· reflex sympathetic dystrophy (rsd)/crps/sudeck … · 2019-08-03 · (rsd)/crps/sudeck does not...
TRANSCRIPT
ifsshezine
CONNECTING OUR GLOBAL HAND SURGERY FAMILY
www.ifssh.info VOLUME 9 | ISSUE 3 | NUMBER 35 | August 2019
UPCOMING EVENTS RESEARCH ROUND-UP
SPECIAL FEATURES · REFLEX SYMPATHETIC DYSTROPHY
(RSD)/CRPS/SUDECK DOES NOT EXIST · OUTCOME MEASUREMENT IN
HAND SURGERY
SUDECK / RSD / CRPS1
1
August 2019
3 EDITORIAL • IFSSH/IFSHT Congress, Berlin 2019 • Points to Ponder - Ulrich Mennen
4 EXECUTIVE NEWS President: Acceptance Speech - Marc Garcia-Elias
5 SECRETARY-GENERAL REPORT 14th IFSSH Congress Berlin, 2019 - Goo Hyun Baek - Daniel J. Nagle
8 PIONEER PROFILES • Stewart H. Harrison • Hanno Millesi
10 COMMITTEE REPORT • Asian-PacificFederationofSocietiesfor
SurgeryoftheHand(APFSSH)2019Report • Hand and Wrist Biomechanics International
(HWBI) • IFSHT report to IFSSH executive committee
meeting
14 SPECIAL FEATURES • Outcome measurement in hand surgery - Miriam Marks, - Daniel B. Herren • ReflexSympatheticDystrophy(RSD)/CRPS SUDECK does not exist. - F. del Piñal
21 ART "Together Strong"
34 RESEARCH ROUND-UP OutcomesFollowingReplantation RevascularizationintheHand - Hoyune Esther Cho, - Sandra V. Kotsis - Kevin C. Chung
36 MEMBER SOCIETY NEWS • TheBelgianSocietyforSurgeryoftheHand • AssociationofChinese-speakingHand
Surgeons United • Ecuadorian Hand Surgery Society
(ECUMANO) • BrazilianSocietyforSurgeryoftheHand
(SBCM) • AustrianSocietyforSurgeryoftheHand • ChileanSocietyforSurgeryoftheHand
42 SHARE SECTION ImagesfromtheIFSSH/IFSHTCongressin Berlin June 2019
57 UPCOMING EVENTS Listofgloballearningeventsandconferences
forHandSurgeonsandTherapists
www.ifssh.info VOLUME 9 | ISSUE 3 | NUMBER 35 | AUGUST 2019
contents
ThisAugustEzineissuefeaturestwothoughtprovokingpresentations. Both challenge conventual thinking. Both examine long held “truths”. Bothdemandarethinkofconceptswhichwehavepropagatedfromone generation to the next. Bothaskforaparadigmshiftinourclinicalpractice. Theremaybe(andprobablyare)morelonghelddiagnoses,concepts,didactic dogmas, surgical techniques, diagnostic methods, customs, and mannerisms which need “updating”. The challenge is on! With sincere regards,Ulrich
The14thtriennialIFSSHCongresshasbeenahugesuccess.Notonly“biggerandbetter”insize,attendanceandorganization,butalsoacademically the choice was outstanding. ThisagainemphasizestheimportanceoftheIFSSHfunction:tocreateaplatformforHandSurgeonsandHandTherapistsfromallovertheworld to share their experience, ideas and expertise. Andtointeract:buildingbridges Well done Berlin!
IFSSH/IFSHT Congress, Berlin 2019
EDITORIAL
IFSSH DISCLAIMER:The IFSSH ezine is the official mouthpiece of the International Federation of Societies for Surgery of the Hand. The IFSSH does not endorse the commercial advertising in this publication, nor the content or views of the contributors to the publication. Subscription to the IFSSH ezine is free of charge and the ezine is distributed on a quarterly basis. Should you be interested to advertise in this publication, please contact the Editor: [email protected]
IFSSH EZINE EDITORIAL TEAM:EDITOR:Professor Ulrich Mennen Past President: IFSSH
DEPUTY EDITOR: Professor Michael Tonkin Past President: IFSSH
GRAPHIC DESIGNER: Tamrin [email protected]
TO SUBSCRIBE GO TO: [email protected]
ifsshezine
CONNECTING OUR GLOBAL HAND SURGERY FAMILY
Points to Ponder
Prof. Ulrich Mennen
Editor: IFSSH Ezine
Past President: IFSSH
EDITORIAL
2 3
August 2019www.ifssh.info
EXECUTIVE NEWS
President: Acceptance SpeechMy dear colleagues:Iwishtothankyou,membersoftheMemberSocietiesofthisFederation,forhavingplacedyourtrustandconfidenceinme.Beingaskedtoserveasthe19thPresidentoftheInternationalFederationofSocietiesforSurgeryoftheHandisanhonour,andanundeservedprivilegewhichIwilltreasureallmylife.
Asyouprobablyknow,Iamawristsurgeon,andabasicscienceenthusiast,fascinatedbytheanatomyandmechanicsofthewrist.Maybebecauseofthis,Iknowthateventhemostsimplestructurebecomescomplexwhenyoulookatitcarefullyenough.Yet,weshouldnotregardcomplexityasathreat,butasanopportunitytoseefurther,achallengetoovercome.Complexityisonlyaproblemifoneisafraidoffacingit.ThisishowIthinkwe should work in this Federation. Let us not see “the different”asathreat,butasanotherindispensablefaceofthe polyhedron,we live in. In the IFSSH there is no place forqualifyingadjectivesthatsetborders,butonlyforthose that erase them.
Asidefromananti-supremacist,Iamalsoacompulsoryoptimist,apositivethinkingtypeofpersonwhoisnotafraidoffacingproblemsasapartoflife.Ilikeseeingtheglasshalffullratherthanhalfempty.Ibelieveinfindingsolutionswhereothersonlyseeproblems,andI wish I could contaminate you all with this attitude. To me that is the only way to do things. This does not mean thatIdisregardhowsignificantthiscommitmentis.Iknowitwillbehard,butIamreadytobuilduponthesuccessesofthepastanddowhateverIcantofulfillourmission, which is no other than to promote hand surgery throughout the world, to protect your interests worldwide, andtolookafterthewidercommunityofhandpatients.
Let’snotfinishthiswithoutexpressingourgratitudetothe outgoing Immediate Past President Michael Tonkin. Alwayskind,alwayshumble,heprovidedtheIFSSHwithdirectionandleadershipoverthelastfewyears.Hehandledmanydifficultissueseffectively.Ilearnedfromhim what “keep calm” means, despite my pronunciation wasneverbeingright.Butaboveall,hewaseffectiveatkeepingnon-essentialissuesoutoftheboardroom.Thesetraits I intend to continue during my term.
Thank you, Michael, and thank you all so much again.
Best wishes!
MarcKind regards,
Marc Garcia-EliasPresident: IFSSH.
SECRETARY-GENERAL REPORT
ItisagreathonourformetohavetheopportunitytoservetheIFSSHasSecretary-General.DuringthepreviousthreeyearsasSecretary-GeneralElect,ItriedtolearntheheritagesandlegaciesoftheFederationasmuchaspossible.
TheIFSSHnowhas60MemberSocietiesfromallovertheworldwhosecultures,languages,andwaysofthinkingdifferfromeachother.AlthoughIdonotunderstandallthedifferencesofthevariouscountries,Ifoundthatwecanfindagreementamongstourselvesthroughharmonyandteamwork.
TheBylawsoftheFederationstatethatitsmissionistocoordinatetheactivitiesofalltheSocietiesforSurgeryoftheHandthroughouttheworld,andinthiswaytopromoteknowledgeofsurgeryofthehand.
UndertheguidanceofMarcGarcia-Elias,ournewPresident,andwiththehelpoftheExecutiveCommitteemembersandtheMemberSocieties,IwilldomybesttocoordinatetheactivitiesoftheMemberSocietiesandtoincreaseandspreadthisknowledge,especiallytothedisadvantagedmembersandyounghandsurgeons. Future Meetings Adetailedlistofnationalandregionalhandsurgerymeetingsisavailableonthe IFSSHwebsite.ThetriennialIFSSHCongressesareasfollows:
XVth IFSSH – XIIth IFSHT Congress London, United Kingdrom 27th June - 1st July, 2022
XVIth IFSSH – XIIIth IFSHT Congress Washington D.C., USA 29th March - 3rd April, 2025
Goo Hyun Baek
Secretary-General, IFSSH
Email: [email protected]
Welcome from the incoming Secretary-General
4 5
August 2019www.ifssh.info
The14thTriennialCongressoftheInternationalFederationofSocietiesforSurgeryoftheHandandthe11thTriennialCongressoftheInternationalFederationofSocietiesforHandTherapywereheldintheBerlinCityCubefromJune17throughJune21.ThiswasthefirstCongresstoincludemanyactivitiesoftheFederationofEuropeanSocietiesforSurgeryoftheHand(FESSH).TheorganizingcommitteechairedbyProfessorJörgvanSchoonhoven,ProfessorMaxHaerle,ProfessorAndreasEisenschenk,NataschaWeihs&BeateJungorchestrated an extraordinary Congress. Over 4000 physicians and therapists participated in this meeting representing 92 countries. The Congress theme was “Building Bridges Hand in Hand” and given the massive international attendance it is clear the Congress did indeed accomplish that goal.
Themeetingfeaturedapre-CongressMondayeducationdaywhichfeaturedmanyindustrysponsoredcoursesandlectures.TheCongressofficiallyopenedMondayafternoonwiththeOpeningCeremonythatfeaturedtherecognitionofnewlynominatedPioneersofHandSurgery.Thirty-sevenPioneersfrom19societieswerehonored.ThesePioneersalongwiththeirfamiliestravelledfromallovertheworldtoparticipateinthisceremonythatwasindeedmonumentalandinspiring.TheOpeningCeremonywasfollowedbyacocktailpartywithanentertainingperformancefrom“TheCarpalBossandLooseBodies”band,featuringmanyhandsurgeonsandtherapistsfromaroundtheworld.
Thescientificprogramwasimpressive.TherewasanoverwhelmingresponsetotheCallforAbstracts,with1800submissionsassessedby242reviewers.TheCongressOrganizingCommitteethenappointed45Germancolleaguestolead27subgroupsandworkwith27internationalhandexpertstobuildthescientificprogramme.Thefinalprogramincluded357invitedlecturesand1123freepapersoverseenby347chairpersons.
TheIFSSHDelegatesmetonWednesday,June19,2019.ThefirstorderofbusinesswastowelcomeanewmembertotheIFSSHfamily,theEcuadorianSocietyforSurgeryoftheHand.TheEcuadoriansocietyisthe60thsocietytojointheIFSSH!
ThenextorderofbusinesswastheelectionofthenewExecutiveCommittee(ExCo):ImmediatePastPresident: Dr.ZsoltSzaboofHungaryPresident: Dr.MarcGarciaEliasofSpainPresidentElect: Dr.DanielNagleoftheUnitedStatesSecretary-General: Dr.GooHyunBaekofSouthKoreaSecretary-GeneralElect: Dr.RajaSabapathyofIndiaHistorian: Dr.DavidWarwickofEnglandMemberatLarge: Dr.JinBoTangofAssociationofChinese-speakingHandSurgeonsUnited
TheExCo,duringthecomingmonths,willbeworkingwiththeDelegatesonmuchneededbylawschangesaswell as structural changes to increase Society participation in the ExCo.
SECRETARY-GENERAL REPORT
TheDelegateswerethenchargedwiththeselectionofthe2025IFSSHtriennialmeetingsite.Dr.ScottLevin,thecurrentPresidentoftheASSH,presentedthewell-preparedbidbyTheAmericanSocietyforSurgeryoftheHandandtheAmericanAssociationofHandSurgerytohostthe2025IFSSHTriennialCongressinWashingtonDC.Dr.MarcelloRosadeRezende,PresidentoftheBrazilianSocietyforSurgeryoftheHand,providedtheDelegateswithanexcellentpresentationpromotingRiodeJaneiroforthe2025IFSSHCongress.Finally,Dr.LuisNaquira,PresidentoftheColombianAssociationofHandSurgery,gavearousingpresentationurgingtheDelegatestosupporttheColombianbidtotakethe2025IFSSHCongresstoCartagenadeIndias.InspiteofexcellentpresentationsbyDr.RezendeandDr.Naquira,theAmericanbidprevailed.The202515thTriennialIFSSHCongresswillbeheldinWashingtonDC,USAfromMarch29toApril3.TheIFSSHisveryindebtedtotheAmerican,BrazilianandColombianSocietiesfortheirdedicationtothecreationofextraordinarybidsandsuperbpresentations.
Thisyear’sinvitedSwansonLecturerwasDr.StevenHoviuswhoprovidedaninsightfulandthought-provokingdiscussionofthechallengesfacinghandsurgeonsaroundtheworldastheytrytoprovidethebestcaretotheirpatients.ThePresidentialGuestLecturewasdeliveredbyProfessorDr.KlausLeisinger,raisingtheinterestofparticipantswithhisthoughtson“Criticalissuesforaworldwewant:Whatdoweknow?Whatshallwedo?Whatmaywehope?”
Ofcourse,everyIFSSHCongressprovidesopportunitiesforsocialinteractionbetweenthemembersofourmembersocieties.TheGermansocietyorganizeda“BerlinNight”atarenovatedcoldstoragefacility(TheKühlhaus)datingbacktotheearly20thcentury.HighpoweredmusicfilledtheairwhileattendeesdancedandenjoyediconicGermanfoodanddrink.TheGaladinnerwasheldonThursdaynightattheRitz-Carltonandfeaturedgreatfoodanddrinkaswellasanoutstandingbandthatkepthandsurgeonsandtherapistsdancingintotheweehoursofthemorning.
Onceagain,manythankstotheGermanSocietyforHandSurgery,GermanSocietyforHandTherapy,FederationofEuropeanSocietiesforSurgeryoftheHandandtheInternationalFederationofSocietiesforHandTherapyforputtingonatrulyextraordinaryCongress,Bravo!
Best wishes to all. Dan
Daniel Nagle
President Elect, IFSSH
SECRETARY-GENERAL REPORT
MESSAGE FROM OUTGOING SECRETARY-GENERAL: DANIEL NAGLE
6 7
August 2019www.ifssh.info

PIONEER PROFILES
StewartH.Harrisonwasbornon 15 July 1912 in Highgate, London, UK. Both parents died when he was still a pre-schooler.Hewasbroughtupbyhismaternalgrandparentsin Dunblane, Scotland, andattended Stanley House SchoolinBridgeofAllan.
In1934hequalifiedinDentistryandin1935inMedicineattheEdinburghUniversity,Scotland.HeobtainedhisFRCSfromEdinburghin1938.
During the SecondWorldWar, he served asMajor inthe Royal Army Medical Corps, stationed in Nigeriaand later in north-west Europe. Following the war, he worked at the Birmingham Accident Hospital, training under Sir Harold Gillies. In 1958 he worked with RainsfordMowlemattheMountVernonHospitalwherehedevelopedanumberofoperations,amongstothersthe techniqueofdelayedprimaryflexor tendongraftsforflexortendoninjuries.Hisplasticandreconstructivesurgery background saw him promoting the novelconceptofprimaryflapcoverofopenlowerleginjuriesby cross leg flaps. This new technique drasticallyreduced the infection rate.Thesecross legflapshavenowbeenreplacedbymicro-vascularfreeflaps,buttheprinciple stays the same.
Another of his pioneering contributions waspollicisation for the Thalidomide cases, tendontransfers as a prophylactic procedure to prevent thedeformingcycleoftherheumatoidwrist,andearlyPIP
joint fusion with his newly developed polypropyleneintramedullary pegs. In 1979 Harrison was appointed the Hunterian Professor for his contribution to thetreatmentoftherheumatoidhand.Healsowrotearticleson thesurgicalmanagementofburninjuries,cranio-facialreconstructionandchronicinfectionoftheaxilla.
In1956StewartHarrison,AdrianFlatt,RobertRobbins,Douglas Reid and Graham Stack started the SecondHandClub,whichunlike the FirstHandClub, had anopenmembership!ThetwoHandClubsjoinedtogetherin1968tobecometheBritishSocietyforSurgeryoftheHand. He served as President in 1972. In 1976 he was electedPresident of theBritishAssociationofPlasticSurgeons.
Hislast5yearsofretirementwasspentinSpainwherehediedon12May2011attheageof98years.Stewart Harrison was married to Phyllis Eustace in 1942, and they have one son.
AtTheEighthCongressoftheInternationalFederationofSocietiesforSurgeryoftheHandinIstanbul,Turkey,10 June 2001, Stewart H. Harrison was honoured as “PioneerofHandSurgery”.
