radiation exposure in growing rod surgery for early onset scoliosis
TRANSCRIPT
11/8/2013
1
Behrooz A. Akbarnia, MD
Clinical Professor, University of California, San Diego
Medical Director, San Diego Center for Spinal Disorders
La Jolla, California
Magnetically Controlled Growing Rods (MCGR)
for
Early Onset Scoliosis (EOS)
UCSF Practical Course in Advanced Spinal techniques
Las Vegas, November 8, 2013
Disclosures (Growing Spine)
Growing Spine Foundation (a)
DePuy Spine (a,b)
Ellipse Tech. (a,b)
K2M (a,b)
Kspine (b)
a. Grants/Research Support b. Consultant c. Stock/Shareholder d. Speakers’ Bureau e. Other Financial Support
Treating very young children
with progressive EOS remains challenging…
Early Onset Spinal Deformity Challenges in EOS
• Many etiologies
• Many different treatments
• High rate of complications
• Limited outcome measures
• Comparisons difficult!
11/8/2013
2
• Options between growing rods, nonoperative treatment, VEPTR, Shilla, and fusion.
• Practical variation exists (as each patient needs special consideration) but consensus exists on the utility of GR in EOS specifically about starting age, curve and etiology.
• Vitale Study
J Ped Ortho 2010
No Evidence Based (EBM) Data
OBM (Opinion Based)
Literature Review
Growing Spine Study Group Growing Spine Foundation
Growing Spine Organization Acknowledgement
GSSG Sites

11/8/2013
3
GSSG- San Diego Site
Rady Children’s Hospital EOS Program
Development and Initial Validation of a Novel Classification System in Early Onset Scoliosis
Brendan A. Williams1, MD; Hiroko Matsumoto1, MA; Daren J. McCalla1, BS; Behrooz A. Akbarnia2, MD;
Laurel C. Blakemore3, MD; Randal R. Betz4, MD; John M. Flynn5, MD; Charles E. Johnston6, MD;
Richard E. McCarthy7, MD; David P. Roye Jr.1, MD; David L. Skaggs8, MD; John T. Smith9, MD;
Brian D. Snyder10, MD, PhD; Paul D. Sponseller11, MD, MBA; Peter F. Sturm12, MD;
George H. Thompson13, MD; Muharrem Yazici14, MD; Michael G. Vitale1, MD, MPH.
Cobb Angle Etiology Congenital/Structural Neuromuscular Syndromic Idiopathic
Results Not
Useful Useful Essential CVR
Sum of Ranks
COBB 0 1 14 0.87 29
ETIOLOGY 0 3 12 0.60 27
KYPHOSIS 0 4 11 0.47 26
AGE 5 0 10 0.33 20
PROGRESSION 3 5 7 -0.07 19
CHEST WALL ABNORMALITIES 2 9 4 -0.47 17
FLEXIBILITY 4 6 5 -0.33 16
OTHER CO-MORBIDITIES 3 8 4 -0.47 16
PULMONARY FUNCTION 3 9 3 -0.60 15
AMBULATORY ABILITY 2 12 1 -0.87 14
NUTRITIONAL STATUS 5 8 2 -0.73 12
MENTAL FUNCTION 10 5 0 -1.00 5
BONE QUALITY 11 4 0 -1.00 4
Vitale et al
Etiology
Congenital/
Structural
Neuromuscular
Syndromic
Idiopathic
Cobb Angle
1: <20°
2: 21-50°
3: 51-90°
4: >90°
Kyphosis
(-): <20°
N: 21-50°
(+): >50°
APR Modifier
P0: <10°/yr
P1: 10-20°/yr
P2: >20°/yr
Classification of EOS (C-EOS)

11/8/2013
4
Validation Studies (ICEOS)
Risk by Classification: Lower Risk of Rapid Failure • Congenital (21-50& 51-90); C2, C3 • Syndromic (21-50); S2 • Idiopathic (51-90); I3 Higher Risk of Rapid Failure • Congenital (>90); C4 • Neuromuscular (>51-90); N3 • Neuromuscular (>90); N4 • Syndromic (51-90); S3
Flynn, Vitale et al.
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the treatment options including growth friendly options?
• What are the expected outcomes?
• Can we minimize complications?
• What to expect in the future?
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• Can we minimize complications?
• What is the expected outcomes?
• What to expect in the future?
