quest provider bulletin - 5/1/2008
TRANSCRIPT

Bulletin Q08-03 May 2008
A MessAge froM our MedicAl director
HMSA strives to update and maintain our QUEST formulary so that it will continue to facilitate high-quality and cost-effective health
care. In fact, our formulary includes more than the minimum formulary required by Med-QUEST.
Your suggestions for additions to the formulary are most welcome. HMSA has a formal mechanism to review and implement formulary changes (see HMSA QUEST Provider Bulletin Q06-02, April 3, 2006). In addition, I invite you to discuss your suggestions with me directly, in conjunction with or as a prelude to submitting a formal request. I may be able to help you review supporting scientific literature or other references, and work with HMSA pharmacists to evaluate and implement suggested additions.
I am best reached by email at [email protected]. I look forward to your suggestions.
Frank Smith, M.D.
oPeN eNrollMeNt PlAN cHANge Period
The annual plan change period is now underway. Last month, the Department of Human Services’ Med-QUEST office should have sent informational packets to members who are eligible to participate in the plan change process.
Members wishing to change QUEST plans, subject to any enrollment caps that may be initiated by Med-QUEST, must return the plan change form to Med-QUEST by the stated deadline on the form. No action is required for members wish-ing to remain with their existing QUEST plan. Changes will be effective beginning with services on July 1, 2008.
If your patients have any questions on the plan change pro-cess, please have them call our Member Service representatives at 948-6486 on Oahu or 1 (800) 440-0640 toll-free.
iN tHis issue: • A Message from Our Medical Director
• Open Enrollment Plan Change Period
• EPSDT Matters — Clinical Information Forms Required — TB Risk Assessment — TB Testing
— Blood Lead Testing for Children Not at Risk
— Dental Surveillance — Screening Tools
• Referral Registration
• Claims Filing Information
— Deadline for New Claim Forms
— Tuberculin Testing
• Benefit Policies
— 3D Reconstruction — Brachytherapy, Intravascular — Non-Ionic Contrast Agents — Spinal Cord Stimulators for
Pain Management
• Provider Handbook Updates
If you have any comments, questions or suggestions for our Bulletin, please call us at 948-6486 on Oahu or 1 (800) 440-0640 toll-free from the Neighbor Islands.
correctioN
The second bullet of Dr. Smith’s April message should have read:• Non-emergency health care for QUEST members
through age 18 years while traveling or visiting OOS. In addition, a non-medical attendant (an adult fam-
ily member) may be approved to accompany a child through age 18 years for approved OOS care.
HMSA Provider BulletinH M S A ’ S P l a n F o r Q U E S T M E M B E r S
P . o . B o x 3 5 2 0 , H o n o l u l u , H I 9 6 8 1 1 - 3 5 2 0 • o a h u 9 4 8 - 6 3 2 1 • n e i g h b o r I s l a n d s 1 ( 8 0 0 ) 7 7 1 - 0 6 7 7

Bulletin Q08-03 May 2008
2
clinical information forms required
In addition to providing important information on a patient’s health status, the clinical information forms are vital resources for data required to generate reports to the state and federal governments. All claims for EPSDT exams, whether regular screening or catch-up/follow-up exams, must be submitted with a fully completed and appropriate EPSDT form. Regular EPSDT screening ex-ams must be submitted with DHS Form 8015. Catch-up exams must be submitted with DHS Form 8016.
Effective July 1, claims for EPSDT exams, including the catch-up and follow-up visit exams, that are submitted without the valid DHS form or with forms that are not correctly completed will be denied. Please take the neces-sary steps to ensure that the required forms are properly completed and submitted with claims.
If you need assistance with the forms, we are more than happy to help. You can call QUEST Provider Service at 948-6486, or toll-free from the Neighbor Islands at 1 (800) 440-0640.
tB risk Assessment
An annual TB risk assessment is a required part of the surveillance for patients from 2 to15 months, and 2 to 20 years (see Periodic Screening Guidelines matrix in the QUEST Provider Handbook General InformatIon “EPSDT”). A verbal TB risk assessment satisfies this requirement.
The following three questions should be asked of the patient or parent to assess a patient’s risk:
1. Does anyone in the household have TB?
2. Is anyone in the household a recent immigrant from an area with endemic TB, such as Southeast Asia?
3. Does anyone in the household have an unexplained and/or prolonged (more than a few weeks) cough, fever, night sweats or weight loss?
Negative risk responses are not required to be noted on DHS Form 8015. However, be sure to document in the patient’s record that the risk assessment was done and
that the child is not at risk. If the answer to any of the above questions is “yes,”
it is expected that the appropriate referrals for diagnosis and care will be made.
tB testing
Testing is required at the ages specified on the Periodic Screening Guidelines matrix. The matrix is also printed on the back of DHS Form 8015. Please remember, the professional components the testing, such as administra-tion and reading the test results, are included as part of the EPSDT exam and are not separately payable. How-ever, the testing materials may be paid separately when billed with the NDC number. See the related article in the Claims Filing Information section of this Bulletin.
Blood lead testing for children Not at risk
The federal government requires that all children in the 9 to 12 month and 24 month age groups are tested for lead as part of their EPSDT exams even if the child is not at risk for elevated blood lead levels. This is not an op-tional test, and risk is not a factor in determining whether or not to test a child in this age group. To minimize trips to a lab for the 9 to 12 month age group, you may wish to do the hematocrit or hemoglobin at the same time.
Children in the 36 to 72 month age group must also be tested if they have not previously been tested at the earlier age requirements. For example, new QUEST enrollees who have not previously had EPSDT screening exams must be tested.
Please remember, you do not need to attach the Child Lead Risk Questionnaire to the lab requisition form.
dental surveillance
All patients must undergo a visual check of the mouth, teeth and/or gums as part of their EPSDT visit to deter-mine if there are any problems requiring a referral to a dental provider. Even young infants can benefit from this check to identify potential problems, such as baby bottle
ePsdt MAtters

Bulletin Q08-03 May 2008
3
clAiMs filiNg iNforMAtioN
tooth decay. These exams enable you to counsel the par-ent about oral habits and hygiene, and prescribe supple-mental fluoride as needed.
Please refer children who need dental services to their family dental practitioner for care. If the family does not have a dental provider or know where to go for care, the Community Case Management Corporation (CCMC) can help them find a dentist. You can call CCMC at 792-1070 or 1 (888) 792-1070 toll-free.
Need Help finding screening tools?
The Maternal and Child Health Library’s MCH Alert issued March 7, 2008, provided a link to a web-based manual developed by the Commonwealth Fund and based on a review of available developmental screening instru-ments. Pediatric Developmental Screening: Understanding and Selecting Screening Instruments is available at www.commonwealthfund.org/publications/publications_show.htm?doc_id=614864.
PCPs are required to register referrals for specialty care, except as listed under “Referrals” in the QUEST Provider Handbook General InformatIon. Coordinated efforts be-tween the PCP and the specialty provider help ensure that a patient receives specialty care and that claims for those services are paid.
To help this process work smoothly, we ask PCPs to
ensure you register referrals with us before the specialist submits the claim. Sometimes PCPs send the referral docu-ments to the specialist, but not to us, or sends them to us after we have already denied the specialist’s claim. This puts a burden on the specialty provider to then expend additional time and effort resolving these claim denials. Please help specialists by submitting timely referrals to us.
deadline for New claim forms is July 1.
Effective July 1, 2008, all claims must be submitted us-ing the CMS 1500 (08-05) version. Claims submitted on the old CMS 1500 claim form on or after July 1, 2008, will be returned.
Effective July 1, 2008, HMSA will no longer be accept-ing UB-92 forms from facilities for hard-copy claims. By that date, all hospitals and institutional providers must be submitting claims using the UB-04 (CMS-1450) form.
tuberculin testing
Skin testing is covered for adults once per benefit year and as needed for children. See “Tuberculin Testing/Treat-ment” in the General InformatIon section of the QUEST Provider Handbook for details.
The QUEST reimbursement for testing includes the ad-
ministration and the subsequent reading of the test results. An E&M charge for a visit for the sole purpose of reading the test result is not payable. In addition, when testing is done as part of an EPSDT exam for a child, the testing is considered part of the global fee paid for the exam and no separate payment is made for the testing.
QUEST pays for the material used for testing adults and children when billed with the national drug code (NDC). The material may be billed on the same claim as the test-ing for an adult, or the EPSDT exam for a child. When utilizing a multiple dose vial, bill for the units actually used. For example, a 5 ml multiple dose vial can provide up to 50 tests when the typical amount of 0.1 ml is given to patients. If 0.1 ml is used, the metric quantity billed must be 0.1 ml. Careful coding of the units will help prevent overpayments.
referrAl registrAtioN reQuired

BeNefit Policies 3d reconstruction
Beginning immediately, QUEST will cover medically necessary 3D renderings for certain clini-cal situations in association with computed tomography/magnetic resonance imaging, ultrasound, and echocardiography. Precertification is not required; however, the radiology report must in-clude medical necessity justification for the use of 3D rendering. Details for coverage and docu-mentation are provided on the attached updates to the QUEST Provider Handbook.
Brachytherapy, intravascular
Intravascular brachytherapy (IVB), including intracoronary brachytherapy (ICB), are covered under HMSA’s QUEST plan. Precertification is not required; however, documentation for the procedure, including operative reports and the treatment plan signed and dated by the physician, must be kept in the patient’s medical record and be made available to HMSA upon request. Cov-erage details are included in the attached update to the QUEST Provider Handbook.
Non-ionic contrast Agents
Beginning March 1, QUEST began applying the same criteria for non-ionic contrast agents used by HMSA’s private business plans. This service is no longer restricted to high risk indica-tions. An update to the QUEST Provider Handbook is attached.
spinal cord stimulators for Pain Management
The criteria and guidelines for coverage for the treatment of severe and chronic pain of the trunk or limbs that is refractory to all other pain therapies have been expanded and clarified on the attached update to the QUEST Provider Handbook. Precertification continues to be required, for both the implantation of a temporary electrode and before permanent implantation of the stimulator.
4
Bulletin Q08-03 May 2008

Bulletin Q08-03 May 2008
5
PROVIDER HANDBOOK uPdAtesThe following sections of the QUEST Provider Handbook have been updated to clarify
procedures, correct minor typographical errors, or update codes. Please add the new sections alphabetically and replace outdated pages.
general information
• Facility Role in Providing Technical Services for Procedures Requiring Precertification (add new section)
• HMSA’s Business Association with NIA (add new section)
Benefit Policies
• 3D Reconstruction (add new policy)
• Bone (Mineral) Density Studies (replace entire policy)
• Bortezomib (Velcade) (replace entire policy)
• Brachytherapy, Intravascular (add new policy)
• Continuous Glucose Monitoring of Interstitial Fluid (replace entire policy)
• Coronary CT Angiography (CCTA) Pilot Pro-gram (replace policy)
• Efalizumab (Raptiva) (replace entire policy)
• Etanercept (Enbrel) for the Treatment of Psoriasis (replace entire policy)
• Genetic Testing (Keep exisiting policy until 6/30/08 then replace with this new policy)
• Genetic Testing for Inherited BRCA1 or BRCA2 Mutations (add new policy)
• Home Apnea Monitor for Infants (replace entire policy)
• Home Phototherapy for Neonatal Jaundice (replace entire policy)
• Imaging Studies that Require Precertification (add new section)
• Imatinib Mesylate (Gleevec) (replace entire policy)
• Intrastromal Corneal Ring Segments for Keratoconus (INTACS) (replace entire policy)
• Leuprolide Acetate (Lupron) (replace entire policy)
• MRI, Functional (add new policy)
• Non-ionic Contrast Agents (replace entire policy)
• Oscillatory Device for Bronchial Drainage (The Vest) (replace policy)
• Outpatient Surgical Procedure Related Group (PRG) List (replace entire list)
• Physician Responsibility for Obtaining Precerti-fication of Imaging Studies (add new section)
• Place of Treatment Program – Office Procedures List (replace entire list)
• Place of Treatment Program – Outpatient Procedures List (replace entire list)
• Spinal Cord Stimulators for Pain Management (replace policy)
• Sunitinib (Sutent) (replace entire policy)
• Transcutaneous Electrical Nerve Stimulation (TENS) (replace entire policy)
• Vacuum Assisted Breast Biopsy (replace updated page)
Quick reference
• Radiology Management – Quick Reference Guide (add new section)


Radiology Management – Quick Reference Guide
QUEST Provider Handbook Quick Reference Guide 05/08
To promote the appropriate utilization of advanced diagnostic imaging in cases where traditional imaging would provide sufficient diagnostic information to treat the member or where another imaging study would be more appropriate based on the patient’s condition, HMSA has contracted with National Imaging Associates, Inc. (NIA) to assist by providing pre-certification services for MRI, MRA and PET scans that do not meet guidelines. The NIA’s role in pre-certifying MRI, MRA and PET services is effective October 16, 2006. For more information see: HMSA’s Business Association with NIA – (in the General Information section) Imaging Studies that Require Pre-certification – (in the Benefit Policies section) Physician Responsibility for Obtaining Pre-certification of Imaging Studies – (in the Benefit Policies section) Facility Role in Providing Technical Services for Procedures Requiring Pre-certification – (in the General Information section) HMSA Diagnostic Imaging Guidelines – (refer to Physicians Responsibility for Obtaining Pre-certification of Imaging Studies; in the Benefit Policies section) Magnetic Resonance Imaging – (in the Benefit Policies section) Positron Emission Tomography (PET) – (in the Benefit Policies section) Magnetic Resonance Angiography (MRA) and Magnetic Resonance Venography (MRV) – (in the Benefit Policies section)


F Facility Role in Providing Technical Services for Procedures Requiring Pre-certification
(Continued on Next Page) QUEST Provider Handbook General Information 05/08
I. It is the responsibility of the ordering physician to obtain pre-certification for imaging studies.
II. It is in the best interest of facilities providing diagnostic imaging services to develop internal processes to ensure that pre-certification has been obtained, when needed, for the services they provide.
A. The facility should verify that pre-certification for outpatient diagnostic imaging has been
obtained, when required. Pre-certification is required for:
1. MRIs and MRAs that do not meet guidelines
2. PET scans that do not meet guidelines (Note: It is suggested that NIA input be sought for all PET services.)
B. Pre-certification is not required for MRI, MRA or PET services when performed in the
emergency department or observation room, or for services performed on an inpatient basis. III. If more than one procedure requiring pre-certification is planned, a separate pre-certification
number is required for each procedure ordered. IV. The following suggestions may assist facility staff and prevent denials of claims for services that
have not been pre-certified or of claims for services for which pre-certification was denied.
A. Communicate to all personnel involved in outpatient scheduling that pre-certification is required for the MRI, MRA and PET scans that do not meet HMSA Diagnostic Imaging Guidelines.
B. If a physician’s office calls to schedule a patient for a procedure requiring pre-certification,
the facility should request the pre-certification number.
C. If a physician’s office has not obtained pre-certification, the facility should inform them of this requirement and advise them to call National Imaging Associates, Inc. (NIA), toll free, at 1 (866) 306-9729.
1. The facility may elect to give the provider a tentative schedule for the test, but institute a
time period for the physician to call back with the pre-certification number (e.g., one or two business days), or
2. The facility may wish to tell the provider that it will schedule the test after pre-
certification has been obtained.
3. In an urgent situation, it is recommended that the facility schedule the test as soon as possible, but remind the ordering physician that pre-certification must be obtained the following business day.

QUEST Provider Handbook General Information 05/08
D. If a member calls to schedule an appointment for a procedure that requires pre-certification and does not have the pre-certification number, the patient should be directed back to the ordering physician.
V. Facilities will be able to check the status of a pre-certification request by logging on to the NIA
Web site at www.RADMD.com. Review RadMD Get Started instructions and refer to the RadMD Quick Start Guide to request an exam.
VI. If pre-certification is denied because the services are determined not to be medically indicated,
payment will not be made. The facility may not bill the member for the denied services, except in cases where the member has been informed of the pre-certification denial, has agreed to be financially responsible for the charges, and has signed an Agreement of Financial Responsibility - Medical prior to the services being rendered.
VII. If pre-certification was not sought or given prior to services being performed, the claim will be
subject to review. HMSA will seek additional information from the ordering physician and will review the claim based on the information provided. If the information provided by the ordering physician does not meet criteria for coverage, benefits will be denied for the services. Neither the facility nor the radiologist may bill the member for the denied services.
VIII. A pre-certification number from NIA does not guarantee HMSA payment. Payment is subject to
plan benefits and deductibles, any applicable waiting periods and member eligibility at the time of service.

H HMSA’s Business Association with NIA
QUEST Provider Handbook General Information 05/08
I. Effective October 16, 2006, to ensure appropriate utilization of advanced diagnostic imaging services in cases where traditional imaging would provide sufficient diagnostic information to treat the member or where another study would be more appropriate based on the patient’s condition, HMSA has contracted with National Imaging Associates, Inc. (NIA) to provide outpatient imaging management services.
A. NIA is experienced in the field of radiology management and has a client base that includes
several Blue Cross and Blue Shield Plans, Aetna, and Humana – covering more than 18 million lives.
B. NIA is certified by both NCQA and URAC in utilization management.
C. NIA is accredited by URAC for HIPAA privacy and security and holds NCQA’s Privacy
Certification for Business Associates.
II. Under the terms of the agreement, HMSA retains claims adjudication functions, as well as oversight of the program, including medical policies and procedures. NIA will be responsible for managing the pre-certification of MRA, MRI and PET scans that do not meet guidelines.
III. NIA has also provided clinical guidelines adapted to HMSA needs and specifications (see HMSA
Diagnostic Imaging Guidelines). IV. For more information about NIA, see www.RADMD.com.


3D 3D Reconstruction
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
I. Description In 2005, both 2D and 3D postprocessing were reported using CPT code 76375. In 2006, 76375 was deleted and replaced by two codes, 76376 and 76377, specific for 3D rendering. These codes differ based on how the postprocessing is done. 3D postprocessing performed on the modality console by a technologist is reported as 76376 and postprocessing performed on an independent workstation is coded using 76377. It is generally accepted that the 76377 studies are the more complex examinations requiring significant physician input for generating the models. The new 3D codes require concurrent physician supervision of image post-processing, 3D manipulation of volumetric data sets and image rendering. 2D reconstructions are considered part of the base procedure code and should not be reported separately as of January 1, 2006.
The code description for each of these CPT codes is as follows:
76375 Coronal, sagittal, multiplanar, oblique, 3-dimensional and/or holographic
reconstruction of computed tomography, magnetic resonance imaging, or other tomographic modality
76376 3D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality, not requiring image postprocessing on an independent workstation
76377 3D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality; requiring image postprocessing on an independent workstation
With this change, coronal, sagittal, oblique, multiplanar and tomographic renderings are no longer separately billable (there is no longer a code for these procedures). The 2006 codes are specifically for 3D reconstruction.
II. Criteria/Guidelines
A. 3D renderings may be considered medically necessary in the following clinical situations*:
1. Computed tomography/magnetic resonance imaging:
a. Complicated multi-fragmented pelvic fractures (e.g., comminuted) or congenital skeletal deformities when ordered by the orthopedic surgeon to plan a surgical approach determine the need for requisite hardware and/or determine the most appropriate reduction approach.
b. Renal/ureteral masses, strictures, or congenital anomalies when ordered by the
urologist/general surgeon to evaluate the need for or the approach to surgery, or in the evaluation and work-up of hematuria (including CTIVP).
c. Complex oncology cases when ordered by the surgeon to assess for resectability
and/or reconstruction.
2. Ultrasound:
CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies 05/08
a. Evaluation of intrauterine fetal anomalies when the 3D images are used to plan appropriate prenatal or perinatal interventions.
3. Echocardiography:
a. Evaluation of cardiac masses and congenital abnormalities when ordered by a cardiologist or cardiac surgeon for surgical planning.
*Note: A separate report must be provided.
B. Prior to 2006, an order for 2D and 3D reconstruction imaging was not necessary. However, based on the over utilization and routine use, there must be an order from the referring physician, or radiologist. There must be medical necessity justification for the use of 3D rendering in the radiology report in order to make a separate charge under 76376 or 76377.
C. The 3D codes (76376 and 76377) should be reserved for situations where additional imaging is
necessary for surgical planning or for complete depiction of an abnormality from the two-dimensional study.
III. Limitations/Exclusions
A. HMSA will not pay separately for 3D rendering in the following situations:
1. When billed with codes with which 76376 and 76377 should not be separately reported.
2. When conventional imaging study results are normal, non-complex or non-surgical, or have what are considered incidental findings.
3. When 2D reformatting is able to resolve the clinical question(s).
4. When contiguous body parts are imaged, the technical component for 76376 and/or
76377 will be paid only once (i.e., abdomen and pelvis).
5. When only 2D multiplanar reconstruction is done.
B. Payment will be made for 76377 when both 76376 and 76377 are billed, per study.
C. 3D reconstruction will not be paid with a CTA or MRA study.
D. According to CPT guidelines, 76376 and 76377 are not to be reported in association with the following codes:
1. CTA head 70496
2. CTA neck 70498
3. MRA head 70544-70546
4. MRA neck 70547-70549
5. CTA chest 71275

3D 3D Reconstruction (continued)
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
6. MRA chest 71555
7. MRA spinal canal 72159
8. CTA pelvis 72191
9. MRA pelvis 72198
10. CTA upper extremity 73206
11. MRA upper extremity 73225
12. CTA upper extremity 73706
13. MRA lower extremity 73725
14. CTA abdomen 74175
15. MRA abdomen 74185
16. CTA abdominal aorta 75635
17. Radiopharmaceutical localization of tumor through unlisted procedure, diagnostic nuclear medicine 78800-78999
18. CT colonoscopy 0066T, 0067T
19. CT heart 0144T-0151T
E. 3D reconstruction codes should not be used for radiation oncology. The correct code for
radiation tomography guidance for the placement of radiation therapy fields is 76370.
F. CPT codes 76376 and 76377 may be considered medically unnecessary and denied if equivalent information to that obtained from the test has already been provided by another procedure (magnetic resonance imaging, ultrasound, angiography, etc.) or could be provided by a standard CT scan (two-dimensional) without reconstruction.
IV. Administrative Guidelines
A. Pre-certification is not required. Documentation supporting the medical necessity should be legible, maintained in the patient's medical record and must be made available to HMSA upon request.
1. The written request for the study from the referring physician should also be kept in the
patient’s medical record. If done on an urgent basis without a referral, the 3D report should document the time of the study, the specific need for the study and the summary of the findings that were urgently transmitted to the practitioner named as the referring physician. This documentation must be maintained by the radiologist and made available to HMSA upon request.