PIONEER PROFILES
Hanno Millesi was born on24 March 1927, the son of ageneral practioner in Villach, Carinthia, Austria. In 1951, he received his medical degree from the Universityof InnsbruckMedicalSchool.He then trained in pathology and internal medicine at the Wilhelminen Hospital in
Vienna, and in general surgery and plastic surgery at the 1stSurgicalClinic,UniversityofViennaMedicalSchool.He studied with Dr. Alan Ragnell at the StockholmSurgical Hospital, Sweden. In 1967 he obtained hispostdoctoral qualification based on extensive researchonthepathogenesesofDupuytren’scontracture. Millesi was appointed Head of the Section of PlasticSurgery,1stSurgicalClinic,UniversityofViennaMedicalSchool and Associate Professor of Plastic Surgery in1972.HewasProfessorofPlasticSurgeryattheViennaUniversityMedicalSchoolfrom1982until1995,whenhebecameProfessorEmeritus.In1974hefoundedthefirst24-hour replantation service in Europe with colleagues frombothSurgicalUniversityClinicsinVienna.HewasappointedDirectoroftheLudwig-BoltzmannInstituteforExperimentalPlasticSurgery,Vienna(1975),andHeadofthenewPlasticandReconstructiveSurgeryClinicoftheUniversityofVienna(1993).InJanuary1996,hebecameMedicalDirectoroftheViennaPrivateHospital. He authored or edited 20 textbooks and over 320scientific publications on his areas of study, includingthepathogenesisofDupuytren’scontracture;mechanicalpropertiesofpalmaraponeurosis,tendon,skin,andscartissue; biomechanical properties of elastase; healingof nerves; gliding apparatus of peripheral nerves;
microsurgery of peripheral nerves; interfasiculargraftingofmedianandulnarnerves,andnervegraftingofthebrachialplexus. He was a member of 21 scientific societies includingthe Austrian Society for Surgery of the Hand, and theAmerican,British,French,Italian,Spanish,Venezuelan,and Turkish Hand Societies, and the International College of Surgeons. He was FoundingMember and Presidentof the Austrian Society of Plastic Surgery (1971-75),International Society of Reconstructive Microsurgery(1972-73), GermanSpeakingStudyGroup onPeripheralNervesandVessels (1978-82), and theAustrianSocietyforSurgeryof theHand(1989-96). HewasPresidentofthe Sunderland Society (1985-86) and the InternationalCollege of Surgeons-Austrian Section (1985-1998), andmember of the Executive Council of the InternationalConfederationforPlastic,ReconstructiveandAestheticSurgery(1987-95). Prof.Millesihasreceivednumeroushonoursandawards,amongst others: Hoechst (1967), Eiselsberg (1972) andGerman Society of Surgery Jubilee (1974) prizes. GoldMedals from the Italian Club of Microsurgery (1980)andthecitiesofVienna(1987)andMilan(1988),DoctorHonoris Causa University of Breslau, Poland (1980),Commandant of the Italian Republic (1982), AustrianGoldenAwardforScienceandResearch(1995).HegavetheMoberg (1973),Kazanjian (1975) andASSHFounder(1987)Lectures. Attheageof90years,HannoMillesipassedawayon28April 2017 in Viena, Austria. In May1998, Prof.Dr.HannoMillesiwashonouredas”Pioneer ofHandSurgery” by the IFSSHat its SeventhInternational Congress in Vancouver, B.C., Canada
STEWART H. HARRISON LDS, RCS (Edinburgh), FRCS (England)United Kingdom (1912 - 2011)
HANNO MILLESI MDAustria (1927 - 2017)
8 9
August 2019www.ifssh.info
COMMITTEE REPORTS
Reports from IFSSH affiliated OrganisationsASIAN-PACIFIC FEDERATION OF SOCIETIES FOR SURGERY OF THE HAND (APFSSH) 2019 REPORT
19th June 2019, Goo Hyun Baek
Current Member Societies (13)Australian Hand Surgery SocietyBangladeshSocietyforSurgeryoftheHandHongKongSocietyforSurgeryoftheHandIndianSocietyforSurgeryoftheHandIndonesianSocietyforSurgeryoftheHandJapaneseSocietyforSurgeryoftheHandKoreanSocietyforSurgeryoftheHandMalaysianSocietyforSurgeryoftheHandNewZealandSocietyforSurgeryoftheHandAssociationofHandSurgeonsforthePhilippinesSingaporeSocietyforHandSurgeryTaiwanSocietyforSurgeryoftheHandThaiSocietyforSurgeryoftheHand Observer Societies (5)ChinaSocietyforSurgeryoftheHandMyanmarSocietyforSurgeryoftheHandPakistanSocietyforSurgeryoftheHandVietnamSocietyforSurgeryoftheHandSriLankaSocietyforSurgeryoftheHand APFSSH Executive CommitteePresident:GooHyunBaek(Korea)President-Elect:RajaSabapathy(India)GeneralSecretary:TonyBerger(Australia)GeneralSecretary-Elect:FuminoriKanaya(Japan)ImmediatePastPresident:Yuan-KunTu(Taiwan)
Official Journal of APFSSH‘TheJournalofHandSurgeryAsian-PacificVolume’since 1996Published4issues(Mar,June,Sep,Dec) APFSSH Congresses11thAPFSSHMeeting:CebuCity,Philippines(7th-10thOctober,2017)12thAPFSSHMeeting,Melbourne,Australia(9th-11thMarch,2020)13thAPFSSHMeeting,Singapore(May,2023)
This past year has seen many developments in the activitiesoftheAPFSSH.ManyoftheoriginalaimsofthefirstCharteroftheAPFSSHbeingtopromoteHandSurgeryandEducationintheRegionandtosupportaTravellingFellowshiphavebeensomewhathamperedbyalackoffundsanddifficultiesincoordinatingactivitiesthroughouttheregionundertheumbrellaoftheAPFSSH.Allthemembersocietiesareveryactiveintheirowncountriesandhavefrequentcombinedscientificmeetings.TheFederationhassomefundsbutthesearebeingheldbymembersocietiesfromdonationsandfromtherunningofourscientificmeetings.InordertoincreasetheactivityoftheFederationtheexecutivehasoverthepast2yearsbeenworkingtowardsestablishinganofficeandabankaccountwherefundscanbecollectedandthenusedtoachievetheaimsoftheFederation.WithsomanydifferingcountriesandlawsintheregionthisprovedtobealittledifficultbutwiththeworkofourSingaporeancolleaguesweareonthethresholdof
opening an account and having an administrative baseinSingapore.InordertosatisfythefinancialrequirementsofSingaporeithasalsobeennecessarytoestablishaproperConstitution.ThishasbeenamonumentaltaskwithusefulcontributionsfrommanymembersofourFederation.TheConstitutionwasvotedonandadoptedbytheexecutiveandmemberdelegatesat a Council meeting in Taiwan last month. With a fewdetailstocompleteoverthenextfewmonthstheFederationwillsoonbeabletoachieveitsaimsintheregion. TheJournalofHandSurgeryAsianPacificVolume,istheofficialjournaloftheAPFSSHwhichispublished4timesayear.181articlesaresubmittedin2018,andacceptance rate was 36%. TheFederationwebsiteisalsoundergoingaredevelopmentandwiththeincreasedactivityoftheFederationwehopetoencouragemorecontributionstothewebsitewithmeetingannouncementsandothereducational activities. With the Constitutional work completed the attention oftheFederationisnowdirectedtowardsthenextAPFSSHmeetingtobeheldinMelbourneAustraliainMarch2020.Thisisco-convenedbytheAustralianand New Zealand Hand Surgery Societies and the AsianPacificWristAssociation.ItisagainheldinconjunctionwiththeAPFSHTwithmanycombinedsessions. We are also trying to support registrations fromhandsurgerysocietiesfromdevelopingnationsinourregionbyofferingreducedregistrationratesandraisingfundsfromotherregistrationstofurthersupportattendeesfromthesemembersocieties. WhilstMelbournemaybefartotravelforsomeMembers,Iwouldliketoencourageasmanyofyouaspossibletoattend.Iamsurethetripwillbeworthwhile.
HAND AND WRIST BIOMECHANICS INTERNATIONAL (HWBI)
www.hwbi.org
Thehandandwristrepresentoneofthemostchallengingstructuresinthestudyofbiomechanics,aswellasintheevaluationofmanybiomechanicalprinciples.Handandwristbiomechanicshasbeensomewhatunderdevelopedincomparisontomainstreambiomechanicsresearchoverthepastcentury.Whilenumerousbiomechanicalstudieshavebeeninitiatedbysurgeonsandengineers,collaborativeeffortsamongscientistsandcliniciansarerequiredinorderforcontinuingprogressioninresearchandfurtherimprovementoftreatmentmodalitiesandoutcomes.
For over 25 years, the International Symposia on Hand and Wrist Biomechanics have provided the opportunityforglobalscientificexchangeandmutualencouragementamongbasicscienceandclinicalinvestigators. In 2012, the International Advisory BoarddecidedtoformHandandWristBiomechanicsInternational(HWBI)tofurtherenhancethedevelopmentofhandandwristbiomechanicsanditsclinical applications. It is our hope that through the structuredorganizationofHWBI,researchactivitiesrelatedtohandandwristbiomechanicswillbeelevatedandclinicaltranslationwillbeimproved.
HWBIisaffiliatedwithInternationalFederationofSocietiesforSurgeryoftheHand(IFSSH)andtheInternationalSocietyofBiomechanics(ISB).Withtheseaffiliations,theHWBIbenefitsfromIFSSH’sandISB’sestablishedexcellenceaspremierinternationalorganizationsandtheirvastumbrellanetworksinpromotingbasicscienceandclinicalapplications.Inturn,theHWBIcontributesitsspecialtyknowledgetothebroadfieldsofhandsurgeryandbiomechanics.HWBIregularlyorganizessymposiainconjunctionwith IFSSH and ISB congresses.
COMMITTEE REPORTS
10 11
August 2019www.ifssh.info
COMMITTEE REPORTS COMMITTEE REPORTS
IFSHT REPORT TO IFSSH EXECUTIVE COMMITTEE MEETING
17JUNE2019.AnneWajon,PresidentIFSHTCityCube,Berlin
IFSHT PRESIDENT ACTIVITIES 2016-2019• Hosted IFSHT EXCO interim meeting in Hong Kong,
2017topreparegoalsforcurrentterm• Approved and appointed an administrative
assistant• FinalisedadjustmentofIFSHTmembershipfeesto
bemoreequitableandsustainable,effective• January 2020• DeletedtheCommercialmembershipcategory(to
bevotedonatCouncilmeeting)• RewrotetheIFSHTcontracttemplateforfuture
congresses,andupdatedsignedagreementsfor• Berlin 2019 and London 2022• RepresentedIFSHTatEurohand2017,ASHT2017
and 2018, APFSHT 2017, EFSHT 2018• Attended site visit in Berlin, 17-19 June 2018, in
preparationfor2019Congress• Continuetoupdatewebsitecontent,including
offeringonlineapplicationsformembership,awardsandgrants,aswellasinformingmembersofonlineresourcesandeducationalopportunities.
IFSHT TRIENNIAL MEETINGS11th IFSHT Triennial Congress / 14th IFSSH Triennial Congress, 2019 Berlin, Germany• 30-year IFSHT anniversary – goniometers
purchasedascelebratorykeep-sake• InauguralpresentationofLifetimeAchievement
award• WorkedwithourinternationalCo-chairsof
theScientificProgramtoensurehighqualityworkshops and papers at Congress
12th IFSHT Triennial Congress / 15th IFSSH Triennial Congress, 2022 London, UK• Websiteaddressupdatedtoifssh-ifsht2022.com.• NicolaGoldsmith(President-elect)workingwith
BAHTandIFSSHaftercompletionofBerlin2019.
13th IFSHT Triennial Congress / 16th IFSSH Triennial Congress, 2025• Receivedbids:Delegateswillbevotingon
combinedASSH/AAHS/ASHTinWashington• DC, ASOCIMANO/ASCOTEMA in Cartagena,
ColumbiaandfromSBCM/SBTMRiode• Janeiro,Brazil.
IFSHT MEMBERSHIP• Fullmembers:37,representingmorethan9500
hand therapists worldwide. Greece reinstated• Associatemembers:Bangladesh,Mexico,Nepal,
Philippines, Qatar, Singapore, Thailand, and United ArabEmirates.
• Correspondingmembers:Bahrain,Barbados,Gaza,Ghana,Iran,Malta,Romania,SaudiArabia,SriLankaandZimbabwe.
Regional Liaison Organisations: American Association forHandSurgery(AAHS),AsiaPacificFederationofSocietiesforHandTherapy(APFSHT),EuropeanFederationofSocietiesforHandTherapy(EFSSH),InternationalFederationofSocietiesforSurgeryoftheHAND(IFSSH)andInternationalSocietyforSportTraumatologyoftheHand(ISSPORTH)andSouthAmericanSocietyHandTherapy(SSTM).
COMMUNICATIONWithin IFSHT:- Executive committee:• Continue to chair regular Skype-call meetings, and
useTeamworksasourvirtualoffice• Havebeenworkingcloselywithsecretarygeneral
to ensure goals achieved and queries addressed.• Preparedthebudgetfor2019-2022,allocatingfunds
formajorwebsiteupdate
- Committee activity:• Educationcommittee:hascompletedasurveyof
fullmembersinvestigatingsocietyactivities,andalsoaskedassociate/correspondingmembersfortheir needs to aid development
• Ad Hoc Social Media Committee has posted updatesaboutIFSHTandtheCongressinBerlin
• By-laws Committee has made some updates, especiallytoreflectdeletionofcommercialmembershipcategory
• Translation committee: now translating IFSHT Update into Japanese and Spanish.
- Delegate communication:• Delegatescontinuetoreceiveregularupdatesfrom
the IFSHT Secretary General and vote electronically in IFSHT elections.
With Hand Therapists around the world:• IFSHTUpdate:published4xannuallyintheUS
andtheBritishJournalsofHandTherapyanddistributedtoallmembercountries.NowincludedintheIFSSHEzine.
• IFSHTwebsite(www.ifsht.org):Continuetoregularlyupdatewebsitewithnewfeaturesandcontent.Over300requestsforhandtherapyinformation,education,internationalreferralforpatient care received over last three years.
• IFSHT Hand Therapy Connections E-Newsletter: 2x peryear.Currently,1937subscribers.
• IFSHTFacebook:remainsactiveIFSHTcontributiontoIFSSHE-zine:IFSHThascontinued to source and prepare a short clinically relevantarticlefortheIFSSHEzine.RecenttopicsincludesplintingforthumbMPjointhypermobility.
IFSHT AWARDS AND SPONSORSHIP ACTIVITY
-EvelynMackinAward:sponsorshipofatherapist(s)fromadevelopingcountrytoattendtriennialcongress.In2019,IFSHTfullysupportedfourtherapiststoattendthecongress.TherapistswerefromBhutan,Zimbabwe,EstoniaandPoland.IFSHThas
bookedandpaidforflights,accommodationandregistrationinfull.
- IFSSH/IFSHT Triennial Congress Travel Grant: Eighteenapplicantsreceivedfundstosupport,registration, accommodation and/or travel. Funds were distributedbasedonguidelines,specificallyforcountrieswithlowGDP,forassociatememberswhohadnotattendedtheCongresspreviously,withfundsfromthe2016SilentAuctionspecificallyusedtosupport speakers and poster presenters.
- IFSHT-IFSSH International Hand Therapy Teaching Awards. During this term, grants madeavailabletosupporttherapiststeachinghandtherapyin less-developed countries have increased to$US1500. Four applications were received and support offeredto:• JaneFedorczyk(USA)travelledtoRwandainApril
2018(fundsnotrequired)• JennyBall(Australia)travelledtoNepalinMay
2018• MerylGlover(UK)travelledtoMalawiinOctober
2018• ShrikantChinchalkar(Canada)travelledtoSri
LankainFebruary2019
-CristinaAlegriAwardforInnovationinHandTherapywillbeawardedatcloseofinnovationsessionon Friday. Eight worthy nominations were received.
-TheinauguralIFSHTLifetimeAchievementAwardwillbeawardedin2019tohonorthosewhohavemadeaglobalimpactonprofessionofhandtherapy. 13 recipients will receive award at IFSHTopening ceremony on Tuesday 18 June.
-Dynamometers:~15available.SinceJune2018,deliveredtoNepal,Bolivia,Tanzania,Rwanda,Zimbabwe,India,Vietnam,Malawi,Argentina,Kathmandubyvisitingtherapists.
12 13
August 2019www.ifssh.info

SPECIAL FEATURE
Outcome measurement in hand surgery
This article provides an overview on why and how data can help to improve high-quality patient care inhandsurgery.Itsummarizesthemostcommonpatient-reportedoutcomemeasures(PROMs)thatcanbeusedindailypracticeandforstudies.Furthermore,itfocusesonhowtointerpretPROMsdataandshowsthat several clinically relevant interpretation methods areavailable,regardlessofthestatisticalp-value.
Why outcome measures? Without measuring treatment outcome, we can neither improve our hand surgical interventions nordemonstratetheireffectiveness.Althoughsomeinterventionshavebeenproveneffectiveandsafefora certain patient population, this does not necessarily
meantheycanbeappliedtopatientsinanotherclinicalsetting.Therefore,standardizeddocumentationofoutcomesisessentialnotonlyinstudies,butalsoin clinical routine. For the latter, documentation is bestrealizedusingregistries.Largeregistriesinhandsurgery are rare. Unlike in orthopedics, where such registries have a long tradition, hand surgical data are onlynowbeingcollectedonlargerscalesinasmallnumberofcountries.
Thesebigdatabasesarerequiredtogainmoreevidenceaboutinterventionsthatisstatisticallysoundandrepresentsareal-worldsetting.Registrydatamaybeconsideredadvantageousoverresultsstemmingfromindividual and somewhat restricted clinical trials.
SPECIAL FEATURE
Table 1: Most common and validated PROMs for patients with hand conditions
Name Target population No of items Domains Pros / Cons
MHQ3-10 All hand conditions 37 items Six subscales: overall hand function, activities of Pros: Good measurement properties, scores both hands separately, subscales can be scored individually
daily living, pain, work performance, aesthetics, Cons: Quite long
satisfaction
Brief MHQ8,11-13 All hand conditions 12 items Six domains: overall hand function, activities of Pros: Good measurement properties, short
daily living, pain, work performance, aesthetics, Cons: Subscales cannot be scored individually
satisfaction
URAM14-16 Dupuytren’s disease 9 items One domain measuring functional disability of Pros: Good measurement properties, specific for patients with Dupuytren’s disease, short
patients with Dupuytren’s disease Cons: Not suitable for other hand conditions
BCTQ / Levine Carpal tunnel 19 items Two subscales: symptom severity scale, functional Pros: Specific for CTS, good measurement properties
Scale17-19 syndrome (CTS) status scale Cons: Not suitable for other hand disorders, potential item redundancy
Overall,outcomemeasurementshelptoquantifypatientbenefitandtheeffectofanewinterventioncomparedtoestablishedprocedures.Theycanalsohelpinidentifyingremainingdeficitsafterinterventions as well as the associated socio-economic consequences. In the modern world with its increasing healthcosts,outcomemeasuredatacanformthebasisfornegotiationswithhealthauthorities.Ultimately,wewouldalsoliketoknowjusthowourpatientsarereallydoing.