Natural History Untreated Scoliosis
•Infantile: 0 to 3 years
•Juvenile: 4 to 9 years
•Adolescent: 10 to 16 years
Pehrsson, Larssson, Oden & Nachemson, Spine,
1992
11/8/2013
5
Thoracic Insufficiency Syndrome
The Inability of the Thorax to Support
Normal Respiration
Or
Lung Growth
Campbell, Smith, et al.
J BJS Mar, 2003
J BJS Aug, 2004
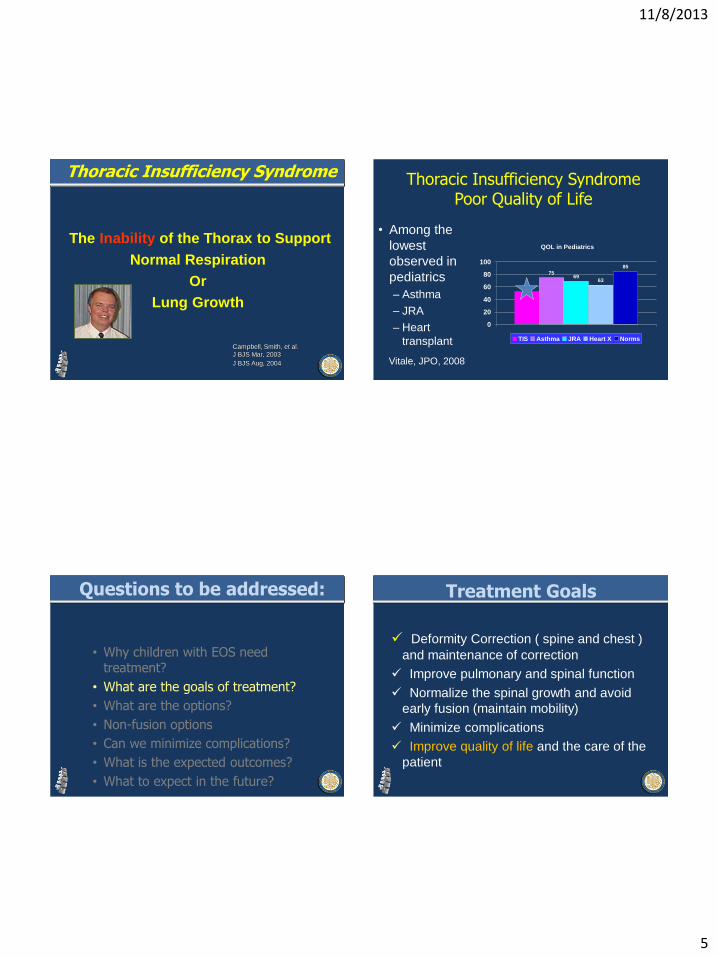
Thoracic Insufficiency Syndrome Poor Quality of Life
• Among the
lowest
observed in
pediatrics
– Asthma
– JRA
– Heart
transplant
QOL in Pediatrics
53
7569
63
85
0
20
40
60
80
100
TIS Asthma JRA Heart X Norms
Vitale, JPO, 2008
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• Can we minimize complications?
• What is the expected outcomes?
• What to expect in the future?
Treatment Goals
Deformity Correction ( spine and chest )
and maintenance of correction
Improve pulmonary and spinal function
Normalize the spinal growth and avoid
early fusion (maintain mobility)
Minimize complications
Improve quality of life and the care of the
patient
11/8/2013
6
Fusing scoliosis early may contribute to
shortening of the thoracic spine, TIS, and
respiratory insufficiency
• 28 pts, early thoracic fusion before the age 9 years,
– evaluated by pulmonary function testing at a minimum of 5 years f/u
– compared to age matched controls
• Average age at surgery was 3.3 yrs and at follow up was 14.6 yrs.
• Thoracic spinal height FVC < 50%
< 18 cm 63% pts
18 to 22 cm 25% pts
22 cm to normal† 0% pts
† normal 28 cm males, 26 cm females
Karol, et al., JBJS 2008, 90: 1272-1281.
Deceased
13 cm
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• Can we minimize complications?
• What is the expected outcomes?
• What to expect in the future?