QUEST Provider Handbook Benefit Policies 05/08
V. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. Alcazar J, Garcia-Manero M, Galvan R. Three-Dimensional Sonographic Morphologic Assessment of Adnexal Masses A Reproducibility Study. J Ultrasound Med 2007; 26:1007-1011.
2. April 2006. Hospital Quadrant Meeting Handouts. Blue Cross and Blue Shield of Kansas A
CMS Contracted Intermediary. http://www.kansasmedicare.com/part_A/manuals/handouts/quadrant/
3. Ciesielczyk M, Drozdz J, Krzeminska-Pakula M, Plewka M, Zwierzak M, Wierzbowska K,
Kasprzak JD. Clinical application of 3-dimensional echocardiography: a 3-year single center experience. Przegl Lek. 2002; 59(8):658-62.
4. Coakley F, Yeh B, Breiman R, Qayyum A. What’s New in Abdominal Imaging Three-
Dimensional CT. Department of Radiology University of California San Francisco School of Medicine, San Francisco, CA. Last updated November 17, 2004. Accessed September 2007. Available at URL address: http://www.radiology.ucsf.edu/research/04abdo_news.shtml.
5. Current Procedural Terminology (CPT) 2007 Standard Edition. American Medical
Association.
6. John NW, McCloy RF. Navigating and Visualizing Three-Dimensional Data Sets. The British Journal of Radiology, 77, 2004: Pages S108-S113.
7. LCD for 3D Interpretation and Reporting of Imaging Studies - X-45B (L24941). TrailBlazer
Health Enterprises, LLC. Effective 5/17/07.
8. Myers S, Fresquez M, Hamill N. Four-Dimensional Sonography of the Fetal Heart With Spatiotemporal Image Correlation Directed at the Interventricular Septum. J Ultrasound Med 2007; 26:1071-1075.

B Bone (Mineral) Density Studies
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description A bone mineral density study is a non-invasive technique that is used to measure bone mineral content and bone mineral density. Its primary role is to detect osteoporosis and to predict the risk of fractures. The most commonly used bone densitometry techniques include single energy x-ray absorptiometry (SEXA), dual energy x-ray absorptiometry (DEXA), ultrasonic bone densitometry, photodensitometry, and quantitative computed tomography (QCT).
Osteoporosis is a disease that results in the loss of bone mineral content or bone density. This leads to thinning and weakening of bones and problems such as increase risk of fractures and pain. Individuals with osteopenia have sustained some bone loss and may be at risk for further loss. Primary osteoporosis is usually related to age deficient calcium intake, early menopause, smoking, sedentary life-style without adequate exercise, and a familial history of the disease.
While central or peripheral techniques may be used for bone mass measurement, in the medical community there is a consensus that central DEXA is the most widely used method. If serial monitoring is considered, a central DEXA should be the initial bone mineral density test performed in patients at high risk for osteoporosis.
II. Criteria/Guidelines
A. A baseline BMD study is covered for the following individuals considered to be at high risk for low bone mass and future fractures, (subject to Limitations/Exclusions and Administrative Guidelines):
1. Women 65 years of age or older regardless of risk factors.
2. For postmenopausal women with any of the following risk factors:
a. History of a nontraumatic fracture after age 45 in a first-degree relative.
b. Body weight of less than 127 lbs or BMI of 20 or less.
c. Current smoker.
d. Surgical menopause or natural menopause before age 40.
3. Men 70 years of age or older regardless of risk factors.
4. Men or women with suspected osteoporosis associated with the following conditions:
a. Endocrine disorders:
i. Cushing’s syndrome
ii. Male or female hypogonadism
iii. Hyperthyroidism
iv. Primary hyperparathyroidism

QUEST Provider Handbook Benefit Policies Rev. 05/08
b. Rheumatologic disorders:
i. Ankylosing spondylitis
ii. Juvenile polyarticular arthritis
iii. Rheumatoid arthritis
c. Malignancy:
i. Leukemia
ii. Multiple myeloma
iii. Systemic mastocytosis
d. Primary biliary cirrhosis
e. Chronic renal failure
f. Gastrointestinal disease:
i. Celiac disease
ii. Inflammatory bowel disease (Crohn’s disease in particular)
g. Prolonged immobilization
5. Men or women on a prescribed drug regimen receiving any of the following:
a. Anticonvulsants
b. Glucocorticoid excess equivalent to 5.0 mg of prednisone or greater per day for over three months.
c. Aromatase inhibitors
d. Chemotherapy (methotrexate or other antimetabolites)
e. Depo-medroxy progesterone acetate (Depo-Provera)
f. Gonadotropin-releasing hormone (GnRH) agonists (buserelin, leuprolide,
nafarelin)
6. Premenopausal women with amenorrhea greater than one year.
7. Solid organ or allogenic bone marrow transplant recipients (men or women).

B Bone (Mineral) Density Studies (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
8. Men or women with vertebral abnormalities (shown in x-ray) indicative of osteoporosis, osteopenia or vertebral fracture or has had a prior fracture with minor trauma (fall from standing height or less).
9. Children with a disease or condition associated with bone loss or on prolonged
medications that are known to decrease bone mass. III. Limitations/Exclusions
A. A repeat BMD study to monitor response in patients with osteopenir or osteoporosis is limited to one every 24 months.
B. Follow up BMD studies for patients who met criteria in II.1-9 without osteopenia or
osteoporosis is limited to one every three years.
C. Repeat BMD studies performed more frequently than once every two years is limited to individuals on glucocorticoid (steroid) therapy equivalent to 5.0 mg or more of prednisone per day for more than three months, with pre-certification.
D. Clinicians are encouraged to use the same modality for initial and follow-up testing for greater
consistency.
E. Dual Photon Absorptiometry (DPA) and images obtained during a BMD study (e.g., rapid vertebral assessment) are not covered.
IV. Administrative Guidelines
A. Pre-certification is required for patients under the age of 18. To pre-certify, please complete HMSA’s Pre-certification Request form and mail or fax the form as indicated. The request must include supporting documentation from the patient’s medical records with the high risk indications that would justify a BMD study as well as the proposed therapy for the patient.
B. Pre-certification is required for follow up studies performed more frequently than once every
two years. Requests must include the previous BMD study results, other pertinent test findings and a medication list.
C. Compliance with the provisions in this policy is subject to monitoring and post payment data
analysis and subsequent medical review. The following documentation should be kept in the patient’s medical records and made available upon request.
1. Clinical indications to substantiate that procedure is reasonable and necessary should be
indicated in medical record.
2. Physician’s order signed (not rubber stamped) and dated (MM/DD/YY).
3. The acute diagnostic evaluation documenting symptoms, other diagnostic X-rays, and physical exam findings must have been dated at a time reasonably proximate to the scan.
4. The name and medication regimen for patients undergoing drug therapy.

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies Rev 05/08
D. If a patient does not meet HMSA’s guidelines for coverage but has indicated that he or she wants the services performed despite noncoverage, the patient should be asked to sign HMSA’s Bone Density Waiver Form. This signed waiver indicates that the patient will be responsible for the denied charges.
1. When submitting a claim for a BMD study that does not meet HMSA guidelines, append
modifier code GA to the CPT code for the service. The use of the GA modifier will alert HMSA that the claim should be processed to indicate that the patient will be financially responsible for the service, and that the noncovered charges should not be a provider adjustment.
2. The signed waiver should be kept in the patient’s record. HMSA reserves the right to
conduct periodic audits on claims submitted with the GA modifier and review medical records for signed waivers for this service.
CPT Code Description 76977 Ultrasound bone density measurement and interpretation, peripheral site(s),
any method 77078 Computed tomography bone mineral density study, one or more sites; axial
skeleton (e.g., hips, pelvis, spine) 77079 appendicular skeleton (peripheral) (e.g., radius, wrist, heel) 77080 Dual energy X-ray absorptiometry (DXA), bone density study, one or more
sites; axial skeleton (e.g., hips, pelvis, spine) 77081 appendicular skeleton (peripheral (e.g., radius, wrist, heel) 77083 Radiographic absorptiometry (e.g., photodensitometry, radiogrammetry),
one or more sites 78350 Bone density (bone mineral content) study, one or more sites; single photon
absorptiometry
HCPCS Code Description G0130 Single energy X-ray absorptiometry (SEXA) bone density study, one or
more sites; appendicular skeleton (peripheral) (e.g., radius, wrist, heel)
ICD-9-CM Code Description 252.00 – 252.08 Disorders of parathyroid gland 255.0 Cushing’s syndrome 255.3 Other corticoadrenal overactivity 256.2 Postablative ovarian failure 256.31 Premature menopause 256.39 Other ovarian failure 256.9 Unspecified ovarian dysfunction 257.2 Other testicular hypofunction 259.3 Ectopic hormone secretion, not elsewhere classified (includes ectopic
hyperparathyroidism) 345.00 – 345.91 Epilepsy 579.0 Celiac disease 585.3 Chronic kidney disease, Stage III (moderate)

B Bone (Mineral) Density Studies (continued)
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev 05/08
ICD-9-CM Code Description 585.4 Stage IV (severe) 585.5 Stage V 588.0 Renal osteodystrophy 588.81 Secondary hyperparathyroidism (of renal origin) 588.89 Other specified disorders resulting from impaired renal function 626.0 Absence of menstruation 627.2 – 627.9 Menopausal and postmenopausal disorders 714.0 Rheumatoid arthritis 720.0 Ankylosing Spondylitis 733.00 – 733.09 Osteoporosis 733.13 Pathologic fracture of vertebrae (includes collapse of vertebra NOS) 733.90 Disorder of bone and cartilage, unspecified 737.10 – 737.19 Kyphosis (acquired) 737.20 – 737.29 Lordosis (acquired) 737.30 Scoliosis (kyphoscoliosis), idiopathic 758.6 Gonadal dysgenesis (includes Turner’s syndrome) 805.00 – 806.09 Fracture, vertebral column E932.0 Adrenal cortical steroids (cortisone derivatives, desoxycorticosterone
derivatives, fluorinated corticosteroids). To be used with ICD-9-CM 733.09 for reporting an individual receiving (or expecting to receive) glucocorticoid therapy equivalent to 7.5 mg of prednisone, or greater, for more than three months.
E932.2 Ovarian hormones and synthetic substitutes. To be used with ICD-9-CM V58.69 for reporting an individual receiving long term Depo Provera injections.
V58.65 Long term (current) use of steroids V58.69 Long-term (current) use of other medications (includes high-risk
medications). To be used for reporting individuals on long-term chronic corticosteroids or Depo Provera (E932.0 should be added as a secondary diagnosis for corticosteroids and E932.2 should be used for Depo Provera.)
V67.51 Following completed treatment with high-risk medication, not elsewhere classified. To be used for reporting an individual who has completed drug therapy for osteoporosis and is being monitored for response to therapy.
V67.59 Following other treatment. To be used for reporting an individual who is receiving ongoing drug therapy for osteoporosis and is being monitored for effectiveness.
V82.81 Special screening for other conditions, osteoporosis
Non-Covered Procedure Code
CPT Code Description 78351 Bone density (bone mineral content) study, one or more sites; dual photon
absorptiometry, one or more sites 77082 Vertebral fracture assessment

QUEST Provider Handbook Benefit Policies Rev 05/08
V. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. American Association of Clinical Endocrinologists. Medical guidelines for clinical practice for the prevention and management of postmenopausal osteoporosis. Endocrine Practice. Vol 9, No. 6 November/December 2003.
2. Blue Cross and Blue Shield Association. Bone density studies. Medical Policy Reference
Manual. #6.01.01. April 2007.
3. Centers for Medicare & Medicaid Services. LCD for Bone (Mineral) density studies. (L23649) Effective 4/1/2007.
4. Diagnosis of osteoporosis in men, premenopausal women, and children. J Clin Densitom 2004
spring; 7 (1):17-26. [82 references]
5. FDA Talk Paper. Black box warning added concerning long-term use of Depo-Provera contraceptive injection. November 17, 2004.
6. Institute for Clinical Systems Improvement (ICSI). Health care guidelines, Diagnosis and
treatment of osteoporosis. July 2006.
7. U.S. Preventive Services Task Force. Screening for Osteoporosis in Postmenopausal Women: Recommendations and Rationale. September 2002. Agency for Healthcare Research and Quality, Rockville, MD.
8. Ward L, et al; Bisphosphonate therapy for children and adolescents with secondary
osteoporosis. Premedline identifier 17943849. Cochrane database sys rev. 2007.

B Bortezomib (Velcade)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Bortezomib (Velcade) is the first in a new class of anti-cancer agents known as proteasome inhibitors. The proteasome is an enzyme complex that exists in all cells and is responsible for the degradation of proteins that controls the cell cycle and cellular processes. By blocking the proteasome, bortezomib disrupts numerous biologic pathways, including those related to the growth and survival of cancer cells and induces apoptosis. Bortezomib causes cancer cells to be more vulnerable to the killing effects of chemotherapy in refractory cells. Bortezomib is an injectable and is currently FDA approved for patients with multiple myeloma who have received at least one prior therapy and for patients with mantle cell lymphoma who have received at least one prior therapy.
II. Criteria/Guidelines
A. Bortezomib may be considered medically necessary when recommended by a hematologist/oncologist for the following indications:
1. For the treatment of refractory or relapsed multiple myeloma.
2. For the treatment of refractory or relapsed mantle cell lymphoma.
B. Refractory is defined as no longer responding to therapy. Relapsed is defined as the
reappearance of disease in the region of prior disease (recurrence) and/or in new regions (extension) after initial therapy and attainment of complete response.
III. Limitations/Exclusions
Bortezomib is not to be used for first line treatment. IV. Administrative Guidelines
A. Pre-certification is required. To pre-certify, please complete HMSA’s Drug Review Request and mail or fax the form as indicated.
B. Initial authorizations may be approved for up to six months.
C. Pre-certification extensions may be approved for an additional six months if there is a
documented response (i.e., no progression of tumor).
HCPCS Code Description J9041 Injection, bortezomib, 0.1 mg
ICD-9-CM Code Description 202.80 – 202.88 Other lymphomas 203.00 Multiple myeloma, without mention of remission
Note: Drugs should be billed separately from the administration using the applicable national drug code (NDC).
QUEST Provider Handbook Benefit Policies Rev. 05/08
V. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. FDA, Center for Drug Evaluation and Research. Label and approval history. Velcade, New or modified indication. Approved 12/08/06.
2. Millennium Pharmaceuticals, Inc. Velcade prescribing information. Cambridge, MA. Issued
December 2006.
3. Richardson PG, Barlogie B, Berenson J, et al. A phase II study of bortezomib in relapsed, refractory myeloma. N Engl J Med. June 26, 2003; 348(26): 2609-17.
4. The Medical Letter. July 21, 2003; 45(1161):57-58.
5. Thompson Micromedex USP DI Drug Information for the Health Care Professional.
Bortezomib (Systemic) 12/12/2006.
6. BlueCross BlueShield of Tennessee Medical Policy Manual. Bortezomib. Effective date 02/16/07.
7. O’Connor OA R, Wright J, Moskowitz C, et al: Phase II clinical experience with the novel
proteasome inhibitor bortezomib in patients with indolent non-Hodgkin’s lymphoma and mantle cell lymphoma. J Clin Oncol 2005; 23(4):676-684.
8. Lenz G, Dreyling M, Hiddemann W: Mantle cell lymphoma: established therapeutic options
and future directions. Ann Hematol 2004; 83:71-77.
9. Aetna Clinical Policy Bulletins. Number 0675 Bortezomib (Velcade). Reviewed 11/10/06.

B Brachytherapy, Intravascular
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
I. Description Intravascular brachytherapy (IVB) involves the temporary placement of radioactive substances, usually in the form of a thin catheter filled with radioactive seeds, a radioactive wire, or a balloon coated or filled with radioactive material, into previously cleared vessels at the site of restenosis. When used to treat lesions in the coronary arteries, the blood vessels that supply blood to the heart, IVB is referred to as intracoronary brachytherapy (ICB). The dose of radiation to the site of restenosis helps to reduce the proliferation of the vessel’s smooth muscle cells, preventing or delaying long-term occurrence of restenosis.
II. Criteria/Guidelines
A. Intracoronary brachytherapy using gamma or beta-emitting radiation may be considered medically necessary to treat restenosis of a previously placed bare-metal stent in a native coronary artery.
B. Intracoronary brachytherapy using gamma radiation only may be considered medically
necessary to treat in-stent restenosis of a non-native coronary artery (i.e., saphenous vein graft).
III. Limitations/Exclusions
Intravascular brachytherapy has not been shown to improve health outcomes in the following situations:
A. When used in conjunction with PTCA to reduce the risk of de novo restenosis, with or without
stent placement.
B. When used to treat or prevent restenosis of drug eluding stents.
C. When used to treat conditions of the femoropopliteal system. IV. Administrative Guidelines
A. Pre-certification is not required.
B. Documentation must be kept in the patient’s medical record. If the patient had a percutaneous transluminal coronary angioplasty (PTCA), the operative report should be included along with a treatment plan signed and dated by the physician. The medical records must be made available to HMSA upon request.
C. The following ICD-9-CM diagnosis codes are appropriate for intracoronary brachytherapy:
ICD-9-CM Code Description 411 – 414 Coronary atherosclerosis; code range 996.72 Other complications of internal (biological) (synthetic) prosthetic device,
implant and graft, due to other cardiac device, implant and graft

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies 05/08
D. Applicable CPT codes:
CPT Code Description 77263 Therapeutic radiology treatment planning: complex 77290-26 Therapeutic radiology stimulation-aided field setting; complex 77300-26 Basic radiation dosimetry calculation 77327-26 Brachytherapy isodose calculation; intermediate 77331-26 Special dosimetry 77336 Continuing medical physics consultation 77370 Special medical radiation physics consultation 77431 Radiation therapy management with complete course of therapy consisting
of one or two fractions only 77470-26 Special treatment procedure 77782-26 Remote afterloading high intensity brachytherapy; 5-8 source positions or
catheters 77783-26 Remote afterloading high-intensity brachytherapy; 9-12 source positions or
catheters 77784-26 Remote afterloading high-intensity brachytherapy; over 12 source positions
or catheters
Note: Modifier -26 appended to the above codes represents the professional component of the service.
E. Other applicable CPT codes:
CPT Code Description 92974 Transcatheter placement of radiation delivery device for subsequent
coronary intravascular brachytherapy. 92980 Transcatheter placement of an intracoronary stent(s), percutaneous, with or
without other therapeutic intervention, any method; single vessel 92981 each additional vessel (List separately in addition to code for primary
procedure) 92982 Percutaneous transluminal coronary balloon angioplasty; single vessel 92984 each additional vessel (List separately in addition to code for primary
procedure) 92995 Percutaneous transluminal coronary atherectomy, by mechanical or other
method, with or without balloon angioplasty, single vessel 92996 each additional vessel (List separately in addition to code for primary
procedure)

B Brachytherapy, Intravascular (continued)
QUEST Provider Handbook Benefit Policies 05/08
V. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR): Radiation Oncology Coding User’s guide 2001.
2. Blue Cross Blue Shield Association. Intracoronary brachytherapy for the prevention and
management of restenosis. TEC Assessment 2000.
3. Blue Cross Blue Shield Association. Intravascular brachytherapy for preventing and managing restenosis after Percutaneous Transluminal Angioplasty PTA. #2.02.11. Revised 08/02/07.
4. Medicare coverage database. LCD for Intracoronary brachytherapy (L23896). Effective
04/01/2007.
5. Mukherjee D and Moliterno DJ. Brachytherapy for in-stent restenosis: a distant second choice to drug-eluting stent placement. JAMA 2006; 295(11):1307-9.
6. Parikh SK, Nori D, et al. Practical consideration in setting up an intracoronary brachytherapy
program: Results of a multicenter survey. Radiology. Dec 2000; 217(3):723-728.
7. Stone GW, Ellis SG, O’Shaughnessy CD et al. Paclitaxel eluting stents vs. vascular brachytherapy for in-stent restenosis within bare metal stents. JAMA 2006; 295(11):1253-63.
8. Teirstein EM, Steuterman V, et al. Three-year follow-up after catheter-based radiotherapy:
Results of a randomized clinical trial. Circulation. Feb 2000; 101(4):360-365.
9. Vitali V, Youri P, et al. Endoluminal beta-radiation therapy for the prevention of coronary restenosis after balloon angioplasty. New Eng J of Med. Jan 25, 2001; 334(4):243-299.


