refer, don’t defer; coordinating with sleep specialists ... · request treatment of primary...
TRANSCRIPT
Refer, Don’t Defer; Coordinating with Sleep Specialists for Stable Outcomes
Nicole D. Chenet, DDS, DABDSM 200 Commerce Dr. Suite 203, Moon Twp Pa AGH Center for Sleep Medicine, 490 East North Ave , Suite 309, Pgh Pa 412-367-0367 Fax: 412-367-0366 www.sadcpgh.com

Nicole D Chenet, DDS
Diplomate of the AmericanBoard of Dental Sleep Medicine
Nicole D. Chenet, DDS, DABDSM 200 Commerce Dr. Suite 203, Moon Twp Pa AGH Center for Sleep Medicine, 490 East North Ave , Suite 309, Pgh Pa 412-367-0367 Fax: 412-367-0366 www.sadcpgh.com

2015 practice parameters of the American Academy of Sleep Medicine (AASM)
• The clinical practice guideline comprises the following recommendations:
• 1. We recommend that sleep physicians prescribe oral appliances, rather than no therapy, for adult patients who request treatment of primary snoring (without obstructive sleep apnea). (STANDARD)
• 2. When oral appliance therapy is prescribed by a sleep physician for an adult patient with obstructive sleep apnea, we suggest that a qualified dentist use a custom, titratable appliance over non-custom oral devices. (GUIDELINE)
• 3. We recommend that sleep physicians consider prescription of oral appliances, rather than no treatment, for adult patients with obstructive sleep apnea who are intolerant of CPAP therapy or prefer alternate therapy. (STANDARD)
Hi

• 4. We suggest that qualified dentists provide oversight - rather than no follow-up - of oral appliance therapy in adult patients with obstructive sleep apnea, to survey for dental-related side effects or occlusal changes and reduce their incidence. (GUIDELINE)
• 5. We suggest that sleep physicians conduct follow-up sleep testing to improve or confirm treatment efficacy, rather than conduct follow-up without sleep testing, for patients fitted with oral appliances. (GUIDELINE)
• 6. We suggest that sleep physicians and qualified dentists instruct adult patients treated with oral appliances for obstructive sleep apnea to return for periodic office visits - as opposed to no follow-up - with a qualified dentist and a sleep physician. (GUIDELINE)

Who do we coordinate care with ?
• Ear Nose and Throat/ Sleep Physicians • Pulmonary/Sleep Physicians • Primary Care • Oral and Maxillofacial Surgeons • Orthodontists • Cardiology • Psychiatry

The Comprehensive Initial Exam
• Make sure you obtain all physicians the patient sees that need to be aware that you are treating their OSA with an oral device
• A thorough exam not only the oral environment, but also the sino-nasal area as well. Ask the patient about any nasal symptoms they may be experiencing.
• A thorough review of medications and past medical history.
• Prepare and explain to the patient , the anatomical concerns that may impact your final outcomes.
Comorbidities Associated with Obstructive Sleep Apnea: a Retrospective Study José Antonio Pinto,1,2 Davi Knoll Ribeiro,1,2 Andre Freitas da Silva Cavallini,1,2 Caue Duarte,1,2 and Gabriel Santos Freitas1,2
Comorbidities occurred in 56.2% patients diagnosed with mild OSA, 67.6% with moderate OSA, and 70% of patients with severe OSA.
100 patients with OSA (84 men,16 women) hypertension (39%) obesity (34%) depression (19%) gastroesophageal reflux disease (GERD) (18%) diabetes mellitus (15%) hypercholesterolemia (10%) asthma (4%)
Medications that impact Sleep Disordered Breathing
• Antidepressants - Tricyclic Antidepressants-Amitriptyline. Amoxapine. Desipramine (Norpramin) Doxepin. Imipramine (Tofranil) Nortriptyline (Pamelor) Protriptyline (Vivactil) Trimipramine (Surmontil)
• Narcotics- Oxycotin, Percocet, Lorcet
• SSRI- Selective serotonin reuptake inhibitors-Escitalopram (Lexapro), Fluoxetine (Prozac), Paroxetine (Paxil, Pexeva), Sertraline (Zoloft), Vilazodone (Viibryd), Citalopram (Celexa)
• Depakote - Valproic Acid- bipolar depression/ some forms of migrane
• Atypical Antipsychotics- Abilify, Risperdal, Seroquel, Zyprexa
• Prednisone
• Antihistamines- Allegra, Zyrtec
• Insulin
• Beta blockers - Atenolol, Metoprolol, Propanolol

