relationship between expression of the kai1 metastasis suppressor and other markers of advanced...
TRANSCRIPT

Original Paper
Relationship between expression of the KAI1 metastasissuppressor and other markers of advanced bladdercancer
Kim Ow1, Warick Delprado2, Richard Fisher3, Julie Barrett1, Yan Yu4, Paul Jackson1 and Pamela J. Russell1*1 The Oncology Research Centre, Prince of Wales Hospital, Randwick, Sydney and Department of Medicine, University of New South Wales,Kensington, Australia
2 Douglass Hanly Moir Pathology, Sydney, Australia3 Department of Radiation Oncology, Prince of Wales Hospital, Randwick, Sydney, Australia4 Department of Surgery, Prince of Wales Hospital, Randwick, Sydney, Australia
*Correspondence to:Professor Pamela J. Russell,Oncology Research Centre,Level 2, Parkes Building,Prince of Wales Hospital,Barker Street, Randwick,NSW 2031, Australia.E-mail: [email protected]
Received: 31 March 1999
Revised: 13 October 1999
Accepted: 9 November 1999
Abstract
Expression of a newly described inhibitor of tumour metastasis, KAI1, was examined in bladder
cancer progression and compared with the expression of p53 and pRb, which are markers of
advanced disease. KAI1 mRNA (by in situ hybridization) and protein levels (by immunohisto-
chemistry) were examined in 135 paraf®n-embedded bladder tissue sections. Signi®cant decreases
in KAI1 mRNA and protein levels were detected between normal and tumour tissue ( p<0.001 and
p=0.026, respectively), and between non-invasive and invasive tumours ( p=0.046 and p<0.001,
respectively). Loss of KAI1 protein expression was accompanied by a shift in staining pattern
from a uniform distribution to a weaker, membranous or heterogeneous pattern. Normal tissue
and low-grade tumours showed little p53 protein staining. High level staining (indicative of mutant
p53) was associated with increased grade in non-invasive tumours (p=0.031) but was not
signi®cantly higher in invasive tumours. Whilst p53 protein staining increased with malignant
progression and KAI1 mRNA expression decreased, there was no signi®cant correlation between
the two patterns ( p=0.33, adjusted for group, p=0.18) or when only cancer samples were
analysed ( p=0.065, adjusted for group, p=0.26), even when taking into account overexpression
of MDM-2 protein as a pathway for inactivation of p53. There was no correlation between loss of
KAI1 mRNA expression and gain of abnormal pRb staining ( p=0.30, or adjusted for tumour
samples only, p=0.59). These results suggest that loss of KAI1 expression is associated with
invasive bladder cancer, but is not related to mutation of p53 or to loss of normal pRb expression.
Copyright # 2000 John Wiley & Sons, Ltd.
Keywords: KAI1; bladder; metastasis; tumour marker; p53; pRb
Introduction
KAI1, a newly described marker on human chromo-some 11p11.2, may be important in preventing thedevelopment of metastasis. KAI1 was initially pro-posed to be a speci®c inhibitor of prostate tumourmetastasis [1±3], but more recently, loss ofKAI1 mRNA expression was observed in the progres-sion of bladder cancer to high grade or stage [4] andwas associated with invasive/metastatic potential inbreast cancer [5,6], colon cancer [7,8], and melanoma[9]. Expression of KAI1 also correlated with goodprognosis in patients with non-small cell lung cancer[10,11]. In other cancer types, the relationship betweenKAI1 expression and progression appears more com-plex. For example, KAI protein levels increase in earlypancreatic cancer before a decrease associated withmetastasis [12,13] and in gastric cancer, decreasedprotein levels in metastases can occur in the absence ofany changes in mRNA expression between non-metastatic and metastatic disease [14,15]. Takentogether, these ®ndings suggest that KAI1 may act as
a suppressor of invasion/metastasis in a wide group ofdifferent human cancers, including bladder cancer.
The KAI1 gene encodes a 2.4 kb transcript which istranslated into an N-glycosylated, transmembraneprotein of 267 amino acids of the transmembrane-4superfamily (TM4SF) of proteins [16]. Althoughidentical in amino acid sequence to another memberof this family, CD82, a surface marker of lymphocytes,antibodies to CD82 do not recognise KAI1 (Yu,unpublished data), possibly due to differences in theglycosylation patterns between the two proteins.Furthermore, KAI1 has a much wider tissue distribu-tion than does CD82 [1,4,17]. The biological functionsof TM4SF proteins have not been fully elucidated.Some are involved in cell signalling [18], but theirlocation in the cell membrane and their interactionswith speci®c integrins [19] have also led to the proposalthat many of these proteins may be important forcell±cell and cell±matrix adhesion. Given such a role,loss of KAI1 protein would be consistent with theability of cells to invade or metastasize [6±9].
The classi®cation of urothelial neoplasia is being
Journal of PathologyJ Pathol 2000; 191: 39±47.
Copyright # 2000 John Wiley & Sons, Ltd.

reassessed. Murphy et al. [20] have argued thatpapillary TCC (transitional cell carcinoma) Grade I isnot carcinoma but a papilloma, and that those caseswhich progress to invasive carcinoma or a higher-gradepapillary tumour re¯ect a higher-grade tumour arisingseparately within the urothelium. The InternationalSociety of Urological Pathology, in conjunction withthe World Health Organisation, has published a`consensus classi®cation of urothelial neoplasms' [21]with the aim of providing a `universally acceptableclassi®cation system for bladder neoplasia that couldbe used effectively by pathologists, urologists andoncologists'. With clinical and pathological criteria aswell as classi®cation being controversial, it would bedesirable to delineate cell markers that could de®nepapilloma/low malignant tumours separately from low-and high-grade carcinomas.