C Continuous Glucose Monitoring of Interstitial Fluid
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Measurements of glucose in the interstitial fluid have been developed as a technique for automatically measuring glucose values throughout the day, producing data that show the trends in glucose measurements, in contrast to the isolated glucose measurements of the traditional blood glucose measurements.
The Medtronic MiniMed Continuous Glucose Monitoring system (CGMS) marketed under the trade name CGMS System Gold is an FDA-approved device used as a tool to supplement, not replace, blood glucose information obtained from standard home glucose monitors. The data collected by the MiniMed CGMS is processed on a computer and intended to provide adjunctive data to physicians who are interested in monitoring the daily fluctuations in their patients’ glucose levels. It is currently intended for one-time or occasional testing rather than ongoing daily use. It is comprised of a sensor which is implanted subcutaneously to record tissue glucose levels at five-minute intervals over a 24-hour period for up to three days (72 hours). The sensor is attached to a small plastic disk and taped to the skin to hold the sensor in place. A thin wire connects the sensor to a pager-sized glucose monitor, which records and stores glucose values in memory. The glucose values are not displayed and, thus cannot be used by the patient for self monitoring.
The Guardian REAL-Time Continuous Glucose Monitoring System also from Medtronic MiniMed is a provider prescribed device that is owned by the patient, and designed for use over extended periods of time to provide real-time glucose readings and alarms twenty four hours a day.
The MiniMed Paradigm REAL-Time Insulin Pump and Continuous Glucose Monitoring System integrate an insulin pump with real-time continuous glucose monitoring. The device allows the diabetic patient to be alerted to fluctuating glucose levels and then the patient must confirm the reading with a finger stick glucose measurement before activating the insulin pump to administer additional insulin. This policy does not pertain to the Paradigm insulin pumps which may be used independently of the glucose monitoring component of the Paradigm REAL-Time system. HMSA follows Medicare Region D criteria on the coverage of an insulin pump used alone.
The GlucoWatch G2 Biographer is a noninvasive device worn like a wristwatch. It measures glucose in the interstitial fluid through the skin with a constant low level electric current by the process of reverse iontophoresis.
II. Criteria/Guidelines
A. The MiniMed CGMS (CGMS System Gold) is eligible for coverage as a diagnostic test for patients who meet all of the following criteria:
1. Patients have not obtained acceptable diabetes control using home glucose monitoring
and aggressive insulin therapy.
2. Patients must be managed or co-managed by an endocrinologist who is experienced with the equipment and the interpretation of data from the continuous glucose monitoring system.
3. Patients with Type I diabetes.

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies Rev. 05/08
4. Patients who are monitoring their blood glucose four or more times per day (average).
5. Patients who either have Hgb A1c levels that are inconsistent with the glucose monitoring or frequent hypoglycemia or wide swings in blood glucose when on four shots of insulin a day.
6. The need for additional data from continuous glucose monitoring is clearly documented.
B. Special situations where coverage of the MiniMed CGMS (CGMS System Gold) may be
considered medically appropriate are as follows:
1. Patients on insulin pumps.
2. Pre-pregnancy patients and pregnancy control of Type I and Type II patients.
3. Patients with Type II diabetes on multiple dose insulin and otherwise meeting the above criteria would be considered on a case-by-case basis.
III. Limitations/Exclusions
A. For patients who meet the above criteria and patients on insulin pumps, MiniMed CGMS studies are limited to two studies in the first six months and two studies every two years thereafter.
B. Pre-pregnancy patients and pregnancy control of Type I and Type II patients may have up to
two MiniMed CGMS studies in the pre-pregnancy period and up to three studies during the pregnancy.
C. GlucoWatch (HCPCS codes S1030, S1031) is considered investigational as durable medical
equipment to monitor glucose levels for patients with diabetes based on the lack of clinical data demonstrating improvement in health outcomes.
D. Continuous use of real time monitors such as the Guardian REAL-Time or the Minimed
Paradigm REAL-Time system is considered investigational. Although FDA-approved, there is a lack of evidence demonstrating that the use of these devices is associated with an improvement in health outcomes.
IV. Administrative Guidelines
CPT Code Description 95250 Ambulatory continuous glucose monitoring of interstitial tissue fluid via a
subcutaneous sensor for up to 72 hours; sensor placement, hook-up, calibration of monitor, patient training, removal of sensor, and printout of recording.
95251 Ambulatory continuous glucose monitoring of interstitial tissue fluid via a subcutaneous sensor for up to 72 hours; physician interpretation and report.

C Continuous Glucose Monitoring of Interstitial Fluid (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Code Description 250.01 Diabetes mellitus; diabetes mellitus without mention of complication; type
I (juvenile type), not stated as uncontrolled 250.02 Diabetes mellitus; diabetes mellitus without mention of complication; type
II or unspecified type, uncontrolled 250.03 Diabetes mellitus, diabetes mellitus without mention of complication, Type
I, (juvenile type), uncontrolled 648.00 Diabetes mellitus, complicating pregnancy 648.03 Diabetes mellitus in the mother classifiable elsewhere but complicating
pregnancy-antepartum condition or complication
Pre-certification is not required for this service (see ICD-9-CM codes above). HMSA reserves the right to conduct retrospective review of these services. Documentation regarding medical necessity should be kept in the patient’s medical file.
V. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. Blue Cross Blue Shield Association. Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid. Medical Policy Reference Manual. Policy 1.01.20. Last reviewed 12/13/07.
2. Boland E, Monsod T, Delucia M, et al. Limitations of Conventional Methods of Self-
monitoring of Blood glucose: lessons learned from 3 days of continuous glucose sensing in pediatric patients with type I diabetes. Diabetes Care 2001 Nov; 24 (11): 1858-62.
3. Chase HP, Kim LM, Owen SL, et al. Continuous Subcutaneous Glucose Monitoring in
Children with Type I Diabetes. Pediatrics 2002; 107: 222-26.
4. Chase HP, Roberts MD, Wightman C, et al. Use of the GlucoWatch Biographer in Children with Type I Diabetes. Pediatrics 2003 April; 111(4 pt1): 885.

QUEST Provider Handbook Benefit Policies Rev. 05/08
5. ECRI Target Database. Real-time continuous glucose monitoring. March 2007.
6. FDA News: FDA Approves New Glucose Test for Adult Diabetics, March 22, 2001.
7. FDA News: FDA approves GlucoWatch Device for Children with Diabetes, August 27, 2002.
8. Kaufman FR, Gibson LC, Halvorson M, et al. A pilot study of the continuous glucose monitoring system: clinical decisions and glycemic control after its use in pediatric type I diabetes subjects. Diabetes Care 2001 Dec; 24(12): 2030-4.
9. Noridian Administrative Services, LLC. Article for Continuous Glucose Monitoring (A28892).
Effective 9/1/2000.

C Coronary CT Angiography (CCTA) Pilot Program
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
Policy is effective April 16, 2007 I. Payment arrangements for a new Coronary CT Angiography (CCTA) Pilot Program
Effective April 16, 2007 for a period of six months, HMSA will provide benefit coverage for coronary CT angiography (CCTA) under a pilot program. Note: The pilot program is extended through the end of the 2008 calendar year, through December 31, 2008.)
As part of the study, HMSA and NIA will also establish a patient registry and track patients in the registry using claims and other data. Reports will be generated to indicate at minimum, the number of CCTAs performed vs. the number of MPIs as the initial test, any subsequent tests ordered and their associated costs and the number of cardiac catheterizations performed on this population. The information gathered will then be reviewed by the CCTA workgroup previously engaged with HMSA on the concept of the pilot.
At this time, the exact role of CCTA in the spectrum of coronary diagnostic testing is not yet defined and the potential for layering of tests is a concern. While several national guidelines consider this service to be investigational, for purposes of this study, HMSA and NIA have adopted appropriateness guidelines based on the American College of Cardiology recommendations.
II. Participating providers for the pilot program
A. The pilot study will be conducted at these locations:
1. The Queen’s Medical Center
2. Straub Hospital & Clinic
3. Kapiolani Medical Center at Pali Momi
4. Pacific Cardiology
5. AccuImaging Pearlridge, LCC
6. Wahiawa General
B. CCTAs may only be ordered by participating cardiologists. III. Members eligible to participate in the pilot program
A. Members must meet the guidelines for admission into the pilot program. See HMSA CCTA Guidelines
IV. Use of the trial data
A. All data obtained during the project will be aggregated to ensure patient confidentiality.
B. Results will be used to determine the role of CCTA in the spectrum of coronary diagnostic testing.

QUEST Provider Handbook Benefit Policies Rev. 05/08
V. Excluded participants of the pilot program A. CCTA is contraindicated in patients with any of the following conditions (See HMSA CCTA
Guidelines for additional criteria):
1. Renal failure (creatinine >1.8, GFR < 40)
2. Severe allergy to iodinated contrast material
3. Inability to receive beta-blockers (e.g., Class 3 or Class 4 heart failure, significant aortic stenosis, significant asthma)
4. Sickle cell anemia or multiple myeloma
5. Irregular heart rhythm
6. Stent less than 3 mm in diameter
VI. Questions regarding the program
Physicians may comment on the guidelines by emailing Joan Kendall, M.D. ([email protected]) or by telephone at 948-5030.
For questions regarding operational issues, please contact Ione Fujio ([email protected]) or by telephone at 948-6551.
VII. Pre-certification Requirements
A. Pre-certification must be obtained by the ordering physician through NIA. (See Physician Responsibility for Obtaining Pre-certification of Imaging Studies.)
CPT Code Description 0146T Computed tomographic angiography of coronary arteries (including native
and anomalous coronary arteries, coronary bypass grafts), without quantitative evaluation of coronary calcium
0148T Cardiac structure and morphology and computed tomographic angiography of coronary arteries (including native and anomalous coronary arteries, coronary bypass grafts), without quantitative evaluation of coronary calcium
B. The ordering physician should have the information on the NIA Information Checklist -
Medical Practitioner readily available.
C. The ordering physician should also be prepared to answer the following questions:
1. Has the patient had a nuclear cardiology study within the past six months?
2. Why is the study being ordered?
3. Does the patient have new onset CHF?

C Coronary CT Angiography (CCTA) Pilot Program (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
4. Does the patient have chronic chest pain or chest pain syndrome (chest tightness, chest pain, chest burning, dyspnea, and shoulder or jaw pain)?
5. Does the patient have acute chest pain or angina?
6. Does the patient have three or more of the following conditions:
a. Age over 50
b. Diabetes
c. History of hypertension
d. History of LDL > 130
e. History of HDL < 35
f. Obesity (BMI > 35)
g. History of smoking
7. Does the patient have an equivocal or uninterpretable stress test (exercise, perfusion or
stress echo)?
8. Is this examination for noninvasive coronary arterial mapping, including internal mammary artery prior to repeat cardiac surgical revascularization, pacemaker placement, aorta or cardiac valve surgery or pulmonary vein ablation for treatment of atrial fibrillation?
D. NIA may also ask for the following information as needed to make a determination:
1. Clinical notes, BMI, serum creatinine or GFR
2. EKGs
3. Echo report
4. Prior test results
E. The facility may verify the status of the pre-certification request at www.radmd.com.

QUEST Provider Handbook Benefit Policies Rev. 05/08
VIII. References 1. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 Appropriateness Criteria for
Cardiac Computed Tomography and Cardiac Magnetic Resonance Imaging A Report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, Journal of the American College of Cardiology Vol. 48, No. 7, 2006 © 2006 by the American College of Cardiology Foundation.
2. Contrast-Enhanced Cardiac Computed Tomographic Angiography for Coronary Artery
Evaluation, BCBSA 2006 TEC Assessment: Tab 5.
3. Martin H, Hoffmann K, et al. Noninvasive coronary angiography with multi-slice computed tomography. JAMA. 2005; 293:2471-8.
4. Ropers D, Baum U, Pohle K, et al. Detection of coronary artery stenoses with thin-slice
multidetector row spiral computed tomography and multi-planer reconstruction. Circulation. 2003; 107:664-6.
5. US Nuclear Regulatory Commission. Exposure beyond this limit will disqualify an individual
from employment. http://www.nrc.gov/reading-rm/doc-collections/cfr/part020-1201.html Accessed January 2007.
6. http://www.coronaryctangio.com Accessed April 2006.

E Efalizumab (Raptiva)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Efalizumab (Raptiva) is a human monoclonal antibody that affects the activation and movement of T-cells, a type of immune system cell involved in the development of psoriasis symptoms. Efalizumab is a self-administered injectable indicated for the treatment of chronic plaque psoriasis.
II. Criteria/Guidelines
A. Efalizumab may be considered medically necessary when recommended by a dermatologist for the treatment of severe, chronic plaque psoriasis if all of the following criteria are met:
1. The patient is 18 years of age or older with severe, chronic, plaque psoriasis.
a. Severe psoriasis is defined as having more than 10 percent body involvement.
b. Chronic psoriasis is defined as a history of psoriasis for more than 12 months.
c. Plaque psoriasis is defined by well-defined patches of red and raised skin.
B. The patient has tried and failed or was intolerant to at least one other systemic therapy for
psoriasis (i.e., methotrexate, cyclosporine or oral retinoids, phototherapy). III. Administrative Guidelines
A. Pre-certification is required. To pre-certify, please complete HMSA’s Drug Review Request and mail or fax the form as indicated. Clinical notes must be included documenting the severity of the psoriasis (i.e., the percentage of body surface area involvement is over 10 percent) and the other treatments that have been tried and or failed.
B. Initial approvals will be given for up to three months.
C. Requests for extensions of efalizumab may be approved for up to 12 months. Documentation
must be submitted verifying a decrease in body surface area involvement compared to the initial baseline.
HCPCS Code Description S0162 Injection, efalizumab, 125 mg
ICD-9-CM Code Description 696.1 Other psoriasis
Note: Drugs should be billed separately from the administration using the applicable national drug
code (NDC).

QUEST Provider Handbook Benefit Policies Rev. 05/08
IV. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii's Patients' Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice, and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
V. References
1. Gauvreau GM, Becker AB, et al. The effects of an anti-CD11a mAb, efalizumab, on allergen-induced airway responses and airway inflammation in subjects with atopic asthma. J Allergy Clin Immunol. Aug 2003; 112(2): 331-338.
2. Gottlieb AM, Krueger JG, et al. Psoriasis as a model for T-cell-mediated disease:
immunobiologic and clinical effects of treatment with multiple doses of efalizumab, an anti-CD11a antibody. Arch Dermatol. May 2002; 138(5): 591-600.
3. Lebwohl M, Tyring SK, et al. A novel targeted T-cell modulator, efalizumab, for plaque
psoriasis. N Engl J Med. 2003; 349: 2004-2013.
4. Ortonne JP, Shumack S, Henninger E; CLEAR Multinational Study Group. Impact of efalizumab on patient-reported outcomes in high-need psoriasis patients: results of the international, randomized, placebo-controlled Phase II Clinical Experience Acquired with Raptiva (CLEAR) trial [NCT00256139]. BMC Dermatol, 2005 Dec 16;5:3
5. Raptiva (efalizumab) prescribing information. Genentech, Inc., San Francisco, CA, June 2005.
6. The Medical Letter. Efalizumab (Raptiva) for treatment of psoriasis. Dec. 8, 2003; 45(1171).
7. Woolacott N, Hawkins N et. al.: Etanercept and efalizumab for the treatment of psoriasis: a
systematic review. Health Technol Assess 2006; 10(46):1-252

E Etanercept (Enbrel) for the Treatment of Psoriasis
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Etanercept (Enbrel) is a self-administered drug that binds to and inhibits the activity of tumor necrosis factor TNF, a proinflammatory cytokine. TNF triggers an inflammatory process in response to injury or infection. Psoriasis is a chronic immune disorder in which certain immune cells become overactive and release cytokines. This leads to the formation of painful and often disfiguring psoriasis plaques. Etanercept blocks the activity of TNF resulting in a significant reduction in the inflammatory Process in patients with psoriasis.
II. Criteria/Guidelines
Etanercept for the treatment of psoriasis may be considered medically necessary when all of the following criteria are met:
A. The use of etanercept must be recommended by a dermatologist.
B. The patient is 18 years of age or older with severe, chronic plaque psoriasis.
1. Severe psoriasis is defined as having more than 10 percent body involvement.
2. Chronic is defined as a history of psoriasis longer than 12 months.
3. Plaque psoriasis is defined by well-defined patches of red and raised skin.
C. The patient has tried and failed at least one other systemic therapy for psoriasis (i.e.,
methotrexate, cyclosporine, oral retinoids, phototherapy) or the agents are contraindicated. III. Administrative Guidelines
A. Pre-certification is required. To pre-certify, please complete HMSA’s Drug Review Request and mail or fax the form as indicated.
B. Pre-certification is required for an initial three months of treatment. Patients may be eligible
for coverage when documentation shows ten percent or more body surface are involvement.
C. Requests for extensions of etanercept may be authorized for up to 12 months when documentation shows a decrease in percent body surface involvement when compared to baseline.
CPT Code Description J1438 Injection, etanercept, 25 mg
ICD-9-CM Code Description 696.1 Other psoriasis

QUEST Provider Handbook Benefit Policies 10/06
IV. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice, and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
V. References
1. Enbrel prescribing information. Amgen and Wyeth, Inc., Issue Date 12/1/06.
2. National Psoriasis Foundation. Biologic Treatments, Enbrel. Updated June 2006.

G Genetic Testing
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Genetic testing involves the analysis of human DNA, RNA, chromosomes, certain metabolites and proteins to detect heritable disease-related genotypes, mutations, phenotypes, or karyotypes for clinical purposes. Certain genetic molecular tests have been demonstrated to be of significant value in providing information with regard to diagnosis and treatment of a given condition. However, clinical usefulness of any genetic molecular test is dependent on the availability of specific, effective interventions to reduce risk or treat disease. When the results of a conventional test are inconclusive, the use of genetic molecular testing may add an additional measure of certainty to diagnosis, permitting refinement of clinical therapy.
For purposes of this policy first-degree relatives are defined as parents, full siblings, and offspring. Second-degree relatives are defined as grandparents, grandchildren, aunts, uncles, nephews, nieces, half-siblings and third-degree relatives are defined as great-grandparents, great aunts, great uncles, first cousins.
II. Criteria/Guidelines
A. Genetic testing will be covered (subject to Limitations/Exclusions and Administrative Guidelines) to establish a diagnosis of an inheritable disease when both of the following criteria are met:
1. The patient displays clinical features, or is at direct risk of inheriting the mutation in
question (pre-symptomatic).
2. The result of the test will directly impact the treatment being delivered.
B. BRCA1 and BRCA2 (See Genetic Testing for Inherited BRCA1 or BRCA2 Mutations – Effective July 1, 2008) policy.
C. Genetic testing to determine carrier status of the adenomatous polyposis coli (APC) gene will
be covered (subject to Limitations/Exclusions and Administrative Guidelines) when one of the following criteria is met:
1. The patient has more than 20 colonic polyps; or
2. The patient is the first-degree relative (i.e., sibling, parent, offspring) of a person
diagnoses with familial adenomatous polyposis
D. Genetic testing to determine the carrier status of the hereditary nonpolyposis colorectal cancer (HNPCC) gene will be covered (subject to Limitations/Exclusions and Administrative Guidelines) for patients with a history or colorectal cancer who meet either the Amsterdam II or the revised Bethesda criteria as described below:
1. Amsterdam II criteria (the patient must meet all of the following):
a. Three or more relatives with a histologically verified HNPCC associated cancer
(colorectal cancer or cancer of the endometrium, small bowel, ureter or renal pelvis), one of whom is a first-degree relative of the other two.

