radiological presentation of pulmonary pathology
TRANSCRIPT

Gamal Rabie Agmy MD FCCP
Professor of Chest Diseases Assiut University
Types of Collapse
6-Compression Atelectasis
Flat waist Sign
This sign refers to flattening of the contours of the aortic knob and adjacent
main pulmonary artery
It is seen in severe collapse of the left lower lobe and is caused by leftward
displacement and rotation of the heart
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Types of Collapse
6-Compression Atelectasis
Flat waist Sign
This sign refers to flattening of the contours of the aortic knob and adjacent
main pulmonary artery
It is seen in severe collapse of the left lower lobe and is caused by leftward
displacement and rotation of the heart
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Flat waist Sign
This sign refers to flattening of the contours of the aortic knob and adjacent
main pulmonary artery
It is seen in severe collapse of the left lower lobe and is caused by leftward
displacement and rotation of the heart
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Comet Tail Sign
bullSeen on CT of the chest
bullConsists of curvilinear opacity extending
from subpleural mass toward hilum
bullProduced by the distortion vessels and
bronchi that lead to adjacent rounded
atelectasis
(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

(posterioranterior) position Note
that the x-ray tube is 72 inches away
the supine AP (anteriorposterior)
position the x-ray tube is 40 inches
from the patient
Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Dee method for approximating the position o f the carina can
be used This involves defining the aortic arch and then drawing a line Inferomedially through the middle of the arch
at a 45 degree angle to t he midline
The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

The Ideal position for endotracheal tubes is in the
mid trachea 5cm from the carina when the head is
neither flexed nor extended This allows for
movement of the tip with head movements The
minimal safe distance from the carina is 2cm
Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Notice the increased lucency of the cardiophrenic sulci in this patient
with inferior anteromedial pneumothoraces A CT scan confirms the
diagnosis
a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

a hyperlucent upper
quadrant with
visualization of the
superior surface of the
diaphragm and
visualization of the
inferiorvena cava
double-diaphragm
sign
Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Antero lateral air may
increase the
radiolucency at the
costo phrenicsulcus
This is called the deep
sulcus sign
Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Apicolateral
pneumothorax
(arrows) with right upper lobe collapse
(arrowheads)
shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

shifting of the heart
border
the superior vena cava
and the inferior vena
cava
The shifting of these
structures can lead to
decreased venous return
bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

bullMediastinal shifT is
usually
seen in a tension
pneumothorax
bullThe most reliable sign of
tension pneumothorax is
depression of a
hemidiaphragm
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Nodular Patternitie
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)
Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Nodular Pattern
Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Perilymphatic distribution
Centrilobular distribution
Random distribution
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Size Distribution Appearance
Nodules and Nodular Opacities
Size
Small Nodules lt10 mm Miliary - lt3 mm
Large Nodules gt10 mm Masses - gt3 cms
Appearance
Interstitial opacity
Well-defined homogenous
Soft-tissue density
Obscures the edges of vessels or adjacent structure
Air space
Ill-defined inhomogeneous
Less dense than adjacent vessel ndash GGO
small nodule is difficult to identify
Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Interstitial
nodules Air space opacity
Miliary tuberculosis
sarcoidosis
in a lung transplant patient
with bronchopneumonia
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
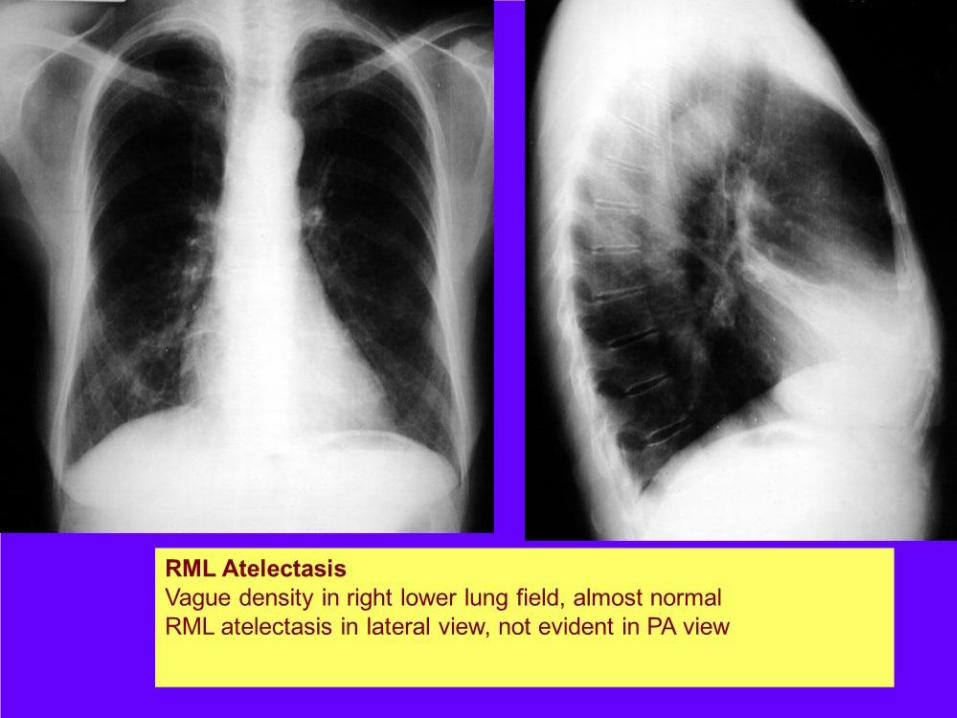
RANDOM no consistent relationship to any structures
PERILYMPHATIC corresponds to distribution of lymphatics
CENTRILOBULAR related to centrilobular structures Distribution
75
Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Disseminated histoplasmosis and nodular ILD
CT scan shows multiple bilateral round circumscribed
pulmonary nodules
Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Notice the nodules along the fissures indicating a
perilymphatic distribution (red arrows)
The majority of nodules located along the bronchovascular
bundle (yellow arrow)
Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Sarcoidosis
The majority of nodules located
along the bronchovascular bundle
(yellow arrow)
PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

