r. h. gilman*,†,¶ a. bowering†,# m. z. levy†,** c. a. … · tst reactions were compared to...
TRANSCRIPT

The value of counting BCG scars for interpretation of tuberculinskin tests in a tuberculosis hyperendemic shanty-town, Peru
M. Saito*,†,‡, C. T. Bautista§, R. H. Gilman*,†,¶, A. Bowering†,#, M. Z. Levy†,**, and C. A.Evans*,†,††
* Department of International Health, Johns Hopkins School of Public Health, Baltimore,Maryland, USA† Asociación Benéfica Proyectos en Informática, Salud, Medicina y Agricultura (AB PRISMA),Lima, Peru‡ Clinical Research Support Unit, St Luke's International Hospital, Tokyo, Japan§ US Military HIV Research Program, Henry M Jackson Foundation, Rockville, Maryland, USA¶ Department of Microbiology, Universidad Peruana Cayetano Heredia, Lima, Peru# Tufts University School of Medicine, Boston, Massachusetts,** Division of Biological and Biomedical Sciences, Emory University, Atlanta, Georgia, USA†† Wellcome Trust Center for Clinical Tropical Medicine, Imperial College, London, UK
SUMMARYSETTING—The tuberculin skin test (TST) is widely used as a diagnostic or screening test forMycobacterium tuberculosis infection and disease. A peri-urban shanty-town in the desert hills ofsouth Lima, Peru, highly endemic for tuberculosis, and where bacille Calmette-Guérin (BCG)vaccine had been given in multiple doses until 1995.
OBJECTIVE—To analyze the effect of multiple BCG vaccines on TST in a community-basedsetting.
DESIGN—Point-prevalence survey of TST reactions of 572 people aged 6–26 years from 255households. TST reactions were compared to the observed number of BCG scars and otherpotential risk factors (age, living with a TST-positive person, and contact with activetuberculosis).
RESULT—People with two or more scars had significantly larger reactions, even after adjustingfor potential risk factors. The adjusted population attributable fraction of being TST-positive andhaving two or more BCG scars was 26%.
CONCLUSION—There is no demonstrated benefit of repeat BCG vaccination. We thereforerecommend that physicians take into consideration the number of BCG scars when interpreting theTST and that programs give no more than one BCG vaccination.
© 2004 IUATLD
Correspondence to: Dr Robert H Gilman, Department of International Health, The Johns Hopkins School of Public Health, 615 NorthWolfe Street, Room W5515, Baltimore, MD 21205, USA. Tel: (+1) 410-614-3959. Fax: (+1) 410-614-6060. [email protected] [email protected].
Europe PMC Funders GroupAuthor ManuscriptInt J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Published in final edited form as:Int J Tuberc Lung Dis. 2004 July ; 8(7): 842–847.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

KeywordsMycobacterium tuberculosis; tuberculin skin test; purified protein derivative; BCG vaccine;vaccination
Tuberculosis (TB) is of major importance in developing countries. Ninety-five per cent oftuberculosis cases and 98% of tuberculosis deaths are in developing countries, and 75% ofthese cases are in the economically productive age group.1 Poverty, poorer health care, andmigration make TB control difficult in developing countries. In industrialized countries, alarge percentage of tuberculosis cases are among recent immigrants. In the United States, forexample, nearly 50% of TB cases are among immigrants.2
Although Peru has recently been removed from the World Health Organization's (WHO) listof 23 highburden countries, TB is still a major problem in this country.3 The reportedincidence in 2000 was 134 per 100 000 population;4 however, the WHO estimates theannual incidence at 228/100 000,3 and epidemiological studies in a Lima shantytown havedemonstrated even higher incidences (364/100 000).5
Recent studies have shown that bacille Calmette-Guérin (BCG) is effective in the preventionof tuberculous meningitis and disseminated TB, but its protective effect against pulmonaryTB is controversial.6,7 The results of a recent randomized trial of multiple BCG vaccinationshow no benefit of two or more vaccinations.8 Since 1995 the WHO has recommended asingle dose of the BCG vaccine at or soon after birth in all countries with a high incidence ofTB infection.9 However, multiple BCG vaccines are still given in 39 intermediate- and high-incidence countries as a part of their standard TB control programs.10
Peru's national BCG vaccination program has undergone numerous modifications. Theprogram was initiated in 1962 and originally included one intradermal dose for newborns(0.1 mg live bacillus in 0.1 ml, Pasteur Institute, Paris, France). The program was modifiedin the 1970s to include three vaccinations given at 5-year intervals up to age 15, as it wasthought that the immunity provided by BCG vaccination wanes within 5 years. The thirdvaccination, given at age 15, was dropped from the program in 1979, and the second, givenat age 10, was finally dropped in 1996. The program, however, was administered erratically.