QUEST Provider Handbook Benefit Policies Rev. 05/08
b. HNPCC-associated cancer involving two generations.
c. Cancer in one or more affected relatives diagnosed before the age 50.
d. Familial adenomatous polyposis should be excluded in cases of colorectal cancer.
2. Modifications on the criteria listed above allow for small HNPCC families: these families must have two colorectal cancers in first degree relatives involving at least two generations, with at least one individual diagnosed by age 55.
3. Revised Bethesda criteria (patients must meet one of the following):
a. Patients diagnosed with colorectal cancer before age 50.
b. Patients with HNPCC-related cancer, including synchronous and metachronous
colorectal cancers or associated extracolonic cancers* regardless of age.
c. Patients with colorectal cancer with the MSI-H (high microsatellite instability) histology diagnosed before the age of 60.
d. Patients with colorectal cancer and one or more first- degree relatives with
colorectal cancer and/or HNPCC-related extracolonic cancer*, if one of the cancers was diagnosed at or before the age of 50.
e. Patients with colorectal cancer and colorectal cancer diagnosed in two or more
first- or second- degree relatives with HNPCC-related tumors, regardless of age.
* Extracolonic cancers include stomach, bladder, ureter, and renal pelvis, biliary tract, brain (usually glioblastoma), pancreas, sebaceous gland adenomas, keratocanthomas, carcinoma of the small bowel, endometrial, or ovarian cancer.
E. The microsatellite instability (MSI) test and the immunohistochemistry (IHC) test for
expression of MLH1 and MSH2 will be covered (subject to Limitations/Exclusions and Administrative Guidelines) as a means of identifying which members with colon cancer, who also meet the Amsterdam II or the Bethesda criteria, should undergo HNPCC genetic testing. MSI and IHC testing may provide additional information when HNPCC genetic testing is inconclusive.
F. Genetic testing to determine the carrier status of the HNPCC gene will be covered (subject to
Limitations/Exclusions and Administrative Guidelines) for members without a history of colorectal cancer but who have a first- or second-degree relative with a known HNPCC mutation. (See I. for genetic risk assessment information). risk assessments must meet the following criteria:
G. Genetic testing for cystic fibrosis (CF) will be covered (subject to Limitations/Exclusions and
Administrative Guidelines) with pre-certification for the following high risk individuals:
1. Patients with a positive family history of CF, limited to first- or second-degree relative.

G Genetic Testing (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
2. Reproductive partner of an individual with CF.
3. Patients with a first-degree relative identified as a CF carrier.
H. Genetic testing for congenital Long QT Syndrome (LQTS) will be covered (subject to Limitations/Exclusions and Administrative Guidelines) with pre-certification for patients who do not meet the clinical criteria for LQTS but have one of the following:
1. A first- or second-degree relative with a known LQTS mutation.
2. A first- or second-degree relative diagnosed with LQTS by clinical means whose genetic
status is unavailable.
3. Signs and/or symptoms indicating a moderate to high pretest probability of LQTS, defined as a Schwartz score of 2-3. (see Appendix)
I. Prior authorization will be required for predictive genetic testing in asymptomatic individuals
with a symptomatic first-degree or second-degree relative or relative with a known deleterious mutation, where early diagnosis is important and therapeutic measure, instituted as a result of knowledge of a particular defect, can prevent or mitigate future morbidity, for the following indications:
1. Family history of breast cancer
2. Family history of ovarian cancer
3. Familial adenomatous polyposis
4. Hereditary nonpolyposis colorectal cancer
J. For the conditions listed in I., HMSA will use its genetic testing policies to screen for
appropriate candidates. For these individuals, HMSA requires a pre-test genetic risk assessment (one visit with pre-certification) as a condition for approval of genetic testing.
K. Genetic risk assessments are covered only for the conditions listed in I. and must also meet the
following criteria:
1. Services must be conducted by a properly certified/licensed and credentialed genetic specialist (i.e., board-certified medical geneticist (MD), board-certified clinical geneticist (PhD), board-certified genetic counselor (MS and/or CGC), or licensed advanced practice registered nurse in genetics (APRN)).
2. Services must be conducted in a face-to-face consultation and/or telemedicine consult
visit (in accordance with HMSA’s current telemedicine payment policy) and a subsequent consultation letter or report must be submitted to the treating physician.

QUEST Provider Handbook Benefit Policies Rev. 05/08
L. One post-test genetic risk assessment visit will be covered for predictive genetic testing in asymptomatic individuals (section II.I.) under the following conditions:
1. Pre-test genetic risk assessment was conducted and covered as part of pre-certification
for selected genetic tests as stated above.
2. The patient qualified and received the ordered genetic test according to the pre-test assessment.
3. A CLIA-certified laboratory submits a viable claim for the completed genetic test.
III. Limitations/Exclusions
A. Benefits are provided only for HMSA members; benefits are not provided for family members without current HMSA coverage.
B. Except as referenced in Criteria/Guidelines, genetic screening of individuals is not covered in
the absence of associated signs, symptoms or complaints. General population screening for genetic disorders is not covered except where mandated by State and Federal law.
C. Laboratories that conduct genetic testing must be CLIA certified.
D. Genetic counseling is not a separately covered benefit. However, genetic risk assessment may
be required for selected genetic tests for specific conditions and procedures and pre-certification is required. See Criteria/Guidelines for coverage.
E. Genetic tests for a specific inherited disease will be covered once per lifetime.
F. Home genetic testing is not a covered benefit.
G. For a known deleterious mutation, HMSA will only cover a targeting single site analysis
genetic test not a full analysis (i.e., testing for the mutation that has been identified in the family).
IV. Administrative Guidelines
A. Pre-certification is required for the following:
1. Genetic risk assessments and predictive genetic testing in asymptomatic individuals for the following clinical conditions (Subject to II.I.):
a. Family history of breast cancer
b. Family history of ovarian cancer
c. Familial adenomatous polyposis
d. Hereditary nonpolyposis colorectal cancer
2. Cystic fibrosis carrier testing (Subject to II.G.)

G Genetic Testing (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
3. Long QT syndrome (Subject to II.H.1 and H.2)
4. Genetic tests for diagnoses or procedures not on the approved list below requires pre-certification.
B. To pre-certify please complete HMSA’s Pre-certification Request and fax or mail the form as
indicated. The information received should include the member’s family history and a brief summary as to why the genetic test is needed.
C. If pre-certification is not sought, the member will not be held responsible for payment of
denied services unless an Agreement of Financial Responsibility is completed and signed.
D. Procedure codes should be reported as precisely as possible. ICD-9 codes should reflect the patient’s condition or symptoms. Do not code “rule out” diagnoses.
* Indicates codes are also included in the Amniocentesis and Chorionic Villus Sampling Policy.
ICD-9-CM Description 094.0 Neurosyphilis tabes dorsalis (includes locomotor ataxia, progressive) 153.0 – 153.9 Malignant neoplasm colon 154.0 rectosigmoid junction 170.9 bone and articular cartilage, site unspecified 171.9 connective and other soft tissue, site unspecified 182.0 endometrium 189.1 renal pelvis 189.2 ureter 190.5* retina 193 thyroid gland 194.0 – 194.9 other endocrine glands and related structures 197.4 Secondary malignant neoplasm of small intestine, including duodenum 197.5 Secondary malignant neoplasm of the large intestine and rectum 204.00 – 204.91 Lymphoid leukemia 205.00 – 205.91 Myeloid leukemia 206.00 – 206.91 Monocytic leukemia 207.00 – 207.81 Other specified leukemia 208.00 – 208.91 Leukemia of unspecified cell type 211.3 Benign neoplasm, colon 211.4 rectum and anal canal 227.0 adrenal gland 230.3 Carcinoma in situ, colon 230.4 rectum (rectosigmoid junction) 235.2 Neoplasm of uncertain behavior stomach, intestines and rectum 237.70 – 237.72* Neurofibromatosis 238.71 – 238.79 Neoplasm of uncertain behavior, other lymphatic and hematopoietic tissues
(includes myelodysplastic syndrome) 239.0 Neoplasms of digestive system

QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Description 252.00 Hyperparathyroidism, unspecified 252.01 Primary hyperparathyroidism 252.02 Secondary hyperparathyroidism, non-renal 252.08 Other hyperparathyroidism 255.8 Other specified disorders of adrenal glands 257.2 Other testicular hypofunction (includes defective biosynthesis of testicular
androgen) 259.0 Delay in sexual development and puberty, not elsewhere classified 270.1* Phenylketonuria (PKU) 270.2 Other disturbances of aromatic amino-acid metabolism (includes albinism) 270.3 Disturbances of branched-chain amino-acid metabolism (includes maple
syrup urine disease) 270.4* Disturbances of sulphur-bearing amino-acid metabolism (includes
homocystinuria) 270.6 Disorders of urea cycle metabolism 271.1 Galactosemia 272.0 Pure hypercholesterolemia 272.4 Other and unspecified hyperlipidemia 272.5 Lipoprotein deficiencies 272.7* Lipodoses (includes Niemann-Pick and Gaucher's disease) 272.8 Other disorders of lipoid metabolism 275.0* Disorders of iron metabolism (includes hemochromatosis) 275.1* Disorders of copper metabolism 277.00 – 277.01* Cystic fibrosis (requires pre-certification) 277.2 Other disorders of purine and pyrimidine metabolism (includes Lesch-
Nyhan syndrome) 277.30 – 277.39 Amyloidosis 277.5 Mucopolysaccharidosis (includes Hunter’s syndrome, Hurler’s syndrome) 277.6 Other deficiencies of circulating enzymes (including hereditary
angioedema) 277.81 – 277.89 Other specified disorders of metabolism 277.9 Unspecified disorders of metabolism 279.11* DiGeorge’s syndrome 282.0 Hereditary spherocytosis 282.1 Hereditary elliptocytosis 282.2 Anemias due to disorders of glutathione metabolism (includes G6PD
deficiency) 282.41* Sickle-cell, thalassemia, without crisis 282.42* Sickle-cell, thalassemia, with crisis 282.49* Other thalassemia 282.5 Sickle-cell trait 282.61* Hb-SS disease without crisis 282.62* Hb-SS disease with crisis 282.63* Sickle-cell/Hb-C disease without crisis 282.7 Other hemoglobinopathies 284.0 Constitutional aplastic anemia (including Fanconi’s anemia)

G Genetic Testing (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Description 286.0* Congenital factor VIII disorder 286.1* Congenital factor IX disorder 286.3 Congenital deficiency of other clotting factors 286.4 Von Willebrand disease 286.9 Other and unspecified coagulation defects 287.5 Thrombocytopenia, unspecified 288.00 – 288.09 Agranulocytosis 288.1 Functional disorders of polymorphonuclear neutrophils 299.00 Autistic disorder, current or active state 317 Mild mental retardation 318.0 Moderate mental retardation 318.1 Severe mental retardation 318.2 Profound mental retardation 319 Unspecified mental retardation 330.0* Cerebral degenerations usually manifest in childhood; leukodystrophy 330.1* Cerebral degenerations usually manifest in childhood; cerebral lipodoses
(Tay-Sachs disease) 330.8 Other specified cerebral degenerations in childhood (includes Leigh’s
disease) 333.4* Huntington’s chorea 334.0 – 334.9* Spinocerebellar disease 335.0 Werdnig-Hoffmann disease 335.10 – 335.19* Spinal muscular atrophy* 335.20 Amyotrophic lateral sclerosis 335.22 Progressive bulbar palsy 345.10 Generalized convulsive epilepsy; without mention of intractable epilepsy,
(includes myoclonic epilepsy) 345.11 Generalized convulsive epilepsy; with intractable epilepsy 356.0 – 356.4* Hereditary and idiopathic peripheral neuropathy 359.1* Hereditary progressive muscular dystrophy (includes limb-girdle and
Duchenne muscular dystrophy) 359.21* Myotonic muscular dystrophy 359.22* Myotonia congenital 359.23* Myotonic chondrodystrophy 359.81 Critical illness myopathy 359.89 Other myopathies 426.82 Long QT syndrome (requires pre-certification) 434.00 Cerebral thrombosis; without mention of cerebral infarction 434.01 Cerebral thrombosis; with cerebral infarction 451.0 – 451.9 Phlebitis and thrombophlebitis 453.0 – 453.9 Other venous embolism and thrombosis 527.7 Disturbance of salivary secretion (includes Xerostomia) 626.0 Absence of menstruation (includes amenorrhea) 632 Missed abortion 646.30* Habitual aborter; unspecified as to episode of care or not applicable

QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Description 646.31* Habitual aborter; delivered, with or without mention of antepartum
condition 646.33* Habitual aborter; antepartum condition or complication 655.13 Chromosomal abnormality in fetus, antepartum condition or complication 655.20 – 655.23* Hereditary disease in family, possibly affecting fetus 656.13* Rhesus isoimmunization – antepartum condition or complication 659.50 – 659.53* Elderly primigravida 659.60 – 659.63* Elderly multigravida 671 Venous complications in pregnancy and the puerperium 695.4 Lupus erythematosus 710.0 Systemic lupus erythematosus 710.1 Systemic sclerosis 710.2 Sicca syndrome (including Sjögren’s disease) 710.3 Dermatomyositis 710.4 Polymyositis 710.5 Eosinophilia myalgia syndrome 710.9 Unspecified, diffuse connective tissue disorder 742.1 Microcephalus 742.2 Reduction deformities of brain 742.4 Other specified anomalies of brain (includes macroencephaly) 752.81* Scrotal transposition 752.89* Other specified anomaly of genital organs 753.10 – 753.19* Cystic kidney disease (including polycystic kidney, autosomal dominant) 755.13 Syndactyly of toes without fusion of bones 756.0 Anomalies of skull and face bones (includes craniosynostosis) 756.4 Chondrodystrophy 756.51 Osteogenesis imperfecta 756.56 Multiple epiphyseal dysplasia 756.59 Osteodystrophies, other (includes Albright (-McCune)-Sternberg
syndrome) 756.83 Ehlers-Danlos syndrome 757.33* Congenital pigmentary anomalies of the skin (includes Xeroderma
pigmentosum) 758.0* Down’s syndrome 758.1* Patau’s syndrome 758.2* Edward’s syndrome 758.31* Autosomal deletion syndromes; cri-du-chat syndrome 758.32 velo-cardio-facial syndrome 758.33 other microdeletions 758.39 other autosomal deletions 758.4* Balance autosomal translocation in normal individual 758.5* Other conditions due to autosomal anomalies (accessory autosomes, NEC) 758.6* Gonadal dysgenesis (ovarian dysgenesis, Turner’s syndrome, XO
syndrome) 758.7* Klinefelter’s syndrome

G Genetic Testing (continued)
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Description 758.81 Other conditions due to sex chromosome anomalies 759.5 Tuberous sclerosis 759.6* Other hamartoses, not elsewhere classified (including von Hippel-Lindau
syndrome) 759.7 Multiple congenital anomalies, so described 759.81* Prader-Willi syndrome 759.82* Marfan syndrome 759.83* Fragile X syndrome 759.89* Other specified anomalies (includes congenital malformation syndromes
affecting multiple systems, not elsewhere classified and Laurence-Moon-Biedl syndrome)
760.2 Maternal infections (includes fetus or newborn affected by maternal infectious disease classifiable to 001-136 and 487, but fetus or newborn not manifesting that disease)
760.8 Other specified maternal conditions affecting fetus or newborn 774.0 – 774.7 Other perinatal jaundice 775.7 Late metabolic acidosis of newborn 776.0 – 776.9* Hematological disorders of fetus and newborn 790.8* Viremia, unspecified 796.5* Abnormal finding on antenatal screening V10.05 Personal history of malignant neoplasm; large intestine V10.06 Personal history of malignant neoplasm; rectum, rectosigmoid junction,
and anus V12.51 Personal history of certain other diseases, venous thrombosis and embolism V16.0 Family history of malignant neoplasm; gastrointestinal tract V17.2 Family history of other neurological diseases
V76.41 Special screening for malignant neoplasm; rectum V78.3 Special screening for other hemoglobinopathies
The following CPT codes and HCPCS codes represent appropriate procedures for genetic testing if the previously listed criteria are met.
CPT Codes Description 83080* b-Hexosaminidase, each assay 83890* Molecular diagnostics; molecular isolation or extraction 83891* isolation or extraction of highly purified nucleic acid 83892* enzymatic digestion 83893* dot/slot blot production 83894* separation by gel electrophoresis (e.g., agarose, polyacrylamide) 83896* nucleic acid probe, each 83897* nucleic acid transfer (e.g. Southern, Northern) 83898* amplification of patient nucleic acid (e.g., PCR, LCR), single primer pair,
each primer pair

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies Rev. 05/08
CPT Codes Description 83901* amplification of patient nucleic acid, multiplex, each multiplex reaction 83902* reverse transcription 83903* mutation scanning, by physical properties (e.g., single strand
conformational polymorphisms (SSCP), heteroduplex, denaturing gradient gel electrophoresis (DGGE), RNA’ase A, single segment, each
83904* mutation identification by sequencing, single segment, each segment 83905* mutation identification by allele specific transcription, single segment,
each segment 83906* mutation identification by allele specific translation, single segment, each
segment 83912* interpretation and report 88230* Tissue culture for non-neoplastic disorders; lymphocyte 88233 skin or other solid tissue biopsy 88237* Tissue culture for neoplastic disorders; bone marrow, blood cells 88239 solid tumor (approved for breast only) 88240* Cryopreservation, freezing and storage of cells, each cell line 88241* Thawing and expansion of frozen cells, each aliquot 88245* Chromosome analysis for breakage syndromes; baseline Sister Chromatid
Exchange (SCE), 20-25 cells 88248* baseline breakage, score 50-100 cells, count 20 cells, 2 karyotypes (e.g.,
for ataxia telangiectasia, Fanconi anemia, fragile X) 88249* score 100 cells, clastogen stress (e.g., diepoxybutane, mitomycin C,
ionizing radiation, UV radiation) 88261* Chromosome analysis; count 5 cells, 1 karyotype, with banding 88262* count 15-20 cells, 2 karyotypes, with banding 88263* count 45 cells for mosaicism, 2 karyotypes, with banding 88264* analyze 20-25 cells 88271* Molecular cytogenetics, DNA probe, each (e.g., FISH) 88272* chromosomal in situ hybridization, analyze 3-5 cells (e.g., for derivatives
and markers) 88273* chromosomal in situ hybridization, analyze 10-30 cells (e.g., for
microdeletions) 88274* interphase in situ hybridization, analyze 25-99 cells 88275* interphase in situ hybridization, analyze 100-300 cells 88280* Chromosome analysis; additional karyotypes, each study 88283* additional specialized banding technique (e.g., NOR, C-banding) 88285* additional cells counted, each study 88289* additional high resolution study 88291* Cytogenetics and molecular cytogenetics, interpretation and report
HCPCS Codes Description S3828 Complete gene sequence analysis; MLH1 gene S3829 MSH2 gene S3830 Complete MLH1 and MLH2 gene sequence analysis for hereditary
nonpolyposis colorectal cancer (HNPCC) genetic testing

G Genetic Testing (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
HCPCS Codes Description S3831 Single mutation analysis (in individuals with a known MLH1 and MLH2
mutation in the family) for hereditary nonpolyposis colorectal (HNPCC) genetic testing
S3833 Complete APC gene sequence analysis for susceptibility to familial adenomatous polyposis (FAP) and attenuated (FAP)
S3834 Single mutation analysis (in individual with a known APC mutation in the family) for susceptibility to familial adenomatous polyposis (FAP) and attenuated FAP
S3835 Complete gene sequence analysis for cystic fibrosis genetic testing (PRECERT REQUIRED)
S3837 Complete gene sequence analysis for hemochromatosis genetic testing. S3840 DNA analysis for germline mutations of the RET proto-oncogene for
susceptibility to multiple endocrine neoplasia type 2 S3841 Genetic testing for retinoblastoma S3842 Genetic testing for Von Hippel-Lindau disease S3843 DNA analysis of the F5 gene for susceptibility to Factor V Leiden
thrombophilia S3844 DNA analysis of the connexin 26 gene (GJB2) for susceptibility to
congenital, profound deafness S3845 Genetic testing for alpha-thalassemia S3846 hemoglobin E beta-thalassemia S3847 Tay-Sachs disease S3848 Gaucher disease S3849 Niemann-Pick disease S3850 sickle cell anemia S3851 Canavan disease S3852 DNA analysis for APOE epsilon 4 allele for susceptibility to Alzheimer’s
disease S3853 Genetic testing for myotronic dystrophy
V. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients' Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice, and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.