We have previously shown that KAI1 mRNA ispoorly expressed in both high-grade and invasivebladder cancer [4]. To examine further the role ofKAI1 in bladder cancer and in an attempt to de®ne aset of markers for bladder cancer progression, we haveexamined both KAI1 mRNA and KAI1 proteinexpression in relation to other markers which may beassociated with advanced disease, speci®cally p53 andpRb [22±24]. In addition, we have assessed the statusof MDM-2, which regulates both p53 function andexpression [25,26].
Materials and methods
Archival tissues
Sixty-six bladder tissue sections were provided byAMRAD Proprietary Ltd. (Melbourne, Victoria, Aus-tralia) [ten normals, seven with in¯ammatory changes,eight transitional cell carcinomas (TCCs) grade I, 13TCCs grade II, 11 TCCs grade III, and 17 high-gradeinvasive carcinomas of the bladder]. A further 69sections [ten normal, nine dysplasia, and ten each ofCIS (de®ned as TCC in situ or carcinoma in situ), TCCgrade I, TCC grade II, TCC grade III, and high-gradeinvasive] were obtained from Douglass Hanly MoirPathology (Sydney, NSW, Australia). The presence ofinvasion was noted, but stage was not able to beassessed. Fresh tissues from both sources were allroutinely ®xed in 10% buffered formaldehyde solutionfor more than 24 h, embedded in paraf®n, and cut into5 mm sections. Twenty-one cases contained normalbladder tissue with no evidence of bladder cancer, butsix showed chronic bladder in¯ammation. Normaltissue was assessed in three cases in which tumourtissue was found. There were nine specimens of bladderdysplasia. Biopsy samples were graded according tothe original WHO classi®cation (normal; dysplasia;TCC in situ; papilloma; papillary TCC grades I, II, III;invasive) and also according to the Consensus Classi-®cation [normal; dysplasia; TCC in situ; urothelialpapilloma (UP); papillary neoplasm of low malignantpotential (LMP); papillary carcinoma low-grade (LG)/
high-grade (HG); invasive [21]) (summarized inTable 1). The study was approved by the ResearchEthics Committee of the South Eastern Sydney AreaHealth Service (SESAHS).
In situ hybridization (ISH)
A modi®ed ISH procedure [27] was used to detect KAImRNA expression in paraf®n-embedded tissue sectionsas described in detail previously [4]. KAI1 mRNA wasdetected using a 1.03 kb probe (residues 64±1094 of theKAI1 cDNA sequence) derived by PCR ampli®cationfrom plasmid pCMVKAI1 [1] as described previously[4]. A b-actin cDNA probe [28] was used as an internalcontrol for RNA integrity and pBR322 DNA as anegative control. All sections were ®rst screened forb-actin mRNA and only those that were positive(34/36 normals and 88/99 biopsies with cancer) werechosen for further analysis of KAI1 expression by ISH.The substrates used were naphthol AS-MX phosphateand fast red TR salt (Sigma Chemical Co., Sydney,NSW, Australia), giving a red colour to positivesignals, which was not in¯uenced by counterstainingwith Mayer's haematoxylin. All staining was assessedby an experienced pathologist (WD). Only thosesections with expression of KAI1 mRNA in morethan 20% of cells were considered positive. Specimenswere recorded as positive or negative; the degree ofstaining was not further quanti®ed.
Immunohistochemistry
Paraf®n-embedded tissue sections were dewaxed inHistochoice Clearing Solution (Amresco, Ohio, USA),rehydrated in a graded series of ethanol (100%, 95%,70%, and 50%), and washed in distilled water. Sectionswere heated in a microwave oven for 10 min in antigenretrieval buffer (0.01 M disodium EDTA; 0.01 M
tri-sodium citrate; 0.02 M Tris, pH. 8), cooled for
Table 1. Histological classi®cation of biopsy samples
Consensus classi®cation
WHO n Unclassi®ed UP LMP LG HG
Normals 20
In¯ammation 7
Dysplasia 9
All non-cancer 36
CIS 10
Papillary TCC GI 18 x 1 15 2 xPapillary TCC GII 23 x x 6 11 6Papillary TCC GIII 21 x x x 2 19
All papillary TCCs, GI±III 62 x 1 21 15 25
Invasive 1 1 x x xGII±invasive 5 x x x 3 xGIII±invasive 21 x x x x 23
All invasive, all grades 27 1 x x 3 23
TCC=transitional cell carcinoma; CIS=Carcinoma in situ; G=grade;
UP=urothelial papilloma; LMP=low malignant potential; LG=low grade;
HG=high grade.
40 K. Ow et al.
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

15 min, and washed twice in PBS. This techniqueprovided a clear background and a high intensity ofspeci®c immunostaining. Endogenous peroxidase activ-ity was quenched in 1.5% H2O2/PBS (Sigma, St. Louis,MO, USA) for 15 min, followed by washing twice withPBS. Non-speci®c protein binding was blocked incasein wash buffer (0.3% casein/0.5% Tween 20/PBS)for 30 min. Sections were then incubated with primaryantibodies for 1 h at room temperature for KAI1 orovernight at 4 uC for p53, MDM-2, and pRb anti-bodies. Sections were then washed twice in 1 : 10 caseinwash buffer for 5 min and incubated with 1 : 200biotinylated anti-mouse IgG or 1 : 250 biotinylatedanti-rabbit Ig (Vector Laboratories, Burlingame, CA,USA) for 30 min. Speci®c intracellular immuno-reactivity was detected by incubation with avidin±biotin/horseradish peroxidase complex (VectorLaboratories, Burlingame, CA, USA) for 45 min atroom temperature followed by colour development in0.05% diaminobenzidine/0.01% H2O2/PBS, pH 7.6chromogen (Sigma, St. Louis, MO, USA) for 5 min.Colour development was stopped by washing indistilled water and the section was lightly counter-stained in haematoxylin, dehydrated in a graded seriesof alcohol, cleared in xylene, and ®nally mounted inEukitt. For KAI1, semi-quantitative scoring ofimmunoreactivity was assessed as follows: 1+, weakfocal immunostaining; 2+, moderate focal/widespreadstaining; 3+, strong widespread staining. Negativesections were scored as 0. Negative or heterogeneousstaining was assessed as abnormal staining. Stainingfor p53 and MDM-2 was only considered positive forstatistical purposes if more than 20% of cells werestained, and in the case of MDM-2, if highly intensestaining was observed. Staining for pRb was classi®edas abnormal if negative staining, or highly intensestaining was observed in over 80% of cells.