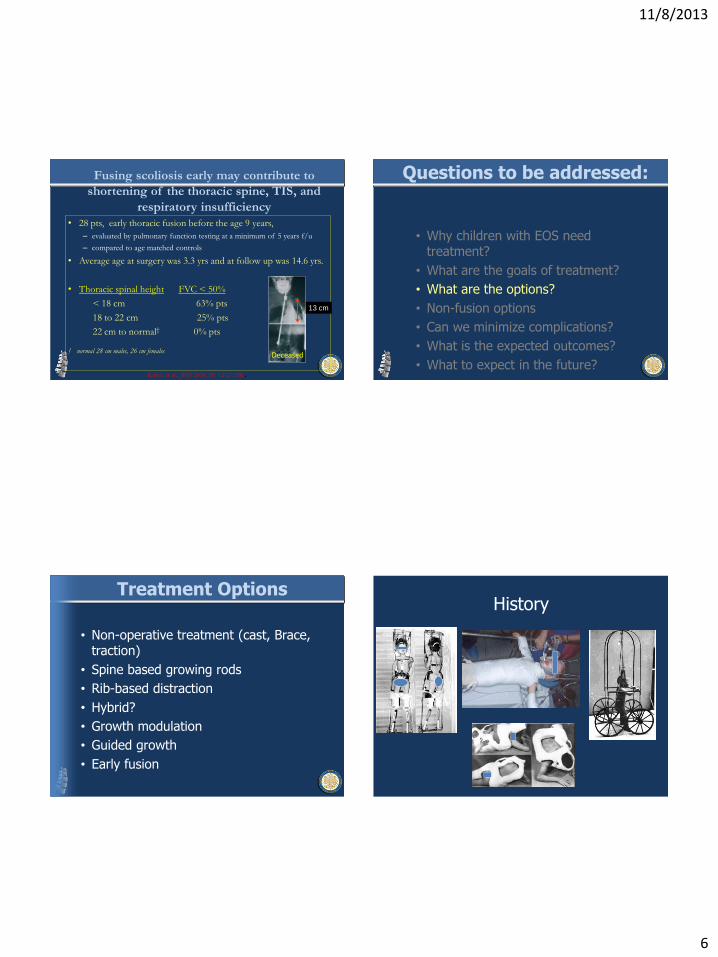
Treatment Options
• Non-operative treatment (cast, Brace, traction)
• Spine based growing rods
• Rib-based distraction
• Hybrid?
• Growth modulation
• Guided growth
• Early fusion
History

11/8/2013
7
Casting and Bracing is well tolerated Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• What is the expected outcomes?
• Can we minimize complications?
• What to expect in the future?
Growth Friendly Implant Classification
1. Distraction based – Growing Rods
– VEPTR
– MCGR
2. Guided Growth – Luque-Trolley
– Shilla
3. Tension Based – Tether
– Staple
>age 8
Non-congenital
< age 8 ? All etiologies
< age 9 ?
All etiologies
< age 9 ?
All etiologies
Skaggs
ONLY VEPTR IS APPROVED in USA
Indications for Growth-Friendly Surgery
• Progressive curves not controlled or amenable to bracing or casting
• Curves where growth preservation would be beneficial
• Curves that require management of both the chest wall and the scoliosis

11/8/2013
8
Absent Ribs: Expansion Thoracoplasty by Multiple Devices
Shilla
3 level fusion
compression
distraction
derotation
Open Screws – no fusion
no bone exposed
allow rod to slide
multiaxial
Richard McCarthy
Preop Postop 1 year Postop
Newton
Single Rod Techniques
Growing Rods
11/8/2013
9
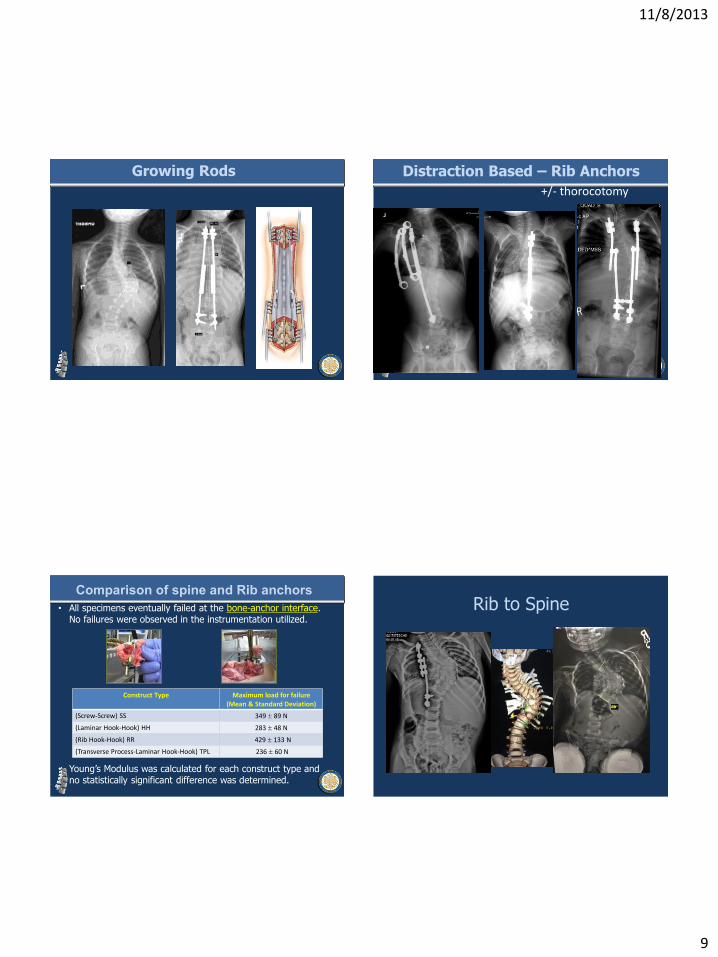
Growing Rods Distraction Based – Rib Anchors
+/- thorocotomy
Comparison of spine and Rib anchors
• All specimens eventually failed at the bone-anchor interface. No failures were observed in the instrumentation utilized.
• Young’s Modulus was calculated for each construct type and no statistically significant difference was determined.
Construct Type Maximum load for failure (Mean & Standard Deviation)
(Screw-Screw) SS 349 89 N
(Laminar Hook-Hook) HH 283 48 N
(Rib Hook-Hook) RR 429 133 N
(Transverse Process-Laminar Hook-Hook) TPL 236 60 N
Rib to Spine