Most commonly used patient-reported outcome measures (PROMs) Awidevarietyofoutcomemeasuresareavailableforassessinghandconditions.Aliteraturereviewanalyzingaseriesofstudiesfocusedontreatmentfortrapeziometacarpalosteoarthritis,forexample,revealedthattherewere21differentquestionnairesinuse.1SimilarfindingshavebeenreportedforDupuytrenstudies,wherebyonly14%usedvalidatedPROMs2. The diversityinreportingoutcomesmakesitdifficulttocompareresultsbetweenstudies.Table1highlightsthemostcommonandvalidatedPROMsforpatientswithdifferenthandconditions.
TheDisabilitiesoftheArm,ShoulderandHandquestionnaire(DASH)oritsshortenedform,thequickDASH24,25ismissinghere.Why?TheDASHisstillthe
most commonly used questionnaire in hand surgery, and several studies attest to its good measurement properties26-29. BUT: The DASH is intended to measure functionoftheentireupperextremityandnotjustthe hand. The questionnaire contains items relevant toshoulderandelbowfunctionthatsignificantlyinfluencethetotalscore.Therefore,itisrecommendedtouseahand-specificquestionnairefortheprimaryevaluationofhandsurgicalprocedures.TheDASHmightstillhaveitsplace,forexample,inmorecomplexdisease patterns such as rheumatoid arthritis, where thewholeupperextremityisinvolvedandtheeffectofasingleinterventiononglobalfunctionrequiresevaluation.
Core setsOutcomemeasuresshouldcoveralldomainsofinteresttocomprehensivelyassessthehealthstatusofapatient.Forexample,thedimensionsofobjectivedata(clinicalmeasures,radiologicalcriteria),functionaloutcome(handandextremityspecific)andpatient-ratedsubjectivedata(qualityoflife,functionandpain)togetherwithsocio-economicdataandcomorbiditiesareofinterest.Thisimpliestheuseofmanydifferentoutcomemeasuretools,whichmaycontributetoahighadministrativeburdenforboththehealth-careproviderandpatient.Ifavailable,coresetsassessingthe clinical and patient-reported outcomes as well
MHQ=MichiganHandOutcomesQuestionnaire;URAM=UnitéRhumatologiquedesAffectionsdelaMain(URAM)scale;BCTQ=BostonCarpalTunnelQuestionnaire;PRWE=PatientRatedWristEvaluation
“If you can’t measure it, you can’t improve it” - P. Drucker
14 15
August 2019www.ifssh.info
SPECIAL FEATURE SPECIAL FEATURE
ascomplicationsshouldbeused,suchasthealreadyestablishedcoresetsforassessingpatientswithdistalradiusfractures30orhandosteoarthritis(OA)31.
Somerecentprojectsareconcentratingontheestablishmentofaminimaldatasettoevaluatesubjectiveoutcomewithonlyasmallnumberofrelevantquestions.Inthefieldsofthelowerandupperextremity as well as spine surgery, this approach has provensuccessful.A6-item“CoreOutcomeMeasuresIndex”questionnairedevelopedforpatientswithspine, hip and knee disorders32-34 and the 1-item “Single AssessmentNumericEvaluation”toolforpatientswithshoulder disorders35bothcompriseaminimaldatasetthatdeliversusefulinformationonthetreatmentoutcomes. Such a short, multidimensional tool could alsobeappliedinhandsurgery.Itcouldevenserveasapreoperative evaluation tool to determine the patient’s needs and expectations, which may in turn help to improvetheindicationqualityfordifferenttherapyoptions.
Statistical versus clinical significance Theinterpretationofstudyresultsistraditionallybasedonstatisticalsignificance.However,astatisticallysignificanttreatmenteffectdoesnotnecessarilyequatetoameaningfuloutcomeforthepatient36,37.Thepatient’sperceptionofatreatmenteffectisimportantandshouldbeconsideredineveryinstanceofclinicalcare.
“Basedonthep-value≤0.05,weconcludethatourtreatmentwaseffective”.Inresearcharticles,weoftenencounterthiskindofstatement.However,isthisstatisticaleffectivenessdirectlyrelatedtothatperceivedbythepatientsthemselves?Toanswerthis question, one should take a closer look at the characteristicsofp-values.TheAmericanStatisticalAssociation(ASA)highlightsthecommonissueswithp-value.Asmallp-valueofteninducesaninappropriateconclusionthatalargetreatmenteffectwasachieved36. However,ap-valueprovidesneitheradirectmeasureofthemagnitudeofatreatmenteffectnordescribesthe
importanceoftheresults.Thecalculationofap-valueisbasedonthesamplesize.Thelargerthesamplesize,the more likely a statistical analysis will result in a “significant”p-valueregardlessofwhethertherewasonlyasmalltreatmenteffect.Incontrast,“significance”mayprobablynotbeattainedwithasmallsamplesize,althoughalargetreatmenteffectisapparent36.Therefore,alternativeinterpretationsoftreatmenteffectsbasedonclinicalrelevancehavebecomeincreasingly popular38,39. There are three underlying concepts that measure this aspect:
1. Minimal Important Change (MIC) Theminimalimportantchange(MIC)isthesmallestchange in a score, which patients perceive as important. This outcome considers any change within a single group or patient40,41, and changes exceeding theMICcanbeconsideredrelevantforthepatient42.A related term known as the minimal clinically importantdifference(MCID)isalsowidelydescribedintheliterature.SeveralstudiesdefinedtheMICforvarious outcome measures in hand surgery13,43-48;forexample,theMICfortheMichiganHandOutcomesQuestionnaire(MHQ)is11points47.
2. Minimal Important Difference (MID) Theminimalimportantdifference(MID)isthesmallestdifferencebetweenpatientsorpatientgroupsthatisconsidered important40,41. In hand surgery, the MID has onlybeencharacterizedfortheUnitéRhumatologiquedesAffectionsdelaMain(URAM)scaleinpatientswith Dupuytren’s disease and is 8 points44.
3. Patient acceptable symptom state (PASS) Thepatientacceptablesymptomstate(PASS)isthevaluebeyondwhichpatientsconsiderthemselveswell49.ThisvaluehasbeendeterminedforthequickDASHinpatientsaftercarpaltunneldecompression(PASS≤34)27. In patients with hand osteoarthritis, PASSvaluesaredefinedfortheAustralian/Canadian(AUSCAN)HandOsteoarthritisIndex(PASS≤43)50, pain numericratingscale(PASS≤1-5-4.1)12,51andthebriefMHQ(PASS≥64)12.
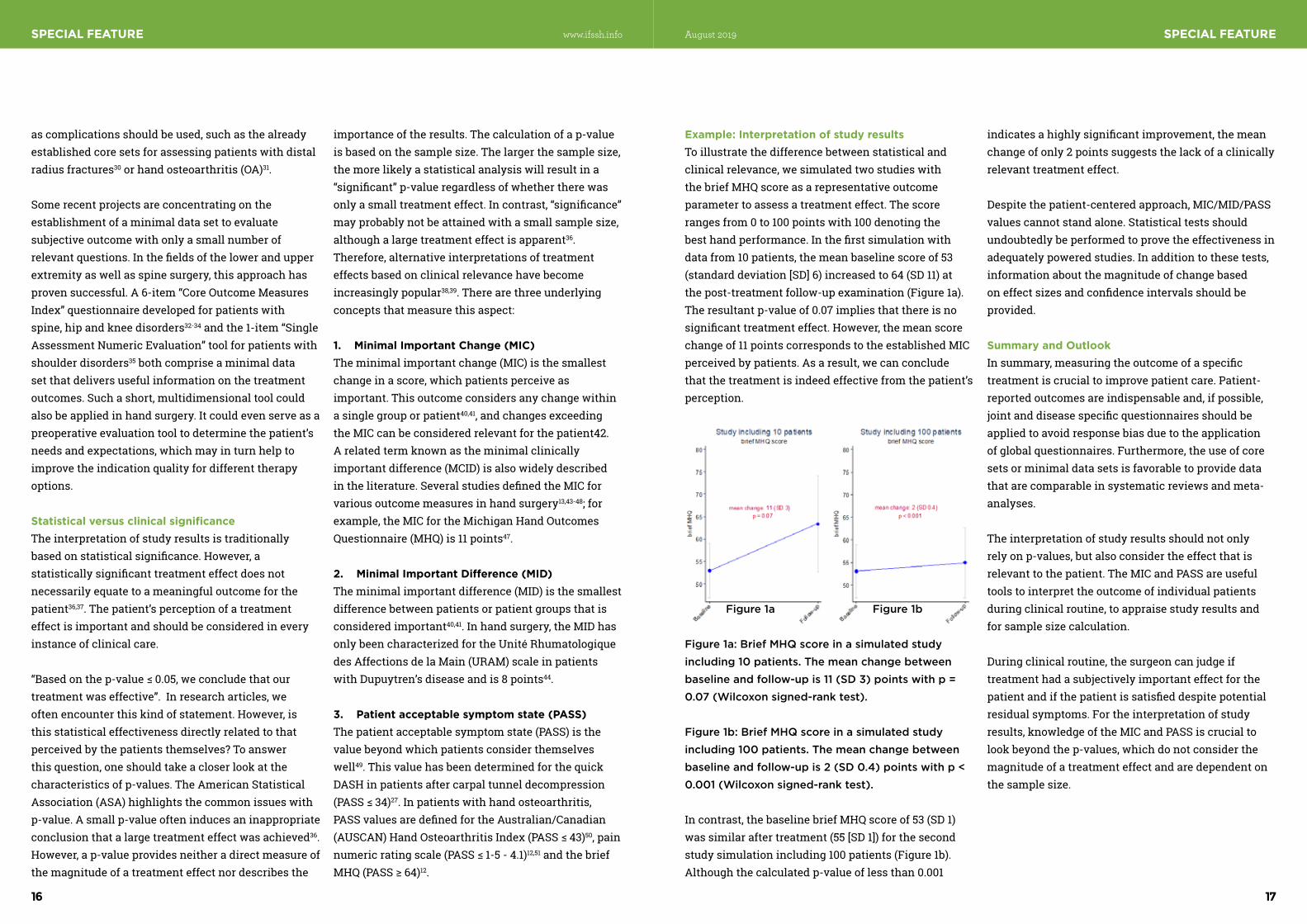
Example: Interpretation of study results Toillustratethedifferencebetweenstatisticalandclinical relevance, we simulated two studies with thebriefMHQscoreasarepresentativeoutcomeparametertoassessatreatmenteffect.Thescorerangesfrom0to100pointswith100denotingthebesthandperformance.Inthefirstsimulationwithdatafrom10patients,themeanbaselinescoreof53(standarddeviation[SD]6)increasedto64(SD11)atthepost-treatmentfollow-upexamination(Figure1a).Theresultantp-valueof0.07impliesthatthereisnosignificanttreatmenteffect.However,themeanscorechangeof11pointscorrespondstotheestablishedMICperceivedbypatients.Asaresult,wecanconcludethatthetreatmentisindeedeffectivefromthepatient’sperception.
Incontrast,thebaselinebriefMHQscoreof53(SD1)wassimilaraftertreatment(55[SD1])forthesecondstudysimulationincluding100patients(Figure1b).Althoughthecalculatedp-valueoflessthan0.001
indicatesahighlysignificantimprovement,themeanchangeofonly2pointssuggeststhelackofaclinicallyrelevanttreatmenteffect.
Despite the patient-centered approach, MIC/MID/PASS values cannot stand alone. Statistical tests should undoubtedlybeperformedtoprovetheeffectivenessinadequately powered studies. In addition to these tests, informationaboutthemagnitudeofchangebasedoneffectsizesandconfidenceintervalsshouldbeprovided.
Summary and Outlook Insummary,measuringtheoutcomeofaspecifictreatment is crucial to improve patient care. Patient-reportedoutcomesareindispensableand,ifpossible,jointanddiseasespecificquestionnairesshouldbeappliedtoavoidresponsebiasduetotheapplicationofglobalquestionnaires.Furthermore,theuseofcoresetsorminimaldatasetsisfavorabletoprovidedatathatarecomparableinsystematicreviewsandmeta-analyses.
Theinterpretationofstudyresultsshouldnotonlyrelyonp-values,butalsoconsidertheeffectthatisrelevanttothepatient.TheMICandPASSareusefultoolstointerprettheoutcomeofindividualpatientsduring clinical routine, to appraise study results and forsamplesizecalculation.
Duringclinicalroutine,thesurgeoncanjudgeiftreatmenthadasubjectivelyimportanteffectforthepatientandifthepatientissatisfieddespitepotentialresidualsymptoms.Fortheinterpretationofstudyresults,knowledgeoftheMICandPASSiscrucialtolookbeyondthep-values,whichdonotconsiderthemagnitudeofatreatmenteffectandaredependentonthesamplesize.
Figure 1a: Brief MHQ score in a simulated study including 10 patients. The mean change between baseline and follow-up is 11 (SD 3) points with p = 0.07 (Wilcoxon signed-rank test).
Figure 1b: Brief MHQ score in a simulated study including 100 patients. The mean change between baseline and follow-up is 2 (SD 0.4) points with p < 0.001 (Wilcoxon signed-rank test).
Figure 1a Figure 1b
16 17
August 2019www.ifssh.info
SPECIAL FEATURE SPECIAL FEATURE
References 1. Marks M, Schoones JW, Kolling C, Herren DB,
Goldhahn J, Vliet Vlieland TPM. Outcome measuresandtheirmeasurementpropertiesfortrapeziometacarpalosteoarthritis:asystematicliteraturereview.JHandSurgEurVol.2013;38:822- 838.
2. BallC,PrattAL,NanchahalJ.OptimalfunctionaloutcomemeasuresforassessingtreatmentforDupuytren’s disease: a systematic review and recommendationsforfuturepractice.BMCMusculoskeletDisord.2013;14:131.
3. ChungKC,PillsburyMS,WaltersMR,HaywardRA.ReliabilityandvaliditytestingoftheMichiganHand Outcomes Questionnaire. J Hand Surg Am. 1998;23:575-587.
4. MarksM,AudigéL,HerrenDB,SchindeleS,NelissenRG,VlietVlielandTP.MeasurementpropertiesoftheGermanMichiganHandOutcomesQuestionnaireinpatientswithtrapeziometacarpalosteoarthritis.ArthritisCareRes(Hoboken).2014;66:245-252.
5. KroonFPB,BoersmaA,BoonenAetal.PerformanceoftheMichiganHandOutcomesQuestionnairein hand osteoarthritis. Osteoarthritis Cartilage. 2018;26:1627-1635.
6. ChungBT,MorrisSF.Reliabilityandinternalvalidityofthemichiganhandquestionnaire.AnnPlastSurg.2014;73:385-389.
7. Shauver MJ, Chung KC. The Michigan Hand OutcomesQuestionnaireafter15yearsoffieldtrial.PlastReconstrSurg.2013;131:779e-787e.
8. BusuiocSA,KarimM,EfanovJIetal.TheMichiganHandQuestionnaireandBriefMichiganHand
QuestionnaireweresuccessfullytranslatedtoCanadianFrench.JHandTher.2018;31:564-567.
9. WaljeeJF,ChungKC,KimHMetal.ValidityandresponsivenessoftheMichiganHandQuestionnaire in patients with rheumatoid arthritis: a multicenter, international study. ArthritisCareRes(Hoboken).2010;62:1569-1577.
10. Nolte MT, Shauver MJ, Chung KC. Normative Values oftheMichiganHandOutcomesQuestionnaireforPatients with and without Hand Conditions. Plast ReconstrSurg.2017;140:425e-433e.
11. WaljeeJF,KimHM,BurnsPB,ChungKC.Developmentofabrief,12-itemversionoftheMichiganHandQuestionnaire.PlastReconstrSurg.2011;128:208-220.
12. Marks M, Hensler S, Wehrli M, Schindele S, Herren DB. Minimal important change and patient acceptablesymptomstateforpatientsafterproximalinterphalangealjointarthroplasty.JHandSurgEurVol.2019;44:175-180.
13. Wehrli M, Hensler S, Schindele S, Herren DB, Marks M.MeasurementPropertiesoftheBriefMichiganHand Outcomes Questionnaire in Patients With Dupuytren Contracture. J Hand Surg Am. 2016;41:896-902.
14. BeaudreuilJ,AllardA,ZerkakDetal.UnitéRhumatologiquedesAffectionsdelaMain(URAM)scale:developmentandvalidationofatooltoassessDupuytren’sdisease-specificdisability.ArthritisCareRes(Hoboken).2011;63:1448-1455.
15. BernabéB,LasbleizS,GerberRAetal.URAMscaleforfunctionalassessmentinDupuytren’sdisease:acomparativestudyofitsproperties.JointBone
Spine.2014;81:441-444.16. 16.RodriguesJN,ZhangW,ScammellBE,Davis
TR.WhatpatientswantfromthetreatmentofDupuytren’sdisease--istheUniteRhumatologiquedesAffectionsdelaMain(URAM)scalerelevant?JHandSurgEurVol.2015;40:150-154.