Antibodies
Antibodies for the immunostaining of p53 (Clone1801), MDM-2 (1B10) and pRb (84-B3±1) were fromNovocastra Laboratories (Newcastle upon Tyne, UK);polyclonal serum to KAI1 (C-16) was from Santa CruzBiotechnology (Santa Cruz, CA, USA). All sera werecerti®ed for use on paraf®n-embedded sections andsuitable for high-temperature antigen retrieval. Controlcell lines were used as positive and negative controls.Cell pellets were harvested in plasma clots as describedpreviously [29] and ®xed in 10% buffered formalinbefore paraf®n embedding. Sections were stained asabove. UCRU-BL-17/2, which expresses mutant p53[30], and p53 null CALU-6 were used as positive andnegative controls of p53 staining, respectively. SV40-immortalized GM847DM and SJSA-1 (both obtainedfrom Dr R. Reddel, Children's Medical ResearchInstitute, Westmead, NSW, Australia) were used aspositives for pRb and MDM-2 staining, respectively.Preliminary experiments determined optimal dilutionsfor each antibody: p53, 1 : 40; MDM-2, 1 : 60; pRb,
1 : 60; KAI1, 1 : 100. All dilutions were in 1% BSA/PBS.
Statistical methods
Chi-square analysis of two-way frequency tables wasused to test for associations between KAI mRNA,KAI protein, abnormal staining, and other markers.To re¯ect the manner in which specimens weresampled, analyses where appropriate were performedover strata determined by neoplasia group using theMantel±Haenszel procedure. Exact p values (Fisher)were used for 2r2 tables and p values for trend wereused when analysing grade of tumour and markerlevels. All p values were two-sided and no formaladjustment for multiple comparisons was made.
Results
KAI1 mRNA and protein expression in bladderbiopsies
An initial study of KAI1 mRNA expression by in situhybridization (ISH) on a series of 66 normal andtumour samples showed decreased expression in bothhigh-grade and invasive bladder cancer [4]. This studywas extended to include a further 69 samples and aninvestigation of KAI1 protein expression. The datashown represent the analysis of a total of 135 samples,which were histopathologically assessed for grade bytwo systems (Table 1).
KAI1 mRNA was only assessed in biopsies positiveby ISH for a house-keeping gene (b-actin). Therewas signi®cant loss of KAI1 mRNA expression incancer specimens compared with non-cancer biopsies(Table 2; p<0.001, see, for example, Figures 1A, 1Band 1I, 1J) and between invasive (stages TI±TIII) andnon-invasive (stage Ta) papillary TCCs (Table 2;p=0.046). Taking all TCCs into consideration, asigni®cant loss of KAI1 mRNA expression occurredwith increasing tumour grade as measured by theWHO classi®cation system (Table 3). Expression washighest in low-grade, non-invasive, papillary TCCs(45%, grade I and 59%, grade II) and lowest in gradeIII (17%) and TCC in situ or carcinoma in situ (CIS)(2/8, 25%; data not shown in Table 2). A similarpattern was observed if tumours were classi®ed by thenew consensus classi®cation system (Table 4). Expres-sion was highest in low-grade, non-invasive samples(67%, LMP and 47%, LG), and lowest in high-gradetumours (HG, 22%). However, when considering non-invasive TCC only, loss of KAI1 mRNA expressionwith increasing grade was not statistically signi®cantwhen measured by either the WHO system [gradesI±III p (trend)=0.103; Table 3] or the ConsensusClassi®cation [p (trend)=0.058; Table 4].
KAI1 protein expression was examined in the samesamples by immunohistochemistry using a polyclonalserum (C-16) developed by Santa Cruz, which hassuccessfully detected human KAI1 protein by both
Role of KAI1 in bladder cancer 41
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

¯ow cytometry and immunohistochemistry [7,28]. Theresults in Table 2 showed that KAI1 protein expressionwas lost in cancers compared with non-cancers (83%positive compared with 97% positive, p=0.026) and ininvasive (stages TI±TIII) cancers compared with non-invasive TCC grades I±III (44% versus 97% positive,p<0.001). Sixty of 61 low-stage papillary TCCsexamined were positive for KAI1 protein expressionand hence there was no trend between different gradesof cancer.