QUEST Provider Handbook Benefit Policies 05/08
VI. References 1. American College of Medical Genetics Foundation. Genetic susceptibility to breast and
ovarian cancer: Assessment, counseling and testing guidelines. 1999.
2. American College of Obstetricians and Gynecologists. Committee Opinion: Update on Carrier Screening for Cystic Fibrosis, Number 325, December 2005.
3. American Gastroenterological Association. American Gastroenterological Association medical
position statement: Hereditary colorectal cancer and genetic testing. Gastroenterology 2001; 121:195-197.
4. BCBS Association Medical Policy Reference Manual. Genetic Testing for Inherited BRCA1 or
BRCA2 Mutations. Policy #2.04.02. Reviewed September 2005.
5. BCBS Association Draft Medical Policy Reference manual. Genetic Testing for Congenital Long QT Syndrome. Policy 2.04.43 Reviewed December 13, 2007.
6. BCBS Association. Medical Policy Reference Manual. Genetic Testing for Inherited
Susceptibility to Colon Cancer Including Microsatellite Instability. Policy # 2.04.08 Reviewed May 2005.
7. ECRI. Genetic Testing for BRCA1 and BRCA2 Mutations for Assessing Breast Cancer Risk.
Published 02/2006.
8. ECRI. Microsatellite instability testing for hereditary nonpolyposis colorectal cancer. Windows on Medical Technology. Jan. 2002.
9. Excellus. Medical Policy Manual. Genetic testing for inherited susceptibility to colorectal
cancer: familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer. Policy # 2.02.11. June 2007.
10. FitzGerald, MG, et al. Germ-line BRCA1 mutations in Jewish and non-Jewish women with
early-onset breast cancer. NEJM. 1996; 334(3):143-149.
11. Giardiello FM, Brensinger JD, Petersen GM. American Gastroenterological Association technical review on hereditary colorectal cancer and genetic testing. April 2001.
12. Hayes, Winifred S, Hayes Directory. Genetic testing for susceptibility to hereditary
nonpolyposis colorectal cancer. March 5, 1998; GENE0103.05:1-25.
13. Ikenaga M, et al. Use of microsatellite analysis in young patients with colorectal cancer to identify those with hereditary nonpolyposis colorectal cancer. J Surg Oncol. 2002 Mar; 79(3):157-165.
14. International Society for Gastrointestinal Hereditary Tumours (InSIGHT). Guidelines for
Management of HNPCC families, Amsterdam and Amsterdam II diagnostic criteria. http://www.insight-group.org/ accessed on 04/26/06.
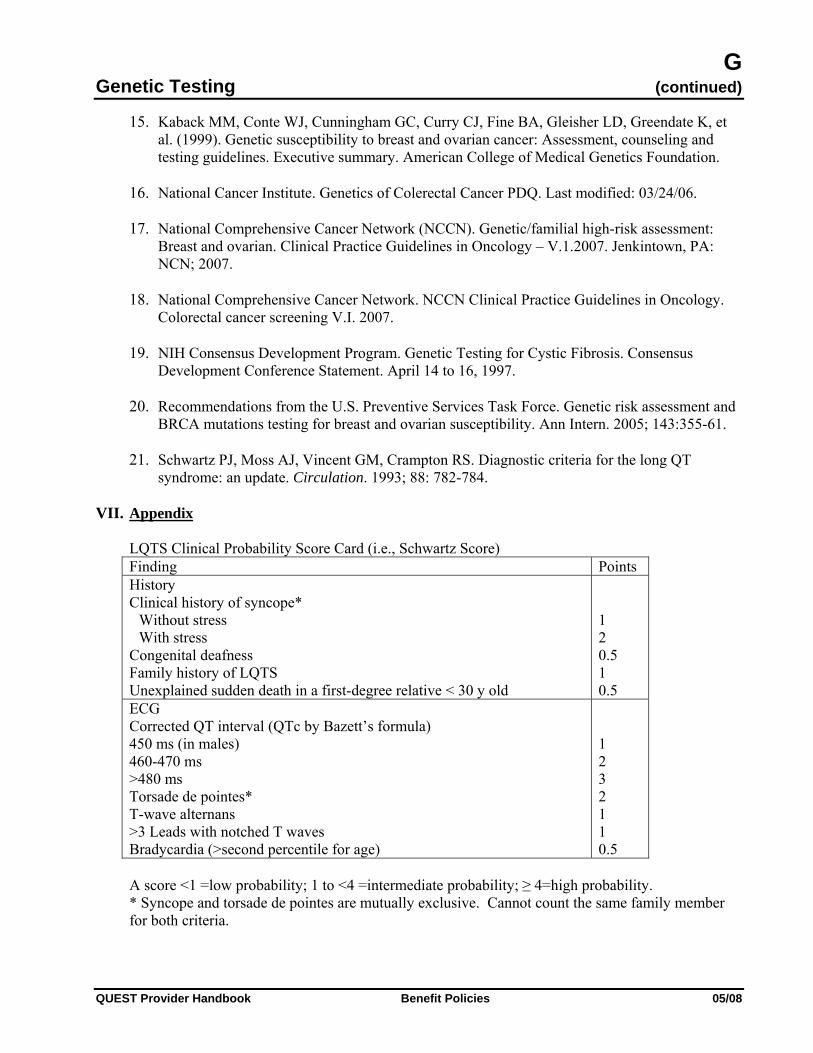
G Genetic Testing (continued)
QUEST Provider Handbook Benefit Policies 05/08
15. Kaback MM, Conte WJ, Cunningham GC, Curry CJ, Fine BA, Gleisher LD, Greendate K, et al. (1999). Genetic susceptibility to breast and ovarian cancer: Assessment, counseling and testing guidelines. Executive summary. American College of Medical Genetics Foundation.
16. National Cancer Institute. Genetics of Colerectal Cancer PDQ. Last modified: 03/24/06.
17. National Comprehensive Cancer Network (NCCN). Genetic/familial high-risk assessment:
Breast and ovarian. Clinical Practice Guidelines in Oncology – V.1.2007. Jenkintown, PA: NCN; 2007.
18. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology.
Colorectal cancer screening V.I. 2007.
19. NIH Consensus Development Program. Genetic Testing for Cystic Fibrosis. Consensus Development Conference Statement. April 14 to 16, 1997.
20. Recommendations from the U.S. Preventive Services Task Force. Genetic risk assessment and
BRCA mutations testing for breast and ovarian susceptibility. Ann Intern. 2005; 143:355-61.
21. Schwartz PJ, Moss AJ, Vincent GM, Crampton RS. Diagnostic criteria for the long QT syndrome: an update. Circulation. 1993; 88: 782-784.
VII. Appendix
LQTS Clinical Probability Score Card (i.e., Schwartz Score) Finding Points History Clinical history of syncope*
Without stress With stress
Congenital deafness Family history of LQTS Unexplained sudden death in a first-degree relative < 30 y old
1 2 0.5 1 0.5
ECG Corrected QT interval (QTc by Bazett’s formula) 450 ms (in males) 460-470 ms >480 ms Torsade de pointes* T-wave alternans >3 Leads with notched T waves Bradycardia (>second percentile for age)
1 2 3 2 1 1 0.5
A score <1 =low probability; 1 to <4 =intermediate probability; ≥ 4=high probability. * Syncope and torsade de pointes are mutually exclusive. Cannot count the same family member for both criteria.


G Genetic Testing for Inherited BRCA1 or BRCA2 Mutations
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
This policy is effective July 1, 2008 I. Description
Families suspected of having hereditary breast and/or ovarian cancer are characterized by cancer occurring at an early age, in multiple generations, and often bilaterally and in a pattern suggesting an autosomal dominant pattern of inheritance. The susceptibility may be transmitted through the maternal or paternal side of the family. Germline alterations in two genes, BRCA1 and BRCA2, are associated with an increased risk of breast and ovarian cancer. Alterations in BRCA1 and BRCA2 explain much but not all inherited forms of breast and ovarian cancer. With the identification of BRCA1 and BRCA2, it is now possible to test for abnormalities in these genes to provide information on future risk of cancer.
In the majority of cases, testing is more informative when first carried out in an affected family member and a known deleterious BRCA1 or BRCA2 mutation is found.
II. Criteria/Guidelines
A. Genetic testing for BRCA1 and/or BRCA2 genes will be covered (subject to Limitations/ Exclusions and Administrative Guidelines) according to the American College of Medical Genetics (ACMG) guidelines for Genetic Susceptibility to Breast and Ovarian Cancer. The patient must be 18 years of age or older and the results of the testing will result in a treatment decision for the patient tested. In addition, the affected or unaffected patient must meet one of following:
1. There are three or more first and/or second degree relatives* with breast cancer on the
same side of the family, regardless of age at diagnosis, OR
2. There are fewer than three affected relatives, but
a. The patient was diagnosed with breast cancer at 45 years of age or less (or is premenopausal), or
b. The patient was diagnosed at any age and a first- or second-degree relative* was
diagnosed with breast cancer at 45 years of age or less, or
c. A first-, second-degree or third-degree relative* has been identified with a known BRCA1 or BRCA2 deleterious mutation, or
d. There are one or more cases (including the patient) of ovarian cancer diagnosed at
any age , and at least one first or second degree relative* on the same side of the family with breast cancer at any age, or
e. There are multiple primary or bilateral breast cancers in the patient, or first and/or
second degree relative*, or
f. There is breast cancer in a male patient or in a first or second degree male relative*, or
QUEST Provider Handbook Benefit Policies 05/08
g. The patient is at increased risk for specific mutation(s) due to ethnic background (for instance: Ashkenazi Jewish descent) and has one or more first or second degree relatives* with breast or ovarian cancer diagnosed at any age (including the patient).
*First degree relatives=parents, full siblings, offspring. Second degree relatives=grandparents, grandchildren, aunts, uncles, nephews, nieces, half-siblings. Third degree relatives= great-grandparents, great-aunts, great-uncles, first cousins.
B. Pre-certification will be required for genetic risk assessment in asymptomatic individuals with
a symptomatic first-degree or second-degree relative or relative with a known deleterious mutation, where early diagnosis is important and therapeutic measures, instituted as a result of knowledge of a particular defect, can prevent or mitigate future morbidity, or for the following indications:
1. History of breast cancer in a first- or second-degree relative
2. History of ovarian cancer in a first- or second-degree relative
C. For asymptomatic individuals, HMSA requires a pre-test genetic risk assessment (one visit
with pre-certification) as a condition for approval of genetic testing.
D. Genetic risk assessments are covered only for the criteria listed in B. and must also meet the following:
1. Services must be conducted by a properly certified/licensed and credentialed genetic
specialist (i.e., board-certified medical geneticist (MD), board-certified clinical geneticist (PhD), board-certified genetic counselor (MS and/or CGC), or licensed advanced practice registered nurse in genetics (APRN)).
2. Services must be conducted in a face-to-face consultation and/or telemedicine consult
visit (in accordance with HMSA's current telemedicine payment policy) and a subsequent consultation letter or report must be submitted to the treating physician.
E. One risk assessment visit after genetic testing will be covered for patients who qualified for
predictive genetic testing in asymptomatic individuals (section B.) under the following conditions:
1. Pre-test genetic risk assessment was conducted and covered as part of pre-certification
for selected genetic tests as stated above.
2. The patient qualified and received the ordered genetic test according to the pre-test assessment.
3. A CLIA-certified laboratory submits a viable claim for the completed genetic test.

G Genetic Testing for Inherited BRCA1 or BRCA2 Mutations (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
III. Limitations/Exclusions A. An affected family member should be tested first whenever possible. Should a BRCA
mutation be found in an affected family member(s), the DNA from the unaffected family member can be tested specifically using a tailored study for the same mutation of the affected family member without having to sequence the entire gene.
B. Genetic testing for unaffected individuals (of both the general population and of potentially
high-risk ethnic populations) without a family history suggesting increased risk of BRCA mutation is not covered.
C. Genetic testing in minors for BRCA1 and BRCA2 mutations is not covered.
D. Genetic testing for BRCA1 and BRCA2 mutations is not covered for assessment of risk of
other cancers including but not limited to pancreatic, prostate and colon cancer.
E. Testing in eligible individuals who belong to ethnic populations in which there are well-characterized founder mutation should begin with tests specifically for these mutations. For example, founder mutations account for approximately three quarters of the BRCA mutations found in Ashkenazi Jewish populations. When the testing for founder mutations is negative, full gene sequencing should then be performed.
F. Separate BRCA Analysis Rearrangement Test (or BART testing) for individuals who have
previously tested negative for the BRCA1 or BRCA2 mutation is not covered as there is insufficient evidence at this time that this study alone improves health outcomes.
G. Benefits are provided only for HMSA members; benefits are not provided for family members
without current HMSA coverage.
H. Laboratories that conduct genetic testing must be CLIA certified.
I. Genetic counseling is not a separately covered benefit. See Criteria/Guidelines for coverage of genetic risk assessment.
J. Genetic risk assessment is not a benefit of the FED87 plan.
K. Repeat BRCA1 or BRCA2 mutation testing is not covered.
IV. Administrative Guidelines
A. Pre-certification is required for the following:
1. Genetic testing for inherited BRCA1 or BRCA2 mutations.
2. Genetic risk assessment is required in asymptomatic individuals for the following clinical conditions (Subject to II.A.):
a. History of breast cancer in a first or second degree relative.
b. History of ovarian cancer in a first or second degree relative.

QUEST Provider Handbook Benefit Policies 05/08
B. To pre-certify please complete HMSA’s Pre-certification Request and fax or mail the form as indicated. The information received should include the member's family history and a brief summary as to why the genetic test is needed.
C. If pre-certification is not sought, the member will not be held responsible for payment of
denied services unless an Agreement of Financial Responsibility is completed and signed.
HCPCS Codes Description S3818 Complete gene sequence analysis; BRCA 1 gene S3819 Complete gene sequence analysis; BRCA 2 gene S3820 Complete BRCA 1 and BRCA 2 gene sequence analysis for susceptibility
to breast and ovarian cancer S3822 Single mutation analysis (in individual with a known BRCA1 or BRCA 2
mutation in family) for susceptibility to breast and ovarian cancer S3823 Three-mutation BRCA 1 and BRCA 2 analysis for susceptibility to breast
and ovarian cancer in Ashkenazi individuals V. Scientific Background
2005 Update Articles published since the 2004 update were reviewed for information that might affect the policy statements or relevant background information in this document. However, nothing was found that would prompt reconsideration of the policy statements. Nor did any new publications contradict or substantially add to the background information. Guidelines published by the American Society of Clinical Oncology and the American College of Medical Genetics have not been updated since 2004.
2004 Update Articles published since the BCBSA TEC Assessment (1) and last policy update were reviewed for information regarding professional guidelines for BRCA testing, testing of unaffected family members, and testing of high-risk ethnic populations. In addition, Web sites for relevant professional organizations were consulted for posted guidelines.
The American Society of Clinical Oncology (ASCO) (2) recommends that cancer predisposition testing be offered when 1) the person has a strong family history of cancer or very early age of onset of disease, 2) the test can be adequately interpreted, and 3) the results will influence the medical management of the patient or family member.
In 1999, the American College of Medical Genetics (ACMG) (3) published guidelines for BRCA testing under the auspices of a grant from the New York State Department of Health to the ACMG Foundation. The guidelines suggest that increased risk for a mutation in a known cancer susceptibility gene is evident if:
• “There are three or more affected first or second degree relatives on the same side of the
family, regardless of age at diagnosis, or
• There are fewer than three affected relatives, but
• the patient was diagnosed at 45 years of age or less, or

G Genetic Testing for Inherited BRCA1 or BRCA2 Mutations (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
• a family member has been identified with a detectable mutation, or
• there are one or more cases of ovarian cancer at any age, and one or more members on the same side of the family with breast cancer at any age, or
• there are multiple primary or bilateral breast cancers in the patient or one family
member, or
• there is breast cancer in a male patient, or in a male relative, or
• the patient is at increased risk for specific mutation(s) due to ethnic background (for instance: Ashkenazi Jewish descent) and has one or more relatives with breast cancer or ovarian cancer at any age.”
“At present, it is not recommended that the health care provider initiate discussion of the testing option with unaffected Ashkenazi Jewish individuals unless additional factors are uncovered in the family or personal history (i.e., one or more relatives with breast and/or ovarian cancer). For that matter, it is not currently recommended that widespread screening of any subpopulation be initiated.”
Early estimates of lifetime risk of cancer for BRCA mutation carriers (penetrance), based on studies of families with extensive history of disease, have been as high as 85 percent. Because other factors that influence risk may be present in families with extensive breast and ovarian cancer histories, early penetrance estimates may have been biased upward. (4) Studies of founder mutations in ethnic populations (e.g., Ashkenazi Jewish, Polish, and Icelandic populations) unselected for family history indicated lower penetrance estimates, in the range of 40%–60% for BRCA1 and 25 percent to 40 percent for BRCA2. (5-8) However, a recent genotyping study of Ashkenazi Jewish women with incident, invasive breast cancer, selected regardless of family history of cancer, and their family members resulted in an 82 percent lifetime risk of breast cancer for carriers of any of three BRCA founder mutations. (9) Importantly, the risk of cancer in mutation carriers from families with little history of cancer (~50 percent of all carriers) was not significantly different. Lifetime risks of ovarian cancer were 54 percent for BRCA1 and 23 percent for BRCA2 mutation carriers. Women with a history of breast cancer and a BRCA mutation have a significant risk of contralateral breast cancer; in one study the risk was 29.5 percent at 10 years for women with initially stage I or II disease. (10)
Thus, the risk of cancer in a BRCA mutation carrier is significant, and knowledge of mutation status in individuals at potentially increased risk of a BRCA mutation may impact healthcare decisions to reduce risk. (11-19) Risk-reducing options include intensive surveillance, prophylactic mastectomy, or prophylactic oophorectomy. Prophylactic mastectomy reduces the risk of breast cancer in high-risk women (based on family history) by 90% or more but is invasive and disfiguring. (11) Prophylactic oophorectomy significantly reduces the risk of ovarian cancer to less than 10 percent (13, 15) and reduces the risk of breast cancer by approximately 50 percent. (13) In women who have already had breast cancer, prophylactic oophorectomy reduces the risk of cancer relapse. (16) Studies indicate that genotyping results significantly influence treatment choices. (17-19)

QUEST Provider Handbook Benefit Policies 05/08
BRCA mutation-associated cancers may have biologically different properties. In 1 study, 5-year survival was reported as poorer in women with BRCA1-associated breast cancer compared to noncarriers (63 percent vs. 91 percent). (16) Conversely, in another study BRCA mutation carrier vs. noncarrier median survival of ovarian cancer was 53.4 vs. 37.8 months. (20) However, there is no clear indication that cancer treatment should be modified based on BRCA status.
The prevalence of BRCA mutations is approximately 0.1 percent to 0.2 percent in the general population. Prevalence may be much higher for particular ethnic groups with characterized founder mutations (e.g., 2 percent to 3 percent in the Ashkenazi Jewish population). Family history of breast and ovarian cancer is an important risk factor for BRCA mutation. Age and, in some cases, ethnic background can also be independent risk factors.
Young age of onset of breast cancer, even in the absence of family history, has been demonstrated to be a risk factor for BRCA1 mutations. Winchester (21) estimated that hereditary breast cancer accounts for 36 percent to 85 percent of patients diagnosed under age 30. In several studies, BRCA mutations are independently predicted by early age at onset, being present in 6 percent to 10 percent of breast cancer cases diagnosed at ages younger than various premenopausal age cutoffs (ages 35–50 years). (21-24) In cancer-prone families, the mean age of breast cancer diagnosis among women carrying BRCA1 or BRCA2 mutations is in the 40s. (25) In the Ashkenazi Jewish population, Frank et al. (24) Reported that 13 percent of 248 cases with no known family history and diagnosed before 50 years of age had BRCA mutations. In a similar study, 31percent of Ashkenazi Jewish women, unselected for family history, diagnosed with breast cancer at younger than 42 years of age had BRCA mutations. (26) Additional studies indicate that early age of breast cancer diagnosis is a significant predictor of BRCA mutations in the absence of family history in this population. (7, 27, 28)
As in the general population, family history of breast or ovarian cancer, particularly of early age onset, is a significant risk factor for a BRCA mutation in ethnic populations characterized by founder mutations. For example, in unaffected individuals of Ashkenazi Jewish descent, 12 percent to 31 percent will have a BRCA mutation depending on the extent and nature of the family history. (24) Several other studies document the significant influence of family history. (6, 7, 26-28)
Unaffected individuals with a known family history but unknown family mutation may obtain interpretable results in most cases of a positive test. Most BRCA1 and BRCA2 mutations reported to date consist of frameshift deletions, insertions, or nonsense mutations leading to premature truncation of protein transcription. These are invariably deleterious and thus are informative in the absence of an established family genotype. (24, 29) In addition, specific missense mutations and noncoding intervening sequence mutations may be interpreted as deleterious on the basis of accumulated data or from specific functional or biochemical studies. However, some mutations may have uncertain significance in the absence of a family study, and negative results offer no useful information, i.e., the patient may still be at increased risk of a mutation.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.