Patient example
• Margie-57 y/o, BMI- 29.5, • Baseline AHI= 43.2, Nadir=81%, time below 90%=
19% • Patient of my practice since 2013. • PMH= Hypertension, Depression/Anxiety • Medications=Effexor 150 mg, Lipitor • TAP appliance in 2013, replaced with Herbst
appliance in 2017. • On follow up visit - significant EDS and husband
reports she is snoring.

In Lab PSG with Oral Appliance Titration
ENT/Sleep Referral-DISE
• Nose is clear • No septal obstruction • No unusual excessive lateral pharyngeal
wall component • Despite use of heavy rubber bands with
Herbst appliance, patient’s mouth continues to drop open causing obstruction.

Final Outcome
• Replaced her Herbst with a TAP post PSG results and DISE study. • Patient is a significant “mouth dropper”. • Rubber bands were not enough to keep her mouth closed. • Patient’s Effexor was decreased from 150 mg down to 37.5mg,
coordinated with her PCP • BMI has increased to 35. • AHI=13.5, 22, 24,5 (three night HST), Nadir=66% , Time below
90%=10% • Symptomatically, her EDS significantly improved, reports of
large decrease in snoring and sleep interruption and she is dreaming again. Patient is motivated to lose 20 lbs and will retest again in near future.
Pulmonary Referrals
• COPD- Overlap Syndrome • Congestive Heart Failure • Pulmonary Hypertension • Obesity Hypoventilation Syndrome • Acute Pulmonary Embolism • Venous Thromboembolism • Polycystic Ovarian Syndrome

Cardiology Referrals
• Atrial fibrilation • Hypertension (uncontrolled hypertension ) • Congestive Heart Failure • Pulmonary Hypertension • Cardiomyopathy • Ischemic Heart Disease
Obstructive Sleep Apnea and Cardiovascular Comorbidities A Large Epidemiologic Study Hanna Gilat, MD, Shlomo Vinker, MD, Inon Buda, MD, Ethan Soudry, MD, Michal Shani, MD, MPH, and Gideon Bachar, MD

Patient Example
• Ron- 73 y/o, 6’5”, BMI= 27.3 • Initial AHI= 9/hr, supine AHI=30hr • Symptoms- EDS, sleep interruption (4-5
times a night), frequent nocturia, snoring, naps during daytime.


Follow up in lab PSG
• Symptomatically- less EDS, less snoring, only awakens 1-2 times a night
• AHI= 26/hour , supine AHI=60/hr, 40 central apneas
• Recently had a defibrillator placed for Congestive heart failure.
• Determined best with OA and ASV pap combination.

Ear, Nose and Throat Care Coordination
• Review your panorex or CBCT • Assess nasal turbinates, nasal septum,
tonsils, soft palate lateral pharyngeal walls
• Perform the Cottle Test

Nasal Assessment
• Positive Cottle Test- Obstruction is occurring at the nasal valve and/or turbinates are swollen/inflamed
• Guide the patient with conservative measures
• (Saline rinse, Nasal Steroid Spray, MUTE nasal dilators or Breath right Strips for nighttime use)

Nasal Assessment
• Negative Cottle Test- The patient may have bony obstruction present (septal deviation) if they are also symptomatic for chronic nasal congestion.
• The patient can attempt conservative measures (ie, Afrin) for 4-5 days to see if there is any symptomatic improvement, if not, schedule with the ENT.
• Aid in determining whether their snoring/symptoms is strictly from the nose or multi-level

Hypertrophy of nasal turbinates

Conservative ENT measuresBaseline Sleep Test? Yes Type: HST Baseline - View Study Most Recent: 98 months ago - 01/17/2010 Diagnosis: G47.33 - OBSTRUCTIVE SLEEP APNEA AHI/RDI: 21/ Low O2: 93% T < 90%: N/A
Recent Titration Type: HST Titration - View Study Most Recent: 8 months ago - 05/17/2017 Diagnosis: G47.33 - OBSTRUCTIVE SLEEP APNEA AHI/RDI: 0.9 / N/A Low O2: 91% T < 90%:
Achieved symptomatic improvement with Dymista, saline rinse, Breath right strips after ENT evaluation.