The purpose of our study was to analyze the effect of multiple BCG vaccinations ontuberculin skin test (TST) reaction size in an endemic, community-based setting. Severalstudies have examined the effects of multiple BCG vaccines on TST reaction size.11-18None of these studies included household surveys, and thus could not assess the effect ofhousehold contact with a person with TST-positive reaction (Table 1). Two studies inCanada and the Philippines, in which household contact with an active tuberculosis case wasconsidered as an independent risk factor for adjustment, failed to demonstrate anindependent effect of multiple vaccinations.12,15 The absence of significant effect in thesestudies, however, may be due to their limited sample size.
STUDY POPULATION AND METHODSLas Pampas de San Juan de Miraflores is a shantytown comprised of fifty communities anda total population of 40 000. Located in the desert hills of south Lima, these communitiesconsist mainly of migrants of low socio-economic status from the Andean highlands. Livingconditions tend to be crowded, sanitation systems inadequate, and access to potable waterlimited. Shantytowns account for 30% of the 8 million inhabitants of Lima. Epidemiologicaldata on TB in this region have been reported previously.19,20 The same BCG strain was
Saito et al. Page 2
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

used throughout the period. There has never been any community- or school-basedrevaccination program based on TST in Peru.
A sample size of 397 households in Las Pampas was randomly selected from 1649households using a census performed by the Asociación Benéfica Proyectos en Informática,Salud, Medicina y Agricultura (AB PRISMA) in 2000. A household was defined as a groupof people living together and sharing common living spaces (kitchen, bedroom and livingroom). Within each household, all individuals except those with a history of TB, or thosewho had received a TST in the past 6 months, were invited to participate in the study. Thereis no screening or active case finding of tuberculosis using TST in these communities.Written informed consent was obtained from participants, or, in the case of those aged under18, by a parent or guardian.
Subjects were surveyed with structured questionnaires regarding exposure to tuberculosisand overall health. The Mantoux skin test was given intradermally with a 1 ml syringe and25-gauge needle, using 0.1 mm of five tuberculin units (Tubersol, Connaught Laboratories,Inc, Ontario, Canada) on the volar surface of one forearm. All skin tests were performed andread by a trained research nurse after 48–72 h and supervised by one of the authors (MS).The diameter of indurations along and transverse to the longitudinal axis of the arm weremeasured by the ballpoint pen method21 and recorded in mm. BCG scars were counted onboth arms. Participants with mean induration sizes ≥ 10 mm in both directions wereconsidered to be TST-positive following recommendations from both the AmericanThoracic Society for persons born in countries with high prevalence of tuberculosis andgroups with poor access to health care22 and the Peruvian Ministry of Health.23 Patientswith a positive TST and symptoms associated with tuberculosis underwent serial sputumexaminations and a chest X-ray. Children aged <15 years in recent contact with someonewith active tuberculosis were referred to the national tuberculosis control program to ruleout active TB or to start on preventive therapy for latent TB infection. The study wasapproved by the ethical review boards of AB PRISMA and the Johns Hopkins UniversityBloomberg School of Public Health.
ExclusionHousehold members aged ≥ 27 years were excluded from the analysis because of possibleconfusion between smallpox and BCG vaccination scars. Smallpox vaccination terminatedin Peru in 1974. Children aged <6 years were also excluded because of the low probabilityof having multiple BCG vaccines. However, they and subjects aged > 26 years wereincluded for TST data for the variable ‘presence of another person with TST-positivereaction in the same household’.
