quick response code a localized gingival …rep.nacd.in/ijda/pdf/3.4.711.pdf · introduction...
TRANSCRIPT

A Localized Gingival Enlargement asPeripheral Ossifying Fibroma
Gita Malathi K1, Ravichandra PV2, Suresh KumarK3
CASE REPORT
INDIAN JOURNAL OF DENTAL ADVANCEMENTS
Jour nal homepage: www. nacd. in
Article InfoReceived: July 16, 2011Review Completed: August, 19, 2011Accepted: September, 20, 2011Available Online: January, 2012© NAD, 2011 - All rights reserved
ABSTRACT:
Peripheral ossifying fibroma, a oral pathologic condition thatappears in the mouth as an overgrowth of gingival tissue is arelatively common lesion accounting for upto 15% of all biopsygingival lesions. A 24-year-old female patient presented with thechief complaint of a painless swelling in the upper maxillary areaof 1 year duration. Clinical examination revealed gingivalenlargement localized between upper central and lateral incisors.Excisional biopsy of the gingival lesion and the specimen weresubmitted for histopathological analysis. Biopsy of the gingivallesion revealed Stratified Squamous Epithelium & highly cellularfibroblastic component presenting central areas of calcificationand features consistent with a diagnosis of POF. After 1 year followup, no recurrence has been observed. Clinician awarenessregarding the possibility of such a presentation and its implicationwill help to ensure optimal treatment outcome.
Key words: peripheral ossifying fibroma, oral cavity, Biopsy,peripheral cementifying fibroma, fibrous epulis,calcifying fibroblastic granuloma
Senior Lecturer1
Department of PeriodonticsSVS Institute of Dental SciencesMahabubnagar - 509002. AP
Professor and HOD2
Department of Conservative DentistryKamineni Institute of Dental SciencesNarketpally, Nalgonda Dist. A.P.
Professor and HOD3
Department of PeriodonticsRama Dental College, Kanpur, U.P.
Email for correspondence:[email protected]
INTRODUCTION
Peripheral ossifying fibroma (POF) is a reactivegingival nodule composed of a cellular fibroblasticconnective tissue stroma associated with theformation of randomly dispersed foci of mineralizedproduct consisting of bone, cementum-like tissue, ordystrophic calcification.1 It is widely considered thatthis non-neoplastic enlargement of the gingivaoriginates from the cells of the periodontal ligament2
and is often associated with trauma or local irritants.Some authors have called it fibrous epulis, calcifyingfibroblastic granuloma, or peripheral fibroma withcalcification.
Peripheral ossifying fibroma presents as apainless, hemorrhagic and often lobulated mass ofthe gingiva or alveolar mucosa sometimespresenting with large areas of surface ulceration.
Most lesions are 1-2 cm in size, but some may slowlyenlarge to more than 4 cm.
The POF may occur at any age range,3 especiallyin individuals with poor oral hygiene; but the lesionexhibits a peak incidence between the second andthird decades with females being affected more thanmales.4 The maxillary gingiva is involved more oftenthan the mandibular gingival with a predispositiontowards the anterior regions.5 Mobility and/ormigration of adjacent teeth are occasionallyobserved. However, on rare occasions, superficialerosion of bone can be seen. The lesions should besurgically excised and submitted for microscopicexamination for confirmation of diagnosis.
