reaching mental health recovery together · the family experience of mental illness ... reaching...
TRANSCRIPT

ReachingMental Health
RecoveryTogether
TOOLS
A joint collaboration between:
Family Institute for Education, Practice & Research
Mental Health Resources
National Alliance on Mental Illness of New York State (NAMI-NYS)
New York State Office of Mental Health
January 5, 2010

Endorsements:
"This Family Survival Handbook is an important tool ...to aid families in providing a most comprehensive care and treatment available.
I thoroughly endorse this Family Survival Handbook as an important tool for the mental health
and wellness of the people of New York"Michael F. Hogan, PhD, Commissioner New York State Office of Mental Health
"This Handbook assists patients, families and others concerned in demystifying this complex issue and offering
a wide repertoire of assists... it is an invaluable tool...I am sure it will be seen as an outstanding help in making the exposure to this
very considerable stress from psychiatric disorders more manageable."Herbert Pardes, MD, President and Chief Executive Officer
New York-Presbyterian
"The Handbook is truly a well-written document with the potential to help many, many families and individuals
in navigating the mental health system."John B. Allen, Special Assistant to the Commissioner
New York State Office of Mental Health
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
I
Family Survival Handbook:Reaching Mental Health Recovery Together
Tools for and by families
A joint collaboration between Family Institute for Education, Practice & Research, Mental Health Resources,
National Alliance on Mental Illness of New York State (NAMI-NYS), New York State Office of Mental Health
ContentsABOUT THIS HANDBOOK ................................................................................................................................................1
INTRODUCTION ................................................................................................................................................3
THE FAMILY EXPERIENCE OF MENTAL ILLNESS ................................................................................................3
HOSPITAL CARE - WHAT TO EXPECT ................................................................................................................................5
Confidentiality - Getting consent........................................................................................................................5
Participation without consent ............................................................................................................................6
Treatment Team ................................................................................................................................................6
Family members as partners with the treatment team........................................................................................6
Roles and Responsibilities: Achieving Treatment Plan Goals ..............................................................................7
Treatment Plan ..................................................................................................................................................8
Cultural issues and support................................................................................................................................8
How to get hospital records ..............................................................................................................................9
What to do if you’re dissatisfied with your loved one’s care ..............................................................................9

II
PAYING FOR IT ALL ........................................................................................................................................................11
Introduction to Social Security Disability Insurance and Supplemental Security ................................................11
Income ............................................................................................................................................................11
Medicaid Buy-in Program for Working People with Disabilities ........................................................................11
How to get Food Stamps ................................................................................................................................12
How to get a Reduced Fare card......................................................................................................................12
DISCHARGE PLANNING: IMPORTANT CROSSROADS......................................................................................................13
Assisted Outpatient Treatment (AOT) ..............................................................................................................13
Emergency Planning (Crisis plans, WRAP and Advance Directives)....................................................................14
Family Contract................................................................................................................................................15
Housing ..........................................................................................................................................................15
Housing application in NYC & State pgs ..........................................................................................................15
Types of housing..............................................................................................................................................16
GETTING WELL, STAYING WELL ......................................................................................................................................17
Rehabilitation ..................................................................................................................................................17
Living with a loved one out of the hospital ......................................................................................................17
Sticking with medication..................................................................................................................................18
Don’t forget physical Health ............................................................................................................................18
Education and support programs ....................................................................................................................19
Cognitive Rehabilitation ..................................................................................................................................20
Nutrient approach to mental illness: Complementary and Alternative Medicine (CAM) ....................................20
Employment ....................................................................................................................................................21
Empowerment and the Peer Movement ..........................................................................................................22
Recovery..........................................................................................................................................................23
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
III
TOOLS YOU CAN USE ....................................................................................................................................................25
Hospital Checklist ............................................................................................................................................25
Management Log Sheets ................................................................................................................................35
Sample form: Family Contract ..........................................................................................................................36
RESOURCES....................................................................................................................................................................37
APPENDIX, MEDICAID BUY-IN........................................................................................................................................49
CONTRIBUTORS..............................................................................................................................................................53

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
IV
This page intentionally left blank.

The Family Survival Handbook is a collection ofpractical, useful information contributed by over65 family caregivers from New York City and State
who have learned from experience how to navigate thepublic mental health system in New York State. Intendedfor use by families when a loved one is first diagnosed,admitted to a hospital, and after his/her discharge, thishandbook’s purpose is to provide information and re-sources while guiding users with informative tips de-signed to enable them to:
� Access educational materials;*� Build a support network;� Advocate for their loved one;� Become meaningfully involved with their loved
one’s treatment team,� Participate in the development of meaningful, re-
covery-oriented Treatment and Discharge Plans;� Become informed about the spectrum of services
their loved one might need,*� Enable them to both request these services and
access them themselves, as necessary*With its companion pamphlets, When Families
Join the Mental Health Care Team Everyone Benefits!,and how-to guide, Understanding HIPAA, NYS MentalHygiene Law and the Confidentiality of Mental HealthTreatment and Information in New York State, this Hand-book will provide you with essential tools to help you bet-ter understand the many aspects of the mental healthsystem so you can effectively support your loved one whilehe or she navigates the mental health system. Whetherhe or she is experiencing a “first break” (i.e., first episodeof psychosis or first admission to a psychiatric ward) or arelapse, these materials will arm you with informationabout laws, policies, professional guidelines and resourcesto make your involvement in your loved one’s recoverydynamic and effective. Because this Handbook is focusedon a team approach to recovery, we encourage sharing allor part of it with your family member, as well as with theproviders that are caring for your loved one.
HOW DOES IT WORK?The Family Survival Handbook is organized into twosections. Part One highlights information you mayneed to quickly access, such as how to obtain yourloved one’s consent to have his/her treatment informa-tion disclosed to you, or how to apply for supplemen-
tal income or insurance benefits. Part Two includes re-sources and reading lists, as well as tools such as theHospital Checklist and Management Log Sheets tohelp you record important information, and captureand organize documents, in one easy-to-locate place.Part two also includes a list of resources. We encour-age you to make use of the Handbook during all meet-ings and telephone calls with mental healthprofessionals, and use the Pamphlet and How-to guideas a basis for your advocacy efforts.
The Handbook uses the following logos to make iteasy to find the information you need:
The Resource Logo identifies where you canfind additional information about a particu-lar topic, such as contact information, linksand/or websites. This information is locatedin the “Resource” section in the back of theHandbook. Resource pages start at pg. 37.
The Toolbox Logo alerts the user that the ref-erenced worksheet can be found in the“Tools You Can Use” section in the back ofthe handbook. These tools include:
� The Hospital Checklist: this is a worksheet youcan use to store all pertinent information regard-ing your loved one and his/her treatment. It iscritically important to have this informationreadily available when your loved one is hospital-ized. The Checklist provides space where youcan record information including your lovedone’s contact information, the names/ contactinformation of mental health professionals whohave been involved in providing care to him/her,diagnoses, status of government benefits, treat-ment goals, medication lists and discharge plan-ning. This Checklist is located at the back of theHandbook in the “Tools You Can Use” section,will arm you with the facts you need to intelli-gently and effectively represent your loved one ifhe or she is hospitalized, and ensure the hospitalhas the critical information it needs to providequality care.*
� Management Log Sheets: These forms can serveas your “working papers” where you can record a
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
1
About this handbook
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
2
chronological list of people with whom you speakwith respect to your loved one’s care, noting whatwas said and what determinations were made,both in and out of the hospital setting. Thesesheets are located at the back of the Handbook inthe Tools You Can Use section, will help yourecord information that may be difficult to recallor gather at a later time. Information docu-mented on these sheets can form the foundationfor future dialogues, inform the decisions madeby future treatment teams, and serve as a record ifever you need to file a complaint. If you needhelp in completing these forms, we recommendthat you ask a hospital social worker or case man-ager to assist you.
Pamphlet and How-to guide on inside flap andare also available on the NYS OMH and NAMINYS web sites:
It’s not possible to advocate for your rights if you don’tknow what they are. The materials below, which areavailable in the side flap of the Handbook, not only ap-prise you as to what your rights are, but can serve as pow-erful tools for your advocacy efforts:
� When Families Join the Mental Health CareTeam Everyone Benefits!
� Understanding HIPAA, NYS Mental HygieneLaw and the Confidentiality of Mental HealthTreatment and Information in New York State

FINDING OUT YOUR LOVED ONE has a men-tal illness may be the toughest experience of yourlife. Few families are prepared or equipped to han-
dle the traumatic and demanding responsibility suddenlythrust upon them. You are in an unfamiliar world with nocompass to guide you. Yet, you must immediately be-come an advocate as you find information, locate serv-ices, navigate the mental health system, and manage theemotional, social and financial consequences of mentalillness that affects everyone involved. How will you cope?
Here’s the good news. Never before have weknown so much about mental illnesses and how to en-able people living with the diseases to live, work, learnand participate fully in the community. Long-term stud-ies have consistently shown that over half of people diag-nosed with major mental illness go on to a significant orcomplete recovery. The new field of neuroscience isproving that the brain can regenerate to a greater degreethan was previously thought possible. Significant ad-vances in research are providing a wider range of med-ications and psychosocial treatments that offer tools forself- and peer- help. Meanwhile, the mental health sys-tem is beginning to accept the truth that recovery is pos-sible, particularly with support from peers, family andcommunity. For the first time, optimal well-being or“wellness,” not just absence or reduction of symptoms, isthe goal of mental illness treatment.
Despite gains made in recent years, challenges re-main. Although research and everyday experience hasshown recovery occurs best when treatment profession-als, the family and the patient work together, much of theinformation needed by consumers and families is still noteasily accessible. This means families not only have tolearn what information they need, but they must alsowork hard to get it and understand how to use it.
Successful families learn how to advocate, whichmeans to “plead the cause” to “argue, defend, recom-mend.” In order to stand up for what your loved one de-serves, you must know. You must know the laws thatgovern their, and your, rights, and you must be persistentand vigilant to ensure that facilities comply with them. Tosome degree, the services you get will be the ones youfight for and insist on.
In this time of economic hardship, families have tofill the gap left from diminishing services. Families mustbe resilient and self reliant—we need to help ourselvesand our loved one as never before.
We know we are throwing a lot of ideas and possi-bly unfamiliar language at you all at once. First-timersmay want to initially focus on the Hospital Care/PayingFor it All/Discharge Planning sections located in the frontof the Handbook. Our goal, however, is to provide a ref-erence to enable you to become familiar with the entirespectrum of what you’ll potentially have to deal with.There is a huge amount of help for you in the mentalhealth system, but it’s up to you to find it and use it. ThisHandbook can empower you to ask informed questions,track the professionals’ progress, have the tools to takeover when necessary and even be ten steps ahead of thegame! We hope, with this Handbook reference, questionswill be answered for you in a way that they haven’t beenfor families in the past.NOTE: We use the term “Loved One,” “Con-sumer,” “Patient” and “Peer” interchangeably.
FAMILY EXPERIENCE OF MENTAL ILLNESS
WHEN MENTAL ILLNESS STRIKES, it is afamily affair. Regardless of who carries the symp-toms, the event is a catastrophic one that affects
all family members. Therefore, the entire family needsto be involved. The ill family member must be supportedand stabilized. Well family members need assurance thatthey are not to blame for their loved one’s circumstanceand that the situation is not hopeless.
Most often, when a loved one has been hospital-ized, he or she is experiencing symptoms and may displaybehaviors that can make them seem unrecognizable—even to family members who have known the person allof his/her life. Educating yourself about the nature ofmental illness will give you a window into your loved
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
3
Introduction: Your loved ones in the hospital.
Now what?

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
4
one’s struggle and help you understand that their illnessis not their identity.
A mental illness can rob your loved one ofstrengths, coping skills and cognitive abilities—which arethe basic mental skills we use to think and learn. In fact,depending on their diagnosis, your loved one may not re-alize he or she is sick, displaying a common symptomcalled Anosognosia or “lack of insight.”
Severe lack of awareness is part of the disorder. Psy-chologist Xavier Amador, who has studied this phenom-enon, counsels to "externalize the illness by Listening,Empathizing, Agreeing and finding Partnership (theLEAP approach). LEAP is a way of connecting and get-ting out of the battle... to find a common ground to allowan ill person to find his own reasons for being adherent.You can't use logic and expect insight when someone isdelusional-the brain dysfunction is the enemy, not thepatient.
GETTING SUPPORT: OTHER FAMILIES ARE THE BEST SUPPORT
Some people have one episode of mental illness andthen get on with their lives with little or no impairment.For others, these disorders of the brain can be lifelong ill-nesses, with a level of disability ranging from modest to se-vere.
The process and outcome of mental illness cancause family members to cycle through feelings of hopeand despair. While it is a normal part of the family re-covery process, shifts in feelings can be extreme, painfuland confusing.
One of the most useful sources of support for fam-ilies is.... other families!. Families can experience one ormore of the following stresses when coping with mentalillness in the family: financial, interpersonal, marital, so-cial, emotional, physical and/or spiritual. Sharing expe-riences and feelings in family support groups can reducetension and help identify solutions that others with sim-ilar experiences have found useful.
And don’t wait! Experienced caregivers say joininga good support group as early as possible is critical. Overtime, you must learn to create a balanced life for yourselfand other well family members, even as you care for thefamily member who is ill.
NAMI’s signature Family-to-Family Program is afree twelve-week course offered by National Alliance onMental Illness affiliates or chapters all over the country.Call them at NAMI-NYS at (518) 462-2000 or 800-950-3228 to locate the one nearest you.
SUPPORT GROUPS
The time to join a support group is right now.Here’s what they can offer:� Emotional support� A break from isolation� An outlet for from the range of emotional
stresses named above� How-to information� A chance to compare notes on local services*� Ability to draw on the experience of others*� Opportunity to work through the “Stages of
Grief”, including denial, anger, bargaining, andacceptance.
LACK OF INSIGHT: THERE’S NOTHING WRONG WITH ME1
Your loved one may not realize he is ill. Instead, hemay actually believe his delusions and hallucina-tions are real. The term used by neurologists is“anosognosia,” which comes from the Greekword for disease (nosos) and knowledge (gnosis),literally meaning, “to not know a disease.”
Here’s what we know about anosogosia:� It is not denial, but a symptom of illness.� It is caused by damage to specific parts of the
brain, most likely the frontal and parts of theparietal lobe.
� It affects approximately 50% of individualswith schizophrenia and 40% of individualswith bipolar disorder.
� Individuals can be partially aware or fluctuate,being more aware when they are in remissionand less aware when they relapse.
� It is the single largest reason why individualswith schizophrenia and bipolar disorders donot take their medications.
� Medications can improve awareness in somepatients.

HOSPITAL CARE
IN THE CASE of an airplane crash landing, adult pas-sengers are instructed to first put the oxygen mask ontheir own faces and then help their children with
theirs. Likewise, when mental illness hits, families willbe in the best position to help an ill family member ifthey make sure they take care of themselves and othermembers of the family.
The dictionary defines rehabilitation in this way:“To restore to a state of physical and mental healththrough treatment and training.” For families, rehabili-tation is about acquiring information and education,working through feelings and reaching acceptance,while learning ways to help the family rebuild.
Rehabilitation is a process that begins in the hos-pital and continues after your loved one’s discharge. A re-habilitation program includes many components (see“Rehabilitation” on page 17). Several activities thatshould take place while your loved one is hospitalized andimmediately after his/her discharge:
1. The patient and his/her family should receivetimely education about the illness and the impor-tance of staying on medications.
2. The family should immediately become involvedwith the patient’s Treatment Team, as authorizedby the patient.
3. The patient, and family members as appropriate,should attend programs and post-discharge meet-ings to monitor the patient’s illness, watch forearly signs of relapse, and obtain support and in-formation.
The extent and depth to which you are involvedwith your loved one’s treatment could affect the course ofhis or her illness. One main goal of this section is to showyou what you should expect to be entitled to, and how toget what you deserve.
CONFIDENTIALITY—GETTING CONSENTIn general, an adult competent patient must give per-mission to the hospital before a family member can beprovided with information about the patient’s case. TheFederal Health Insurance Portability and AccountabilityAct (HIPAA) and New York State Mental Hygiene Lawwhich protect the confidentiality of patient informationare unfortunately misunderstood, and sometimes evenmisused, to create an artificial barrier to family involve-ment in a loved one’s treatment.
Under HIPAA, persons have the right to “agree orobject” to disclosures to family members or persons in-volved in their care. Similarly, New York State’s MentalHygiene Law state that patient “consent” must be givenbefore disclosures to family members can be made., butthe actual form the “consent” must take is not specified.Therefore, as a general rule, an adult patient must givepermission before families can be provided with infor-mation about them, and the fact that this permission hasbeen obtained should always be documented.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
5
INFORMATION NEEDS OF FAMILIES
� While your loved one is in the hospital, make sure you find out the following information:� What is the patient’s psychiatric diagnosis (for example, schizophrenia), and what does it mean?� What is the patient’s treatment plan for the psychiatric disability?� What are some ideas and strategies on how to prevent a relapse?� How can symptoms be identified?� What resources and supports are available?� What are some sources of personal stress and how can they be addressed?� What is the family recovery process?� What family/patient self-help/ advocacy groups are available?� What are the legal issues to be aware of , e.g., patient rights, trusts and commitment laws?
Record the specifics in the Hospital Checklist pgs. 25-34, and the Management Log Sheets (pg 35.)