Statistical analysisThe χ2 test, Fisher's exact tests, and Kruskal-Wallis H test (a non-parametric test),24 wereused to compare the distribution of the variables in the BCG categorical groups. The Cuzicknon-parametric test25 was used to evaluate trends across ordered groups. Body mass index(BMI) was also compared in each BCG group as it is related to anergy and vulnerability ofdeveloping active tuberculosis.15,26
Because TST reactions were not normally distributed, we used multivariate ordinal logisticregression with the partial proportional odds model to calculate the adjusted odds ratio (OR)of having an increased TST reaction size among different categories of BCG scars, with thesize of the TST reaction coded as 1 (0 mm), 2 (1–4 mm), 3 (5–9 mm), 4 (10–14 mm), and 5(≥ 15 mm). The adjusted variables included age, history of living with a person with activeTB, and presence of another TST-positive person in the same household. Logistic regression
Saito et al. Page 3
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

analysis was applied to calculate the adjusted OR of being TST-positive using cut-off pointsof 10 mm and 15 mm and adjusting for potential confounders.
To estimate the attributable risk of a positive TST from having two or more BCG scars inthe study population we used the method described by Zhang and Yu.27 BCG scar countwas considered as both a categorical variable (no scar, one scar, two scars and three or morescars) and a binominal variable (having two or more scars or less than two scars).
All statistical tests were interpreted in a two-tailed fashion to estimate P values and 95%confidence intervals (CI). Binary logistic regression analysis was performed using Statastatistical software package (version 7.0, Stata Corporation, College Station, TX, USA). Themultivariate ordinal logistic regression with the partial proportional odds model wasperformed using SAS-NT software (version 8.1, SAS Institute, Cary, NC, USA).
RESULTSThree hundred and ninety-seven households were visited over 6 months. Of these, 307(77%) agreed to participate in the study, and 700 individuals aged 6 to 26 years from 280households were identified. Among the 700 individuals, both TST results and informationon the observed number of BCG scars on both arms were available from 588 (84%)individuals. Sixteen of these 588 individuals had a history of tuberculosis disease and wereexcluded from the study. None reported receiving a TST in the previous 6 months. The finalstudy population was comprised of 572 individuals from 255 households. These 572individuals were divided into four groups based on the number of BCG scars observed.Sixty-eight (12%) had no BCG scars, 310 (54%) had one scar, 164 (29%) had two scars and30 (5%) had three or more scars. As shown in Table 2, those with one scar accounted for thelargest percentage among groups and had the youngest mean age (P < 0.001, χ2 test). Thegroup without BCG scars had the lowest proportion of people who had completed secondaryschool (P = 0.003, χ2 test). The male to female ratio, mean BMI (≥ 15 years), meanhousehold income, presence of known TB contact and presence of another TST-positiveperson in the household were all similar across groups (Table 2).
Figure 1 shows the mean TST reaction size by age group and number of BCG scars. Therewas a stepwise increase in TST reaction size with increasing number of BCG scars which,when stratified by age groups, remained significant for each group (P <0.01, Cuzick non-parametric trend test), except for those aged 6–10 years (P = 0.21). The effect of two ormore BCG scars on the TST reaction size was still significant after adjusting for age, historyof living with a patient with active TB, and the presence of another TST-positive person inthe household, using an ordinal logistic model (Table 3). Level of education was not foundto be associated with a positive TST by logistic regression.
Figure 2 shows the percentage of TST-positive reactors (reaction size ≥10 mm vs. negative<10 mm) by number of BCG scars. The percentage of TST positives significantly increasedfrom the group with no scar to those with three or more scars in each group (P <0.017),except for those aged 6–10 years (P = 0.522). As shown in Table 3, after adjusting for agegroup, history of living with a patient with active TB, and the presence of another TST-positive person in the household, TST positivity was still strongly associated with havingtwo or three or more scars (OR 5.4, 95%CI 2.0–14.2 and OR 8.3, 95%CI 2.5–27.8,respectively). It was not significantly associated with having one scar. The effect of multipleBCGs on TST positivity remained after changing the cut-off point of a positive TST from 10to 15 mm. After adjusting for the above variables, the population attributable fraction ofTST positivity from having two or more BCG scars was 26%.