17. Leite JC, Jerosch-Herold C, Song F. A systematic reviewofthepsychometricpropertiesoftheBostonCarpal Tunnel Questionnaire. BMC Musculoskelet Disord.2006;7:78.
18. LevineDW,SimmonsBP,KorisMJetal.Aself-administeredquestionnairefortheassessmentofseverityofsymptomsandfunctionalstatusincarpal tunnel syndrome. J Bone Joint Surg Am. 1993;75:1585-1592.
19. De Kleermaeker FGCM, Boogaarts HD, Meulstee J, Verhagen WIM. Minimal clinically important differencefortheBostonCarpalTunnelQuestionnaire:newinsightsandreviewofliterature.JHandSurgEurVol.2019;44:283-289.
20. MacDermidJC.ThePRWE/PRWHEupdate.JHandTher. 2019.
21. MehtaSP,MacDermidJC,RichardsonJ,MacIntyreNJ,GrewalR.Asystematicreviewofthemeasurementpropertiesofthepatient-ratedwristevaluation.JOrthopSportsPhysTher.2015;45:289-298.
22. Mulders MAM, Kleipool SC, Dingemans SA et al.NormativedataforthePatient-RatedWristEvaluationquestionnaire.JHandTher.2018;31:287-294.
23. MacDermidJC.Developmentofascaleforpatientratingofwristpainanddisability.JHandTher.1996;9:178-183.
24. HudakPL,AmadioPC,BombardierC.Developmentofanupperextremityoutcomemeasure:theDASH(disabilitiesofthearm,shoulderandhand)[corrected].TheUpperExtremityCollaborativeGroup(UECG).AmJIndMed.1996;29:602-608.
25. BeatonDE,WrightJG,KatzJN,UpperExtremityCollaborativeG.DevelopmentoftheQuickDASH:comparisonofthreeitem-reductionapproaches.JBoneJointSurgAm.2005;87:1038-1046.
26. RodriguesJ,ZhangW,ScammellBetal.ValidityoftheDisabilitiesoftheArm,ShoulderandHandpatient-reportedoutcomemeasure(DASH)andtheQuickdash when used in Dupuytren’s disease. J HandSurgEurVol.2016;41:589-599.
27. Clement ND, Duckworth AD, Jenkins PJ, McEachan JE.InterpretationoftheQuickDASHscoreafteropen carpal tunnel decompression: threshold valuesassociatedwithpatientsatisfaction.JHandSurgEurVol.2016;41:624-631.
28. Forget NJ, Jerosch-Herold C, Shepstone L, Higgins J.PsychometricevaluationoftheDisabilitiesoftheArm,ShoulderandHand(DASH)withDupuytren’scontracture:validityevidenceusingRaschmodeling.BMCMusculoskeletDisord.2014;15:361.
29. Kennedy CA, Beaton DE, Smith P et al. MeasurementpropertiesoftheQuickDASH(disabilitiesofthearm,shoulderandhand)outcomemeasureandcross-culturaladaptationsoftheQuickDASH:asystematicreview.QualLifeRes.2013;22:2509-2547.
30. Goldhahn J, Beaton D, Ladd A et al. Recommendationformeasuringclinicaloutcomeindistalradiusfractures:acoresetofdomainsforstandardizedreportinginclinicalpracticeandresearch.ArchOrthopTraumaSurg.2014;134:197-205.
31. KloppenburgM,BoyesenP,SmeetsWetal.ReportfromtheOMERACTHandOsteoarthritisSpecialInterestGroup:advancesandfutureresearchpriorities.JRheumatol.2014;41:810-818.
32. ImpellizzeriFM,MannionAF,NaalFD,LeunigM.ACoreOutcomeMeasuresIndex(COMI)forpatientsundergoing hip arthroplasty. J Arthroplasty. 2013;28:1681-1686.
33. ImpellizzeriFM,LeunigM,PreissS,GuggiT,MannionAF.TheuseoftheCoreOutcomeMeasuresIndex(COMI)inpatientsundergoingtotalkneereplacement.TheKnee.2017;24:372-379.
34. MannionAF,ElferingA,StaerkleRetal.Outcomeassessmentinlowbackpain:howlowcanyougo?EurSpineJ.2005;14:1014-1026.
35. WilliamsGN,GangelTJ,ArcieroRA,UhorchakJM,
Daniel Herren MD MHAChief of Hand Surgery
Schulthess Klinik
Zurich/ Switzerland
Miriam Marks, PhDResearch Associate
Department of Teaching, Research and
Development
Schulthess Klinik, Zurich, Switzerland
18 19
August 2019www.ifssh.info
TaylorDC.ComparisonoftheSingleAssessmentNumeric Evaluation method and two shoulder ratingscales.Outcomesmeasuresaftershouldersurgery.AmJSportsMed.1999;27:214-221.
36. WassersteinRL,LazarNA.TheASA’sStatementon p-Values: Context, Process, and Purpose. The AmericanStatistician.2016;70:129-133.
37. GreenlandS,SennSJ,RothmanKJetal.Statisticaltests,Pvalues,confidenceintervals,andpower:a guide to misinterpretations. Eur J Epidemiol. 2016;31:337-350.
38. Harris JD, Brand JC, Cote MP, Faucett SC, Dhawan A. ResearchPearls:TheSignificanceofStatisticsandPerilsofPooling.Part1:ClinicalVersusStatisticalSignificance.Arthroscopy.2017;33:1102-1112.
39. MarksM,RodriguesJN.Correctreportingandinterpretationofclinicaldata.JHandSurgEurVol.2017;42:977-979.
40. Mokkink LB, Terwee CB, Knol DL et al. The COSMIN checklistforevaluatingthemethodologicalqualityofstudiesonmeasurementproperties:aclarificationofitscontent.BMCMedResMethodol.2010;10:22.
41. de Vet HC, Beckerman H, Terwee CB, Terluin B, BouterLM.Definitionofclinicaldifferences.JRheumatol.2006;33:434.
42. Engel L, Beaton DE, Touma Z. Minimal Clinically ImportantDifference:AReviewofOutcomeMeasureScoreInterpretation.RheumDisClinNorthAm.2018;44:177-188.
43. RodriguesJN,MabvuureNT,NikkhahD,ShariffZ,DavisTR.Minimalimportantchangesanddifferencesinelectivehandsurgery.JHandSurgEurVol.2015;40:900-912.
44. RodriguesJN,ZhangW,ScammellBEetal.Recovery,responsivenessandinterpretabilityofpatient-reportedoutcomemeasuresaftersurgeryforDupuytren’sdisease.JHandSurgEurVol.2017;42:301-309.
45. Marti C, Hensler S, Herren DB, Niedermann K, MarksM.MeasurementpropertiesoftheEuroQoLEQ-5D-5Ltoassessqualityoflifeinpatientsundergoing carpal tunnel release. J Hand Surg Eur
Vol.2016;41:957-962.46. MaiaMV,deMoraesVY,DosSantosJB,FaloppaF,
BellotiJC.Minimalimportantdifferenceafterhandsurgery:aprospectiveassessmentforDASH,MHQ,andSF-12.SICOTJ.2016;2:32.
47. LondonDA,StepanJG,CalfeeRP.DeterminingtheMichigan Hand Outcomes Questionnaire minimal clinicallyimportantdifferencebymeansofthreemethods.PlastReconstrSurg.2014;133:616-625.
48. Shauver MJ, Chung KC. The minimal clinically importantdifferenceoftheMichiganhandoutcomes questionnaire. J Hand Surg Am. 2009;34:509-514.
49. TubachF,RavaudP,BaronGetal.Evaluationofclinicallyrelevantstatesinpatientreportedoutcomes in knee and hip osteoarthritis: the patientacceptablesymptomstate.AnnRheumDis.2005;64:34-37.
50. BellamyN,HochbergM,TubachFetal.Developmentofmultinationaldefinitionsofminimal clinically important improvement andpatientacceptablesymptomaticstateinosteoarthritis.ArthritisCareRes(Hoboken).2015;67:972-980.
51. TubachF,RavaudP,Martin-MolaEetal.Minimumclinically important improvement and patient acceptablesymptomstateinpainandfunctionin rheumatoid arthritis, ankylosing spondylitis, chronicbackpain,handosteoarthritis,andhipandkneeosteoarthritis:Resultsfromaprospectivemultinationalstudy.ArthritisCareRes(Hoboken).2012;64:1699-1707.
SPECIAL FEATURE ART
TOGETHER STRONG | Artist: Norma MacDonald | 1992 Australia Oil on Watercolour
Art Exibit #8
20 21
August 2019www.ifssh.info
SPECIAL FEATURE
alreadybeenburntonastake,asIwillhavedeliveredmyInvitedKeynoteSpeechbeforetheAmericanSocietyforSurgeryoftheHandonmyfindingsonRSD.However,likeGalileo,whowhenbeforetheInquisitionTribunalandpressedtorenouncehisthoughtspublicly,mumbled““Eppursimuove”(yetitmoves)”,Itoowillstandandsayoutloud:RSD/CRPS1doesnotexist.
THE BEGINNING OF THE END:
PreliminariesIconsiderthewholeconditionnamedRSD-CRPS1-Sudeck,tobeacompletefabrication.Inmyview,itis a very convenient “trashcan” diagnosis, where all paincomplaintsthatwedonotunderstandcanbeplaced. The patient with this “syndrome” is sent away fromthesurgeontoPhysicalTherapy(andlatertothePainClinic).Inthismanner,wesurgeons,getridoftheproblem,ofthepatient,andwecancontinuesleepinghappilyfeelingwecouldnothavepreventedtheproblem.Inotherwords,thesourceofchronicpost-operativepaincanbeblamedonRSD,and,ofcourse,onthepatient,whoistheultimatepersonresponsibleforbeingsosicklythattheydevelopthiscondition.Let’sstressfromthebeginningthatmanyofusthinkthatthereissomethingverysuspiciousaboutthewholeconcept.However,sinceeverybodyacceptsit,weplaywhatinpsychologyiscalledthebystandereffect:“ifnobodyiswillingtodoanything,whyshouldI?”5
TheoriginofCRPSisconfusing,butitbegan150yearsagowhenSilasMitchell,aneurologist,describedtheburningpainandvasomotorchangessoldiershadintheirlimbsaftersustainingmajornervetrunkinjuries.The condition was named causalgia and it had an evidentincitingpathology-anerveinjury.ThisinitialconceptwasdistortedbyPaulSudeckin1900,whoextended the condition to cases with similar clinical picturebutcausedbyminororevenanon-traumaticevent(minorcausalgia).Later,LericheandPolicardwouldattributeoveractivationofthesympatheticnervoussystemasforthepathologyresultinginthe
unusualclinicalpicture.Itisdifficulttodeterminewhen and how this totúm revolutum ended up in what weknowtodayasRSD/CRPS1/Sudeck.Butevenwithtoday’s medical advances,6,7 this “condition” has no consistentclinicalpicture,nospecificdiagnostictests,an unknown pathophysiology, and lacks pragmatic curative treatment. Surprisingly, with such a meagre pedigree,itcommandsamajorplaceinthemedicalliterature.Itisbackedbynofewerthan6000papersinasimplePubMedsearchandhundredsofchaptersinreferencebooks.
Indeed,itisremarkablethatnow,inthecurrenttrendofprecisescientificvirtuosity,whenthereisadorationforstatisticsversusobservation;now,whenanythingpublishedinanyofthe“reputed”journalshastobeproved,doublytested,doublyblinded,anddoublywrappedinnumbers;preciselyNOW,itsohappensthat this condition survives, as concocted more than 100yearsago,purelythankstoourblindadherencetolong-establishedtenets,withnoscientificfoottostandon.Isthisnotconcerning?
Tobefair,theconditionhasbeennottotallystaticsinceitsinceptionbyMitchell,SudeckandLeriche.Someyearsago,theterminologyandtaxonomyofreflexsympatheticdystrophywererevisedinordertododgethelackofsympatheticsysteminvolvement.8 The new terms are complex regional pain syndrome type1(CRPStype1)andCRPStype2.9BothCRPS1and2sharedsymptomsandsigns,butwhileintype2thereisaninjurednerve,inCRPS1nonerveinjurycanberecognized.Thus,reflexsympatheticdystrophy(RSD)andSudeckisparentheticallyretainedforCRPStype1andcausalgiaisinturnmaintainedforCRPStype2.
AlthoughinthispaperIwillrefermoretoCRPS1,Iwillunavoidablydiscussboth,asCRPS1and2areoftenmixedintheliterature,sharecorediagnosticfeatures,and hence, make the distinction quite elusive at times.10,11 FromthebeginningIshouldremarkthattrueCRPS2(causalgia)isadifferentanimalfromCRPS1:ithasanunderlyingpathology(adamagednerve),
SPECIAL FEATURE
Reflex Sympathetic Dystrophy (RSD)/CRPS/SUDECK does not existIntroduction The beginning of the end:
- Preliminaries - The literature.- The recognition that Pain Clinics are graveyards.-Thelackofknowledge/CRPSratio.- The Budapest criteria
• The importance of “Irritative CTS”.• The series: 100 patients diagnosed with RSD• The aftermath.• Conclusions.
ThisessaywaspromptedbyaletterfromProfessorMennen,EditorofEzine,askingmetoupdatetheEditorialIwroteintheJournalofHandSurgeryEuropean Volume.
ThispaperisaboutmyextremescepticismintheexistenceoftheSudeckatrophy,alsoknownasreflexsympatheticdystrophy(RSD)orcomplexregionalpainsyndrome(CRPS).Thenameforthisdiagnosisvariesdependingontheageofthesurgeon,theirbackground,andtheircountry,buttheyalldescribethesame:anabnormalpainfulresponseaftertraumaorsurgery,accompaniedbyvasomotorchanges,atleastintheearlystages,andthelackofaplausiblecauseforitsdevelopment.
Iwasemotionallymoved,whenProfessorMennenwrote:“Your“message”isveryimportantbecausesomanypatientsareunfairlylabelled[withthediagnosisofCRPS1]oftenbecauseofdoctors’slapdashdiagnosis-making,ignoranceorincompetence”(seealso:IFSSHEzine,Volume29,February2018,Editorial,“ChecklistforHolisticManagement”).Icannotagreemorewiththisstatementandtheimportanttruthsitbearsonourprofession.InmanycasesdiagnosingapatientwithCRPSistantamounttolabellingthemasapariah.Itisknownthatsomedoctorswillrefusetoseeanypatientwith this diagnosis. Even worse, are the iatrogenic and psychologicalconsequencesofthisdiagnosistothepatient: 2-4noceboeffect,medicalization,addictiontoopioids and psychotropic drugs, personality changes, lowself-esteem,catastrophicthoughts,etc.Manyofthese medications and therapies make it increasingly difficulttoreversetheprocess.Mysecondconcernaboutthisdiagnosisisthatitoftenistheendresultofpoordoctoring;inmostcasesrigorousphysicalexamand listening to the patient will elucidate the true mechanicalorphysicalsourceoftheirpain.
InthisreportIwilldescribetheprocesswhichdrovemeintoplayingthisQuixotesqueroleofplacingmyreputationonthelineateverymeetingforthesakeofdebunkingthisdiagnosisonceandforall.Asamatteroffact,bythetimethiswritingcomesoutImayhave
“Eppur si muove” G. Galilei.
22 23
August 2019www.ifssh.info
SPECIAL FEATURE
The recognition that the Pain Clinics are graveyardsAgain,manycluescomebychance.Ihadapatientwho,havingbeeninthePainClinicwiththediagnosisofRSDfor10yearsfollowingaminorcrushtohisthumb,cameforanotheropinion.Ifoundhehadaglomus tumor, which I treated and cured. As I used to liveinasmalltownwhereeverybodybumpsintoeachother, when I ran into the pain doctor whom I told, quite excitedly,thatIhadsuccessfullytreatedapatientofhiswhohadbeendiagnosedwithCRPS.Hereplied,somewhatoffended:“Myroleisnottoknowwhatthepatientshavebuttoeasetheirpain”….andhewasright,buthealsogavemeamostimportantclueformyfuture:onceyouareinthePainClinicnobodyisgoingtohelpyoutogetoutofthere.
The lack of knowledge/CRPS ratioAfterthisveryfirstpatientIbegantoseemoreandmorepatientsdiagnosedwithRSDand,inmost,Iwasabletofindthecauseandtreatthemsuccessfully.