G Genetic Testing for Inherited BRCA1 or BRCA2 Mutations (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VII. References
1. BCBSA TEC Assessments 1997; Tab 4.
2. American Society of Clinical Oncology. Policy Statement Update: Genetic Testing for Cancer Susceptibility (posted online April 11, 2003). J Clin Oncol 2003; 21(12):1-10.
3. The American College of Medical Genetics, Policy Statement: Genetic Susceptibility to Breast
and Ovarian Cancer: Assessment, Counseling and Testing Guidelines, 1999, available at http://www.acmg.net.
4. Begg CB. On the use of familial aggregation in population-based case probands for calculating
penetrance. J Natl Cancer Inst 2002; 94(16):1221-6.
5. Satagopan JM, Offit K, Foulkes W, et al. The lifetime risks of breast cancer in Ashkenazi Jewish carriers of BRCA1 and BRCA2 mutations. Cancer Epidemiol Biomarkers Prev 2001; 10(5):467-73.
6. Moslehi R, Chu W, Karlan B, et al. BRCA1 and BRCA2 mutation analysis of 208 Ashkenazi
Jewish women with ovarian cancer. Am J Hum Genet 2000; 66(4):1259-72.
7. Warner E, Foulkes W, Goodwin P, et al. Prevalence and penetrance of BRCA1 and BRCA2 gene mutations in unselected Ashkenazi Jewish women with breast cancer. J Natl Cancer Inst 1999; 91(14):1241-7.
8. Thorlacius S, Struewing JP, Hartge P, et al. Population-based study of risk of breast cancer in
carriers of BRCA2 mutation. Lancet 1998; 352(9137):1337-9.
9. King MC, Marks JH, Mandell JB. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 2003; 302(5645):643-6.
10. Metcalfe K, Lynch HT, Ghadirian P, et al. Contralateral breast cancer in BRCA1 and BRCA2
mutation carriers. J Clin Oncol 2004; 22(12):2328-35.
11. Hartmann LC, Schaid DJ, Woods JE, et al. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med 1999; 340(2):77-84.

QUEST Provider Handbook Benefit Policies 05/08
12. Grann VR, Whang W, Jacobson JS, et al. Benefits and costs of screening Ashkenazi Jewish women for BRCA1 and BRCA2. J Clin Oncol 1999; 17(2):494-500.
13. Rebbeck TR, Lynch HT, Neuhausen SL, et al. Prophylactic oophorectomy in carriers of
BRCA1 or BRCA2 mutations. N Engl J Med 2002; 346(21):1616-22.
14. Scheuer L, Kauff N, Robson M, et al. Outcome of preventive surgery and screening for breast and ovarian cancer in BRCA mutation carriers. J Clin Oncol 2002; 20(5):1260-8.
15. Olopade OI, Artioli G. Efficacy of risk-reducing salpingo-oophorectomy in women with
BRCA-1 and BRCA-2 mutations. Breast J 2004; 10(suppl 1):S5-9.
16. Moller P, Borg A, Evans DG, et al. Survival in prospectively ascertained familial breast cancer: analysis of a series stratified by tumour characteristics, BRCA mutations and oophorectomy. Int J Cancer 2002; 101(6):555-9.
17. Menkiszak J, Rzepka-Gorska I, Gorski B, et al. Attitudes toward preventive oophorectomy
among BRCA1 mutation carriers in Poland. Eur J Gynaecol Oncol 2004; 25(1):93-5.
18. Weitzel JN, McCaffrey SM, Nedelcu R, et al. Effect of genetic cancer risk assessment on surgical decisions at breast cancer diagnosis. Arch Surg 2003; 138(12):1323-8.
19. Scheuer L, Kauff N, Robson M, et al. Outcome of preventive surgery and screening for breast
and ovarian cancer in BRCA mutation carriers. J Clin Oncol 2002; 20(5):1260-8.
20. Ben David Y, Chetrit A, Hirsh-Yechezkel G, et al. National Israeli Study of Ovarian Cancer. Effect of BRCA mutations on the length of survival in epithelial ovarian tumors. J Clin Oncol 2002; 20(2):463-6.
21. Winchester DP. Breast cancer in young women. Surg Clin North Am 1996; 76(2):279-87.
22. Langston AA, Malone KE, Thompson JD, et al. BRCA1 mutations in a population-based
sample of young women with breast cancer. N Engl J Med 1996; 334(3):137-42.
23. Malone KE, Daling JR, Thompson JD, et al. BRCA1 mutations and breast cancer in the general population: analyses in women before age 35 years and in women before age 45 years with first-degree family history. JAMA 1998; 279(12): 922-9.
24. Frank TS, Deffenbaugh AM, Reid JE, et al. Clinical characteristics of individuals with
germline mutations in BRCA1 and BRCA2: analysis of 10,000 individuals. J Clin Oncol 2002; 20(6):1480-90.
25. Ford D, Easton DF, Stratton M, et al. Genetic heterogeneity and penetrance analysis of the
BRCA1 and BRCA2 genes in breast cancer families. Am J Hum Genet 1998; 62(3): 676-89.
26. Gershoni-Baruch R, Dagan E, Fried G, et al. Significantly lower rates of BRCA1/BRCA2 founder mutations in Ashkenazi women with sporadic compared with familial early onset breast cancer. Eur J Cancer 2000; 36(8):983-6.

G Genetic Testing for Inherited BRCA1 or BRCA2 Mutations (continued
QUEST Provider Handbook Benefit Policies 05/08
27. Hodgson SV, Heap E, Cameron J, et al. Risk factors for detecting germline BRCA1 and BRCA2 founder mutations in Ashkenazi Jewish women with breast or ovarian cancer. J Med Genet 1999; 36(5):369-73.
28. Hartge P, Struewing JP, Wacholder S, et al. The prevalence of common BRCA1 and BRCA2
mutations among Ashkenazi Jews. Am J Hum Genet 1999; 64(4):963-70.
29. Narod SA, Foulkes WD. BRCA1 and BRCA2: 1994 and beyond. Nat Rev Cancer 2004; 4(9):665-76.
30. BlueCross BlueShield Association. Genetic Testing for Inherited BRCA1 or BRCA2
Mutations. 2.04.02. 9/27/05.


H Home Apnea Monitor for Infants
CPT only © 2007, American Medical Association. All rights reserved (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Home cardiorespiratory (e.g., apnea) monitors generally monitor both respiratory and heart rates. An alarm will sound if there is respiratory cessation (apnea) beyond a predetermined time limit (e.g., 20 seconds) or if the heart rate falls below a preset rate (bradycardia).
II. Criteria/Guidelines
A home apnea monitor will be considered for the following conditions (subject to Limitations/ Exclusions and Administrative Guidelines):
A. Infants who have experienced an apparent life-threatening event; defined as an episode that is
frightening to observe and is characterized by some combination of apnea, color change, marked change in muscle tone, choking or gagging.
B. Infants with tracheostomies or anatomic abnormalities making them vulnerable to airway
compromises.
C. Infants with neurologic or metabolic disorders affecting respiratory control.
D. Infants with chronic lung disease (i.e., bronchopulmonary dysplasia), particularly those requiring supplemental oxygen, continuous positive airway pressure, or mechanical ventilation.
III. Limitations/Exclusions
Siblings with a history of sudden infant death syndrome (SIDS) do not establish medical necessity for use of a home apnea monitor for infants.
IV. Administrative Guidelines
A. Pre-certification is not required.
B. Medical records must be made available to HMSA if requested.
CPT Code Description 94774 Pediatric home apnea monitoring event recording including respiratory
rate, pattern and heart rate per 30-day period of time; includes monitor attachment, download of data, physician review, interpretation, and preparation of report.
94775 monitor attachment only (includes hook-up; initiation of recording and disconnection
94776 monitoring, download of information, receipt of transmission(s) and analyses by computer only
94777 physician review, interpretation and preparation of report only
HCPCS Code Description E0618 Apnea monitor, without recording feature E0619 Apnea monitor, with recording feature

QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Code Description 770.81 Primary apnea of newborn 770.82 Other apnea of newborn 770.89 Other respiratory problems after birth
V. Scientific Background
This policy is based on the American Academy of Pediatrics policy statement on Apnea, Sudden infant Death Syndrome, and Home Monitoring. The policy statement does not recommend apnea monitoring in SIDS siblings, noting that the theory that apneic episodes are related to SIDS has never been proven in spite of extensive research over several decades. In addition, epidemiologic studies have failed to document any impact of home cardiorespiratory monitoring for apnea and/or bradycardia on the incidence of SIDS. Moreover, the document noted that there is no evidence that the presence of apnea and/or bradycardia can identify a group at increased risk of SIDS, that home monitoring can provide warning in time for intervention to prevent sudden death, or that intervention would be successful in preventing unexpected death. The statement concludes that “given the lack of evidence that home cardiorespiratory monitoring has any impact on SIDS, prevention of SIDS is not an acceptable indication for home cardiorespiratory monitoring.” The American Academy of Pediatrics recommends that pediatricians should promote proven practices that decrease the risk of SIDS – supine sleep position, safe sleeping environments, and elimination of prenatal and postnatal exposure to tobacco smoke. Parents should also be advised that home cardiorespiratory monitoring has not been proven to prevent sudden unexpected death in infants.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
VII. References
1. American Academy of Pediatrics Policy Statement. Apnea, Sudden Infant Death Syndrome, and Home Monitoring. Pediatrics Vol. 111 No. 4 April 2003, pp 914-917.
2. Blue Cross Blue Shield Association. Medical Policy Reference Manual. Home Apnea
Monitors. Issue 2:2003. Policy # 1.01.06. No further revisions have been performed.

H Home Phototherapy for Neonatal Jaundice
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Home phototherapy for neonatal jaundice is a treatment that subjects a jaundiced infant to continuous light from a special lamp (phototherapy unit) for a prescribed period of time. Application of continuous phototherapy light helps reduce elevated bilirubin to acceptable levels. Successful phototherapy can prevent brain damage in an infant.
II. Criteria Guidelines
Home phototherapy is covered when the following criteria are met (subject to the Limitations/ Exclusions and Administrative Guidelines):
1. The infant is 38 weeks or more gestational age.
2. Total serum bilirubin at discharge or post-discharge must be monitored daily by a CLIA
approved lab and fall within the levels listed below:
Age Total Serum Bilirubin (mg/dL) 24 hours 8.5 – 11.5 36 hours 10.5 – 13.5 48 hours 12.0 – 15.0 60 hours 13.5 – 16.5 72 hours 15.0 – 18.0 84 hours 16.0 – 19.0 96 hours 17.0 – 20.0 120 hours 18.0 – 21.0
III. Limitations/Exclusions
A. The treating physician is responsible for ensuring the caregiver receives proper instructions relating to: infant care, use of home phototherapy, and follow-up treatment. These instructions must be in accordance with the American Academy of Pediatrics guidelines.
B. Home phototherapy is contraindicated for infants with any of the following risk factors,
including but not limited to:
1. Isoimmune hemolytic anemia
2. G6PD deficiency
3. History of asphyxia
4. Lethargy
5. Temperature instability
6. Infection, suspected or treated
7. Acidosis

QUEST Provider Handbook Benefit Policies Rev. 05/08
C. Home phototherapy is not indicated for infants with a gestational age of less than 38 weeks.
D. Transcutaneous bilirubin determinations are not an acceptable monitoring alternative once phototherapy is initiated.
E. Phototherapy should be discontinued once the total serum bilirubin level has fallen below the
age-specific range listed in the table above.
F. Refer to HMSA’s Home Health Care policy for eligibility requirements for home nursing care. Home nursing services, if applicable, is limited to the evaluation of the infant only, it does not include set up or retrieval of the phototherapy unit or instructing the caregiver on its use.
IV. Administrative Guidelines
A. Pre-certification is not required for home phototherapy for neonatal jaundice.
B. The DME supplier is responsible for obtaining and keeping the following information in the patient’s file:
1. The physician orders
2. Gestational age of the infant
3. Date/time of birth
4. Start/end dates of phototherapy services
5. Daily total serum bilirubin levels through the phototherapy period, including date and
time of collection.
C. Documentation of the caregiver’s homebound status must be kept in the patient’s medical file by the home health agency (if billing S9098).
D. HMSA will perform retrospective reviews to ensure that services rendered were appropriate
and may request supporting documentation from the DME supplier.
HCPCS Code Description E0202 Phototherapy (bilirubin) light with photometer S9098 Home visit, phototherapy services (e.g., bili-lite), including equipment
rental, nursing services, blood draw, supplies, and other services, per diem
ICD-9-CM Code Description 774.6 Unspecified fetal and neonatal jaundice
V. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.

H Home Phototherapy for Neonatal Jaundice (continued)
QUEST Provider Handbook Benefit Policies Rev. 05/08
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
VI. References
American Academy of Pediatrics Subcommittee of Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004 Jul; 114(1):297-316.

I Imaging Studies that Require Pre-certification
QUEST Provider Handbook Benefit Policies 05/08
I. Effective October 16, 2006, responsibility for pre-certification of the following is being transferred to National Imaging Associates, Inc. (NIA):
A. MRIs and MRAs that do not meet guidelines (required)
B. PET scans that do not meet guidelines (required)
(Note: It is suggested that NIA input be sought for all PET services.) II. In addition, consultation through NIA is available for the following:
A. Imaging services for which the ordering physician wishes to establish medical necessity
B. Imaging services for which the ordering physician would like to consult with a practicing radiologist regarding the efficacy of various options
III. The ordering physician can obtain pre-certification or consult with NIA by calling
1 (866) 306-9729, from 6 a.m. to 6 p.m., weekdays, Hawaii Time. IV. Clinical guidelines that have been adapted to meet HMSA requirements are available for reference
(see HMSA Diagnostic Imaging Guidelines). V. If more than one procedure is planned, a separate pre-certification number must be obtained for
each procedure ordered. VI. Pre-certification requirements apply only to outpatient services (POS 11 or 22). Services
performed in connection with an emergency department visit or observation room confinement (POS 23) and services rendered on an inpatient basis (POS 21) do not require pre-certification.
VII. The following lines of business are affected by the pre-certification requirements:
A. All private business plans, including PPO, HMO, Federal Plan 87, the EUTF Plan, individual plans and point-of-service (POS) plans
B. The HMSA Plan for QUEST Members
VIII. Pre-certification is not required for services ordered for 65C Plus or FEP members. IX. Pre-certification will not be given for the following:
A. Services that are considered experimental or investigative in nature
B. Services that are specifically excluded as benefits of HMSA plans X. A pre-certification number from NIA does not guarantee HMSA payment. Payment is subject to
plan benefits and deductibles, any applicable waiting periods and member eligibility at the time of service.


I Imatinib Mesylate (Gleevec)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Imatinib mesylate (Gleevec) is an oral protein-tyrosine kinase inhibitor that inhibits the abnormal bcr-abl tyrosine kinase created by the Philadelphia chromosome in chronic myeloid leukemia (CML). It inhibits proliferation and induces apoptosis in bcr-abl positive cell lines as well as fresh leukemic cells from Philadelphia chromosome positive chronic myeloid leukemia.
Imatinib is also an inhibitor of the receptor tyrosine kinases for platelet-deprived growth factor (PDGF) and stem cell factor (SCF), c-kit and inhibits PDGF and SCF mediated cellular events. In vitro, imatinib inhibits proliferation and induces apoptosis in gastrointestinal stromal tumor (GIST) cells, which express an activating c-kit mutation.
II. Criteria/Guidelines
Imatinib mesylate will be covered (subject to Administrative Guidelines) when recommended by an oncologist or a hematologist for the following patients:
A. Adult patients with Philadelphia chromosome positive chronic myeloid leukemia (ph+ CML)
in blast crisis, accelerated phase or chronic phase.
B. Pediatric patients (two years of age and older) with Ph+CML in chronic phase, who are newly diagnosed or whose disease has recurred after stem cell transplant or resistant to interferon-alpha therapy.
C. Adult patients with relapsed or refractory Philadelphia chromosome positive acute
lymphoblastic leukemia (Ph+ALL).
D. Adult patients with myelodysplastic/myeloprolifertive diseases (MDS/MPD) associated with PDGFR (platelet-derived growth factor receptor) gene rearrangements.
E. Adult patients with aggressive systemic mastocytosis (ASM) without the D816V c-Kit
mutation or with c-Kit mutational status unknown.
F. Adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukemia (CEL).
G. Adult patients with unresectable, recurrent and/or metastatic dermatofibrosarcoma protuberans
(DFSP).
H. Patients with Kit (CD117) positive unresectable and/or metastatic malignant gastrointestinal stromal tumors (GIST).
III. Administrative Guidelines
A. Pre-certification is required for imatinib mesylate. To pre-certify, please complete HMSA’s Drug Review Request form and mail or fax the request as indicated. Include the following documentation:
1. Current medical notes
2. Pathology reports

QUEST Provider Handbook Benefit Policies Rev. 05/08
3. Imaging studies (if applicable)
4. Pertinent lab reports (e.g., CBC, cytogenetic, molecular/genetic tests)
B. Initial approvals will be given for six months to evaluate the patient’s response to therapy.
C. Requests for continuation of therapy will be approved for 12 months as long as there is no evidence of disease progression or unacceptable toxicity.
IV. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guideline and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice, and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
V. References
1. American Cancer Society News Center. Gleevec: New Uses, New Warning. Available at http://cancer.org accessed on January 19, 2007.
2. FDA Label and Approval History for Gleevec, Available at http://www.accessdata.fds.gov
accessed January 08, 2008.
3. Gleevec prescribing information. Novartis Pharmaceuticals Corporation, East Hanover, NJ: September 2007.
4. Thompson Healthcare series. Drugdex evaluations. Imatinib updated 02/15/07.

I Intrastromal Corneal Ring Segments for Keratoconus (INTACS)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Intrastromal corneal ring segments, also known as INTACS, are prescribed, removable inserts designed to reshape the anterior surface of the cornea. The rings consist of two arc-shaped segments that are surgically inserted through a radial incision and are placed in the corneal stroma. The procedure is performed in an outpatient setting under local anesthesia.
Keratoconus is a non-inflammatory eye condition in which the normally round dome-shaped cornea progressively thins causing a cone-like bulge to develop. This results in significant visual impairment.
II. Criteria/Guidelines
A. INTACS prescription inserts are covered (subject to Limitations/Exclusions and Administrative Guidelines) for the treatment of keratoconus all of the following criteria are met:
1. The patient is no longer able to achieve vision of at least 20/40 or better with contact
lenses or glasses.
2. The patient has become intolerant to the use of contact lenses.
3. The patient demonstrates an inability to perform activities of daily living or occupational functions due to progressive vision deterioration.
4. The thickness of the cornea is greater than or equal to 450 microns at the proposed
incision site.
5. The central corneas are clear.
6. Corneal transplantation is the only other remaining option to improve functional vision. III. Limitations/Exclusions
A. INTACS is contraindicated in patients taking any of the following medications: isotretinoin, amiodarone or sumitriptan.
B. INTACS is contraindicated in patients with collagen vascular, autoimmune or
immunodeficiency diseases.
C. INTACS is not covered for any other indication except keratoconus. IV. Administrative Guidelines
A. Pre-certification is required for INTACS.
B. To pre-certify, please complete HMSA’s Pre-certification Request form and mail or fax the form as indicated. The pre-certification request must include documentation substantiating the progressive deterioration of the patient’s vision.