Saito et al. Page 4
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

DISCUSSIONTST has been a useful diagnostic test to identify persons infected with TB. However, withthe rise in reported numbers of TB cases and the continued use of multiple BCG vaccines inmany countries, the need for better guidelines for interpretation of the TST has become moreapparent.
In this study, we found that with an increasing number of BCG scars, the prevalence ofpositive TST also increased among children of school age and young adults. Increasing TSTpositivity is associated with increased age at BCG vaccination and decreasing time since lastBCG vaccination.28 Age is therefore an important confounder. In our study, even afteradjusting for age, the effect of multiple BCG vaccinations remained, even in the oldest agegroup (age 21–26 years) who had received their last vaccination 10–15 years before. Thefindings of this study are consistent with other studies of more selected populations.13-15
The TST-positive prevalence was higher in older age groups regardless of the number ofBCG scars, probably due to the increased frequency of latent TB infection with increasedage.
Many factors affect a person's response to the TST, such as strain and dose of BCGvaccination, age at vaccination, number of years since last vaccination, and frequency ofTST.28-30 Therefore, all studies examining the relationship of BCG and TST areconstrained by the above variables and are most valid when used locally.31 Nevertheless,the strong association between the number of BCG scars and TST positivity appears to betrue world-wide.
In Peru, in this population, scarring after BCG is a highly reliable indicator. Our group hasdemonstrated that 99% of children given a BCG at or soon after birth will have a scar.32 Incountries with more severe malnutrition and low birth weights, others have noted a decreasein scarring after BCG vaccination.33
Based on our data, we recommend that physicians in developing countries and those whocare for immigrants from these countries must take into account the number of BCG scars,and not simply a history of BCG vaccination when interpreting TST readings. BCG given atbirth does not change the proportion of TST-positive results when the cut-off point is 10mm, despite a significant increase in size of TST reaction.34 Thus a single BCG given atbirth is less likely to distort the interpretation of the TST. There appears to be no benefit ingiving additional doses of BCG for tuberculosis prevention.6,7 We therefore recommendthat physicians take into consideration the number of BCG scars when interpreting the TSTand that programs give no more than one BCG vaccination.
AcknowledgmentsWe would like to thank Drs Lawrence Moulton, Caryn Bern, and Margaret Kosec for their advice on this paper andcomments on the manuscript, Ms Eleana Sanchez and Ms Lilia Cabrera for data collection, Mr Marco Varela fordata management and Ms JB Phu and Ms D Sara for technical assistance. We also thank the communities of LasPampas de San Juan de Miraflores for their cooperation.
This study was supported by the USAID–Tuberculosis Award HRN-5986-A-00-6006-00, the NIH ITREID grant5D43-TW00910, the Fogarty-NIH AIDS training program 3T22-TW00016-05S3, the NIAID tutorial training grant5T35-AI07646-02, and the anonymous RG-ER fund. M Saito is funded by St Luke's Life Science Institute. M ZLevy is a Howard Hughes Pre-Doctoral Fellow. C A Evans is funded by a Wellcome Trust Fellowship.
Saito et al. Page 5
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

References1. World Health Organization. Guidelines for the management of drug-resistant tuberculosis. WHO;
Geneva, Switzerland: 1997.
2. Centers for Disease Control and Prevention. Tuberculosis morbidity among U.S.-born and foreign-born populations—United States, 2000. MMWR. 51:101–104. 101.
3. World Health Organization. Global tuberculosis control. WHO report 2001. WHO; Geneva,Switzerland: 2001.
4. Ministerio de Salud. Tuberculosis en el Perú: Informe 2000. Dirección General de Salud de lasPersonas; Lima, Perú: 2001.