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
6
PARTICIPATING WITHOUT CONSENT
If the patient will not give consent to a family membervoluntarily, here’s what you need to know:
1. General information (such as mental health in-formational materials or information about com-munity resources) is not confidential and can betremendously helpful to family members.
2. Staff may discuss a range of subjects in a generalfashion, provided they do not reveal specific in-formation about the patient, such as the availableprograms offered by the hospital, or general pro-cedural information, such as how privileges canbe obtained. .
TREATMENT TEAMThe term “treatment team” usually refers to those em-ployees of a facility who are responsible for the direct careof a patient (doctors, case managers, psychiatric nursesetc.). Sometimes, the treatment team can be expanded toinclude outside specialists such as vocational rehabilita-tion providers. However, the patient usually must grant
permission for them to be on the team and have accessto confidential treatment information.
FAMILY MEMBERS AS PARTNERS WITH THE TREATMENT TEAMFamily members are often called upon to play a significantrole in the support of their ill family member. Becausefamily members can have insight that is incredibly valu-able to the treatment team, such as family health history,the history of a loved one’s illness, the patient’s current
FIRST THINGS FIRST - TRY TO GET CONSENT!
Confidentiality rules reflect the fact that health and mental health information is sensitive. These rules are designedto protect the privacy of the person to whom the information pertains. As a general rule, competent adult patients(age 18 years of age and older) have the right to choose with whom their medical information is shared.
In order to allow the hospital to share confidential information with family members, your loved one should sign a“consent form.” Although consent can be made verbally (and should be documented in his or her clinical record), ifsomething is not in writing, it is harder to prove it exists. Having a signed consent form in hand will increase yourability to fully participate in confidential aspects of your loved one’s treatment and discharge planning.
On the inside flap you’ll find Understanding HIPAA, NYS Mental Hygiene Law and the Confidentiality of MentalHealth Treatment and Information in New York State this is also available on the NYS OMH website. For the firsttime, this “how-to” guide addresses many issues around when and how family can work with the mental healthteam, whether or not with patient consent. In plain English, with lots of examples applicable for consumers, familyand providers, this exhaustive look includes such subjects as:� What is the difference between NY State Mental Hygiene Law and HIPAA?� What are the rules that govern disclosure of clinical records?� How can family provide important information, even without the patient’s consent?� Why is confidentiality an important principle in health care; what is the Hippocratic Oath?*
A complete guide to the Confidentiality of Mental Health Treatment and Information is provided in the inside Flap:
—Understanding HIPAA, NYS Mental Hygiene Law and the Confidentiality of Mental Health Treatment and Informa-tion in New York State
TIP: Although professionals might not be able to talkto you if your loved one has refused to sign a con-sent form, there is no reason why they shouldn’t lis-ten to you, directly or by phone, fax or email (pleasenote some facilities may require that communica-tions that include patient identifying information bemade in a secure fashion to protect patient privacy) .Also, staff may share information provided by thefamily to the patients, such as messages of support,unless the doctor does not allow it

strengths and deficits, what was the level of his/her func-tioning before the onset of the illness, and/or knowledge oftheir loved one’s use/abuse of alcohol or illegal substances,they are an important resource. Family involvement andcollaboration with the treatment team should be activelyencouraged and supported whenever appropriate.
Unfortunately, some facilities may not encouragefamily involvement with the treatment team, eventhough organizations such as the American PsychiatricAssociation recognize in their guidelines the consider-able benefits to treatment of doing so: “A guiding princi-ple is that the patient’s family members should be involvedand engaged in a collaborative treatment process to thegreatest extent possible.” (American Psychiatric Associa-tion, Practice Guidelines for the Treatment of Patients withSchizophrenia, second ed., 2004, pp. 70, 106).
Furthermore, with respect to facilities operated bythe New York State Office of Mental Health, Section29.13 of the Mental Hygiene Law requires the develop-ment of a written treatment plan. The treatment planoutlines treatment goals, what programs or therapies willbe undertaken to achieve these goals, and a timetable forassessing progress. Under this law, parents of minors inOMH operated facilities must be involved in the devel-opment of a treatment plan, (unless the minor is over 16years of age and objects to such participation, and a cli-nician determines it is not clinically appropriate to in-volve them). If an adult patient in an Office of MentalHealth operated facility requests that a family memberbe involved in the development of his/her treatmentplan, that person must be included in its development
Other accrediting organizations, such as The JointCommission, have stated that “patients and, when ap-propriate, their families [must be] informed about theoutcomes of care, treatment and services.” (The JointCommission, Comprehensive Accreditation Manual forHospitals (CAMH), 2006, §RI.2.90, second ed., 2004)
All of these references, as well as others, are in-cluded in the pamphlet, When Families Join the MentalHealth Care Team Everyone Benefits! (see inside flap).We encourage you to become familiar with the infor-mation in this pamphlet and feel free to share it with yourloved one’s providers of care!
ROLES AND RESPONSIBILITIES: ACHIEVING TREATMENT PLAN GOALSThe contributions that should be expected of mentalhealth professionals, family members, and the patient, asthey partner together to develop and achieve the goals ofthe treatment plan, follow below:
Mental Health Professionals (the following assumes anynecessary consents have been obtained)
1. Encourage and include families in discharge andtreatment planning.
2. Seek information from families about the history,background and day-to-day progress of their rela-tive’s illness.
3. Inform families of shifts in treatment strategiesand changes in medication.
4. Give timely reports on the patient’s progress.5. Consult with and inform families about possibili-
ties for improving their relative’s condition.6. Establish open channels for family complaints
and grievances.7. Validate the family’s early warning signs of relapse.8. Remain in close contact during crises to offer
concrete advice and assistance.
Family members1. Provide the treatment team with details, prefer-
ably written, of the history of your loved one’s ill-ness (e.g., how it started, warning signs and familymental illness and/or addiction history) Keep itupdated and be ready to give out copies to anynew professional involved.
2. Cooperate with mental health professionals.3. Maintain the Hospital Checklist
and Management Log4. Keep a journal.5. Become educated about mental illness.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
7
TIPS FOR WORKING WITH TREATMENT TEAM MEMBERS
� Act professionally - be calm, polite and persistent.
� Respect others’ time - be prepared for meetings, and don’t be late.
� Prepare for meetings by writing down the points you want to cover (to be submittedat the meeting, as necessary). Be concise butthorough in your communications.
� Record information on the Hospital Checklistand Management Log Sheets (pgs 25-35)

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
8
6. Become familiar with the laws and professionalguidelines surrounding mental health practicesand family involvement (see pamphlet on insideflap, “When Families Join the Mental HealthCare Team Everyone Benefits!” and Understand-ing HIPAA, NYS Mental Hygiene Law and theConfidentiality of Mental Health Treatment andInformation in New York State).
7. Become informed about mental illness and themental health system so you know what to ask forand how to ask for it.
8. Advocate for, and support, your loved one.
PatientsPatients have a personal responsibility for their own self-care and journeys to recovery. Taking steps toward theirgoals requires great courage. Patients must strive to un-derstand and give meaning to their experiences and iden-tify coping strategies and healing processes to promotetheir own wellness. Their job is to manage their symp-toms or their symptoms will manage them.
TREATMENT PLANThe Treatment Plan outlines treatment goals along withprograms and/or therapies that will enable the patient toachieve his or her goals. In addition to a timetable fortracking progress, the treatment plan should address atleast these six elements:
1. Role of family and professional staff2. Pertinent information related to mental illness3. The facility’s programs and services , as well as
others offered locally and by the state4. Names and telephone numbers of key staff and
administrators5. Names of Mental Hygiene Legal Service attor-
neys6. Hotline numbers and regularly scheduled hours
when families may make telephone contact ormeet with specific staff
Chances are, after your loved one is dischargedfrom the hospital, you’ll be called upon to provide somesort of assistance, such as providing housing or trans-portation. You should be consulted first. If you are un-able to provide a service, and the patient is a competentadult, you are under no obligation to do so—you canrefuse for any reason. This includes the right not to ac-cept the loved one back into your home.
CULTURAL ISSUES AND SUPPORT
As you partner with the treatment team, you must makesure the treatment plan is realistic, effective and sup-portive of your loved one’s goals. One factor often over-looked by both family members and mental healthprofessionals alike is the role culture plays in the familyexperience of mental illness.
When we talk about culture, what we mean is a setof beliefs, behaviors, norms, values, and language sharedby people grouped together because of common tiesbased upon race, ethnicity, faith, gender, age, sexual ori-entation, etc. Because culture impacts the way peopleinteract with one another, it is important to recognizethat a person’s culture shapes the way they perceive andexperience mental illness. A family’s culture could in-fluence whether and when they seek help, what type ofhelp they seek, what coping styles and supports they have,and what treatments might work. Mental health profes-sionals are not only affected by their personal culture, butalso by the culture of the medical field, which relies heav-ily on science and open communication for diagnosis.
When the provider’s cultural background differsfrom that of the patient and/or family (especially if thereis a language barrier), the lack of knowledge about thepatient/family’s culture can create impediments to effec-tive treatment, including misunderstandings that can re-sult in a wrong diagnosis. Although most providers wantto work sensitively and effectively within various culturalcontexts, it may be easier to find written information innon-English languages, than to find professionals skilledat delivering treatment that is sensitive, relevant and cul-turally competent.
In addition, after a patient has been discharged,some families have difficulty finding support groups withwhich they are comfortable. These are some problemsfamily members have reported experiencing when tryingto integrate themselves into mainstream support groups:
� Lack of aggressive and innovative outreach tofamilies outside of mainstream culture.
� Structure and leadership styles may not reflectdifferent cultures’ preferred styles.*
� Support group leadership and membership maylack comfort with issues of diversity or may simplylack knowledge or information.
� Social activities sponsored by groups may not befamiliar, appealing or comfortable.
� Programs may be held in settings outside ofneighborhood communities or in places wherepeople feel uncomfortable.
� Lack of people from cultural group may cause fam-ilies to feel alienated, isolated or uncomfortable.

In order to receive appropriate treatment and finda support model for your loved one and family memberthat is consistent with your cultural style and strengths, beprepared to reach out, bridge knowledge gaps, make con-nections and educate others about your culture.
Cultural differences to consider:� Communication and presentation styles� Verbal expression: open, self-disclosing, or closed?� Eye contact� Distance in personal space� Problem-solving and decision-making� Familial or gender role expectations and responsi-
bilities� Religious or spiritual beliefs and practices
What works?A. Find a mainstream program that already exists.B. Consider a “family network” approach. As op-
posed to building a group of unrelated individu-als, this approach builds upon a large familynetwork that shares kinship ties or membership inkey community institutions, such as a church orwell-regarded neighborhood community center.Family network approaches can make use of col-lective problem-solving and conflict resolution,which is common in many cultures.
C. Join or create an ethnically or culturally specificpsycho-educational group where all members arefrom the same cultural group.
See “CULTURAL ISSUES AND SUP-PORT” in the resource section. (p. 40)
HOW TO GET HOSPITAL RECORDSYour loved one has the right to request access to his orher hospital records. If the hospital is required to complywith HIPAA, it will give the patient a Notice of PrivacyPractices, which should provide information on how torequest this access. Usually, this is done by dropping offa written request at the “Records” window, signed by thepatient, before he or she is discharged. Although the hos-pital has the right to charge a reasonable fee for copyinga record (unless the patient does not have the ability topay) most often, they are provided without cost. It’s im-portant to have these records, which document infor-mation that was used to make decisions about the patient,as a basis for building a recovery history.
WHAT TO DO IF YOU ARE DISSATISFIED WITH YOUR LOVED ONE’S CARE
Locate the most appropriate staff member to address yourissue. If you cannot reach that person by phone, write aletter and deliver it by fax or email. The Mental HygieneLegal Services (MHLS) should be available to assist pa-tients and their families with complaints and are often lo-cated on or near the grounds of State operated psychiatrichospitals (note that MHLS is part of the Office of CourtAdministration and is not part of, nor does it legally rep-resent, the hospital). Within the hospital itself, the fol-lowing personnel or departments can handle complaints:Director of the Hospital, Office of Patient Relations, orRisk Management (Quality Assurance). A hospital’sBoard of Visitors is empowered to inquire into the work-ings of the hospital and make recommendations. You canalso contact the Office of Mental Health Customer Re-lations/General Information line at 1-800-597-8481 forguidance. Use the Management Log Sheets, included inthis Handbook, to document the relevant facts and dates,and to substantiate your complaint
See “COMPLAINTS” (p. 38) and “LEGALISSUES” (p. 45)
PEER BRIDGERS: COMPLEMENTARY SERVICES TOSUPPORT RECOVERY
As a complement to mental health services, PeerSpecialists, who have taken additional training to qualifythem as "Bridgers," can not only assist with discharge, butcan also assist with community integration, resource link-ing, attainment of independent living, gainful employ-ment, and other services needed to complete the journeyto recovery. "Bridger" services are currently available in 6counties (Albany, Ulster, Broome, Queens, Suffolk andWestchester). It is recommended that Bridgers be con-tacted early in the process to provide support in the hos-pital as the consumer explores or approaches discharge.For more information: www.nyaprs.org
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
9
R
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
10
This page intentionally left blank.

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
11
INTRODUCTION TO SOCIAL SECURITY DISABILITY INSURANCE AND SUPPLEMENTALSECURITY INCOME
THERE ARE TWO U.S. government disability pro-grams in the Social Security Administration thatmay help. One is Social Security Disability Insur-
ance (SSDI), an insurance program. The other is Sup-plemental Security Income (SSI), an income basedprogram.
If mental illness is preventing your family memberfrom working, obtaining income and health coverage topay for hospital care is essential. The patient may file forSSI and/or SSDI, as well as Medicaid or Medicare cov-erage. Here’s what you need to know about these pro-grams:
� A person may receive both SSDI and SSI.� Both programs have the same standard of disabil-
ity for adults. The impairment must be severeenough to prevent the person from performingany substantial gainful activity to obtain SSDI.
� A person earning more than $980 per month—the figure for 2009—is presumed to be perform-ing substantial gainful activity, and is ineligible.
� SSI recipients automatically qualify for Medicaidin New York State, if a person gets as little as $1in SSI benefits
� Former SSI recipients can still maintain Medi-caid if otherwise eligible.
Once a disability claim is filed at the district office,it will be sent to the Disability Determination Services(DDS) for evaluation of disability.
The process may be tedious; however, the effort isvital in both the short- and long-term to get coverage forcrucial services, which might otherwise be unaffordable.(p 36 Benefits Eligibility, p. 44, “Health Insurance, p. 47Social Services)
See “BENEFITS ELIGIBILITY” (pg 37)
A SUBSTANTIAL SALARY DOESN’T HAVE TO JEOPARDIZE YOUR BENEFITS: MEDICAID BUY-IN PROGRAM FOR WORKINGPEOPLE WITH DISABILITIES (MBI-WPD)
The Medicaid Buy-In program offers Medicaid health in-surance coverage to people with disabilities who areworking and earning more than the allowable limits forregular Medicaid. Your loved one can earn as much as$55,188 per year without the risk of losing Medicaid.Through this program, your loved one will have the op-portunity to return to the work life and aspirations he orshe had prior to the onset of illness.
To qualify for the Medicaid Buy-In program forworking people with disabilities, you must
� Be a resident of New York State;*� Be at least 16 years of age (coverage up to 65
years of age);*� Have a disability as defined by the Social Security
Administration;*� Be engaged in part- or full-time paid work*� Have a gross income less than $55,188 for an in-
dividual, $73,884 for a disabled couple in 2009� Have non-exempt resources that do not exceed
$13,800 for an individual, $20,100 for a disabledcouple in 2009.
If you apply, be prepared to submit proof of the following:� Disability (if you are currently receiving a form
of Social Security benefits for the disabled, thatproof should be sufficient). Even if you don’t re-ceive benefits, you also qualify if you meet SocialSecurity eligibility requirements as “disabled.”
� Medical: Name, address and telephone numberof physician.
� Benefits: Medicare Part A and B, private healthinsurance (if you have these benefits).
� Income: Social security, alimony, veteran’s bene-fits, monetary support from family members.
� Citizenship: Birth certificate, U.S. Passport, Nat-uralization certificate with photo ID
� Residency: ID card, letter/lease/rent receipt withhome address.
� Resources: Money in a bank, stocks, bonds, mu-tual funds, certificates of deposit, money marketaccounts, and 402k plans, trusts, cash value of lifeinsurance.
PAYING FOR IT ALL
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
12
Don’t be overwhelmed. Medicaid customer service spe-cialists can provide support and a “Tool Kit” to help guideyou through the process. Missing application items maybe submitted for up to ten days.
See a step-by-step guide to obtaining Medicaid-Buy-In and a “Medicaid Buy-in At-A-Glance” sheet to share at the MedicaidOffice to assure obtaining the service you
need (pgs. 49-52 Appendix)
HOW TO GET FOOD STAMPSYour loved one may qualify for Food Stamps to supple-ment his or her food budget (and you don’t have to bedestitute). You don’t have to wait for a mental healthprovider to get it for you. You can take action yourself.
This federal Supplemental Nutrition AssistanceProgram (SNAP) program, run by state and local agen-cies, gives Food Stamps, in the form of a debit card forlow-income households. How much you receive is basedon your income.
See “FOOD STAMPS.” for information of whereto download applications and to find contact informa-tion for office locations where you can apply (p. 42)
GET A REDUCED FARE CARDThose on Medicare who have serious mental illness orreceive Supplemental Security Income (SSI) can get“Reduced Fare” NYC Metro Card and enjoy half-fare.You don’t have to wait for a mental health provider to getit for you. You can take action yourself. (p. 46.)
R

BY LAW, hospitals must develop a written treatmentplan for every patient. An important component ofthe treatment plan is the discharge plan, as it acts
as a guide for treatment and identifies which services andsupports will be offered to help your loved one recover.
As with the treatment plan, with the patient’s con-sent, family members should be involved in the devel-opment of the discharge plan—especially since familycaregivers will be directly affected by these decisions.
With respect to NYS Office of Mental Health op-erated psychiatric centers, Mental Hygiene Law §29.15(f) (reference “When Families Join the Mental HealthCare Team Everyone Benefits! Pamphlet inside flap) saysthat the discharge plan must be a written one, preparedin consultation with someone authorized to represent thepatient, and must at least address the following:
1. Statement of patient’s need, if any, for supervi-sion, medication, aftercare services, and assis-tance in finding employment followingdischarge;
2. Housing recommendations and a list of availableservices ;
3. List of organizations, facilities, and individualswho will provide services in accordance withidentified patient needs
4. Notification of appropriate school district andspecial education for patients under 21
5. Evaluation of patient’s need and potential eligi-bility for public benefits.
ASSISTED OUTPATIENT TREATMENT (AOT): A WAY TO DEAL WITH RISKAn Assisted Outpatient Treatment or an AOT designa-tion is a court-ordered treatment plan designed to help se-riously mentally ill individuals who are “at risk” tothemselves or others to comply with treatment. The orderwill require a person to accept the treatment that thecourt determines is necessary, and will require the localcounty director to provide such treatment.
An AOT treatment plan can detail a range of serv-ices that a person might need: medical, educational, vo-cational and supervision of living arrangements, to namea few. A patient with an AOT designation is assigned to acase manager, who assists the person in following the
plan. Because the county director is required to furnishthe treatment, AOT status usually gives the person top pri-ority for services from their local mental health system.
Once a person is under an AOT court order, it isexpected that he or she will comply with it. If a doctordetermines that the person has not complied with someaspects of the order, and also determines that he/she mayneed involuntary admission to a hospital, the doctor canrecommend to the county director that the person betransported to a hospital and held for up to 72 hours todetermine if inpatient care and treatment are necessary.If the person has refused to take prescribed medication,or has failed a test designed to determine either medica-tion compliance or alcohol or drug use, that refusal orfailure may be considered by the doctor in making thisdecision. Any decision to hold the person for more than72 hours must be in accordance with the legal proce-dures for involuntary admission.
The process to obtain an AOT order begins with apetition to a civil court. An investigation will follow to de-termine if the patient meets the criteria. The court mustbe satisfied that AOT is the least restrictive alternative be-
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
13
DISCHARGE PLANNING:IMPORTANT CROSSROADS
QUALIFYING FOR AOT
To qualify for AOT designation, a patient must:� Be at least 18 years of age and have a mental
illness;� Be unlikely to survive in the community with-
out supervision, based on a clinical determina-tion;
� Have a history of non-compliance with treat-ment for mental illness that has been a signifi-cant factor in his or her being in a hospital,prison or jail within the preceding three years,or which has resulted in one or more acts, at-tempts, or threats of serious violent behaviortoward self or others within the preceding fouryears
� Be unlikely to voluntarily accept the treatmentrecommended in the treatment plan
� Need AOT to avoid a relapse or deteriorationthat would likely result in serious harm to selfor others
� Be likely to benefit from AOT.

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
14
fore granting an AOT order. If a less restrictive treatmentor program exists that could effectively address the per-son’s mental health needs, the court will not grant thepetition for an AOT order.
The director of the hospital can make an AOT pe-tition or arrange for it to be done through the localcounty, so it’s easiest and best to ask for it while the patientis in the hospital.
See “AOT” to find information for contactingyour local county AOT Coordinator (p. 37)and/or area Family Liaison (p. 54);for re-sources on New York State’s Kendra’s Law, thelaw from which AOT was derived. (p. 45)
EMERGENCY PLANNINGNo recovery plan can be complete if it avoids planningfor the next possible crisis. Crisis planning allows patientsthe opportunity to express preferences for their care incase of an emergency.
The crisis plan can be an effective tool in engage-ment, and sets the stage for consumer choice and recov-ery. When consumer engagement is an issue, the crisisplan can be used as an effective tool for dialogue betweenthe clinician and the consumer. Crisis plans are typicallyupdated during an annual review process or when thelife circumstances of the consumer change.
There are three types of plans to prepare for or pre-vent a crisis. They include:
1. Crisis plans2. Wellness Recovery Action Plan (WRAP)3. Psychiatric Advance directives
Crisis PlansA crisis plan document can be part of a patient’s treat-ment plan. Initially, a patient’s crisis plan may have onlyone item such as, “this is how I know when I need help”or “this is who to call when I need help.” The basic ele-ments of the Crisis plan can include any of the following,and can be expanded to include anything else that thepatient feels is important to address in this document :
1. Signs that I am not feeling well2. Signs that I need help from others3. Who to call when I need help (My support team)4. Who not to call when I need help5. My medications are6. I take medication to7. My doctor or provider is
8. This is what usually works when I need help9. Please make sure someone on my support team
takes care to
Wellness Recovery Action Plan (WRAP)The Wellness Recovery Action Plan (WRAP) is a self-management and recovery system developed by personsliving successfully with mental illness. The programteaches people in recovery to develop activities for every-day well-being, track triggering events and early warningsigns, prepare personal responses for when they are feel-ing badly, and create a plan for supports to care for them-selves to decrease the severity and frequency of symptomsand improve the quality of their lives. WRAP comes inmany forms: seminars, “WRAP groups,” books, DVDsand online classes
See “WRAP” in the resource section. (p. 48)
Psychiatric Advance DirectivesPsychiatric Advance Directives are another group of toolsthat are useful to have in place before a relapse or otherpsychiatric emergency occurs. These legal forms are pre-pared when a person is competent and provide instruc-tions about health care to be followed if a person isdetermined to be incapable of making decisions regard-ing her/his physical or mental health treatment.
There are several types of Advance Directives:Durable Power of Attorney - A legal document that
allows an individual to designate a person (usuallya trusted family member or friend) to manage hisor her financial affairs if he/she becomes unableto do so/t . Before the NYS Health Care Proxy lawwas enacted, durable powers of attorney could beused to delegate health care decision making pow-ers, but that is no longer true. Now that theHealth Care Proxy law is in place, durable powersof attorney cannot be used to assign authority tomake health care decisions, unless it was signedprior to July 1, 1990 (which is when the HealthCare Proxy law went into effect).
Health Care Proxy - A legal document that allowsan individual to designate a person (usually atrusted family member or friend) to make healthcare decisions if he/she becomes unable to do so.The designated person is known as the “healthcare agent.” The Health Care Proxy can give thehealth care agent the authority to make decisionsabout both mental and physical health care.
R
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
15
These decisions can include the provision of careas well as the withholding of consent to treat-ment. The agent’s authority to make health caredecisions begins when an attending physician hasdetermined that the individual lacks the capacityto make these decisions.
Declaration for Mental Health Treatment - A doc-ument or statement that includes patient prefer-ences regarding medication, hospitalization andelectroconvulsive therapy (ECT), for example.
Living Will - A document that specifies your lovedone’s wishes regarding health care treatment if heor she becomes incapacitated. Although aliving will is not restricted in terms of what typesof health care matters it should address, they fre-quently are used to set forth a person’swishes withrespect to end-of-life treatment. There is no spe-cific law that addresses living wills, but courtshave upheld them as valid documents that ex-press a person’s wishes and instructions if they arepresented in a “clear and convincing” manner.Often, a living will is a document that a healthcare agent will use to guide his or her decision-making under a Health Care Proxy.
Do not Resuscitate (DNR) Order - A legal docu-ment that provides a person’s advance instruc-tions relating to the withholding or withdrawal ofcardiopulmonary resuscitation (CPR)
See “ADVANCE DIRECTIVES” to findsample Advance Directive for Mental andPhysical Care forms (p. 37)
FAMILY CONTRACTIf your loved one will return home after a mental healthhospitalization, having a clear set of rules and expecta-tions can reduce stress and act as a guide for starting over.
Many families have found it best to create andagree upon a set of “House Rules.” These rules can formthe basis of a family contract, which makes clear whateach party pledges to do and includes specific conse-quences for breaking the contract.
The optimal place to draw up the family contractis in the hospital, where staff can take part in the negoti-ations. A family contract document is signed by all partiesand can become part of the treatment plan.
At home, family members can follow-up on howthe contract is working in periodic family meetings.
These meetings can also provide an opportunity to makenew agreements and/or adjustments to the contract asnecessary or desired.
Find a sample “FAMILY CONTRACT” in the “Tools you can use” section ( p. 36)
HOUSINGHousing is often viewed as the most essential element tohelp patients to start building a life for themselves and tofurther the process of recovery. Preferences for housingand services should have been specified as part of yourloved one’s Discharge Plan.
The first housing placement can often be in LevelII supportive housing. This is transitional, service-en-riched housing. In Level II supportive housing, residentsoften live with a roommate and receive both rehabilita-tive and case management services. Housing costs are de-ducted from the individual’s benefits check. The goal ofsupportive housing is to help individuals transition tomore independent “supported” housing once the neces-sary independent living skills are gained. In supportedhousing, the tenant signs a lease or sub-lease, and is li-able for rent amounting to no more than one-third oftheir income. Services may be used as needed.
Because of lack of availability of immediate hous-ing, patients often return to their family’s home while fil-ing housing applications, which can take several monthsor even years, depending on clinical needs and prefer-ences. It benefits the consumer and/or family memberto educate themselves about the steps in the housing ap-plication and referral process, stay in close contact withhis/her case managers or housing coordinators, (whooften have large caseloads), and assist wherever possible.Remember—the required application, psychosocial andmedical forms expire after six months, so be sure to keepall three up-to-date.
In New York City, the supportive housing applica-tion and referral process is as follows:
Work with the case manager to complete and sub-mit the required Supportive Housing HRA 2010E appli-cation, which must be filed and submitted electronicallyto the Department of Human Resources Administration(HRA) by a staff person.
The HRA 2010E requires that all applicants submitthese three documents:
1. A current psychiatric evaluation from a psychia-trist or Psychiatric Nurse Practitioner (Completedwithin the last 6 months)
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
16
2. A psychosocial assessment, which is usually com-pleted by the case manager or a social worker(completed within the last 6 months)
3. Current TB test results (administered within thelast 12 months).
If HRA approves the application—and the eligi-bility determination process usually takes between oneand three business days—the case manager starts mak-ing referrals to specific housing programs in New YorkCity. Family members and consumers also have the rightto conduct placement providing they coordinate closelywith the mental health professionals.
Decide whether or not to utilize the Single Point ofAccess (SPOA) Housing Program administered by theCenter for Urban Community Services (CUCS) for theNew York State Office of Mental Health. Since it guar-antees three housing referrals in New York City, it is rec-ommended for the City. If you elect to use their services,SPOA staff can access a centralized database containingdetailed information on all mental health housing pro-grams in New York City and provide referrals to clinicallyappropriate housing programs based on the needs andpreferences of the applicant. Applicants are guaranteedthree face-to-face interview at any housing program inNew York City that they are referred to by SPOA.
**HINT - Family members can help by trackingall supporting documents, making sure they are receivedby the case manager, who will submit them electroni-cally to the Human Resources Administration with thefinal application.
TYPES OF HOUSING
FOR NEW YORK STATE AND IN SOMEINSTANCES CITY
State-Operated Community Residences(SOCR’s). These transitional residences are typi-cally located on the grounds of State PsychiatricCenters.
Private Proprietary Homes for Adults (also knownas Adult Homes) These residences are licensedby the New York State Department of Health.
Family Type Homes for Adults are private homesin the New York State communities where one ormore persons living with mental illness may payfor room and board. The level of supervisionvaries. Also, these residences may be licensed bythe local department of social services or may beunlicensed.
Section 8 rental voucher program Federal Housing& Urban Development (HUD) offers affordablehousing choices for low-income households byallowing families to choose privately ownedrental housing. This privately owned rental hous-ing can be accessed through the HUD programproviding Section 8 rental vouchers for low-in-come individuals on a limited basis through thelocal housing authority or certain non-profit or-ganizations. Call your local Public Housing Au-thority and/or local Department of MentalHealth to check out the availability of Section 8vouchers in your locality. Unfortunately, HUDopens their lists periodically and with unpre-dictability, it is sometimes a difficult system to navigate.
See HUD Section 8 Housing Program on p.45 for contact information.
Supported housing and Supported Single RoomOccupancy (SROs) are the only permanent housingmodels funded or licensed by the state. These housingprograms are targeted to individuals living with mentalillnesses who are capable of living more independently.A rent subsidy and mental health support services areprovided through nonprofit housing agencies. Supportedhousing may be apartments scattered throughout thecommunity or may be a single site residence. SupportedSROs are single-site buildings.
APPLICATIONS OUTSIDE OF NYCApplication procedures vary by county. In most up-
state counties, the application for state licensed and sup-portive housing options must be made by referral throughthe local Single Point of Access or SPOA. (As mentioned,In New York City, use of the SPOA Housing Program isoptional). Check with your local Department of MentalHealth to find out who is the administrator of the SPOAprogram in your community, and find out how to obtaina supportive housing application.
See “HOUSING” for a detailed descriptionsof licensed and supported housing optionsand listings of mental health housing pro-grams with their related vacancy and wait listinformation.
R
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
17
REHABILITATION
UNTIL RECENTLY, a diagnosis of mental illnessmeant the end of one’s hopes and prospects.There was little vision that people with mental ill-
nesses could return to school, work or otherwise lead pro-ductive lives. Today, the long-term focus of mental illnessis recovery. Many leaders in psychiatric rehabilitationrightly assert that recovery from mental illness is possibleand claim that much of the chronic nature of mental ill-ness is due to failures of services and not necessarily duethe nature of the illness itself.
An ideal rehabilitation program builds in assistanceat each step of recovery. It also assumes the family willbe part of a team that will help rebuild a loved one’s skillsand confidence, and provides the family with educationand support as well.
Below is a list of what an innovative rehabilitationprogram might include.
1. Immediate “first break” education in the hospitalabout the illness and the importance of stayingon medications.
2. Immediate inclusion of family by the treatmentteam.
3. Continued close collaboration between the con-sumer, treatment professionals and family mem-ber to monitor illness and watch for early signs ofrelapse.
4. Family Education program such as the NAMIFamily-to-Family program for family members,referral to a NAMI support Group and supportivecounseling for family members if necessary.
5. Extensive peer group education about mental ill-ness
6. Peer support group—NAMI Connection pro-gram, Peer Bridger Program, and in NY,Peer2Peer .p 49
7. Supportive services while consumer is recoveringand upon return to work or school.
8. Introduction to peer movement and opportuni-ties to join in advocacy activities.
LIVING WITH A LOVED ONE RIGHT OUT OF THE HOSPITALComing out of the hospital, people need time to recu-perate. Not only do returning loved ones have to copewith the circumstances of a mental disorder and adjust-ing to strong psychiatric medication, but they can alsoneed time to recover from the sheer trauma of commit-ment and hospitalization and the sedation caused dur-ing the stabilization process. They may, temporarilyrequire many hours of sleep.
The following family guidelines (adapted from theFamily Institute for Education, Practice and Research,University of Rochester Medical Center and NYS Officeof Mental Health) are designed to aid the recoveryprocess. They are designed with the biology of mentalillness in mind. Use them as a guide to slow down sensoryinput for a person who may be coping with a psychoticillness and to help establish basic ground rules for livingwith and recovering from a mental illness.
1. GO SLOW. Recovery takes time. Rest is impor-tant. Things will get better in their own time.
2. KEEP IT COOL. Enthusiasm is normal, butkeep it toned down. Disagreement is normal, butkeep this toned down too. Avoid over-stimulatingyour loved one during this difficult time.
3. KEEP IT WARM. Family bonds are meaningfuland important. Create an environment that iscaring, supportive and loving.
4. GIVE EACH OTHER SPACE. Time out is im-portant for everyone. Allow your loved one towithdraw when they need to, and learn to recog-nize the behaviors that signal this need.
5. SET LIMITS. Everyone needs to knowwhat the rules are. A few good rules keepthings clear. Establish house rules and con-sider a Family Contract . p. 36
6. IGNORE WHAT YOU CAN’T CHANGE. Letsome things slide but don’t ignore threatening, vi-olent or psychotic behavior.
7. KEEP IT SIMPLE. Say what you have to sayclearly, calmly and positively.
8. FOLLOW THE TREATMENT PLAN.9. CARRY ON BUSINESS AS USUAL. Reestab-
lish family routines as quickly as possible.10.TAKE CARE OF YOURSELF. It is difficult to
care for someone else if you are not taking goodcare of yourself.
GETTING WELL, STAYING WELL