Surgical ENT Recommendations 1. Deviated Septum2. Turbinate Hypertrophy Patient had failed nasal steroid spray. Very symptomatic. Septoplasty and radio frequency turbinate ablation was completed.Baseline Sleep Test? Yes Type: PSG Baseline - View Study Most Recent: 15 months ago - 11/07/2016 Diagnosis: G47.33 - OBSTRUCTIVE SLEEP APNEA AHI/RDI: 26.3/ Low O2: 77% T < 90%: N/A
Recent Titration Type: HST Titration - View Study Most Recent: 7 months ago - 06/14/2017 Diagnosis: G47.33 - OBSTRUCTIVE SLEEP APNEA AHI/RDI: 4.9 / 4.9 Low O2: 85% T < 90%: N/A

Excessive Lateral Pharyngeal Walls
• Explain to the patient what you see on the initial exam. Make them aware that if we do not get a stable outcome with OA alone, will refer to ENT/Sleep Specialist that performs Expansion Sphincter Pharyngoplasty.


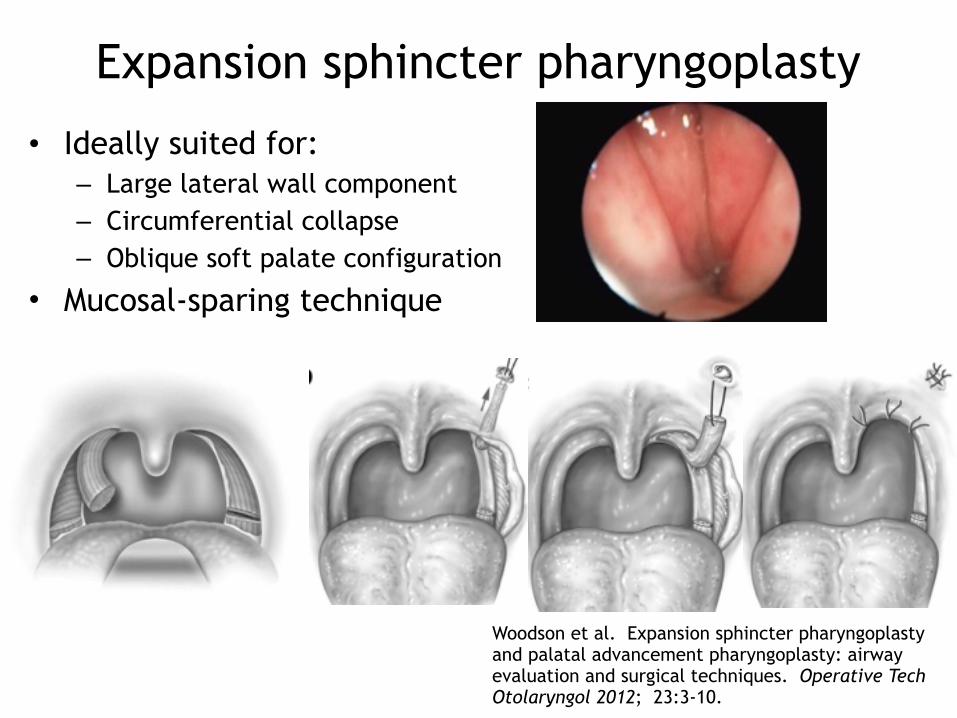
• Ideally suited for: – Large lateral wall component – Circumferential collapse – Oblique soft palate configuration
• Mucosal-sparing technique
Expansion sphincter pharyngoplasty
Woodson et al. Expansion sphincter pharyngoplasty and palatal advancement pharyngoplasty: airway evaluation and surgical techniques. Operative Tech Otolaryngol 2012; 23:3-10.
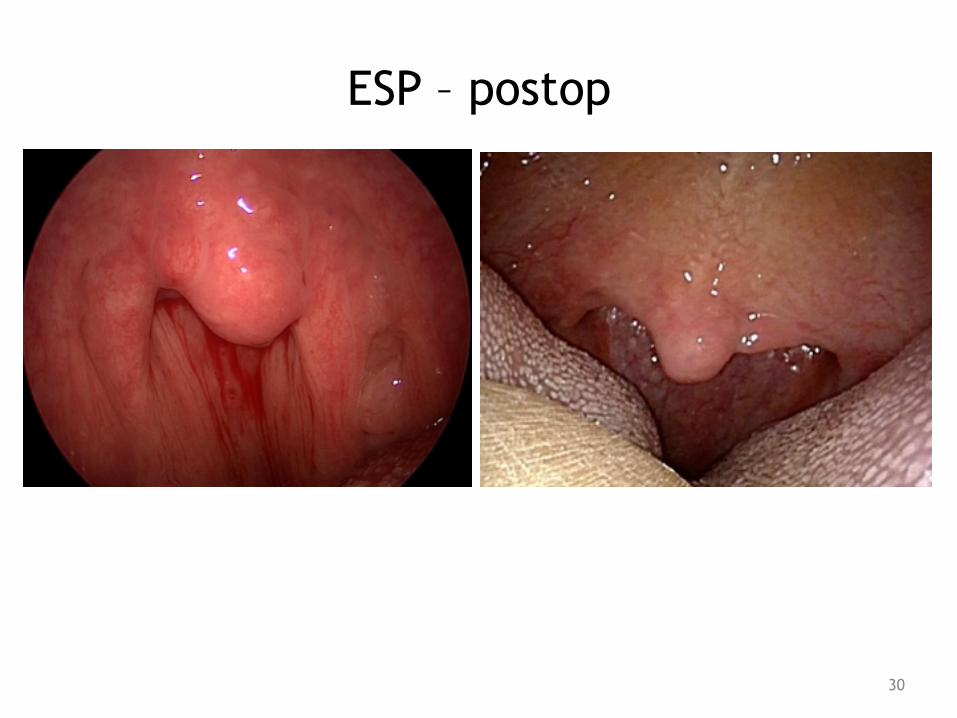
ESP – postop
30