5. Sanghavi DM, Gilman RH, Lescano-Guevara AG, Checkley W, Cabrera LZ, Cardenas V.Hyperendemic pulmonary tuberculosis in a Peruvian shantytown. Am J Epidemiol. 1998; 148:384–389. [PubMed: 9717883]
6. Colditz GA, Brewer TF, Berkey CS, et al. Efficacy of BCG vaccine in the prevention oftuberculosis. Meta-analysis of the published literature. JAMA. 1994; 271:698–702. [PubMed:8309034]
7. Leung CC, Tam CM, Chan SL, Chan-Yeung M, Chan CK, Chang KC. Efficacy of the BCGrevaccination programme in a cohort given BCG vaccination at birth in Hong Kong. Int J TubercLung Dis. 2001; 5:717–723. [PubMed: 11495262]
8. Karonga Prevention Trial Group. Randomized controlled trial of single BCG, repeated BCG, orcombined BCG and killed Mycobacterium leprae vaccine for prevention of leprosy and tuberculosisin Malawi. Lancet. 1996; 348:17–24. [PubMed: 8691924]
9. World Health Organization. Global Tuberculosis Programme and Global Programme on Vaccines.Statement on BCG revaccination for the prevention of tuberculosis. Wkly Epidemiol Rec. 1995;70:229–231. [PubMed: 7669527]
10. Fine, P.; Carneiro, I.; Milstein, J.; Clements, C. Issues relating to the use of BCG in immunizationprogrammes: a discussion document. WHO; Geneva, Switzerland: 1999.
11. Sepulveda RL, Ferrer X, Latrach C, Sorensen RU. The influence of Calmette-Guérin bacillusimmunization on the booster effect of tuberculin testing in healthy young adults. Am Rev RespirDis. 1990; 142:24–28. [PubMed: 2368973]
12. Young TK, Mirdad S. Determinants of tuberculin sensitivity in a child population covered by massBCG vaccination. Tubercle Lung Dis. 1992; 73:94–100.
13. Menzies R, Vissandjee B. Effect of bacille Calmette-Guérin vaccination on tuberculin reactivity.Am Rev Respir Dis. 1992; 145:621–625. [PubMed: 1546843]
14. Ildirim I, Hacimustafaoglu M, Ediz B. Correlation of tuberculin induration with the number ofBacillus Calmette-Guérin vaccines. Pediatr Infect Dis J. 1995; 14:1060–1063. [PubMed: 8745018]
15. Lao LY, De Guia T. Tuberculin skin testing: determinants and reaction. Respirology. 1999; 4:311–317. [PubMed: 10489682]
16. Chee CB, Soh CH, Boudville IC, Chor SS, Wang YT. Interpretation of the tuberculin skin test inMycobacterium bovis BCG-vaccinated Singaporean schoolchildren. Am J Respir Crit Care Med.2001; 164:958–961. [PubMed: 11587978]
17. Kuyucu N, Kuyucu S, Bakirtas A, Karacan C. BCG revaccination and tuberculin reactivity. IndianJ Pediatr. 2001; 68:21–25. [PubMed: 11237231]
18. Bierrenbach AL, Cunha SS, Barreto ML, et al. Tuberculin reactivity in a population ofschoolchildren with high BCG vaccination coverage. Rev Panam Salud Publica. 2003; 13:285–293. [PubMed: 12831432]
19. Madico G, Gilman RH, Checkley W, et al. Community infection ratio as an indicator fortuberculosis control. Lancet. 1995; 345:416–419. [PubMed: 7853950]
20. Getchell WS, Davis CE, Gilman J, Urueta G, Ruiz-Huidubro E, Gilman RH. Basic epidemiologyof tuberculosis in Peru: a prevalence study of tuberculin sensitivity in a Pueblo joven. Am J TropMed Hyg. 1992; 47:721–729. [PubMed: 1471732]
21. Jordan TJ, Sunderam G, Thomas L, Reichman LB. Tuberculin reaction size measurement by thepen method compared to traditional palpation. Chest. 1987; 92:234–236. [PubMed: 3608594]
Saito et al. Page 6
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

22. The American Thoracic Society and the Centers for Disease Control and Prevention. Diagnosticstandards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med.2000; 161:1376–1395. [PubMed: 10764337]
23. Dirección del Programa Nacional de Control de Enfermedades Transmisibles Control de laTuberculosis. Actualización en la técnica de aplicación, lectura e interpretación de la prueba detuberculina. Directiva No 003-2000-PCT. Ministry of Health; Lima, Peru: 2000.
24. Kruskal WH, Wallis WA. Use of ranks in one-criterion variance analysis. J Am Statist Assoc.1952; 47:583–621.
25. Stata Corp. Stata Reference Manuel. Vol. 1 A–G. Stata Press; College Station, TX: 1999. Release6
26. Hoge CW, Fisher L, Donnell HD Jr, et al. Risk factors for transmission of Mycobacteriumtuberculosis in a primary school outbreak: lack of racial difference in susceptibility to infection.Am J Epidemiol. Mar 1.1994 139:520–530. [PubMed: 8154476]
27. Zhang J, Yu KF. What's the relative risk? A method of correcting the odds ratio in cohort studiesof common outcomes. JAMA. 1998; 280:1690–1691. [PubMed: 9832001]
28. Menzies D. What does tuberculin reactivity after bacillus Calmette-Guérin vaccination tell us? ClinInfect Dis. 2000; 31(Suppl 3):S71–S74. [PubMed: 11010826]
29. Centers for Disease Control. Use of BCG vaccines in the control of tuberculosis: A joint statementby the ACIP and the Advisory Committee for Elimination of Tuberculosis. MMWR. 1988;37:663–664. 669–675. [PubMed: 3141765]
30. Sepulveda R, Burr C, Ferrer X, Sorensen RU. Booster effect of tuberculin testing in healthy 6-year-old school children vaccinated with Bacillus Calmette-Guérin at birth in Santiago, Chile.Pediatr Infect Dis J. 1998; 7:578–581. [PubMed: 3140208]
31. Wang L, Turner MO, Elwood RK, Schulzer M, FitzGerald JM. A meta-analysis of the effect ofBacille Calmette Guérin vaccination on tuberculin skin test measurements. Thorax. 2002; 57:804–809. [PubMed: 12200526]
32. Santiago EM, Lawson E, Gillenwater K, et al. A prospective study of bacillus Calmette-Guérinscar formation and tuberculin skin test reactivity in infants in Lima, Peru. Pediatrics. 2003;112:298–302.
33. Rani SH, Vijayalakshni V, Sunil K, Lakshmi KA, Suman LG, Murthy KJ. Cell mediated immunityin children with scar-failure following BCG vaccination. Indian Pediatr. 1998; 35:569–571.[PubMed: 10216662]
34. Karalliedde S, Katugaha LP, Uragoda CG. Tuberculin response of Sri Lankan children after BCGvaccination at birth. Tubercle. 1987; 68:33–38. [PubMed: 3660460]
Saito et al. Page 7
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
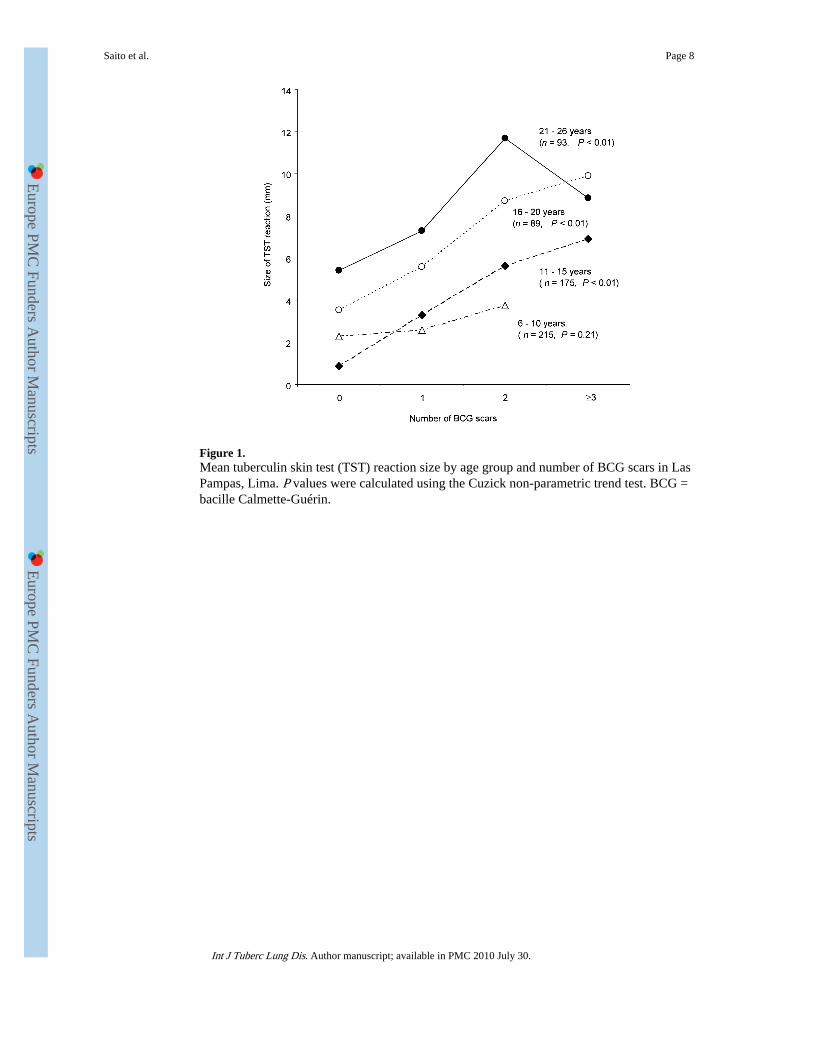
Figure 1.Mean tuberculin skin test (TST) reaction size by age group and number of BCG scars in LasPampas, Lima. P values were calculated using the Cuzick non-parametric trend test. BCG =bacille Calmette-Guérin.
Saito et al. Page 8
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Figure 2.Tuberculin skin test (TST) positivity by age group and number of BCG scars in Las Pampas,Lima. TST reactivity was defined as positive (≥ 10 mm) and negative (< 10 mm). P valueswere tested for linear trend of the log odds. BCG = bacille Calmette-Guérin.
Saito et al. Page 9
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Saito et al. Page 10
Tabl
e 1
Stud
ies
of m
ultip
le B
CG
vac
cina
tion
on tu
berc
ulin
ski
n te
st
Aut
hor
Yea
rC
ount
ryP
opul
atio
nA
ge, y
ears
Par
tici
pant
s, n
Sepu
lved
a et
al.1
119
89C
hile
Med
ical
stu
dent
s19
(m
ean)
208
You
ng e
t al.1
219
92C
anad
aC
anad
ian
Indi
an c
hild
ren
1–15
701
Men
zies
et a
l.13
1992
Can
ada
Scho
olch
ildre
n, a
dults
grad
e 6
& 1
0, 1
8–25
yea
rs4
629
Ildi
rim
et a
l.14
1995
Tur
key
Scho
olch
ildre
n6–
123
548
Lao
et a
l.15
1999
Phili
ppin
esSc
hool
child
ren
5 (m
ean)
284
Che
e et
al.1
620
01Si
ngap
ore
Scho
olch
ildre
n12
,16
266
005
Kuy
ucu
et a
l.17
2001
Tur
key
Scho
olch
ildre
n7–
142
810
Bie
rren
bach
et a
l.18
2003
Bra
zil
Scho
olch
ildre
n14
1 14
8
BC
G =
bac
ille
Cal
met
te-G
uéri
n.
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Saito et al. Page 11
Tabl
e 2
Cha
ract
eris
tics
of p
artic
ipan
ts w
ith tu
berc
ulin
ski
n te
st b
y nu
mbe
rs o
f B
CG
sca
rs in
Las
Pam
pas,
Lim
a
Num
ber
of B
CG
sca
rs
Fea
ture
No
scar
One
sca
rT
wo
scar
s≥3
sca
rsP
val
ue
Part
icip
ants
, n68
310
164
30
Age
gro
up, y
ears
6–
1025
165
25
11
–15
769
8118
16
–20
1235
357
21
–26
2441
235
Mea
n ag
e, y
ears
15.5
12.1
14.8
15.4
<0.
001*
Fem
ale/
mal
e ra
tio1.
31.
01.
00.
90.
625†
Mea
n bo
dy m
ass
inde
x (≥
15 y
ears
)23
.523
.122
.923
.30.
299*
Mea
n ho
useh
old
inco
me,
$18
717
718
116
80.
266*
Seco
ndar
y sc
hool
com
plet
ed (
≥18
year
s), %
41.4
70.5
78.6
900.
003†
Hav
ing
a hi
stor
y of
livi
ng w
ith a
pat
ient
with
act
ive
tube
rcul
osis
with
in la
st 5
yea
rs, %
14.7
9.4
11.7
16.7
0.41
9†
Pres
ence
of
anot
her
TST
-pos
itive
per
son
in th
e ho
useh
old,
%49
.360
.963
.866
.70.
188†
Tub
ercu
lin s
kin
test
rea
ctio
n si
ze, n
(%
)
0
mm
34 (
50.0
)12
4 (4
0.0)
42 (
25.6
)5
(16.
7)<
0.00
1†
1–
4 m
m23
(33
.8)
128
(41.
3)57
(34
.8)
9 (3
0.0)
0.32
4†
5–
9 m
m4
(5.9
)22
(7.
1)20
(12
.2)
4 (1
3.3)
0.17
2 †
10
–14
mm
1 (1
.5)
13 (
4.2)
16 (
9.7)
7 (2
3.3)
<0.
001†
≥1
5 m
m6
(8.8
)23
(7.
4)29
(17
.7)
5 (1
6.7)
0.00
5†
* Kru
skal
-Wal
lis H
test
.
† χ2
test
.
BC
G =
bac
ille
Cal
met
te-G
uéri
n; T
ST =
tube
rcul
in s
kin
test
.
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Saito et al. Page 12
Tabl
e 3
Adj
uste
d od
ds r
atio
(A
OR
) fo
r ha
ving
a la
rger
rea
ctio
n si
ze a
nd a
pos
itive
tube
rcul
in s
kin
test
(T
ST)
Fea
ture
Ord
inal
logi
stic
regr
essi
on*
AO
R‡
(95%
CI)
Bin
ary
logi
stic
regr
essi
on†
AO
R‡
(95%
CI)
BC
G v
acci
natio
n
N
o B
CG
Ref
Ref
O
ne B
CG
sca
r1.
9 (1
.1–2
.4)§
2.2
(0.8
–5.7
)
T
wo
BC
G s
cars
3.5
(1.9
–4.3
)¶4.
8 (1
.9–1
2.5)
#
≥3
BC
G s
cars
4.9
(2.1
–6.2
)¶7.
8 (2
.4–2
5.4)
#
Age
Si
x ye
ars
of a
geR
efR
ef
E
ffec
t of
each
add
ition
al y
ear
of a
ge1.
1 (1
.06–
1.13
)¶1.
2 (1
.1–1
.3)¶
Edu
catio
n (≥
18 y
ears
)**
<
10 y
ears
(in
com
plet
e se
cond
ary
scho
ol o
r le
ss)
Ref
Ref
≥1
0 ye
ars
(sec
onda
ry s
choo
l or
mor
e)0.
8 (0
.4–1
.6)
0.5
(0.2
–1.2
)
His
tory
of
livin
g w
ith a
pat
ient
with
act
ive
tube
rcul
osis
N
oR
efR
ef
Y
es2.
0 (1
.2–3
.3)#
3.8
(2.0
–7.6
)¶
Pres
ence
of
anot
her
TST
-pos
itive
per
son
in th
e ho
useh
old
N
oR
efR
ef
Y
es1.
4 (1
.0–2
.0)§
2.7
(1.6
–4.8
)#
* TST
rea
ctio
n si
ze w
as c
ateg
oriz
ed a
s 0,
1–4
, 5–9
10–
14 a
nd 1
5 m
m.
† TST
rea
ctiv
ity w
as d
efin
ed a
s po
sitiv
e (≥
10 m
m)
and
nega
tive
(<10
).
‡ AO
Rs
are
adju
sted
by
all o
ther
var
iabl
es e
xcep
t ‘ed
ucat
ion’
for
all
part
icip
ants
.
§ P <
0.0
5.
¶ P <
0.0
01.
# P <
0.0
1.
**V
aria
ble
‘edu
catio
n’ w
as a
djus
ted
for
all o
ther
var
iabl
es f
or p
artic
ipan
ts a
ged
mor
e th
an 1
8 ye
ars.
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Saito et al. Page 13R
ef =
ref
eren
ce g
roup
.
Int J Tuberc Lung Dis. Author manuscript; available in PMC 2010 July 30.