Interestingly, KAI1 protein showed different pat-terns of staining in cancer compared with normaltissues. In normal bladder, epithelial cell staining wasuniformly intense and often appeared granular(Figure 1C). In cancer specimens, the pattern changedand staining became weaker and either membranous(Figure 1D) or heterogeneous (Figures 1E and 1F). Insome cases of heterogeneous staining, there werepockets of cells with negative staining and others ofpositive staining cells; in other cases, mixed popula-tions of positive and negative cells were seen through-
out. The incidence of abnormal staining (de®ned asnegative staining or heterogeneous staining) increasedin cancer compared with non-cancer (Table 2,p<0.001) and was higher in invasive than in non-invasive cancers (Table 2, p=0.017). Comparing allpapillary TCCs or non-invasive only TCCs, therewas a signi®cant trend towards gain of abnormalstaining with increasing grade using either gradingsystem (Tables 3 and 4). In CIS, only 1/10 specimenswas totally negative for KAI1 protein expression(Figure 1G) whilst another showed a mixed pattern(Figure 1H). Expression of KAI1 protein was normalin 8/10 CIS samples. Given the small numbers, furthersamples are needed to con®rm these data.
The loss of both mRNA expression and normalprotein staining (measured as gain of heterogeneousstaining or complete loss of staining, Tables 3 and 4)clearly correlated with increasing tumour stage. Impor-tantly, approximately 80% of invasive cancers werenegative for KAI1 mRNA expression and most wereeither negative or showed heterogeneous KAI1 protein
Table 2. Expression of KAI1 mRNA and protein, and p53protein in normal versus tumourigenic bladder biopsies
All papillary cancers
N: 135 89
Normal TCC Ta TI, II, III
N 36 99 62 27
KAI mRNA
x/n 31/34 31/88 24/54 5/26
% 91 35 45 19p <0.001 0.046
KAI1 Prot!
x/n 35/36 81/98 60/61 12/27% 97 83 97 44
p 0.026 <0.001
KAI1 Prot*x/n 1/36 73/98 45/61 26/27
% 4 74 75 96
p <0.001 0.017
p53x/n 3/36 32/99 24/62 10/27
% 8 33 39 37
p 0.002 1.000
MDM-2**
x/n 8/36 32/97 19/59 10/27
% 23 33 32 37
p53*x/n 11/36 67/97 43/59 20/27
% 30 66 73 74
p 0.160 1.000
`Normal' indicates normal samples or those with dysplasia or in¯ammatory
changes. CIS costs are not included in the table. The data for these ten
specimens are included in the text. Paraf®n-embedded sections were
examined for KAI1 mRNA expression, and for KAI1, p53, and MDM-2protein expression as described in the Materials and methods section. KAI1
Prot! indicates positive versus negative staining for KAI1 protein. KAI1
Prot* indicates abnormal staining de®ned as negative or heterogeneousstaining. MDM-2** represents samples that were p53-negative but >1+for MDM-2. p53* represents total abnormal p53 staining, including p53
staining >1+ and MDM**.
Table 3. Expression of KAI1 mRNA and protein, and p53protein in bladder biopsies classi®ed by the WHO grad-ing system
All TCCs Non-invasive TCCs
N: 88 62
I II III I II III
N: 18 28 42 18 23 21
KAI mRNA
x/n 5/11 16/27 7/41 5/11 14/22 5/21
% 45 59 17 45 64 24p <0.005 (trend) 0.013 (trend)
KAI1 Prot!
x/n 17/18 24/27 30/42 Not relevant% 94 89 71
p 0.020 (trend)
KAI1 Prot*x/n 8/18 23/27 39/42 8/18 18/22 19/21
% 44 85 93 44 82 90
p <0.001 (trend) 0.001 (trend)
p53
x/n 4/18 6/28 22/42 4/18 5/23 13/21
% 22 21 52 22 22 62
p 0.008 (trend) 0.008 (trend)
MDM-2**
x/n 4/17 13/27 12/42 4/17 10/22 5/21
% 23 48 29 24 45 24p53*
x/n 8/17 19/27 34/42 8/17 15/22 18/21
% 47 70 81 47 65 86
p 0.004 (trend) 0.020 (trend)
Paraf®n-embedded sections were examined for KAI1 mRNA expression by
in situ hybridization, and for KAI1, p53, and MDM-2 protein expression by
immunohistochemistry as described in the Materials and methods section.KAI1 Prot! indicates positive versus negative staining for KAI1 protein. KAI1
Prot* indicates abnormal staining de®ned as negative or heterogeneous
staining. MDM-2** represents samples which were p53 negative for p53
but >1+ for MDM-2. p53* represents total abnormal p53 stainingincluding p53 staining >1+ and MDM**.
42 K. Ow et al.
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

expression. For invasive cancers, loss of KAI1 mRNAand protein expression were positively correlated, butthis was not statistically signi®cant ( p=0.13). Bothexpression of KAI1 mRNA and of normal KAI1
protein staining were reduced with increasing neoplasiafor the whole group (Tables 3 and 4), but within thecancers, adjusting for group, this correlation was notstatistically signi®cant ( p=0.89).
Figure 1. Patterns of KAI1 mRNA expression (A, B, and I, J) and protein staining (C±H) in normal bladder and bladder tumoursamples were assessed as described in the Materials and methods section. In situ hybridization for KAI1 mRNA showed strongexpression in normal bladder (A) but negative expression of the control vector pBR322 (B). Negative expression of KAI1 mRNAwas observed in invasive bladder cancer (I) even though the positive control (b-actin, J) was strongly expressed.Immunohistochemical analysis for KAI1 protein expression showed uniformly intense staining in all normal cells (C), whichbecame weaker and membranous (D) or heterogeneous (E, F) in papillary TCC tumour samples. CIS samples either were negativefor KAI1 protein expression (G) or showed a mixed pattern (H). r36
Role of KAI1 in bladder cancer 43
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.
