recently highlighted non-neoplastic pathologic entities … · recently highlighted non-neoplastic...
TRANSCRIPT

REVIEW ARTICLE
Abbrenterliche
DISCto th
Copy0016http:
960
Recently highlighted non-neoplastic pathologic entities of theupper GI tract and their clinical significance
eviatioochromn plan
LOSURis artic
right ª-5107/$//dx.do
GAST
Changqing Ma, MD, PhD,1 Berkeley N. Limketkai, MD,2 Elizabeth A. Montgomery, MD1
Baltimore, Maryland, USA
Several non-neoplastic entities involving the esophagusand the stomach have been recently highlighted in themedical literature. Some of these entities are newly recog-nized and are often underdiagnosed because of insufficientawareness. Furthermore, much of the etiology, pathogen-esis, natural history, treatment, and patient outcomesremain unknown or only partially defined. The objectiveof this review is to increase familiarity with these entitiesamong gastroenterologists and pathologists alike with thegoal of promoting detection and increased reporting ofcases and ultimately improving our understanding of theseentities.
ESOPHAGITIS DISSECANS SUPERFICIALIS ORSLOUGHING ESOPHAGITIS
Some authors consider esophagitis dissecans superficia-lis (EDS) and sloughing esophagitis (SE) as 2 differententities with overlapping endoscopic and histopathologicfeatures,1 whereas others consider them as 1 disease.2
They are discussed together in this review because of theshared characteristic endoscopic findings of SE mucosa.
EDS/SE is a rare benign condition; there are fewerthan 200 cases reported in the English medical literature.It affects the superficial layers of the squamous lining ofthe esophagus. Early reports of EDS had rather dramaticdescriptions including vomiting of the esophageal epithe-lium in the form of a “tubular cast.”3,4 In most casesof EDS/SE, however, the endoscopic findings are not asdramatic and range from white patches of peeling esopha-geal epithelium affecting the mid to distal esophagusto diffuse sloughing of the entire esophageal epithelium(Fig. 1).1,2,5,6 Involvement limited to the proximal esoph-agus has only been reported in a few cases.1 One study
ns: AMAG, autoimmune metaplastic atrophic gastritis; ECL,affin-like; EDS, esophagitis dissecans superficialis; LP,
us; SE, sloughing esophagitis.
E: All authors disclosed no financial relationships relevantle.
2014 by the American Society for Gastrointestinal Endoscopy36.00i.org/10.1016/j.gie.2014.09.009
ROINTESTINAL ENDOSCOPY Volume 80, No. 6 : 2014
described the esophageal endoscopic impression of EDSas “filled with gift-wrap paper.”2 The mucosa underneaththe peeled “membrane” is often unremarkable (Figs. 1Aand 1D). Additional esophageal findings during endoscopyare infrequent and may include erythema, ulceration,mucosal nodularity, rings, and even strictures.1,2,6
The most characteristic histopathologic feature ofEDS/SE is a “mummified” superficial squamous epitheliumand an unaltered basal layer; this gives a 2-toned appear-ance at low magnification (Fig. 2). Squamous cells in thesuperficial layers are necrotic (coagulative necrosis) andthus have pyknotic to faded (ghost) nuclei and intenseeosinophilic cytoplasm on routine hematoxylin and eosinstain. The eosinophilic top layer of the squamous mucosais often separated from the underlying intact squamousmucosa, and this sometimes creates a blister-like appear-ance (Figs. 2A and 2C). Inflammation is rarely seen and,if present, is often seen at the junction between thenecrotic epithelium and the underlying normal squamousmucosa.1,2
EDS/SE affects patients between the third and theeighth decades of life (range 14-90) with probable equal dis-tribution between the sexes; only a few cases have been re-ported in pediatric patients.1,2,4-7 EDS/SE often presentswith nonspecific clinical symptoms (eg, cough, dysphagia,globus sensation, regurgitation, chest or epigastric pain,heartburn, nausea and vomiting),1,2,5,6 and the diagnosis isoften not suspected until endoscopic examination.
The etiology remains unknown, but EDS/SE is frequentlyassociated with chemical trauma to the esophageal mucosacaused by polypharmacy, especially central nervous systemdepressants, nonsteroidal anti-inflammatory drugs, and bi-sphosphonates.1,2,5,8-11 In addition, this condition hasbeen associated with thermal and physical trauma to theesophageal mucosa including ingestion of hot beveragesand very rarely sclerotherapy for esophageal varices.4,12
Other reported rare associations include bullous skin dis-eases such as bullous pemphigoid and pemphigus vulga-ris,13 celiac disease,14 and heavy smoking.2 DistinguishingEDS/SE from esophageal manifestations of bullous skin dis-eases can be challenging on clinical grounds, but their his-tologic and immunofluorescence patterns differ.
In the study by Purdy et al,1 SE was encountered inpatients affected by debilitating conditions such as being
www.giejournal.org

Figure 1. Endoscopic photographs of esophagitis dissecans superficialis or sloughing esophagitis showing peeling (A, B) or sloughing (C, D) of translu-cent to nearly opaque patches or sheets of the superficial squamous epithelium. The underlying mucosa may be unremarkable (A,D) or erythematous (C).
