reduction techniques in minimally invasive ... - acvs.org · cranio-medial approach the dog is...
TRANSCRIPT

REDUCTION TECHNIQUES IN MINIMALLY INVASIVE TRAUMATOLOGY Gian Luca Rovesti, DrMedVet, DECVS
Clinica veterinaria "M. E. Miller" – Cavriago – Italy
Fracture reduction implies restoring the original limb length and alignment. In mini-mally invasive osteosynthesis (MIO) this should be achieved without disrupting the local vas-cularization, and by means of a very reduced or closed surgical approach. The rationale be-hind fracture reduction by intraoperative skeletal traction (IST) is to counteract muscle con-traction. IST can be performed in different ways, but the most consistent results are usually achieved when using a specifically designed surgical table and by applying safe opposition and anchorage points. Standard procedures are described in this proceeding. ANTEBRACHIUM Cranio-medial approach The dog is positioned in lateral recumbency with the affected limb lowermost and the contralateral forelimb maintained against the thoracic wall with the shoulder flexed. The neck is extended. The limb that is to be subjected to traction is positioned with the midshaft of the humerus at the edge of the table. A dedicated traction stand is attached to the table caudal to the forelimb. Its short component is oriented cranially, so that traction can be exerted with the cranio-medial region of the antebrachium remaining completely unobstructed (Fig. 1 Left).
Figure 1 – Left: Position for IST of the radius-ulna with cranio-medial approach available. Right: The band crossing over the neck is passed over the stabilizer, to avoid causing pressure on the neck. Cranio-lateral approach The forelimb subjected to traction is placed uppermost with the dog positioned in lat-eral recumbency. The contralateral forelimb is flexed at the elbow and secured with the car-pus under the dog’s muzzle. In all other respects, the positioning of the dog and traction stand are the same as for the cranio-medial approach to the antebrachium. Opposition points Two bands are crossed over the sternum. A dorsal stabilizer is used on the dorsal area of the neck. The band crossing the upper surface of the neck region is passed over the stabi-lizer (Fig. 1 Right) so that excessive pressure on the base of the neck by this band is avoided. Anchorage points For this technique, traction belts applied to the carpo-metacarpal region of the fore-limb are most effective (Fig. 1 Left). Alternatively, in case of chronique, displaced or over-
212
riding fractures, a transosseous K-wire can be inserted through the distal epiphyseal region of the radius or through the metacarpal bones for anchorage to provide more distraction without risk of slippage. HUMERUS The dog is positioned in lateral recumbency with the affected limb uppermost, similar to that used for the cranio-lateral approach to the antebrachium. In order to exert axial traction on the humerus, the traction stand is placed caudal to the forelimb with the short component oriented caudally (Fig. 2 Left). Opposition points
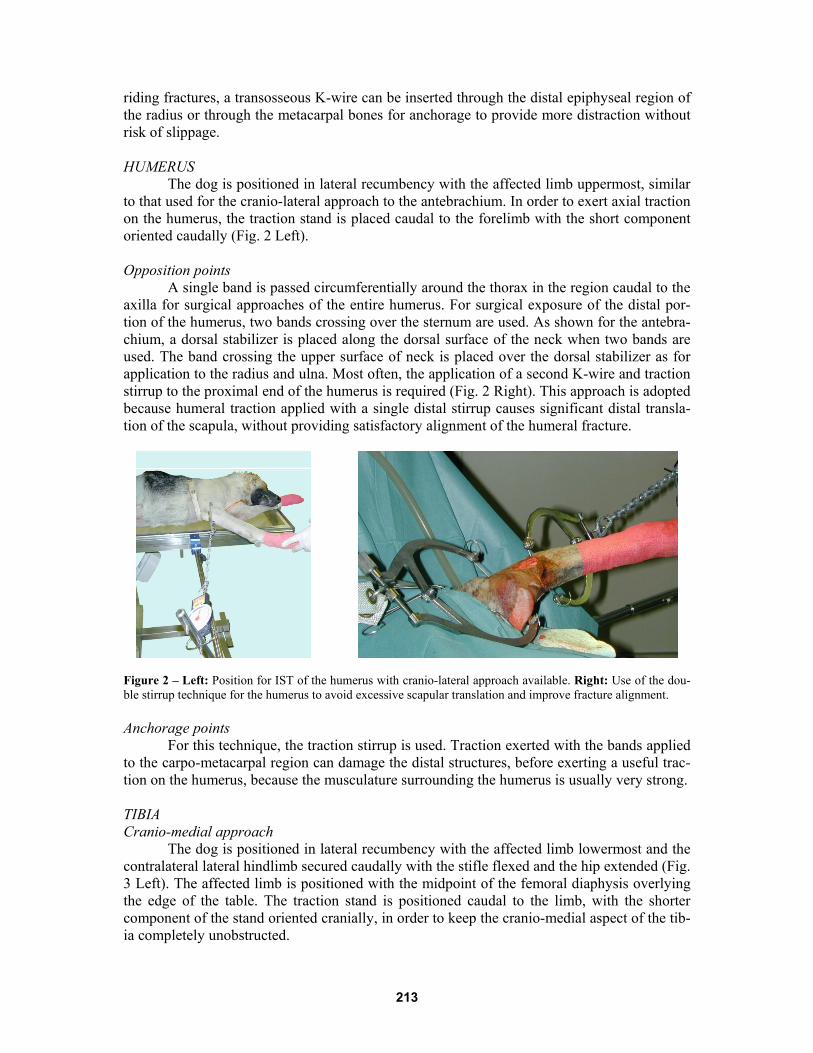