QUEST Provider Handbook Benefit Policies Rev. 05/08
CPT Code Description 0099T Intrastromal corneal ring segments (INTACS) L8699 Prosthetic implant, not otherwise specified
ICD-9-CM Code Description 371.60 Keratoconus, unspecified 371.61 Keratoconus, stable condition 371.62 Keratoconus, acute hydrops
V. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician. Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control. This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VI. References
1. Aetna. Corneal Remodeling Policy # 0023. Revised 01/23/07.
2. Alio JL, Artola A, Ruiz-Moreno JM, Hassanein A, Galal A, Awadalla MA. Changes in keratoconic corneas after intracorneal ring segment explantation and reimplantation. Ophthalmology 2004 Apr; 111(4):747-51.
3. BlueCross BlueShield of Tennessee Medical Policy Manual. Intrastromal Corneal Ring
Segments (ICRS) for Vision Correction. Effective 06/22/06.
4. Boxer W, Christie JP, Chandra NS, Chou B, Korn T, and Nepomuceno R. (2003). Intacs for keratoconus. Ophthalmology, 110 (5), 1031-1040.
5. Colin J, Cochener B, Savary G, et al. Correcting keratoconus with intracorneal rings. J
Cataract Refract Surg. 2000; 26(8):1117-1122.
6. Colin J, Cochener B, Savary G, et al. INTACS inserts for treating keratoconus: One-year results. Ophthalmology 2001; 108(8):1409-1414.
7. FDA-New Humanitarian Device Approval. INTACS Prescription Inserts for Keratoconus-
H04002. Updated June 6, 2006.

I Intrastromal Corneal Ring Segments for Keratoconus (INTACS) (continued)
QUEST Provider Handbook Benefit Policies Rev. 05/08
8. FDA INTACS Prescription Inserts for Keratoconus-H04002. Summary of Safety and Probable Benefit. Updated June 8, 2006.
9. Hellstedt T, Makela J, Uusitalo R, Emre S, Uusitalo R. Treating keratoconus with INTACS
corneal ring segments. J Refract Surg 2005 May-Jun; 21(3); 236-46.


L Leuprolide Acetate (Lupron)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description
Form: Injection Leuprolide acetate (Lupron) belongs to a class of drugs called gonadotropin-releasing hormone (GnRH) agonists. It is used to decrease the body’s production of specific hormones, natural chemicals that influence the behavior of certain cells. Because leuprolide acetate can reduce the production of both male and female hormones, it is used to treat specific conditions in men, women and children.
II. Criteria/Guidelines
A. Leuprolide acetate may be considered medically necessary for the following indications:
1. Prostate cancer
2. Anemia due to uterine leiomyomas
a. Women with uterine leiomyomata must meet all of the following criteria:
i. The patient must have been diagnosed with iron deficiency anemia secondary to vaginal bleeding associated with leiomyomata.
ii. The patient’s hemoglobin is less than 11, or hematocrit less than 33.
iii. The patient is scheduled for surgery to remove the leiomyomata, and the
physician feels that it is necessary to increase the hematocrit prior to surgery.
b. Therapy must continue uninterrupted for three months.
3. Precocious puberty
a. Leuprolide acetate is indicated for the treatment of central precocious puberty
(CPP), idiopathic or neurogenic, in children with the onset of secondary sexual characteristics before the age of eight in females and age nine in males.
b. Prior to initiation of leuprolide acetate therapy, the clinical diagnosis of central
precocious puberty must be accompanied by bone ate test results verifying that bone age is one year beyond chronological age.
4. Breast Cancer
Leuprolide acetate is indicated for off-label use in the palliative treatment of advanced breast cancer in premenopausal and perimenopausal women.

QUEST Provider Handbook Benefit Policies Rev. 05/08
III. Limitations/Exclusions A. Leuprolide acetate is not covered for any indications other than those listed in this policy.
Only limited information has been published and further research including randomized, controlled trials is required to determine its efficacy.
B. Leuprolide acetate as a treatment prior to surgery for leiomyomata in patients without anemia
is not indicated by the FDA and USPDI. It does not meet the criteria for off-label drug use.
C. Leuprolide acetate as a treatment for CPP should be discontinued before the age of 11 in females or the age of 12 in males except as specified in IV.A.2.
D. Leuprolide acetate as a treatment of endometriosis should have a duration of initial treatment
or retreatment limited to six months each. Reliable evidence shows that further studies or clinical trials are necessary to determine maximum tolerated dose, toxicity and safety. Treatment for this indication is limited to females age 18 or older.
IV. Administrative Guidelines
Pre-certification is required for any of the following indications as specified. Please complete the Drug Review Request and mail or fax the form as indicated.
1. Uterine leiomyomas: therapy that will extend beyond one course of treatment (three
months)
2. Central precocious puberty: therapy extending beyond age 11 or older for girls or age 12 or older for boys may be authorized when clinical notes, growth charts, and/or test results documenting the continued need to delay puberty beyond the normal age of onset are submitted. Examples include extreme short stature (height below the mean by more than two standard deviations and open growth plates).
3. Endometriosis: therapy that will extend beyond one course of treatment (six months).
4. For the off-label use in palliative treatment of advanced breast cancer. Documentation
of other treatments tried and failed (e.g., Tamoxifen) is required.
A. Therapy with leuprolide acetate beyond one course of treatment must be continuous and without interruption between courses.
HCPCS Code Description J1950 Injection, leuprolide acetate (for depot suspension), per 3.75 mg. (use this
code for Lupron Depot) J9217 Leuprolide acetate (for depot suspension), 7.5 mg (use this code for Lupron
Depot, Eligard) J9218 Leuprolide acetate, per 1 mg (use this code for Lupron, Eligard) J9219 Leuprolide acetate implant, 65 mg (use this code for Lupron implant)

L Leuprolide Acetate (Lupron) (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
ICD-9-CM Code Description 174.0 – 174.9 Malignant neoplasm of female breast 185 Malignant neoplasm of prostate 218.0 – 218.9 Uterine leiomyoma (fibroids) 259.1 Other endocrine disorders, Precocious sexual development and puberty, not
elsewhere classified 617.0 – 617.9 Endometriosis
V. Scientific Background
Anemia due to uterine fibroids According to the Agency for Healthcare Research and Quality (AHRQ) Evidence Report/ Technology Assessment: Number 34, Management of Uterine Fibroids, there is insufficient data to allow conclusions about the most appropriate therapy for a given symptomatic patient. The majority of randomized clinical trials identified which used gonadotropin-releasing hormone (GnRH) agonists were done as adjunctive treatment prior to uterine surgery. The remainder of citations were uncontrolled case series, case series with historical or nonrandomized controls, case-control studies, or in a few instances, prospective cohort studies. The principal findings of the report included the finding that there is good evidence based on randomized trials that use of GnRH agonists prior to myomectomy or hysterectomy reduces estimated blood loss and may facilitate certain surgical approaches. There is also no information on long-term clinical significance of these effects. Also, there is no data supporting prophylactic hysterectomy or myomectomy in women with asymptomatic fibroids.
According to USP DI dosing information, therapy for anemia due to uterine leiomyomas should continue uninterrupted for three months. Retreatment is not recommended. If retreatment is contemplated, bone density should be assessed prior to beginning treatment to verify that values are in the normal range. In clinical trials, GnRH agonists reduced fibroid size and were useful as a pre-operative adjunct with rapid regrowth of fibroids following discontinuation. Available literature states short-term treatment only is recommended (i.e., one to three months) especially to prevent bone loss after menopause.
Central precocious puberty According to USP DI dosing information, dose must be individualized for each patient and titrated upward until the patient’s pituitary-gonadal axis is suppressed, according to clinical and/or laboratory parameters. Usually the dose that adequately suppresses the pituitary-gonadal axis is appropriate for the entire therapy. However, there are insufficient data to guide dosage adjustments as a child’s weight changes, a special concern for children who started therapy at a very early age at a low dose. Careful monitoring for suppression of the pituitary-gonadal axis is required, especially one or two months after treatment initiation or following changes in dose.
If the patient responds and tolerates leuprolide therapy, treatment should continue until resumption of puberty is desired. Discontinuation of leuprolide therapy should be considered before the age of 11 years in females and 12 years in males. Normal function of pituitary-gonadal axis is restored within 4 to 12 weeks after treatment discontinuation.
QUEST Provider Handbook Benefit Policies Rev. 05/08
Endometriosis According to USP DI dosing information, it is recommended that therapy begin with the first day of the menstrual cycle after pregnancy has been ruled out.
Development of amenorrhea is usually evidence of a clinical response, although spotting or bleeding from the atrophic endometrium can still occur.
Therapy should continue uninterrupted for six months. Retreatment is not recommended. However, if retreatment is contemplated, bone density should be assessed prior to beginning treatment to verify that values are in the normal range.
Studies of leuprolide acetate for endometriosis indicate that six months is an appropriate length for therapy. There is a lack of safety data with long-term use as well as concerns in the available literature regarding effects on bone density.
Prostatic carcinoma According to USP DI dosing information, patients receiving leuprolide should be under supervision of a physician experienced in cancer chemotherapy.
Isolated short-term worsening of neurologic symptoms may contribute to paralysis with or without fatal complications in patients with vertebral metastases. For patients at risk, therapy may be initiated with daily leuprolide injection for the first two weeks to observe patient reaction, since worsening of symptoms occasionally requires discontinuation of therapy and possible surgical intervention.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guideline to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice, and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.

L Leuprolide Acetate (Lupron) (continued)
QUEST Provider Handbook Benefit Policies Rev. 05/08
VII. References 1. Arkansas Blue Cross Blue Shield. Leuprolide. Reviewed March 2006.
2. BCBSA. Combined Androgen Blockade for the Treatment of Metastatic Prostate Cancer.
5.01.14. Issued 1:2003. No further review scheduled.
3. Blue Cross Blue Shield of Minnesota. Lupron. Reviewed November 12, 2003.
4. TAP Pharmaceutical Products Inc. (February 2004) Lupron prescribing information. Retrieved May 23, 2006, from Prescribing Information.
5. Ornstein MD, Surrey ES, et al. Leuprolide acetate depot and hormonal add-back in
endometriosis: a 12-month study. Lupron Add-Back Study Group. Obstet Gynecol. 1998 Jan; 91(1):16-24.
6. Jasonni VM, D’Anna R, et al. Randomized double-blind study evaluating the efficacy on
uterine fibroids shrinkage and on intra-operative blood loss of different length of leuprolide acetate depot treatment before myomectomy. Acta Obstet Gynecol Scand. 2001 Oct; 80(10):956-8.
7. Management of Uterine Fibroids. Summary, Evidence Report/Technology Assessment:
Number 34. AHRQ Publication No. 01-E051, January 2001. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/clinic/epcsums/utersumm.html.
8. USPDI Drug Information for the Health Care Professional. Leuprolide (Systemic). 11/29/2005
Thomson Micromedex.


M MRI, Functional
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
I. Description Before neurological surgery for seizure disorders or resection of brain tumors, localization of certain areas of the brain, such as speech centers, is important. For example, from 25 to 60 percent of patients who undergo left anterior temporal lobectomy develop dysnomia (language/naming difficulties).
Most often these “eloquent” areas are assessed using the Wada test and direct electrical simulation. Both of these tests are invasive and require involvement of various specialists. The Wada test involves angiography and injection of amobarbital into the carotid artery. Direct electrical stimulation involves surgical placement of electrodes in the brain.
Functional Magnetic Resonance Imaging (MRI) is proposed as a noninvasive alternative for evaluation of these eloquent brain areas. Functional MR imaging uses sequences based on T2-weighted blood oxygen. Images are collected as various activities are conducted. Laterality indices are calculated reflecting the interhemispheric difference between activated volumes in the left and right hemispheric regions of interest. These studies are often done on MR scanners with field strengths of 1.5 Tesla or greater.
II. Criteria/Guidelines
Functional MRI is considered medically necessary in the preoperative evaluation of patients with seizures or brain tumors, who are candidates for neurosurgical therapy, when the results of testing will obviate the need for either the Wada test or direct electrical stimulation.
III. Limitations/Exclusions
Functional MRI is considered investigational for all other applications. IV. Administrative Guidelines
A. Pre-certification is required. Effective July 1, 2007, National Imaging Associates (NIA) will be handling these pre-certification requests.
Ordering Physician
1. The ordering physician is responsible for obtaining pre-certification.
a. To obtain pre-certification, physicians should call the NIA, toll free, at
1 (866) 306-9729, from 6 a.m. to 6 p.m. weekdays, Hawaii Time. The NIA center is closed on Saturdays, Sundays and federal holidays.
b. If a planned study is scheduled after hours, on weekends or holidays, call the NIA
in advance to obtain pre-certification.
c. If a study is performed on an urgent basis, contact the NIA on the following business day to obtain a retrospective certification.
2. If additional clinical review by NIA clinical staff is required, the ordering physician can
check the status of a pending pre-certification request through NIA’s Authorization Verification System at RadMD.com. Review RadMD Get Started instructions and refer to the RadMD Quick Start to request an exam.
CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies 05/08
B. The following codes differentiate between circumstances when a physician or psychologist does all of the functional testing and when the testing is done by other professionals:
CPT Code Description 70554 Magnetic resonance imaging, brain, functional MRI; including test
selection and administration of repetitive body part movement and/or visual stimulation, not requiring physician or psychologist administration
70555 Magnetic resonance imaging, brain, functional MRI; requiring physician or psychologist administration of entire neurofunctional testing
C. The physician or psychologist that administers the testing would code using the following CPT
code:
CPT Code Description 96020 Neurofunctional testing selection and administration during noninvasive
imaging functional brain mapping, with test administered entirely by a physician or psychologist, with review of test results and report
V. Scientific Background
Studies (2 Medina) have summarized the high degree of concordance of language lateralization of functional MR imaging and either Wada test or direct electrical stimulation. (2) In this summary, functional MRI was concordant with the Wada test in 78 of 83 (94%) cases and with direct electrical stimulation in 23 of 26 (88%) cases.
Sabsevitz and colleagues reported on a series of 24 consecutive patients who underwent both functional MRI and Wada testing before left anterior temporal lobectomy for seizures disorders. While both tests were predictive of language changes, in this study functional MRI had a sensitivity of 100% and specificity of 57% while results for the Wada test were 100% and 43% respectively. (4)
Medina and colleagues evaluated 60 consecutive patients prior to surgery. (2) In 53 patients’ language mapping was performed, in 33 motor mapping, and in 7 visual mapping. The functional MRI study revealed change in anatomic location or lateralization of language-receptive (Wernicke) in 28% of patients and in language-expressive (Broca) in 21%. In 38 (63%) patients, functional MRI helped to avoid further studies, including Wada test. In 31 (52%) and 25 (42%) of the patients, intraoperative mapping and surgical plans were altered because of functional MRI results.
Petrella and colleagues reported on the impact of functional MRI preoperatively on 39 consecutive patients with brain tumors. (3) In four patients, additional tests, e.g. the Wada test, were not ordered because of the functional MRI result. Treatment plans differed in 19 patients after functional MRI with a more aggressive approach recommended after imaging in 18 patients. However, the impact of the altered treatment plans on patient outcome was not assessed. Functional MRI resulted in reduced surgical time for 22 patients; it also led to decisions to perform crainiotomy in 13 patients where less invasive approaches had been initially planned.
Thus, studies show that functional MRI is comparable to the Wada test and direct electrical stimulation in localizing certain eloquent functions; although there are less data for direct electrical

M MRI, Functional (continued)
QUEST Provider Handbook Benefit Policies 05/08
stimulation. In patients who are to undergo neurosurgery for seizures or brain tumors, functional MRI may obviate the need for these tests. However, the impact of function MRI on other outcomes in these patients is uncertain.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VII. References
1. Blue Cross and Blue Shield Association. Functional MRI. Policy 6.01.47 Original policy date 12/12/06.
2. Medina LS, Bernal B, Dunoyer C, et al. Seizure disorders: Functional MR imaging for
diagnostic evaluation and surgical treatment - prospective study. Radiology 2005; 236:247-53.
3. Petrella JR, Shah LM, Harris KM, et al. Preoperative functional MR imaging localization of language and motor areas: Effect of therapeutic decision making in patients with potentially resectable brain tumors. Radiology. 2006; 240:793-802.
4. Sabsevitz DX, Swanson SJ, Hammeke TA, et al. Use of preoperative functional neuroimaging
to predict language deficits from epilepsy surgery. Neurology. 2003; 60:1788-92.


N Non-Ionic Contrast Agents
QUEST Provider Handbook Benefit Policies Rev. 05/08
Effective for services rendered March 1, 2008, HMSA will no longer apply high-risk criteria to claims for the use of non-ionic contrast agents.


O Oscillatory Device for Bronchial Drainage (The Vest)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description The Vest™ is a portable oscillatory bronchial drainage system that provides external thoracic percussion. It consists of a non-stretching inflatable vest linked to an air pulse generator by two flexible hoses. The generator rapidly inflates and deflates compressing and releasing the chest wall to create airflow within the lungs, moving the mucous toward the larger airways where it can be cleared by coughing. This airway clearance therapy is commonly referred to as high-frequency chest wall oscillation and promotes respiratory secretions by an individual without the assistance of a caregiver.
II. Criteria/Guidelines
The Vest™ is covered when all of the following criteria are met (subject to the Limitations/ Exclusions and Administrative Guidelines in this policy):
1. The device must be recommended by a pulmonologist.
2. The patient has a diagnosis of cystic fibrosis or bronchiectasis.
3. The patient has been hospitalized more than once for pulmonary related conditions
within the past two years.
4. Recent pulmonary function studies demonstrate all of the following:
Forced expiratory volume (FEV-1) < 80 percent of predicted Forced vital capacity (FVC) < 50 percent of predicted Forced expiratory flow (FEF) (25 to 75) has decreased by 25 percent in the past year
5. Caregiver is unable to provide effective chest percussion and postural drainage.
6. Alternative therapy (e.g., daily percussion and postural drainage (P/PD), autologous
drainage or positive end expiratory pressure, flutter link device) is ineffective, not tolerated, or contraindicated.
III. Limitations/Exclusions
Individuals with a contraindication for external manipulation of the thorax as defined by the American Association of Respiratory Care (AARC) will be excluded from use of the bronchial drainage system vest. These contraindications include:
1. Bronchospasms
2. Complaint of chest wall pain
3. Unstable head and/or neck injury
4. Subcutaneous emphysema
5. Recent epidural spinal infusion or spinal anesthesia
6. Recent skin grafts, or flaps, on the thorax

QUEST Provider Handbook Benefit Policies Rev. 05/08
7. Burns, open wounds and skin infections of the thorax
8. Recently placed transvenous pacemaker or subcutaneous pacemaker
9. Osteomyelitis of the ribs
10. Active hemorrhage with hemodynamic instability
11. Suspected pulmonary tuberculosis
12. Lung contusion IV. Administrative Guidelines
A. Pre-certification is required. To pre-certify, please complete HMSA’s Pre-certification Request and mail or fax the form as indicated. Requests must include the following documentation from the medical record:
1. CT scan or bronchiogram results for patients with bronchiectasis.
2. More than one hospitalization in the past two years.
3. Recent pulmonary function study results.
4. The alternative therapy is ineffective, not tolerated or contraindicated or the caregiver is
unable to provide effective chest therapy.
B. Authorizations will be given for a rental period of two months. After the two month rental period, the device may be considered for purchase. The physician must submit documentation from the medical record that the patient is compliant with the use of The Vest.
HCPCS Code Description E0483 High-frequency chest wall oscillation air-pulse generator system, (includes
hoses and vest), each
ICD-9-CM Code Description 277.00 Cystic fibrosis, without mention of meconium ileus 277.02 Cystic fibrosis, with pulmonary manifestations 494.0 Bronchiectasis, without acute exacerbation 494.1 Bronchiectasis with acute exacerbation
V. Scientific Background
A literature search included a number of small, randomized studies that compared different mucus clearance techniques, typically in crossover studies. Pulmonary function and weight of expectorated sputum are typically analyzed immediately after treatment. Thus these small short-term studies focus on intermediate outcomes, and do not include any data regarding long-term stabilization or improvement of lung function or a decrease in pulmonary exacerbations resulting in hospitalization.