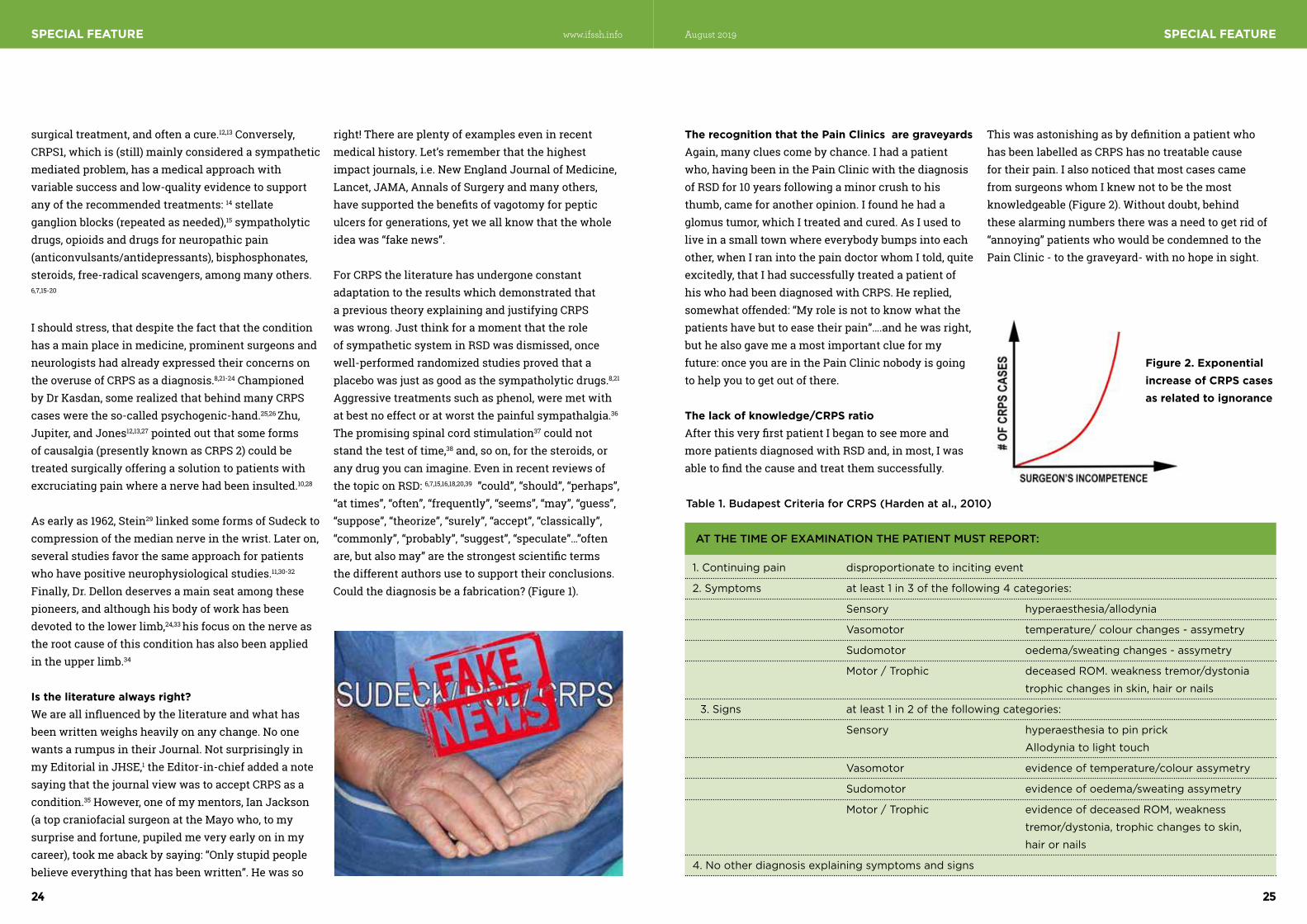
ThiswasastonishingasbydefinitionapatientwhohasbeenlabelledasCRPShasnotreatablecausefortheirpain.IalsonoticedthatmostcasescamefromsurgeonswhomIknewnottobethemostknowledgeable(Figure2).Withoutdoubt,behindthesealarmingnumberstherewasaneedtogetridof“annoying”patientswhowouldbecondemnedtothePain Clinic - to the graveyard- with no hope in sight.
Figure 2. Exponential increase of CRPS cases as related to ignorance
Table 1. Budapest Criteria for CRPS (Harden at al., 2010)
AT THE TIME OF EXAMINATION THE PATIENT MUST REPORT:
1. Continuing pain disproportionate to inciting event
2. Symptoms at least 1 in 3 of the following 4 categories:
Sensory hyperaesthesia/allodynia
Vasomotor temperature/ colour changes - assymetry
Sudomotor oedema/sweating changes - assymetry
Motor / Trophic deceased ROM. weakness tremor/dystonia
trophic changes in skin, hair or nails
3. Signs at least 1 in 2 of the following categories:
Sensory hyperaesthesia to pin prick
Allodynia to light touch
Vasomotor evidence of temperature/colour assymetry
Sudomotor evidence of oedema/sweating assymetry
Motor / Trophic evidence of deceased ROM, weakness
tremor/dystonia, trophic changes to skin,
hair or nails
4. No other diagnosis explaining symptoms and signs
SPECIAL FEATURE
surgicaltreatment,andoftenacure.12,13 Conversely, CRPS1,whichis(still)mainlyconsideredasympatheticmediatedproblem,hasamedicalapproachwithvariablesuccessandlow-qualityevidencetosupportanyoftherecommendedtreatments:14 stellate ganglionblocks(repeatedasneeded),15 sympatholytic drugs,opioidsanddrugsforneuropathicpain(anticonvulsants/antidepressants),bisphosphonates,steroids,free-radicalscavengers,amongmanyothers.6,7,15-20
Ishouldstress,thatdespitethefactthattheconditionhas a main place in medicine, prominent surgeons and neurologists had already expressed their concerns on theoveruseofCRPSasadiagnosis.8,21-24 Championed byDrKasdan,somerealizedthatbehindmanyCRPScases were the so-called psychogenic-hand.25,26 Zhu, Jupiter, and Jones12,13,27pointedoutthatsomeformsofcausalgia(presentlyknownasCRPS2)couldbetreatedsurgicallyofferingasolutiontopatientswithexcruciatingpainwhereanervehadbeeninsulted.10,28
As early as 1962, Stein29linkedsomeformsofSudecktocompressionofthemediannerveinthewrist.Lateron,severalstudiesfavorthesameapproachforpatientswho have positive neurophysiological studies.11,30-32 Finally, Dr. Dellon deserves a main seat among these pioneers,andalthoughhisbodyofworkhasbeendevotedtothelowerlimb,24,33 hisfocusonthenerveastherootcauseofthisconditionhasalsobeenappliedintheupperlimb.34
Is the literature always right?Weareallinfluencedbytheliteratureandwhathasbeenwrittenweighsheavilyonanychange.Noonewants a rumpus in their Journal. Not surprisingly in my Editorial in JHSE,1theEditor-in-chiefaddedanotesayingthatthejournalviewwastoacceptCRPSasacondition.35However,oneofmymentors,IanJackson(atopcraniofacialsurgeonattheMayowho,tomysurpriseandfortune,pupiledmeveryearlyoninmycareer),tookmeabackbysaying:“Onlystupidpeoplebelieveeverythingthathasbeenwritten”.Hewasso
right!Thereareplentyofexampleseveninrecentmedicalhistory.Let’srememberthatthehighestimpactjournals,i.e.NewEnglandJournalofMedicine,Lancet,JAMA,AnnalsofSurgeryandmanyothers,havesupportedthebenefitsofvagotomyforpepticulcersforgenerations,yetweallknowthatthewholeideawas“fakenews”.
ForCRPStheliteraturehasundergoneconstantadaptation to the results which demonstrated that aprevioustheoryexplainingandjustifyingCRPSwaswrong.JustthinkforamomentthattheroleofsympatheticsysteminRSDwasdismissed,oncewell-performedrandomizedstudiesprovedthataplacebowasjustasgoodasthesympatholyticdrugs.8,21
Aggressive treatments such as phenol, were met with atbestnoeffectoratworstthepainfulsympathalgia.36 The promising spinal cord stimulation37 could not standthetestoftime,38and,soon,forthesteroids,oranydrugyoucanimagine.EveninrecentreviewsofthetopiconRSD:6,7,15,16,18,20,39 ”could”, “should”, “perhaps”, “attimes”,“often”,“frequently”,“seems”,“may”,“guess”,“suppose”,“theorize”,“surely”,“accept”,“classically”,“commonly”,“probably”,“suggest”,“speculate”…”oftenare,butalsomay”arethestrongestscientifictermsthedifferentauthorsusetosupporttheirconclusions.Couldthediagnosisbeafabrication?(Figure1).
24 25
August 2019www.ifssh.info

SPECIAL FEATURE
Asalways,mostresponsescouldbefoundintheliterature.Ithasbeenlongknownthatbrachialgiaorevenmoreproximalpain,canbeoriginatedbycompressionofthemediannerveinthecarpaltunnel,andthatbyreleasingtheligamentthepaindisappears.41,42SwellinghasnotbeenconsideredaprominentfeatureinCTS,yetBurkeetal.haveprovedittobeamostprevalentsymptominidiopathicCTS.43 TheworksofOchoaandothersopenedmyeyesandhelped me to understand that the median nerve could cause pain in the ulnar nerve territory, proximally or even simulate an acute myocardial attack.10,44
Furthermore, Bennett and Xie45 demonstrated in rats that nerve compression triggered a clinical picture similartoaCRPS1.ThisassuredmeIwasverymuchon the right track: the median nerve. Nevertheless, I still needed more evidence.
Currently,anyground-breakingchangeinourpractices, or any new condition, is accepted only ifaccompaniedbyobjectivedata,statisticsand“evidence”.Albeitgood,weshouldnotforgetthatobservationhascontributedenormouslytotheprogressofMedicine.Throughobservation,Flemingrealizedthatpenicilliumhadabactericidaleffect.Throughobservation,syndromessuchas“partialthenaratrophy”and“acroparesthesia”(derogativelyknown,asitaffectedmostlywomen,as“hystericalnocturnal paresthesias” – these were certainly pre #metoodays)werelinkedtogether,givingbirthtoanewcondition:theultrafamouscarpaltunnelsyndrome(CTS).46Itisastonishingtorealizethatthemostcommonoperationahandsurgeonperformstoday,carpaltunnelrelease(CTR),wasunknownuntil1950.Thousandsofpatientshavebenefitedfromthisimportantunderstanding-simplybasedonobservation.47,48 Beforethislinkageseveral“treatments”foridiopathicCTSpatientshadbeenrecommended:quinine,iron,arsenic,morphine,strychnine,henbane,galvanizationofthehandswithinterruptedandcontinuouscurrent,PhenobarbitalandBromidecombinedwithavasodilator,andribresection,amongmany others.46 To sum up, all these advances, and so
manymoreintheHistoryofMedicine,werethankstoobservation,presentlyreviledbythescientificmethodology.
Throughobservationwenoticedthatagroupofpatientswhohad“compression”ofthemediannerve,did not display the typical CTS signs and symptoms. Chiefcomplaintswerepainandtinglinginthemediannervedistribution(butoftennotlimitedtoit),worseningofthesymptomsatnight,swelling,and,aboveall,inabilitytomakeafullfist(Figure4).Thosewere exactly the same signs and symptoms a very differentgroupofpatientsdisplayed.Thelatterwereall patients with previous trauma to their hands and whohadbeenlabelledandtreatedforCRPSpriortoreferral.Bothgroupswereindistinguishableclinicallyandbothweretreatedwithcarpaltunnelrelease(CTR).Innocasewerecontinuousaxillaryblocks,sympatholyticmedication,orstellateganglionblocksgivenafterthesurgery.Lightpainkillers(paracetamolorally)wasprescribedasperourusualprotocolforpatientswhohaveidiopathicCTR.Theresponseandoutcometosurgerywasindistinguishable.Wenamedthis new condition irritative carpal tunnel syndrome, asthemediannerveseemedtobeirritatedratherthan
Figure 4.
SPECIAL FEATURE
Weaknesses of the Budapest criteriaButwhywasitpossibleforasurgeontolabelaconditionasbeingCRPSifithadatreatablecause?How could we make a diagnosis that has such anenormousimpactonapatient’swell-beingsofrivolously?Thereasonwas,withoutadoubt,thatthecriteriaappliedtodiagnoseCRPSwereextremelyindistinctandbiased:anythingwouldfit(Table1).40 Specifically,pain(criteria1)wassubjective,andcriteria2and3weresharedbytrauma,inflammatoryconditions, ischemia, etc, and were thus quite unspecific.However,themostunfairofalldiagnosticcriteria,andtheonewhichlaterprovedtobethemain“sinkhole”,wasitem4.Criteria4lefttoadoctor’sdiscretionwhichpatienttheyfelthadanunknowncondition.AsIalreadypointedoutinmyformereditorial,“Theonlypersonwhoshouldreliablystatethatthereisnotanovertorganiccauseforapatient’spainshouldbethespecialistinthefieldi.e.aHandSurgeon”. The rest do not have the knowledge and understandingtolabelapatientwithCRPS.Butevenintherealmofhandsurgery,doweallknowthesame?
THE IMPORTANCE OF IRRITATIVE CTSTherecognitionthatIcouldsuccessfullytreatpatientslabelledashavingRSDbyfellowsurgeons/doctors, and the direct relationship to their lack ofknowledge,triggeredinmymindthefollowing“anti-establishment”thought:“Ifonlyweallknewallthefacts,RSD/CRPS/Sudeckwouldnotexist”.I,hence,becameobsessedtryingtounderstandwhatthese patients really had. It was clear that some had factitiousissues,othershadsustainedanervetrauma(Causalgia/CRPS2),andalargegrouphadsufferedfrombad-doctoring.But,whatabouttherest?
IamnotsureexactlyhowandwhenIrealizedthatthecomplaintofworseningofsymptomsatnightreportedbysomeCRPSpatientswastheclueintheremainingcases. The only condition that I knew to produce this wascompressionofthemediannerveinthecarpaltunnel.However,thesepatientslabelledasCRPShadaverydifferentpicturefromaclassiccarpaltunnel
syndrome(CTS):painandnumbnessawayfromthemediannerveterritory,swelling,stiffness,burningpain,etc(Figure3).
Figure 3. Asampleofchartsofmyongoingstudy,showingtheareaofallodynia-dysesthesiasinthehandreportedbythepatients(marked).Notethatmosthad more symptoms in the ulnar nerve territory, some inaglovedistributionandfewinthemediannerveterritory.
26 27
August 2019www.ifssh.info

SPECIAL FEATURE
CTscanshowsthestatusofthewristathisveryfirstvisit,3monthsaftertheaccident.ThemalunionwasaggravatedbyaconcurrentVolkmannandintrinsicmusclescontracture.Surgerywasadvisedbutthepatient declined, arguing that his treating doctor had stressed to him that any surgery in a Sudeck patient wouldharmhim.Instead,a4-monthcourseofPTandpsychotropic medication were recommended. He was losttofollowupafterthis“confrontation”.
Thosewhohadsurgeryhadtheirproblemsolvedallbarone.Thisspecificpatientremainedunhappyduetostiffness.Herpainwasratedduringphysicaltherapyas8over10inaVAS(0-10).Nevertheless,herpainatnightanddaytimedroppedfrom10to0atthesixmonthfollowup.Thisparticularpatienthad a metastatic lung cancer and was undergoing chemotherapy. She developed shoulder and wrist pain afterhavingbeenoperatedonforawristfracture.Itis worth stressing that those with Irritative CTS were operated on disregarding their nerve conduction studieswhichwerenegativeinasignificantnumberofthose whom were asked.
Tosummarize,bykeepingthecategorizationchartinmind,nopatientsweretobelabelledasRSD/CRPS1/Sudeck.
THE AFTERMATHTThebirth,orthedeath,ofanyconditionorassumedtreatmentis,inevitably,surroundedbycontroversy.Recently,wehavewitnessedthedeathofvagotomyinpepticulcermanagement,despiteawealthofsupportiveliteratureinhigh-rankingjournals.
In my Quixotesque role to kill this condition, I am notalone-Iamstandingontheshoulderofgiants,surgeons and neurologists,8,10-13,21-34 whose keen eyes havebeencorneringthecondition:psychogenichand,causalgia(CRPS2)werebutapartofthepicture.But this was not enough, there were some patients leftoutwhohadsymptomsandsignsthatcouldbeassignedtoCRPS.Mybackgroundasawristand
microsurgeonallowedmetospotstructuralbad-doctoringastherootcauseofmanyCRPScases.Thefinalpiecetothejigsawwasnotingthatthemediannervecouldbeirritatedwithoutbeingcompressed,thusfrequentlythestandardneurologicalstudieswerenon-contributory.Morethan40patientshavebeenoperatedonforirritativeCTS(Figure7)andallexceptone,aforementioned,responded.Whethershehad an “unknown condition”, a psychogenic hand, or a grievancebecauseofherunderlyingmedicalcondition,requiresfurtherstudy.Inthisrespect,patientswhodonotimproveafterarigoroussearchforthecauseorafterfailedsurgery,mightneedtogotothePainClinic.Thismustalwaysbeunderthesupervisionofthe treating surgeon. For sure, the Pain Clinic should notbeagraveyardofdiscardedpatients,buttheplacewherepatientsaretobetreatedtemporarily,whiletherootcauseoftheproblemissoughtoutandsolved.
Figure7.Thispatientwasseen8monthsaftersustainingaDRFtreatedinacast.Nomalalignmentexisted on the X-rays. Nevertheless, she developed pain and swelling that required intensive PT and treatmentinthePainClinic(seepatient’spictureontheleftat5monthswithpersistingswelling).Onherfirstvisit,despitebeingongabapentin,lidocainepatches/opioidssheratedherpainas8(onaVAS:0-10)andcouldnotmakeafist.FiveweeksafterCTRunder local her pain was 0. She returned to work as a housekeeper in a hotel.
Butdonotgetmewrong,theproblemisnotsolvedbysimplyreleasingthecarpalligament.Infact,doingso,canevenbedetrimental:therearemany
Figure 7
SPECIAL FEATURE
compressed. I should stress that these patients were operated disregarding their nerve conduction studies whichwerenegativein2/3ofthosewhomwereasked.
Figure4.Severeformofbilateralirritativecarpaltunnelsyndrome.Inbothpictures,thepatientisbeingaskedtomakeatightfist.Ontheleft,heisshownpreoperatively,ontherightheisshownintheORafterbilateralCTRunderlocalanesthesia.Noantecedenttraumacouldberecalled.
THE SERIES: 100 patients with the diagnosis of RSDIrritative carpal tunnel syndrome was the missing link Iwaslookingfortobeabletocomefullcircle!!!
