rapid assessment: healthcare waste component of … waste management zimb… · dots directly...
TRANSCRIPT
Empowered lives. Resilient nations.
Supplement to the Healthcare Waste Management Toolkit for Global Fund Practitioners and Policy Makers
Rapid Assessment:
in Zimbabwe
Healthcare Waste Component of Global
Fund HIV, TB and Malaria Projects

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe22
Rapid Assessment: Healthcare Waste Component of Global Fund HIV,
TB and Malaria Projects in Zimbabwe
Supplement to the Healthcare Waste Management Toolkit for Global Fund
Practitioners and Policy Makers
All rights reserved ©2014 UNDP
June 2014
Author:
Jan-Gerd Kühling, Environment & Hygiene Consultant
ETLog Health GmbH, E-mail: [email protected]
UNDP contact: Dr. Christoph Hamelmann, [email protected]
Disclaimer: The consultant prepared this assessment report for the sole
use of the Client and for the intended purposes as stated in the agreement
between the Client and the consultant under which this work was completed.
The Consultant has exercised due and customary care in conducting this
assessment. The views set out in this assessment are those of the author and
do not necessarily reflect the official opinion of the UNDP. Neither the UNDP
nor any person acting on their behalf may be held responsible for the use
which may be made of the information contained therein.
Design & Layout: Phoenix Design Aid A/S, Denmark
Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 3
Table of Contents
1 Executive Summary .........................................................................................................................6
2 Assessed Projects .............................................................................................................................7
3 Background Information ................................................................................................................9 3.1 Assessment strategy ..............................................................................................................................................................9 3.2 Provided and reviewed project documents ........................................................................................................10
4 Legal Framework ............................................................................................................................11 4.1 International conventions ...............................................................................................................................................11 4.2 National legal healthcare waste framework ........................................................................................................12
5 Assessment of the Healthcare Waste Situation ........................................................................14 5.1 Input-output analysis .........................................................................................................................................................14 5.1.1 ZIM-809-G11-H (HIV) ..............................................................................................................................................14 5.1.2 ZIM-M-UNDP (Malaria) ...........................................................................................................................................14 5.1.3 ZIM-809-G12-T (Tuberculosis) ...........................................................................................................................15 5.1.4 ZIM-809-G14-S (Health System Strengthening) ....................................................................................15 5.2 Generated and expected waste quantities ..........................................................................................................15 5.3 Current waste management procedures within the GF programme .................................................16 5.4 Current healthcare waste disposal practices in Zimbabwe .......................................................................17
6 Findings & Recommendations .....................................................................................................18 6.1 Recommendations, generally applicable to all GF-financed health programmes ......................18 6.2 Recommendations for the GF programme addressing the country-specific context in Zimbabwe ...........................................................................................................................................................................20
7 Annexes ............................................................................................................................................21 7.1 Input analysis ...........................................................................................................................................................................21 7.2 Participants in the stakeholder interviews ............................................................................................................26

Abbreviations
ACSM Advocacy, communication and social mobilization
ART Antiretroviral therapyARV Antiretroviral (medicine)DOTS Directly observed treatment,
short-courseEMA Environmental Management AgencyGDF Global Drug FacilityGF Global Fund to Fight AIDS, Tuberculosis
and MalariaHCW Healthcare waste HIV Human Immunodeficiency VirusHSS Health system strengtheningITNs Insecticide-treated netsLLINs Long lasting insecticide-treated netsMOHCC Ministry of Health and Child Care
MOHCW Ministry of Health and Child WelfarePMTCT Prevention of mother-to-child
transmissionPPE Personal Protection Equipment PR Principal recipientPSM Procurement and supply managementQA/QC Quality assurance / quality controlRDT Rapid diagnostic testSOP Standard operating procedureSR Sub-RecipientSSF Single Stream FundingTB TuberculosisUNDP United Nation Development ProgrammeWEEE Waste of electrical and electronic
equipmentWHO World Health Organization
44 Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe
List of Figures
Figure 1: Assessment methodology ................................................................10
List of Tables
Table 1: Management structure – GF projects .................................................8
Table 2: Status of ratification of international conventions ............................11
Acknowledgements
This assessment report is part of the development of a toolkit to improve the planning and
implementation of better healthcare waste systems in future projects financed by the Glob-
al Fund to Fight AIDS, Tuberculosis and Malaria and implemented by UNDP. I would like to
acknowledge the valuable input of the following participants, without whom this research
would not have been possible.
From the UNDP Istanbul Regional Centre for Europe and Central Asia, Dr. Christoph
Hamelmann, Regional Team Leader HIV, Health and Development, coordinated the entire
work and concept, and peer reviewed all developed documents. John Macauley provided
continuous management support during the project time and peer review input.
We would like to express our thanks to Dr. Celestino Basera, Coordinator of GF grants in the
Ministry of Health and Child Care of Zimbabwe. Also our thanks are extended to the UNDP’s
Regional Service Centre for Africa and the UNDP country office in Zimbabwe which provided
the required documents and organized stakeholder interviews. Special thanks to Saleban
Omar and Tilly Sellers for coordination and Elliman Jagne, Adam Valois and all the other
UNDP colleagues for their work and continuous support.
5supplement to tHe HealtHcaRe Waste manaGement toolkit foR Global fund pRactitioneRs and policy makeRs

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe66
© UNDP
1 Executive Summary
over the course of the last 10 years, undp has been a strategic partner of the Global fund to fight aids, tuberculosis and malaria (Gf), and acts as interim principal Recipient (pR) of last resort for countries in which the Gf cannot identify a national pR for its grants. in order to deepen the understanding of the environmental impact caused by waste created through its Gf project implementation, an assessment of Gf health projects with undp pR-ship was conducted in tajikistan, uzbekistan and Zimbabwe.
This report outlines the results of the assessment in Zimbabwe which was carried out in the first half of 2014 in collaboration with national partners and undp representatives (annex, 7.2). With us$ 857,651,637 signed for Zimbabwe, it is one of the main recipient countries of Gf grants. With Gf support, already over 640,000 people have been put on antiretroviral (aRV) treatment, 25,000 new smear-positive tuberculosis (tb) cases have been detected and treated, 2.3 million insecticide treated nets (itns) were distributed to protect families from malaria and close to 800 tonnes of insecticides provided for indoor residual spraying. These activities also created different waste streams, and a need exists to ensure the environmentally safe disposal of waste already created (historical waste) and waste expected to be generated during the future implementation of such grants.
The rapid assessment of the Gf health grants identified the different types of waste. The country analysis showed that in Zimbabwe, a need exists for improved waste disposal solutions, especially for healthcare waste (HcW). The infrastructure for the treatment or disposal of hazardous waste is insufficient, and more advanced management methods are seldom introduced. first steps to improve the current situation were taken by developing a national HcW management plan and a draft guideline on the management of
HcW. However, further efforts are required by all stakeholders involved. Recommendations made in this report to improve the disposal of waste created by the Gf projects—for example, through the product life cycle of pharmaceuticals—could have a valuable impact beyond the Gf projects for the whole national health sector, and therefore serve as critical components of health systems strengthening (Hss). environmental safeguarding policies of the Gf should make the integration of HcW management components mandatory in grant-making processes with appropriate budget allocations. further recommendations are provided on how the HcW management system could be further strengthened within the framework of future Gf grants in Zimbabwe.
The HcW assessment of the Gf grants in Zimbabwe resulted in valuable information which will be included and used for the development of an HcW management toolkit for Gf grant planners and implementers.

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 7
ASSESSEd ProjECTS
2 Assessed Projects
undp is a long-term partner of the Gf and acts in several countries, including Zimbabwe, as the interim pR. in Zimbabwe, the following main projects are managed by undp1 :
HIV/AIDS: ZIM-809-G11-H name: “addressing critical Gaps in HiV prevention, treatment, care and support”:
Grant period from 01 jan 2010 to 31 dec 2014
according to unaids, Zimbabwe is experiencing one of the harshest aids epidemics in the world, with around one in ten members of the population living with HiV in 2010. even though the country has been experiencing a decline in HiV, critical areas of aRV treatment and HiV/aids counselling and testing need additional funding and scale-up to help mitigate the impact of HiV and aids. The Round 8 grant aims to reduce the number of new HiV infections among adults and children, and reduce morbidity and mortality due to aids in Zimbabwe. The grant targets youth, people living with HiV and aids, women and children. The programme will build upon the existing priority interventions that are being implemented within the national strategic framework with a focus on bringing the best practices to scale, as to curtail the estimated 40,000 new HiV infections occurring in adults and children, and bridging the gap to obtain universal access by scaling up antiretroviral therapy (aRt) service delivery (including treatment of opportunistic infections). The grant will also contribute to reaching 71 per cent of national prevention of mother-to-child transmission (pmtct) that targets pregnant women receiving more effective pmtct.
service delivery areas:
{ care and support P support for orphans and vulnerable children P care and support for the chronically ill{ prevention P behavioural change communication - community
outreach P behavioural change communication - mass media P counselling and testing P pmtct{ supportive environment P strengthening of civil society P treatment P aRV treatment and monitoring{ Hss P Health workforce{ other P community outreach and schools P collaborative activities: tb/HiV
Malaria: ZIM-M-UNDP - Zimbabwe Grant period from 01 apr 2012 to 31 dec 2014
no overview is provided on the official internet site.
service delivery areas:
{ prevention P indoor residual spraying/vector control P insecticide-treated nets (itns) P malaria in pregnancy{ treatment P diagnosis P prompt, effective antimalarial treatment{ other P epidemic preparedness and response P enhanced surveillance
1 all information has been taken from the Gf web site: http://portfolio.theglobalfund.org/en/Grant/list/ZWe

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe88
TB: ZIM-809-G12-T name: “towards universal access: improving accessibility to high quality directly observed treatment, short-course (dots) in Zimbabwe”
Grant period from 01 jan 2010 to 31 dec 2014
tb is a major public health problem in Zimbabwe which ranks 20th on the list of 22 high-burden tb countries in the world. according to WHo’s Global tuberculosis control Report 2008, Zimbabwe had an estimated 73,714 new tb cases in 2006, with an estimated incidence rate of 557 cases per 100,000 people. The overall goal of the programme is to further strengthen and expand the activities of the national tuberculosis programme by building on activities funded under the Round 5 grant and addressing some of the remaining identified gaps and weaknesses. The programme targets tb patients, people living with HiV and the at-risk populations. activities include the improvement of diagnostic services through the strengthening and expansion of dots (the basic package that underpins the stop tb strategy), salary support and provision of incentives for the recruitment and retention of critical staff, and establishment and equipping of two peripheral microscopy centres per rural district. tb/HiV will be addressed through the recruitment of a focal person for training all national programme staff in the diagnosis of sputum smear-negative cases. people with tb and communities will be empowered by the development of a national policy, training and social mobilization.
Service delivery areas:
{ other P procurement and supply management P improving diagnosis P tb/HiV P mdR-tb P acsm (advocacy, communication and social
mobilization) P High quality dots
Health Systems: ZIM-809-G14-S name: “Health systems strengthening cross-cutting interventions”:
Grant period from 01 jan 2010 to 31 dec 2014
a decade of high inflation, severe economic decline and rising poverty led to the departure of skilled health staff and the deterioration of infrastructure, which have seriously compromised efforts by the government of Zimbabwe and its international partners to provide universal access to basic health services and to combat HiV, tb and malaria. The goal of the programme supported by this grant is to achieve a strengthened and more effective health delivery system through the retention of the health workforce, the strengthening of community health systems and the scale-up in community programmes for the three pandemics. in addition, this grant will support the integration of monitoring and evaluation systems for the three diseases in a strengthened national health information management system, and the communication and information technology support required.
table 1 shows the management structure of the Gf projects.
Table 1: Management structure – GF projects
Position Organization
Fund Portfolio Manager GF
Country Coordination Mechanism
Country Coordination Mechanism (CCM) Zimbabwe (Chair: Ministry of Health and Child Welfare - MOHCW), National stakeholders and development partners
Principal Recipient UNDP, Zimbabwe
Local Fund Agent PriceWaterhouseCoopers, Zimbabwe

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 9
BACkground InFormATIon
3 Background Information
Key Country Data:
Full Name: Republic of ZimbabweTotal Population (2012)*: 13,724,000Area**: 390,757 sq kmLife expectancy at birth m/f (years)(2011)*: 53/55Infant mortality rate (2012)**: 26.55 deaths/1000 live birthsHospital bed density (2009)**: 1.7 beds/1000 populationGDP - per capita (PPP)(2013 estimate)**: $ 600
The Republic of Zimbabwe2 is a landlocked country in southern africa, bordering botswana, mozambique, south africa and Zambia. The Zambezi river forms a natural riverine boundary with Zambia. The climate is tropical, with a rainy season from november to march. Zimbabwe is divided into 8 provinces and 2 cities (bulawayo, Harare) with provincial status. The HiV/aids adult prevalence rate is 14.7 % (2012), the fifth highest in the world. tb and malaria are also widely spread. accordingly, the Gf is active in all three key areas.3
in the wake of Zimbabwe’s economic crisis in 2009, undp was appointed as pR for all Gf grants in the country, and additional safeguards were applied to these grants under the Gf’s additional safeguards policy. as pR, undp supports national partners in the implementation of the grants, and the development of national capacity and strengthening of national systems. undp implements the grants through various sub-recipients (sRs) including government (ministry
of Health and child care—moHcc—and national aids council), civil society organizations and un agencies. large parts of procurements are done through international commercial long-term agreements and partnerships with unicef and unfpa.
3.1 Assessment strategyfor carrying out the assessment, the consultant conducted a review of relevant and publicly available Gf grant documents. The focus of the analysis included: waste streams, waste amounts, available treatment systems and disposal options in Zimbabwe, and the current procurement processes. additionally, key project documents were provided by the undp country office in Zimbabwe.
after the review and analysis of the document, a desk review of the current HcW situation in Zimbabwe was carried out, which included the review of key
2 all country data provided in this chapter are sourced from the following: * World Health organization country data (http://www.who.int/countries/en/) ** central intelligence agency’s The World factbook (https://www.cia.gov/library/publications/the-world-factbook/geos/as.html) – current as accessed by the
consultant in 2013 unless indicated 3 for more information on Zimbabwe’s ongoing grants, visit the following web site: http://portfolio.theglobalfund.org/en/Grant/list/ZWe

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe1010
documents (e.g. national HcW management plan) and the review of relevant acts and regulations. based on these findings, a telephone conference with key stakeholders from the ccm, the moHcc, undp and others was held to discuss open questions.
3.2 Provided and reviewed project documents
The following documents were reviewed as part of the assessment:
a) Downloads from GF webpage a. Grant performance Report b. amended and Restated programme
Grant agreement 1
b) Project documents provided by the UNDP Office a. Zim-809-G11-H i. HiV original proposal ii. update of performance framework iii. full psm plan HiV iv. HiV – work plan and budget - phase2 b. Zim-m-undp i. malaria original proposal ii. update of performance framework iii. full psm plan malaria iv. single stream funding (ssf) malaria –
final dip c. Zim-809-G12-t i. tb original proposal ii. implementation letter 11 iii. full psm plan tb iv. tb interim funding Round 8 d. Zim-809-G14-s i. Hss – work plan and budget – rev 2
GF project
documents review
Inpu
t- Ou
tput
Anal
ysis
procurement processes
Analysis of GF callConference
Review of legal
documents
Figure 1: Assessment methodology
Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 11
LEgAL FrAmEwork
4.1 International conventions The assessment of relevant international conventions for HcW management showed that Zimbabwe recently (2012) acceded to the basel convention, the Rotterdam
convention and the stockholm convention. Zimbabwe is also a signatory of the new minamata convention (2013):
4 Legal Framework
Table 2: Status of ratification of international conventions
Name of convention Status of ratification Date
Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and their Disposal: (UNEP 2003)
Accessionhttp://www.basel.int/Countries/StatusofRatifications/PartiesSignatories/tabid/1290/Default.aspx
01/03/2012
Rotterdam Convention on the Prior Informed Consent Procedure for Certain Hazardous Chemicals and Pesticides in International Trade
Accessionhttp://www.pic.int/Countries/Statusofratifications/tabid/1072/language/en-US/Default.aspx
01/03/2012
Vienna Convention for the Protection of the Ozone Layer and its Montreal Protocol on Substances that Deplete the Ozone Layer
Accessionhttp://ozone.unep.org/new_site/en/treaty_ratification_status.php?treaty_id=&country_id=169&srchcrit=1&input=Display
Both on 03.11.1992
Stockholm Convention on Persistent Organic Pollutions (POPS), Stockholm
Accessionhttp://chm.pops.int/Countries/StatusofRatifications/tabid/252/Default.aspx
01/03/2012
Minamata Convention on Mercury (UNEP 2013)
Signaturehttp://www.mercuryconvention.org/Countries/tabid/3428/Default.aspx
11/10/2013

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe1212
4.2 national legal healthcare waste framework
The public Health act [chapter 15:09] of 1996 forms the basis for healthcare and environmental health services. The national Health policy forms the basis for this public act. to achieve the goals of the public Health act, an environmental health policy has been drafted but is so far not finalized.
The legal framework for HcW management is based on the environmental management act [chapter 20:27] of 2002. This act provides for the establishment of the national environmental council, the environmental management agency, the environment management board, the standards and enforcement committee and the environment fund; the formulation of environmental quality standards and environmental plans; environmental impact assessments, audit and monitoring of projects; and other matters related to management and conservation of the environment.
The act consists of 143 sections divided into 16 parts. The most relevant are:
{ environmental management agency (iV); { environment fund (Viii); { environmental Quality standards (iX); { environmental plans (X); { environmental impact assessments audit and
monitoring of projects (Xi);
a standards and enforcement committee is established as a committee of the board (sect. 55). The standards and enforcement committee shall, in consultation with the agency, advise the board on water quality standards in accordance with section 56. The committee shall also prescribe standards for air quality, waste, hazardous waste, pesticides and toxic substances, noise, and noxious smells. every pesticide or toxic substance shall be registered under section 76. The minister shall prepare a national environmental plan (sect. 87).
The environmental management agency (ema), which was established under this act, is a statutory body responsible for ensuring the sustainable management of natural resources and the protection of
the environment; the prevention of pollution and environmental degradation; and the preparation of national environmental plans for the management and protection of the environment (as requested in section X of the environmental management act).
ema’s environmental quality management unit has a mandate to enforce waste management regulations and implement and monitor waste management programmes. The agency promotes the participation of community-based organisations in solid waste management. ema issued several regulations relevant to waste management:
{ effluent and solid Waste disposal Regulations si 6, 2007 P This instrument regulates the disposal of waste
(solid waste and effluent), using the “polluter pays” principle.
{ Hazardous Waste management Regulations si 10, 2007
P This statutory instrument provides for the issuing of licenses for the generation, storage, use, recycling, treatment, transportation or disposal of hazardous waste for waste generators and waste handlers. Generators of hazardous waste are also required to prepare waste management plans and targets. This statutory instrument also regulates waste collection and management by local authorities. The importation and exportation of hazardous waste and waste soils is also regulated by this statutory instrument.
{ environmental and natural Resources management (hazardous substances, pesticides and other toxic substances) (amendment) Regulation, 2011(no2).
P amendment of the Hazardous substances, pesticides and toxic substances Regulations si 12, 2007.
{ air pollution control Regulations si 72, 2009 P The objective is to provide for prevention,
control and abatement of air pollution to ensure clean and healthy ambient air. it provides for the establishment of emission standards for various sources such as mobile sources (e.g. motor vehicles) and stationary sources (e.g. industries) as outlined in the air pollution control Regulations si 72, 2009.