Case #3: ESP + OAT
• S/P ESP and turbinate reduction
AHI LSAT T90 ESS
Baseline 116 65% 35% 14
OAT 55 58% 16% 7
ESP + OAT 2.1 80% 1% 1

Clinical Case
• Patient- 70 year old male • PMH- Brain injury (1997), Septoplasty,
Heart attack (2000), Restless leg syndrome, Severe nocturnal myoclonus
• Severe AHI- 39.5/ Nadir- 74%, time below 90%- 16 minutes
• AHI with oral appliance - Severe AHI- 40.1/Nadir-84%, time below 90%- 8 minutes

DISE- Drug Induced Sleep Endoscopy

Build your Team
• Difficult cases need a team of multi- level specialists
• Case involved ENT/Sleep/ OMFS and Dental Sleep in order to provide a positive outcome for the next patient.
• Patient had DISE completed prior to OMFS assessment for MMA/Genioglossus Advancement.
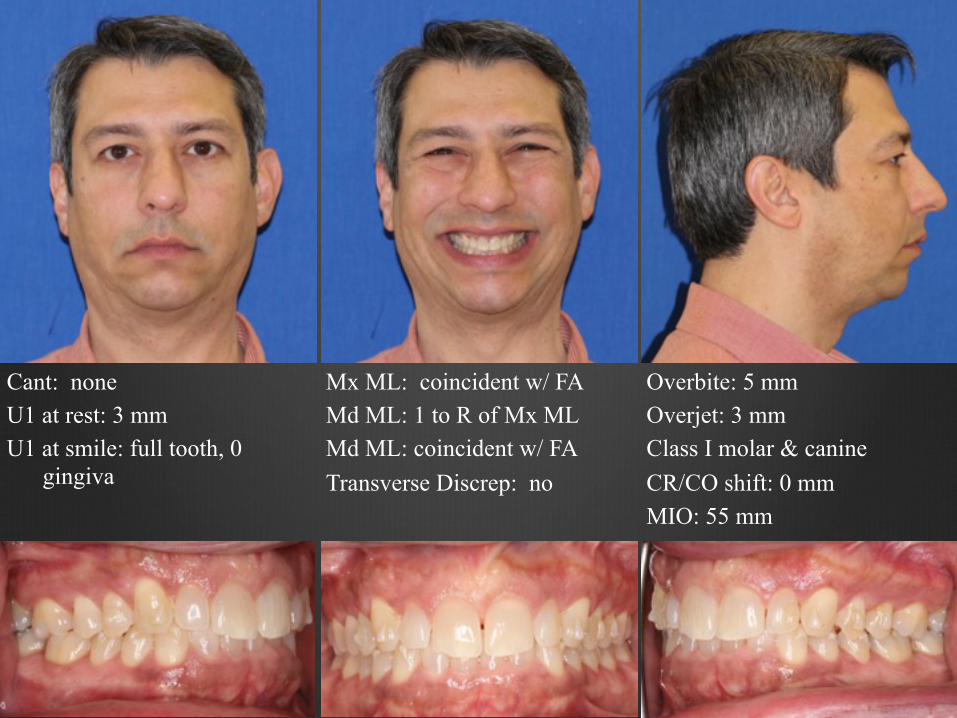
Cant: none U1 at rest: 3 mm U1 at smile: full tooth, 0
gingiva
Mx ML: coincident w/ FA Md ML: 1 to R of Mx ML Md ML: coincident w/ FA Transverse Discrep: no
Overbite: 5 mm Overjet: 3 mm Class I molar & canine CR/CO shift: 0 mm MIO: 55 mm
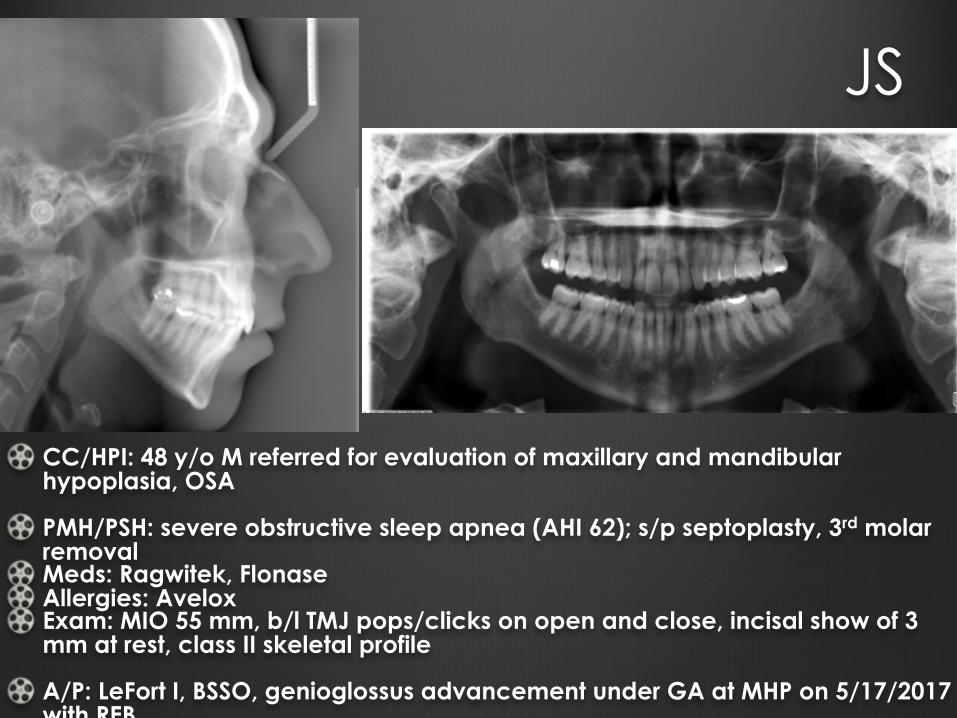
CC/HPI: 48 y/o M referred for evaluation of maxillary and mandibular hypoplasia, OSA
PMH/PSH: severe obstructive sleep apnea (AHI 62); s/p septoplasty, 3rd molar removal Meds: Ragwitek, Flonase Allergies: Avelox Exam: MIO 55 mm, b/l TMJ pops/clicks on open and close, incisal show of 3 mm at rest, class II skeletal profile
A/P: LeFort I, BSSO, genioglossus advancement under GA at MHP on 5/17/2017 with REB.
JS

