticamente los tiempos que cada proveedor
destina al total de procedimientos.
(iii) La parte inferior, para mostrar los resultados.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 149
I. PARTE SUPERIOR
Para el ingreso de datos
II. PARTE
INTERMEDIA
Para el procesamiento de
datos ingresados.
III. PARTE INFERIOR
Para mostrar los resulta-
dos
Ingreso de datos: Cada responsable en la microrred deberá introducir los datos
relacionados con cada uno de los establecimientos de salud de la MR, para ello deberá
llenar los espacios que se encuentran en color rosado.
Cada establecimiento de salud tiene una hoja de cálculo donde se ingresarán sus datos.
SOLO DEBERÁ LLENARSE LA INFORMACIÓN QUE SE DETALLA A CONTINUACIÓN. A
continuación se detalla el tipo de información a llenar.
a. Datos Generales: Esta información permitirá identificar la unidad de análisis. Los
datos que se ingresen en los campos respectivos, permanecerán a lo largo del
análisis.
Ejemplo:
DIRESA Ayacucho
RED Cora Cora
MR Cora Cora
EESS CS Pacapausa
b. Población asignada: En este campo, se deberá colocar la población total de la
unidad de análisis.
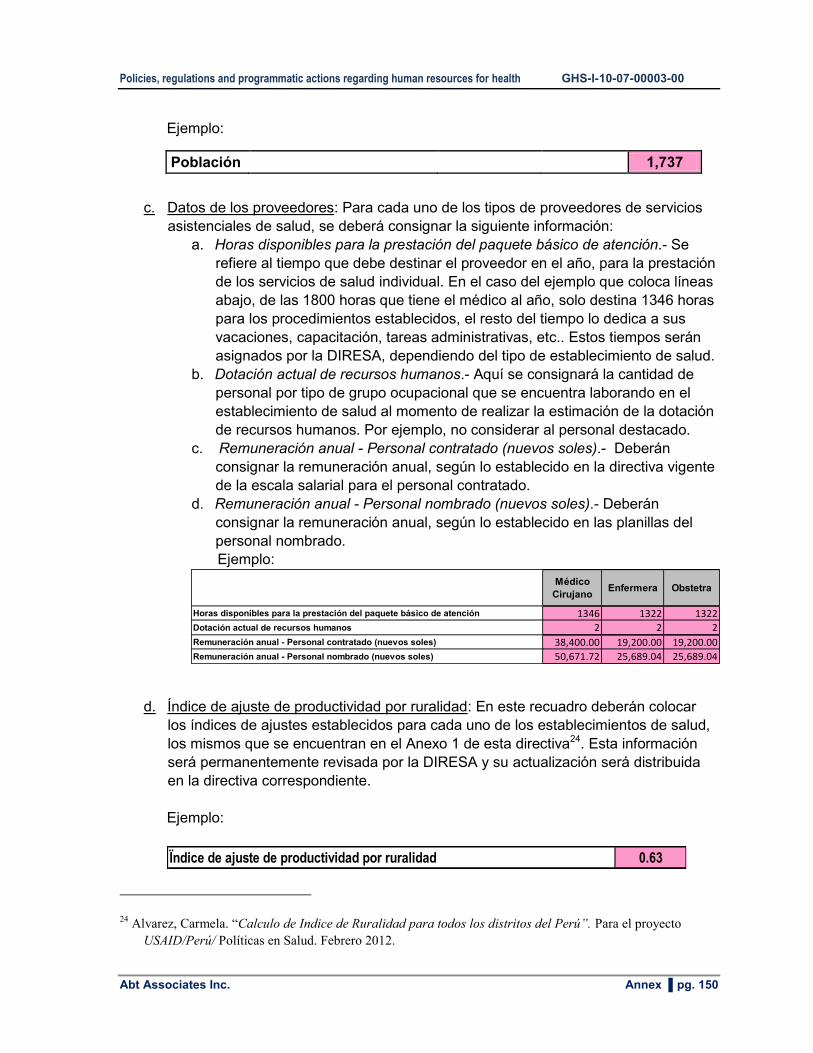
Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 150
Ejemplo:
Población 1,737
c. Datos de los proveedores: Para cada uno de los tipos de proveedores de servicios
asistenciales de salud, se deberá consignar la siguiente información:
a. Horas disponibles para la prestación del paquete básico de atención.- Se
refiere al tiempo que debe destinar el proveedor en el año, para la prestación
de los servicios de salud individual. En el caso del ejemplo que coloca líneas
abajo, de las 1800 horas que tiene el médico al año, solo destina 1346 horas
para los procedimientos establecidos, el resto del tiempo lo dedica a sus
vacaciones, capacitación, tareas administrativas, etc.. Estos tiempos serán
asignados por la DIRESA, dependiendo del tipo de establecimiento de salud.
b. Dotación actual de recursos humanos.- Aquí se consignará la cantidad de
personal por tipo de grupo ocupacional que se encuentra laborando en el
establecimiento de salud al momento de realizar la estimación de la dotación
de recursos humanos. Por ejemplo, no considerar al personal destacado.
c. Remuneración anual - Personal contratado (nuevos soles).- Deberán
consignar la remuneración anual, según lo establecido en la directiva vigente
de la escala salarial para el personal contratado.
d. Remuneración anual - Personal nombrado (nuevos soles).- Deberán
consignar la remuneración anual, según lo establecido en las planillas del
personal nombrado.
Ejemplo:
Médico
CirujanoEnfermera Obstetra
Horas disponibles para la prestación del paquete básico de atención 1346 1322 1322
Dotación actual de recursos humanos 2 2 2
Remuneración anual - Personal contratado (nuevos soles) 38,400.00 19,200.00 19,200.00
Remuneración anual - Personal nombrado (nuevos soles) 50,671.72 25,689.04 25,689.04
d. Índice de ajuste de productividad por ruralidad: En este recuadro deberán colocar
los índices de ajustes establecidos para cada uno de los establecimientos de salud,
los mismos que se encuentran en el Anexo 1 de esta directiva24. Esta información
será permanentemente revisada por la DIRESA y su actualización será distribuida
en la directiva correspondiente.
Ejemplo:
Ïndice de ajuste de productividad por ruralidad 0.63
24 Alvarez, Carmela. “Calculo de Indice de Ruralidad para todos los distritos del Perú”. Para el proyecto
USAID/Perú/ Políticas en Salud. Febrero 2012.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 151
Resultados a nivel del establecimiento de salud: Una vez que se han ingresado los
datos, los resultados aparecerán automáticamente al final de la hoja de cálculo respectiva.
Los resultados que aparecerán son los siguientes:
Ejemplo:
TOTAL DE HORAS NECESARIAS 804.60 3,028.85 942.06
Médico
CirujanoEnfermera Obstetra
RRHH NECESARIOS SIN AJUSTE 0.60 2.29 0.71
RRHH AJUSTADOS POR RURALIDAD 0.95 3.64 1.13
DOTACIÓN ACTUAL 2.00 2.00 2.00
BRECHA DE RRHH SIN AJUSTE -1.40 0.29 -1.29
BRECHA DE RRHH CON AJUSTE -1.05 1.64 -0.87
a. Total de horas necesarias: Lo que aparece es el total de horas al año que se requiere
para la prestación de todos los procedimientos, por cada tipo de proveedor. En el
ejemplo que se muestra a continuación, se requiere un total de 804.6 horas del Médico
Cirujano para todas las atenciones previstas.
b. RRHH necesarios sin ajuste: Se efiere al número de RRHH que se requiere para
realizar todos los procedimientos establecidos para la población asignada. Esta
cantidad resulta de dividir el “Total de horas necesarias” entre la cantidad de “Horas
disponibles para la prestación del paquete básico de atención”. En el ejemplo que se
muestra, se requieren 804.6 horas del Médico que divididas entre las 1346 horas
disponibles, nos dan 0.60 médicos.
c. RRHH ajustados por ruralidad: La cantidad de “RRHH necesarios sin ajuste” se divide
entre el “Índice de ajuste de productividad por ruralidad” para tener una nueva
estimación de requerimientos de RRHH ajustados por el nivel de ruralidad del distrito
donde se ubica el establecimiento de salud. En el ejemplo que se muestra, los 0.6
médicos que se necesitan, se dividen entre 0.63 que es su índice de ajuste por
ruralidad, y sale una nueva estimación: 0.95 médicos.
d. Dotación actual: Es una copia de la información introducida en la parte superior de la
hoja de cálculo.
e. Brecha de RRHH sin ajuste: Resulta de realizar la resta de “RRHH necesarios sin
ajuste” menos la “dotación actual”. En el ejemplo, el EESS necesita 0.6 médicos y tiene
2 médicos, lo que significa que tiene una sobredotación de 1.40 médicos (sale en
negativo). Si se observa el caso de las enfermeras, se requieren 2.29 enfermeras y se
tienen 2, por lo que faltan 0.29 enfermeras.
f. Brecha de RRHH con ajuste: Resulta de realizar la resta de “RRHH necesarios con
ajuste” menos la “dotación actual”. En el ejemplo, el EESS necesita 0.95 médicos
ajustados por ruralidad y tiene 2 médicos, lo que significa que tiene una sobredotación
de 1.05 médicos (sale en negativo). Si se observa el caso de las enfermeras, se
requieren 3.64 enfermeras (con el ajuste)y se tienen 2, por lo que faltan 1.64
enfermeras.
g. Información complementaria: Conociendo la brecha por cubrir y la remuneración
anual, se puede obtener el costo de cubrir la brecha.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 152
Ejemplo:
COSTO PARA CUBRIR LA BRECHA SIN AJUSTE
Con personal contratado -53,845.62 5,589.40 -24,717.99
Con personal nombrado -53,263.99 42,045.00 -22,320.73
COSTO PARA CUBRIR LA BRECHA CON AJUSTE
Con personal contratado -40,364.47 31,424.45 -16,682.53
Con personal nombrado -53,263.99 42,045.00 -22,320.73
h. Resultados a nivel de la microrred: Un visión global de la situación de dotación de
recursos humanos a nivel de la MR se observa en la hoja de cálculo “Comparativo”,
donde se puede observar de manera integrada la infomación de todos los EESS de la
MR.
La matriz que se observará contiene la columna EESS donde están todos los EESS
de esa MR, con sus respectivas poblaciones. Para cada grupo ocupacional, se
tienen los siguientes indicadores:
- RRHH necesarios ajustados por ruralidad (A).
- Dotación actual (B)
- Brecha de RRHH (A-B)
- Ratio de carga laboral (B/A): Es un indicador para la gestión de RRHH que nos
mide la magnitud de la carga de trabajo que tiene el prestador. Lo deseado es