KAI1 expression versus p53 status in bladderbiopsies
We compared KAI1 mRNA expression with p53 status(determined using PAb1801) in bladder cancer speci-mens. No staining or weak staining for p53 (score 0,1+) was considered to indicate `wild-type' p53, whereashigh level staining (>1+, equivalent to more than 20%positive cells) was taken to indicate mutant p53. Theresults summarized in Table 2 showed that in general,little or no p53 staining was observed in normal tissues(0%), in¯ammatory tissues (0%) or dysplasia (22%),with a total of 3/36 (8%) in non-cancer tissues. Takingall TCCs into consideration, p53 staining was less inlow-grade papillary TCCs (22% grade I and 21% gradeII, WHO system, Table 3) and tumours of LMP (24%Consensus Classi®cation, Table 4) than in high-grade(52% in grade III, WHO system, Table 3; 46% in HG,Consensus Classi®cation, Table 4). In non-invasiveTCCs only, p53 staining was less in low-grade (Grade
I, II, WHO System, Table 3; LMP, Consensus Classi-®cation, Table 4) tumours than in high-grade tumours(Grade III, WHO System, Table 3; HG, ConsensusClassi®cation, Table 4). The p53 staining was also highin invasive papillary TCC (37%, Table 2) and 20% ofCIS biopsies showed p53 staining (data not shown).Overall, staining for p53 was signi®cantly increased incancer versus non-cancer specimens ( p=0.002, Table 2)and with increasing grade in all tumours (WHOgrading, p=0.008, Table 3; Consensus Classi®cation,0.043, Table 4) or non-invasive only cancers [WHOgrading, p=0.008, Table 3; Consensus Classi®cation, p
(trend)=0.031, Table 4], but was not more elevated ininvasive than in non-invasive cancers ( p=1.000,Table 2), probably because of the high percentage ofp53 positive staining in non-invasive high-gradetumours. Abnormal p53 staining was increased withincreasing neoplasia, whilst KAI1 mRNA expressionwas generally decreased (Tables 3 and 4), but thenegative correlation between KAI1 mRNA and p53was not statistically signi®cant when the results from alltissues were included ( p=0.33; adjusted for group,p=0.18), nor when only cancer samples were analysed(p=0.65; adjusted for group, p=0.26).
We also examined protein levels of the p53 regulatorMDM-2, because overexpression of MDM-2 is analternative mechanism for inactivating p53 functionwithout p53 mutation [31]. Some tissues which stained
Table 4. Expression of KAI1 mRNA and protein, and p53protein in bladder biopsies classi®ed by the conventionalclassi®cation system
All TCCs Non-invasive TCCs
N:
88 62
UP LMP LG HG UP LMP LG HGN 1 21 18 48 1 21 15 25
KAI mRNA
x/nx/n 0/1 10/15 8/17 10/46
% 0 67 47 22
p 0.004 (trend) 0.058 (trend)
KAI1 Prot!
x/n 1/1 20/21 16/18 34/47 Not relevant
% 100 95 89 72
p 0.015 (trend)
KAI1 Prot*
x/n 0/1 13/21 14/18 43/47 0/1 13/21 11/15 21/24
% 0 62 78 91 0 62 73 88p 0.001 (trend) 0.018 (trend)
p53
x/n 0/1 5/21 5/18 22/48 0/1 5/21 4/15 13/25% 0 24 28 46 0 24 27 52
p 0.043 (trend) 0.031 (trend)
MDM-2**x/n 0/1 6/20 7/18 16/47 0/1 6/20 6/15 7/24
% 0 30 39 34 0 30 40 29
p53*
x/n 0/1 11/20 12/18 37/47% 0 55 67 79 0 55 67 83
p 0.020 (trend) 0.018 (trend)
Paraf®n-embedded sections were examined for KAI1 mRNA expression byin situ hybridization, and for KAI1, p53, and MDM-2 protein expression by
as described in the Materials and methods section. KAI1 Prot! indicates
positive versus negative staining for KAI1 protein. KAI1 Prot* indicates
abnormal staining de®ned as negative or heterogeneous staining. MDM-2**represents samples which were p53-negative for p53 but >1+ for MDM-
2. p53* represents total abnormal p53 staining including p53 staining >1+and MDM**.
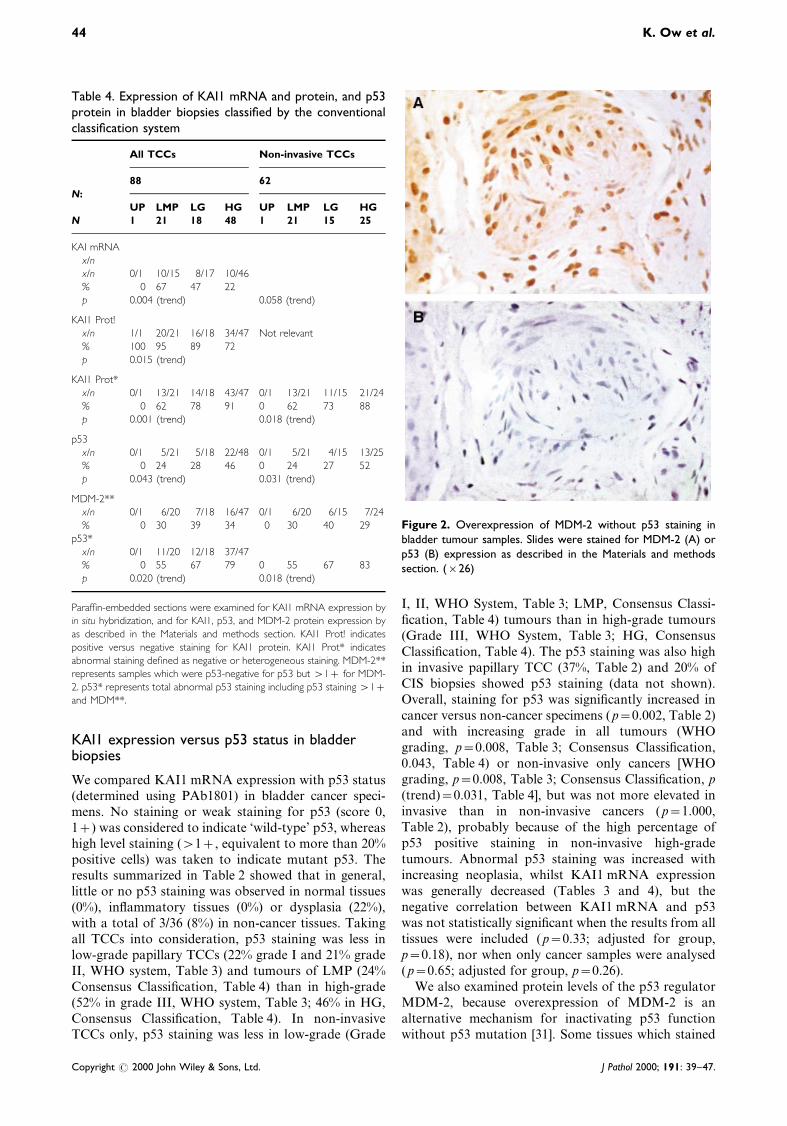
Figure 2. Overexpression of MDM-2 without p53 staining inbladder tumour samples. Slides were stained for MDM-2 (A) orp53 (B) expression as described in the Materials and methodssection. (r26)