Ma et al Non-neoplastic upper GI pathology
bedridden, and being immunosuppressed for transplanta-tion. These patients did not receive treatment, and allhad poor overall clinical outcomes as a result of their un-derlying diseases.1 In contrast, most other studies in themedical literature with follow-up information reported im-provements and often complete resolution after discontin-uation of the precipitating medications and treatment withproton pump inhibitors and/or corticosteroids.2,5
ESOPHAGEAL LEUKOPLAKIA OR ESOPHAGEALEPIDERMOID METAPLASIA
Leukoplakia is a clinical term used to describe a persis-tent white patch or plaque encountered on the mucousmembrane. Leukoplakia of the esophagus or esophagealepidermoid metaplasia is a rare condition reported inthe medical literature only in case reports and a few smallcase series.15-20 Only 6 cases were observed in a study of1000 autopsies,21 and none was encountered among 198consecutive esophageal biopsies over a 6-month periodat 3 academic institutions in the United States.19
The characteristic endoscopic features of leukoplakia ofthe esophagus or esophageal epidermoid metaplasiainclude a slightly elevated lesion, clear demarcation fromthe surrounding uninvolved tissue, a translucent white co-lor, and a shaggy or cobblestone surface (Fig. 3).15,17,19
The distal third of the esophagus is most often affected.
www.giejournal.org
The endoscopic differential diagnosis includes glycogenicacanthosis, esophageal papilloma, plaques associatedwith reflux, infections such as Candida esophagitis, andsuperficial esophageal cancer.15,16,22 The key feature todistinguish this entity from inflammatory lesions is its clearborder.15 Lugol’s iodine stain may be helpful to distinguishepidermoid metaplasia from papilloma and esophageal gly-cogenic acanthosis. The former has no staining, whereasthe latter 2 show weak (squamous papilloma) to strongstaining (glycogenic acanthosis).15,16,18 In terms of superfi-cial carcinomas, they tend to be multiple and tinged withpink color over time on Lugol’s iodine stain. Readers arereferred to the study by Ezoe et al15 for additional criteriafor distinguishing epidermoid metaplasia from otherplaque-like lesions during endoscopic examination. Need-less to say, esophageal biopsy also greatly facilitates thediagnosis of the lesion.
Although sharing the same endoscopic findings, esoph-ageal leukoplakia and esophageal epidermoid metaplasiahave slightly different histopathologic features. We believethat they are within the same spectrum of changes thatone can appreciate in epidermal hyperplasia. In fact,we provide the 2 diagnostic terms together as “esophagealleukoplakia/esophageal epidermoid metaplasia” in ourdaily pathology practice. The characteristic histopathologicfeatures of esophageal leukoplakia include hyperplasia,acanthosis, and parakeratosis of the superficial layersof esophageal squamous mucosa. Sometimes these are
Volume 80, No. 6 : 2014 GASTROINTESTINAL ENDOSCOPY 961

Figure 2. Histopathologic features of esophagitis dissecans superficialis or sloughing esophagitis include a 2-toned appearance at low magnification (A,B). The superficial layers of the esophageal squamous epithelium have coagulative necrosis and thus are eosinophilic (C, D). They are often partially(A) or completely (B) separated from the unaltered basal layers. The intraepithelial splitting appearance (A) may suggest a blister. There is little inflam-mation in these 2 examples. A, B, Original magnification �100; C, D, original magnification �200; all photomicrographs are from hematoxylin and eosin–stained tissue sections.
Non-neoplastic upper GI pathology Ma et al
accompanied by pronounced basal hyperplasia and/or asharply demarcated midzone with vacuolated cells and,sometimes, scatter neutrophils.17 The key histopathologicfinding in esophageal epidermoid metaplasia is a promi-nent granular layer accompanied by an overlying compacthyperorthokeratotic layer (Fig. 4). This feature is verysimilar to and even can be indistinguishable from theskin; hence the terminology. Additional features of epider-moid metaplasia include sharp demarcation from sur-rounding normal esophageal mucosa (Fig. 4A), flatteningof the rete pegs, a thickened basal layer, and moderateacanthosis of the midzone.15,16,18,19,22 The term orthokera-totic dysplasia has been used for essentially identical le-sions of the oral mucosa by Japanese colleagues.23
The etiology is not clear, but chronic irritation causedby esophageal stenosis and dysmotility has been suggestedas the inciting factor.24,25 Unlike oral leukoplakia, whichis considered a potentially malignant disorder by the WorldHealth Organization,26 the malignant potential of esopha-geal leukoplakia or esophageal epidermoid metaplasiahas not been extensively studied and thus is not clear.This is in part attributable to the rarity of the conditionand the lack of reported cases in the literature. A recentstudy by Singhi et al19 showed persistent disease in 54%of patients (7/13) with esophageal epidermoid metaplasia,and none progressed to dysplasia or carcinoma within amean follow-up period of 2.3 years (range 2–8.3 years).
962 GASTROINTESTINAL ENDOSCOPY Volume 80, No. 6 : 2014
On the other hand, this study, together with otherstudies, suggests an association between leukoplakia ofthe esophagus or esophageal epidermoid metaplasia andadjacent high-grade squamous dysplasia and/or squamouscell carcinoma.15,19,20,22 Because of this association, althoughdata remain limited, we suggest that our gastroenterologycolleagues initiate a surveillance program for patients witha diagnosis of esophageal leukoplakia or esophageal epider-moid metaplasia in our pathology practice.
ESOPHAGEAL LICHEN PLANUS ANDLICHENOID ESOPHAGITIS
Lichen planus (LP) is an idiopathic papulosquamouseruption involving the skin, nails, and mucosal surfaces.Cutaneous LP has a prevalence as high as 1% worldwideand affects predominantly middle-aged adults without sexpredilection.27 In contrast, LP of mucosal surfaces is pre-dominantly a disease of middle-aged women. It can includelesions of the oral mucosa, pharynx, and perineum butmost commonly affects the oral mucosa. In fact, oralinvolvement may coexist with cutaneous LP in 30% to50% of LP patients and 25% of patients affected by LP pre-sent with oral lesions alone.27,28 Although as many as 7% oforal LP patients may have spontaneous remission, 1.2% to2.3% of patients with oral LP may progress to malignancy,
www.giejournal.org

Figure 3. Endoscopic photograph of esophageal leukoplakia or esopha-geal epidermoid metaplasia showing a translucently white, well-demarcated plaque that is slightly raised from the adjacent esophagealsquamous mucosa and possessing a cobblestone-appearing surface.