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
18
11.HELP YOUR LOVED ONE AVOID STREETDRUGS & ALCOHOL. They make symptomsworse, can cause relapse, prevent recovery and in-terfere with prescribed medications. If your rela-tive uses alcohol or street drugs, encourage opendialogue about it with them and the treatmentteam in order to best optimize their recovery.Avoid caffeine too, as it can interfere with sleep.
12.PICK UP ON EARLY WARNING SIGNS. De-velop a list of early warning signs that may indi-cate your relative is relapsing. Discuss anychanges with your family member and theirprovider in order to head off a relapse.
13.LOWER EXPECTATIONS, TEMPORARILY.After an acute psychotic episode, an extended pe-riod of recovery is usually necessary. Comparethis month to last month instead of last year ornext year.
TIP - Don’t forget your Family Contract! (p 36)
Relapses can and must be avoided. One of the mostimportant contributions a family can make is to be vigi-lant for early warning signs and report them to the doc-tor immediately. Injurious multiple relapses areunnecessary and must be avoided.
DON’T FORGET PHYSICAL HEALTHIndividuals with a serious mental illness are two to threetimes more likely to have the risk factors for cardiovascu-lar disease than the general population, and are increas-ingly being recognized as a high-risk population fordiabetes. Factors include obesity, smoking, high bloodpressure and high cholesterol, can be effectively treated
through good medical care, beginning with properscreening and monitoring. If a medication causes dra-matic weight gain or blood pressure rise, an alternativemedication should be considered before the conditionadvances. Observing good nutrition and getting regularexercise are essential for general health and to combatthe effects of pharmaceuticals.
EARLY WARNING SIGNS OF RELAPSE� Trouble Sleeping� Feelings of tension or stress� Anger, irritability or short-temperedness� Difficulty concentrating� Lack of energy� Restlessness� Loss of interest in previously enjoyed activities� Fears people are talking about them� Depression or sadness� Withdrawn� Discomfort around people� Confusion or fear
STICKING WITH MEDICATIONS1) Keep a list of all medications, including over
the counter medication and herbal supple-ments. Show this list to all doctors and yourpharmacist.
2) Use one pharmacy, so they can detect drug in-teractions and call the doctor if any are de-tected.
3) Help your loved one follow the doctor’s instruc-tions for taking medications. However, advo-cate with the doctor to fit the medicationschedule to your loved one’s schedule.
4) Learn in advance how to manage a misseddose. Also, make sure the doctor explainsunder what circumstances he should stop tak-ing a certain medication.
5) Help your loved one avoid alcohol and otherstreet drugs. Changes in nicotine and caffeineconsumption should be reported to all doctorssince these changes can affect the way med-ications work.
6) Keep all appointments. Don’t hesitate to askquestions (make a list ahead of time). Tell thedoctor about any health problems or side ef-fects or if your loved one is pregnant, planningto get pregnant or nursing.
7) Make sure the psychiatrist knows what themedical doctor is doing (whether prescribing amedication or recommending an operation ormedical procedure) and vice versa.
8) Safely store medications in a cool, dry placeaway from children and pets.
9) Link your loved one’s medication schedule todaily routines, like eating breakfast or brushingteeth.
10)Encourage patience. Remember, many side ef-fects diminish in a few weeks. It may take afew weeks before he begins to feel better, too.
11)Help monitor any metabolic changes. Makesure the medical doctor keeps track of hisweight and blood pressure and periodicallytests for cholesterol problems and diabetes.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
19
See “WELLNESS SELF MANAGE-MENT” to find information on a tool kitcreated by the New York State Office ofMental Health to help consumers to im-prove and maintain their health p 48.
EDUCATION AND SUPPORT PROGRAMSSince the founding of the National Alliance for MentalIllness (NAMI) in 1979, families living with serious andpersistent mental illness have been looking after eachother and providing a range of support groups, coursesand educational events.
Recovery-centered rehabilitation programs andpeer support services can reduce the number of psychi-atric hospitalizations and relapses, so consumers and fam-ilies need to use and, if necessary, create thesecommunity-based resources...
Find contact information for all programslisted below under “EDUCATION” (p. 41)OR “SUPPORT” (pg. 47)
PROGRAMS FOR FAMILY MEMBERSAs soon as possible get a crash course in dealing withmental illness during and out of the hospital. Here’s astarter:
NAMI Family-to-Family (F2F) is the most compre-hensive family education course about mental ill-ness. This free 12-week education course istaught by family members of those suffering fromsevere mental illness. F2F provides practical in-formation on the biology of mental illness, med-ications and research, crisis management,communications skills, problem solving, self-care,advocacy and recovery. Based on the traumamodel, participants work through the stages ofgrief (shock, anger, grief to, acceptance). F2Fparticipant report greater understanding of men-tal illness, which leads to better coping skills, lessworrying and feeling newly empowered to advo-cate for better treatment and services for theirloved ones. (P. 59)
NAMI Support Groups - Contact your local NAMIaffiliate to learn which groups are offered or callNAMI-New York State to identify your local affili-ate. (p. 47) Referrals to the mobile crisis teamsare made by calling 1-800-543-3638 (LIFENET)
JOINT FAMILY AND CONSUMER PROGRAMSBehavioral Therapy (BT) - These privately or insur-
ance paid for sessions between a clinician and aconsumer and/or his or her family provide educa-tion and information, which can last a few ses-sions or a couple of years. BT typicallyemphasizes illness education and symptom man-agement, practical problem solving, relapse pre-vention, family support and assistance to navigatethe mental health system.
Consumer-Centered Family Consultation and re-ferral linkage - Family Consultation is an out-reach program in which a family consultant froman agency serving the patient visits the familyafter discharge from the hospital. During sessions(one to three, typically), concerns are discussedfollowed by an exploration of potential solutionsand a plan for addressing them. Family Consulta-tion is also a gateway service for the full Spectrumof Family Services offered by the Family Institutefor Education, Practice & Research. (p. 41)
Multi-family Psychoeduction (“MultifamilyGroups” or MFG) - These treatment programsbring together a group of six families, includingthe patient, for engagement, education and prob-lem solving. Twice a month (for nine months totwo years), program participants create a support-ive community and practice a specific method ofproblem solving to help their loved ones obtainstability and prepare to re-enter the community atlarge. It has Evidence-based status from NIMH’sPORT study as proving to reduce relapse rates byhalf in the first year. Family Institute for Educa-tion, Practice & Research (p. 41)
R
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
20
FOR CONSUMERS
NAMI’s Peer-to-Peer, 518-462-2000 or 800-950-3328 (P2P) For people with. mental illness whowant to establish. and maintain their wellnessand recovery. The program provides a binder ofmaterials, including an advance directive; a “re-lapse prevention plan”; and mindfulness exercisesto help focus and calm thinking; and survivalskills for working with providers and the generalpublic. Limited to New York State. p. 39.
NAMI Connection is a weekly recovery supportgroup for people living with mental illness tolearn from each others’ experiences, share copingstrategies, and offer encouragement and under-standing. If you Google NAMI Connection itwill bring up a map showing where in almost fiftystates the group is available.
Peer Bridger project, sponsored by the New YorkAssociation of Psychiatric Rehabilitation Services(www.nyaprs.org) helps individuals being dis-charged from New York State Psychiatric Centersin six counties, ease transition into communitylife. (p. 39)
The Wellness Recovery Action Plan (WRAP) is astructured, self-monitoring system to identify un-comfortable and distressing signs and symptomsand, through planned responses, to reduce, mod-ify or eliminate them. WRAP includes plans forothers when symptoms prevent good decision-making, self-care and self-safety. WRAP Plans areindividual. A daily self-monitoring journal helpsorganize behavior and actions to manage mentalillness. (p. 48)
Founder Mary Ellen Copeland has provided forNew Yorkers the contents of the plan and a 45-minute training session on this nationally ac-claimed self-help tool if they visitwww.nycnetworkofcare.org and search “WRAP.”(p. 43)
Wellness Self-Management - Developed by theNYS Office of Mental Health, the Wellness Self-Management program consists of 57 lessons thatare presented to groups of consumers in both in-patient and outpatient settings. The three majorsubjects covered are recovery, mental health well-ness and relapse prevention, and healthy living.(p. 48)
COGNITIVE REHABILITATION
A majority of people suffering a psychotic episode lose“Executive Functioning” skills such as recall, categoriz-ing and organizing information, solving problems andsolving problems. Such cognitive problems pose majorobstacles to employment.
Research shows that these problems can be re-duced through cognitive rehabilitation combined withvocational rehabilitation, which, in turn, improves self-es-teem and decreases depression.
Effective programs include using software for com-puterized remediation at one’s own pace or “errorlessteaching,” which breaks down complex tasks into smallcomponent steps. For example, Alice Medalia, Ph.D. Di-rector of Neuropsychology at Montefiore Medical Cen-ter, has developed a computer games for use with groupsof eight patients. Clients who have used this Edmark soft-ware have found it fun and have increased their atten-tion span and retention.
See “COGNITIVE REHABILITATION”(p. 44)
NUTRIENT APPROACH TO MENTAL ILLNESS:COMPLEMENTARY AND ALTERNATIVE MEDICINE(CAM) - AN EVOLVING OPTIONResearch starting in the 1970’s with Nobel prize winnersLinus Pauling and his colleagues , laid a scientific basisto show that that mental health problems including de-pression, bipolar disorder, schizophrenia, ADHD, learn-ing disorders and obsessive-compulsive disorders oftenhave a common cause: insufficient nutrients in the brain.They call this approach “orthomolecular” meaning “theright molecule” to bring about a state of health by bal-ancing the concentration of natural substances normallypresent in the human body: vitamins, minerals, aminoacids, trace elements and hormones.” They have intro-duced a protocol of megavitamin and mineral supple-ments in recommended dosages, which many havebenefitted from (www.orthomed.org).
EMPowerplus, a formulation from a Canadian EM-Powerplus, a formulation from a Canadian companycalled Truehope, was developed out of animal husbandryinitiatives. EMPowerplus is receiving attention from main-stream neuropsychologists and many users with a range ofbrain disorders. The company's website offers informationabout scientific and case studies (www.truehope.com).Truehope believes that the nutrients can correct deficien-cies that affect brain, organ function and nerve growth. Ex-
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
21
periments with rats which were fed the nutrients appear toshow brain regeneration and growth of the neuron den-drite endings to address cognitive deficits. Regimens re-quire taking nutrients three to four times a day, optimallyunder a doctor’s supervision and with substantial supportfrom Truehope’s support team. This modality has not re-ceived mainstream acceptance for a number of reasons re-lating to lack of ability to patent formulations and lack ofwidespread and low cost availability.
(Inclusion of this information in no way constitutesany recommendation or endorsement for not takingmedications; this information is offered for considerationas a possible aid to wellness for interested, well-informed,motivated and disciplined individuals)
EMPLOYMENTThe two magic ingredients for building a life are housingand a job.
Your loved one is entitled to assistance in address-ing his or her employment needs. Section 29.15 (g) ofthe NYS Mental Hygiene Law provides that written dis-charge plans “shall include a statement of patient’sneed...for aftercare services and assistance in finding em-ployment...” (Refer When Families Join the MentalHealth Care Team Everyone Benefits!)
The main approaches for helping seriously men-tally ill persons obtain employment are Pre-vocationalTraining (PT) and Supported Employment (SE). SE in-cludes rapid job search, integrated vocational and clini-cal services and employment assistance. The goal is torapidly acquire competitive jobs in integrated commu-nity settings, working along-side non-disabled workers,and to provide ongoing supports to facilitate success onthe job. This contrasts with traditional vocational servicesthat use extensive pre-employment training.
Pre-Vocational TrainingThe key principle of Pre-vocational Training is that a pe-riod of preparation is necessary before an individual en-ters competitive or open employment. One way yourloved one can obtain this type of preparation is by join-ing a “Clubhouse” that offers a pre-vocational trainingapproach. This approach also sets the standard for an in-ternational network.
A “Clubhouse” is a restorative community organ-ized by and for persons with mental illness. It serves as acollegial place for consumers to pursue a range of activ-ities, including seeking and obtaining housing, employ-ment, and friendships. The first Clubhouse, FountainHouse in New York City, was started in 1948 by con-
sumers who coined the word “clubhouse” to communi-cate a place of membership and belonging. Since then,Fountain House has served as the model for other club-houses internationally. (see p. 38)
Clubhouse participants are called “members” be-cause the focus is on the person’s strengths not their ill-ness. Employment opportunities are provided as a rightof membership into the Clubhouse. Members transitionto paid employment ,while staff members assist in jobplacement, job retention and on the job training. Mean-ingful work in a Clubhouse may lead to transitional, sup-ported or independent employment at local businesses
Transitional Employment (TE) is a well-respectedstrategy for facilitating the vocational adjustment of menand women with serious mental illness in the commu-nity. The Clubhouse manages several job sites within thecommunity that allows members a job coach for the du-ration of the six to eight months. While members areworking at this job site, they are paid the prevailing wage.
Clubhouses usually train workers at the work site,and provide back-up for the employee when necessary. ATE position helps increase self-esteem, develops inter-personal and vocational skills, and develops a work his-tory for future job applications.
Supported Employment (SE) is grounded in theprinciple that placement in competitive employmentshould occur as quickly as possible, followed by on-the-job support and training. In SE, a job is developed witha particular member in mind. After an adjustment pe-riod, the member remains on the job, receiving supportwhen and as needed.
EMPLOYMENT: AGENCY SERVICES
Ticket to WorkAdministered by the Federal Social Security Administra-tion, the “Ticket to Work” is actually a cash voucher aperson can take to any Employment Network or StateVocational Rehabilitation agency to obtain assistance injob training, preparing materials to use when seeking ajob, locating employers, obtaining information aboutwork incentives, and other assistance neededin order toreach employment goals. The program is available forpeople between the ages of 18 and 65 who receive So-cial Security Disability Insurance (SSDI) or Supple-mental Security Income (SSI) benefits because they aredisabled or blind. p. 42
There are a number of benefits to using the “Ticketto Work” program. For example, consumers can “testout” a job without losing their benefits and maintain ac-

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
22
cess to other Social Security Administration programsand work incentives as they transition into work. Hereare the details:
1. If you have to stop working, you can easily regainyour benefits (known as “expedited reinstatementof benefits”). Also, for an additional 36 monthsafter completing the trial work period, benefitscan be reinstated again if a consumer’s earningsfall below the “substantial” level and he or shecontinues to have a disabling impairment.
2. If you go back to work, you will NOT automati-cally lose your disability benefits. The Ticket toWork and special rules called “work incentives”allow you to keep your cash benefits andMedicare or Medicaid during a trial period whileyou test your ability to work. For the Social Secu-rity Disability Insurance (SSDI) program, there isa trial work period during which you can receivefull benefits regardless of how much you earn, aslong as you report your work activity and con-tinue to have a disabling impairment.
3. Consumers will not receive a medical continuingdisability review (CDR) while using the “Ticket.”p. 42
NYS Office of Vocational and Educational Servicesfor Individuals with Disabilities (VESID)Through the VESID program, Vocational Rehabilitationagencies furnish a wide variety of services, through specialeducation and vocational rehabilitation programs, tohelp people with disabilities return to work, enter a newline of work, or to enter the workforce for the first time.
VESID coordinates services relating to vocationalassessment, vocational counseling, training and place-ment, and job follow-up/ It works to ensure that both theindividual and the employer are satisfied with the place-ment and will intervene if problems occur once an indi-vidual is placed in a job.
VESID participants have an Individual Plan forEmployment (IPE), which details specific occupationalgoals and steps needed to achieve them. The IPE couldinclude such things as vocational training at a tradeschool, a certificate program at a Continuing EducationDepartment of a college, supportive employment, or atwo or four-year degree. Ask VESID about the availabil-ity of cognitive rehabilitation if you think this service willimprove your loved one’s chance of employment. p. 42
In New York City, Workforce 1 centers are locatedin every NYC borough. These centers have a DisabilityNavigator on staff. All NYC residents are eligible for this
program. In addition to placement assistance, they pro-vide some limited training vouchers, access to a com-puter, printer, phone, and fax, and GED classes.(p. 51)
See “EMPLOYMENT” (pg. 41) for all em-ployment and agency resources.
NOTE: The future looks rosier for vocational supportdue to a generous grant from Medicaid to the New YorkState Office of Mental Health. Coalitions and potential formultiple year funding could result in raising the currentlylow employment rate for those with mental illness.
Hint - CUNY and SUNY two- and four-yearcollege has an office for students with dis-abilities that can be very helpful.
EMPOWERMENT AND THE PEER MOVEMENTThe thriving and articulate consumer movement hasspearheaded recovery as a right. This social movementfor self-determination asserts that the consumer has pri-mary control over decisions about his/her own care andadvocates for “peer support specialists” to manage a rangeof services: Peer Drop in Centers, Peer EmploymentSupports and Peer Crisis Diversion, Bridger, AdvocacyServices and now Peer health services. That those whoexperience illness are best equipped to provide these serv-ices is expressed in their slogan, “Nothing About UsWithout Us.” They see peer services as an approachwhose time has come, whether it be to promote recovery,empowerment and employment or to provide timely in-terventions to help people avoid crisis and improve theirhealth and wellness.
Ten thousand consumers have clearly stated how torespect their choices in a 2006 White Paper, entitled, In-fusing Recovery-Based Principles into Mental HealthService. At the heart are ten rules:
(1) There must be informed choice; (2) Treatment must be recovery-focused;(3) Treatment must be person-centered; (4) First, do no harm; (5) There must be free access to records; (6) The system must be based on trust; (7) Treatment must have a focus on cultural values; (8) Treatment must be knowledge-based;(9) Treatment must be based on a partnership be-
tween consumer and provider; and (10)There must be access to services regardless of
ability to pay (www.thewhitepaper.org)
R

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
23
RECOVERY
Official definitions include: “Mental health recov-ery is a journey of healing and transformation enabling aperson with a mental health problem to live a meaning-ful life in a community of their choice while striving toachieve their full potential.”
This is much broader than the definition histori-cally used in the mental health treatment system: com-pensating for, or accommodating, the impairment of apsychiatric disability.
Viewing recovery as remission or as a return to theway your loved one was before could damage recoveryefforts. Being “in recovery” however, opens up the possi-bility to operate under a new set of parameters withgrowth potential as defined by the individual.
Recovery is not something you can do to or for yourloved one. Your loved one must take responsibility for hisor her own recovery. The family’s role is to share the pow-erful consumer sources in this Handbook to empowertheir loved one to design their own recovery goals andplan. (pgs 38-39).

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
24
This page intentionally left blank.

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
25
Tools You Can Use
HOSPITAL CHECKLISTPATIENT INFORMATION:
PATIENT'S HOSPITAL ADDRESS: ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
PATIENT'S PHONE NUMBERS:Hospital Ward Public Phones: ______________________________________________________________________
Front Desk numbers: ______________________________________________________________________
Home: ______________________________________________________________________
Cell: ______________________________________________________________________
VISITING HOURS & OTHER PERTINENT INFORMATION:______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
CURRENT AND PAST MEDICAL DIAGNOSESCurrent diagnosis (if any) ______________________________________________________________________
Medication(s), if any ______________________________________________________________________
Primary care physician ______________________________________________________________________
Psychiatrist? ______________________________________________________________________
Dentist ______________________________________________________________________
PHYSICAL ISSUES______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
HISTORY OF MENTAL ILLNESS/BRAIN DISORDERS IN THE FAMILY______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
PROFESSIONAL CONTACT INFORMATION:______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
26
HOSPITAL CHECKLIST (continued)Attending Psychiatrists (in charge of assigning medications)
#1 Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
#2 Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
Social worker (recommends resources: social services, housing, employment and does counseling)
Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
Nurse Practitioner (advises on diagnosis and treatment)
Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
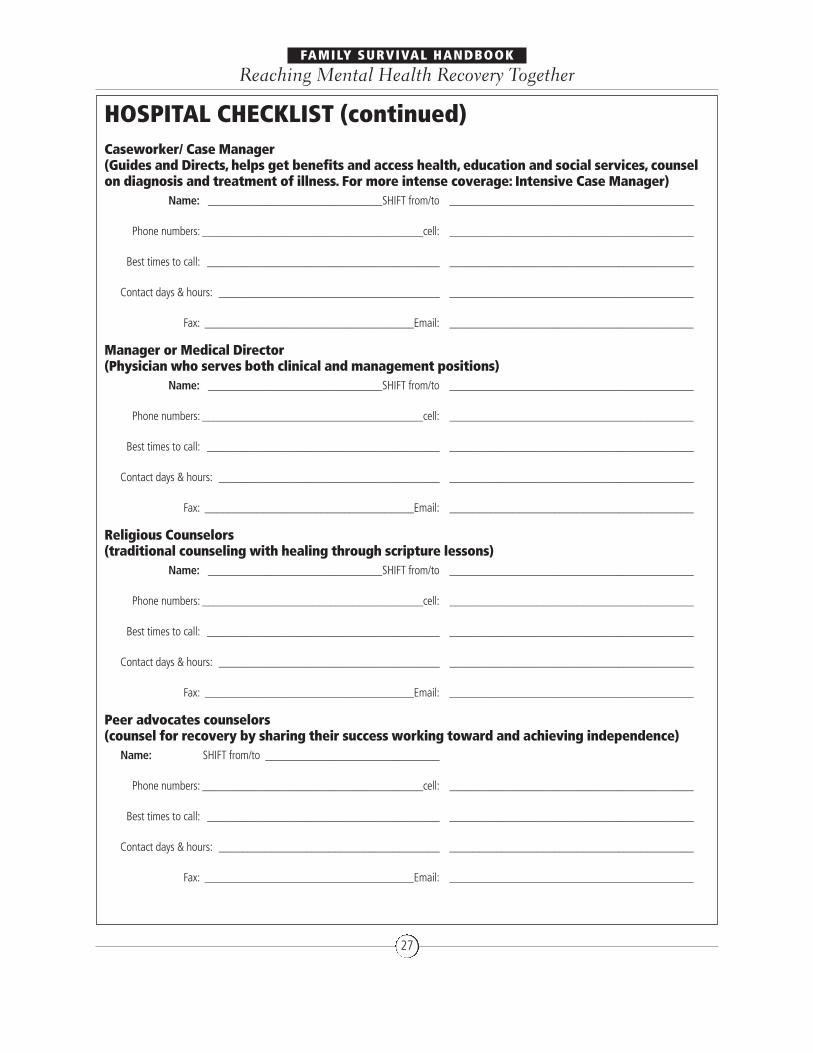
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
27
HOSPITAL CHECKLIST (continued)Caseworker/ Case Manager (Guides and Directs, helps get benefits and access health, education and social services, counselon diagnosis and treatment of illness. For more intense coverage: Intensive Case Manager)
Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
Manager or Medical Director (Physician who serves both clinical and management positions)
Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
Religious Counselors (traditional counseling with healing through scripture lessons)
Name: ______________________________SHIFT from/to __________________________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________
Peer advocates counselors (counsel for recovery by sharing their success working toward and achieving independence)
Name: SHIFT from/to ______________________________
Phone numbers: ______________________________________cell: __________________________________________
Best times to call: ________________________________________ __________________________________________
Contact days & hours: ______________________________________ __________________________________________
Fax: ____________________________________Email: __________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
28
HOSPITAL CHECKLIST (continued)WORKING DIAGNOSIS
A) upon admission ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
B) upon discharge ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Basis of Working Diagnosis ______________________________________________________________________
(How was diagnosis arrived at?): ______________________________________________________________________
______________________________________________________________________
4. TREATMENT GOALS:______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
5. INITIAL MEDICATIONS
1) Name ________________________Dosage/when to take __________________________________________
Benefits ________________________________________ __________________________________________
Side Effects ________________________________________ __________________________________________
________________________________________ __________________________________________
Contact doctor (name(s)) if any:________________________________ __________________________________________
2) Name ________________________Dosage/when to take __________________________________________
Benefits ________________________________________ __________________________________________
Side Effects ________________________________________ __________________________________________
________________________________________ __________________________________________
Contact doctor (name(s)) if any:________________________________ __________________________________________
3) Name ________________________Dosage/when to take __________________________________________
Benefits ________________________________________ __________________________________________
Side Effects ________________________________________ __________________________________________
________________________________________ __________________________________________
Contact doctor (name(s)) if any:________________________________ __________________________________________
4) Name ________________________Dosage/when to take __________________________________________
Benefits ________________________________________ __________________________________________
Side Effects ________________________________________ __________________________________________
________________________________________ __________________________________________
Contact doctor (name(s)) if any:________________________________ __________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
29
HOSPITAL CHECKLIST (continued)6. DISCHARGE MEDICATIONS
SAME AS IN-PATIENT Yes ______________________________________________________________________
No ______________________________________________________________________
(If outpatient medications differ from inpatient medications, please note the changes below.)
______________________________________________________________________
______________________________________________________________________
` ______________________________________________________________________
Contact doctor (name) if any: ______________________________________________________________________
IN DEPTH PERSONAL MEDICAL HISTORY• This can be crucial to the doctors and social workers.
• Describe as much as you can, from earliest symptoms to present.
• Point out any family history of mental illness, use of medications, hospitalizations, and substance abuse.
• Submit to the hospital your description and keep an updated copy with this checklist.
• NOTE: Each new doctor, social worker and case manager should get a copy of this medical history
(their files may only store electronic data, so typing it for ease of reading and copying would be optimum
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
` ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
30
IN DEPTH PERSONAL MEDICAL HISTORY (continued)______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
31
7. GOVERNMENT INSURANCE BENEFITSA social worker or representative from the hospital's financial office should help you obtain appropriate financial assistance.
Insurance benefits representative(s) 1. ____________________________________________________________2. ______________________________________________________________________
3. ______________________________________________________________________
Patient qualifies for: ______________________________________________________________________
Benefit Application date ______________________________________________________________________
Date effective ______________________________________________________________________
Costs covered/other benefits: ______________________________________________________________________
Patient qualifies for: ______________________________________________________________________
Benefit Application date ______________________________________________________________________
Date effective ______________________________________________________________________
Costs covered/other benefits: ______________________________________________________________________
Patient qualifies for: ______________________________________________________________________
Benefit Application date ______________________________________________________________________
Date effective ______________________________________________________________________
Costs covered/other benefits: ______________________________________________________________________
SOCIAL SECURITY contact person(s):Name ________________________Phone number __________________________________________
Fax: ________________________________Email: __________________________________________
MEDICAID contact person(s):Name ________________________Phone number __________________________________________
Fax: ________________________________Email: __________________________________________
MEDICARE contact person(s):Name ________________________Phone number __________________________________________
Fax: ________________________________Email: __________________________________________
Other Pertinent Information:______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
DESCRIPTION OF PATIENT'S LEGAL STATUS______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
32
8. DISCHARGE PLANNING(In the case of two diagnoses, e.g. substance abuse and mental illness, services must address both.)
A) CASE MANAGEMENT SERVICES
Assertive Community Treatment
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Supportive Case Management
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Intensive Case Management
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
B) MENTAL HEALTH TREATMENT
Outpatient treatment (individual or group)
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Day Treatment Program
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Psychiatrist/social/worker/therapist
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
33
C) OTHER COMMUNITY SUPPORTS
Self-Help Groups, AA, NA, MHA, NAMI, NYAPRS, Double Trouble (circle)
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Psychosocial Club
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Other program
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Support Group
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
IPRT (Individual Psychiatric Rehabilitative Treatment)
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Vocational Program
Provider __________________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
D) HOUSING: WHERE TO LIVE AFTER DISCHARGE
Community based Housing Provider ____________________________If yes, start date ________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
34
E) FOR DUAL DIAGNOSIS
MICA (Mentally Ill Chemically Addicted) Program
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________
Support Group
Treatment Provider __________________________Start date ____________________________________
Contact information: Name__________________________________________________________________
Phone ____________________________Cell Phone __________________________________________
Fax ________________________________E Mail __________________________________________

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
35
MANAGEMENT LOG SHEET(Use these log sheets to record all meetings, phone conversations, emails, letters, side effects in the hospital or at home.)
DATE ______________________________________________________________________
WHO ATTENDING ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
WHAT WAS DECIDED ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
SYMPTOMS ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
ACTION STEPS ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Who Does What By When ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
SIDE-EFFECTS ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
CHANGES: Physical ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
CHANGES: Behavioral ______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Tools You Can Use #2

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
36
FAMILY CONTRACT SAMPLE(adapt parenthetical parts for your individual situation) family member) agree to the following terms:
1. I will (make my home available during the transition while family member awaits supported housingplacement)
2. I will (not enter ________________________________’s room without knocking)
3. I will (provide ________________________________ with meals and spending money in the amount of $_______per week)
4. I will (help ________________________________with transportation to appointments and services, and, when I am able to do so, other appropriate destinations)
5. Other ________________________________ I, (consumer) agree to the following terms:
1. I (agree to take my medications as prescribed from a credentialed psychiatrist, to keep the twice-a-month appointments with my case manager and to cooperate with treatment and planning goals).
2. I (understand that getting the medication right is trial and error and that it’s my responsibility to regularly report to the doctor to “get it right.”)
3. I (promise to report early warning signs like sleeplessness, anxiety and hearing voices).
4. I (agree not to harm myself or others, and I will not threaten to harm others).
5. I agree to do the following task: (list chores and when they are to be accomplished).
6. I (will not expect monetary help from my family, other than the $_______ weekly spending money.
7. I (will be civil in my family’s home and use stress and emotional regulation techniques).
8. I (agree to commit to a plan toward getting full-time work: set up volunteer hours on a flexible basiswhile stabilizing and attend a skills-building program).
9. Other ________________________________
Family member
____________________________________________ __________________________Signature Date
Consumer
____________________________________________ __________________________Signature Date
Provider
____________________________________________ __________________________Signature Date
Tools You Can Use #3

ADVANCE DIRECTIVES
New York Association ofPsychiatric Rehabilitation Services518-436-0008 x19
www.nyaprs.org
Visit this website to download Planningfor Your Mental and Physical Health Careand Treatment, which is a comprehensiveset of Advance Directives forms and in-structions, as well as a carrying card:http://www.nyaprs.org/Pages/View_Content_A.cfm?ContentID=39
AOT
New York State Office of Mental Healthhttp://www.omh.state.ny.us/omhweb/kendra_web/ksummary.htm
BENEFITS ELIGIBILITY
Advocacy Counseling andEntitlement Services (ACES)212-614-5552
Call to find out which benefits your lovedone qualifies for.
Centers for Medicare and Medicaid Services800-342-3009 (Medicaid) 877 472-8411 (NYC only)
http://www.cms.hhs.gov/medicaideligibility/
800-772-1213 (Medicare Basic Information Line for sign-up/eligibility)
http://www.medicare.gov/Help/MET.asp
NYC Human ResourceAdministration, Department of Social Services718-472-8411, (TTY) 718-262-3566 or toll free 1-800-342-3009
http://www.nyc.gov/html/hra/html/home/home.shtml
New York State Office of Temporary and Disability Services800-342-3009
https://www.mybenefits.ny.gov/selfservice/
The “My Benefits” home page is a quickand easy way for people in New YorkState to find answers to questions aboutNew York State’s programs and services,including eligibility for benefits.
New York Association of Psychiatric RehabilitationServices (NYAPRS)Social Security Disability Benefits
800-772-1213, (TTY) 800-325-0778
http://www.ssa.gov/dibplan/dqualify.htm
CHILDREN
American Academy of Child and Adolescent Psychiatry202-966-7300
www.aacap.org
The site offers news alerts, fact sheets,legislative action, publications, research,and a directory of mental health organiza-tions and doctor organized by regions.
Families Together in New York State518-432-0333 or 888-326-8644
www.ftnys.org
Families Together is a non-profit, family-run organization that strives to establish aunified voice for children and youth withemotional, behavioral, and social chal-lenges. Its mission is to ensure that everyfamily has access to needed information,support, and services. Website featurespublications, guides and reports.
Families USAwww.familiesusa.org
A comprehensive clearinghouse for children’s issues.
CRISIS
Mobile Crisis Teams.800-543-3638 (LIFENET)
Are a team of mental health professionals(nurses, social workers, psychiatrists, men-tal health technicians, addiction special-ists, peer counselors and sometimespolice). responding to persons in the com-munity, usually at home. Their 23 NewYork Citywide teams serve anyone experi-encing or at risk of, a psychological crisisand requiring mental health intervention.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
37
RESOURCES

38
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery TogetherCOGNITIVE REHABILITATION
NYS Office of Vocational and Educational Services forIndividuals with Disabilities(VESID)http://www.vesid.nysed.gov/
Offers access to a full range of servicesthat may be needed by persons with dis-abilities through their lives, including spe-cial education, cognitive rehabilitation,vocational rehabilitation and independentliving programs. Visit the website for con-tact information for the district office inyour county.
Lieber Recovery andRehabilitation ServicesColumbia University Medical Center Eastside
16 East 60th Street, Suite 400, New York,New York 10022
212-326-8441
Offers the NEAR method (Neuropsycho-logical Educational Approach to Rehabili-tation), which provides specificneurocognitive exercises to improve atten-tion, planning, memory, and other cogni-tive skills. Computer-based exercises andgroup exercises teach cognitive awarenessand cognitive skills and improve self-es-teem and intrinsic motivation. Private pay.
New York State Office of Mental Healthwww.omh.state.ny.us
From the website, search “Dealing withCognitive Dysfunction” to download ahandbook on the cognitive remediationauthored by Alice Medalia
COMPLAINTS (ALSO SEE“LEGAL SERVICES”)
NYS Commission on Quality of Care800-624-4143 (Voice/TTY/Spanish)
http://www.cqcapd.state.ny.us/
For problems concerning inpatient andoutpatient treatment
NYS Office of Mental Healthmain hotline1-800-597-8481in Spanish 1 800 210-6456
NYS Office of Mental HealthFamily Liaisons518-474-4888
Assists families in advocating for lovedone in hospital or clinic settings)
NYS Office of Recipient Affairs518-473-6579
Peer advocates assist consumers withproblems with treatment and/or gettingservices)
CONSUMER SUPPORT AND SELF HELP
Center for Independence of the Disabled, NY212-674-2300212-674-5619 TTY (Manhattan)
646-442-1520718-886-0427 TTY (Queens)
http://www.cidny.org
This not-for-profit is part of the Independ-ent Living Centers movement. Its goal isto ensure full integration, independenceand equal opportunity for all people withdisabilities by removing barriers to the so-cial, economic, cultural and civic life of thecommunity. CIDNY’s offices in Manhattanand Queens provide benefits counseling,direct services (e.g. housing assistance,
transition services for youth with disabili-ties, employment-related assistance,healthcare access, peer support groups),information and referrals, and recreationalactivities.
Depression and Bipolar Support Alliancewww.dbsalliance.org
Dedicated to educating about depressionand bipolar disorder, fostering self-help,eliminating discrimination and improvingaccess to treatment.
Community [email protected]
212 632-4611
This program, run by the Jewish Board ofFamily and Children’s Services, has trainedvolunteers contact ill members to breakany sense of isolation by offering themsimple get together such as a walk in thepark or a coffee at Starbucks progressingto more stimulating outings that take ad-vantage of the endless free opportunitiesof the City.
Fountain Housewww.fountainhouse.org
582-0340
A “Clubhouse” restorative community or-ganized by and for the mentally ill. Withsome staff, it’s basically consumer run. Itsmembers pursue a range of activities in abeautiful and warm clubhouse, as well asprovide opportunities to obtain housing, ajob and friendships. The first Clubhouse,Fountain House in New York City, wasstarted in 1948 by a group of consumers,sitting on the steps of New York’s 42ndStreet Public Library discussing what kindof place they would like to “hang out” in.Founding this first one, they coined theword “clubhouse” for their “members,”defining it as a place of membership andbelonging... Since then, Fountain House’model sets rigorous standards for a net-work of Clubhouses internationally.

39
Friendship Networkwww.friendshipnetwork.org
Serving the five boroughs of New YorkCity (Queens, Bronx, Manhattan, StatenIsland, Brooklyn); Long Island (Nassau andSuffolk County); Westchester County andNorthern New Jersey, the Friendship Net-work is a not-for-profit organization thatintroduces single men and women recov-ering from mental illness to one another.Sponsored by NAMI Queens-Nassau.
Mental Health EmpowermentProject800-643-7462 (for list of consumer self-help groups)
Mental Health Recovery802-254-2092
www.mentalhealthrecovery.com
www.copelandcenter.com
Mary Ellen Copeland has written severalbooks and developed a variety of pro-grams for helping people in the recoveryprocess, including Wellness Recovery Ac-tion Plan (WRAP), a program that teachesself-help monitoring skills for handlingparticularly the ups and downs of Bi-PolarDisorder. Websites offers helpful informa-tion, a free newsletter, and a list of publi-cations and workshops that can bepurchased.
NAMI’s Peer-to-Peer518-462-2000 or 800-950—3328(P2P)
For people with. mental illness who wantto establish. and maintain their wellnessand recovery. The program provides abinder of materials, including an advancedirective; a “relapse prevention plan”; andmindfulness exercises to help focus andcalm thinking; and survival skills for work-ing with providers and the general public.Limited to New York State. .
NAMI ConnectionGoogle NAMI Connection for a mapshowing where (in almost all fifty states )the groups are.
It is a weekly recovery support group forpeople living with mental illness to learnfrom each others’ experiences, share cop-ing strategies, and offer encouragementand understanding.
Mental Health Association of New York State518-434-0439
http://www.mhanys.org
This hundred-year organization providesprograms, resources, education and refer-rals. All other national chapters are knownas “Mental Health America”
National Mental HealthConsumers Clearinghousewww.mhselfhelp.org
News, publications, resources, trainingmaterials, technical assistance and a direc-tory of consumer-driven services.
New York City Voiceswww.nycvoices.org
A peer journal for mental health advocacy,New York City Voices is an excellent publi-cation written by consumers for con-sumers and the New York community.
New York Association forPsychiatric Rehabilitation(518) 436-0008, www.nyaprs.org
The premier consumer organization is astatewide coalition of people who useand/or provide recovery-oriented commu-nity based services. Dedicated to improv-ing services and social conditions forpeople with psychiatric it sponsors a com-prehensive listserv, provides training andlobbying and sponsors the Peer Bridgerproject (see below). Their listserv is one ofthe most comprehensive tracking of policyand legislative issues currently available(call above number to be placed on it).
New York State Office of Mental Health, Bureau of Recipient Affairs (518) 473-6579
Staffed by consumers, OCA offers advo-cacy trainings, technical assistance andpeer support, as well as quarterly "advi-sory committee meetings.
Peer Bridger Project518-436-0008
[email protected],http://www.nyaprs.org/Index.cfm
The NYAPRS Peer Bridger Project hashelped individuals being discharged fromNew York State Psychiatric Centers in sixcounties (Albany, Ulster, Broome, Queens,Suffolk and Westchester) to ease the tran-sition into community life and to signifi-cantly decrease their need forreadmission.
Recovery x-Changehttp://www.recoveryxchange.org/about.html
The Recovery x-Change is a wellnessmanagement training partnership of peerspecialists and providers partnering withproviders to create, design and customizerecovery focused trainings for an inte-grated approach necessary for recovery.
CRIMINAL JUSTICE
NAMI-NYS Criminal JusticeAdvocacy program260 Washington AvenueAlbany, NY 12210
518-462-2000 or 1-800-950-3228
http://naminys.org/criminaljustice.html
Helps families navigate their loved onethrough the criminal justice system andadvocate for jail diversion initiatives.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

40
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
New York State Office of Mental Health (OMH) Bureau of Forensic Services and Criminal Procedures518-474-7219
http://www.omh.state.ny.us/omhweb/forensic/BFS.htm
Responsible for services provided to personswith mental illness as mandated via Crimi-nal Procedure Law or Corrections Law.
Reentry Resource Center - New Yorkhttp://www.reentry.net/ny/
Reentry Net/NY is the first ever supportnetwork and information clearinghouseon prison and jail reentry, and the collat-eral consequences of criminal proceedingson individuals and families in New YorkState.
Urban Justice NYC646-602-5600
www.urbanjustice.org
- The Urban Justice Center serves NewYork City’s most vulnerable residentsthrough a combination of direct legalservice, systemic advocacy, community ed-ucation and political organizing.
CRISIS INTERVENTION
LIFENET Mobile CrisisIntervention team800 543-3638
CULTURAL ISSUES AND SUPPORT
NAMI Multicultural ActionCenter (MAC)Online resources include fact sheets, man-uals, and other informational materialsabout mental health issues specific to tra-ditionally underserved communities:African American, American Indian Alaska
Native, Asian American Pacific Islander,Latino and GLBT. Resources are availablein Spanish, Chinese, Italian, and Por-tuguese. Website: Go to www.NAMI.org.From the home page, choose the “FindSupport” drop down menu and select“Multicultural Action Center.”
New York State Office of MentalHealth’s Bureau of CulturalCompetence518-474-4144
Furthers multicultural interests and activi-ties
Office of Minority Health240-453-2882
www.health.statee.ny.us/nydoh/omhMis-sion is to improve the health of racial andethnic minorities through communication,and customized services and practical ap-proaches to problems and issues
MEDICATION (FINANCIAL) ASSISTANCE
PhRMA Patient AssistanceProgramswww.phrma.org
Find patient assistance programs forwhich you may qualify.
The Medicine Programwww.themedicineprogram.com
An organization established by volunteersto help obtain prescription medicationsfree of charge for those who cannot af-ford them.
Rx Assistwww.rxassist.org
This searchable database locates patient as-sistance programs by company, brand name,generic name and drug class. It includes eli-gibility and application instructions.
Together Rxhttp://www.togetherrxaccess.com/Tx/jsp/apply.jsp
A free prescription-savings card for eligi-ble residents of the United States andPuerto Rico who have no prescriptiondrug coverage.
EPIChttp://www.health.state.ny.us/health_care/epic/
EPIC is a New York State program thathelps seniors pay for their prescriptiondrugs. Most enrollees have Medicare PartD or other drug coverage, and use EPIC tolower their drug costs even more by help-ing them pay the deductibles and co-pay-ments required by their other drug plan.EPIC also helps members pay forMedicare Part D premiums.
Medicare Part D800-633-4227, TTY: 1-877-486-2048
http://www.medicare.gov/pdphome.asp
Medicare prescription drug coverage is in-surance that covers both brand-name andgeneric prescription drugs at participatingpharmacies in your area for anyone withMedicare, regardless of income and re-sources, health status, or current prescrip-tion expenses.
DUAL DIAGNOSIS
Office of Alcoholism andSubstance Abuse Services(OASAS)518-473-3460 or 212-399-8404
http://www.oasas.state.ny.us/
National Association for theDually Diagnosed1-800-331-5362
http://www.thenadd.org/
Provides educational services, training ma-terials, advocacy and some referrals. Thisnot-for-profit’s mission is to address the

41
mental health needs of persons with de-velopmental disabilities.
EATING DISORDERS
National Eating DisordersAssociation (NEDA)800-931-2237
http://www.nationaleatingdisorders.org/
Dedicated to providing education, re-sources and support to those affected byeating disorders.
American Anorexia/BulimiaAssociation212-575-6200
Support groups, information and referrals
EDUCATION
Family Institute for Education,Practice and Research (FIEPR)585-224-1324
http://www.nysfamilyinstitute.org/
Offers Consumer-Centered Family Consul-tation and referral linkage. With consumerconsent, their Family Consultation pro-vides one-to-three session meetings posthospital with a mental health provider todiscuss concerns, explore solutions and aplan for addressing them. It is also a gate-way service for FIEPR’s full Spectrum ofFamily Services. . Contact: Anne Smith,[email protected].
Mental Illness Education Project(MIEP)800-343-5540
www.miepvideos.org
Seeks to improve understanding of mentalillness through the production of video-tapes for people with psychiatric disorders,their families, mental health practitioners,administrators, educators and the generalpublic.
National Alliance on MentalIllness - New York State (NAMI-NYS)518-462-2000 or 800-950-3228
www.naminys.org
Offers comprehensive education and train-ing programs for patients and families in-cluding the 12-week Family-to-Familyprogram. Visit the website at http://naminys.org/educationandtraining.html, contact yourlocal NAMI chapter (you can find affiliatelistings on our website) or call NAMI-NYS tofind details about education course offer-ings near you. They sponsor an annual con-ference presenting speakers leaders in thefield of mental health, workshops and anopportunity to network statewide.
National Alliance on MentalIllness of New York City Metro(NAMI-NYC Metro)212-684-3264
http://www.naminycmetro.org/
One of the largest affiliates of the Na-tional Alliance on Mental Illness, thisgrassroots organization provides support,education and advocacy for families andconsumers of all ethnic and socio-eco-nomic backgrounds who live with mentalillness. Their twenty support groups ad-dress the needs of those suffering fromschizophrenia, bipolar Disorder, with fam-ily and children dealing with mental ill-ness, even providing pet therapy. The onlyadvocacy group us held the first-Friday-of-the-month. The Media & Advocacy Group(MAG) provides advocacy information,skill-building, networking and a monthlyspeaker from the field. NAMI-NYC Metro’sHelpline is available Monday through Fri-day, noon to 7PM Mon - Thurs, noon to6PM Fridays (212) 684-3264. (pgs 47, 58)
NYS Office of Mental Health(NYSOMH), Bureau of Family & Recipient Affairs518-473-6579
The quarterly meeting, of their Commis-sioner’s Committee for Families, is an op-portunity for families and providers to learn
about NYSOMH’s latest activities, networkwith their colleagues, and become a focusgroup for OMH’s internal projects as wellas ones they generate. Call to obtain aWellness Self Management “Toolkit” or tojoin their listserv: listserv.omh.stte.ny.us.
EMPLOYMENT
The Center for Rehabilitation and Recovery212-742-1600
www.coalitionny.org
The center has created a comprehensiveworkbook listing of 115 NYC mentalhealth programs supporting employment.It also offers information on how to workwithout letting a salary interfere with re-ceiving benefits as well as how to chooseand employment program. The workbookis downloadable from their website.
Employer Assistance & RecruitingNetwork (EARN)http://www.earnworks.com
This free service connects employers look-ing for quality employees with skilled jobcandidates. Federal and private employers,employment service providers, and jobseekers can sign-up through the website,and either post openings or locate job op-portunities in their local region.
Equal Employment OpportunityCommission (EEOC)800-669-4000 or (TTY) 800-669-6820
http://www.eeoc.gov/
The EEOC is responsible for the enforce-ment of the Americans With DisabilitiesAct (ADA). In addition to mental illness is-sues in the workplace, this site also dealswith a variety of other topics related todiscrimination, including reporting proce-dures to file a complaint. Other interestingtopics include Best Practices for the Em-ployment of People with Disabilities inState Government and Information forSmall Businesses in Complying with theAmericans with Disabilities Act.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

42
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
Job Accommodation Network(JAN).1-800-526-7234 (V/TTY)
http://www.jan.wvu.edu/
This free consulting service of the Office ofDisability Employment Policy through theU.S. Department of Labor is designed to in-crease the employability of people with dis-abilities by: 1) providing individualizedworksite accommodations solutions; 2) pro-viding technical assistance regarding theAmericans with Disabilities Act and otherdisability related legislation; and 3) educat-ing callers about self-employment options.
New York State Department ofLabor and Workforce New Yorkhttp://www.nycareerzone.org/
The New York State Department of Laborand Workforce New York sponsors CareerZone, which offers careers explorationsand helps match interests, skills and abili-ties of job-seekers to job openings.
Vocational and EducationalServices for Individuals withDisabilities (VESID)518-474-1711, 800 222-jobs or 5626)
VESID, New York State’s vocational reha-bilitation system, offers both transitionaland supportive employment opportunities.VESID coordinates services relating to vo-cational assessment, vocational counsel-ing, training and placement, and jobfollow-up. VESID ensures that both the in-dividual and the employer are satisfiedwith the placement and VESID will inter-vene if problems occur once an individualis placed in a job. VESID is also a vendor inthe Ticket to Work Program administeredby the Social Security Administration.
Partnership for Workplace Mental Health703-907-8561 or 703-907-8673
http://www.workplacementalhealth.org/
This site offers educational materials anda forum to explore mental health issuesfor employers and employees, including
the publications Mental HealthWorks andA Mentally Healthy Workforce: It’s Goodfor Business.
Ticket to Work866-968-7842 or (TTD) 866-833-2967
www. http://www.yourtickettowork.com/
A federal program administered by theSocial Security Administration, the Ticketto Work is a coupon you can take to anyprovider to gain vocational rehabilitation,training, job referrals, and other ongoingsupport and services to reach employmentgoals.
NYS Office of Vocational and Educational Services for Individuals with Disabilities(VESID)http://www.vesid.nysed.gov/
Offers access to a full range of servicesthat may be needed by persons with dis-abilities through their lives, including spe-cial education, cognitive rehabilitation,vocational rehabilitation and independentliving programs. Visit the website for con-tact information for the district office inyour county.
Workforce One Centers (NYC Only)954-677-5555
http://www.wf1broward.com/
Located in every NYC borough, have aDisability Navigator on staff. All NYC resi-dents are eligible. In addition to place-ment assistance they provide some limitedtraining vouchers, access to a computer,printer, phone, and fax, and GED classes.
FOOD STAMPS
NYC Human ResourceAdministration, Department of Social Services718 472-8411, (TTY) 718-262-3566 or800-342-3009
http://www.nyc.gov/html/hra/html/direc-tory/food.shtml
Visit the website to download applicationas well as locate addresses and informa-tion for 19 centers throughout the cityopen from 8:30AM to 5PM Mondaythrough Friday. (see p. 14)
New York State Office ofTemporary Disability Assistance1-800-342-3009 and press “1” for FoodStamps
http://www.otda.state.ny.us/main/food-stamps/
FUTURE CARE PLANNING FORSPECIAL NEEDS TRUSTS
Future Care PlanningClearinghouse800-652-2090
Information on wills, trusts, guardianshipand some referrals. A Special Needs Trust(SNT) needs to be set up in the case of aninheritance to a) protect consumer from lossof benefits and b) to keep the inheritanceintact to provide for supplemental needs.
HEALTH, GENERAL
Healthfinderwww.healthfinder.gov
This web site can help locate selected on-line publications, clearinghouses, data-bases, and support and self-help groupsas well as government agencies and not-for-profit organizations.
MedicineNetwww.medicinenet.com
Produced by a network of doctors, thissite includes news and perspectives, treat-ment updates, health facts, a medical dic-tionary and an index of commonly usedmedications.

43
HEALTH - MENTAL (GENERAL)
Center for Mental Health Serviceswww.mentalhealth.org
A Substance Abuse and Mental HealthServices Administration (SAMHSA) sitethat promotes education of mental illnesson a large scale. It includes mental illnessstatistics regarding mental as well asnews and a searchable database. Theyoffer excellent ongoing gratis educationalmaterials to subscribers to their listserv.
Family Institute for Education,Practice and Researchwww.nysfamilyinstitute.org
Provides statewide training, technical assis-tance and supervision to mental healthproviders in the design, implementation,and evaluation of research-based family in-terventions for individuals with severe men-tal illness and their families. It’s Consumer-Centered Family Consultation is a gatewayservice for the full Spectrum of Family Serv-ices. . For more information, contact: AnneSmith by phone or send an email [email protected]. (p. 25)
Mental Health Americawww.nmha.org
Formerly the National Mental Health As-sociation. News, legislative alerts, freepublications, extensive resources, linksand more. Their website is very easy tonavigate.
Mental Health Association in New York State518-434-0439www.mhanys.org
Mental Health [email protected]
Family run, Mental Health Resources edu-cates families about how to exercise theirrights, navigate the mental health system,
get services and partner with their lovedone to build an independent life—securingtreatment, employment, housing and more.
National Alliance on Mental Illnesswww.nami.org
The National Alliance on Mental Illness(NAMI) is a nonprofit, grassroots, self-help, support and advocacy organizationof consumers, families, and friends of peo-ple with severe mental illnesses. Foundedin 1979, NAMI has more than 210,000members who seek equitable services forpeople with severe mental illnesses.
National Alliance on MentalIllness of New York State518-462-2000 or 800-950-3228
www.naminys.org
The National Alliance on Mental Illness ofNew York State (NAMI-NYS) is a grass-roots education, advocacy and support or-ganization of persons with mental illnessand their families in 56 affiliatesstatewide. The website features a varietyof information and resources, includingthis handbook.
National Alliance on MentalIllness of New York City Metro212-684-3264http://www.naminycmetro.org/
The National Alliance on Mental Illness ofNew York City Metro, Inc. is one of thelargest affiliates of the National Allianceon Mental Illness. This grassroots organi-zation provides support, education andadvocacy for families and individuals of allethnic and socio-economic backgroundswho live with mental illness.
Network of Care for Behavioral Healthhttp://newyorkcity.ny.networkofcare.org/mh/home/
A highly interactive, one-stop site to ac-cess information on NYC services.
New York City Division of Mental Hygiene212-219-5003http://www.nyc.gov/html/doh/html/dmh/dmh.shtml
Division Of Consumer Services, offers theconsumer services in a wide range of re-covery-oriented programs.
New York State Office of Mental Health518-474-2568 or 800-597-8481http://www.omh.state.ny.us/44 Holland AvenueAlbany, New York 12229
New York State Office of Mental Health.This New York State agency is authorizedby law to operate 25 psychiatric hospitalsand oversees 2500 local non-profit andgovernment providers of mental healthservices statewide (including inpatient andoutpatient, emergency, community sup-port, residential and family care programs).
National Institute of MentalHealth (NIMH)www.nimh.nih.giv
Authority on mental health research. Visitthis website to learn about mental ill-nesses, research and treatment.
GOVERNMENT
Mental Health Links to Federal Web Siteshttp://mentalhealth.samhsa.gov
National Institute of Mental Healthwww.nimh.nih.gov
This web site provides information onbasic and clinical research activities.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

44
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
New York City Servicesww.nyc.gov
New York City Services provides the publicwith access to information about NewYork City agencies and services
New York State Governmenthttp://www.state.ny.us/
New York State Governorwww.state.ny.us/governor
New York State Senatewww.nysenate.gov
New York State Senate features informationon the activities of the state senate as wellas the location of your senators offices.
New York State Assemblywww.assembly.state.ny.us
This web site allows you to contact yourdistrict Assembly representative by e-mail.
New York State Office of Mental Healthwww.omh.state.ny.us
Social Security Onlinewww.ssa.gov
Answers to your FAQ’s, news, a specialsection on understanding social securityand much more. Information in Englishand Spanish.
HEALTH INSURANCE (private)
Health Insurance Hotline800-333-4114
NYS Insurance Department800-342-3355
NYS Attorney General Health Care Bureau800-692-4422
HEALTH INSURANCE (public)
Medicaid: New York StateMedicaid Hotline800-342-3009
Medicare: Basic Information Line for sign-up/eligibility: 800-772-1213
Medicare Hotline800-MEDICARE (pgs. 13, 41)
Children’s Health InsuranceProgramhttp://www.cms.hhs.gov/LowCostHealthInsFamChild/
Previously known as the State Children’sHealth Insurance Program (SCHIP), thisstate and federal partnership targets unin-sured children and pregnant women infamilies with incomes too high to qualifyfor most state Medicaid programs, butoften too low to afford private coverage.
Child Health Plus800-300-8181 /718-630-0126
http://www.healthplus-ny.org/en/119_ENG_HTML.html
Child Health Plus/Health Plus provides achild or teenager with free or affordablehealth coverage depending on theirhousehold income.
Family Health Plushttp://www.health.state.ny.us/nysdoh/fhplus/
Family Health Plus is a public health insur-ance program for adults who are aged 19to 64 who have income or resources toohigh to qualify for Medicaid. Family HealthPlus is available to single adults, coupleswithout children, and parents who areresidents of New York State and are
United States citizens or fall under one ofmany immigration categories.
Family Health Plus provides comprehen-sive coverage, including prevention, pri-mary care, hospitalization, prescriptionsand other services. There are minimal co-payments for some Family Health Plusservices, which are provided through par-ticipating managed care plans.
Healthy New Yorkhttp://www.ins.state.ny.us/website2/hny/english/hny.htm
An extremely basic State health insuranceplan that does not include mental healthcoverage.
HELPLINES
New York City Department of Mental Health1-800-LIFENET (24 hours, professional staff)
NAMI-New York City Metro Helpline212-684-3264 (open noon to 7PM Mon - Thurs, Friday noon to 6PM)
HOUSING
Association for Community Living (ACL)518-426-3635
www.aclnys.org
ACL is a statewide membership organiza-tion of not-for-profit agencies that providehousing and rehabilitation services tomore than 20,000 people diagnosed withserious and persistent mental illness. Thiswebsite offers detailed descriptions of li-censed and supported housing options aswell as resources, links, discussion forumsand a shortcut to the Office of MentalHealth residential program finder.

45
Center for Independence of the Disabled, NY212-674-2300212-674-5619 TTY (Manhattan)
646-442-1520718-886-0427 TTY (Queens)
http://www.cidny.org
This not-for-profit is part of the Independ-ent Living Centers movement. Its goal isto ensure full integration, independenceand equal opportunity for all people withdisabilities by removing barriers to the so-cial, economic, cultural and civic life of thecommunity. CIDNY’s offices in Manhattanand Queens provide benefits counseling,direct services (e.g. housing assistance,transition services for youth with disabili-ties, employment-related assistance,healthcare access, peer support groups),information and referrals, and recreationalactivities.
Center for Urban CommunityServices (CUCS)212-801-3300
www.cucs.org
Since 1987, CUCS’ Housing ResourceCenter has provided information and ac-cess to housing for homeless people withpsychiatric disabilities and other specialneeds. CUCS administers the Single Pointof Access service. (SPOA). One-stop shop-ping for New York City residents to workwith consultants in a housing outreachcampaign.
Community Access Inc.212-780-1400
http://www.communityaccess.org/
Community Access, Inc. (CA) helps hun-dreds of people with psychiatric disabili-ties make the transition from hospitalsand shelters to independent living. CA’sprimary mission is to identify needs andcreate solutions for homeless people withpsychiatric disabilities. Our programs in-clude housing, support services, counsel-ing, education and employmentopportunities. Community Access believesthat all people can lead productive, self-
sufficient, dignified lives, and we are dedi-cated to providing the resources neededto achieve that goal.
Corporation for Supported Housing212-986-2966
Advocacy, information and referrals andhousing services
New York State Department of Healthhttp://www.health.state.ny.us/
Find a statewide listing of adult homes,including a list of homes on the State’s‘Do Not Refer’ List: http://www.health.state.ny.us/facilities/adult_care/memorandum.htm
NYS Office of Mental HealthSingle Point of AccessMoira Tashjian, Director of Housing Re-Design
(518) 402-5233
US Department of Housing and Urban Development also known as the “Section 8Housing Program(212) 306-3322
http://www.hud.gov/progdesc/voucher.cfm
Find information and eligibility require-ments for the federal government’s Hous-ing Choice Voucher program, whichenables very low-income families, the eld-erly, and the disabled to afford decent,safe, and sanitary housing in the privatemarket. -Under the Section 8 Program, thepublic housing authority (PHA) generallypays a supplement to the landlord. Al-though currently HUD is not acceptingnew applications and it only extending ex-piring commitments it does periodicallyopen the vouchers.
JAILS AND PRISONS
New York State Department of Correctional Serviceshttp://www.docs.state.ny.us/faclist.html
This website provides an alphabetical list-ing of all correctional facilities within NewYork State, including the phone number,mailing address, security level, and links toMapQuest.
KENDRA’S LAW (AssistedOutpatient Treatment, AOT)New York State Office of Mental Health
http://www.omh.state.ny.us/omhweb/Kendra_web/Khome.htm
New York State law provides for court-or-dered assisted outpatient treatment (AOT)for certain people with mental illness that,in view of their treatment history and cir-cumstances, are unlikely to survive safelyin the community without supervision.Visit the above OMH website to find linksto further information concerning Kendra’sLaw and Assisted Outpatient Treatment.
LEGAL SERVICES
Bazelon Center for Mental Health Lawwww.bazelon.org
Focuses on legal issues pertaining to men-tal illness and developmental disabilities,including involuntary admissions and ad-vance psychiatric directives.
Disability Advocateshttp://www.disability-advocates.org/
Legal Aid Society of Northeastern New York800-462-2922
http://www.lasnny.org/
Covers Albany, NY area, but can giveother regional numbers
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

46
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
Legal Referral Service (Sponsoredby the NYS Bar Association)800-342-3661
Mental Hygiene Legal ServicesProvides legal representation for inpa-tients, for those referred for Assisted Out-patient Treatment, and for outpatientswith mental illness and developmentaldisabilities if they are in a certified com-munity residence)
Bronx/Manhattan: 212-779-1734
Duchess, Kings, Nassau, Orange, Putnam,Queens, Richmond, Rockland, Suffolk andWestchester counties: 516-746-4545.
Allegheny, Cattaraugus, Cayuga, Chau-tauqua, Erie, Genesee, Herkimer, Jefferson,Lewis, Livingston, Monroe, Niagara,Oneida, Onondaga, Ontario, Orleans, Os-wego, Seneca, Steuben, Wayne, Wyomingand Yates counties: 716-530-3050.
All other counties: 518-474-4453
New York Lawyers for the Public Interesthttp://www.nylpi.org/
Advocates on behalf of disabled groups.Offers fact sheets about employment dis-crimination.
Protection and Advocacy for Individuals with Mental Illness(PAIMI)800-624-4143
Urban Justice Centerhttp://www.urbanjustice.org/
The Urban Justice Center serves New YorkCity’s most vulnerable residents through acombination of direct legal service, sys-temic advocacy, community education andpolitical organizing.
MEDICAID
New York State Medicaid Hotline: 800-342-3009
MEDICARE
Basic Information Line for sign-up/eligibility800-772-1213
Medicare Hotline800-MEDICARE (pgs 13, 41)
REDUCED FARE CARD1. Go to: www.mta.info
Put in “Reduced Fare Card” in thesearch box on the left
2. Double click on the link top of theGoogle list “Reduced Fare Card”
3. Print” Application and Condition.” Aska physician or other licensed healthprovider “certifier” to fill out the “Cer-tification” sheet and return it with theapplication and a passport photo to:130 Livingston Street, Brooklyn NY11201-9625
For Metro Card Customer Service (212) 638-7622
If you don’t have a computer you can callfor the application at (718) 243-4999. Ittakes six to eight weeks to process.
For those outside the five boroughs agood start to locate where to get a HalfFare card would be your local CountyTransit Authority of the Department oftransportation. (p. 14)
RESEARCH
National Alliance for Research on Schizophrenia and Depression(NARSAD)800-829-8289 or 516-829-0091www.narsad.org
A private, not-for-profit organization thatraises funds for scientific research into thecauses, cures, treatments and preventionof brain disorders such as schizophreniaand depression.
National Institute of MentalHealth (NIMH)www.nimh.nih.giv
Engages in research on the causes andtreatment of mental disorders. Its websiteprovides educational materials and an ex-tensive list of free publications on psychi-atric disorders, including a comprehensivelisting of helpful resources.
Nathan Kline Institute forPsychiatric Research (NKI)http://www.rfmh.org/nki/index.cfm
Focuses on patient-oriented research pro-grams emphasizing the causes, diagnosis,treatment, prevention, and care of severeand long-term mental disorders, also basicresearch on physiological and biochemicalaspects of mental disease.
New York State PsychiatricInstitutehttp://www.nyspi.org/research.html
Research on a wealth of subjects rangingfrom basic neurobiology to clinical, epi-demiological, child psychiatry and serv-ices-related studies. Conducts ongoingclinical trials in disorders ranging from de-pression to schizophrenia to borderlinepersonality disorder.
SOCIAL SECURITY800-772-1213http://www.ssa.gov/

47
SOCIAL SERVICES
NYC Human ResourceAdministration, Department of Social Services718 472-8411, (TTY) 718-262-3566 or 800-342-3009
http://www.nyc.gov/html/hra/html/directory/directory.shtml
Visit the website to download applicationas well as locate addresses and informa-tion for 19 centers throughout the city.They administer Medicaid. Open from8:30AM to 5PM Monday through Friday.
Community Service Societywww.cssny.org212-254-8900
160 years of providing services for threemillion low income New Yorkers in suchareas as improving literacy, assisting chil-dren and families of the incarcerated andhelp in navigating the health care system
NYS Department of Social Services518-474-2121 or 518-463-4829
General information on eligibility require-ments, local phone numbers/locations,how to get HEAP, food stamps, emergencyshelter, etc.
SUPPORT GROUPS
NYC Depressive & ManicDepressive Group (DMDG)(917) 445-2399
A support group for persons with mooddisorders, depression and bipolar disorderas well as their family members andfriends
National Alliance on MentalIllness - New York State518-462-2000 or 800-950-3228
www.naminys.org
NAMI-NYS lists local affiliates of the Na-tional Alliance for the Mentally Ill in NewYork State. Call or visit the website to finda support group in your area.
National Alliance on MentalIllness of New York City Metro(NAMI-NYC Metro)212-684-3264
http://www.naminycmetro.org/
One of the largest affiliates of the Na-tional Alliance on Mental Illness, thisgrassroots organization, it provides sup-port, education and advocacy for familiesand consumers of all ethnic and socio-economic backgrounds who live withmental illness. Their twenty supportgroups address the needs of those suffer-ing from schizophrenia, bipolar disorder,for family and children dealing with men-tal illness as examples. The only groupdedicated to advocacy is held the first-Fri-day-of-the-month Media & AdvocacyGroup (MAG). It provides advocacy infor-mation, skill-building, networking and amonthly speaker from the field. NAMI-NYC Metro’s Helpline is available Mondaythrough Friday, noon to 7PM and Fridayfrom noon to 6PM 5PM (212) 684-3264.
NYS OMH Bureau of Family Affairs (518) 473-6579
NYS OMH Commissioner'sCommittee for FamiliesOffers a listserv and quarterly advisorymeetings to learn about OMH's activities,an opportunity to network with otherstatewide family groups and to learn howto improve the system through informedand focused advocacy.
PEER SUPPORT
The Alliance EmpowermentCoalition800 654-7227
The Alliance Peer Support Center315 732-5377
Dreamweavers Peer Support315 542-3427
The Empowerment Center(914) 576-7022
Hands Across Long Island631 234-1925
Howie the Harp Advocacy Center212 865-0775
Mental Health EmpowermentProject1-800-MHEPinc
NAMI Peer-to-Peer:www.naminycmetro.org
NAMI Connectionwww.nami.org
Peer Bridger projectwww.nyaprs.org
P.E.O.P.L.E s., Inc.845 452-2728
Step by Step315 394-0597
Treatment & ResearchAdvancements NationalAssociation for PersonalityDisorder (TARA),www.tara4bpd.org888-4-TARA APD
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together

48
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery TogetherA national association devoted to personal-ity disorders, has pioneered raising publicawareness about this least understood men-tal illness. TARA’s hotline, workshops, educa-tional seminars, symposia, teen groups,advocacy and referral service, provide all-round support to families and sufferers
Family Support:Family-to-Family program. Contact yourlocal NAMI chapter (you can find affiliatelistings on our website) or call NAMI-NYSat 518-462-2000 or 800-950-3228 tofind an education course near you.
SUICIDE HOTLINES AND PREVENTION
American Foundation for Suicide PreventionToll-free: 1-888-333 AFSP (2377)Phone: 212-363-3500Fax: 212-363-6237Email: [email protected]: www.afsp.org
Covenant House1-800-999-9999
Deaf Hotline1-800-799-4889
LivingWorks OfficesPhone: 910-867-8822Fax: 910-867-8832Email: [email protected]: www.livingworks.net
National Hope Line1-800-SUICIDE (784-2433)1-800-273-TALK (8255)
New York State Office of Mental Health (S.P.EA.K.Suicide Prevention kit)1-800 597-8481
Suicide Prevention ActionNetwork USA (SPAN USA)Phone: 202-449-3600Fax: 202-449-3601Email: [email protected]
The Trevor Project Gay Hotline1-800-850-8078
WELLNESS SELF MANAGEMENT
New York State Office of Mental Healthhttp://www.omh.state.ny.us/omhweb/ebp/adult_wellness.htm
Wellness self-management program offerstools, in the form of workbooks to struc-ture a path to recovery: to assist manag-ing stress, to provide education on thesymptoms of a diagnosis and to offerskills overcome barriers to pursue per-sonal goals.
WRAP
Copeland Center802-254-2092 or 866-IDOWRAP
www.mentalhealthrecovery.com
To find a WRAP group in your community,send an email to [email protected] specifying where you live.

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
49
Note: Share At -A-Glance Medicaid Buy-In attached with .the Medicaid office to assure you get the service you need)
FAMILIES TAKE NOTE:YOUR LOVED ONE CAN EARN AS MUCH AS $55,188 PER YEAR (2009-2010) AND NOT LOSETHEIR ACCESS TO HEALTH BENEFITS. TO THE RESCUE:
Medicaid Buy-In Programfor Working People withDisabilities (MBI-WPD)
The Medicaid Buy-In program offers Medicaidcoverage to people with disabilities who are working, andearning more than the allowable limits for regular Med-icaid, the opportunity to retain their health care cover-age through Medicaid. This program allows workingpeople with disabilities to earn more income without therisk of losing vital health care coverage.
To qualify for the Medicaid Buy-In program forWorking People with Disabilities, you must
• Be a resident of New York State;• Be at least 16 years of age (coverage up to 65
years of age);• Have a disability as defined by the Social Security
Administration;• Be engaged in paid work (includes part-time and
full-time work• Have a gross income that may be as high as
$55,188 for an individual, $73,884 for a disabledcouple
• Have non-exempt resources that do not exceed$13,800 for an individual, $20,100 for a disabledcouple in 2009.To Apply:
1. Be prepared to submit proof of disability (if youare currently receiving a form of Social Securitybenefits for the disabled that proof should be suf-ficient). Even if you don't receive benefits, youalso qualify for MBI-WBD if you meet Social Se-curity eligibility requirements as "disabled."
2. In NYC contact your local NYS_ State Medicaidoffice and fill out their LDSS-2021 form. Don'tbe overwhelmed. A customer service specialist isthere to provide support and a "Tool Kit" to takeyou through the process. Since the LDSS-2021 isa Medicaid common application, identify it as"MBI-WPD" with a bold black marker on theupper right, corner, date it and make a copy.
**To help the staff person be clear about which pro-gram you're referring to, you may want to attach thetwo-page "At a Glance" sheet found on p. 51. Also,bring it with you to your appointment.
For the rest of NYS contact your local Dept. of So-cial Services/Medicaid office and Neighborhood LegalServices (see below).
Make sure you take to your appointment proof ofthe following:
a) Medical: Physicians' name, address and tele-phone number.
b) Benefits: Medicare Part A and B, private healthinsurance (if you have these benefits).
c) Proof of income: social security, alimony, veteran'sbenefits, $ support from family members et al.
d) Citizenship: birth certificate, U.S. Passport, Natu-ralization certificate with photo ID.
e) Residency home address: ID card, letter/lease/rent receipt with home address etc.
APPENDIXMEDICAID BUY-IN

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
50
f) Resources: money in a bank, stocks, bonds, mu-tual funds CDs. money market accts, 402k plans,trusts, cash value of life insurance. If anything ismissing you have ten days provide it to the pro-cessing can go ahead.
MEDICAID BUY-IN OFFICES ETC.
New York CityBronx Medicaid Offices: Bronx Lebanon Hospital,
Lincoln Hospital, North Central Bronx Hospital,Jacobi Hospital, And Morrisania
Brooklyn Medicaid Offices: Boerum Hill, ConeyIsland, Kings County Hospital, East New York,Woodhull Hospital
Manhattan Medicaid Offices: Bellevue Hospital,Chinatown, Metropolitan Hospital, ColumbiaPresbyterian Hospital, and Harlem Hospital
Queens Medicaid Office: Elmhurst Hospital,Rockaway, Jamaica
Staten Island Medicaid Office: Staten Island
To determine where you should apply and getanswers to additional questions concerningMBI-WPD and Work Incentives programsstatewide call:
Neighborhood Legal ServicesWork Incentives Hotline888) 224-3272www.nls.org
(Share with the Medicaid office to assure get the service you need)
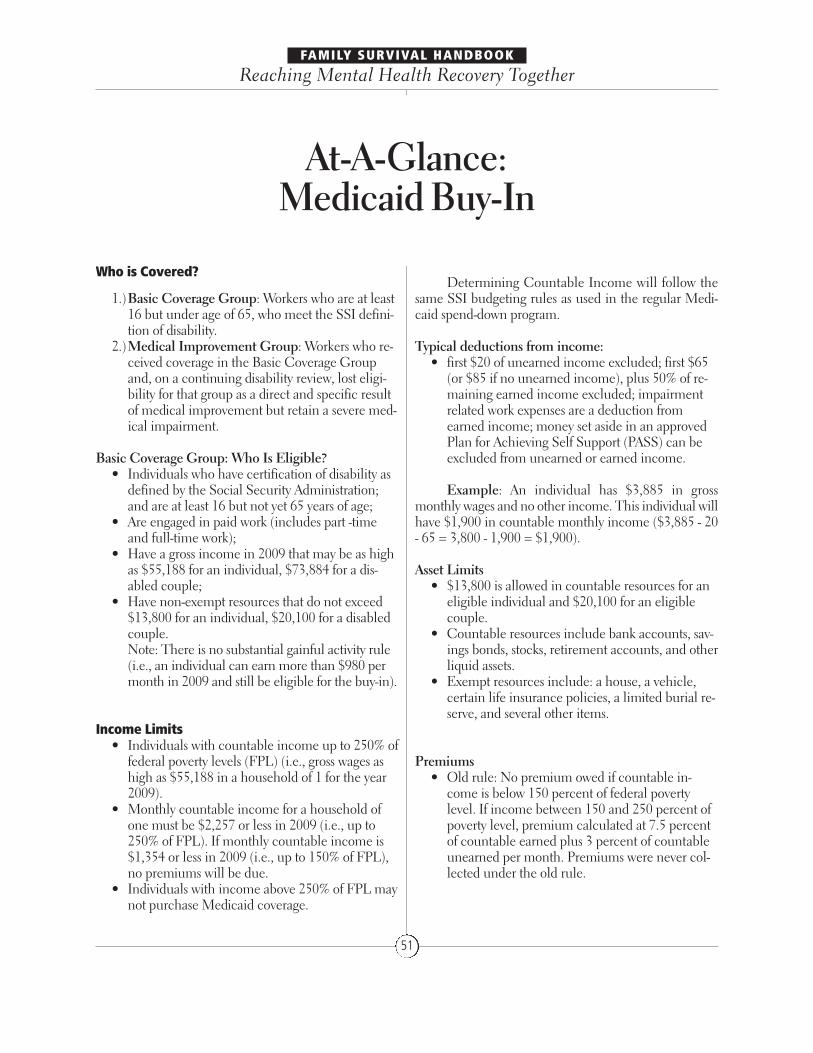
Who is Covered?
1.)Basic Coverage Group: Workers who are at least16 but under age of 65, who meet the SSI defini-tion of disability.
2.)Medical Improvement Group: Workers who re-ceived coverage in the Basic Coverage Groupand, on a continuing disability review, lost eligi-bility for that group as a direct and specific resultof medical improvement but retain a severe med-ical impairment.
Basic Coverage Group: Who Is Eligible?• Individuals who have certification of disability as
defined by the Social Security Administration;and are at least 16 but not yet 65 years of age;
• Are engaged in paid work (includes part -timeand full-time work);
• Have a gross income in 2009 that may be as highas $55,188 for an individual, $73,884 for a dis-abled couple;
• Have non-exempt resources that do not exceed$13,800 for an individual, $20,100 for a disabledcouple.Note: There is no substantial gainful activity rule(i.e., an individual can earn more than $980 permonth in 2009 and still be eligible for the buy-in).
Income Limits• Individuals with countable income up to 250% of
federal poverty levels (FPL) (i.e., gross wages ashigh as $55,188 in a household of 1 for the year2009).
• Monthly countable income for a household ofone must be $2,257 or less in 2009 (i.e., up to250% of FPL). If monthly countable income is$1,354 or less in 2009 (i.e., up to 150% of FPL),no premiums will be due.
• Individuals with income above 250% of FPL maynot purchase Medicaid coverage.
Determining Countable Income will follow thesame SSI budgeting rules as used in the regular Medi-caid spend-down program.
Typical deductions from income: • first $20 of unearned income excluded; first $65
(or $85 if no unearned income), plus 50% of re-maining earned income excluded; impairmentrelated work expenses are a deduction fromearned income; money set aside in an approvedPlan for Achieving Self Support (PASS) can beexcluded from unearned or earned income.
Example: An individual has $3,885 in grossmonthly wages and no other income. This individual willhave $1,900 in countable monthly income ($3,885 - 20- 65 = 3,800 - 1,900 = $1,900).
Asset Limits• $13,800 is allowed in countable resources for an
eligible individual and $20,100 for an eligiblecouple.
• Countable resources include bank accounts, sav-ings bonds, stocks, retirement accounts, and otherliquid assets.
• Exempt resources include: a house, a vehicle,certain life insurance policies, a limited burial re-serve, and several other items.
Premiums• Old rule: No premium owed if countable in-
come is below 150 percent of federal povertylevel. If income between 150 and 250 percent ofpoverty level, premium calculated at 7.5 percentof countable earned plus 3 percent of countableunearned per month. Premiums were never col-lected under the old rule.
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
51
At-A-Glance: Medicaid Buy-In

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
52
• New rule: No premium is owed if countable in-come is below 150 percent of the federal povertylevel. If income is between 150 and 250 percentof the federal poverty level, premium will be $25per month for an eligible individual, $50 permonth for an eligible couple. As this is written,the State Department of Health still does nothave a system in place to collect premiums.
Applying For the Medicaid Buy-In ProgramAn application for the Medicaid Buy -In Program
for Working People with Disabilities must be made at theLocal Department of Social Services or the Human Re-sources Agency in New York City.
Medical Improvement Group: Who Is Eligible?
Individuals who are• Members of the Basic Coverage Group, who lose
eligibility for the Basic Coverage Group due tomedical improvement but retain a severe medicalimpairment, and
• Are engaged in paid work (40 hours per monthand earn at least the federal minimum wage)
Grace Periods Or What If I Lose My Job?
Change in Medical Condition: A grace period ofup to six months will be allowed if, for medical reasons,the Medicaid Buy-In recipient is unable to continueworking. Medical verification will be required.
Job Loss (through no fault of recipient): A grace pe-riod of up to six months will be allowed if, through no faultof the recipient, a job loss occurs (layoff, etc.). Verificationwill be required that the recipient is reasonably expected toreturn to work, or that the recipient is actively seeking newemployment. If this is less than 250% of the FPL for 2009,this individual will be eligible for the Buy-in.
Plan for Achieving Self-Support (PASS) is a planthat allows a person to exclude income other than SSI sothe money could be used for education, training orequipment that will help them to return to employment.The goal of a PASS is to help a person become self-suffi-cient and lessen their dependency on disability benefits.There are 2 cadre offices in NY Contact: NYC PassCadres at 800 551-9583 x4048 or x4045, or outside of theMetro NYC area, 800-510-5680 or 716-551-4640 x242,246, 286.

The Family Survival Handbook is a collaborativeproject between Family Institute for Education, Prac-tice & Research, Mental Health Resources, NationalAlliance on Mental Illness of New York State and NewYork State Office of Mental Health.
We thank the following individuals and/or organi-zations for their contributions to the following sections:
EMPLOYMENTSandy Regenbogen Weiss, Director of Consumer
Services, and Hallie Schneider, Consumer Specialist,Center for Independence of the Disabled, New York,841 Broadway # 301, New York, NY 10003
EMPLOYMENT RESOURCESLana Sullivan, MS, Program Director, Con-
sumer & Business Outreach, Mental Health Associa-tion in New York State, Inc., 194 Washington Avenue,Suite 415, Albany, NY 12210, (518) 434-0439 ext. 224,(518) 427-8676 fax, www.mhanys.org/programs/cbop/
HOUSINGRena Finkelstein, Senior NAMI State member,
[email protected] and Daniel J. Stern, Hous-ing Consultant, Center for Urban Community Services(CUCS), Moira Tashjian, Director of Housing Re-De-sign, Single Point of Access, (518) 402-4233, [email protected].
MEDICAID AT-A-GLANCEKrista McDonald, Staff Paralegal/Benefits Spe-
cialist, Neighborhood Legal Services, Inc., (716) 847-0650 Work Incentives Hotline: 1-888-224-3272 •www.nls.org , Main - Seneca Building, 237 Main St,Suite 400, Buffalo, NY 14203, 716-847-0650 , OlgaIvnitsky, (718) 256-5631, [email protected]
And thanks for.....� The 40 families who are rooting for this Hand-
book and put their heart and souls into a focusgroup critique to assure multiple perspectives arerepresented
� To NYSOMH Commissioner Hogan who re-sponded to our initial requests and to John Allenand Tom O’Clair of the Commissioner’s Com-mittee for Families for not only allowing the fam-ily voice to be heard but saw that it was bysupporting this project in every way
� Lori Cullen, Communications Specialist atNAMI NYS whose stalwart and thorough edito-rial and organizational contributions are seenthroughout
� Jeff Keller, who, as part of the originating team,promoted the idea and contributed copy andsources.
� Anne Smith, a true believer of a Handbook andstalwart champion of families
� Judith Carrington, initiator and primary writerPresident, Mental Health Resources
Let us hear how this Handbook works for you,what should be added or eliminated—it’s a work inprogress.
Here’s how to reach us:Anne Smith, Dir. Family Institute
for Education, Practice & Research,[email protected]
Judith Carrington: President, Mental Health Resources, [email protected]
Lori Cullen, Communications Specialist, NAMI-NYS, [email protected]
FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
53
CONTRIBUTORS

FAMILY SURVIVAL HANDBOOK
Reaching Mental Health Recovery Together
54
The Bureau of Family Affairs works directly withfamilies, recipients and local and state mental healthproviders. This coordinated approach was developed tostrengthen communications, linkages, policies and bestpractice standards to improve the quality of mentalhealth care in New York State.
The Commissioner of the Office of Mental Healthhas designated Family Liaisons in each of these regionsto assist family members and other advocates of individ-uals with psychiatric disabilities.
The names, addresses and telephone number ofthe five Family Liaisons and their staff are available onthe OMH website at www.omh.state.ny.us or by calling:
OMH Bureau of Family Affairs44 Holland Avenue, Albany, NY 12229Phone: 518-474-4888 Fax: 518-473-0373.
OMH FAMILY LIAISONS