O Oscillatory Device for Bronchial Drainage (The Vest) (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
Arens and colleagues prospectively studied 50 patients with cystic fibrosis admitted for acute pulmonary exacerbation to randomly receive either conventional physiotherapy or high-frequency chest compression three times a day. Both groups showed significant improvements in clinical status and pulmonary function tests were observed after seven and 14 days of treatment. Both methods were found to be equally safe and effective in acute pulmonary exacerbations in cystic fibrosis patients.
Braggion and colleagues conducted a study of 16 hospitalized patients with cystic fibrosis to compare short-term efficacy of three different chest physiotherapy (CPT) regimens: postural drainage, positive expiratory pressure physiotherapy and high-frequency chest compression physiotherapy. The three CPT regimens and a control treatment (CONT) were administered in a random sequence, each patient receiving each treatment twice a day (in 50 minute sessions) for two consecutive days. Wet and dry weights of sputum collected during the sessions were greater for all CPT regimens than for CONT. No significant differences between the three CPT regimens for both wet and dry weights were found when the number of coughs was taken into account.
Kluft and colleagues in a crossover trial, compared chest physical therapy and postural drainage (CPT/PD) to high-frequency chest wall oscillation (HFCWO) in stable cystic fibrosis patients. Twenty-nine patients were randomly assigned to alternate CPT/PD and HFCWO, on a daily basis, over a four-day period. Each patient received two days of each form of therapy; treatment frequency and length of treatment were the same for both techniques. Significantly more sputum was expectorated during HFCWO than during CPT/PD as determined by both wet and dry measurements.
Oermann and colleagues conducted a pilot study of 24 patients with cystic fibrosis who were randomly assigned to receive either The Vest™ Airway Clearance System or the Flutter device for four weeks followed by crossover to the other group. Spirometry, lung volume measures, quality of life and patient satisfaction were measured after each four-week treatment period. The only significant difference between the two groups was patient satisfaction; 50 percent of the participants preferred The Vest™ Airway Clearance System, while 37 percent preferred the flutter device.
Varekojis and colleagues compared high-frequency chest wall compression using The Vest ä and intrapulmonary percussive ventilation using the Percussionaire device to percussion and postural drainage (P/PD) in 24 hospitalized patients with cystic fibrosis. Patients used each modality for two days in a randomized order over a six-day period. While wet sputum weights from use of the Percussionaire device were significantly greater than The Vest™, there was no significant difference in any of the modalities in dry sputum weights. In addition, patients found use of each of the devices to be equally acceptable when questioned about comfort, convenience, effectiveness and ease of use.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.

QUEST Provider Handbook Benefit Policies Rev. 05/08
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VII. References
1. American Association Respiratory Care (AARC) clinical practice guideline. Postural drainage therapy. Respiratory Care. December 1991; 36(12): 1418-1426.
2. Arens R, Gozal D, Omlin KJ, et al. Comparison of high-frequency chest compression and
conventional chest physiotherapy in hospitalized patients with cystic fibrosis. American Journal Respiratory Critical Care Medicine. October 1994; 150(4): 1154-1157.
3. Blue Cross and Blue Shield Association, Medical Policy Reference Manual. Oscillatory
devices for the treatment of cystic fibrosis and Other Respiratory Disorders. Policy #1.01.15. Issue 4:2006 (October).
4. Blue Cross Blue Shield of Tennessee, Percussion Devices for the Treatment of Respiratory
Conditions. Effective 7/26/2007.
5. Braggion C, Cappelletti LM, Cornacchia M, et al. Short-term effects of three chest physiotherapy regimens in patients hospitalized for pulmonary exacerbations of cystic fibrosis: A cross-over randomized study. Pediatric Pulmonology. January 1995; 19(1):16-22.
6. Medicare: LCD for High Frequency Chest Wall Oscillation Devices (L12739). Revised
7/1/2007.
7. Health Technology Assessment Information Service, Windows on Medical Technology™. “High-frequency chest compression for cystic fibrosis.” October 2000:1-18.
8. Health Technology Assessment Information Service, Target database. High frequency chest
compression for chronic obstructive pulmonary disease. March, 2003.
9. Kluft J, Beker L, Castagnino M, et al. Comparison of bronchial drainage treatments in cystic fibrosis. Pediatr Pulmonol. October 1996; 22 (4):271-324.
10. Langenderfer B. Alternatives to percussion and postural drainage. A review of mucus
clearance therapies: percussion and postural drainage, autogenic drainage, positive expiratory pressure, flutter valve, intrapulmonary percussive ventilation, and high-frequency chest compression with the ThAIRapy Vest. Journal of Cardiopulmonary Rehabilitation. July-August 1998; 18(4):283-289.
11. Oermann CM, Sockrider MM, Giles D, et al. Comparison of high-frequency chest wall
oscillation and oscillating positive expiratory pressure in the home management of cystic fibrosis: a pilot study. Pediatr Pulmonol 2001; 32(5):372-377.

O Outpatient Surgical (PRG) List
QUEST Provider Handbook Benefit Policies Rev. 05/08
Effective May 1, 2008, the QUEST plan adopted the list of codes used by HMSA for its private plans. Please refer to the list in the HMSA Provider E-library for its private business plans.


P Physician Responsibility for Obtaining Precertification of Imaging Studies
(Continued on Next Page) QUEST Provider Handbook Benefit Policies 05/08
I. Effective October 16, 2006, the pre-certification of diagnostic imaging is being transferred to National Imaging Associates, Inc. (NIA). Pre-certification is required for:
A. MRIs and MRAs that do not meet guidelines for coverage
B. PET scans that do not meet guidelines for coverage
(Note: It is suggested the NIA input be sought for all PET services.) II. In addition, consultation through NIA is available for the following:
A. Imaging services for which the ordering physician wishes to establish medical necessity
B. Imaging services for which the ordering physician would like to consult with a practicing radiologist regarding the efficacy of various options
III. Pre-certification is not required for MRI, MRA or PET services when performed in the emergency
department or observation room or for services performed on an inpatient basis. IV. The ordering physician is responsible for obtaining pre-certification. Physicians may call the NIA
toll free at 1 (866) 306-9729, from 6 a.m. to 6 p.m., weekdays, Hawaii Time.
A. NIA’s call center is closed on Saturdays, Sundays and federal holidays.
B. If a planned study is to be performed after hours or on weekends or holidays, the ordering physician should contact the NIA in advance to obtain pre-certification.
C. If a study is on an urgent basis, the physician should contact the NIA on the following business
day to obtain pre-certification.
D. The average call takes less than five minutes to complete. V. The NIA Call Center is staffed with experienced Call Center representatives, nurses, board-certified
radiologists and physicians from other specialties.
A. NIA will request information about the patient’s symptoms, past clinical history and prior treatment, and the physician should have this information available at the time of the call.
Click here for a sample NIA Information Checklist that can be printed and kept by the telephone.
B. Evidence-based clinical guidelines and algorithms that have been modified to meet HMSA’s
needs are used to speed-up the consultation, and immediate pre-certification can be given by NIA staff about 60 percent of the time.
C. If clinical input is required, the case will be referred to clinical staff for review. In these cases
a determination can generally be made within two working days, assuming all pertinent clinical information is available.

QUEST Provider Handbook Benefit Policies 05/08
VI. A pre-certification number from NIA does not guarantee HMSA payment. Payment is subject to plan benefits and deductibles, any applicable waiting periods and member eligibility at the time of service.
VII. Clinical guidelines that have been adapted to meet HMSA’s needs are available for reference (see
HMSA Diagnostic Imaging Guidelines). The guidelines are presented in the form of a PDF file that can be bookmarked or printed for future reference. The guidelines are frequently updated based on the latest medical literature, specialty criteria sets and empirical data.

P Place of Treatment Program – Office Procedure List
QUEST Provider Handbook Benefit Policies Rev. 05/08
Effective July 1, 2008, the QUEST plan is adopting the list of codes used by HMSA for its private plans. Please refer to the list in the HMSA Provider E-Library for its private business plans.


P Place of Treatment Program – Outpatient Procedure List
QUEST Provider Handbook Benefit Policies Rev. 05/08
Effective July 1, 2008 the QUEST plan is adopting the list of codes used by HMSA for its private plans. Please refer to the list in the HMSA Provider E-Library for its private plans.


S Spinal Cord Stimulators for Pain Management
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Spinal cord stimulation delivers low voltage electrical stimulation to the dorsal columns of the spinal cord to block the sensation of pain. The neurophysiology of pain relief after spinal cord stimulation is uncertain, but may be related to either activation of an inhibitory system or blockage of facilitative circuits. Spinal cord stimulation devices consist of several components: 1) the lead that delivers the electrical stimulation to the spinal cord; 2) an extension wire that conducts the electrical stimulation from the power source to the lead, and 3) a power source that generates the electrical stimulation. The lead may incorporate from four to eight electrodes, with eight electrodes more commonly used for complex pain patterns, such as bilateral pain or pain extending from the limbs to the trunk. There are two basic types of power source. In one type, the power source (battery) can be surgically implanted. In another a radiofrequency receiver is implanted, and the power source is worn externally with an antenna over the receiver. Totally implantable systems are most commonly used.
The patient’s pain distribution pattern dictates at what level in the spinal cord the stimulation lead is placed. The pain pattern may influence the type of device used; for example, a lead with eight electrodes may be selected for those with complex pain patterns or bilateral pain. Implantation of the spinal cord stimulator is typically a two-step process. Initially, the electrode is temporarily implanted in the epidural space, allowing a trial period of stimulation. Once treatment effectiveness is confirmed, defined as at least 50 percent reduction in pain, the electrodes and radio-receiver/transducer are permanently implanted. Successful spinal cord stimulation may require extensive programming of the neurostimulators to identify the optimal electrode combinations and stimulation channels. Computer-controlled programs are often used to assist the physician in studying the millions of programming options when complex systems are used.
II. Criteria/Guidelines
A. Spinal cord stimulation is covered (subject to the Limitations/Exclusions and Administrative Guidelines below) for the treatment of severe and chronic pain of the trunk or limbs that is refractory to all other pain therapies.
B. Patient selection focuses on determining whether or not the patient is refractory to other types
of treatment. All of the following criteria must be met before implantation of a temporary electrode:
1. The treatment is used only as a last resort; other treatment modalities including
pharmacological, surgical, psychological, and/or physical have been tried and failed or are judged to be unsuitable or contraindicated;
2. Pain is neuropathic in nature; i.e., resulting from actual damage to the peripheral nerves.
Common indications include, but are not limited to failed back syndrome, complex regional pain syndrome (i.e., reflex sympathetic dystrophy), arachnoiditis, radiculopathies, phantom limb/stump pain, peripheral neuropathy;
3. No serious untreated drug habituation exists;
4. Patient was carefully screened, evaluated and diagnosed by a multidisciplinary team
prior to application of this therapy.

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies Rev. 05/08
C. In addition to the above criteria, the following must be met prior to permanent implantation of the stimulator:
1. The patient demonstrates at least 50% pain relief for one week with a temporarily
implanted electrode preceding permanent implantation. III. Limitations
A. Spinal cord stimulation is not covered for all other indications including but not limited to the following:
1. Critical limb ischemia as a technique to forestall amputation.
2. Nociceptive pain (resulting from irritation, not damage to the nerves)
3. Central deafferentation pain (related to CNS damage from a stroke or spinal cord injury).
IV. Administrative Guidelines
A. Pre-certification is required before implantation of a temporary electrode AND before permanent implantation of the stimulator. To pre-certify, please complete HMSA’s Pre-certification Request and mail or fax the form as indicated along with documentation demonstrating that criteria have been met.
B. The following documentation should be included with the pre-certification request for the
implantation of a temporary electrode:
1. Clinical notes related to the diagnosis and treatment of chronic neuropathic pain of the trunk or limbs.
2. Documentation of all treatments tried and failed (e.g., medications, surgical notes,
physical therapy notes, psychological notes, etc.).
3. Consultation notes from a psychologist and/or psychiatrist.
C. The following must be submitted before the permanent implantation of the stimulator:
1. The patient’s pain log (e.g., diary) and physician clinical notes documenting a successful one week trial of a temporarily implanted electrode.
CPT Code Description 63650 Percutaneous implantation of neurostimulator electrode array; epidural 63655 Laminectomy for implantation of neurostimulator electrode plate/paddle;
epidural 63685 Insertion of replacement of spinal neurostimulator pulse generator or
receiver, direct or inductive coupling Code for revision/removal: 63688 Revision of removal of implanted spinal neurostimulator pulse generator or
receiver

S Spinal Cord Stimulators for Pain Management (continued)
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
CPT Code Description Codes for programming spinal cord stimulators: 95970 Electronic analysis of implanted neurostimulator pulse generator system
(e.g., rate, pulse amplitude and duration, configuration of wave form, battery status, electrode selectability, output modulation, cycling, impedance and patient compliance measurements); simple or complex brain, spinal cord, or peripheral (i.e., cranial nerve, peripheral nerve, autonomic nerve, neuromuscular) neurostimulator pulse generator/transmitter, without reprogramming
95971 simple spinal cord, or peripheral (i.e., peripheral nerve, autonomic nerve, neuromuscular) neurostimulator pulse generator/transmitter, with intraoperative or subsequent programming
95972 complex spinal cord, or peripheral (except cranial nerve) neurostimator pulse generator/transmitter, with intraoperative subsequent programming, first hour
95973 complex spinal cord, or peripheral (except cranial nerve) neurostimulator pulse generator/transmitter, with intraoperative subsequent programming, each additional 30 minutes after first hour
HCPCS Code Description L8680 Implantable neurostimulator electrode, each L8685 Implantable neurostimulator pulse generator, single array, rechargeable,
includes extension L8686 Implantable neurostimulator pulse generator, single array, nonrechargeable,
includes extension L8687 Implantable neurostimulator pulse generator, dual array, rechargeable,
includes extension L8688 Implantable neurostimulator pulse generator, dual array, nonrechargeable,
includes extension ICD-9-CM Procedure
Description
02.93 Implantation or replacement of intracranial neurostimulator lead(s) 03.93 Insertion or replacement of spinal neurostimulator lead(s) 86.94 Insertion or replacement of single array neurostimulator pulse generator,
not specified as rechargeable 86.95 Insertion or replacement of dual array neurostimulator pulse generator, not
specified as rechargeable 86.97 Insertion or replacement of single array rechargeable neurostimulator pulse
generator 86.98 Insertion or replacement of dual array rechargeable neurostimulator pulse
generator ICD-9-CM Diagnosis
Description
See “Pain” in ICD-9 diagnosis index

QUEST Provider Handbook Benefit Policies Rev. 05/08
V. Scientific Background The bulk of published literature regarding spinal cord stimulation (SCS) consists of case series. In a systematic literature synthesis of these studies, Turner and colleagues reported that in patients with chronic low back pain, an average of 59 percent of patients had 50 percent or greater pain relief. (1)
Preliminary results of a randomized controlled trial reported that a significantly greater proportion of patients initially randomized to repeat lumbosacral surgery opted to cross over to the SCS arm of the trial, compared to those initially in the SCS of the trial crossing over to lumbosacral surgery. (2) A prospective multicenter study of SCS in 219 patients with chronic back and extremity pain reported successful management of pain in 55 percent of patients. (3) Most recently, Kemler and colleagues reported on favorable outcomes of SCS among patients with chronic reflex sympathetic dystrophy who were randomized to the SCS arm, as compared to those treated with physical therapy alone. (4) The favorable outcomes were still present at two years’ follow-up. (5)
2005 Update A literature search was performed on the MEDLINE database for the period of 1998 through June 2005, with a specific focus on SCS as a treatment of limb ischemia.
Critical limb ischemia is described as pain at rest or the presence of ischemic limb lesions. If the patient is not a suitable candidate for limb revascularization (typically due to insufficient distal runoff), it is estimated that amputation will be required in 60 percent to 80 percent of these patients within a year. SCS has been investigated in this small subset of patients as a technique to relieve pain and decrease the incidence of amputation. Klomp and colleagues conducted a study that randomized 120 patients with critical limb ischemia not suitable for vascular reconstruction to undergo either best medical care or medical care in addition to spinal cord stimulation. The primary endpoint was limb survival at two years. (6) Amputation-free survival was not improved nor was the risk of major amputation significantly reduced. Both groups also reported similar levels of pain reduction. In both groups, the rates of amputation were highest within the first three months of the study, reflecting the limitations with both treatment options.
2006 Update A search of the MEDLINE database was performed for the period of January 2005 through September 2006 with a focus on SCS as a treatment of limb ischemia. There are no new clinical studies on this topic.
A systematic review from the Cochrane group on use in peripheral vascular diseases was updated in 2005. Included were six European studies of generally good quality with a total of 444 patients. (7) None of the studies were blinded due to the nature of the treatment. At 12 months’ follow-up, limb salvage improved by 11 percent compared with any form of conservative treatment with a number needed to treat (NNT) of nine. The SCS patients required significantly less analgesics, and more patients reached Fontaine stage II than in the conservative group. There was no difference in ulcer healing. The overall risk of complications or additional SCS treatment was 17 percent, with a number needed to harm (NNH) of six. The report concludes that there is evidence to favor SCS over standard conservative treatment to improve salvage and clinical situation in patients with critical leg ischemia and that, “The benefits of SCS against the possible harm of relatively mild complications and costs must be considered.” Analysis of data and cost calculations from a previously published study (6) showed that the difference in amputation rate at 12 months was no longer present at 24 months. (8) There was no difference in survival rate at 24 months.

S Spinal Cord Stimulators for Pain Management (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
Evidence supports a decrease in pain with a short-term decrease in limb amputations following treatment with SCS. Complications include the need for operative repositioning procedures. There is no scientific evidence for improvement in pain and limb salvage at an endpoint of 24 months.
The use of SCS for other conditions such as visceral pain has been reported. The British Pain Society recommends that its use in this and other emerging indications be carefully audited (9).
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the medical necessity criteria to the case at issue in light of any supporting documentation.
VII. References
1. Turner JA, Loeser JD, Bell KG. Spinal cord stimulation for chronic low back pain: a systematic literature synthesis. Neurosurgery 1995; 37(6):1088-96.
2. Burchiel KJ, Anderson VC, Brown FD, et al. Prospective, multicenter study of spinal cord
stimulation for relief of chronic back and extremity pain. Spine 1996; 21(23):2786-94.
3. North RB, Kidd DH, Lee MS, et al. A prospective, randomized study of spinal cord stimulation versus reoperation for failed back surgery syndrome: initial results. Stereotact Funct Neurosurg 1994; 62(1-4):267-72.
4. Kemler MA, Barendse GA, van Kleef M, et al. Spinal cord stimulation in patients with chronic
reflex sympathetic dystrophy. N Engl J Med 2000; 343(9):618-24.
5. Kemler MA, De Vet HC, Barendse GA, et al. The effect of spinal cord stimulation in patients with chronic reflex sympathetic dystrophy: two years’ follow-up of the randomized controlled trial. Ann Neurol 2004; 55(1):13-8.
6. Klomp HM, Spincemaille GH, Steyerberg EW, et al. Spinal cord stimulation in critical limb
ischemia: a randomized trial. Lancet 1999; 353(9158):1040-4.
7. Ubbink DT, Vermeulen H. Spinal cord stimulation for non-reconstructable chronic critical leg ischaemia. Cochrane Database Syst Rev 2005; 3:CD004001.

QUEST Provider Handbook Benefit Policies Rev. 05/08
8. Klomp HM, Steyerberg EW, van Urk H, et al. ESES Study Group. Spinal cord stimulation is not cost-effective for non-surgical management of critical limb ischaemia. Eur J Vasc Endovasc Surg. 2006; 31(5):500-8.
9. The British Pain Society. Spinal cord stimulation for the management of chronic pain:
Recommendations for best clinical practice. http://www.britishpainsociety.org/SCS_2005.pdf.
10. BCBSA Medical Policy Reference Manual. Spinal Cord Stimulation. 7.01.25. Issue 5:2006.
11. Centers for Medicare & Medicaid Services. NCD for Electrical Nerve Stimulators (160.7).
Effective 8/7/1995.

S Sunitinib (Sutent)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Sunitinib (Sutent) is FDA approved for the treatment of gastrointestinal stromal tumor (GIST) after disease progression on or intolerance to imatinib mesylate (Gleevec) and for the treatment of and advanced renal cell carcinoma (RCC). Sunitinib is a multi-kinase inhibitor that targets several receptor tyrosine kinases to deprive the tumor cells of the blood supply and nutrients needed to grow. It is an orally administered medication.
II. Criteria/Guidelines
A. Sunitinib will be covered (subject to the Limitations/Exclusions and Administrative Guidelines) for an initial three months when recommended by an oncologist for one of the following indications:
1. Treatment of GIST after disease progression on or intolerance to imatinib (Gleevec).
2. Treatment of advanced RCC.
B. Continuation of therapy will be covered if the patient shows no progression of disease.
III. Limitations/Exclusions
A. These criteria will continue to apply when sunitinib becomes available in a generic form. IV. Administrative Guidelines
A. