rebecca j saunders pt/cht - asht 2016_htrc... · fractures rebecca j saunders pt/cht ......
TRANSCRIPT

Hand Therapy Review CourseCurtis National Hand Center
Baltimore, MDOctober 7‐9, 2016
Fractures
Rebecca J Saunders PT/CHT
Epiphysis Physis Metaphysis Diaphysis Periosteum Endosteum
Cortical bone – compact bone◦ Concentrated in diaphysis of long bone◦ Houses osteons (contain osteocytes)◦ 80% of skeletal mass
Cancellous bone – trabecular or spongy) ◦ 20% skeletal mass◦ Concentrated at epiphysis and
metaphysis of long bones◦ Metabolic turnover is greater than for
cortical; usually faster healing
Energy absorbed by bone
mechanical & structural failure
Loss of Continuity of Bone
vascular disruption at fracture site
soft tissue injury
Location in Bone◦Diaphyseal◦Metaphyseal◦Articular

Depth of fracture: complete, incomplete Angle: transverse, oblique, spiral, longitudinal, Complexity: simple, comminuted or crushed Closed versus Open Intra articular vs. extra articular Avulsion
Inflammatory Phase (0-2 weeks)◦ Accumulation of a hematoma between fracture ends under elevated periosteum
◦ Bone necrosis (osteocytes lose nutrition)◦ Proliferation of fibroblasts and osteoblasts◦ Invasion of leukocytes and macrophages
Hematoma organizes forming fibrin scaffold
External carilagenous callous forms from periosteum
Internal callous forms from endosteum
Gradual increase in stability toward clinical union
New bone and oteogenic cells bridge fracture site
Occurs over prolonged period of time
Process of continuous bone resorption and formation
Bone is remodeled as oteoclasts reabsorb callous
Can be influenced by stress
Primary Healing: ◦ No Callus
formation◦ Direct apposition
of bone ends with compression◦ Rigid fixation
(substitute for callus)
Secondary Healing: Callus
formation Slight
movement /micromotion

Patient’s age Complexity/Character
of fracture Systemic Disease Bone Disease/metabolic
bone disease Medications Nutritional factors,
ETOH, tobacco use
Nicotine has detrimental effects on the health of bone
Has deleterious effects on blood vessels and the transport of O2 to body cells
Decreases red blood cell function
Higher nonunion, delayed union rates
Higher rates of postop infection
Compliance
Emotional status
Other injuries: tendon, nerve, soft tissue, multiple fx’s
Joint stability
Infections
Buckle or Torus fracture (incomplete fracture) Greenstick fracture Physeal fractures
Greenstick fractures occur midshaft where bone is slower to healRequire 6 wks of cast immobilization
Salter I – separation through growth plate (physis)
Salter II – injury through physis with part of metaphysis attached
Salter III – injury thru physis; longitudinal fracture thru epiphysis

Salter IV – longitudinal fx extending into metaphysis,physis,epi-physis; complete reduction necessary to restore joint surfaces
Salter V – crush injury to germinal cells of physis; premature closure of growth plate “This cast won’t slow me down!”
Angular deformities better tolerated in children, greater capacity for remodeling as bone grows
Cast/splint may need to include more proximal joints to keep cast on
StabilityMobilityFunction
Therapists should have understanding of:◦ Fracture stability/alignment◦ Operative procedures performed◦ Potential dysfunction at uninvolved joints◦ Appropriate timing for ROM, splinting,
strengthening◦ Balancing act between protection and applying
controlled stress for motion and strength
◦ ***Motion or stress to the bone promotes bone healing.
Edema control Pain management
Protection AROM PROM Sensory eval and desens.
Functional activities
Strengthening
Closed Reduction Indication= stable fracture Immobilized with cast or splint
What’s wrong with this cast?
External Fixation-provides traction to prevent fx. shortening or angulation
Indications◦ unstable fx’s
◦ fx’s requiring early motion
◦ fx’s w/ high incidence of non-union
K-wires: open vs. closed
Screws Plates Wires Intermedulary Nails Bone Grafts
Soft tissue injury
Periosteal stripping
Hardware irritation
Adhesions
Tendon Ruptures
What’s wrong with the xray at 6 weeks?
Non union Malunion/Bone length
alteration Delayed union Edema Pain Stiff joint Tendon adhesions Decreased strength Nerve entrapments or
compressions Post-traumatic OA
6 P’s: Pain, paresthesia, pallor, paralysis, pulselessness, pressure