Ma et al Non-neoplastic upper GI pathology
namely, squamous cell dysplasia and squamous cell carci-noma. Neither remission nor malignant transformation isrelated to the duration of disease.29,30
Similar to oral LP, esophageal LP affects mainly middle-aged women and often coexists with cutaneous andmucosal LP.31-35 In the study by Katzka et al,35 esophagealLP was the sole manifestation of LP in 2 of 27 patients, andthe esophagus was the initial presenting site in 13 of the27 patients. In contrast to cutaneous and oral LP, esopha-geal LP remains underdiagnosed, and therefore the preva-lence is unknown. This is partly because many patientsremain asymptomatic or experience only minor nonspe-cific esophageal symptoms, predominantly dysphagia,until their disease progresses to esophageal stricture. Ina recent study by Quispel et al,33 50% (12 of 24) of patientswith oral and/or cutaneous LP had esophageal LP detectedby magnification chromoendoscopy and further proven byhistopathologic evaluation. For the same reason, the riskof malignancy is also not well established, but a small num-ber of cases associated with malignant transformation toesophageal squamous dysplasia, squamous cell carcinoma,and verrucous carcinoma have been reported.32,34-37
Esophageal LP most often affects the upper and middlethirds of the esophagus.32,33 The characteristic endoscopicfeatures of esophageal LP include mucosal sloughing, fria-bility on contact, hyperemia, and ulceration (Fig. 5).32,33,35
Whitish papules are often seen in esophageal LP, but thisfinding is nonspecific.33 In advanced disease, esophageal
www.giejournal.org
strictures may form, mainly in the proximal esophagusbut also elsewhere in the esophagus.35
The characteristic histologic features include a promi-nent bandlike infiltrate of lymphocytes involving the epithe-lium and lamina propria, damage of the basal layer of theepithelium and scattered degenerated keratinocytestermed Civatte bodies (Figs. 6A, C, and D).31 The presenceof bandlike lymphocytosis alone is not diagnosticof esophageal LP. Other conditions associated with esoph-ageal intraepithelial lymphocytosis include medication-associated injury, reactive changes associated with ulcer,and GERD.38 Clinicopathologic and endoscopic-pathologiccorrelation is often required to establish a diagnosis ofesophageal LP. Direct immunofluorescence (DIF) studieshave proved useful.
A recently described pattern of esophageal injury, calledlichenoid esophagitis, has clinical and histopathologicfeatures nearly identical to those of established esophagealLP.34 Patients descriptively diagnosed with lichenoidesophagitis do not have positive DIF, but their esophagealbiopsy specimens demonstrate histopathologic featuresindistinguishable from those seen in esophageal LP(Figs. 6B-D). Lichenoid esophagitis is associated with HIVinfection and viral hepatitis including hepatitis Band hepatitis C; this association with viral infections hasnot been reported in esophageal LP. On the other hand,both esophageal LP and lichenoid esophagitis are associ-ated with polypharmacy, rheumatologic diseases, andesophageal strictures; both may progress to malignancy.34
AUTOIMMUNE METAPLASTIC ATROPHICGASTRITIS AND ATROPHIC AUTOIMMUNEPANGASTRITIS
Autoimmune metaplastic atrophic gastritis (AMAG),although not a newly recognized disease, often causesconfusion and delay in diagnosis, which subjects patientsto increased risk of the development of pernicious anemiaand other the sequelae of AMAG.
AMAG is a chronic gastric inflammatory disease causedby parietal cell antibodies to the gastric proton pump,the H/K ATPase.39 AMAG affects the gastric body andfundus where the parietal cell-containing oxyntic glandsreside, and thus it is different from the antral gastritis typi-cally associated with H pylori infection. In patients affect-ed by AMAG, intrinsic factor antibodies and ultimatelypernicious anemia may develop as a result of vitamin B12
deficiency. Destruction of parietal cells results in hypergas-trinemia and subsequently enterochromaffin-like (ECL)cell hyperplasia in the gastric body and fundus. Thus, pa-tients with AMAG also have increased risk of the develop-ment of neuroendocrine neoplasms and gastric cancer.40,41
The precise prevalence of AMAG remains unknownbecause it is often underdiagnosed in its early stage whenmany patients do not have vitamin B12 deficiency and the
Volume 80, No. 6 : 2014 GASTROINTESTINAL ENDOSCOPY 963

Figure 4. Esophageal epidermoid metaplasia is characterized histologically by an undulating squamous mucosa with clear demarcation from the sur-rounding mucosa (A), prominent granular layer, and an overlying compact hyperorthokeratotic layer (B). A, original magnification, �100; B, originalmagnification, �400; both photomicrographs are from hematoxylin and eosin–stained sections.
Figure 5. Endoscopic photographs of esophageal lichen planus showing sloughing mucosa forming a pseudomembrane layer (A) and friable mucosa (B)with ulceration. A, a thin fibrinous layer at the 3-o’clock position, easily separated from the underlying submucosa on contact and exposing a superficialulcer (not shown). B, taken from a patient with a long-standing history of lichen planus, initially affecting the skin and later involving the oral and esoph-ageal mucosa. The mucosa has a rough granular appearance with a polypoid lesion and luminal narrowing that required periodic dilation. Histopathologicevaluation of the esophageal lesion showed high-grade squamous dysplasia.
Non-neoplastic upper GI pathology Ma et al
histopathologic features are not fully developed. Onceconsidered a disease that preferentially affects elderlywomen of Northern European descent, current data sug-gest that (1) AMAG occurs at a similar frequency across allracial groups, (2) women are preferentially affected, (3)the reported overall prevalence is as high as 2.7% in womenand 1.4% in men, and (4) a higher prevalence, as high as4.3%, and earlier age at onset are seen in nonwhite womenwhen compared with white women.39,42,43
The histopathologic features, endoscopic findings, andclinical presentations of AMAG evolve over time. The histo-pathologic features of early AMAG are subtle and can bechallenging when the stomach is not well sampled or thepathologist is not familiar with early manifestations ofAMAG. The constellation of histopathologic findings sup-porting a diagnosis of early AMAG includes multifocal ordiffuse lymphoplasmacytic infiltration in the deep portionof the lamina propria, ie, a “bottom-heavy” inflammatoryinfiltrate, scattered destruction of individual oxyntic glandsby lymphocytes, parietal cell pseudohypertrophy, ECL cellhyperplasia, and various types of metaplasia (Fig. 7).39,44,45
The latter 3 features may not present in all cases of earlyAMAG. In the study by Torbenson et al,45 22 of 34 cases
964 GASTROINTESTINAL ENDOSCOPY Volume 80, No. 6 : 2014
(65%) of early AMAG in patients without proton pumpinhibitor treatment at the time of biopsy showed parietalcell pseudohypertrophy reminiscent of the effect in parie-tal cells induced by proton pump inhibitors, and 11 casesof early AMAG with positive serologic anti-intrinsic factorantibody or antiparietal cell antibody showed at least linearECL cell hyperplasia on chromogranin A immunostaining.Also reported in this study were 65% of cases (22/34)with intestinal (16/34; 47%), pyloric (16/34; 47%), andeven pancreatic acinar cell (2/34; 6%) metaplasia.45 Pancre-atic acinar cell metaplasia, if present in gastric biopsy spec-imens taken from oxyntic mucosa, may be a strongindicator for AMAG because it is much more frequentlyfound in gastric biopsy specimens with AMAG than speci-mens with other types of gastritis or in biopsy specimensof normal oxyntic mucosa.46
The main histopathologic differential diagnosis for earlyAMAG is H pylori gastritis involving the oxyntic mucosa.Helpful features to distinguish them include the distribu-tion and nature of the inflammatory infiltrate, the distribu-tion of metaplasia, identification of organisms, and ECL cellhyperplasia.45 In addition, a subset of patients affected byearly AMAG may have coexisting H pylori infection.44,45
www.giejournal.org

Figure 6. Histopathologic features of esophageal lichen planus (A) and lichenoid esophagitis (B) are identical and include a bandlike infiltrate of lym-phocytes involving the epithelium and lamina propria. The basal layer is damaged (C), and there are scattered Civatte bodies (A, B, and D; arrows).B, Photomicrograph was taken from esophageal biopsy specimens of a patient who had HIV infection (well controlled) and hepatitis C viral infection.A, B, original magnification, �200; C and D, original magnification, �400; all photomicrographs are from hematoxylin and eosin–stained tissue sections.
Ma et al Non-neoplastic upper GI pathology
Of interest, some authors have proposed that H pyloriinfection may cause AMAG in susceptible individuals byinducing autoantibodies to parietal cell through molecularmimicry.47,48
Fully established AMAG presents with a profound loss ofthe parietal cell mass and thus atrophy of oxyntic glands.This finding together with deep, dense, diffuse lympho-plasmacytic infiltration and metaplasia of the intestinal, py-loric, and pancreatic types are characteristic of AMAG(Figs. 8A, C, and E). Nodular ECL cell hyperplasia caneven be appreciated on hematoxylin and eosin staining;both linear and nodular ECL cell hyperplasia can be high-lighted by chromogranin A immunostaining (Fig. 8E).Late-stage AMAG is characterized by complete atrophy ofoxyntic mucosa with minimal inflammation, and theaffected gastric mucosa often has an empty appearance.Metaplasia is widespread, and ECL cell hyperplasia isalmost always present.39 Compared with the often strik-ingly atrophic and inflamed oxyntic mucosa, the antral mu-cosa is rather unremarkable in the absence of current orpast H pylori infection; there may be reactive changesand foveolar hyperplasia but no atrophy, metaplasia, orECL cell hyperplasia (Figs. 8B, 8D, and 8F).39,49
Patients affected by AMAG have an increased risk ofthe development of non-neoplastic lesions includingoxyntic gland “pseudopolyps” and hyperplastic polyps,as well as neoplastic lesions including intestinal and pylo-ric gland adenomas, well-differentiated neuroendocrine
www.giejournal.org
(carcinoid) tumors, and gastric adenocarcinoma. Aware-ness of this association is of critical importance forgastroenterologists when performing endoscopic evalua-tion of the gastric mucosa of patients with gastric lesions.
In the early phases of AMAG, the body and fundus of thestomach may not have any endoscopically recognizablechanges or may just have nonspecific atrophy with mucosalthinning and loss of rugal folds (Fig. 9A). In this backgroundof incomplete atrophy, the islands of relatively preserved,normal oxyntic glands may appear as polyps endoscopically(Fig. 9B).43,50-53 In the study by Park et al,43 20 pseudopo-lyps were detected in 143 AMAG patients with gastric le-sions. Furthermore, in the study by Krasinskas et al50
pseudopolyps were found in the body and fundus and areoften multiple.
Patients with AMAG may also have true polyps arisingin the gastric mucosa; these include hyperplastic polyps,intestinal-type gastric adenoma, pyloric gland adenoma,and well-differentiated neuroendocrine (carcinoid) tu-mors presenting endoscopically as polypoid lesions. Hy-perplastic polyps are the most common type of gastricpolyps in AMAG patients; 138 hyperplastic polyps weredetected in 143 AMAG patients with gastric lesions inthe study by Park et al.43 Although many of these pa-tients have multiple hyperplastic polyps,49 a subset ofAMAG patients do present with antrum-restricted hyper-plastic polyps (6/16; 38% in the study by Abrahamet al49).
Volume 80, No. 6 : 2014 GASTROINTESTINAL ENDOSCOPY 965

Figure 7. Histologic features of early autoimmune metaplastic atrophic gastritis include a lymphocytic infiltration in the deep portion of the laminapropria (A) and scattered destruction of individual oxyntic glands (B). Enterochromaffin-like (ECL) cell hyperplasia is highlighted by an immunostainwith anti–chromogranin A antibody (C, D). D, Linear ECL cell hyperplasia is defined as at least 5 immunoreactive cells in a row in a gastric gland. Thereis no metaplasia. This biopsy specimen was taken from a patient who had hypergastrinemia (230 pg/mL [normal!101 pg/mL]) but normal hematocrit andnormal serum vitamin B12 concentration). A, C, Original magnification, �100; B and D, original magnification, �400; both A and B are from hematoxylinand eosin–stained tissue sections.
Non-neoplastic upper GI pathology Ma et al
Additionally noted in the study by Park et al43 were18 intestinal-type gastric adenomas, 3 pyloric gland ade-nomas, 46 well-differentiated neuroendocrine (carcinoid)tumors, 1 GI stromal tumor, 3 lymphomas (2 mucosa-associated lymphoid tissue type of extranodal marginalzone lymphoma, and 1 large B-cell lymphoma arisingin gastric mucosa without H pylori infection), and 11 ad-enocarcinomas in the 143 AMAG patients with gastriclesions. Intestinal-type gastric adenoma, although not asfrequently associated with AMAG as hyperplastic polyps,is a precursor lesion.54,55 The well-differentiated neuro-endocrine (carcinoid) tumors associated with AMAG areusually small, often multiple, arise in a background ofECL cell hyperplasia, and have negligible metastaticpotential.56
In patients who present with gastric polyps or polypoidlesions, biopsy of the lesion or polypectomy alone may notbe diagnostic of the underlying gastric disease. Samplingvarious locations of the flat mucosa from both the body/fundus and the antrum away from the gastric polyps duringendoscopic examination is of great importance in identi-fying the underlying gastric pathology.50,52,53
Last, pernicious anemia, the well-known outcome ofthe late-stage AMAG, takes decades to develop.39,48 Atthe initial phase of the disease, many patients maynot have vitamin B12 deficiency but present first with
966 GASTROINTESTINAL ENDOSCOPY Volume 80, No. 6 : 2014
iron deficiency anemia or normocytic anemia.48,57 Asdemonstrated in the study by Hershko et al,48 83 of 160 pa-tients with autoimmune gastritis identified by hypergastri-nemia and positive antiparietal cell antibodies presentedwith iron deficiency anemia, 48 patients with normocyticanemia, and only 29 patients with macrocytic anemia.When stratified by ages from younger than 20 years toolder than 60 years, the mean corpuscular volume andserum concentration of gastrin progressively increased,whereas serum concentration of cobalamin (vitamin B12)progressively decreased among their cohorts.48
Iron deficiency in AMAG patients is a result of achlor-hydria. This is because gastric acidity is required torender dietary iron soluble. The decrease in gastric acid-ity caused by the reduction in gastric acid produced byparietal cells leads to reduced iron absorption and thusiron deficiency anemia. By the same token, these patientsare likely to be refractory to oral iron supplement ther-apy. As such, a high index of suspicion for AMAG isnecessary when evaluating a patient with refractory irondeficiency anemia without clear etiology. The initial eval-uation in the setting of suspected AMAG should alsoinclude serum gastrin concentration and antiparietal cellantibodies.53
The main differential diagnosis for AMAG is the environ-mental atrophic gastritis associated with long-standing
www.giejournal.org
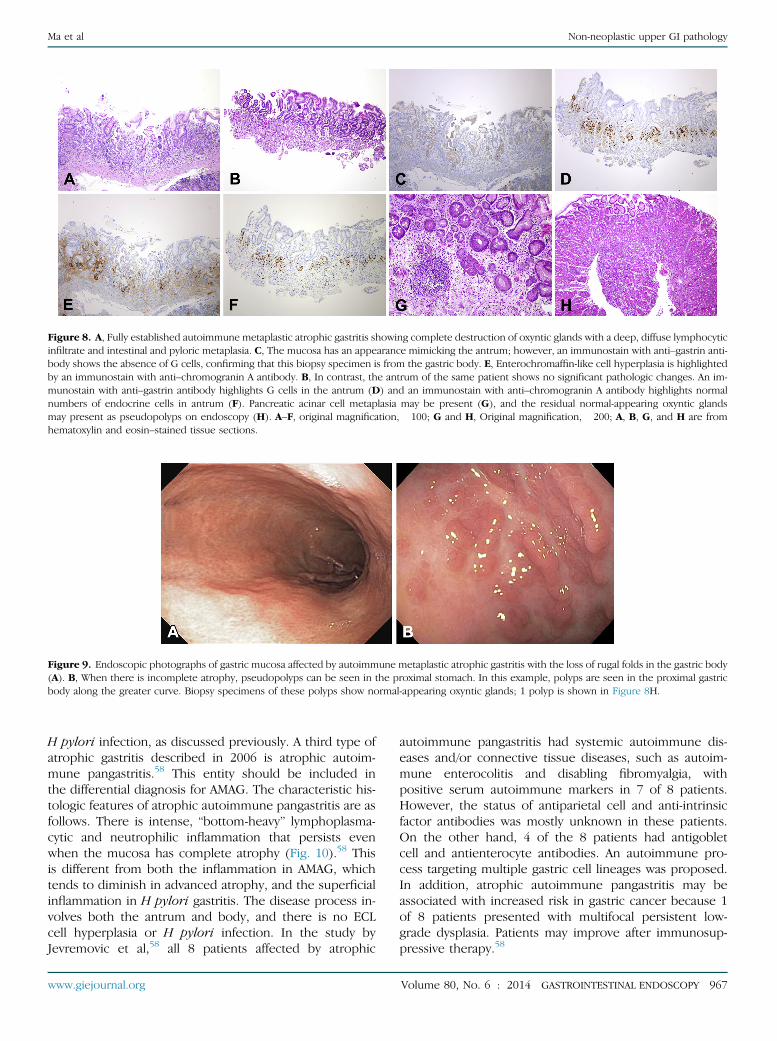
Figure 9. Endoscopic photographs of gastric mucosa affected by autoimmune metaplastic atrophic gastritis with the loss of rugal folds in the gastric body(A). B, When there is incomplete atrophy, pseudopolyps can be seen in the proximal stomach. In this example, polyps are seen in the proximal gastricbody along the greater curve. Biopsy specimens of these polyps show normal-appearing oxyntic glands; 1 polyp is shown in Figure 8H.
Figure 8. A, Fully established autoimmune metaplastic atrophic gastritis showing complete destruction of oxyntic glands with a deep, diffuse lymphocyticinfiltrate and intestinal and pyloric metaplasia. C, The mucosa has an appearance mimicking the antrum; however, an immunostain with anti–gastrin anti-body shows the absence of G cells, confirming that this biopsy specimen is from the gastric body. E, Enterochromaffin-like cell hyperplasia is highlightedby an immunostain with anti–chromogranin A antibody. B, In contrast, the antrum of the same patient shows no significant pathologic changes. An im-munostain with anti–gastrin antibody highlights G cells in the antrum (D) and an immunostain with anti–chromogranin A antibody highlights normalnumbers of endocrine cells in antrum (F). Pancreatic acinar cell metaplasia may be present (G), and the residual normal-appearing oxyntic glandsmay present as pseudopolyps on endoscopy (H). A–F, original magnification, �100; G and H, Original magnification, �200; A, B, G, and H are fromhematoxylin and eosin–stained tissue sections.
Ma et al Non-neoplastic upper GI pathology
H pylori infection, as discussed previously. A third type ofatrophic gastritis described in 2006 is atrophic autoim-mune pangastritis.58 This entity should be included inthe differential diagnosis for AMAG. The characteristic his-tologic features of atrophic autoimmune pangastritis are asfollows. There is intense, “bottom-heavy” lymphoplasma-cytic and neutrophilic inflammation that persists evenwhen the mucosa has complete atrophy (Fig. 10).58 Thisis different from both the inflammation in AMAG, whichtends to diminish in advanced atrophy, and the superficialinflammation in H pylori gastritis. The disease process in-volves both the antrum and body, and there is no ECLcell hyperplasia or H pylori infection. In the study byJevremovic et al,58 all 8 patients affected by atrophic
www.giejournal.org
autoimmune pangastritis had systemic autoimmune dis-eases and/or connective tissue diseases, such as autoim-mune enterocolitis and disabling fibromyalgia, withpositive serum autoimmune markers in 7 of 8 patients.However, the status of antiparietal cell and anti-intrinsicfactor antibodies was mostly unknown in these patients.On the other hand, 4 of the 8 patients had antigobletcell and antienterocyte antibodies. An autoimmune pro-cess targeting multiple gastric cell lineages was proposed.In addition, atrophic autoimmune pangastritis may beassociated with increased risk in gastric cancer because 1of 8 patients presented with multifocal persistent low-grade dysplasia. Patients may improve after immunosup-pressive therapy.58
Volume 80, No. 6 : 2014 GASTROINTESTINAL ENDOSCOPY 967

Figure 10. In this example of atrophic autoimmune pangastritis, the gastric body shows complete loss of oxyntic glands (A) and marked expansion oflaminar propria by lymphocytes and neutrophils. B, There are intraepithelial neutrophils, lymphocytes, and intestinal metaplasia. An immunostain withanti–gastrin antibody demonstrated no G cells and therefore confirmed that the tissue section was from the gastric body (not shown). A, Originalmagnification, �200; B, original magnification, �400; both photomicrographs are from hematoxylin and eosin–stained tissue sections.
Non-neoplastic upper GI pathology Ma et al
SUMMARY
The definitive diagnosis of these entities requires ahigh index of suspicion and correlation among clinical,endoscopic, and pathologic findings. Much about manyaspects of these diseases remains unknown. Awarenessof these entities and their clinical significance may allowimproved recognition and patient care.
REFERENCES
1. Purdy JK, Appelman HD, McKenna BJ. Sloughing esophagitis is associ-ated with chronic debilitation and medications that injure the esoph-ageal mucosa. Mod Pathol 2012;25:767-75.
2. Carmack SWMD, Vemulapalli RMD, Spechler SJMD, et al. Esophagitisdissecans superficialis (“sloughing esophagitis”): a clinicopathologicstudy of 12 cases. Am J Surg Pathol 2009;33:1789-94.
3. Morgenstern M. Tube-like expulsion of esophageal mucosa (esophagi-tis exfoliativasive dissecans superficialis). Zentralbl Allg Pathol 1952;89:17-22.
4. Beck RN. Oesophagitis dissecans superficialis. BMJ 1954;1:501-2.5. Albert DM, Ally MR, Moawad FJ. The sloughing esophagus: a report of
five cases. Am J Gastroenterol 2013;108:1816-7.6. Ponsot P, Molas G, Scoazec JY, et al. Chronic esophagitis dissecans: an
unrecognized clinicopathologic entity? Gastrointest Endosc 1997;45:38-45.
7. Mutalib M, Bates A, Furman M, et al. Oesophagitis dissecans in a childwith vomiting. J Pediatr Gastroenterol Nutr 2013;57:e33.
8. Abbass K, Haveman L, Gertner E. Esophagitis dissecans superficialis dueto severe methotrexate toxicity. Endoscopy 2014;46(Suppl 1):E99-100.
9. Cameron RB. Esophagitis dissecans superficialis and alendronate: casereport. Gastrointest Endosc 1997;46:562-3.
10. Hokama A, Ihama Y, Nakamoto M, et al. Esophagitis dissecans superfi-cialis associated with bisphosphonates. Endoscopy 2007;39(Suppl 1):E91.
11. De Petris G, Gatius Caldero S, et al. Histopathological changes in thegastrointestinal tract due to medications: an update for the surgicalpathologist (part II of II). Int J Surg Pathol 2013;22:202-11.
12. Perez-Carreras M, Castellano G, Colina F, et al. Esophagitis dissecanssuperficialis (esophageal cast) complicating esophageal sclerotherapy.Am J Gastroenterol 1998;93:655-6.
13. Hokama A, Yamamoto Y, Taira K, et al. Esophagitis dissecans superficia-lis and autoimmune bullous dermatoses: a review. World J GastrointestEndosc 2010;2:252-6.
968 GASTROINTESTINAL ENDOSCOPY Volume 80, No. 6 : 2014
14. Hage-Nassar G, Rotterdam H, Frank D, et al. Esophagitis dissecans super-ficialis associated with celiac disease. Gastrointest Endosc 2003;57:140-1.
15. Ezoe Y, Fujii S, Muto M, et al. Epidermoid metaplasia of the esophagus:endoscopic feature and differential diagnosis. Hepatogastroenterology2011;58:809-13.
16. Fukui T, Sakurai T, Miyamoto S, et al. Education and imaging. Gastroin-testinal: epidermal metaplasia of the esophagus. J Gastroenterol Hep-atol 2006;21:1627.
17. Kaye MD. Esophageal leukoplakia. Gastrointest Endosc 1987;33:254-9.18. Nakanishi Y, Ochiai A, Shimoda T, et al. Epidermization in the esopha-
geal mucosa: unusual epithelial changes clearly detected by Lugol’sstaining. Am J Surg Pathol 1997;21:605-9.
19. Singhi AD, Arnold CA, Crowder CD, et al. Esophageal leukoplakia orepidermoid metaplasia: a clinicopathological study of 18 patients.Mod Pathol 2014;27:38-43.
20. Taggart MW, Rashid A, Ross WA, et al. Esophageal hyperkeratosis: clin-icopathologic associations. Histpathology 2013;64:463-73.
21. Postlethwait RW, Musser AW. Changes in the esophagus in 1,000 au-topsy specimens. J Thorac Cardiovascular Surg 1974;68:953-6.
22. Herschman BR, Uppaputhangkule V, Maas L, et al. Esophageal leuko-plakia: a rare entity. JAMA 1978;239:2021.
23. Kobayashi T, Maruyama S, Abe T, et al. Keratin 10-positive orthokera-totic dysplasia: a new leucoplakia-type precancerous entity of theoral mucosa. Histopathology 2012;61:910-20.
24. Montgomery E, Voltaggio L. Biopsy interpretation of the gastrointes-tinal tract mucosa: volume 1: non-neoplastic, 2nd ed. Philadelphia(Pa): Lippincott Williams & Wilkins; 2012. p. 10-1.
25. Lindsay JR. Esophageal lesions in diffuse scleroderma. Laryngoscope1949;59:83-112.
26. Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature andclassification of potentially malignant disorders of the oral mucosa.J Oral Pathol 2007;36:575-80.
27. Scully C, El-Kom M. Lichen planus: review and update on pathogenesis.J Oral Pathol Med 1985;14:431-58.
28. Lund WS. Treatment of superficial lesions of the mouth and pharynx.J Laryngol Otol 1976;90:105-12.
29. Silverman S Jr, GorskyM, Lozada-Nur F. A prospective follow-up study of570 patients with oral lichen planus: persistence, remission, andmalignant association. Oral Surg Oral Med Oral Pathol 1985;60:30-4.
30. Silverman S Jr, Gorsky M, Lozada-Nur F, et al. A prospective study offindings and management in 214 patients with oral lichen planus.Oral Surg Oral Med Oral Pathol 1991;72:665-70.
31. Abraham SC, Ravich WJ, Anhalt GJ, et al. Esophageal lichen planus: casereport and review of the literature. Am J Surg Pathol 2000;24:1678-82.
32. Chryssostalis A, Gaudric M, Terris B, et al. Esophageal lichen planus: aseries of eight cases including a patient with esophageal verrucouscarcinoma. A case series. Endoscopy 2008;40:764-8.
www.giejournal.org

Ma et al Non-neoplastic upper GI pathology
33. Quispel R, van Boxel OS, Schipper ME, et al. High prevalence of esoph-ageal involvement in lichen planus: a study using magnification chro-moendoscopy. Endoscopy 2009;41:187-93.
34. Salaria SN, Abu Alfa AK, Cruise MW, et al. Lichenoid esophagitis: clini-copathologic overlap with established esophageal lichen planus. AmJ Surgical Pathol 2013;37:1889-94.
35. Katzka DA, Smyrk TC, Bruce AJ, et al. Variations in presentations ofesophageal involvement in lichen planus. Clin Gastroenterol Hepatol2010;8:777-82.
36. Calabrese C, Fabbri A, Benni M, et al. Squamous cell carcinoma arisingin esophageal lichen planus. Gastrointest Endosc 2003;57:596-9.
37. Schwartz MP, Sigurdsson V, Vreuls W, et al. Two siblings with lichenplanus and squamous cell carcinoma of the oesophagus. Eur J Gastro-enterol Hepatol 2006;18:1111-5.
38. Montgomery E, Voltaggio L. Biopsy interpretation of the gastrointes-tinal tract mucosa: volume 1: non-neoplastic, 2nd ed Philadelphia(Pa): Lippincott Williams & Wilkins; 2012. p. 28-31.
39. Neumann WL, Coss E, Rugge M, et al. Autoimmune atrophic gastritis–pathogenesis, pathology and management. Nat Rev GastroenterolHepatol 2013;10:529-41.
40. Ye W, Nyren O. Risk of cancers of the oesophagus and stomach by his-tology or subsite in patients hospitalised for pernicious anaemia. Gut2003;52:938-41.