44 K. Ow et al.
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

negatively for p53 showed strongly positive MDM-2staining (Figures 2A and 2B, summarized in Tables 2,3 and 4). Overexpression of MDM-2 (staining greaterthan 1+) was found in a small proportion of normal,low-grade tumours and CIS samples (10±30%), but wasincreased in high-grade invasive tumours (61%)(Table 5).
In a further assessment of staining, we de®nedabnormal p53* status to include both p53 staininggreater than 1+ and samples in which no detectablep53 staining occurred, but which showed overstainingof MDM-2, as these were likely to represent biopsies inwhich p53 could be dysfunctional (Tables 3 and 4).There was no correlation between KAI1 mRNAexpression and p53* status when all specimens wereincluded in the analysis (p=0.98; adjusted for cancerand invasion, p=0.083), or when all cancer specimenswere analysed ( p=0.16; adjusted for grade andinvasion, p=0.077).
KAI1 mRNA expression versus pRb expression inbladder biopsies
The pRb status of bladder biopsies was also assessedas absent, heterogeneous (normal) or strongly homo-
geneous (Table 5) and was compared with expressionof KAI1 mRNA. Comparisons of pRb negative statuswith loss of KAI1 mRNA were not statisticallysigni®cant when all samples were analysed [p(trend)=0.30] or following adjustment for the presenceof cancer [ p (trend)=0.59]. Whilst strong homoge-neous pRb staining was seen in some non-invasiveTCCs, there was no signi®cant relationship betweenKAI1 mRNA expression and pRb staining (Table 6).
Discussion
Several studies have shown that inactivation of bothp53 and pRb genes occurs in bladder tumours thathave a more aggressive clinical outcome and poorprognosis [22]. In a recent study, evidence waspresented that the KAI1 suppressor gene might alsobe an important marker of bladder cancer invasionand metastases [4]. In the present study we haveextended these initial observations and have clearlyshown that invasive bladder cancers exhibit loss ofboth KAI1 mRNA and KAI1 protein expression.Moreover, these cancers show a changed pattern ofKAI1 protein staining compared with normal tissues,
Table 5. MDM-2 and pRb staining in bladder biopsies
MDM-2 (No. >1+/ pRb (No negative/ pRb (No 3+/ total
Designation n total examined) total examined) examined)
Normals 20 3/10 3/20 3/20
In¯ammation 7 6/7 0/7 3/7
Dysplasia 9 2/9 4/9 1/9All non-cancer 36 11/26 7/36 7/36
(42%) (19%) (19%)
CIS 10 2/10 3/10 4/10(20%) (30%) (40%)
Papillary TCC GI 18 6/17 8/18 1/18
Papillary TCC GII 23 8/22 4/23 3/23Papillary TCC GIII 21 5/20 8/21 8/21
All papillary TCCs, GI-III 62 19/59 20/62 13/62
(32%) (32%) (21%)
Urothelial papilloma (UP) 1 0/1 1/1 0/1
Low malignant potential (LMP) 21 8/20 7/21 4/21
Low grade (LG) 15 6/15 4/15 3/15
High grade (HG) 25 8/24 8/25 6/25All TCCs 62 22/60 20/62 13/62
(375) (32%) (21%)
Invasive, all grades 27 14/23 16/27 0/27(61%) (59%) (0%)
Paraf®n-embedded sections of bladder tissues were examined for MDM-2 and pRb protein expression by immunohistochemistry as described in the
Materials and methods section.
Table 6. Relationship between expression of KA11 mRNA and pRb
CategoryNo./total examined (percentage) of samples showing KAI1 mRNA expression
pRb staining: Negative Weak heterogeneous Strong heterogeneous p value
All biopsies 15/41 37% 34/60 57% 13/21 62% 0.075
Cancer samples only 8/33 24% 16/41 39% 7/14 50% 0.19
Role of KAI1 in bladder cancer 45
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

with either noticeable membranous staining, or hetero-geneous staining being apparent in different tumours.Although it is possible that these changes have afunctional signi®cance, they could also result fromdifferences in expression level and/or cellular location.It is also possible that these observations might re¯ectloss in bladder tumour progression of another, as yetunidenti®ed, protein which is important for localiza-tion of KAI1, as occurs for E-cadherin [31,32]. Thesedata emphasize the need to elucidate the normalcellular role of KAI1.