Colles◦ Extra-articular◦ Complete fx. of distal
radius w/ dorsal displacement◦ 80% require reduction
Colles fractures often do not stay reduced and need surgery to maintain alignment.
Smith’s: ◦ Reverse Colles
fracture◦ Distal radius with
volar displacement Barton’s: ◦ Distal radius
fracture with dislocation of radial carpal joint.◦ Rim of distal radius
fracture with volar or dorsal displacement
Oblique fx of distal radius involving radial styloid
Intra-articular fx Generally require
surgery
Stiffness, swelling, pain Malunion/radial shortening DRUJ dysfunction RSD/CRPS Median nerve compression Radiocarpal arthritis Weakness Carpal instability Shoulder stiffness
Watch for substitution of EDC when attempting to perform wrist ext
Teach patient isolated wrist extension to learn to control EDC substitution
Initiate blocking exercises early especially FPL which can be adherent
Inability to flex IP during oppostion indicates FPL adherence
EDEMA CONTROL Splinting for stability and
protection Motion Modalities Pain management-watch for
increased sympathetic reaction, TENS
Function
Strengthening FES – mm. weakness
and retraining Dynamic splinting Work
simulation/hardening Activity Modification

One month post injury: resting position of hand with 25 degrees UD. Final numbers◦ Pro/Sup: 15/60 50/75◦ Ext/flex: 40/45 65/60◦ RD/UD: 35/20 15/30◦ 4 Weeks Post Op:◦ Splint◦ A/AAROM◦ Scar management◦ 6 weeks post op:◦ strengthening
Occur 1/10th as frequently as distal radius fractures
Scaphoid: account for 60-70%
Triquetrum/Lunate: second most common- account for 20%
Others: combined account for only 7-10% of fx
90% occur from force applied with wrist in extension (FOOSH)
Vulnerable to injury ◦ position in both proximal and
distal rows
Difficult to diagnose - often made based on clinical signs◦ Pain in snuff box
Variable healing times according to fracture site

5-20+ weeks depending on level
◦ poor vascular supply Direction of fracture
affects healing-horizontal quicker than vertical
Middle 2/3 10-12 weeks
Proximal 1/3
12+ weeks
Non- union Carpal ligament
injuries◦ Carpal instability
Delayed diagnosis Normal anatomical
alignment not restored
Persistent pain SLAC wrist
SLAC WristS scaphoidL lunateA advanced C collapse
Triquetrum: 2nd most common. FOOSH Lunate: Can result in avascular necrosis
(Kienbocks disease) Trapezium: often associated with
fractures/dislocations involving thumb Pisiform/Hamate: trauma over ulnar/volar
wrist, proximal hypothenar eminence Capitate: rare because this carpal is in a
centrally located and protected position Trapezoid: rare; crush or high energy impact
Focus on wrist and thumb ROM, and composite flexion
May require protective splint between exercise post cast removal
Functional ADL’s encouraged

Static progressive or dynamic splinting for wrist flexion and extension or composite motion
Grip strengthening Wrist strengthening within pain free range Work hardening depending on RTW status
Quick healing Occur more commonly
in the border digits Degree of angular
deformity accepted varies for each ray
Complications of angulation are extensor lag and decreased grip strength
Some degree of angular deformity is acceptable
Rotatory deformityie: fingers overlapping(scissoring) is not acceptable
This check is used for phalangeal fractures also
MP’s need to be immobilized in flexion to maintain collateral ligament length
Goal is to achieve alignment without rotation or shortening
Shortening of 3-5 mm can produce imbalance intrinsic/extrinsic
Malrotation= finger overlap
Angulation tolerated better in 4/5th MC