41. Hsing AW, Hansson LE, McLaughlin JK, et al. Pernicious anemiaand subsequent cancer. A population-based cohort study. Cancer1993;71:745-50.
42. Carmel R. Prevalence of undiagnosed pernicious anemia in the elderly.Arch Intern Med 1996;156:1097-100.
43. Park JY, Cornish TC, Lam-Himlin D, et al. Gastric lesions in patients withautoimmune metaplastic atrophic gastritis (AMAG) in a tertiary caresetting. Am J Surg Pathol 2010;34:1591-8.
44. Stolte M, Baumann K, Bethke B, et al. Active autoimmune gastritiswithout total atrophy of the glands. Z Gastroenterol 1992;30:729-35.
45. Torbenson M, Abraham SC, Boitnott J, et al. Autoimmune gastritis:distinct histological and immunohistochemical findings before com-plete loss of oxyntic glands. Mod Pathol 2002;15:102-9.
46. Jhala NC, Montemor M, Jhala D, et al. Pancreatic acinar cell metaplasiain autoimmune gastritis. Arch Pathol Lab Med 2003;127:854-7.
47. D'Elios MM, Bergman MP, Amedei A, et al. Helicobacter pylori andgastric autoimmunity. Microbes Infect 2004;6:1395-401.
48. Hershko C, Ronson A, Souroujon M, et al. Variable hematologic presen-tation of autoimmune gastritis: age-related progression from iron defi-ciency to cobalamin depletion. Blood 2006;107:1673-9.
www.giejournal.org
49. Abraham SC, Singh VK, Yardley JH, et al. Hyperplastic polyps of thestomach: associations with histologic patterns of gastritis and gastricatrophy. Am J Surg Pathol 2001;25:500-7.
50. Krasinskas AM, Abraham SC, Metz DC, et al. Oxyntic mucosa pseudopo-lyps: a presentation of atrophic autoimmune gastritis. Am J Surg Path-ol 2003;27:236-41.
51. Okano A, Takakuwa H, Matsubayashi Y. Parietal-cell hyperplasiamimicking sporadic fundic gland polyps in the atrophic mucosa ofautoimmune gastritis. Gastrointest Endosc 2007;66:394-5; discussion 5.
52. Dirschmid K, Stolte M. Gastric lesions in patients with autoimmunemetaplastic atrophic gastritis. Am J Surg Pathol 2011;35:1244; authorreply 1245.
53. Park JYMDP, Cornish TCMDP, Lam-Himlin DMD, et al. In response. AmJ Surg Pathol 2011;35:1244-5.
54. Laxen F, Kekki M, Sipponen P, et al. The gastric mucosa in stomachswith polyps: morphologic and dynamic evaluation. Scand J Gastroen-terol 1983;18:503-11.
55. Abraham SC, Montgomery EA, Singh VK, et al. Gastric adenomas:intestinal-type and gastric-type adenomas differ in the risk of adeno-carcinoma and presence of background mucosal pathology. Am JSurg Pathol 2002;26:1276-85.
56. Neuroendocrine neoplasms of the stomach. In: Bosman FT, Carneiro F,Hruban RH, et al, editors. WHO classification of tumours of the diges-tive system, 4th ed. Geneva: World Health Organization; 2010. p. 64-8.
57. Lagarde S, Jovenin N, Diebold MD, et al. Is there any relationship be-tween pernicious anemia and iron deficiency? Gastroenterol ClintBiol 2006;30:1245-9.
58. Jevremovic D, Torbenson M, Murray JA, et al. Atrophic autoimmunepangastritis: a distinctive form of antral and fundic gastritis associatedwith systemic autoimmune disease. Am J Surg Pathol 2006;30:1412-9.
Received May 18, 2014. Accepted September 3, 2014.
Current affiliations: Departments of Pathology (1) and Medicine (2), JohnsHopkins University School of Medicine, Baltimore, Maryland, USA.
Reprint requests: Elizabeth A. Montgomery, MD, Department of Pathology,Johns Hopkins Medical Institutions, Weinberg 2242, 401 North Broadway,Baltimore, MD 21231.
Volume 80, No. 6 : 2014 GASTROINTESTINAL ENDOSCOPY 969

GASTROENTEROLOGY ARTICLE OF THE WEEK February 19, 2015
Ma C, Limketkai BN, Montgomery E. Recently highlighted non-neoplastic pathologic entities of the upper GI tract and their clinical significance. Gastrointest Endosc 2014;80:960-969. 1. The most common type of gastric polyp seen in atrophic autoimmune gastritis is a. hyperplastic b. carcinoid c. gastric type adenomas d. intestinal type adenomas 2. Characteristics of esophageal leukoplakia include a. also known as esophageal epidermoid metaplasia
b. on endoscopy, it appears as a yellow polypoid lesion c. no staining with Lugol’s iodine solution
d. on histology, a prominent granular layer with an overlying hyperorthokeratotic layer is characteristic. 3. Esophageal lichen planus a. most often involves the upper or middle third of the esophagus b. most often affects middle age men who smoke
c. endoscopically it appears as a white plaque d. is associated with HIV and HCV infection
True or False 4. Sloughing esophagitis may be a manifestation of medication-induced esophageal injury 5. Leukoplakia of the esophagus, although not premalignant, may be associated with adjacent squamous cell carcinoma 6. Esophagitis dissecans superficialis is associated with an increased risk of esophageal perforation 7. Patients with pernicious anemia are likely to present first with iron deficiency anemia before developing B12 deficiency. 8. The presence of enterochromaffin cell hyperplasia is typical for autoimmune atrophic gastritis 9. Iron deficiency anemia as a result of atrophic autoimmune gastritis is easily corrected with oral iron supplements 10. Autoimmune atrophic gastritis is characterized by antibodies directed against the gastrin receptor in the parietal cell 11. When gastric polyps are identified, the surrounding mucosa should be biopsied to exclude autoimmune gastritis