11/8/2013
10
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• What is the expected outcomes?
• Can we minimize complications?
• What to expect in the future?
• EOSQ being collected prospectively
Quality of Life Outcomes
RESULTS (cont’d)
GROUP Cobb Angle (Pre-Initial to
Post Final)
%
Correction
Increase in
T1-S1
Length
Single with
apical
85° → 65 ° 23% 6.4cm
Single w/o
apical
61° → 39 °
36% 7.6cm
Dual w/o
apical
92° → 26°
71% 11.8cm
Growth per Year (cm)
• Total Group 1.21
• Under 5 years 1.19
• 5-10 year 1.13
• Under treatment 1.01
• Post final fusion group 1.66

11/8/2013
11
250
270
290
310
330
350
370
390
410
Apr
-98
Dec
-98
Oct-9
9
Oct-9
9
Sep
-00
May
-01
Oct-0
1
Sep
-01
May
-03
Feb-
04
Jan-
05
Dec
-06
0
10
20
30
40
50
60
70
80
90
100
T1-S1 Length
Length of Implant
Cobb Angle
Age 3 +11 Age 12 + 7
3 + 10 Year Old Girl With Marfan’s 7 + 8 yrs Follow Up
Final Fusion
13 cm
RESULTS
mm
.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
Change in T1-T12 (Pre-op to Latest Follow-up)
∆ in T1-T12 was greater in the 4-6 and ≥7 groups (p<0.001)
3 (n=17)
4-6 (n=19)
>7 (n=15)
Number of Spinal Distractions
Mean # of distractions = 5.4 (Range: 3–11)
Early onset scoliosis treated with Growing Rods has more growth and better Cobb correction but
more surgeries compared to Shilla
• 37 GR 37 Shilla
• Same FU (4.1 vs 4.6)
• T1-S1 ( 8.5 vs 6.4)
• Cobb angle Change ( 36 vs 23)
• Number of surgeries (7 vs 2.8)
Lindsay M. Andras, MD1; Elizabeth R. A. Joiner, BS1; Richard E. McCarthy, MD2; Scott J. Luhmann, MD3; Paul D. Sponseller, MD4; John B. Emans5, MD; David L. Skaggs, MD1 and Growing Spine Study Group
ICEOS 2012
Progression
86° 103
33
128
134
2+6

11/8/2013
12
No Trach. Normal activity
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• What is the expected outcomes?
• Can we minimize complications?
• What to expect in the future?
Adequate or Classic
Inadequate
Supra-laminar
Infra-laminar
Cross link
ANCHORS

11/8/2013
13
Significance of sagittal alignment
• Syndromic patients with early onset scoliosis
with thoracic kyphosis over 40 degrees who
undergo growing rod treatment should be
monitored very closely for complications,
particularly for implant failure
Final outcome at final FU
GR treatment abandoned in 11 out of 42 patients (26%)
Questions to be addressed:
• Why children with EOS need treatment?
• What are the goals of treatment?
• What are the options?
• Non-fusion options
• Can we minimize complications?
• What is the expected outcomes?
• What to expect in the future?
Magnetically Controlled
Growing Rod
(MCGR)
Phenix MAGEC

11/8/2013
14
• The use of remotely controlled
lengthening devices has been
previously reported. (Takaso
et al., Soubeiran et al.)
• Goal of MCGR: To reduce
frequency of surgeries while
still providing distraction
Introduction
• The complication risk increased by 24% for each additional
surgical procedure.
• Growth-guided procedures, may reduce the number of
procedures, but do not provide any distraction.
December 2010
Growth modulation with current Growing Rod (GR)
techniques require frequent surgical lengthening and has a high risk of complications
Introduction
2012 • Magentically controlled growing rods (MCGR) were
developed to allow for non-invasive lengthening
• Pre-clinical studies has shown promising results
INTRODUCTION
Spine 2012
• 7-9 levels were un-instrumented between cephalad and caudal foundations
• 7 mm of remote distraction was performed weekly for 7 weeks in EG under sedation
• Implants were removed at week #7
• Animals were sacrificed 3 weeks after implant removal
METHODS

11/8/2013
15
• MCGR was shown to be safe and effective in this study
• No complication resulted directly from distraction
• MCGR distinguishes itself by:
• Distraction accuracy / prediction
• Ability to shorten
CONCLUSIONS
--------------------------------------
-
MCGR Technology
Implantable spinal rod
with magnetic actuator
External remote controller
non-invasive adjustment
Example of current
physician directed
adjustable rod.
Requires surgical
intervention for
adjustment
MAGEC
• This study was designed to evaluate the
safety and efficacy of the MCGR technique in
patients with early onset scoliosis
• 33 MCGR patients in 4 centers (Hong
Kong, London, Cairo and Ankara)
• 14 patients met the inclusion criteria
(1) EOS of any etiology
(2) Minimum of 3 distractions
• T1-T12, T1-S1 and height of
instrumented spine was measured
Materials and Methods
Instru
men
ted h
eight o
f the
spin
e
Actu
ator exp
ansio
n
T1-T1
2
T1-S1

11/8/2013
16
• 14 patients:(7 M, 7 F)
• Mean age: 8 y+10 m
(3 y+6 m to 12 y+7 m)
• 14 initial surgeries
• 68 distractions
Materials and Methods
36%
29%
14%
14% 7%
Etiology
Idiopathic Neuromuscular
Congenital Syndromic
NF
• 5 single rod (SR) and 9 dual rod (DR)
• Average of 10 months follow up (6-18).
• An average of 4.9 distractions per patient
• Mean interval between index MCGR and the
first distraction was 66 days
• Mean interval between two subsequent
distractions was 43 days
Results
• Initial and final Cobb correction were significant in each group.
• Curve correction from initial post-op to final was maintained in both SR
and DR groups.