MC fx’s can result in soft tissue damage
Often excessive dorsal edema
Common because less soft tissue between extensors and MC’s
Result in MCP extension lags and extrinsic extensor tendon tightness
Treatment: isolated EDC exercises, scar massage, FES, combined wrist/finger flexion, other modalities
MP joint contractures can occur following metacarpal head and neck fractures
Proper positioning in splint crucial, at least 60⁰ MP flexion; if unable to obtain correct position readjust in a few days
“Hand Fractures can be complicated by deformity from no treatment, stiffness from overtreatment, and both deformity and stiffness from poor treatment”
Alfred Swanson
Type varies◦ Oblique, transverse,
spiral
Spiral/oblique tend to be unstable
Often cause soft tissue adherence
Comminution = more soft tissue damage
PIP flexion contracture Limited active PIP
extension Tendon adherence at fx
site
Edema control Splinting
Hand based Buddy taping
Motion: AROM AAROM
Once Healed PROM/dynamic splinting Functional activities Strengthening
Can start motion earlier due to stability of fixation
Addition of scar management
Soft tissue involvement
Account for 50% finger fractures
Thumb/middle most commonly injured
Crush common mechanism of injury
Classified by location
Heal w/out excessive treatment
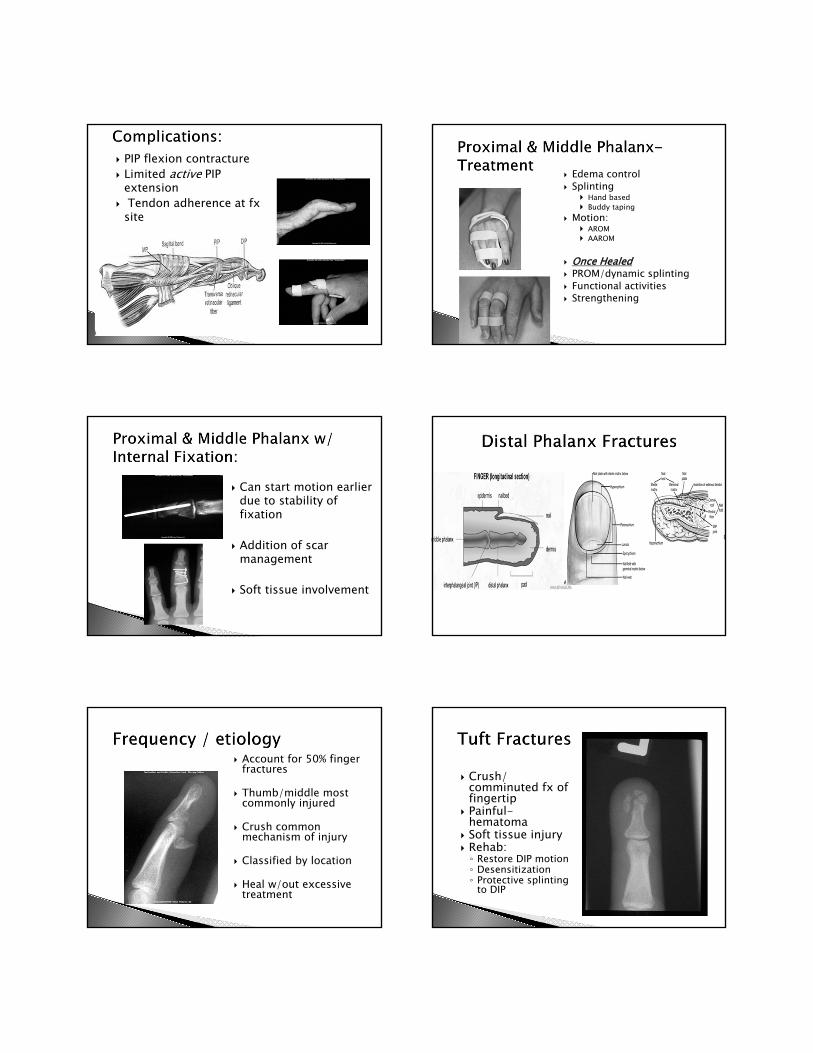
Crush/ comminuted fx of fingertip
Painful-hematoma
Soft tissue injury Rehab:◦ Restore DIP motion◦ Desensitization◦ Protective splinting
to DIP
Extensor tendon avulsion fx or dorsal intra-articular fx
“Flexion drop” deformity
Tx: Mallet splint◦ Slight hyperextension
A/PROM to MP/PIP
Splinting in extension for 6-8 weeks is standard. Once healed/stable may begin DIP flex
Continue splint use between exercise and at night
Watch for extensor lag with exercise (resume splint use if lag increases)
Resume motion and normal activities.
Numbness Hypersensitivity or
tenderness Cold intolerance Limited DIP ROM Nail abnormalities
Follows similar guidelines as for digits
Special considerations: ◦ Thumb joints can lose
motion faster than in fingers◦ Motion at basal joint
helps when MP joint motion is lost◦ Prevent 1st webspace
contracture
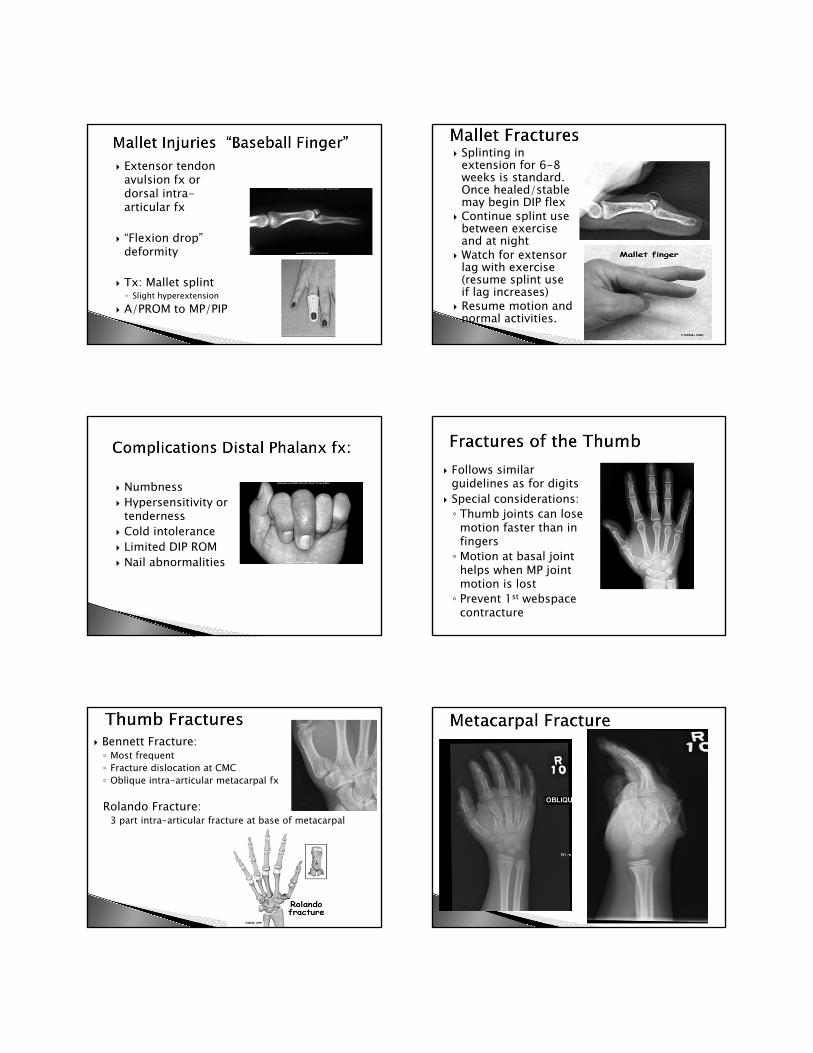
Bennett Fracture: ◦ Most frequent◦ Fracture dislocation at CMC◦ Oblique intra-articular metacarpal fx
Rolando Fracture:3 part intra-articular fracture at base of metacarpal