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 13
LEgAL FrAmEwork
{ plastic packaging and plastic bottles Regulations si 98, 2010
{ importation and transit of Hazardous substances and Waste Regulations si 77, 2009
P The regulations place emphasis on waste minimization, cleaner production and segregation of waste at the source.
a special statutory instrument for HcW does not exist; however, a regulation has been drafted in the past. it is not known when this regulation will be finalized.
in 2011, the national Health care Waste management plan for Zimbabwe was prepared. among other issues, it addresses required equipment, training needs, monitoring and supervision. The plan is still under consideration and has not yet been implemented.
in 2012, the Zimbabwe Guidelines for disposal of expired and obsolete pharmaceutical supplies were issued by moHcW. The guidelines were adapted from WHo’s “Guidelines for safe disposal of unwanted pharmaceuticals in and after emergencies: interagency Guidelines”, Geneva 1999. it provides information on possible disposal methods and requests that, before destroying any expired medical supplies, approval must be sought from the appropriate authority, as outlined in the treasury instructions.
Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe1414
5.1 Input-output analysisbased on the psm plan, an input and output analysis for each of the three programmes on HiV/aids, tb and malaria was conducted.
5.1.1 ZIM-809-G11-H (HIV)Zimbabwe’s current national response to HiV is based on the Zimbabwe national aids strategic plan 2011–15. The plan was a product of a multi-stakeholder consultation process including government, civil society, the private sector, academia, faith groups, local communities, international agencies and development partners. The plan includes a number of detailed sub-components that relate to specific programming areas, such as antiretroviral therapy (aRt), pmtct and HiV testing.
The inputs of the Round 8, phase 2 HiV/aids grant consist of pharmaceuticals (about us$ 83 million), health products and commodities (about us$ 21 million) and non-health products and services (about us$ 3 million).
The pharmaceuticals consist mainly of aRV medicines such as zidovudine, lamivudine, efavirenz, nevirapine, abacavir, didanosine, stavudine, atazanavir, ritonavir, tenofovir, and fixed-dose combinations. The product selection is conducted by the national medicines and Therapeutics policy advisory committee that works through the moHcc’s directorate of pharmacy services.
The non-pharmaceutical products consist of HiV test kits (screening tests and confirmatory tests) and the corresponding consumables, cd4, haematology,
viral load and other test reagents, other medical consumables such as gloves, lancets and related sundries, etc.
The non-health products consist mainly of stationary materials, electronics and it equipment, as well as different print materials.
The expected waste output from the HiV/aids grant will be hazardous pharmaceutical waste (e.g. expired medicines) as well as non-hazardous pharmaceutical waste (e.g. packing materials, blister); infectious waste (e.g. blood contaminated swabs from testing procedures); sharp waste (e.g. used lancets); non-hazardous waste (from standard office operation); easily recyclable waste (e.g. packing and transportation materials such as cardboard boxes and pallets); and some more difficult to dispose of office waste such as old computers or cell phones (waste of electrical and electronic equipment – Weee).
5.1.2 ZIM-M-UNDP (Malaria) in the malaria grant, the input of pharmaceuticals (total about us$ 0.3 million) is low compared to the HiV/aids grant. Health products and commodities (about us$ 6.4 million) and health equipment (us$ 1.4 million) are the major inputs. input of non-health products and services are also low (about us$ 0.3 million).
The pharmaceuticals consist mainly of antimalarial medicines (artemether and lumefantrine). The non-pharmaceutical products consist of long lasting insecticidal nets (llins), pyrethroids4 and rapid diagnostic tests (Rdts) for malaria. The health equipment consists of Hudson sprayer pumps and protective clothing for the spraying of the insecticides.
5 Assessment of the Healthcare waste Situation
4 pyrethroids are synthetic chemical insecticides whose chemical structures are adapted from the chemical structures of the pyrethrins = botanical insecticides derived from chrysanthemum flowers. pyrethroids are less toxic than organophosphate pesticides, but runoff liquids from spraying may expose aquatic life to harmful levels in water and sediment.
Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 15
ASSESSmEnT oF THE HEALTHCArE wASTE SITuATIon
The non-health products consist mainly of stationary materials as well as different printing materials. ddt pesticide will be used as flow over from 2013 activities.
The expected output from the malaria grant will be mainly non-hazardous pharmaceutical waste (artemisinin-based combination therapies are normally considered as non-hazardous) and some amounts of hazardous pharmaceutical waste. The main problematic waste streams will be chemical waste, which will include used packing materials of llins, old and damaged llins, residues from ddt and pyrethroids spraying including liquid waste (left overs, spillages) and solid waste (empty packaging, damaged packages).
5.1.3 ZIM-809-G12-T (Tuberculosis) inputs consist of pharmaceuticals (total about us$ 7 million), health products and commodities (about us$ 1 million), health equipment (about us$ 1 million) and non-health products and services (about us$ 1 million).
The pharmaceuticals mainly consist of anti-tb medicines such as ethambutol, streptomycin, isoniazid, pyrazinamide, rifampicin, kanamycin, levofloxacin and others. The non-pharmaceutical health products mainly include kits and reagents of different laboratory tests and other consumables for tb tests. The health equipment consists of mobile digital x-ray units, refrigerators and audiometry machines. The non-health products consist mainly of stationary materials, electronics and it equipment and different print materials.
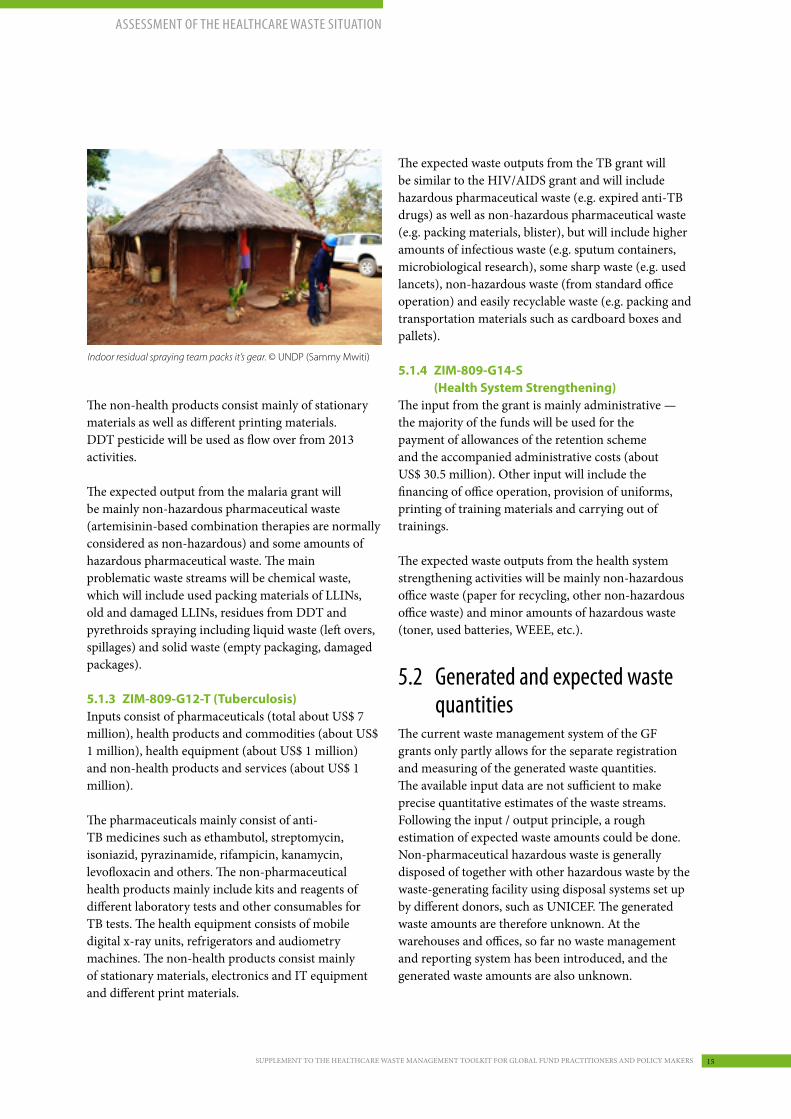
Indoor residual spraying team packs it’s gear. © UNDP (Sammy Mwiti)
The expected waste outputs from the tb grant will be similar to the HiV/aids grant and will include hazardous pharmaceutical waste (e.g. expired anti-tb drugs) as well as non-hazardous pharmaceutical waste (e.g. packing materials, blister), but will include higher amounts of infectious waste (e.g. sputum containers, microbiological research), some sharp waste (e.g. used lancets), non-hazardous waste (from standard office operation) and easily recyclable waste (e.g. packing and transportation materials such as cardboard boxes and pallets).
5.1.4 ZIM-809-G14-S (Health System Strengthening)
The input from the grant is mainly administrative — the majority of the funds will be used for the payment of allowances of the retention scheme and the accompanied administrative costs (about us$ 30.5 million). other input will include the financing of office operation, provision of uniforms, printing of training materials and carrying out of trainings.
The expected waste outputs from the health system strengthening activities will be mainly non-hazardous office waste (paper for recycling, other non-hazardous office waste) and minor amounts of hazardous waste (toner, used batteries, Weee, etc.).
5.2 generated and expected waste quantities
The current waste management system of the Gf grants only partly allows for the separate registration and measuring of the generated waste quantities. The available input data are not sufficient to make precise quantitative estimates of the waste streams. following the input / output principle, a rough estimation of expected waste amounts could be done. non-pharmaceutical hazardous waste is generally disposed of together with other hazardous waste by the waste-generating facility using disposal systems set up by different donors, such as unicef. The generated waste amounts are therefore unknown. at the warehouses and offices, so far no waste management and reporting system has been introduced, and the generated waste amounts are also unknown.