There is no signi®cant difference in expression forKAI1 or p53 between the two different classi®cation/grading systems. This is in accordance with the factthat the two sets of terminologies refer to the sametumours, but use different names, with the ConsensusClassi®cation more closely indicating the true clinicalbehaviour of the tumours. KAI1 showed no variationbetween the grades of papillary, non-invasive tumours.p53, however, showed increased staining in higher-grade non-invasive papillary tumours in both classi®-cations. This may prove useful in the future, after otherlarger studies, to delineate low- from high-gradetumours and may indicate a worse prognosis.
A recent study has provided evidence that KAI1may be a transcriptional target of the p53 tumoursuppressor protein and that in prostate cancer, loss ofKAI1 expression is associated with loss of p53expression and presumably loss of normal p53 [33].We examined the relationship between expression ofp53 and KAI1 mRNA, but the results were not clear-cut. In some cases, but not others, gain of p53expression was associated with loss of KAI1 mRNAexpression. When data from all samples or onlycancer samples were analysed, there was no relation-ship between increased p53 staining and loss ofKAI1 mRNA expression, even after adjustment forgroup ( p=0.26). In addition, the relationship betweenKAI1 mRNA and p53 expression did not appear to bein¯uenced by overexpression of MDM-2, althoughMDM-2 has been shown to modulate p53 actively inother circumstances [34]. These data do not supportthe contention that KAI1 is a cellular target gene forp53, as suggested by Mashimo et al. [33]. To examinemore clearly the relationship between p53 andKAI1 mRNA levels in bladder cancer, we are currentlyinvestigating KAI1 mRNA levels in a series of bladdercancer cell lines in which both the sequence and thefunctional status of the endogenous p53 have beenestablished. In addition, we are using p53-null linesfrom this series in transfection studies to determinewhether the introduction of wild-type affects endogen-ous KAI1 mRNA levels. However, our initial datafrom clinical specimens suggest that loss of p53 is notresponsible for the loss of KAI1 expression in bladdercancer progression.
Loss of normal pRb staining is thought to re¯ect adysfunctional Rb pathway associated with higherrecurrence and lower survival rates in bladder cancer[35,36]. We therefore compared loss of KAI1 mRNA
expression with loss of pRb staining, but did notobserve a statistically signi®cant relationship betweenthese markers.
Apart from the potential role of p53, our presentstudy did not attempt to determine how KAI1expression is decreased in higher-grade and invasivebladder cancer. Possibilities include loss of heterozyg-osity (LOH) on chromosome 11, or methylation of theKAI1 gene. It was not possible to study the genotypeof the tumours studied, but studies of prostate cancerhave shown that the loss of KAI1 expression is notassociated with LOH on chromosome 11 in cancers [2].Preliminary studies of three invasive bladder carcino-mas showed no methylation of the KAI1 gene (PJ,unpublished data); further studies are planned.
In conclusion, we have shown that loss of bothKAI1 mRNA and normal KAI1 protein expression isassociated with high-grade and invasive bladdercancer. The loss of KAI1 mRNA does not correlatewith a gain of p53 staining or with overexpression ofMDM-2, suggesting that loss of p53 function may notbe responsible for the loss of KAI1 expression. Therewas no correlation between loss of KAI1 expressionand loss of normal pRb staining. These data suggestthat loss of KAI1 expression may be useful as a markerof bladder cancer progression.
Acknowledgements
This work was supported by an award from The Leo and Jenny
Leukemia and Cancer Foundation of Australia (PJ and PJR).
References
1. Dong JT, Lamb PW, Rinker-Schaeffer CW, et al. KAI1, a
metastasis suppressor gene for prostate cancer on human
chromosome 11p11.2. Science 1995; 268: 884±886.
2. Dong J-T, Suzuki H, Pin SS, et al. Down-regulation of the KAI1
metastasis gene during the progression of human prostatic cancer
infrequently involves gene mutation or allelic loss. Cancer Res
1996; 56: 4387±4390.
3. Ueda T, Ichikawa T, Tamaru J, et al. Expression of the KAI1
protein in benign prostatic hyperplasia and prostate cancer. Am
J Pathol 1996; 149: 1435±1440.
4. Yu Y, Yang J-L, Marcovic B, et al. Loss of KAI1 messenger
RNA expression in both high grade and invasive bladder
cancers. Clin Cancer Res 1997; 3: 1045±1049.
5. Yang XH, Welch DR, Phillips KK, Weissman BE, Wei LL.
KAI1, a putative marker for metastatic potential in human
breast cancer. Cancer Lett 1997; 119: 149±155.
6. Phillips KK, White AE, Hicks DJ, et al. Correlation between
reduction of metastasis in the MDA-MB-435 model system and
increased expression of the Kai-1 protein. Mol Carcinogen 1998;
21: 111±120.
7. Takaoka A, Hinoda Y, Satoh S, et al. Suppression of invasive
properties of colon cancer cells by a metastasis suppressor KAI1
gene. Oncogene 1998; 16: 1443±1453.
8. Yang J-L, Jackson P, Yu Y, et al. Loss of KAI expression is
associated with invasion and metastasis in cell lines derived from
human sporadic colon cancer (submitted).
9. Takaoka A, Hinoda A, Sato S, et al. Reduced invasive and
metastatic potentials of KAI1-transfected melanoma cells. Jpn
J Cancer Res 1998; 89: 397±404.
10. Adachi M, Taki T, Ieki Y, Huang C-I, Higashiyama M, Miyake
M. Correlation of KAI1/CD82 gene expression with good
46 K. Ow et al.
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.