PERILYMPHATIC NODULES
Perilymphatic and Random distribution of
nodules seen in sarcoidosis
Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Centrilobular distribution
Hypersensitivity pneumonitis
Respiratory bronchiolitis in
smokers
infectious airways diseases
(endobronchial spread of
tuberculosis or
nontuberculous
mycobacteria
bronchopneumonia)
Uncommon in
bronchioloalveolar
carcinoma pulmonary
edema vasculitis
Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Random distribution
Small random nodules
are seen in
Hematogenous
metastases
Miliary tuberculosis
Miliary fungal infections
Sarcoidosis may mimick
this pattern when very
extensive
Langerhans cell
histiocytosis (early
nodular stage)
Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans cell histiocytosis early nodular stage before the typical cysts appear
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Cystic Lung Lesions
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Basal and subpleural distribution
UIP
Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Inconsistent with UIP pattern (any one of seven features
Possible UIP pattern (all three features)
UIP pattern (all four features)
bullUpper or mid lung
predominance subpleural basal
predominance
bullsubpleural basal
predominance
bullperibronchovascular
predominance reticular abnormality bullreticular abnormality
bullextensive ground glass
abnormality (extent gt reticular
abnormality)
bullhoneycombing with or
without traction
bronchiectasis
bullprofuse micronodules
(bilateral predominantly upper
lobes
Absence of features
listed as inconsistent
with UIP pattern
Absence of features
listed as inconsistent
with UIP pattern
bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic attenuationair
trapping (bilateral in three or
more lobes)
bullconsolidation in broncho-
pulmonary segment(s)lobe(s)
Radiological features of idiopathic pulmonary fibrosis 2011
Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Lymphangioleiomyomatosis (LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarkoidosis Silikosis
Only cysts idiopathic Fibrosis
LAM
Destruktive emphysema
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
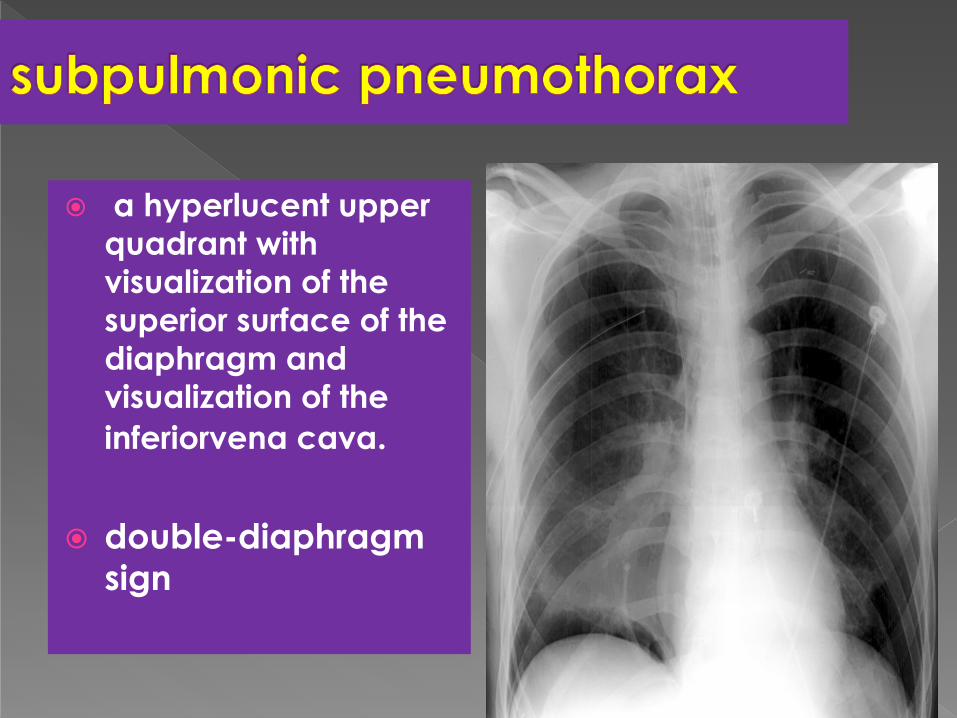
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgrenrsquos syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemeanrsquos disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Wegenerlsquos disease
Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Rheumatoid Arthritis
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
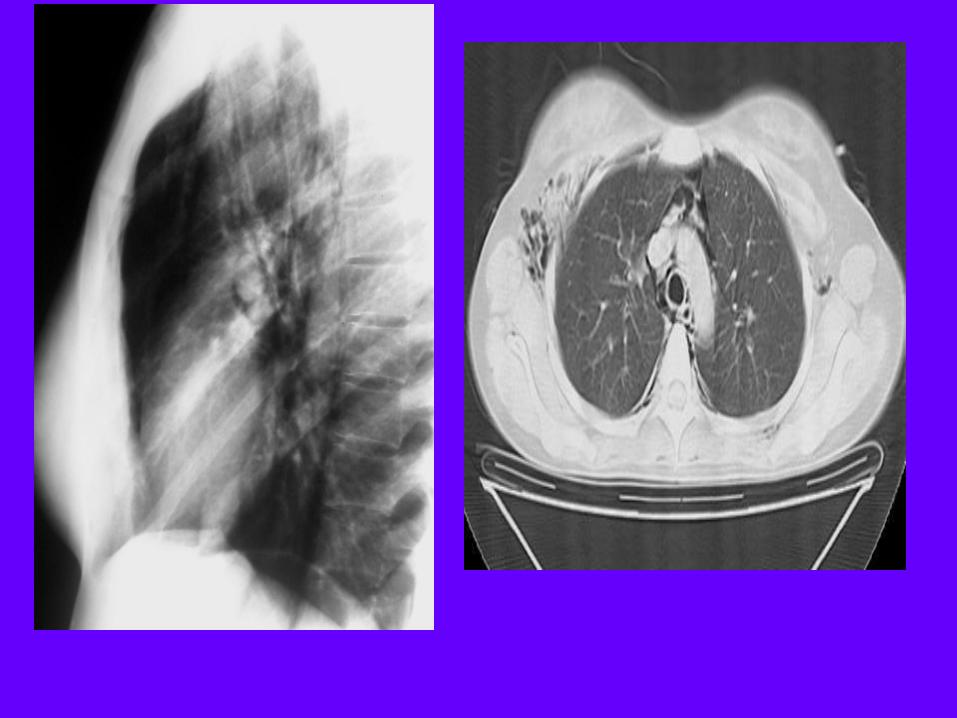
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Distribution within the lung
Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular Pattern
Gamal Rabie Agmy MD FCCP
Professor of chest Diseases
Assiut university
Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Linear Pattern A linear pattern is seen when there is
thickening of the interlobular septa
producing Kerley lines
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics
The most common cause of interlobular
septal thickening producing Kerley A
and B lines is pulmonary edema as a
result of pulmonary venous
hypertension and distension of the
lymphatics Kerley B lines
Kerley A lines
DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

DD of Kerly Lines
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis
HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

HRCT of the lung
Reticular pattern ndash HRCT
numerous clearly visible interlobular septa outlining lobules of characteristic size and shape
interlobular septal thickening
very fine network of lines within visible lobules
intralobular interstitial thickening
several layers of air-filled cysts 3-10 mm in diameter with thick walls (1-3 mm)
honeycombing
Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
Interlobular septal thickening ndash dd
smooth thickening
pulm edema pulm hemorrhage lymphangitic carc lymphoma
nodular thickening
lymphangitic carc sarcoidosis amyloidosis
irregular thickening
fibrosis
Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
Interlobular septal thickening ndash pulmonary edema
smooth septal thickening isolated or in combination with ground-glass opacity
peribronchovascular and subpleural interstitial th
perihilar and gravitational distribution bilateral findings of CHF
Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
Interlobular septal th ndash lymphangitic carcinomatosis
smooth or nodular septal thickening smooth or nodular thickening of peribronchovascular
interstitium and fissures thickening of the intralobular axial interstitium
focal or asymmetric distribution
Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticulation or not reticulation helliphellip
ldquocrazy pavingrdquo
Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
Honeycombing ndash significance
air-containing cystic spaces having thick fibrous walls lined by bronchiolar epithelium
fibrosis is present
UIP is likely the histologic pattern
IPF is very likely in the absence of a known disease
Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
Honeycombing ndash differential diagnosis
basal distribution
middleupper distribution
chronic HP sarcoidosis
IPF collagen vasc dis asbestosis drugs
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
interlobular septal thickening
irregular lung distorsion
nodular smooth
bull fibrosis (sarcoidosis asbestosis)
bull pulm edema bull linf carc bull hemorrhage
bull sarcoidosis bull linf carc
Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Reticular pattern
adapted from Webb RW ndash HRCT of the lung III ed 2001
honeycombing
bull IPF (60) bull collagen vascular dis bull drug reaction bull asbestosis (uncommon)
subpleural posterior LL predominance
bull sarcoidosis bull chronic HP bull radiation
other distribution (UL parahilar)
Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Head cheese sign
It refers to mixed
densities which includes
consolidation
ground glass
opacities
normal lung
Mosaic perfusion
bull Signifies mixed
infiltrative and
obstructive disease
Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Head cheese sign
Common cause are
1 Hypersensitive pneumonitis
2 Sarcoidosis
3 DIP
127
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
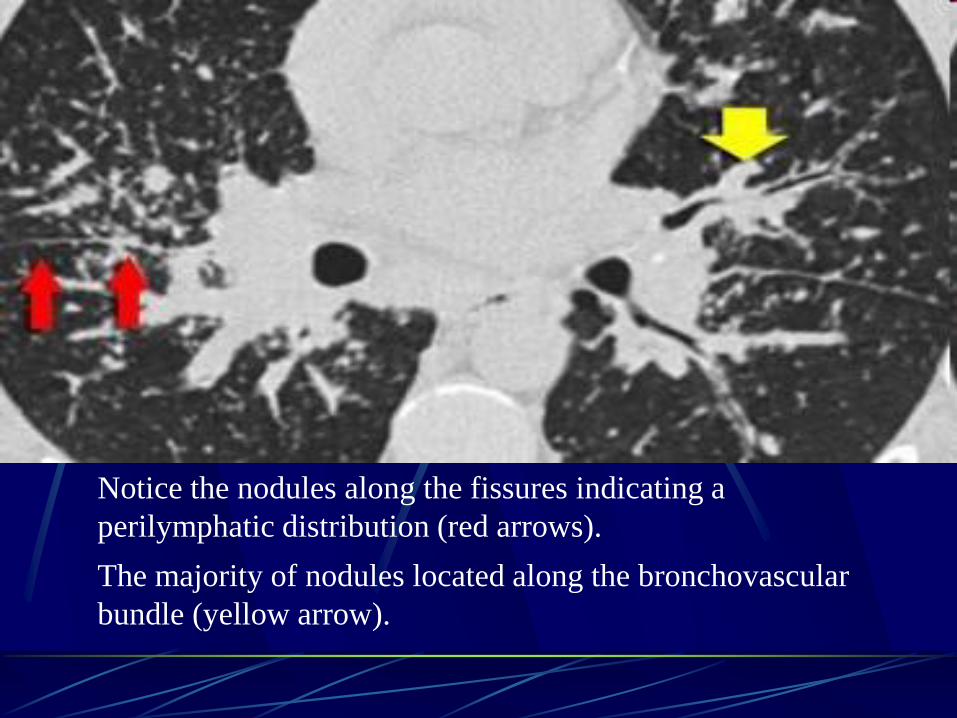
Headcheese sign
Headcheese sign in
hypersensitivity
pneumonitis
HRCT scan shows lung with
a geographic appearance
which represents a
combination of patchy or
lobular ground-glass opacity
(small arrows) and mosaic
perfusion (large arrows)
Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Mosaic Patternitie
By
Gamal Rabie Agmy MD FCCP Professor of Chest Diseases Assiut University
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
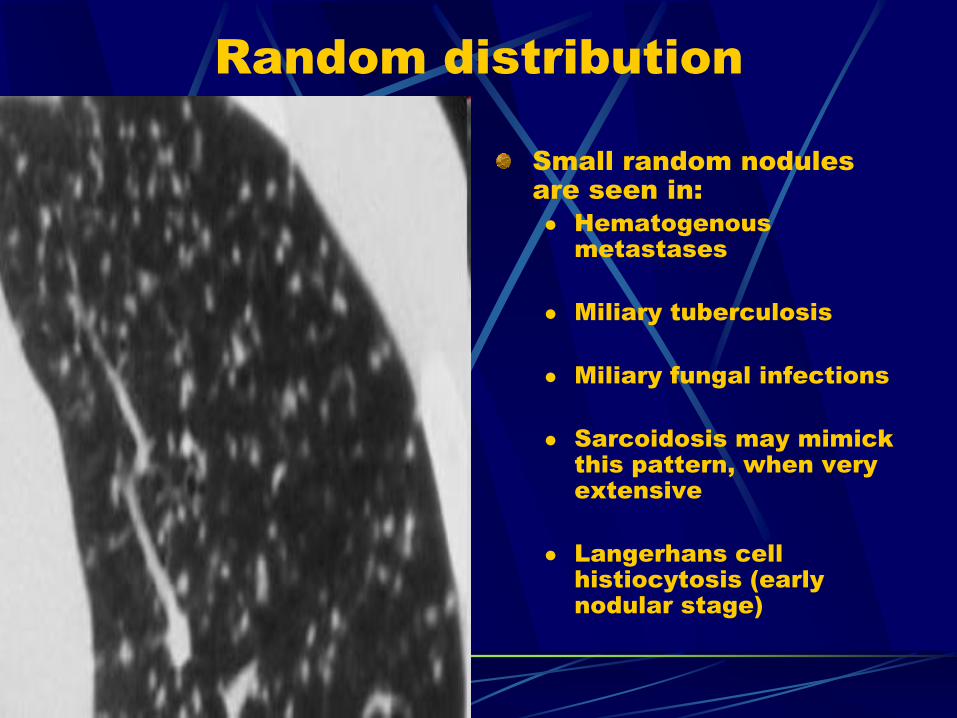
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Bronchiolitis
obliterans
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension

Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
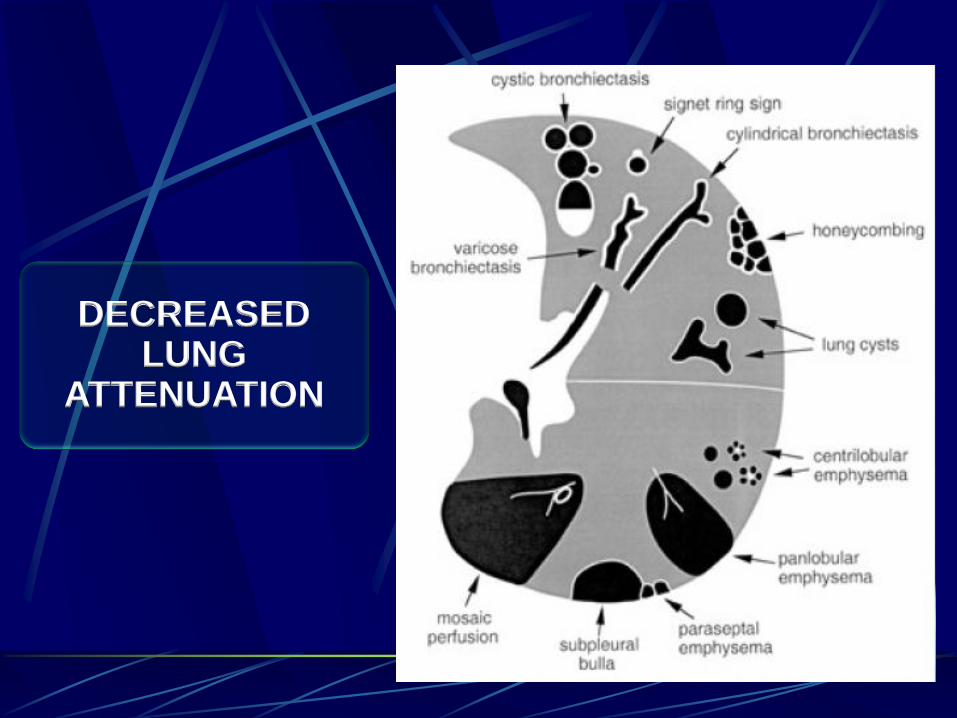
CTEPH =
Chronic thrombembolic
pulmonary hypertension