CASE REPORT
A 24 year- old female patient visited theDepartment of Periodontics, presenting an exophyticmass in oral cavity that had enlarged gradually for 6
Indian J Dent Adv 2011; 3(4): 711-714
doi: 10.5866/3.4.711
Quick Response Code

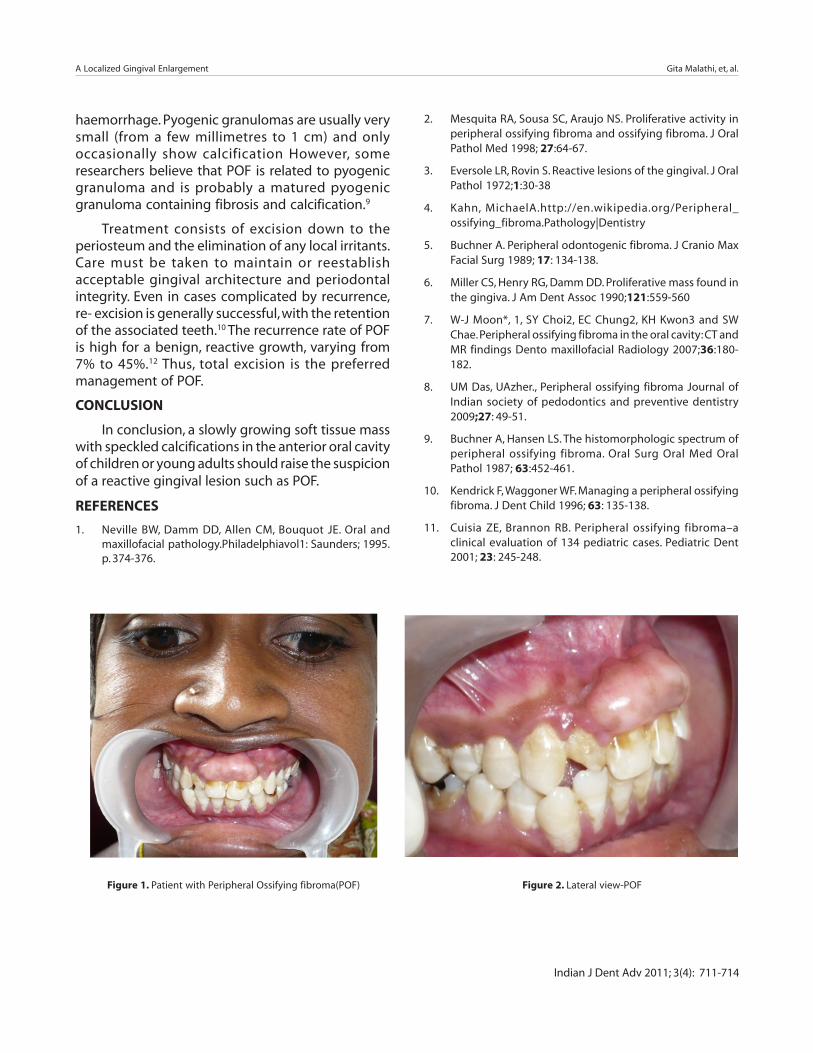
months. Clinical examination revealed gingivalenlargement, measuring 3x2 cm in diameter localizedbetween upper central and lateral incisors with apedunculated, non-tender and light pinkish mass inthe upper anterior maxillary area (Figures 1&2).
The lesion was asymptomatic, non-ulcerated,and the overlying mucosa showed no abnormalchanges. Radiographs of OPG and IOPA X-rays weretaken in relation to upper central incisors. Noradiological signs of involvement of alveolar ridgewere observed on the roentgenogram (Figure 3).
TREATMENT
Under local anaesthesia, the lesion wascompletely excised using electrocautery (Figure4).The excised tissue measured 3x2 cm (Figure 5).Theresultant area was debrided (figure 6) and a COE packwas placed. (Figure 7) The excisional biopsy wassubmitted for histological analysis. Thehistopathological examination (Figure 8) of the lesionrevealed the prominent area of highly cellular fibrousconnective tissue showing collagen fibers andproliferating plump fibroblasts, and focal areas oftrabecular bone lined by osteoblasts. The coveringstratified squamous epithelium was parakeratinizedwith focal areas of acanthosis. The diagnosisestablished according to both clinical andhistopathological patterns was that of POF.
DISCUSSION
Ossifying fibroma occurs mostly in craniofacialbones and is generally categorized into two types,central and POF. The central type arises from theendosteum or the periodontal ligament (PDL)adjacent to the root apex and expands from themedullary cavity of the bone. On the other hand, theperipheral type shows a contiguous relationship withthe PDL, occurring solely on the soft tissues overlyingthe alveolar process. In spite of confusingterminology, POF is not the peripheral counterpartof the central ossifying fibroma of the mandible andmaxilla,6 but instead is a reactive gingival lesionknown under the generic name of epulis.
The etiology of POF is unclear. Trauma or localirritation such as dental plaque, calculus, ill-fittingdental appliances and poor-quality dentalrestorations are all known to precipitate the
development of POF. Inflammatory hyperplasiaoriginating in the superficial PDL is considered to bea factor in the histogenesis of the POF. Furthermore,a high female predilection, rare occurrence in the firstdecade, and decline in incidence after age 30 suggestthat hormonal influence may be a lesional growthfactor.7
Clinically, the POF presents as an exophytic,smooth-surfaced, pink or red nodular mass that issessile, or is less frequently seen on a pedicle. Theinterdental gingival papilla is frequently involved.8 Ingeneral, the pyogenic granuloma presents as a soft,friable nodule that bleeds with minimalmanipulation, but tooth displacement and resorptionof alveolar bone are not observed. Althoughperipheral giant cell granuloma has clinical featuressimilar to those of POF, the latter lacks the purple orblue discoloration commonly associated withperipheral giant cell granuloma and radiographicallyshows small flecks of calcification. Thus, the diagnosisof the POF based only on clinical aspects can bedifficult and histopathological examination of thesurgical specimen obtained by excisional biopsy ismandatory for an accurate diagnosis. In the casereported, the histopathological feature of the POF ischaracterized by the presence of connective tissuewith high cellularity and calcifications.9
Peripheral ossifying fibromas appearmicroscopically as a combination of a mineralizedproduct and fibrous proliferation. Usually fibrousproliferation is accompanied by increased cellularitywith plump, immature fibroblasts and variableamounts of calcified material.10 The mineralizedportion may be osteoid, cementoid, or dystrophic. Insome cases, this characteristic pattern is only part ofthe pattern of a larger lesion that may resemble anirritation fibroma or pyogenic granuloma or fibromahas existed for a longer period of time.
The differential diagnosis for oral cavity tumorsin the pediatric age group includes haemangioma,lymphangioma, salivary gland tumors from the hardpalate and pyogenic granuloma from the gingiva.POFs can be clinically misdiagnosed as a pyogenicgranuloma at an early stage.11 Pyogenic granulomataare highly vascular non-tumourous conditionsinvolving gingival tissues, with a tendency to
A Localized Gingival Enlargement Gita Malathi, et, al.
Indian J Dent Adv 2011; 3(4): 711-714
haemorrhage. Pyogenic granulomas are usually verysmall (from a few millimetres to 1 cm) and onlyoccasionally show calcification However, someresearchers believe that POF is related to pyogenicgranuloma and is probably a matured pyogenicgranuloma containing fibrosis and calcification.9
Treatment consists of excision down to theperiosteum and the elimination of any local irritants.Care must be taken to maintain or reestablishacceptable gingival architecture and periodontalintegrity. Even in cases complicated by recurrence,re- excision is generally successful, with the retentionof the associated teeth.10 The recurrence rate of POFis high for a benign, reactive growth, varying from7% to 45%.12 Thus, total excision is the preferredmanagement of POF.
CONCLUSION
In conclusion, a slowly growing soft tissue masswith speckled calcifications in the anterior oral cavityof children or young adults should raise the suspicionof a reactive gingival lesion such as POF.
REFERENCES
1. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral andmaxillofacial pathology.Philadelphiavol1: Saunders; 1995.p. 374-376.
2. Mesquita RA, Sousa SC, Araujo NS. Proliferative activity inperipheral ossifying fibroma and ossifying fibroma. J OralPathol Med 1998; 27:64-67.
3. Eversole LR, Rovin S. Reactive lesions of the gingival. J OralPathol 1972;1:30-38
4. Kahn, MichaelA.http://en.wikipedia.org/Peripheral_ossifying_fibroma.Pathology|Dentistry
5. Buchner A. Peripheral odontogenic fibroma. J Cranio MaxFacial Surg 1989; 17: 134-138.
6. Miller CS, Henry RG, Damm DD. Proliferative mass found inthe gingiva. J Am Dent Assoc 1990;121:559-560
7. W-J Moon*, 1, SY Choi2, EC Chung2, KH Kwon3 and SWChae. Peripheral ossifying fibroma in the oral cavity: CT andMR findings Dento maxillofacial Radiology 2007;36:180-182.