Results (Height)
T1-T12 (mm) T1-S1 (mm)
Pre
in
dex
Po
st
ind
ex
Fin
al
To
tal G
row
th*
Mo
nth
ly G
row
th
P v
alu
e
Pre
in
dex
Po
st
ind
ex
Fin
al
To
tal G
row
th*
Mo
nth
ly G
row
th
P v
alu
e
Total 177.9 197.7 208.2 10.5 1.65 <0.05 292.4 322 338 16 2.44 <0.05
Single 177.8 196.4 204 7.6 1.09 <0.05 295 322 331 9 1.27 <0.05
Dual 178 198.4 210.5 12.1 1.97 <0.05 290.6 322 342.2 20.2 3.09 <0.05
P > 0.05 P < 0.05

11/8/2013
17
1.27 mm
3.09 mm
2 mm
1.2 mm 1.22 mm
Mean Monthly T1-S1 Height Change (mm/mo)
MCGR Single Rod MCGR Dual Rod Dimeglio 0-5 years
Dimeglio 5-10 years Original GR (Akbarnia)
N=9 N=5 N=23
Results - Mean Monthly T1-S1 Height Change
P<0.05
Case one: 5.5 y/o Female (NM)
T1-T12: 176 mm
T1-S1: 251 mm
T1-T12: 181 mm
T1-S1: 261 mm
45° 21°
Pre Index Post Index
∆T1-T12: 5 mm
∆T1-S1:10 mm
Case one: A 5.5 y/o NM female
Post Index Latest Follow up
21°
9°
T1-T12: 181 mm
T1-S1: 261 mm
T1-T12: 193 mm
T1-S1: 292 mm ∆T1-T12: 11 mm
∆T1-S1: 31 mm
Comparison Data
Pre-operative Most recent Result
GSSG Data (average follow up 28 months)
Cobb Angle (°) 77.6 ± 16.7 41.3 ± 16.6 47% deformity
correction
Thoracic Spine
Height (mm) 165.6 ± 22.1 203.5 ± 27.5
23% Increased
thoracic spine height
MAGEC Data (average follow up 7.6 months)
Cobb Angle (°) 58.8 ± 12.3 31.4 ± 9.3 47% deformity
correction
Thoracic Spine
Height (mm) 186 ± 28 212 ± 28
14% Increased
thoracic spine height

11/8/2013
18
MCGR Cheung, Cheung, Samartzis, Mak, Wong, Cheung,
Akbarnia, Luk (Lancet April 19,2012)
• Five patients , 2 with over 24 months follow
up
• Monthly distractions
• Scoliosis from 67 to 29 at 2 years
• 1.9 mm increase per distraction
• No Anesthesia, No pain
• No complications
Scoliosis
Spinal Length MCGR (Case 1)

11/8/2013
19
MCGR (Case 1) MCGR (Case 2)
Pre Op AP Post Op AP
MCGR- Case 2
12.3 mm
14.5 mm
Post Distraction June 2010
Courtesy of Ken Cheung, MD, University of Hong Kong, HK
B. A. Akbarnia, K. Cheung, G. Demirkiran, H. Elsebaie J. Emans, C. Johnston, G. Mundis, H. Noordeen, J. Pawelek M. Shaw, D. Skaggs, P. Sponseller, G. Thompson, M. Yazici,
Growing Spine Study Group
Traditional Growing Rods Versus Magnetically Controlled Growing Rods in Early Onset Scoliosis:
A Case-Matched Two Year Study
48th Annual Meeting of Scoliosis Research Society September 18-21, 2013 – Lyon, France
11/8/2013
20
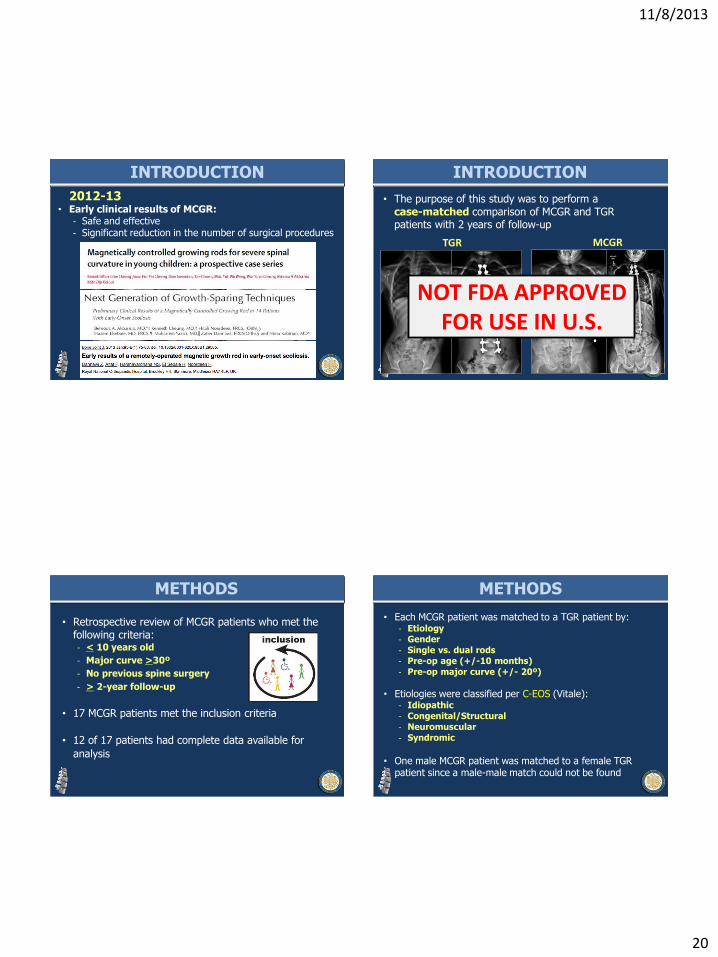
2012-13 • Early clinical results of MCGR:
- Safe and effective - Significant reduction in the number of surgical procedures
INTRODUCTION
• The purpose of this study was to perform a case-matched comparison of MCGR and TGR patients with 2 years of follow-up
INTRODUCTION
MCGR TGR
NOT FDA APPROVED FOR USE IN U.S.
