reply
TRANSCRIPT
1564 CORRESPONDENCE
A
B
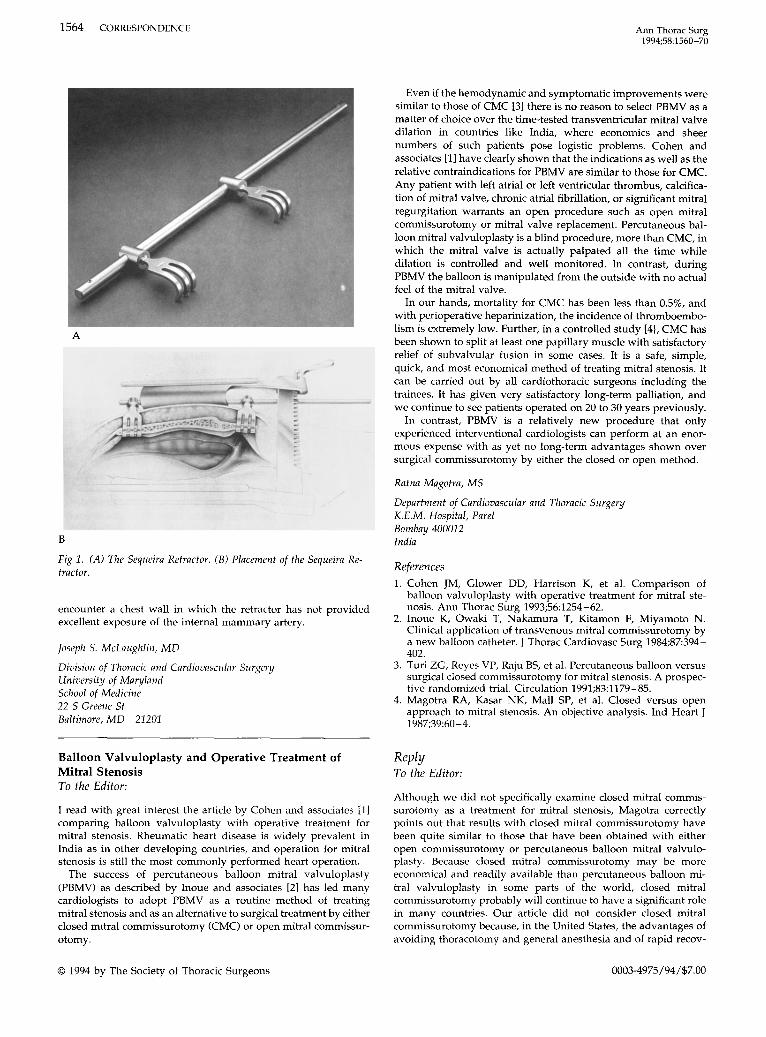
Fig 1. (A) The Sequeira Retractor. (B) Placement of the Sequeira Retractor.
encounter a chest wall in which the retractor has not providedexcellent exposure of the internal mammary artery.
Joseph S. McLaughlin, MD
Division of Thoracic and Cardiovascular SurgeryUniversity of MarylandSchool of Medicine22 S Greene StBaltimore,MD 21201
Balloon Valvuloplasty and Operative Treatment ofMitral StenosisTo the Editor:
I read with great interest the article by Cohen and associates [1]comparing balloon valvuloplasty with operative treatment formitral stenosis. Rheumatic heart disease is widely prevalent inIndia as in other developing countries, and operation for mitralstenosis is still the most commonly performed heart operation.
The success of percutaneous balloon mitral valvuloplasty(PBMV) as described by Inoue and associates [2] has led manycardiologists to adopt PBMV as a routine method of treatingmitral stenosis and as an alternative to surgical treatment by eitherclosed mitral commissurotomy (CMC) or open mitral commissurotomy.
© 1994 by The Society of Thoracic Surgeons
Ann Thorae Surg1994;58:1560-70
Even if the hemodynamic and symptomatic improvements weresimilar to those of CMC [3] there is no reason to select PBMV as amatter of choice over the time-tested transventricular mitral valvedilation in countries like India, where economics and sheernumbers of such patients pose logistic problems. Cohen andassociates [1] have clearly shown that the indications as well as therelative contraindications for PBMV are similar to those for CMC.Any patient with left atrial or left ventricular thrombus, calcification of mitral valve, chronic atrial fibrillation, or significant mitralregurgitation warrants an open procedure such as open mitralcommissurotomy or mitral valve replacement. Percutaneous balloon mitral valvuloplasty is a blind procedure, more than CMC, inwhich the mitral valve is actually palpated all the time whiledilation is controlled and well monitored. In contrast, duringPBMV the balloon is manipulated from the outside with no actualfeel of the mitral valve.