prognosis in patients with non-small cell lung cancer. Cancer Res
1996; 56: 1751±1755.
11. Higashiyama M, Kodama K, Yokouchi H, et al. KAI1/CD82
expression in nonsmall cell lung carcinoma is a novel, favourable
prognostic factor ± an immunohistochemical analysis. Cancer
1998; 83: 466±474.
12. Guo X, Friess H, Graber HU, et al. KAI1 is up-regulated in
early pancreatic cancer and decreased in the presence of
metastasis. Cancer Res 1996; 56: 4876±4880.
13. Friess H, Guo X-Z, Berberat P, et al. Reduced KAI1 expression
in pancreatic cancer is associated with lymph nodes and distant
metastases. Int J Cancer 1998; 79: 349±355.
14. Guo XZ, Friess H, Maurer C, et al. KAI1 is unchanged in
metastatic and nonmetastatic esophogeal and gastric cancer.
Cancer Res 1998; 58: 753±758.
15. Hinoda Y, Adachi Y, Takaoka A, et al. Decreased expression of
the metastasis suppressor gene KAI1 in gastric cancer. Cancer
Lett 1998; 129: 229±234.
16. Wright MD, Tomlinson MG. The ins and outs of the
transmembrane 4 superfamily. Immunol Today 1994; 15:
588±594.
17. Huang CL, Taki T, Adachi M, et al. MRP-1/CD9 and KAI1/
CD82 expression in normal and various cancer tissues. Int
J Oncol 1997; 11: 1045±1051.
18. Bradbury LE, Kansas GS, Levy S, Evans RL, Tedder TF. The
CD19/CD21 signal transducing complex of human B lympho-
cytes includes the target of anti-proliferative antibody-1 and leu-
13 antigen. J Immunol 1992; 149: 2841±2850.
19. Hemler ME, Mannion BA, Berditchevski F. Association of
TM4SF proteins with integrins: relevance to cancer. Biochim
Biophys Acta 1996; 1287: 67±71.
20. Murphy WM, Beckwith JB, Farrow GM. Tumours of the Kidney,
Bladder, and Related Urinary Structures. Atlas of Tumour
Pathology, Series 3, Fascicle 11. Armed Forces Institute of
Pathology: Washington, DC, 1994.
21. Epstein JI, Amin MB, Reuter VR, Mosto® FK, and the Bladder
Consensus Conference Committee. The World Health Organisa-
tion/International Society of Urological Pathology Consensus
Classi®cation of Urothelial (Transitional Cell) Neoplasms of the
Urinary Bladder. Am J Surg Pathol 1998; 22: 1435±1448.
22. Cordon-Cardo C, Scheinfeld J, Dalbagni G. Genetic studies and
molecular markers of bladder cancer. Semin Surg Oncol 1997; 13:
319±327.
23. Dorkin TJ, Robson CN, Neal DE. The molecular pathology of
urological malignancy. J Pathol 1997; 183: 380±387.
24. Ozen H. Bladder cancer. Curr Opin Oncol 1998; 10: 273±278.
25. Haupt Y, Maya R, Kazac A, Oren M. MDM-2 promotes rapid
degradation of p53. Nature 1997; 387: 296±299.
26. Kubbutat MH, Jones SN, Vousden KH. Regulation of p53
stability by MDM-2. Nature 1997; 387: 299±303.
27. Marcovic B, Wu ZH, Chesterman CN, Chong BH. Quantitation
of Fc c RII mRNA in platelets and megakaryoblastic cell lines
by a new method of in situ hybridization. J Immunol Methods
1994; 72: 105±114.
28. Erba HP, Gunning P, Kedes L. Nucleotide sequence of the
human c cytoskeletal actin mRNA: anomalous evolution of
vertebrate non-muscle actin genes. Nucleic Acids Res 1986; 14:
5275±5294.
29. Ow KT, Mameghan H, Lochhead AH, et al. The prognostic
signi®cance of tumour-associated markers p53, HER-2/neu, c-
myc, v-H-ras, PCNA and EGFr of local and distant recurrence
in localized human prostatic adenocarcinoma. Urol Oncol 1995;
1: 144±152.
30. Ribeiro JCC, Barnetson AR, Fisher R, Mameghan H, Russell
PJ. Radiosensitivity is independent of p53 status in three human
bladder cancer cell lines. Int J Radiat Biol 1997; 72: 11±20.
31. Morton RA Jr, Eving CM, Watkins JJ, Isaacs WB. The E-
cadherin cell-cell adhesion pathway in urologic malignancies.
World J Urol 1995; 13: 364±368.
32. Mialhe A, Louis J, Montlevier S, et al. Expression of E-cadherin
and alpha-, beta- and gamma-catenins in human bladder
carcinomas: are they good prognostic factors?. Inv Metastasis
1997; 17: 124±137.
33. Mashimo T, Watabe M, Hirota S, et al. The expression of the
KAI1 gene, a tumour metastasis suppressor, is directly activated
by p53. Proc Natl Acad Sci U S A 1998; 95: 11307±11311.
34. Momand J, Zambetti GP. MDM-2: `big brother' of p53. J Cell
Biochem 1997; 64: 343±352.
35. Grossman HB, Liebert M, Antelo M, et al. p53 and RB
expression predict progression in T1 bladder cancer. Clin
Cancer Res 1998; 4: 829±834.
36. Cote RJ, Dunn MD, Chatterjee SJ, et al. Elevated and absent
pRb expression is associated with bladder cancer progression
and has cooperative effects with p53. Cancer Res 1998; 58:
1090±1094.
Role of KAI1 in bladder cancer 47
Copyright # 2000 John Wiley & Sons, Ltd. J Pathol 2000; 191: 39±47.