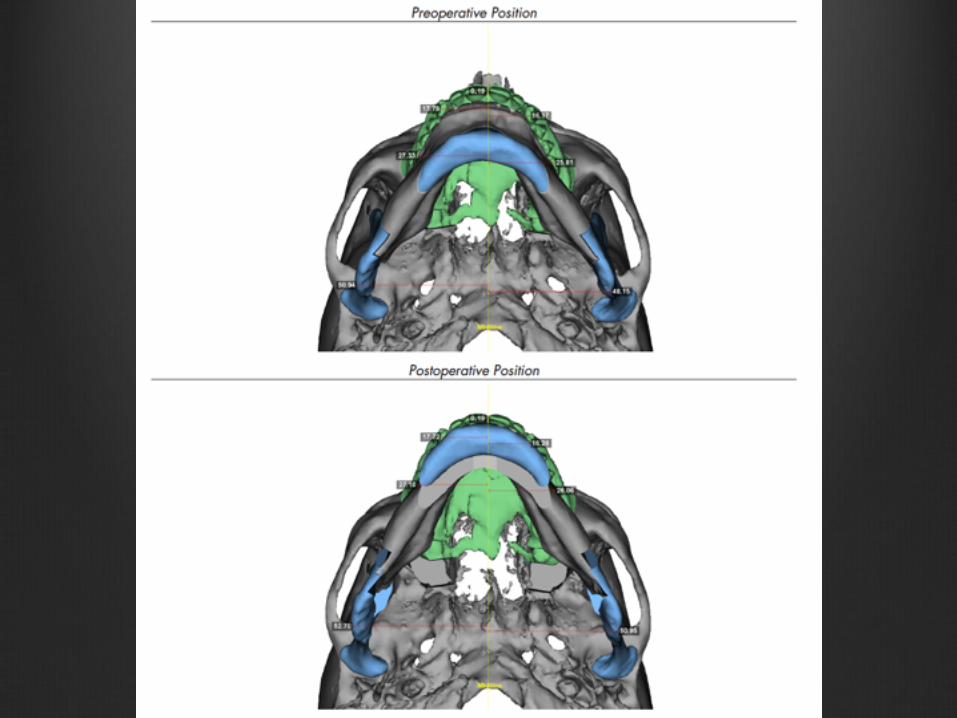



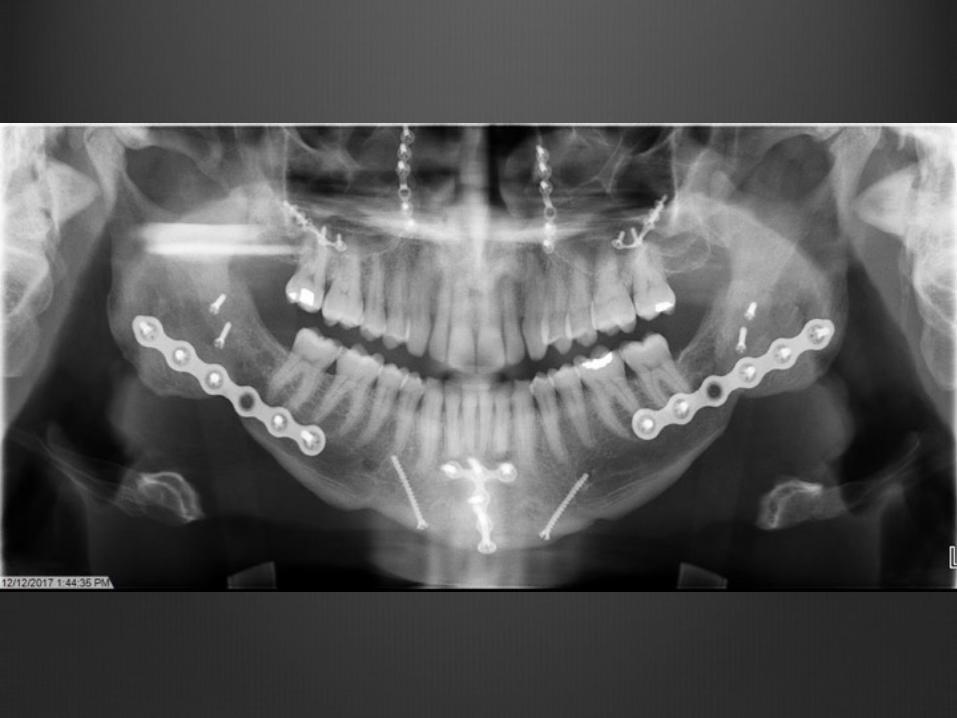

AHI-pre- 62/hr , Time below 90% O2=46%, Nadir=75% AHI-post MMA/Genioglossus Advancement- 11/hr, Time below 90%O2 = , Nadir=
Invisalign Refinement and oral appliance for residual AHI.

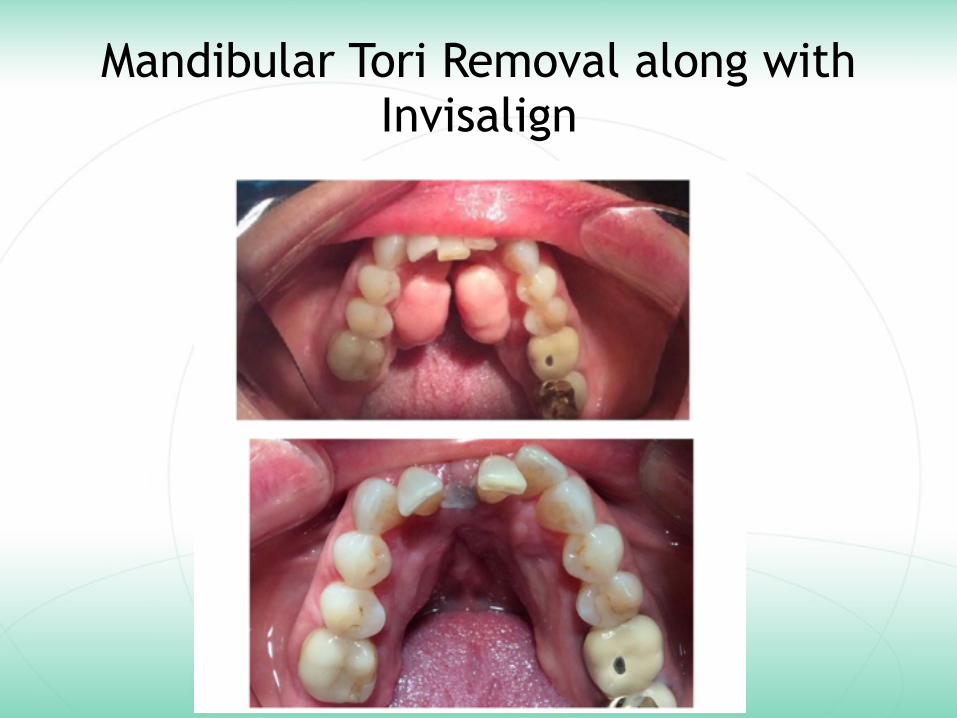
Mandibular Tori Removal along with Invisalign
Severe OSA
• Pre Tori Removal- AHI= 29, Nadir= 84%, speech impediment, EDS, headaches, very loud snore
• Post Tori Removal -AHI=

Invisalign with ASA appliance

Intraoral View

AHI is stable, but patient is still sleepy.
• Refer back to sleep physician • Rule out: Narcolepsy, Restless Leg
Syndrome, Insomnia, Periodic Limb Movement Disorder, Vitamin Deficiency (Vit D), REM behavior disorders
• It is not necessarily just the AHI that is impacting the patient.


Thank you!