In our hands, mortality for CMC has been less than 0.5%, andwith perioperative heparinization, the incidence of thromboembolism is extremely low. Further, in a controlled study [4), CMC hasbeen shown to split at least one papillary muscle with satisfactoryrelief of subvalvular fusion in some cases. It is a safe, simple,quick, and most economical method of treating mitral stenosis. Itcan be carried out by all cardiothoracic surgeons including thetrainees. It has given very satisfactory long-term palliation, andwe continue to see patients operated on 20 to 30 years previously.
In contrast, PBMV is a relatively new procedure that onlyexperienced interventional cardiologists can perform at an enormous expense with as yet no long-term advantages shown oversurgical commissurotomy by either the closed or open method.
Ratna Magotra, MS
Department of Cardiovascular and Thoracic SurgeryK.E.M. Hospital, ParelBombay 400012India
References1. Cohen JM, Glower DD, Harrison K, et al. Comparison of
balloon valvuloplasty with operative treatment for mitral stenosis. Ann Thorac Surg 1993;56:1254-62.
2. Inoue K, Owaki T, Nakamura T, Kitamon F, Miyamoto N.Clinical application of transvenous mitral commissurotomy bya new balloon catheter. J Thorac Cardiovasc Surg 1984;87:394402.
3. Turi ZG, Reyes VP, Raju BS, et al. Percutaneous balloon versussurgical closed commissurotomy for mitral stenosis. A prospective randomized trial. Circulation 1991;83:1179-85.
4. Magotra RA, Kasar NK, Mall SP, et al. Closed versus openapproach to mitral stenosis. An objective analysis. Ind Heart J1987;39:60-4.
ReplyTo the Editor:
Although we did not specifically examine closed mitral commissurotomy as a treatment for mitral stenosis, Magotra correctlypoints out that results with closed mitral commissurotomy havebeen quite similar to those that have been obtained with eitheropen commissurotomy or percutaneous balloon mitral valvuloplasty. Because closed mitral commissurotomy may be moreeconomical and readily available than percutaneous balloon mitral valvuloplasty in some parts of the world, closed mitralcommissurotomy probably will continue to have a significant rolein many countries. Our article did not consider closed mitralcommissurotomy because, in the United States, the advantages ofavoiding thoracotomy and general anesthesia and of rapid recov-
0003-4975/94/$7.00

Ann ThoraeSurg1994;58:1560-70
CORRESPONDENCE 1565
ery have made percutaneous balloon mitral valvuloplasty a lessmorbid procedure and at least as economical as closed mitralcommissurotomy.
Donald D. Glower, MDJ. Kevin Harrison, MDThomas M. Bashore, MD
Department of SurgeryDuke University Medical CenterBox 3851Durham, NC 27710
Congenital Factor XII Deficiency and CardiopulmonaryBypassTo the Editor:
Congenital factor XII deficiency usually does not lead to clinicallyimportant bleeding problems. However, in patients needing heparinization for cardiopulmonary bypass, factor XII deficiencyleads to a problem in not being able to measure adequateanticoagulation levels to proceed with safe cardiopulmonarybypass. Patients with factor XII deficiency have a markedlyelevated baseline activated clotting time (ACT) and activatedpartial thromboplastin time. I overcame this difficulty by administering fresh frozen plasma just before operation and documentedthat the customarily measured parameters of adequate anticoagulation returned to normal and that they became elevated withappropriate doses of heparin.
A 76-year-old, 64.5-kg woman had a 2V2-month history ofexertional dyspnea and fatigue accompanied by a large abdominalaortic aneurysm. Cardiac catheterization showed an occludedright coronary artery, occluded circumflex artery, and an 85%stenotic left anterior descending coronary artery with an oldlateral wall infarction and ejection fraction of 0.50. Hematologicevaluation showed a baseline activated partial thromboplastintime of 171 seconds, ACT of 484 seconds, and factor XII level ofless than 1%. Other hematologic parameters were normal including no bleeding diathesis with two prior operations. Because freshfrozen plasma contains factor XII, two units of fresh frozen plasmaresulted in the activated partial thromboplastin time dropping to24 seconds (normal) and the ACT dropping to 176 seconds. Fourunits of fresh frozen plasma resulted in the ACT dropping to 128seconds (normal). Four milligrams per kilogram of heparin wasgiven before cardiopulmonary bypass and resulted in an ACT of592 seconds. I, therefore, believed that I had an acceptable way ofmeasuring adequate surgical anticoagulation to carry out safecardiopulmonary bypass. The patient had an internal thoracicartery graft and two vein grafts performed and was dischargedhome on postoperative day 5 to recuperate before her abdominalaortic aneurysmectomy.