A single band is passed circumferentially around the thorax in the region caudal to the axilla for surgical approaches of the entire humerus. For surgical exposure of the distal por-tion of the humerus, two bands crossing over the sternum are used. As shown for the antebra-chium, a dorsal stabilizer is placed along the dorsal surface of the neck when two bands are used. The band crossing the upper surface of neck is placed over the dorsal stabilizer as for application to the radius and ulna. Most often, the application of a second K-wire and traction stirrup to the proximal end of the humerus is required (Fig. 2 Right). This approach is adopted because humeral traction applied with a single distal stirrup causes significant distal transla-tion of the scapula, without providing satisfactory alignment of the humeral fracture.
Figure 2 – Left: Position for IST of the humerus with cranio-lateral approach available. Right: Use of the dou-ble stirrup technique for the humerus to avoid excessive scapular translation and improve fracture alignment. Anchorage points For this technique, the traction stirrup is used. Traction exerted with the bands applied to the carpo-metacarpal region can damage the distal structures, before exerting a useful trac-tion on the humerus, because the musculature surrounding the humerus is usually very strong.
TIBIA Cranio-medial approach The dog is positioned in lateral recumbency with the affected limb lowermost and the contralateral lateral hindlimb secured caudally with the stifle flexed and the hip extended (Fig. 3 Left). The affected limb is positioned with the midpoint of the femoral diaphysis overlying the edge of the table. The traction stand is positioned caudal to the limb, with the shorter component of the stand oriented cranially, in order to keep the cranio-medial aspect of the tib-ia completely unobstructed.
213
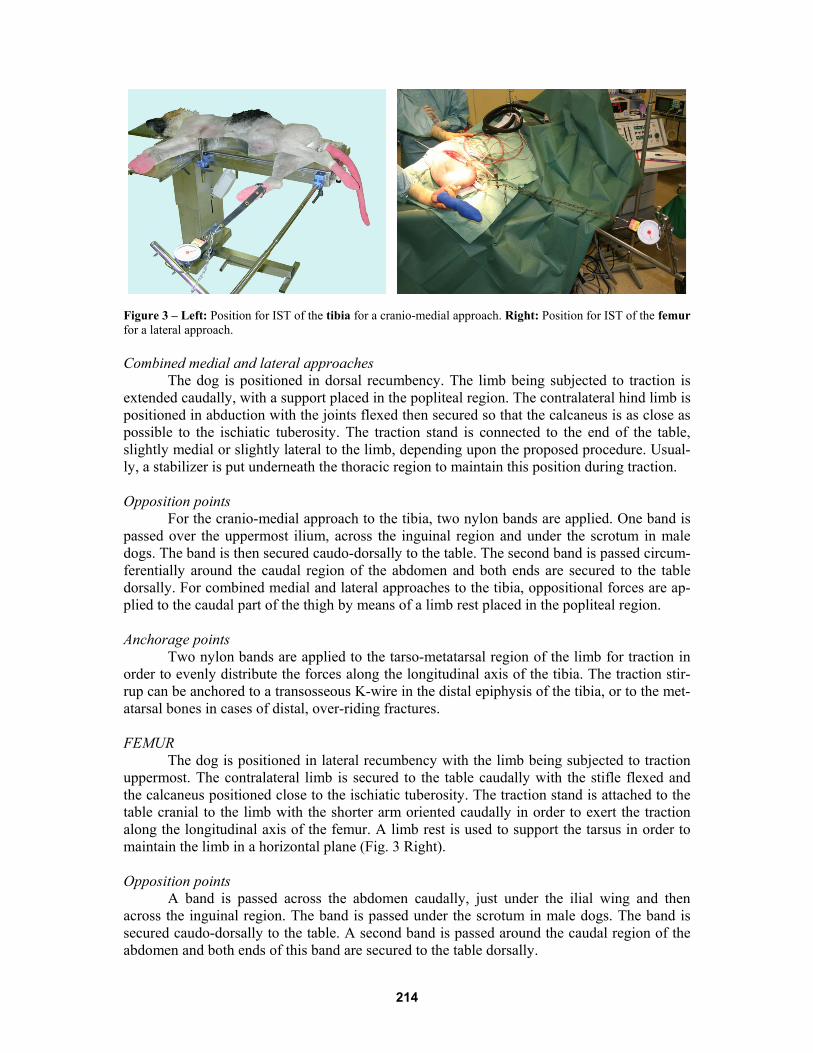
Figure 3 – Left: Position for IST of the tibia for a cranio-medial approach. Right: Position for IST of the femur for a lateral approach. Combined medial and lateral approaches The dog is positioned in dorsal recumbency. The limb being subjected to traction is extended caudally, with a support placed in the popliteal region. The contralateral hind limb is positioned in abduction with the joints flexed then secured so that the calcaneus is as close as possible to the ischiatic tuberosity. The traction stand is connected to the end of the table, slightly medial or slightly lateral to the limb, depending upon the proposed procedure. Usual-ly, a stabilizer is put underneath the thoracic region to maintain this position during traction. Opposition points For the cranio-medial approach to the tibia, two nylon bands are applied. One band is passed over the uppermost ilium, across the inguinal region and under the scrotum in male dogs. The band is then secured caudo-dorsally to the table. The second band is passed circum-ferentially around the caudal region of the abdomen and both ends are secured to the table dorsally. For combined medial and lateral approaches to the tibia, oppositional forces are ap-plied to the caudal part of the thigh by means of a limb rest placed