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe1616
for pharmaceutical waste, it is expected that, on average, 2 to 5 % of the purchased medicines will become waste due to transportation and storage accidents, expiration or other circumstances.
5.3 Current waste management procedures within the gF programme
The different Gf grant programmes in Zimbabwe are in the process of introducing improved waste management procedures. during the design and planning of the programmes, no specific environmental safeguarding policies were followed, or even requested, by the Gf. The Gf itself does not have an environmental safeguarding policy, and interventions ensuring the adequate management of waste generated through the Gf grants are not systematically reviewed by the technical Review panel of the Gf, and are also not mandatory for grant approval. Within the programmes, generated waste was planned to be disposed of using the existing disposal structure. The implementation of monitoring instruments and procedures was planned at a later stage. separate waste collection processes for the grants were not included. for waste management operations, only limited amounts of consumables and equipment were included in the on-going grants, mainly consisting of sharp containers, bins and plastic liners, and some coverage of disposal costs.
The only exemption was the disposal of waste contaminated with ddt. Here, special disposal arrangements were made with a contractor, which included the provision of suitable plastic drums for temporary storage of ddt liquid waste, as well as adequate plastic sheeting to be used in the field to prevent environmental contamination during the cleansing of sprayers. The supplier was required to provide disposable bags which were to be used for temporary storage of ddt solid waste before incineration; the supplier was requested to organize the incineration. monitoring of this contracted procedure has so far not been carried out.
5 http://documents.worldbank.org/curated/en/2011/04/14256625/zimbabwe-health-results-based-financing-project-environmental-assessment-vol-1-2-action-plan
Upper: Destruction of healthcare waste in brick-made incinerator. Lower: Waste workers with PPE. ©UNDP (Sammy Mwiti)
for the near future, there is a plan to set up two centralized waste incinerator systems for the safe disposal and treatment of hazardous pharmaceutical waste. These incinerator systems will be located at the premises of the national pharmaceutical company of Zimbabwe (natpharm) and will most likely be operated by natpharm. management systems for the waste from warehouses and office operations do so far not exist. for the disposal of Weee, the locally present system is used; however, it is limited and mainly consists of a basic collection and informal recycling sector. cooperation for the disposal of waste is arranged with some other donors. The existent HcW management plan, which was set up within the “Health Results based financing project”5 , has so far not been included in the long-term planning process of the Gf programme in Zimbabwe.

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 17
ASSESSmEnT oF THE HEALTHCArE wASTE SITuATIon
5.4 Current healthcare waste disposal practices in Zimbabwe
The management of HcW in Zimbabwe faces several challenges that require urgent attention. on april 26th, 2014, the Zimbabwe mail reported: “almost all of the incinerators at both the public and private clinics, hospitals, uniformed forces institutions and other medical institutions are reportedly dysfunctional. some institutions do not have the facility completely.”
This situation was unearthed at a national meeting held in Harare. senior medical officials drawn from all over the country noted with concern how the population was exposed to environmental hazards and how difficult it has become to contain public uproar and accusations of poor HcW management and lack of responsibility.6 according to WHo, over 90 % of health institutions in Zimbabwe have a waste crisis and action is urgently required, including waste reduction and recycling options.
in 2011, the national HcW management plan was developed. an earlier assessment7 showed that:
{ training in HcW management was lacking at all levels of health services.
{ segregation of HcW was generally good at bigger institutions.
{ colour coding is critical in the proper handling of HcW waste, and this was found to be lacking except at one big private institution.
{ storage areas were provided at big and medium institutions but there was inadequate security resulting in dogs, donkeys, children and vultures accessing untreated HcW.
{ inappropriate transport arrangements for waste disposal were observed at medium and small institutions.
{ lack of functional incinerators at all public big, medium and small institutions compromises the proper treatment of HcW.
{ Reasons for the non-functionality of the incinerators ranged from the lack of availability of fuel, wrong technical specifications, the lack of funding, improper management and poor supervision.
The HcW management plan highlights that most waste treatment facilities are not efficiently operating; that the HcW management system has not been institutionalised and is rather informal; that the private sector is generally not involved in the HcW management area; and re-confirms that action is urgently need to bring the HcW management crisis under control.
typical healthcare practices currently applied include:
{ Waste segregation: in most healthcare facilities, separation of sharps and other waste takes place. also, in some facilities, the remaining waste is separated into infectious and non-infectious waste. a further segregation into pharmaceutical waste, chemical waste and other waste streams does not take place.
{ temporary storage: Waste storage facilities are limited and, if existent, often unsecured and of low quality.
{ Waste treatment and disposal: While non-hazardous waste is typically landfilled or burnt in open pits, infectious waste is partly incinerated (if incineration facilities exist), or is disposed of in lined pits.
based on the existing information, the HcW management system in Zimbabwe is in early stages of development and clearly needs further improvement. key stakeholders are aware of the problem. Workshops and meetings are held to address the challenges, and the public is sensitized by the media.
6 http://www.thezimmail.co.zw/2014/04/26/countrys-incinerators-defunct/7 G.t mangwadu – Rapid assessment of HcWm (2007), environmental Health services moHcW

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe1818
6.1 recommendations, generally applicable to all gF-financed health programmes
a) Integrate and harmonize HCW management activities
Current situation: The undp as pR recognizes the importance of the safe and correct disposal of waste materials generated during the execution of the Gf grants, and plans different measures to reduce possible impacts.
Justification/impact: following the “polluter pays” principle, the Gf grants, with the undp as the pR, have certain responsibilities to ensure that waste generated during the execution of the grants is managed under consideration of national and international environmental laws, regulations and guidelines.
Recommended activities: include interventions with adequate budgets in Gf grants, which will ensure quality HcW management for waste produced under the Gf programmes following national and international laws, regulations, and standard guidelines. environmental safeguard policies of the Gf, pRs and sRs should be introduced or reviewed to be fit for purpose. HcW management should be included in Hss components of the grants as required in order to address structural and procedural deficits of national HcW management systems together with other development partners under the lead of the moHcW. The establishment of a national HcW management working group is recommended.
b) Use quality assurance/quality control (QA/QC) funds to solve environmental problems
Current situation: Qa/Qc is the combination of quality assurance (the process to measure and assure the quality of a provided service) and quality control (the process of meeting products and services to client expectation). a general expectation of Gf grants is not to harm the public and the environment. based on this, funds of the Qa/Qc are planned to be used in Zimbabwe to finance the establishment of central pharmaceutical waste destruction centres. The safe destruction of unwanted or expired pharmaceuticals will benefit the public as well as the environment. in the malaria grant, the estimated budget needed for Qa/Qc is 2 % (for acts) and 8 % (for pyrethroids) of the cost of the goods (total about us$ 0.2 million for the entire grant). The Qa/Qc funds will only partly be used for waste activities.
Justification/impact: Without financial support, the establishment and operation of new HcW infrastructure will not be possible. The usage of the funds will solve the problem of expired or unwanted pharmaceuticals in Zimbabwe. if resources are missing or if disposal possibilities are missing, this might result in the inadequate, unsafe and environmentally risky disposal of this waste.
Recommended activities: use Qa/Qc funds to improve environmental safeguarding standards as an innovative strategy. a budget increase for Qa/Qc may be required.
c) Include disposable products for waste collection (waste bags, sharp containers, etc.)
Current situation: in the projects, often only limited amounts of sharp containers for the collection of syringes and for the collection of infectious waste (e.g.
6 Findings & recommendations

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 19
FIndIngS & rECommEndATIonS
strong yellow bags) or household waste (e.g. black bags) are supplied.
Justification/impact: as bags are missing, infectious waste, such as used swabs, is either disposed of in sharp containers, or in self-procured bags which sometimes do not fulfil quality requirements, or is collected without bags. This results in a faster filling of sharp containers, and in hygiene risks during waste collection.
Recommended activities: include a supply of waste bags in sufficient quantities for infectious waste and normal waste in Gf health programmes.
d) Strengthen cooperation with the private sector, and include budgets for the disposal of waste, allowing outsourcing from the public sector
Current situation: public systems for the disposal of hazardous and non-hazardous waste do not exist in all regions. Waste producers such as healthcare facilities often depend on private entities or persons to pick up and dispose of generated waste.
Justification/impact: Without an existing budget, waste disposal services cannot be outsourced and public sector waste producers may have problems with disposing of waste in a safe manner.
Recommended activities: include a budget for the outsourcing of waste disposal as needed.
e) Develop warehouse waste management plansCurrent situation: Waste management plans for warehouses, including practical and safety instructions (such as spillage plans, etc.), do not exist.
Justification/impact: Warehouses create large amount of packing waste (e.g. transport packing, etc.) which should be adequately managed. stored materials include hazardous and non-hazardous materials, and procedures should be available for expired and/or damaged materials, waste from spillages, etc.
Recommended activities: ensure the development and implementation of waste management plans for the operation of warehouses.
f) Strengthen recycling and the reuse of waste at warehouses
Current situation: systems to collect, reuse or recycle waste at warehouses are not officially implemented.
Justification/impact: Warehouses create large amounts of waste which can be recycled, including cardboard and plastics.
Recommended activities: establish at least a basic recycling programme at all warehouses and report the amount and types of recycled materials.
g) Develop a waste management plan for office operation, including car maintenance
Current situation: The programme offices do not have a waste management system. all generated waste is disposed of via the normal household waste system.
Justification/impact: The operation of the offices creates waste which could be recycled (e.g. paper waste, etc.) but also waste with potential environmental impact such as used oil from car maintenance, or old or damaged electrical or electronic equipment, including batteries (Weee).
Recommended activities: introduce basic standard operating procedures (sops) for the environmentally friendly operation of project offices.
Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe2020
6.2 recommendations for the gF programme addressing the country-specific context in Zimbabwe
a) Develop a system for the collection and disposal of LLINs and LLINs packing materials
Current situation: one of the key methods to prevent malaria used in the Gf grant projects is the distribution of llins. llins, which have an estimated lifespan of three to five years or twenty washes, have an average weight of about 0.5 kg per piece.
Justification/impact: the distribution of llins generates two waste streams. during distribution, packing materials become waste. as the primary packing material was in contact with the pesticides, these bags are classified as “empty pesticide containers” and require special treatment. at the end of their lifespan, the old nets have to be disposed of. they consist of three materials: net, insecticide and the binding process. as the remaining insecticides are typically toxic for aquatic life, it is recommended to collect and dispose of the nets in a safe way after usage.
Recommended activities: support the establishment of a moHcW-coordinated nationwide system for the collection of primary packing materials of llins and used llins in cooperation with other stakeholders. assess whether local recycling of the primary packing is feasible.
b) Develop a system for the collection and disposal of hazardous waste generated during indoor residual spraying
Current situation: indoor residual spraying is the process of spraying the inside of dwellings with an insecticide to kill mosquitoes that spread malaria. While some ddt is still used in the Gf grant projects, new procurement will concentrate on pyrethroids. both are considered as moderately hazardous substances.
Justification/impact: during the preparations and the application of indoor residual spraying, waste such as contaminated packing materials,
packages broken during transport, contaminated personal protection equipment, spillages, etc. will be generated. a system should be in place to ensure the safe disposal of the generated hazardous waste.
Recommended activities: develop a disposal strategy addressing the collection and disposal of hazardous waste from indoor residual spraying during all process steps – from storage, to distribution, to the final usage of the insecticides.
c) Ensure the safe disposal of potentially infectious healthcare waste, especially sharp waste
Current situation: all Gf grants will produce HcW during the testing as well as the treatment of patients. of particular relevance to risk control and occupational health are sharp items, such as used needles and lancets. currently, this waste is disposed by using collection means supplied from other projects and donors (e.g. unicef).
Justification/impact: the safe disposal of hazardous infectious waste depends on factors currently out of the control of the Gf grant projects. external changes such as the stop of certain projects might result in the future unsafe disposal of waste.
Recommended activities: provide Gf health service providers under the Gf programmes with sufficient funds to enable them to set up solutions for the collection and disposal of infectious waste.
d) Integrate the planned disposal system for pharmaceutical waste
Current situation: there is a plan to establish disposal facilities for the destruction of pharmaceutical waste.
Justification/impact: previous projects showed that disposal facilities are often not operating successfully and/or are under-utilised. problems exist especially with the reverse logistic system of pharmaceutical waste and in the financing of running costs.
Recommended activities: consider the operation of the system by private operators under defined and well-monitored quality standards, and allow and support the destruction of other hazardous materials in the same disposal facilities as appropriate.

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 21
AnnExES
7.1 Input analysisHIV/AIDS grant:
A) Pharmaceutical product
7 Annexes
Type of antiretroviral medicines Strength
Zidovudine 300mg tabs/PAC-60 300 mg
Lamivudine 150mg + Zidovudine 300mg tab/PAC-60 150 mg + 300 mg
Efavirenz 600mg + Lamivudine 300mg + Tenofovir 300mg tabs/PAC-30 600 mg + 300mg+300 mg
Abacavir 300mg tabs/PAC-60 300 mg
Didanosine 250mg EC caps/PAC-30 250 mg
Didanosine 400mg EC caps/PAC-30 400 mg
Efavirenz 600mg tabs/PAC-30 600 mg
Lamivudine 150mg + Stavudine 30mg tab/PAC-60 150 mg + 30 mg
Lamivudine 150mg + Nevirapine 200mg + Stavudine 30mg tab/PAC-60 150 mg + 200 mg + 30 mg
Lamivudine 150mg + Nevirapine 200mg + Zidovudine 300mg tab/PAC-60 150 mg + 200 mg + 300 mg
Lopinavir 200mg + Ritonavir 50mg tab/PAC-120 200 mg + 50 mg
Tenofovir/Lamivudine + Nevirapine 300+300+200mg tab/3X10 blister pack 300 mg + 300+200 mg
Tenofovir 300mg + Lamuvidine 300mg tab/PAC-30 300 mg + 300 mg
Nevirapine 200mg tab/PAC-60 200mg
Atazanavir/Ritonavir 300/100mg tab/PAC-30 300 mg + 100 mg
Isoniazid 100 mg tablets, breakable pack of 10 strips of 10 blistered tablets 100 mg
Pyridoxine 25mg tab/Tin-100 25 mg

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe2222
B) Non-pharmaceutical health products
Rapid diagnostic kits HIV Test Kit - Screening Test
HIV Test Kit - Confirming Test
Consumables for Confirming Test
All other health products Medical consumable units (comprising gloves, lancets and related sundries)
All other diagnostic products, supplies and equipment
CD4 reagents for new patients & patients continuing on ART (5 or 10 % wastage) + Service & maintenance of CD4 machines procured under GF 1, 5 and 8
Haematology reagents for new pts & those continuing ART + service & maintenance of haematology machines procured under GF 1, 5 and 8
Clinical chemistry reagents + service & maintenance of chemistry machines procured under GF 1, 5 and 8
viral load reagents (consider providing VL tests to at least 50 % of pts on ART, twice a year)
Reagents for coagulation studies for Parirenyatwa and Mpilo hospitals + service & maintenance of existing coagulation machines
HIV DNA PCR reagent kits for PMTCT settings at the comprehensive sites + service & maintenance of existing PCR machines not under warranty
Service & maintenance of existing gene sequencing machines not under warranty procured under GF 1, 5 and 8
Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 23
AnnExES
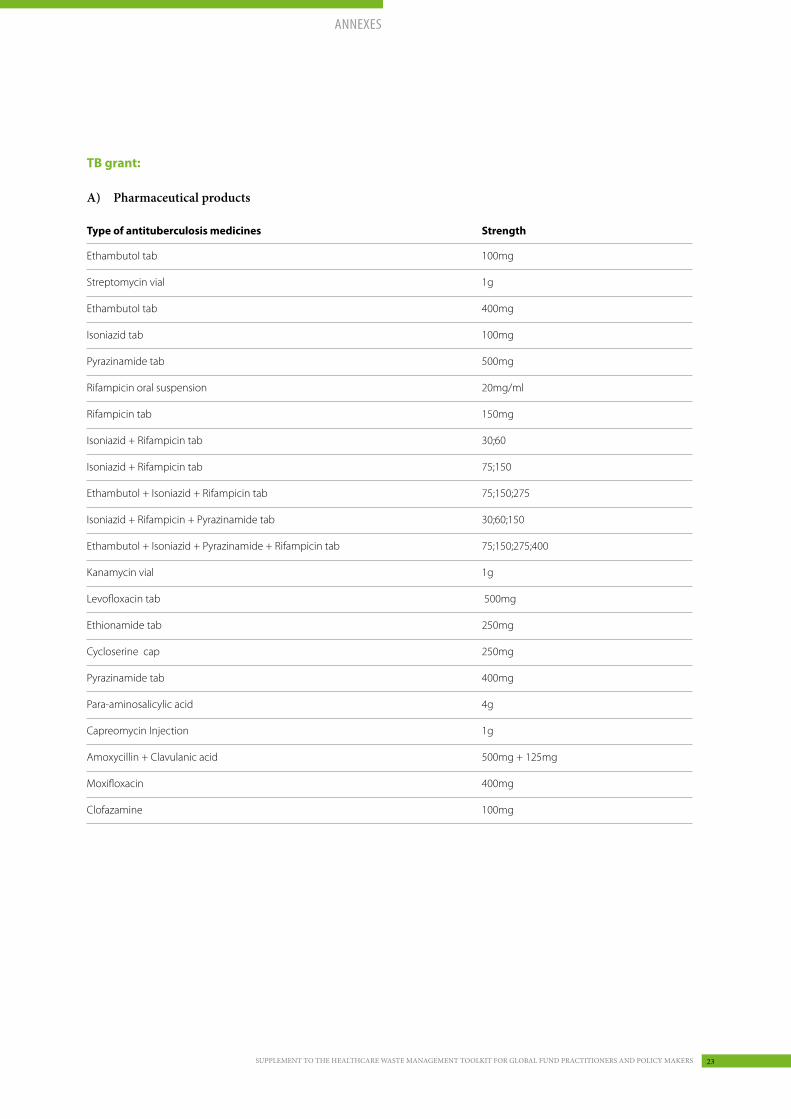
TB grant:
A) Pharmaceutical products
Type of antituberculosis medicines Strength
Ethambutol tab 100mg
Streptomycin vial 1g
Ethambutol tab 400mg
Isoniazid tab 100mg
Pyrazinamide tab 500mg
Rifampicin oral suspension 20mg/ml
Rifampicin tab 150mg
Isoniazid + Rifampicin tab 30;60
Isoniazid + Rifampicin tab 75;150
Ethambutol + Isoniazid + Rifampicin tab 75;150;275
Isoniazid + Rifampicin + Pyrazinamide tab 30;60;150
Ethambutol + Isoniazid + Pyrazinamide + Rifampicin tab 75;150;275;400
Kanamycin vial 1g
Levofloxacin tab 500mg
Ethionamide tab 250mg
Cycloserine cap 250mg
Pyrazinamide tab 400mg
Para-aminosalicylic acid 4g
Capreomycin Injection 1g
Amoxycillin + Clavulanic acid 500mg + 125mg
Moxifloxacin 400mg
Clofazamine 100mg

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe2424
B) Non-pharmaceutical health products
Health products and commodities
GDF consumables kits (1000 tests per kit)
GDF sputum container kits (1000 containers per kit)
Reagents for auramine staining (kit)
MGIT lab reagents
MTBDRplus kits for Hain equipment for 2nd line drugs
GenoType® MTBDRsl kits for Hain equipment for 1st line drugs
GenoType® mycobacterium CM/AS kits for Hain equipment for 2nd line drugs
Powdered latex gloves, box of 100
HIV Elisa test kits
Microlitre plates, pack for 1000 tests
CryoTubes™, pack for 1000 tests
PBS, 1 litre
Tips 200µl
Laboratory disinfectants, 20 l bottle
Calibration and maintenance contracts for 50 x Gene Xpert machines
Additional Consumables to Support TB Prevalence Survey (details TB Prevalence Survey Worksheet)
Xpert MTB/RIF test cartridges for the TB DRS
BD Falcon™ Conical Tubes 50 mL, flat-top screw cap, rack included, Box of 500 tubes for the TB DRS
Ice packs for medical carrier boxes for the TB DRS
Personal protective devices (PPD)/respirators (N95 masks) for staff in MDR wards
Traditional molded and foldable type NIOSH N95 masks/respirators (in equal split of quantity)
Universal bottles for LJ slopes for the TB DRS, 144 bottles/box
Cetylpyridinium chloride (CPC) 500g per bottle for the TB Drug resistance
Centrifuge adapter for 50 mL Falcon tubes for the TB Drug resistance

Supplement to the healthcare WaSte management toolkit for global fund practitionerS and policy makerS 25
AnnExES
C) Non-health products and services
Health equipment BD BACTECTM MGITTM 960 System including accessories and support
Ultralow temperature freezer
Refrigerator (laboratory general purpose)
Double Heating Block 200 deg C
Hain GenoType® MTBDRplus set (for rapid molecular diagnostic for MDR-TB laboratory) for NMRL
Mobile fitted digital x-ray vehicles
Central archive for the Mobile fitted digital x-ray vehicles
Portable x-ray unit for survey back-up
Bench-top micro centrifuge + angle rotor 24-place
Audiometry machine
Hearing aids for patients
Fit test machine
Fit testing equipment
Equipments and commodities
Vehicles to support field work
9kvA diesel generators 3 phase
Motorcycles for 10 provinces for enable monitoring and coordination of TB activities
Personal Digital Assistants
Cell phones and chargers
Internet dongles
Laptops for data entry, analysis and transmission
Network Printer
Laboratory log books
Services Printing of TB DRS Protocol data collection forms
Printing (SOPs, guidelines, etc.)
Service and maintenance contracts for different machines and equipment

Rapid assessment: HealtHcaRe Waste component of Global fund HiV, tb and malaRia pRojects in ZimbabWe2626
Organization Name Title
MOHCW Dr. Celestino Basera GF Grants Coordinator
MOHCW Forward Mudzimu Deputy Director Pharmacy, Logistics & Research
MOHCC Victor Nyamandi
MOHCW Stanford Mashaire National Malaria Control Program
MOHCW Goldberg Mangwadu Environmental Health Department
UNDP Guy Rino Meyers Advisor, GF Partnership
UNDP Elliman Jagne Operations Manager
UNDP Sifiso Moyo Procurement and Supplies Management (PSM) Manager
UNDP Adam Valois PSM Consultant
UNDP John Macauley Regional Programme Specialist
ETLog Jan-Gerd Kühling Environmental Consultant
Malaria grant:
A) Pharmaceutical product
B) Non-pharmaceutical health products
7.2 Participants in the stakeholder interviews
Type of medicines Strength
Artemether + Lumefantrine 20mg+120mg
Rapid diagnostic kits Malaria Ag Pf/Pan Point Of Care Test Kit
Paracheck Pf Rapid Test device
First Response Malaria Ag Combo Test Kit
Indoor residual spraying chemicals
Pyrethroids
DDT 75% WP
Vector Control Insecticide susceptibility monitoring
Bioassay kits
Hudson sprayer pumps and spare parts
Personal protective equipment and clothing
LLINs

Empowered lives. Resilient nations.