que el resultado sea “1”; un número mayor a “1” indica “sobredotación”, un
número menor a “1” indica “sobrecarga de trabajo”; mientras mas cerca de “0”
mayor sobrecarga. Por ejemplo, los 2 médicos del PS Chaviña realizan el trabajo
que debe ser realizado por solo 1 médico (0.95), lo que da un ratio de carga
laboral de 2.11, al ser mayor a “1” indica que hay “sobredotación de médicos en
PS Chaviña”. En el caso de las enfermeras, las 2 que están actualmente en el
CS Chaviña están cargado el trabajo que deberían realizar las casi 4 enfermeras
que se necesitan, lo que da un ratio de carga laboal de 0.55, al ser menor a “1”
indica que hay “sobrecarga”.
- Ratio x 10000 habitantes (B/pob*10000): Es un indicador que es útil para
poblaciones grandes, pero que no ayuda mucho para las poblaciones pequeñas
que existen a nivel de EESS.
Nota: Se mantiene este indicador, ya que estas matrices pued ser usadas a nivel
de Redes y DIRESA.
Ejemplo:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 153
EESS PoblaciónMédico
CirujanoEnfermera Obstetra
RRHH necesarios ajustados por ruralidad (A) 0.95 3.64 1.13
Dotación actual (B) 2.00 2.00 2.00
BRECHA DE RRHH (A-B) -1.05 1.64 -0.87
Ratio de carga de trabajo (B/A) 2.11 0.55 1.77
Ratio x 10,000 habitantes (B/Pob *10000) 8.12 8.12 8.12
RRHH necesarios ajustados por ruralidad (A) 0.30 1.13 0.35
Dotación actual (B) 1.00 0.00 0.00
BRECHA DE RRHH (A-B) -0.70 1.13 0.35
Ratio de carga de trabajo (B/A) 3.39 0.00 0.00
Ratio x 10,000 habitantes (B/Pob *10000) 16.45 0.00 0.00
RRHH necesarios ajustados por ruralidad (A) 0.56 2.16 0.67
Dotación actual (B) 1.00 1.00 1.00
BRECHA DE RRHH (A-B) -0.44 1.16 -0.33
Ratio de carga de trabajo (B/A) 1.78 0.46 1.49
Ratio x 10,000 habitantes (B/Pob *10000) 6.84 6.84 6.84
RRHH necesarios ajustados por ruralidad (A) 5.18 19.34 6.18
Dotación actual (B) 4.00 6.00 6.00
BRECHA DE RRHH (A-B) 1.18 13.34 0.18
Ratio de carga de trabajo (B/A) 0.77 0.31 0.97
Ratio x 10,000 habitantes (B/Pob *10000) 3.58 5.38 5.38
PS Calpamayo
PS Sancos
608
1,461
MR Cora Cora 11,158
PS Chaviña 2,463
Análisis de la información:
En la hoja de cálculo “Gráficos” se encontrarán un conjunto de tablas y gráficos que
permitirán analizar la información relacionada con la distribución de los RRHH entre los
EESS de la MR.
Las últimas tablas resumen todos los cálculos realizados y permiten tomar decisiones.
Ejemplo: MR Cora Cora
Grupo ocupacional
Población EESS
RRHH
necesarios
ajustados por
ruralidad (A)
Dotación
actual (B)
BRECHA DE
RRHH (A-B)
Problema en
gestión de
RRHH
Ratio de
carga de
trabajo (B/A)
Presión en la
carga Laboral
1,737 CS Pacapausa 0.67 0 1 escasez 0.00 alta
1,087 PS Aycara 0.35 0 0 escasez 0.00 alta
682 PS Ccasaccahua 0.22 0 0 escasez 0.00 alta
655 PS Muchapampa 0.21 0 0 escasez 0.00 alta
682 PS San Marcos 0.22 0 0 escasez 0.00 alta
728 PS San Francisco de Rivacayco 0.35 0 0 escasez 0.00 alta
566 PS Ccochani 0.27 0 0 escasez 0.00 alta
409 PS Upahuacho 0.20 0 0 escasez 0.00 alta
450 PS Sansaycca 0.22 0 0 escasez 0.00 alta
1,699 PS Chaquipampa 0.65 0 1 escasez 0.00 alta
2,463 PS Chaviña 0.95 2 -1 sobredotación 2.11 no hay sobrecarga
608 PS Calpamayo 0.30 1 -1 sobredotación 3.39 no hay sobrecarga
1,461 PS Sancos 0.56 1 0 sobredotación 1.78 no hay sobrecarga
13,227 Total de la MR 5.18 4 2 escasez 0.77 alta
Médico Cirujano
El análisis de esta tabla debe realizarse a nivel de la MR. Por ejemplo, esta MR requiere
5.18 médicos, es decir 6 médicos. La pregunta es ¿Dónde asigno a estos 6 médicos?. Si
solo analizo las cantidades puedo decir que requiero colocar médicos en los 6 EESS con
cifras mayores, pero debo tomar en cuenta otras variables como:
- Ubicación del EESS
- Tipo de contrato del personal.
- Nivel de producción del EESS.
La siguiente tabla muestra cómo se modifican los resultados con la reasignación.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 154
DECISIÓNGrupo ocupacional
Población EESS
RRHH
necesarios
ajustados por
ruralidad (A)
Dotación
actual (B)
BRECHA DE
RRHH (A-B)
Problema en
gestión de
RRHH
Ratio de
carga de
trabajo (B/A)
Presión en la
carga Laboral
1,737 CS Pacapausa 1 0 1 escasez 0.00 alta
1,087 PS Aycara 1 0 1 escasez 0.00 alta
682 PS Ccasaccahua 0 0 0 normal #¡DIV/0! #¡DIV/0!
655 PS Muchapampa 0 0 0 normal #¡DIV/0! #¡DIV/0!
682 PS San Marcos 0 0 0 normal #¡DIV/0! #¡DIV/0!
728 PS San Francisco de Rivacayco 1 0 1 escasez 0.00 alta
566 PS Ccochani 0 0 0 normal #¡DIV/0! #¡DIV/0!
409 PS Upahuacho 0 0 0 normal #¡DIV/0! #¡DIV/0!
450 PS Sansaycca 0 0 0 normal #¡DIV/0! #¡DIV/0!
1,699 PS Chaquipampa 1 0 1 escasez 0.00 alta
2,463 PS Chaviña 1 2 -1 sobredotación 2.00 no hay sobrecarga
608 PS Calpamayo 0 1 -1 sobredotación #¡DIV/0! #¡DIV/0!
1,461 PS Sancos 1 1 0 normal 1.00 normal
13,227 Total de la MR 6 4 3 escasez 0.67 alta
Médico Cirujano
Las unidades ejecutoras deberán tomar en cuenta estas matrices para la determinación de
las brechas de RRHH a nivel de MR y EESS, así como para determinar la asignación de
RRHH a nivel de MR.
Es importante que antes de llenar la información, se GRABE el archivo de trabajo con un
nombre diferente. Cada vez que deseen hacer un nuevo cálculo, pueden usar la matriz en
blanco y grabarla con el nombre que más convenga.
VII. RESPONSABILIDADES:
DIRESA:
a) Como autoridad sanitaria en la Región le corresponde la implementación, el
monitoreo, el control y la evaluación del cumplimiento de la presente directiva.
b) Brindar asistencia técnica a las unidades ejecutoras para el correcto cumplimiento
de la presente directiva.
RED/UNIDAD EJECUTORA:
a) Aplicar y ejecutar lo dispuesto en la presente directiva de acuerdo a sus
competencias.
b) Informar a la DIRESA la aplicación de la presente directiva, de manera trimestral.
c) Informar a la DIRESA acerca del uso de los resultados de la matriz de cálculo, cada
vez que realicen contrataciones de personal para el primer nivel de atención.
d) Participar en la reuniones de monitoreo y evaluación de la presente directiva, las
mismas que serán convocadas por la DIRESA.
VIII. Disposiciones Finales.
Disponer que la DIRESA Ayacucho realice una primera evaluación a los tres meses de
haberse aplicado el cálculo de la dotación de RRHH en el primer nivel de atención y si el
caso amerite, proponer los ajustes que se considere necesarios.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 155
7.7 Survey to determine the available working time in the first-level-of-care
ENCUESTA
DISPONIBILIDAD DE TIEMPO EN EL PRIMER NIVEL DE ATENCION
La presente encuesta es anónima e individual, su información será muy útil para la dotación de
RRHH en la región. Por favor, completar toda la información solicitada con la mayor veracidad
posible.
SUS RESPUESTAS MÁRQUELAS CON UNA “X”, ó ESCRÍBALAS EN LOS ESPACIOS
SUBRAYADOS
SECCION N° 1: DATOS GENERALES DE ESTABLECIMIENTO DE SALUD
Localidad y Distrito:
Nombre del Establecimiento:
Categoría del Establecimiento:
Microrred a la que pertenece:
1. ¿Qué cargo desempeña?
( ) Médico ( ) Enfermera ( ) Obstetra
( ) Cirujano dentista ( ) Psicólogo ( ) Biólogo
( ) Nutricionista ( ) Tecnólogo Médico: Laboratorio ( ) Tecnólogo Médico: Radiología
( ) Tecnólogo Médico: Terapia Física ( ) Técnico Laboratorio ( ) Técnico Enfermería
( ) Otro: _______________________________________
2. ¿Cuál es su condición laboral?
( ) Nombrado ( ) Contratado ___________________________
Especifique modalidad
( ) SERUMS
N° de Encuesta:

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 156
3. ¿Cuántas horas al mes está usted contratado?
(Oficialmente el personal nombrado labora 150 horas al mes)
( ) 150 horas ( ) Otro ¿Cuántas horas? ______ ( ) No sabe
SECCION N° 2: AUSENCIAS PREVISTAS Y NO PREVISTAS
4. Cuántos días de vacaciones tiene usted en el año?
( ) 15 días ( ) 30 días ( ) Otro ______días ( ) No tiene vacaciones
5. Durante los meses comprendidos entre octubre del 2011 a marzo del 2012, ha participado
usted en capacitaciones dentro de los días laborables?
( ) Si ( ) No (Si la respuesta es “No” pase a la pregunta 6)
Nombre de la Capacitación
¿Cuántas horas duró
la capacitación?
¿Cuántas horas
empleó en viajar de
ida y regreso?
1.
2.
3.
4.
Sub total horas
Total horas
6. ¿Cuáles son las fiestas o celebraciones regionales y locales cuyos días no son laborables
en su establecimiento? (No considerar los feriados nacionales oficiales, semana santa,
fiestas patrias, fiestas navideñas, otros)
Nombre de la Celebración NO Laborable Nº de días
1. Fiesta patronal
2. Aniversario del Establecimiento

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 157
Nombre de la Celebración NO Laborable Nº de días
3. Otra:______________________________
4. Otra: _____________________________
5. Otra: _____________________________
Total días
6. Durante los meses comprendidos entre octubre del 2011 a marzo del 2012, ¿sufrió algún
imprevisto que lo obligó a ausentarse de su lugar de Establecimiento de Salud?
( ) Si ( ) No (Si la respuesta es “No” pase a la pregunta 8)
7. ¿Cuál fue el motivo de dicho imprevisto que lo obligó a ausentarse?
Motivo Nº de días
( ) Enfermedad
( ) Imprevisto personal o familiar
( ) Fallecimiento de un familiar
( ) Conflicto o huelga
( ) Otros motivos (por favor especifique):
________________________________________
SECCION N° 3: SALUD AMBIENTAL
8. Durante los meses comprendidos entre enero a marzo del 2012, ¿Usted ha realizado o
participado en actividades de salud ambiental, dentro del establecimiento?
( ) Si ( ) No (Si la respuesta es “No” pase a la pregunta 4)
9. Durante los meses comprendidos entre enero a marzo del 2012, ¿Cuántas salidas y
cuántas horas le ha dedicado a las actividades de salud ambiental?
Actividades Extramurales Nº de salidas
realizas
Nº de horas promedio
utilizado en cada salida
Total
horas
Charlas a la comunidad
Fumigaciones

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 158
Actividades Extramurales Nº de salidas
realizas
Nº de horas promedio
utilizado en cada salida
Total
horas
Control de la calidad del agua
Otras: __________________________
Otras: __________________________
Total horas
SECCION N° 4: LABOR ADMINISTRATIVA O DE GESTION
10. ¿Usted realiza actividades administrati
11. vas o de gestión o participa en actividades o reuniones de relacionadas con la
administración o gestión del establecimiento?
( ) Si ( ) No (Si la respuesta es “No” usted ha culminado la encuesta, muchas gracias)
12. ¿cuántas actividades administrativas o de gestión realiza aproximadamente en un mes?
Actividades de Gestión ó Administrativas
Nº de veces al
mes
Nº horas promedio
que utiliza en cada
actividad
Total
horas
Coordinaciones con actores locales
(autoridades, representantes, funcionarios de
otras instituciones)
Participación en la elaboración de planes
estratégicos, operativos, presupuesto, etc.
Trámites administrativos (cuadro de
necesidades, requerimientos, seguimiento a
trámites administrativo, etc.)
Elaboración de informes de: gestión,
capacitación, evaluaciones, supervisiones, etc.)
Codificación, llenado y registro de reportes e
información estadística
Actividades de monitoreo y/o evaluación del
establecimiento
Otra: ___________________________
Total horas
Muchas gracias!

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 159
7.8 Detailed table of "available working time" for health facilities
This table corresponds to health facilities type I-4
Grupo OcupacionalCondición
laboral
Hras totales
anuales
Días de
vacaciones al
año
# total de
horas de
vacaciones al
año
Hrs anuales
de
capacitación
N° total de
días de
celebraciones
N° total de
horas de
celebraciones
N° total de
días de
imprevistos
N° horas de
días de
imprevistos
N° total de
horas de
actividades
administrativ
as
TOTAL DE
HORAS NO
DISPONIBLES
TOTAL DE
HORAS
DISPONIBLES
PARA LA
PRESTACION
% de tiempo
disponible
para NO PEAS
Total de
horas
disponibles
para NO PEAS
Total de
horas
disponibles
para PEAS
% tiempo
disponible
PEAS
Médico Nombrado 1800 25 150 18 2 12 1 6 22 208 1,592 10% 159.2 1,433 80%
Contratado 1800 15 90 18 2 12 1 6 22 148 1,652 10% 165.2 1,487 83%
Enfermera Nombrado 1800 25 150 30 2 12 1 6 22 220 1,580 15% 237 1,343 75%
Contratado 1800 15 90 18 2 12 1 6 22 148 1,652 15% 247.8 1,404 78%
Odontólogo Nombrado 1800 25 150 12 2 12 1 6 22 202 1,598 1% 15.98 1,582 88%
Contratado 1800 15 90 12 2 12 1 6 22 142 1,658 1% 16.58 1,641 91%
Obstetra Nombrado 1800 25 150 18 2 12 1 6 22 208 1,592 5% 79.6 1,512 84%
Contratado 1800 15 90 12 2 12 1 6 22 142 1,658 5% 82.9 1,575 88%
Tecnólogo Médico Nombrado 1800 25 150 6 2 12 1 6 22 196 1,604 1% 16.04 1,588 88%
Radiología Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 1% 16.7 1,653 92%
Tecnólogo Médico Nombrado 1800 25 150 12 2 12 1 6 22 202 1,598 1% 15.98 1,582 88%
Laboratorio Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 1% 16.7 1,653 92%
Tecnólogo Médico Nombrado 1800 25 150 6 2 12 1 6 22 196 1,604 1% 16.04 1,588 88%
Rehabilitación Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 1% 16.7 1,653 92%
Psicólogo Nombrado 1800 25 150 12 2 12 1 6 22 202 1,598 20% 319.6 1,278 71%
Contratado 1800 15 90 12 2 12 1 6 22 142 1,658 20% 331.6 1,326 74%Biologo Nombrado 1800 25 150 6 2 12 1 6 22 196 1,604 20% 320.8 1,283 71%
Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 20% 334 1,336 74%
Nutricionista Nombrado 1800 25 150 12 2 12 1 6 22 202 1,598 5% 79.9 1,518 84%
Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 5% 83.5 1,587 88%
Trabajadora Social Nombrado 1800 25 150 6 2 12 1 6 22 196 1,604 80% 1283.2 321 18%
Contratado 1800 15 90 0 2 12 1 6 22 130 1,670 80% 1336 334 19%
Técnico Laborat. Nombrado 1800 25 150 12 2 12 1 6 22 202 1,598 1% 15.98 1,582 88%
Contratado 1800 15 90 12 2 12 1 6 22 142 1,658 1% 16.58 1,641 91%
Técnico Radiolog. Nombrado 1800 25 150 0 2 12 1 6 22 190 1,610 1% 16.1 1,594 89%
Contratado 1800 15 90 6 2 12 1 6 22 136 1,664 1% 16.64 1,647 92%
Fisioterapista Nombrado 1800 25 150 0 2 12 1 6 22 190 1,610 1% 16.1 1,594 89%
Contratado 1800 15 90 6 2 12 1 6 22 136 1,664 1% 16.64 1,647 92%
Técnico Enferm. Nombrado 1800 25 150 6 2 12 1 6 22 196 1,604 15% 240.6 1,363 76%
Contratado 1800 15 90 6 2 12 1 6 22 136 1,664 15% 249.6 1,414 79%

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 160
7.9 Available working time to provide PEAS in first-level-of-care health facilities
CategoríaSituación
laboral
Médico
Cirujano
Cirujano
DentistaEnfermera Psicólogo Obstetra
TM -
Radiología
TM -
Laboratorio
TM -
Terapia
física
Biólogo NutricionistaTrabajador
Social
Tco.
Radiología
Tco.
Laboratorio
Fisioterapis
ta
Servidor
Tco./Aux
Nombrado 1,453 1,610 1,362 1,301 1,533 1,610 1,610 1,610 1,301 1,545 325 1,616 1,043 1,616 896
Contratado 1,507 1,675 1,423 1,354 1,596 1,675 1,675 1,675 1,354 1,607 338 1,675 1,109 1,675 947
% hras PEAS
contratado 84% 93% 79% 75% 89% 93% 93% 93% 75% 89% 19% 93% 62% 93% 53%
Nombrado 1,453 1,327 1,119 1,072 1,262 1,327 1,327 1,327 1,072 1,273 268 1,180 1,174 1,616 1,382
Contratado 1,507 1,392 1,180 1,125 1,324 1,392 1,392 1,392 1,125 1,336 281 1,675 1,234 1,675 1,059
% hras PEAS
contratado 84% 77% 66% 62% 74% 77% 77% 77% 62% 74% 16% 93% 69% 93% 59%
Nombrado 1,433 1,451 1,231 1,173 1,387 1,457 1,457 1,457 1,178 1,398 294 1,180 1,168 1,180 1,008
Contratado 1,487 1,511 1,292 1,221 1,450 1,523 1,523 1,523 1,230 1,461 308 1,239 1,228 1,239 1,059
% hras PEAS
contratado 83% 84% 72% 68% 81% 85% 85% 85% 68% 81% 17% 69% 68% 69% 59%
Nombrado 1,433 1,582 1,343 1,278 1,512 1,588 1,582 1,588 1,283 1,518 321 1,594 1,582 1,594 1,363
Contratado 1486.8 1641.42 1404.2 1326.4 1575.1 1653.3 1653.3 1653.3 1336 1586.5 334 1647.36 1641.42 1647.36 1414.4
% hras PEAS
contratado 83% 91% 78% 74% 88% 92% 92% 92% 74% 88% 19% 92% 91% 92% 79%
I-1
I-2
I-3
I-4

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 161
7.10 Ministry of health: General competencies for the health sector
FORMULACION DE LAS COMPETENCIAS LABORALES GENERICAS DEL SECTOR SALUD25
La formulación e identificación de las competencias laborales genéricas tiene como
ejes orientadores al propósito clave del sector salud y los objetivos sectoriales (plan
concertado de salud), la que permite responder a cuáles son las competencias
laborales genéricas que todo trabajador del sector salud debe saber hacer para el
cumplimiento de las funciones encomendadas. A continuación se presenta a manera
de esquema el propósito clave, los objetivos del sector y las competencias genéricas
laborales del sector salud.
IDENTIFICACIÓN Y DEFINICIÓN DE LAS COMPETENCIAS GENÉRICAS LABORALES Para el logro del propósito clave y los objetivos del sector, todos los trabajadores del sector salud deberán tener las siguientes competencias genéricas laborales las que se complementaran con las competencias específicas.
25 Extraído de: “Competencias Laborales para la mejora del desempeño de los Recursos Humanos en
Salud”/Ministerio de Salud. Dirección General de Gestión del Desarrollo de Recursos Humanos en Salud. Dirección de Gestión del Trabajo en Salud – Lima: Ministerio de Salud; 2011.177 pág.; ilus.; tab. – (Serie Documentos Técnicos Normativos de Recursos Humanos en Salud; 2)

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 162
1. Compromiso ético
Los trabajadores del sector salud demuestran actitudes y acciones de servicio
responsable, sustentado en principios y valores de justicia, bien común, dignidad de la
persona y el derecho a la salud, en respuesta a las necesidades que la sociedad le
demanda.
Criterios de evaluación del desempeño
Trabaja por el bien común, con honestidad, confidencialidad.
Cumple su trabajo con oportunidad y calidad
2. Respeto por la vida, las personas y el ambiente
Los trabajadores de la salud practican la convivencia en armonía con todas las formas
de vida, con la construcción de una sociedad más humanizada, la defensa y
preservación de la biodiversidad.
Criterios de evaluación del desempeño
Participa defendiendo la importancia de la vida humana y otras formas de vida.
Es consciente de ser parte de una sociedad que requiere mejores condiciones
de salud propiciando la Participación social y el capital social.
3. Trabajo en equipo
Los trabajadores del sector salud cooperan y colaboran, integrándose en equipos
transdisciplinarios, para el logro de objetivos organizacionales y de la calidad de la
atención de los servicios de salud y comunidad.
Criterios de evaluación del desempeño
Participa con otros en la obtención de metas comunes, respetando diferentes
opiniones y evitando competir.
Apoya a los integrantes del equipo compartiendo principalmente información,
conocimiento y recursos.
4. Comunicación en base a interculturalidad
Los trabajadores del sector salud se comunican asertivamente entre ellos y con la
población, mediante mensajes que incorporan patrones culturales, lingüísticos y
sociales, propiciando la inclusión social e identidad con los servicios de salud.
Criterios de evaluación del desempeño
Escucha y expresa sus mensajes (información, ideas, opiniones) con
cordialidad y pertinencia.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 163
Genera y mantiene un flujo de comunicación incorporando patrones culturales,
lingüísticos y sociales
5. Capacidad de organización y planificación
Los trabajadores del sector salud organizan sus metas, objetivos, recursos, funciones,
actividades y tareas, para lograr resultados de mejora de la salud y transformación
social, en el marco de lineamientos y políticas de salud.
Criterios de evaluación del desempeño
Identifica, organiza sus metas, objetivos, funciones, actividades, tareas y
recursos a través de un plan.
Trabaja planificadamente para el logro de resultados estratégicos, en un
horizonte de tiempo sostenido, construyendo situaciones futuras.
7.11 CONEAU: Managerial competencies for health professionals
MAPA FUNCIONAL DE LAS COMPETENCIAS DEL PROFESIONAL EN SALUD EN
GESTION
FUNCION CLAVE UNIDAD DE
COMPETENCIA ELEMENTO DE COMPETENCIA
Gestionar las
organizaciones
sanitarias y las
entidades formadoras
de profesionales en
salud, en el ámbito de
competencia
profesional y según
normatividad vigente.
1. Planificar las actividades
de una organización
sanitaria y entidades
formadoras, según
normatividad vigente.
Elaborar el análisis situacional del ámbito de acción de una
organización sanitaria ó entidad formadora.
Elaborar el plan estratégico, plan operativo y otros
documentos de gestión de una organización sanitaria ó
entidad formadora.
Determinar las necesidades de recursos humanos,
materiales y financieros de una organización sanitaria ó
entidad formadora, de acuerdo a lo planificado.
2. Organizar el
funcionamiento de una
organización sanitaria y
entidades formadoras,
según normas vigentes
Aprobar los procesos de gestión sanitaria o académica a su
cargo, según norma vigente.
Elaborar los flujogramas de los procesos de gestión sanitaria
o académica.
Determinar la necesidad y funciones del personal a su cargo
según normatividad vigente.
Aprobar los programas de adquisición y mantenimiento de
equipos e insumos.
3. Dirigir el funcionamiento
de de una organización
sanitaria y entidades
formadoras, según
Liderar el equipo de gestión aplicando principios y valores
éticos.
Utilizar herramientas de gestión pertinentes para la oportuna

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 164
FUNCION CLAVE UNIDAD DE
COMPETENCIA ELEMENTO DE COMPETENCIA
normas vigentes toma de decisiones.
Implementar planes y procesos de mejora continua de la
calidad.
4. Controlar los servicios de
de una organización
sanitaria y entidades
formadoras, según
normatividad vigente.
Monitorear el cumplimiento de procesos y metas establecidas
en el plan operativo y otros documentos de gestión.
Supervisar el desempeño del talento humano a su cargo.
Evaluar los resultados de plan estratégico y plan operativo,
aplicando medidas preventivas y acciones correctivas.
Fuente: CONEAU
7.12 Human resources management competencies
COMPETENCIAS PARA LA GESTION DE RECURSOS HUMANOS
PROPOSITO PRINCIPAL DE LOS GESTORES DE RECURSOS HUMANOS: Contar con
personal competente, motivado, distribuido en lugares adecuados, haciendo bien lo que tiene
que hacer, en base a las necesidades de salud de la Región Ayacucho.
FUNCIONES CLAVES COMPETENCIAS
PLANIFICACIÓN
Definir los
requerimientos de
recursos humanos y la
dotación adecuada de
recursos humanos
Diseñar directivas, formatos, matrices para el acopio de información de RH
Controlar la implementación y cumplimiento de la normatividad del acopio de la
información regional de RH
Mantener actualizada la base de datos del inventario regional del personal de salud
Estimar las necesidades de RHUS para todos los niveles de atención de acuerdo a las
prioridades sanitarias regionales y locales
Estimar la brecha de recursos humanos de acuerdo a las políticas institucionales
vigentes
Elaborar el diagnóstico de RHUS tomando en cuenta las necesidades tanto de la
formación como de la prestación
Diseñar planes y estrategias para cubrir la brecha de RHUS
ORGANIZACION DEL
TRABAJO
Describir y clasificar
los puestos de trabajo;
define los requisitos y
competencias para
ocuparlos, así como
registra la distribución
del personal en la
organización.
Elaborar los perfiles de puesto de acuerdo a los objetivos institucionales
Elaborar el Cuadro de Asignación de Personal de acuerdo a las necesidades
organizacionales vigentes
Elaborar directivas y normas acerca de perfiles de competencias de acuerdo al marco
normativo vigente
Diseñar los perfiles de competencias de acuerdo a las directivas vigentes
Brindar asistencia técnica para el diseño de los perfiles de competencias de acuerdo a
las necesidades organizacionales
Diseñar los estándares de desempeño laboral de acuerdo a las competencias definidas
GESTIÓN DEL
EMPLEO
Implementar políticas y
prácticas de RRHH
vinculadas al ingreso,
movimiento y salida del
personal.
Desarrollar estudios de mercado de la Oferta y Demanda laboral
Diseñar procesos de reclutamiento de personal de acuerdo a las necesidades
institucionales
Elaborar las bases del proceso de reclutamiento y selección del personal
Evaluar los expedientes de candidatos para verificar requisitos de acuerdo al perfil
Diseñar instrumentos para evaluar candidatos de acuerdo a los perfiles de puesto y
competencias definidos.
Elaborar el documento del contrato en base al informe de resultados de la selección
Realizar la inducción a los nuevos trabajadores de acuerdo a los procedimientos

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 165
FUNCIONES CLAVES COMPETENCIAS
establecidos
Formular políticas y procedimientos que regulan los procesos de desplazamiento
horizontal y vertical del personal, de acuerdo al desempeño del personal, a los años de
permanencia en el puesto, a la progresión desde zonas de menor a mayor desarrollo.
Evaluar y emitir opinión de las solicitudes de desplazamiento en función a las
necesidades
Elaborar el reglamento interno de trabajo
Evaluar expedientes de procesos administrativos de acuerdo a la normatividad vigente.
Realizar el control de asistencia y permanencia de acuerdo a la normatividad vigente
Mantener el legajo del personal actualizado hasta el último año.
Diseñar directivas de desvinculación del personal de acuerdo a la normatividad vigente
Evaluar expedientes para la desvinculación laboral en base a la normatividad vigente
GESTIÓN DEL
DESEMPEÑO
Mejorar el desempeño
del personal y alinearlo
a los valores y
estrategias de la
organización.
Establecer metas de rendimiento conforme a criterios técnicos, de manera concertada y
de acuerdo con las necesidades institucionales
Diseñar procedimientos de evaluación de competencias de acuerdo a la evidencia
nacional o internacional exitosas
Elaborar instrumentos de evaluación de competencias de acuerdo a la normatividad
vigente o evidencia internacional y nacional exitosa
Elaborar el plan de supervisión del desempeño de acuerdo a las brechas de competencia
identificadas
Diseñar los instrumentos de supervisión en función a los objetivos y estándares de
desempeño.
Supervisar el desempeño en el marco de los estándares diseñados para el puesto laboral
Elaborar el informe final de la supervisión conforme a las brechas identificadas
Realizar actividades de reflexión de la práctica diaria para la mejora del desempeño en el
servicio
Elaborar reportes de monitoreo de rendimiento y desempeño del personal de salud de
acuerdo a cumplimiento del Plan de Desempeño
Seleccionar evaluadores del desempeño de acuerdo a los estándares vigentes
Evaluar las metas de rendimiento de acuerdo a los procedimientos establecidos
Certificar a los trabajadores en base a las competencias adquiridas y demostradas
Administrar el portafolio individual de evidencias de acuerdo a las evaluaciones y
certificaciones
Implementar de manera concertada planes individuales de mejora del rendimiento en
función a las brechas encontradas
Elaborar planes de mejora del desempeño en base a los planes de mejora del
rendimiento laboral
GESTION DE LA
COMPENSACION
Definir políticas y
prácticas retributivas,
monetarias y no
monetarias, y el
ordenamiento de las
remuneraciones,
prestaciones e
incentivos por
rendimiento.
Definir una escala salarial equitativa y justa de acuerdo a las políticas institucionales
vigentes
Controlar el cumplimiento de la aplicación de la escala salarial en todos los niveles
Organizar la información de la planilla de pagos, remuneraciones y pensiones según
niveles y grupos profesionales (administrativos y asistenciales)
Definir beneficios extrasalariales y salariales por trabajo extrahorario de acuerdo a la
normatividad vigente
Diseñar políticas de incentivos monetarias y no monetarias para retener al personal
competente de acuerdo a la evaluación del desempeño
Diseñar documentos de reconocimiento al personal de acuerdo a la normatividad vigente
GESTION DEL
DESARROLLO
Definir políticas y
prácticas orientadas a
favorecer el desarrollo
profesional y laboral de
Diseñar políticas para el cambio de grupo ocupacional y ascensos, de acuerdo a
competencias y mérito
Diseñar líneas de carrera en base al mérito, tiempo de permanencia y competencias para
el cargo
Elaborar directivas para la implementación de las líneas de carrera para todos los grupos
ocupacionales, en todos los niveles institucionales (incluye definiciones de cargos)

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 166
FUNCIONES CLAVES COMPETENCIAS
las personas de
acuerdo a sus
aptitudes,
proporcionando
espacios de
aprendizaje y líneas de
carrera de acuerdo a la
dinámica y estructura
organizativa.
Elaborar el diagnóstico de identificación de brechas de competencias y necesidades de
capacitación de acuerdo a las prioridades institucionales
Elaborar el plan de desarrollo de capacidades en base al diagnóstico de brechas de
competencias y necesidades de desarrollo
Elaborar programas de capacitación de acuerdo a la normatividad vigente
Diseñar estrategias comunicacionales para la socialización de las directivas sobre
intervenciones educativas
Elaborar el informe de evaluación de los programas y planes de desarrollo de
competencias de acuerdo a normatividad vigente
Evaluar los procesos de gestión de la capacitación de acuerdo a la normatividad vigente
Diseñar planes de desarrollo de sedes docentes de acuerdo al Plan de Desarrollo de
Capacidades
Calificar las sedes docentes de acuerdo a las normas vigentes
Elaborar el informe de acreditación de la sede docente calificada de acuerdo a la norma
vigente
Elaborar convenios marco y específicos con instituciones de formación conforme al
marco normativo y legal vigente
Diseñar normas para la regulación de los programas de docencia-servicio (pregrado,
internado, SERUMS/SECIGRA y segunda especialización en concordancia con las
políticas institucionales
Gerenciar los programas de docencia-servicio (pregrado, internado, SERUMS/SECIGRA
y segunda especialización en concordancia con las políticas institucionales
GESTIÓN DE
RELACIONES
HUMANAS
Regular y armonizar
las interacciones entre
los individuos, con
énfasis en su
dimensión colectiva, y
la organización, en
base a políticas y
prácticas vinculadas al
clima laboral, las
relaciones laborales y
el bienestar.
Diseñar políticas de desarrollo organizacional de acuerdo a las necesidades
institucionales
Elaborar diagnósticos del clima organizacional de acuerdo a la normatividad vigente
Elaborar planes de mejora del clima organizacional de acuerdo al diagnóstico
Gestionar la implementación de las acciones de mejora del clima laboral conforme al plan
Investigar los conflictos laborales de acuerdo a las necesidades de La organización
Formular estrategias para la resolución de conflictos laborales de acuerdo a las
necesidades de la organización, el trabajador y los usuarios
Definir los canales de comunicación y negociación entre los directivos y trabajadores de
acuerdo a la política institucional
Gestionar la implementación de las estrategias de resolución de conflicto conforme a la
políticas institucional
Diseñar programas de bienestar social de acuerdo a la normatividad vigente
Diseñar políticas, directivas y planes para la gestión de la seguridad en el trabajo (incluye
control y vigilancia) conforme a la normatividad vigente
GESTION DEL
SISTEMA
Alimentar y
retroalimentar a los
demás subsistemas.
Alinear los
subsistemas a la
misión, objetivos y
estrategias de la
organización
Diseñar indicadores de gestión de RHUS de acuerdo a las necesidades institucionales
Monitorear los indicadores de gestión de RHUS de acuerdo a los planes y políticas de
gestión institucional
Diseñar el plan estratégico para la gestión y desarrollo de recursos humanos, en el marco
de las políticas sectoriales y la legislación vigente.
Diseñar políticas de gestión del desarrollo de los RHUS (institucionales y sectoriales) de
acuerdo a las necesidades institucionales y sectoriales
Diseñar el plan operativo de la unidad de recursos humanos de acuerdo con los planes
estratégicos vigentes
Diseñar el presupuesto de la unidad de recursos humanos de acuerdo con los planes
operativos vigentes
Diseñar el modelo de gestión de recursos humanos por competencias apropiados a la
organización institucional
Gerenciar los procesos de la elaboración, administración y uso de la información de
recursos humanos institucionales (y sectoriales) de acuerdo al marco normativo y
necesidades institucionales
Elaborar el Presupuesto Analítico de Personal de acuerdo a la normatividad vigente

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 167
FUNCIONES CLAVES COMPETENCIAS
Elaborar reportes financieros y presupuestales de Personal conforme a criterios técnicos,
administrativos y gerenciales
Elaborar propuestas y recomendaciones al planeamiento y presupuesto institucional de
acuerdo a las conclusiones del análisis
Diseñar ROF, MOF CAP y PAP en base a la normatividad vigente
Elaborar los documentos de gestión de la unidad de RRHH de la organización
7.13 Transversal managerial competencies
En este anexo se presenta la revisión bibliográfica realizada acerca de competencias
gerenciales, especialmente para el sector salud:
Modelos de competencias gerenciales
A continuación se presenta los diferentes modelos de competencias encontrados en la
bibliografía.
Si bien, tenemos el enunciado de la competencia, es necesario establecer una
definición operacional de las mismas para facilitar su mejor comprensión y por
consiguiente su evaluación.
Competencias directivas (Hooghiemstra, 1992)
a) Razonamiento estratégico
b) Liderazgo para el cambio
c) Gestión de las relaciones
Competencias gerenciales (Bethell-Fox 1992)
a) Desarrollo de personas
b) Dirección de personas
c) Trabajo en equipo y cooperación
d) Liderazgo interna
Competencias gerenciales genéricas (Richard Boyayzis, 1982)
a) Competencias de logro de metas y objetivos
Orientación eficiente
Proactividad
Diagnosticar a través de conceptos
Crear impacto
b) Competencias de liderazgo
Confianza en sí mismo
Manejo adecuado de la comunicación oral
Pensamiento lógico
Conceptualización
c) Competencias de recursos humanos
Uso de poder de socialización
Actitud positiva
Manejo de grupos
Autovaloración de certeza