A review of the literature revealed four prior reported cases ofpatients having cardiopulmonary bypass for coronary artery bypass grafting in conjunction with a factor XII deficiency. Candioand Prager [1] reported a case in which "a bolus injection ofheparin was given" and no apparent measurement of anticoagulation levels was reported. Kelsey and associates [2] described apatient who was given 4 mg/kg of heparin and a successfulcardiopulmonary bypass run ensued with no mention of measuring anticoagulation. Salmenpera and colleagues [3] gave 300 Uheparin per kilogram and stated that "in the absence of a clinicallyfeasible method to assess surgical anticoagulation rapidly in thesepatients, heparin must be given according to weight based protocols, and a normal dose response relationship must be assumed."Moorman and co-workers [4] treated a patient who had receivedheparin for 13 days preoperatively with 500 USP units of heparin
© 1994 by The Society of Thoracic Surgeons
per kilogram before undergoing coronary artery bypass graftingand noted that signs of ischemia developed 20 minutes afterprotamine administration, with postoperative angiography demonstrating all grafts being occluded. The grafts were successfullyopened with urokinase but with a significant perioperative myocardial infarction.
By administering fresh frozen plasma just before cardiopulmonary bypass, I believe that it now is possible to document thatappropriate surgical anticoagulation was obtained rather thanhaving to assume that it was present.
Michael K. Wood, MD
Department of Cardiothoracic SurgeryMercy Hospital, Mercy Clinic West1000 Mineral Point AvePO Box 5003Janesville, WI 53547-5003
References1. Candio J, Prager D. Cardiopulmonary bypass and factor XII
deficiency. Penn Med 1981;84:40.2. Kelsey PR, Bottomley J, Grotte GJ, Maciver JE. Congenital factor
XII deficiency: successful open heart surgery and anticoagulation. Clin Lab Haemat 1985;7:379-81.
3. Salmenpera M, Rasi V, Mattila S. Cardiopulmonary bypass in apatient with factor XII deficiency. Anesthesiology 1991;75:539-41.
4. Moorman RM, Reynolds DS, Comunale ME. Management ofcardiopulmonary bypass in a patient with congenital factor XIIdeficiency. J Cardiothorac Vase Anesth 1993;7:452-4.
The Ross Procedure: To Do or Not to DoTo the Editor:
I recently attended a course, sponsored by one of the medicaldevice manufacturers, that was intended to focus on valve replacement and valvuloplasty. The course was divided into amorning didactic session and an afternoon laboratory session. Inthe didactic session the Ross procedure (replacement of the aorticvalve with the patient's own pulmonary valve and reconstructionof the pulmonary valve with an aortic allograft) was discussed inaddition to the other announced topics. The laboratory sessionwas introduced as a session in which the participants first wouldbe taken through a mitral valvuloplasty on a porcine heartfollowed by a Ross procedure.
All the participants were taken, step by step, through the Rossprocedure. Because I have never personally performed this procedure, it was indeed an enjoyable experience, similar to a "wannabe" jet pilot in a flight simulator. Comments from some of theparticipants reflected an eagerness to perform this procedureclinically now that it has been accomplished in the animal laboratory.
In my opinion, the Ross procedure is not a procedure that theentire legion of cardiothoracic surgeons should be presentlyplacing on their operating schedules. The Ross procedure is acomplex procedure requiring considerable expertise. The procedure is still in an evaluation stage and should be considered assuch at this time.
There are alternative strategies, perhaps not as theoretically desirable as the Ross procedure, that are well established with acceptableand proven results. The majority of cardiothoracic surgeons todaycan, without unduly jeopardizing the patient, accomplish a tissuevalve replacement (porcine, pericardial, or homograft) and safelyreplace that valve if it were to fail at any future time with a lessermorbidity and mortality than having to go through a painful learningcurve of the Ross procedure.
As surgeons we are always looking for new and innovativeprocedures to challenge our surgical abilities. We should not
0003-4975/94/$7.00