in the popliteal region. Anchorage points Two nylon bands are applied to the tarso-metatarsal region of the limb for traction in order to evenly distribute the forces along the longitudinal axis of the tibia. The traction stir-rup can be anchored to a transosseous K-wire in the distal epiphysis of the tibia, or to the met-atarsal bones in cases of distal, over-riding fractures. FEMUR The dog is positioned in lateral recumbency with the limb being subjected to traction uppermost. The contralateral limb is secured to the table caudally with the stifle flexed and the calcaneus positioned close to the ischiatic tuberosity. The traction stand is attached to the table cranial to the limb with the shorter arm oriented caudally in order to exert the traction along the longitudinal axis of the femur. A limb rest is used to support the tarsus in order to maintain the limb in a horizontal plane (Fig. 3 Right). Opposition points A band is passed across the abdomen caudally, just under the ilial wing and then across the inguinal region. The band is passed under the scrotum in male dogs. The band is secured caudo-dorsally to the table. A second band is passed around the caudal region of the abdomen and both ends of this band are secured to the table dorsally.
214
Anchorage points For this traction technique, the traction stirrup anchored to a transcondylar K-wire placed in the distal end of the femur is used to more effectively overcome the strength of the thigh muscles. In addition, traction exerted with bands encircling the tarso-metatarsus may damage the distal structures (Fig. 3 Right). SUGGESTED READINGS 1. Aron DN, Palmer RH, Johnson AL. Biologic strategies and a balanced concept for re-
pair of highly comminuted long bone fractures. Comp Cont Educ Small Anim, 1995; 17:35-49.
2. Dueland RT. Open (compound) fractures. In: Brinker WO, Hohn RB, Prieur WD (eds). Manual of internal fixation in small animals, Springer-Verlag, Berlin, 1984;108.
3. Johnson AL. Current concepts in fracture reduction. Vet Comp Orthop Traumatol, 2003; 16: 59-66.
4. King KF, Rush J. Closed intramedullary nailing of femoral shaft fractures. A review of one hundred and twelve cases treated by the Kuntscher technique. J Bone Joint Surg Am, 1981 63:1319-1323.
5. Latte Y. Reduction de la fracture. In: Latte Y, Meynard J-A (eds). Manuel de fixation externe, Editions PMCAC, Paris, 1997; 117-124.
6. McCartney WT, Carmichael S. Talar neck fractures in five cats. J Small Anim Pract, 2000; 41:204-206.
7. Rovesti GL, Margini A, Cappellari G, Peirone B. Intraoperative skeletal traction in the dog. A cadaveric study. Vet Comp Orthop Traumatol, 2006; 19:9-13.
8. Wu CC. An improved surgical technique to treat femoral shaft malunion: revised reamed intramedullary nailing technique. Arch Orthop Trauma Surg, 2001; 121:265-270.
9. Rovesti GL, Margini A, Cappellari G, Peirone B. Clinical application of intraoperative skeletal traction in the dog. Vet Comp Orthop Traumatol, 2006; 19:14-19.
10. Guiot LP, Déjardin LM. Prospective evaluation of minimally invasive plate osteosyn-thesis in 36 nonarticular tibial fractures in dogs and cats. Vet Surg, 2011; 40:171-182.
215