ToconfirmthatIwasright,Istudiedacohortof100consecutivepatientswhohadcometotheofficewiththediagnosisofRSD.(Ittookmemorethan4yearstogatherthefirst25patients,butonceIhadappeared on the national news dealing with this topic,Igatheredtheremaining75inlessthanayear).Briefly,thepreliminarydatashowsthatninety-fivepercenthadbeendiagnosedwithRSDbyaphysician(surgeonorrehabilitationdoctor)andtherestbyatherapist.Ninetypercenthadbeentreatedinapainclinic. Ninety-three percent were on opioids and/or psychotropicmedication,oneformorethan15years.The remaining were on painkillers and steroids. All hadpain,senseofstiffnessand/orlimitedrangeofmotion.
Thegeneralresultscanbesummarizedinthechartbelow(Figure5).Notethaninnearlyhalf,baddoctoringwasbehindthescenes:ignoranceorovertmalpracticemaskedbytheCRPS/RSDacronyms!!
The psychogenic-hand patients were advised to go to a psychiatric consultation with little success. Five patientsdidnotrequireanysurgicaltreatment,butsupportinPTandwereweanedoffdrugs.Iopenhereaparenthesistostressthatitisnotuncommonforsomepatientstodevelop,aftersurgeryortrauma,whatIwastaughttobea“flarereaction”.Theclinicalpictureappearedsomeweeksafterthetrauma/surgeryandsharedthesamesymptomsandsignsasaCRPS1.TheproblemclearedupwithPTandreassurance.Now,duetoabuseofthediagnosisofCRPSandthelaxityofthecriteria,18,40someflarereactionscanbemisinterpretedasCRPS-draggingthepatientintotheperniciouseffectsofsuchamisdiagnosis.2-4
Nearlyhalfdismissedanyoperationonthegrounds:“my doctor advised me against surgery”, “my doctor told me you are only interested in operating on me to make money” and “the literature is against surgery”, yettheyhadtreatableconditions.Theoversightedpathologywasattimesembarrassing(Figure6).
Figure 6. This 34-year-old male diagnosed with Sudeck had neuropathic pain, anesthesia in the mediannerveterritory,andafrozenhand.HehadsustainedamotorbikeaccidentwhichrequiredaweekofICUadmissionforabdominalandheadtrauma.Thewristwasplacedina(tight?)cast.The
Figure 5: True allocation of the patients diagnosed with Sudeck’s in this study.
Figure 6.
28 29
August 2019www.ifssh.info

incontradictionofthecurrenttrendofrocketingnumbersofCRPS1cases(50,000newcasesperyearintheUSA),55 removing the niche will reduce the incidenceoftheproblemdrasticallyinfewyears,ashasalreadyoccurredinotherunsubstantiatedepidemicsinourfield.56,57
Inclosing,IbeseechyoutohelpmetowipeoutthisfabricationthatleavesoursufferingpatientsstrandedinPainClinicsaroundtheglobe.Ourendeavorispavedwithresistance,notonlyhastheexistenceofRSDbeenengravedinstoneinourminds,butstubbornoppositiontonewideasispartofthehumannature.IconfessedinmyEditorial1thatIdreamedabouttheeradicationofthispseudo-condition.Nowthattheenlightenmentissoclose,IadmitthattoooftenIawakeninthemiddleofthenightandittakesmehourstofallsleepagainbecauseoftheexcitementofknowingthatifIsucceedIwillhavedonemoregoodthananythingelseIhaveproducedinmylife.PleasehelptheprogressofsciencebyplacingallyourmedicalknowledgeattheserviceofyournextCRPSpatient.
Asafinalcaveat:Ittakesasmallleapofimagination,thatifIcandebunkthewholeCRPSconceptinmyterrain,therestofthebodywillbeopenforotherstodeliverthefinalblow(ajobalreadystartedbyprominentgiants).13,33,58
References 1. delPiñalF.Editorial.Ihaveadream...reflex
sympatheticdystrophy(RSDorComplexRegionalPainSyndrome-CRPSI)doesnotexist.JHandSurgEurVol.2013Jul;38(6):595-7.
2. RingD,BarthR,BarskyA.Evidence-basedmedicine:disproportionatepainanddisability.JHandSurgAm.2010Aug;35(8):1345-7.
3. Hayes PJ, Louis DS, Kasdan ML. Additional considerations in complex regional pain syndrome. JHandSurgAm.2012Mar;37(3):625.
4. Bass C. Complex regional pain syndrome medicaliseslimbpain.BMJ.2014Apr28;348:g2631
5. RosenbaumL.TheNot-My-ProblemProblem.NEnglJMed.2019Feb28;380(9):881-885
6. MarinusJ,MoseleyGL,BirkleinF,BaronR,MaihöfnerC,KingeryWS,vanHiltenJJ.Clinicalfeaturesandpathophysiologyofcomplexregionalpainsyndrome.LancetNeurol.2011Jul;10(7):637-648.
7. Bruehl S. Complex regional pain syndrome. BMJ. 2015Jul29;351:h2730.
8. OchoaJL.Truths,errors,andliesaround“reflexsympathetic dystrophy” and “complex regional pain syndrome.”JNeurol1999;246:875–879
9. Stanton-HicksM,JänigW,HassebuschSJ,HaddoxJD,BoasR,WilsonP.Reflexsympatheticdystrophy:changingconceptsandtaxonomy.Pain.1995;63:127-133.
10. ThimineurMA,SaberskiL.ComplexregionalpainsyndrometypeI(RSD)orperipheralmononeuropathy?Adiscussionofthreecases.ClinJPain1996;12:145–150.
11. PlaczekJD,BoyerMI,GelbermanRH,SoppB,GoldfarbCA.NervedecompressionforcomplexregionalpainsyndrometypeIIfollowingupperextremitysurgery.JHandSurgAm.2005;30(1):69-74.
12. ZhuSX,LuSB,YaoJX,LiuZS,SunYW,WangXL,LiZY,FuZG,LiuZX.Intrafasciculardecompressioninthetreatmentofcausalgiawithspecialreferencetothemechanism.AnnPlastSurg.1985Dec;15(6):460-4.
SPECIAL FEATURE
Dr. F. del Piñal Serrano 58-1B.
28001- Madrid
Ph:+34-914310051.
Paseo de Pereda 20-1
39004-Santander. Spain
Ph:+34-942364696
Email: [email protected]
Personal: [email protected]
SPECIAL FEATURE
factorsinplay.Justaswhenrecognizingafactitiousinjuryyougettoknowallpossibleanswers,25,26,49,50 the sameappliesforbad-doctoring.Inabout40%ofthecasestherewasamajormedicalerrorbehindthem(includinginadequatecarpaltunnelreleasein15%).Co-existentshoulderpainandestablishedstiffnessinterfereintherecoveryandhastobeaddressed.Besides this, surely the percentages and root causes ofCRPScasesvaryineachsurgeon’spractice.Asanexample,thismaybemoreanerveprobleminDr.Dellon’soffice,moreamechanicalcauseinmine,andamixedetiologyinothers’.Wearecurrentlylookingfora test that could help everyone to spot a patient with atreatablecondition.Wearestudyingthesmallfiberswhicharetheafferentsforpain,burningsensation,andwhichdominatevasomotoreffectors(A∂fibers-smallmyelinated-andCfibers-unmyelinated).Thesefiberscannotberecordedbythestandardneurophysiologicaltests(whichstudylarge–fast-conducting-myelinatedfibers).Perhapstheso-calledSympatheticSkinResponsetestmayproveuseful.51-52 Another avenue isfunctionalbrainMRI.Withthelatter,wewanttosortoutwhohasrealpain,andhowdifferentthisisin irritative carpal tunnel syndrome versus idiopathic carpal tunnel syndrome.
Myfinalwordsgotothesufferingpatientswhoneedourloveandcompassion.Theyhavebeenwanderingfromonedoctortoanotherandresemblezombiesmorethannormalpeople.Veryfewarelookingfora secondary gain, and indeed most are under the effectofmultipledrugsandreceivingnoempathy.(Irecently had, as a patient, an ICU doctor, who could notstopcursingtheincomprehensionshehadbeenthroughbeforewetackledherproblem).Icannotdenythat there are patients whose characteristics may makeusrepudiatethemfromtheveryoutset.Butlet’sberational.Firstofall,astheyhavealreadybeensubjectedtoafailedtreatment,theywillregardthenewsurgeonwithsuspicionandlackofconfidence.Furthermore,thosewhohavebeeninthePainClinicforalongperiod,havebecomeaddictedtoseveral
drugs,withpersonalityimplications(lowself-esteem,passive-aggressiveness, uncoordinated discourse, amongothers).Typically,allofthemhaveaverylowthresholdforpainand,becauseoftheirlonguse-andabuse-ofdrugs,theyself-medicatesettingtheirownrulesmuchtoourdespair.However,afterseveraldaysorweeks,oncetheystarttofeelbetter,theyplacetheirregainedtrustintheirtreatingdoctorandbecomethemostcooperative,thankfulandwillingtohelpothersthat you have ever had. Love them, they need our love and care.
CONCLUSIONS: The amplifier effect.IfIweretocondenseallmyresearchintoaverysimpletheory,Ishouldnameitthe“Amplifiereffect”.Thetermstressesthat,muchliketheamplifierofamusicsystemwhichmultipliesthesoundpickedupbytheneedleoftheturntable,the“damaged/irritated”nervewilllikewisemultiplythefinalpainreadinginourcortextothepowerof“n”(Figure9).Thistheorymayappear as unproven as others that have attempted toexplainthephysiopathologyofCRPS.However,thereisanimportantdifference-thisapproachhaspragmaticallyprovedsuccessful.
AnotherconclusionofthisstudyisthatCRPS1and2arethesamecondition,theformerwithan“irritated”nerve(RSD,Sudeck),andthelatterwithastructurallydamagednerve(causalgia).Nevertheless,botharenervemediatedpathologies.Therefore,amoreappropriatetermforthewholeclinicalpicturecouldbe“Neuralamplifiedpain”.Patientswithoutanerveissue,havetobecategorizedaspsychogenichand,malingerers,victimsofbaddoctoring,andsomeearlycasescouldfallintotheso-called“flarereaction”pigeonhole.Finally,aminoritymaybeascribedtounknownconditions(1in100inmyseries).Ifoneadherestotheseunderstandings,therewillbenomoremysteryhiddeninCRPS.Moreimportantly,thepatientwillbeproperlyallocatedtoarealcondition,nottoCRPS.Consequently,thiswillpreventunnecessarysufferingandmedicalizationinallpatients,2-4 and aboveallinthosemostvulnerable.53,54Iforeseethat
30 31
August 2019www.ifssh.info
34. DellonAL.SurgicalTreatmentofUpperExtremityPain.HandClin.2016;32(1):71-80.
35. GiddingsG.Editor-inchiefcommenton:DelPiñalF.Editorial.Ihaveadream...reflexsympatheticdystrophy(RSDorComplexRegionalPainSyndrome-CRPSI)doesnotexist.JHandSurgEurVol.2013Jul;38(6):595-7.
36. StraubeS,DerryS,MooreRA,etal.Cervico-thoracicorlumbarsympathectomyforneuropathicpainand complex regional pain syndrome. Cochrane DatabaseSystRev2013;9:CD002918.
37. KemlerMA,BarendseGA,vanKleefM,deVetHC,RijksCP,FurnéeCA,vandenWildenbergFA.Spinalcordstimulationinpatientswithchronicreflexsympathetic dystrophy. N Engl J Med. 2000 Aug 31;343(9):618-24.
38. Kemler MA, de Vet HC, Barendse GA, van den WildenbergFA,vanKleefM.EffectofspinalcordstimulationforchroniccomplexregionalpainsyndromeTypeI:five-yearfinalfollow-upofpatientsinarandomizedcontrolledtrial.JNeurosurg.2008Feb;108(2):292-8.
39. Field J. Complex regional pain syndrome: a review. JHandSurgEurVol.2013Jul;38(6):616-26.
40. HardenN,BruehlS,PerezRetal.Validationofproposeddiagnosticcriteria(the‘BudapestCriteria’)forcomplexregionalpainsyndrome.Pain.2010,150:268–74.
41. CrymbleB.Brachialneuralgiaandthecarpaltunnelsyndrome.BrMedJ1968;3:4701.
42. Cherington M. Proximal pain in carpal tunnel syndrome.ArchSurg.1974Jan;108(1):69.
43. BurkeDT,BurkeMA,BellR,StewartGW,MehdiRS,KimHJ.Subjectiveswelling:anewsignforcarpaltunnelsyndrome.AmJPhysMedRehabil.1999;78(6):504-508.
44. TorebjörkHE,OchoaJL,SchadyW.Referredpainfromintraneuralstimulationofmusclefasciclesinthemediannerve.Pain.1984Feb;18(2):145-56.
45. Bennett,C.J.,andXie,Y.-K.:Aperipheralmononeuropathyinratthatproducesdisordersofpain sensation like those seen in man. Pain, 33: 87-107. 1988.
46. Boskovski MT, Thomson JG. Acroparesthesia and carpal tunnel syndrome: a historical perspective. J HandSurgAm.2014Sep;39(9):1813-1821.
47. BrainWR,WrightAD,WilkinsonM.Spontaneouscompressionofbothmediannervesinthecarpaltunnel;sixcasestreatedsurgically.Lancet.1947Mar8;1(6443-6445):277-82.
48. PhalenGS,GardnerWJ,LaLondeAA.Neuropathyofthemediannerveduetocompressionbeneaththetransverse carpal ligament. J Bone Joint Surg Am. 1950Jan;32A(1):109-12.
49. ReadingG.Secretan’ssyndrome:hardedemaofthedorsumofthehand.PlastReconstrSurg.1980Feb;65(2):182-187.
50. SimmonsBP,VasileRG.Theclenchedfistsyndrome.JHandSurgAm.1980Sep;5(5):420-427.
51. Santiago S, Ferrer T, Espinosa ML. Neurophysiologicalstudiesofthinmyelinated(Adelta)andunmyelinated(C)fibers:applicationtoperipheral neuropathies. Neurophysiol Clin. 2000 Feb;30(1):27-42.
52. OaklanderAL,FieldsHL.Isreflexsympatheticdystrophy/complex regional pain syndrome type Iasmall-fiberneuropathy?AnnNeurol.2009Jun;65(6):629-38.
53. GuptaA,SilmanAJ,RayD,MorrissR,DickensC,MacFarlaneGJ,ChiuYH,NichollB,McBethJ.Theroleofpsychosocialfactorsinpredictingtheonsetofchronicwidespreadpain:resultsfromaprospectivepopulation-basedstudy.Rheumatology(Oxford).2007Apr;46(4):666-71.
54. MunglaniR.Doesadiagnosisinpainmedicinepromotedisability?PainNews2012;10:16-8.
55. BreuhlS,ChungOY.Howcommoniscomplexregionalpainsyndrome-Type1?Pain2007;129:1-2
56. IrelandDC.Repetitionstraininjury:theAustralianexperience--1992 update. J Hand Surg Am. 1995 May;20(3Pt2):S53-6.
57. IrelandDC.Australianrepetitionstraininjuryphenomenon.ClinOrthopRelatRes.1998Jun;(351):63-73.
SPECIAL FEATURE
13. JupiterJB,SeilerJG3rd,ZienowiczR.Sympatheticmaintainedpain(causalgia)associatedwithademonstrableperipheral-nervelesion.Operativetreatment.JBoneJointSurgAm.1994;76(9):1376-1384.
14. O’Connell NE, Wand BM, McAuley J, et al. Interventionsfortreatingpainanddisabilityinadults with complex regional pain syndrome. CochraneDatabaseSystRev2013;4:CD009416
15. PattersonRW,LiZ,SmithBP,SmithTL,KomanLA.Complexregionalpainsyndromeoftheupperextremity.JHandSurgAm.2011Sep;36(9):1553-62
16. GayAM,BéréniN,LegréR.TypeIcomplexregionalpainsyndrome.ChirMain.2013Oct;32(5):269-80
17. VarennaM,AdamiS,RossiniM,GattiD,IdolazziL, Zucchi F, Malavolta N, Sinigaglia L. Treatment ofcomplexregionalpainsyndrometypeIwithneridronate:arandomized,double-blind,placebo-controlledstudy.Rheumatology(Oxford).2013Mar;52(3):534-42.
18. ŻylukA,PuchalskiP.Complexregionalpainsyndrome:observationsondiagnosis,treatmentanddefinitionofanewsubgroup.JHandSurgEurVol.2013Jul;38(6):599-606.
19. ChevreauM,RomandX,GaudinP,JuvinR,BailletA.BisphosphonatesfortreatmentofComplexRegionalPain Syndrome type 1: A systematic literature reviewandmeta-analysisofrandomizedcontrolledtrialsversusplacebo.JointBoneSpine.2017Jul;84(4):393-399.
20. KomanAL,SmithBP,SmithTL.Apracticalguideforcomplex regional pain syndrome in the acute stage andlatestage.In:WolfeSW,HotchkissRN,PedersonWC, et al, editors. Green’s operative hand surgery. 7thedition.Philadelphia:ChurchillLivingstone;2017. p.1797-1827.
21. SchottGD.Interruptingthesympatheticoutflowincausalgiaandreflexsympatheticdystrophy.BMJ.1998Mar14;316(7134):792-3.
22. BarthRJ,HaralsonR.Differentialdiagnosisforcomplex regional pain syndrome. The Guides Newsletter,September/October2007.AmericanMedical Association:1– 4, 12–16.
23. BarthRJ.ComplexRegionalPainSyndrome.ChapterKin:MelhornJM,Eskay-AuerbachM,eds.20thAnnualAmericanAcademyofOrthopaedic Surgeons Workers Compensation and MusculoskeletalInjuries:ImprovingOutcomeswithBack-To-Work, Legal, and Administrative Strategies. AmericanAcademyofOrthopaedicSurgeons;2018.