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 168
d) Competencias de dirigir subordinados
Desarrollo de otros
Uso de poder unilateral
Espontaneidad
e) Competencias de madurez
Control en sí mismo
Percepción objetiva
Resistencia y adaptabilidad
Construcción de una filiación
Competencias gerenciales genéricas (Lyle Spencer y Signe Spencer, 1993)
a) Orientación a logros o resultados: Orden y precisión, Iniciativa, Búsqueda de
Información y Pensamiento Analítico o Conceptualización
b) Ayuda y servicio a personas: Capacidad para relaciones interpersonales,
Orientación al usuario.
c) Impacto e influencia: Conciencia organizacional, Construcción de relaciones.
d) Dirección: Desarrollo de otros; Decisión, asertividad y uso adecuado de poder.
e) Cognición: Pensamiento analítico, pensamiento conceptual.
f) Madurez personal: Control de sí mismo, confianza en sí mismo, flexibilidad,
compromiso organizacional.
Competencias directivas (modelo inglés)
a) Dar propósito y dirección
b) Producir impacto personal
c) Pensar estratégicamente
d) Conseguir lo mejor de las personas
e) Aprender a mejorar
f) Centrarse en el servicio
Competencias directivas (modelo canadiense)
a) Intelectual (capacidad cognitiva, creatividad)
b) Construcción de futuro (visión)
c) Gestión (gestión para la acción, comprensión organizacional, trabajo en equipo,
asociación)
d) Relacional (relaciones interpersonales, comunicación)
e) Personal (la vitalidad y resistencia al stress; ética y valores; personalidad;
flexibilidad; autoconfianza; conocimiento de sistemas, políticas y programas de
gobierno).
Competencias directivas fundamentales (modelo brasilero)
a) Compromiso con los resultados (de la organización bajo su autoridad y del
gobierno en su conjunto), con el impacto de las acciones y el uso responsable
de los recursos públicos
b) Ayuda a definir claramente la misión de la institución que dirige, sus estrategias
y prioridades, y estar preparado para ejercer una supervisión permanente de
las acciones hacia la misión, estrategias y prioridades definidas.
c) Liderar con el ejemplo y conducir el cambio en la organización pública para
alcanzar mayores niveles de desempeño institucional: dar el foco y dirección a

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 169
los cambios organizativos y el ejercicio constante de comunicación con todos
los participantes
d) Practicar, promover y recoger el alto desempeño de todos los empleados
e) Desarrollar el interés real por los recursos humanos, finanzas y tecnología
f) Ayudar a preparar la transición de gobierno.
Competencias Gerenciales en Salud (American College of Health care Executives, 2010)
a) Comunicación y Gestión de las Relaciones
Gestión de las relaciones
Destrezas de comunicación
Facilitación y negociación
b) Liderazgo
Destrezas de liderazgo
Cultura y Clima organizacional
Comunicación de la visión
Gestión del cambio
c) Profesionalismo
Rendición de cuentas personal y profesional
Desarrollo profesional y aprendizaje para la vida
Contribución a la comunidad y la profesión
d) Conocimiento del sistema de salud
Sistemas y Organizaciones de salud
Personal de salud
Perspectiva del paciente
Comunidad y medio ambiente
e) Destrezas y conocimientos gerenciales
Gestión General
Gerencia financiera
Gestión de RRHH
Dinámica organizacional y gobernanza
Planeamiento estratégico y marketing
Gestión de la información
Gestión del riesgo
Mejoramiento de la calidad.
Competencias nucleares26 en salud pública (Center for health policy, Columbia
University)
a) Dimensiones comunitarias
b) Planeamiento y gestión financiera
c) Pensamiento sistémico y liderazgo
d) Desarrollo de políticas / planeamiento de programas
e) Evaluación analítica
f) Ciencias básicas de salud pública
26 Nucleares o Core: Representan un set de destrezas, conocimientos y actitudes necesarias para la
práctica de la salud pública aplicada por personal de primera línea; personal de alto nivel; y gerentes y
supervisores Las competencias se han definido en términos generales para que puedan aplicarse
ampliamente a todos los programas, muestra aquellas competencias que son comunes a todos los
residentes de medicina preventiva (American College of Preventive Medicine)

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 170
g) Competencias culturales
h) Comunicación
Competencias gerenciales transversales
En base a la revisión bibliográfica realizada, se definieron las competencias que eran
comunes a los modelos analizados, definiéndose 14 competencias gerenciales que
sirvieron de referencia para que los equipos de gestión de las redes de salud de la
DIRES San Martín identificaran sus competencias gerenciales transversales.
Listado de las 14 competencias gerenciales transversales
1. Lead, mobilize and inspire teams
2. Communicate messages verbally or in writing
3. Help others to solve problems
4. Maintain good interpersonal relationships
5. Develop the potential of others
6. Build a vision
7. Lead people to achieve results, goals and objectives
8. Locate, attract and retain the right people in the right job
9. Use resources responsibly
10. Manage finances efficiently
11. Negotiate
12. Maintain a satisfactory organizational climate
13. Manage change
14. Implement plans, policies and programs in health.

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 171
CUADRO COMPARATIVO DE LOS DIFERENTES MODELOS DE COMPETENCIAS GERENCIALES
Competencias Gerenciales
Genéricas Hooghiemstra
Bethell-
Fox Boyaysis Spencer
Modelo
inglés
Modelo
canadiense
Modelo
brasilero
Modelo
español
para la
gestión
local
ACHCE CHP Total
Liderazgo 1 1 1 1 1 1 1 7
Comunicación / Ayuda y servicio
a otros: Relaciones
interpersonales, orientación al
usuario 1 1 1 1 1 1 6
Dirigir subordinados; Desarrollo
de personas, uso de poder. 1 1 1 2 1 6
Impacto e influencia: Gestión de
relaciones, conciencia
organizacional 1 1 1 1 1 1 6
Competencias de madurez /otras
competencias: Control en sí
mismo, percepción objetiva,
resistencia y adaptabilidad,
construcción de filiación.
Confianza en sí mismo,
compromiso organizacional.
Aprender a mejorar. Ética y
valores, personalidad. 1 1 1 1 1 5
Pensamiento estratégico,
Construcción de futuro (visión) 1 1 1 1 1 5
Orientación al logro de
resultados, metas y objetivos 1 1 1 3
Dirección de personas, recursos
humanos 1 1 1 3
Trabajo en equipo y cooperación 1 1 1 3
Cognición: Pensamiento
analítico, pensamiento
conceptual / Evaluación analítica 1 1 1 3

Policies, regulations and programmatic actions regarding human resources for health GHS-I-10-07-00003-00
Abt Associates Inc. Annex ▌pg. 172
Competencias Gerenciales
Genéricas Hooghiemstra
Bethell-
Fox Boyaysis Spencer
Modelo
inglés
Modelo
canadiense
Modelo
brasilero
Modelo
español
para la
gestión
local
ACHCE CHP Total
Gestión para la acción /
Destrezas gerenciales 1 1 2
Conocimiento de sistemas,
políticas y programas de gobierno
/ Pensamiento sistémico 1 1 2
Uso responsable de recursos
/Gestión financiera 1 1 2
Iniciativa 1 1
Comprensión del entorno político 1 1
Ayudar a preparar la transición de
gobierno 1 1
Facilitación y negociación 1 1
Cultura y Clima organizacional 1 1
Gestión del cambio 1 1
Profesionalismo 1 1
Conocimiento del sistema de
salud 1 1
Dimensiones comunitarias /
competencias culturales 1 1
Desarrollo de políticas /
planeamiento de programas 1 1
Ciencias básicas de salud
pública 1 1
TOTAL 3 4 5 6 6 8 7 7 9 9
ACHE: American College of Health Care Executives
CHP: Center for Health Policy, Columbia University