Clam shell splint: include MP and exclude IP joints
AROM (gentle) of IP joints Edema control
6 Weeks: started MP AROM/AAROM 8 Weeks: d/c splint and begin light
strengthening.
AROM IF MP: 15/60
PIP: 5/85LF MP: 10/75
PIP: 10/85R L
Lat pinch: 11 13.5Tripod: 12.511.5Grip: 33 38
Shortened IF metacarpal with dorsal angulation.
Slade,J, MD, et al, (eds), Hand Clinics: Scaphoid Fractures, Volume 17, No. 4, November 2001
Berger,R et al, (eds), Hand Clinics: External Fixation, Philadelphia, WB Saunders, Volume 9, No. 4, November 1993
Freeland A, Lindley, S, (eds), Hand Clinics: Hand Fractures and Dislocations, Philadelphia, WB Saunders, Volume 22, No. 3, August 2006.
Fischgrund, J, (ed), Orthopaedic Knowledge Update, Chapter 2, Fracture Repair and Bone Grafting, AAOS, 2008, pgs 13-19.
LaStayo, P, Winters, K, et al, Fracture Healing: Bone Healing, Fracture Management, and Current Concepts Related to the hand. Journal of Hand Therapy 2003; 16(2): 81-92
Cannon N: Rehabilitation Approaches for Distal and Middle Phalanx Fractures of the Hand. Journal of Hand Therapy 2003; 16(2): 105-116
Seu,M, Pasqualette,M :Hand Therapy for Dysfunction of the Intrinsic Muscles:, Hand Clin 28 (2012) 87–100
Kollitz M, Hammert WC et al: Metacarpal fractures: treatment and complications HAND (2014) 9:16–23
Sammer DM, Husain T, Ramirez R:Selection of Appropriate Treatment Options for Hand Fractures, Hand Clin 29 (2013) 501–505
Neumeister M et al: Non-surgical Management of Metacarpal Fractures Clin Plastic Surg 41 2014 p451-461
Suh N et al: Carpal Fractures J Hand Surg Am 2014, 39 (4) 785-791 Lalonde D et al: Pain Guided Hand Therapy for Hand Fractures: the Saint John
Protocol: contact Amanda Higgins at [email protected] for a digital copy of the protocol.
Feehan, L, Early Controlled Mobilization of Potentially Unstable Extra-articular Hand Fractures. Journal of Hand Therapy 2003; 16(2): 161-170
“A specialist knows the worst mistakes which can be made in his field and how best to avoid them”
- Nils Bohr