24. DellonAL.RSD,Chapter7,3rdEd.,Painsolutions.LightningSourceInternetPublications,2013,pp205-230.
25. KasdanML,StuttsJT.Factitiousinjuriesoftheupperextremity.JHandSurgAm.1995May;20(3Pt2):S57-60.
26. StuttsJT,KasdanML,HickeySE,BrunerA.Reflexsympathetic dystrophy: misdiagnosis in patients withdysfunctionalposturesoftheupperextremity.JHandSurgAm.2000Nov;25(6):1152-6.
27. JonesNF,ShawWW,KatzRG,AngelesL.Circumferentialwrappingofaflaparoundascarredperipheralnerveforsalvageofend-stagetractionneuritis.JHandSurgAm.1997May;22(3):527-35
28. AdaniR,TosP,TaralloL,CorainM.Treatmentofpainfulmediannerveneuromaswithradialandulnararteryperforatoradipofascialflaps.JHandSurgAm.2014Apr;39(4):721-7.
29. Stein,AHJr.Therelationofmediannervecompression to Sudeck’s syndrome. Surg Gynec Obstet.1962;115:713-720.
30. GrundbergAB,ReaganDS.Compressionsyndromesinreflexsympatheticdystrophy.JHandSurgAm.1991;16(4):731-736.
31. Monsivais JJ, Baker J, Monsivais D. The associationofperipheralnervecompressionandreflexsympatheticdystrophy.JHandSurgBr.1993;18(3):337-338.
32. Koh SM, Moate F, Grinsell D. Co-existing carpal tunnel syndrome in complex regional pain syndromeafterhandtrauma.JHandSurgEurVol.2010;35(3):228-231.
33. DellonAL,AndonianE,RossonGD.CRPSoftheupper or lower extremity: surgical treatment outcomes.JBrachialPlexPeripherNerveInj.2009Feb20;4:1.
SPECIAL FEATURE
32 33
August 2019www.ifssh.info
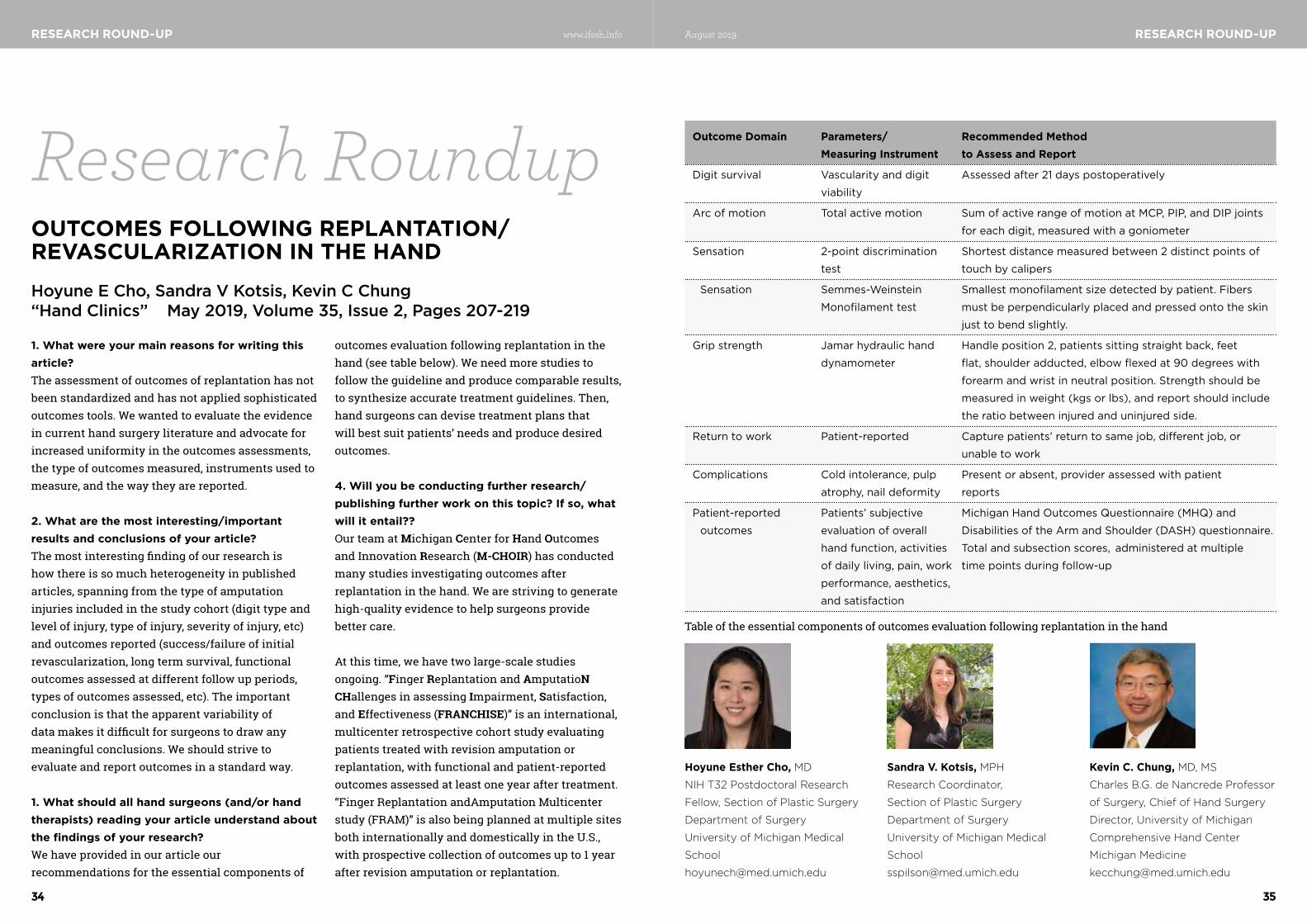
RESEARCH ROUND-UP
1. What were your main reasons for writing this article?Theassessmentofoutcomesofreplantationhasnotbeenstandardizedandhasnotappliedsophisticatedoutcomes tools. We wanted to evaluate the evidence incurrenthandsurgeryliteratureandadvocateforincreaseduniformityintheoutcomesassessments,thetypeofoutcomesmeasured,instrumentsusedtomeasure, and the way they are reported.
2. What are the most interesting/important results and conclusions of your article?Themostinterestingfindingofourresearchishowthereissomuchheterogeneityinpublishedarticles,spanningfromthetypeofamputationinjuriesincludedinthestudycohort(digittypeandlevelofinjury,typeofinjury,severityofinjury,etc)andoutcomesreported(success/failureofinitialrevascularization,longtermsurvival,functionaloutcomesassessedatdifferentfollowupperiods,typesofoutcomesassessed,etc).Theimportantconclusionisthattheapparentvariabilityofdatamakesitdifficultforsurgeonstodrawanymeaningfulconclusions.Weshouldstrivetoevaluate and report outcomes in a standard way.
1. What should all hand surgeons (and/or hand therapists) reading your article understand about the findings of your research?We have provided in our article our recommendationsfortheessentialcomponentsof
outcomesevaluationfollowingreplantationinthehand(seetablebelow).Weneedmorestudiestofollowtheguidelineandproducecomparableresults,tosynthesizeaccuratetreatmentguidelines.Then,hand surgeons can devise treatment plans that willbestsuitpatients’needsandproducedesiredoutcomes.
4. Will you be conducting further research/publishing further work on this topic? If so, what will it entail??Our team at Michigan CenterforHand Outcomes and Innovation Research(M-CHOIR)hasconductedmanystudiesinvestigatingoutcomesafterreplantation in the hand. We are striving to generate high-quality evidence to help surgeons provide bettercare.
At this time, we have two large-scale studies ongoing. “Finger Replantation and AmputatioN CHallenges in assessing Impairment, Satisfaction,and Effectiveness(FRANCHISE)”isaninternational,multicenter retrospective cohort study evaluating patients treated with revision amputation or replantation,withfunctionalandpatient-reportedoutcomesassessedatleastoneyearaftertreatment.“FingerReplantationandAmputationMulticenterstudy(FRAM)”isalsobeingplannedatmultiplesitesbothinternationallyanddomesticallyintheU.S.,withprospectivecollectionofoutcomesupto1yearafterrevisionamputationorreplantation.
OUTCOMES FOLLOWING REPLANTATION/REVASCULARIZATION IN THE HAND
Research Roundup
RESEARCH ROUND-UP
Hoyune E Cho, Sandra V Kotsis, Kevin C Chung “Hand Clinics” May 2019, Volume 35, Issue 2, Pages 207-219
Hoyune Esther Cho, MD
NIH T32 Postdoctoral Research
Fellow, Section of Plastic Surgery
Department of Surgery
University of Michigan Medical
School
Outcome Domain Parameters/ Recommended Method Measuring Instrument to Assess and Report
Digit survival Vascularity and digit Assessed after 21 days postoperatively
viability
Arc of motion Total active motion Sum of active range of motion at MCP, PIP, and DIP joints
for each digit, measured with a goniometer
Sensation 2-point discrimination Shortest distance measured between 2 distinct points of
test touch by calipers
Sensation Semmes-Weinstein Smallest monofilament size detected by patient. Fibers
Monofilament test must be perpendicularly placed and pressed onto the skin
just to bend slightly.
Grip strength Jamar hydraulic hand Handle position 2, patients sitting straight back, feet
dynamometer flat, shoulder adducted, elbow flexed at 90 degrees with
forearm and wrist in neutral position. Strength should be
measured in weight (kgs or lbs), and report should include
the ratio between injured and uninjured side.
Return to work Patient-reported Capture patients’ return to same job, different job, or
unable to work
Complications Cold intolerance, pulp Present or absent, provider assessed with patient
atrophy, nail deformity reports
Patient-reported Patients’ subjective Michigan Hand Outcomes Questionnaire (MHQ) and
outcomes evaluation of overall Disabilities of the Arm and Shoulder (DASH) questionnaire.
hand function, activities Total and subsection scores, administered at multiple
of daily living, pain, work time points during follow-up
performance, aesthetics,
and satisfaction
Tableoftheessentialcomponentsofoutcomesevaluationfollowingreplantationinthehand
Sandra V. Kotsis, MPH
Research Coordinator,
Section of Plastic Surgery
Department of Surgery
University of Michigan Medical
School
Kevin C. Chung, MD, MS
Charles B.G. de Nancrede Professor
of Surgery, Chief of Hand Surgery
Director, University of Michigan
Comprehensive Hand Center
Michigan Medicine
34 35
August 2019www.ifssh.info

MEMBER SOCIETY NEWS
Member Society NewsTHE BELGIAN SOCIETY FOR SURGERY OF THE HAND
TheBelgianSocietyforSurgeryoftheHandintroducedtheBelgianHandSurgeryCertificate(BHSC)inOctober2018.ThisContinuingEducationalProgram(PVG)withaCertificate,isan inter-university training program supported byallsevenBelgianUniversities.Theaimistostandardizethecompetencyinsurgeryofthehandand peripheral nerves.
The BHSC course runs over two years, consists of4modulesperyear,eachmodulerunover2days(FridayandSaturday,8hoursperday).Theprogramentailsamixoftheory,casediscussionand cadaveric training. At least 80% attendance is obligatory.
Themodulesareorganizedinturnbytheuniversitiesandtheteachersarefromtheparticipating universities to ensure an optimal standardoftraining.
The training program is open to all Orthopaedic , General and Plastic Surgeons , as well as residents intheirlasttwoyearsoftrainingfromEuropeandbeyond.
ThestandardoftheprogramisbasicandcanpreparethemfortheEuropeanDiplomainHandSurgeryExaminationaftertherequiredfellowshiptraining.AdmissiontotheprogramissubjecttoreviewbytheBHSCSteeringCommitteeandtheuniversities internal regulations.
Afterthe2yearprogram,twooralexamsareconductedbytwointer-universitypanels,each
havingtwoexaminers,atleastoneofthemwhohasto have a PhD. The student may choose to have the examination conducted in Dutch, French or English.
Theresultoftheexamissimplyapassorfail.ApassearnsthecandidateaCertificate.Astudentwhofails,mayrequestaperformancereport.Onere-exammaybeattemptedwithin3months.
Feedbackbystudentsforqualityimprovementisdoneonthetopics,sessionsandspeakersaftereach session.
Thefirstcyclerunsfrom2018-2020.Moreinformationcanbehadfrom:https://www.bhsc.be/
MEMBER SOCIETY NEWS
ASSOCIATION OF CHINESE-SPEAKING HAND SURGEONS UNITED
The annual event, The Jixia Hand Surgery Forum, washeldinTianjin,June13-16,2019,co-or-ganisedbyTianjinHospital,togetherwithNantongUniversity, Shandong Provincial Hospital and BeijingJishuitanHospital.TheForumwaspairedwithPre-IFSSHmeetingorganisedbytheAssociationofChinese-speakingHandSurgeonsUnitedinTianjin.
The Forum and pre-IFSSH meeting were attended bymorethan500handsurgeonsfrommain-land China and other countries. The entire events werelivebroadcastedthroughWechatalloverChina, with over 2,000 hand surgeons online watchingnationwide.Theyearlyforumisfeaturedwithsystematicpresentationsandlivelydebates.Inthisyear’sevent,thedebatesincludedfingertiprepair,positionofhandimmobilisation,insitucubitaltunnelreleaseversusanteriortranspositionoftheulnarnerve,treatmentofKienbock’sdisease,nervetransfer,nervesuper-chargingprocedures,selectionsoffreeflapsforsofttissuedefects,andtreatmentofcongenitalanomaliesofthehand.International attendees presented techniquesonfreeflaptransfers,biomechanicsofdistalradiusfractures,anddiagnosisofmediannervecompressionintheforearm.NightsessionsfeaturedlecturesfromDrs.DonLalondeandElisabetHagertontendonrepairandnervecompressionoftheupperextremities.Thenightsessions lasted until 10:20 in the evening.
Thepre-IFSSHmeetingfocusedonwide-awakesurgery in China, where wide-awake surgery isverypopular.InTianjinHospital,thehostofthemeeting, more than 20,000 patients underwentwide-awake surgery in the past 3 years. This is perhaps the largest case series in a single unit inthe past 3 years. Other hospitals in China, including
Nantong University, Shandong ProvincialHospital,QiluHospitalofShandongUniversity,and Jiangyin People’s Hospital, popularly use this approach.ThepresentationsfromoutsidemainlandChinaincludedaseriesoftalksfromDrs.DonLalonde,ElisabetHagert,GregoryBain,andSang-HyunWooontheirusesofthisapproach.
Drs. Carlos Henrique Fernandes and Shanshan Jing introducedhandsurgeryinBrazilandUK.Freepapersontreatmentofdistalradialfracture,wristarthroscopy,digitalsensateflaptransfers,fingerjointreplacement,andhandfractures.Thepre-meetingconcludedwithanightboattourinHaihe,withastonishingviewsoftheTianjinskyline and historic area along the Haihe.
TheForumwillbeheldnextyearinBeijing,andwillbeorganisedbyBeijingJishuitanHospitalin April, 2020.
ThephotosarefromtheForumandpre-IFSSHmeeting
36 37
August 2019www.ifssh.info

JOURNAL HIGHLIGHTSMEMBER SOCIETY NEWS MEMBER SOCIETY NEWS
ECUADORIAN HAND SURGERY SOCIETY (ECUMANO)
AbriefhistoryHand surgery in Ecuador has an interesting beginning.In1964thefirsthandtransplantintheworldwasdoneinthecityofGuayaquil,performedbyDrRobertoGilbertElizaldeandhissurgicalteam.Thiscausedinternationalinterest.AteamfromBoston, USA visited to study the case.
Despitethisfactandforsomeotherreasons,thedevelopmentofhandsurgeryasaspecialtyinEcuador was very slow. It was not until 5 years ago thatagroupofspecialistsinhandsurgerysawthe need to have an entity which would unite the EcuadorianHandSurgeons.Beforethen,itwasonly the Ecuadorian Orthopedics and Traumatology Society which had chapter dedicated to hand pathology.
During the 2016 IFSSH Congress in Buenos Aires, this steering group met in a restaurant and signedadocumenttoestablishtheEcuadorianSocietyforSurgeryoftheHand(ECUMANO).ThisdocumentisseenasthecharterofECUMANO(ActofFoundation).LegalstatusoftheSocietytooksometimeandwasofficiallyrecognizedon17May2019bytheEcuadorianPublicHealthMinistry(MinisterialAgreement360-2019).
SinceECUMANOShasbeenmeetingandbeeninexistenceactivelypromotinghandsurgeryforthe
last 3 years in Ecuador, the current IFSSH President MarcGarcia-EliasencouragedourSocietytojointheIFSSHasafullMemberSociety.TheEcuadorianSocietywasvotedthe60thMemberoftheIFSSHinBerlin in June 2019.
DuringtheshortexistenceofourSociety,wehaveorganizedseveralnationalcourses,WebinarswithforeigncolleaguesfromMemberSocieties,andhaveparticipated in international congresses, such as theBi-nationalColombo-VenezuelanCongressandthe 2018 FESSH Congress in Copenhagen.
CurrentlyECUMANOhas5foundingmembers,10associatemembersand4aspiringmembers.WeexpectakeengrowthofmembershipnowthatourSocietyhasbecomeaMemberoftheinternationalhandsurgeryfamily.Thiswillcertainlyboostourefforttoimprovethegeneralstandardofhandsurgery in our country.
BRAZILIAN SOCIETY FOR SURGERY OF THE HAND (SBCM)
1. The 39th Brazilian Congress for Surgery of the Hand
The39thBrazilianCongressforSurgeryoftheHandwillbeheldfrom1-3AugustinthecityofGramado,inthesouthernregionofBrazil.Thisyeartherewillbealargenumberofinternationalspeakers:FranciscoSoldado(Spain),JamesCalandruccio(USA),JeffreyGreenberg(USA),JorgeClifton(Mexico),MichaelHousman(USA),andRonaldo
Carneiro,aBrazilianfromNaples–USA,whowillbeourHonoredGuest.