• Retrospective review of MCGR patients who met the following criteria: - < 10 years old
- Major curve >30º
- No previous spine surgery
- > 2-year follow-up
• 17 MCGR patients met the inclusion criteria
• 12 of 17 patients had complete data available for
analysis
METHODS
• Each MCGR patient was matched to a TGR patient by: - Etiology - Gender - Single vs. dual rods - Pre-op age (+/-10 months) - Pre-op major curve (+/- 20º)
• Etiologies were classified per C-EOS (Vitale): - Idiopathic - Congenital/Structural - Neuromuscular - Syndromic
• One male MCGR patient was matched to a female TGR
patient since a male-male match could not be found
METHODS
11/8/2013
21
Spinal growth calculation: “Annual T1-S1 Growth”
METHODS
Δ in T1-S1 from post index to latest F/U
Length of follow-up
Annual T1-S1 Growth (mm/year)
=
• MCGR patients: - Mean age = 6.8 years - Mean follow-up = 2.5 years
• Follow-up was greater for TGR patients by 1.6 years
• Distribution of etiologies:
- 4 Neuromuscular - 4 Syndromic - 3 Idiopathic - 1 Congenital
RESULTS
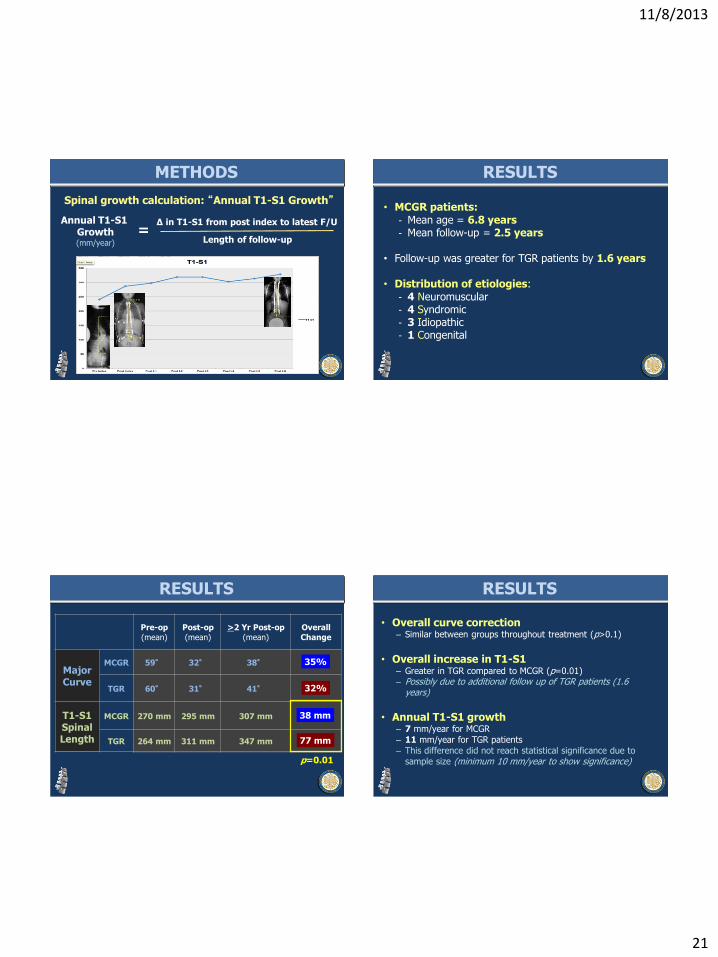
Pre-op
(mean)
Post-op
(mean)
>2 Yr Post-op
(mean)
Overall
Change
Major Curve
MCGR 59° 32° 38°
TGR 60° 31° 41°
T1-S1 Spinal Length
MCGR 270 mm 295 mm 307 mm
TGR 264 mm 311 mm 347 mm
RESULTS
35%
32%
38 mm
77 mm
p=0.01
RESULTS
• Overall curve correction – Similar between groups throughout treatment (p>0.1)
• Overall increase in T1-S1