8. UM Das, UAzher., Peripheral ossifying fibroma Journal ofIndian society of pedodontics and preventive dentistry2009;27: 49-51.
9. Buchner A, Hansen LS. The histomorphologic spectrum ofperipheral ossifying fibroma. Oral Surg Oral Med OralPathol 1987; 63:452-461.
10. Kendrick F, Waggoner WF. Managing a peripheral ossifyingfibroma. J Dent Child 1996; 63: 135-138.
11. Cuisia ZE, Brannon RB. Peripheral ossifying fibroma–aclinical evaluation of 134 pediatric cases. Pediatric Dent2001; 23: 245-248.
Figure 1. Patient with Peripheral Ossifying fibroma(POF) Figure 2. Lateral view-POF
A Localized Gingival Enlargement Gita Malathi, et, al.
Indian J Dent Adv 2011; 3(4): 711-714
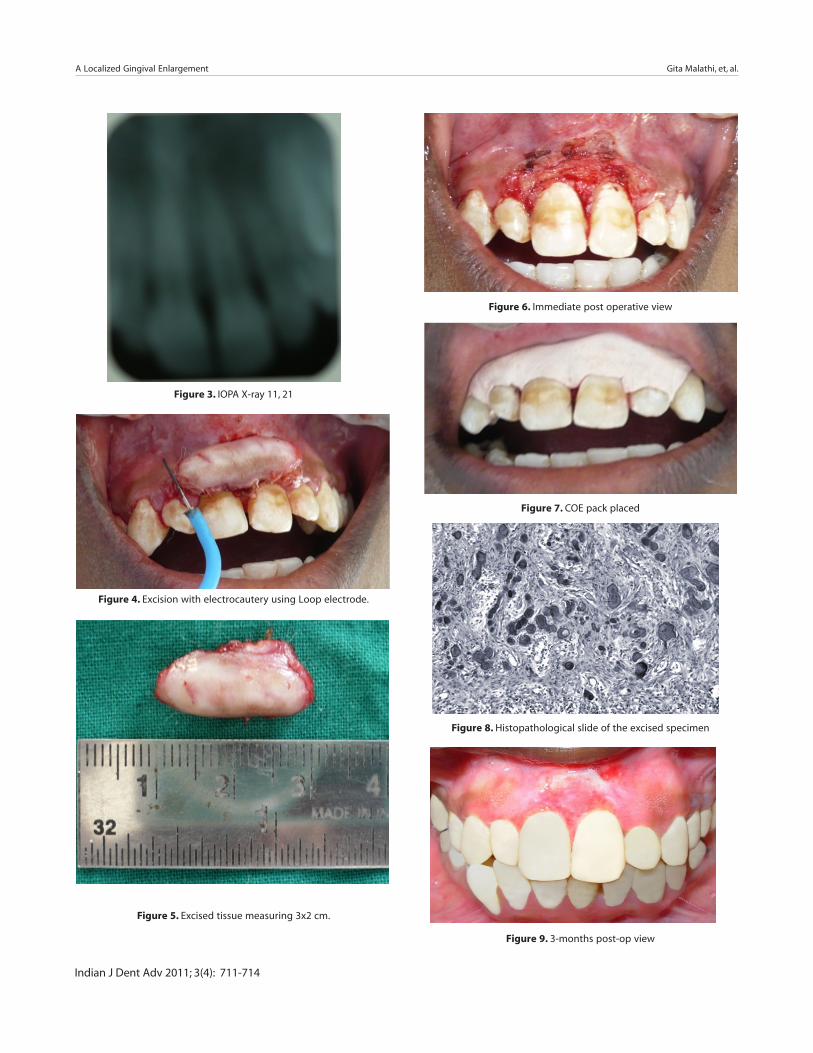
Figure 3. IOPA X-ray 11, 21
Figure 4. Excision with electrocautery using Loop electrode.
Figure 5. Excised tissue measuring 3x2 cm.
Figure 6. Immediate post operative view
Figure 7. COE pack placed
Figure 8. Histopathological slide of the excised specimen
Figure 9. 3-months post-op view
A Localized Gingival Enlargement Gita Malathi, et, al.
Indian J Dent Adv 2011; 3(4): 711-714