TheinvitednationalMemberSocietywillbeIsrael. With an impressive delegation, the Israeli colleagues will share their experiences on various waystotreatinjuries.
Thisyear’sprogramfocusesonnewtreatmentsanddebates.Wewantparticipantstosharetheirideas,clarifydoubts,andsharestories.“Thelecturesaregreattoolsforgettingtoknowsomethingnew,butthediscussionsaretheonestostrengthenlearning,” says SBCM’s Vice President and the 39th CBCM’s President Milton Pignataro.
Formoreinformation,refertothesite:www.mao2019.com.br.
2. The Brazilian Society for Surgery of the Hand actively participated in the 14th IFSSH Congress in Berlin, June 2019
From 17-21 June, during the 14th IFSSH Congress inBerlin(InternationalFederationofSocietiesforSurgeryoftheHand),about120membersoftheBrazilianSocietyforSurgeryoftheHandactivelyparticipatedinthescientificprogram.Itwasoneofthe largest delegations among the 92 participating countries.
TheBrazilianSociety(SBCM)presentedRiodeJaneirotohostthe2025IFSSHCongressandforthat purpose it developed certain actions such asthepresentationofawell-structuredbiddingprocess,withinformationaboutthecityofRioandtheinfrastructureavailablefortheevents,aswellasabookaboutthe60yearsofexistenceoftheBrazilianSocietyforSurgeryoftheHandwhichiscelebratedthisyear.ThismaterialwassenttoallthedelegatesoftheIFSSHMemberSocietiesbeforehand.
Unfortunately,Brazilwasnotthecountrychosen,butthefeelingremains:“WearesurethatwehavedoneourbestfortheSociety.Wearealsosurethatalotstillhastobedone,especiallybythenewgenerationofhandsurgeonsinBrazil.“TopresentBrazilandSBCMtointernationalcolleagueswasaunique experience”, says SBCM’s President Marcelo RosadeRezende.
3. Brazilian surgeons are honored as “Pioneers of Hand Surgery”
Every three years, during the IFSSH Congress, surgeonsfromallovertheworldarehonoredas“PioneersofHandSurgery”.AttheIFSSHCongressinBerlin,theBraziliansClaudioHenriqueBarbieri,and Edie Benedito Caetano, were among the other Pioneers honored.
ClaudioHenriqueBarbieriwasinGermanytoreceive his award while Edie Benedito Caetano could not attend the ceremony and was represented bytheSBCM’ssecretary,SamuelRibak.
38 39
August 2019www.ifssh.info
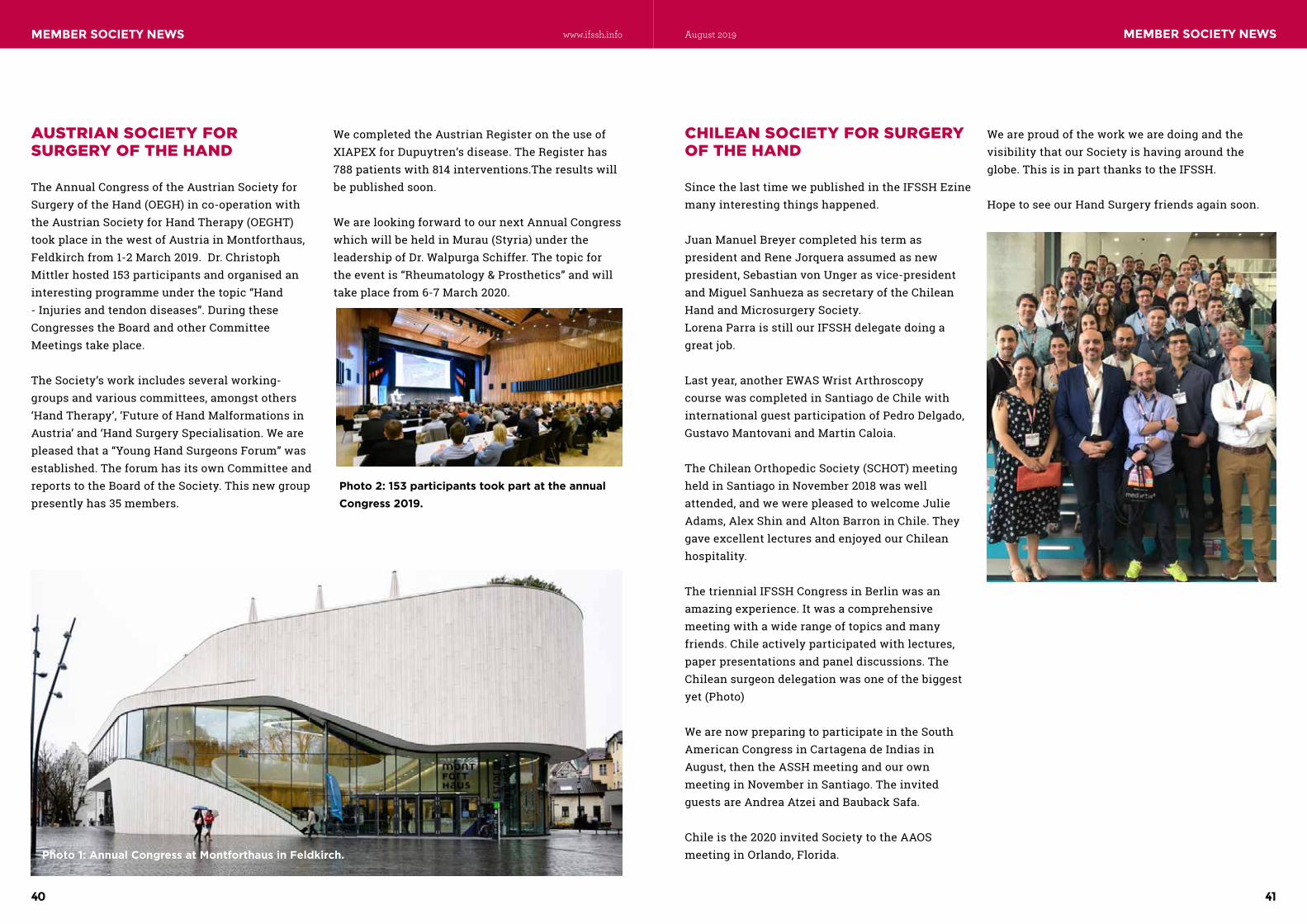
JOURNAL HIGHLIGHTSMEMBER SOCIETY NEWS MEMBER SOCIETY NEWS
AUSTRIAN SOCIETY FOR SURGERY OF THE HAND
TheAnnualCongressoftheAustrianSocietyforSurgeryoftheHand(OEGH)inco-operationwiththeAustrianSocietyforHandTherapy(OEGHT)tookplaceinthewestofAustriainMontforthaus,Feldkirchfrom1-2March2019.Dr.ChristophMittler hosted 153 participants and organised an interesting programme under the topic “Hand -Injuriesandtendondiseases”.DuringtheseCongresses the Board and other Committee Meetings take place.
The Society’s work includes several working-groups and various committees, amongst others ‘HandTherapy’,‘FutureofHandMalformationsinAustria’ and ‘Hand Surgery Specialisation. We are pleasedthata“YoungHandSurgeonsForum”wasestablished.TheforumhasitsownCommitteeandreportstotheBoardoftheSociety.Thisnewgrouppresentlyhas35members.
WecompletedtheAustrianRegisterontheuseofXIAPEXforDupuytren’sdisease.TheRegisterhas788 patients with 814 interventions.The results will bepublishedsoon.
WearelookingforwardtoournextAnnualCongresswhichwillbeheldinMurau(Styria)undertheleadershipofDr.WalpurgaSchiffer.Thetopicfortheeventis“Rheumatology&Prosthetics”andwilltakeplacefrom6-7March2020.
Photo 1: Annual Congress at Montforthaus in Feldkirch.
Photo 2: 153 participants took part at the annual Congress 2019.
CHILEAN SOCIETY FOR SURGERY OF THE HAND
SincethelasttimewepublishedintheIFSSHEzinemany interesting things happened.
Juan Manuel Breyer completed his term as presidentandReneJorqueraassumedasnewpresident,SebastianvonUngerasvice-presidentandMiguelSanhuezaassecretaryoftheChileanHand and Microsurgery Society.Lorena Parra is still our IFSSH delegate doing a greatjob.
Last year, another EWAS Wrist Arthroscopy course was completed in Santiago de Chile with internationalguestparticipationofPedroDelgado,Gustavo Mantovani and Martin Caloia.
TheChileanOrthopedicSociety(SCHOT)meetingheldinSantiagoinNovember2018waswellattended, and we were pleased to welcome Julie Adams, Alex Shin and Alton Barron in Chile. They gaveexcellentlecturesandenjoyedourChileanhospitality.
The triennial IFSSH Congress in Berlin was an amazingexperience.Itwasacomprehensivemeetingwithawiderangeoftopicsandmanyfriends.Chileactivelyparticipatedwithlectures,paper presentations and panel discussions. The Chileansurgeondelegationwasoneofthebiggestyet(Photo)
We are now preparing to participate in the South American Congress in Cartagena de Indias in August, then the ASSH meeting and our own meetinginNovemberinSantiago.TheinvitedguestsareAndreaAtzeiandBaubackSafa.
Chile is the 2020 invited Society to the AAOS meeting in Orlando, Florida.
WeareproudoftheworkwearedoingandthevisibilitythatourSocietyishavingaroundtheglobe.ThisisinpartthankstotheIFSSH.
HopetoseeourHandSurgeryfriendsagainsoon.
40 41
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
Images from the IFSSH/IFSHT Congress in Berlin June 2019
42 43
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
44 45
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
46 47
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
48 49
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
50 51
August 2019www.ifssh.info

JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
52 53
August 2019www.ifssh.info
JOURNAL HIGHLIGHTSSHARE SECTION JOURNAL HIGHLIGHTS SHARE SECTION
54 55
August 2019www.ifssh.info

UPCOMING EVENTS
CRISTINA ALEGRI INNOVATION AWARDA blinded IFSHT international evaluation committee chose Judy Bell-Krotoski posthumously for her contribution to the development and standardization of the Semmes Weinstein monofilaments for sensory testing. She was chosen from eight nominees.
IFSHT LIFETIME ACHIEVEMENT AWARD The NEW Lifetime Achievement Award has been devel-oped to recognise therapists who have made outstand-ing contributions to hand therapy internationally. Their contributions will influence many generations to come.
IFSSH EZINEThe IFSHT contribution to the May 2019 IFSSH EZINE is a valuable resource for hand therapist clinicians: “Improving thumb MCP joint stability with a simple lightweight splint” by Sarah Ewald (CH).
IFSHT is keen to have interesting, clinically relevant articles to con-tribute to the IFSSH Ezine. Contact [email protected] to contribute or if you have a suggested
For hand therapy educational events, go to “National/International Education Events” under “Education” at www.ifsht.org.
11TH IFSHT TRIENNIAL CONGRESS: BERLIN, GERMANY The 11th IFSHT and the 14th IFSSH Triennial Con-gresses June 2019 in Berlin saw THE BIGGEST GATH-ERING EVER IN THE WORLD OF HAND THERAPISTS AND HAND SURGEONS. Of the 4,001 attendees from 92 countries, more than 700 were hand therapists !!!
The four-day programme was packed with instructional lectures, scientific paper presentations, workshops and more than 150 e-posters. Special thanks to Natascha Weihs & Beate Jung who co-chaired the IFSHT Congress and many thanks to Ms. Jung and Dorit Aaron who co-chaired the scientific committee, and Lisa O’Brien, who chaired the abstract review committee, for developing such an educationally stimulating program.
2019-2022 IFSHT EXECUTIVE Six therapists have volunteered to lead IFSHT in the coming three years. Contact details for all EXCO members can be found at www.ifsht.org.
L to R: Anne Wajon (AU), Past-President; Nicola Goldsmith (UK), President; Peggy Boineau (USA), President-Elect; Maureen Hardy (USA), Secretary General; Susan de Klerk (SA), Information Officer and Stacey Doyon (USA), Treasurer.
L to R: D Thomas (FR), J-C Rouzaud (FR), C van Velze (SA), R Prosser (AU), M Persson (SE) (rear), V Frampton (UK) L Feehan (CA) (rear), P McKee (CA), A Estrada (CO), S Chinchalkar (CA), J Colditz, (US) and A Wajon (AU), IFSHT President. E Mackin (US) and A Leveridge (UK) were unable to attend to receive their awards.
Anne Wajon, IFSHT President, (at podium) recognizes the German Organizing Committee: L to R are Katja Karasev, Natascha Weihs, Beate Jung, Johanna Ismaier, Christine Popp, and Dominik Simon
1 2 t h Tr i e n n i a l I F S H T C o n g r e s s | L o n d o n , E n g l a n d | J u n e 2 7 -J u l y 1 , 2 0 2 2 | w w w. i f s s h - i f s h t 2 0 2 2 . c o . u k
VOL 13 NO 3 | JULY 2019
UPCOMING EVENTS
56 57
August 2019www.ifssh.info

November 7~9, 2019
Seoul St. Mary's Hospital, Seoul, South Korea
Abstract Submission Deadline: July 31, 2019
Abstract Acceptance Announcement: August 31, 2019
Early Bird Registration Deadline: September 30, 2019
Website: http://www.APWA2019.com
Secretariat of APWA 2019124, Bukbyeonjung-ro, Gimpo-si, Gyeonggi-do, Republic of Korea 10098Phone : +82-31-987-5963 Fax : +82-31-987-5967E-mail : [email protected]
UPCOMING EVENTS UPCOMING EVENTS
58 59
August 2019www.ifssh.info
UPCOMING EVENTS UPCOMING EVENTS
Foundation for Hand Surgery
Campus Biotech Innovation Park, Bâtiment F2/F3, Avenue de Sécheron 15, CH-1202 Geneva, Switzerland Tel: +41 225 45 12 92 - [email protected]
www.foundation-handsurgery.org nonprofit organization
To European Societies for Surgery of the Hand
We set up the Hand Surgery Foundation dedicated to Education and Research in Hand Surgery.
The Foundation for Hand Surgery is a non-profit European organization, independent, without industrial support or conflict of interest. The status of the foundation based in Geneva can be consulted on the website www.foundation-handsurgery.org.
Its aim is to offer additional training opportunities for hand surgeons at all stages of their professional training, from the early years to the final stages of perfecting their already acquired technical skills.
Education program includes both junior sessions for surgeons-in-training and senior sessions. The "senior" sessions are intended primarily for surgeons wanting to benefit from the experience of expert surgeons with a reputation on a particular issue. Many invited experts from Europa are part of the education training program.
The sessions are organized in Geneva (Swiss Foundation for innovation and training surgery- SFITS- Geneva University Hospital) and at the School of Surgery in the microsurgery laboratory (Nancy, Fr).
The program of the next training modules over a period of three months, is below.
Applicants participating in the training will be able to register on the dedicated site www.foundation-handsurgery.org. We hope to see you and share our experiences.
The Foundation does not belong to anyone; its aim is to be there for everyone.
Best regards,
Gregoire Chick, Gilles Dautel, Philippe Bellemère, Bruno Lussiez, Alain Tchurukdichian
Scientific Board G. Chick (CH) G. Dautel (FR) P. Bellemère (FR) B. Lussiez (MC) A. Tchurukdichian (FR) Scientific Commitee M. Ceruso (IT) A. Ferreres (SP) M. Garcia-Elias (SP) E. Hagert (SE) M. I. Winge (NO) Contact [email protected]
EWAS ISTANBUL, TURKEY
SEPTEMBER 20-21, 2019
5th WRIST ARTHROSCOPY COURSE
UNIVERSITY OF HEALTH SCIENCESBALTALIMANI BONE DISEASES
TEACHING AND RESEARCH HOSPITAL
CHAIRPERSONS
Prof. Dr. Kahraman OZTURK & Prof. Dr. Tufan KALELI
SCIENTIFIC SECRETARIATProf. Dr. I. Bulent OZCELIK
Asst. Prof. Dr. Ayse SENCAN
(with International Participation)http://www.wristarthroscopyturkey.org/
60 61
August 2019www.ifssh.info
UPCOMING EVENTS UPCOMING EVENTS
3rd ‘Overseas Day’ SymposiumEffective Teaching across Cultures in Global Surgery
13 September 2019 | 09:00 - 17:00
LocationRoyal College of Surgeons of Edinburgh
A one-day symposium for anyone interested in overseas work in developing countries, particularly in the fields of plastic or hand surgery.
Topics for Discussion:• How to Get Involved in Surgical Work Overseas• Cultural Factors in Global Surgical Training Expert speaker Local surgeons from across the globe give personal insights• Making use of Technology in Global Surgical Teaching• Designing Surgical Curriculum for the Local Environment
Intended Audience:• Consultant Volunteers• Therapists• Trainees
Places are limited and are secured by giving your credit card details to the BSSH office - no money will be taken but non-attendance will cost £50. Please complete and return the form overleaf if you wish to attend
62 63
August 2019www.ifssh.info

12APFSSH/8APFSHT12th Asian Pacific Federation of Societies for Surgery of the Hand &
the 8th Asian Pacific Federation of Societies of Hand Therapists Triennial Meeting 11-14 March 2020 | Melbourne Convention and Exhibition Centre
apfssh2020.org
We look forward to seeing you in Melbourne from the 11th - 14th March 2020, to learn, be inspired, network with colleagues and enjoy everything Melbourne has to offer.
WEB apfssh2020.org • CONTACT US [email protected]
UPCOMING EVENTS
64 65
August 2019www.ifssh.info