– Greater in TGR compared to MCGR (p=0.01) – Possibly due to additional follow up of TGR patients (1.6
years)
• Annual T1-S1 growth
– 7 mm/year for MCGR – 11 mm/year for TGR patients – This difference did not reach statistical significance due to
sample size (minimum 10 mm/year to show significance)
11/8/2013
22
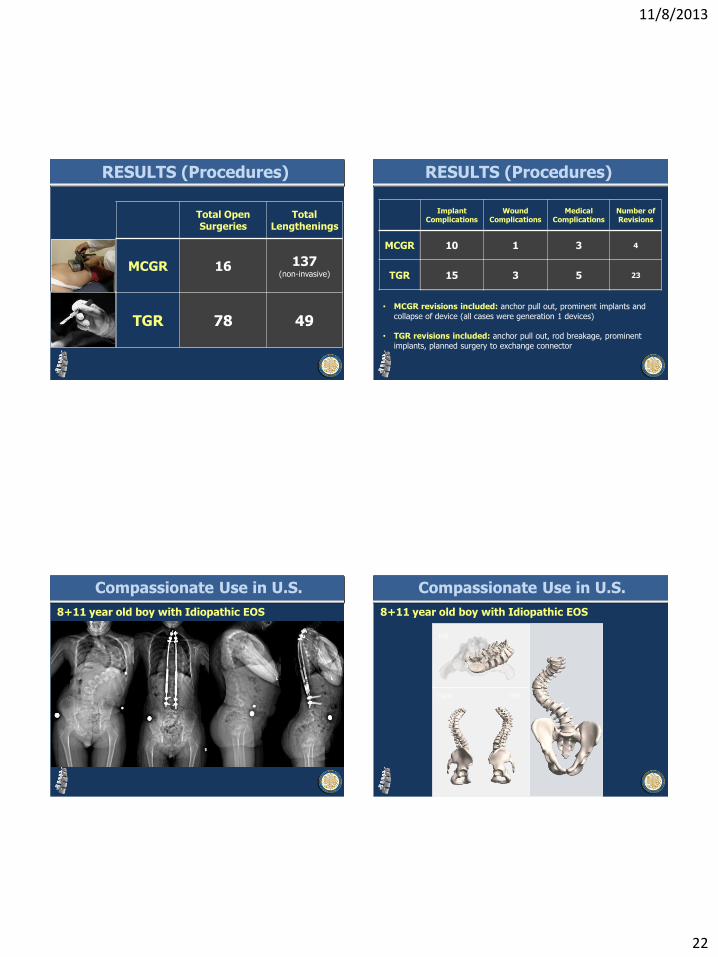
Total Open Surgeries
Total Lengthenings
MCGR 16 137 (non-invasive)
TGR 78 49
RESULTS (Procedures) RESULTS (Procedures)
Implant Complications
Wound Complications
Medical Complications
Number of Revisions
MCGR 10 1 3 4
TGR 15 3 5 23
• MCGR revisions included: anchor pull out, prominent implants and
collapse of device (all cases were generation 1 devices)
• TGR revisions included: anchor pull out, rod breakage, prominent
implants, planned surgery to exchange connector
Compassionate Use in U.S.
8+11 year old boy with Idiopathic EOS
top
right left
Compassionate Use in U.S.
8+11 year old boy with Idiopathic EOS
11/8/2013
23
top
right left
Compassionate Use in U.S.
8+11 year old boy with Idiopathic EOS • Major curve correction was similar between MCGR and
TGR patients throughout treatment
• Overall gain in T1-S1 was greater in TGR compared to MCGR, however, TGR had longer follow-up
• MCGR patients had 62 fewer surgical procedures than TGR patients and more non-invasive lengthenings
• Need to build consensus and develop practice guidelines for non-invasive lengthenings to reduce surgeon variability and improve reproducibility
Summary MCGR
THANK YOU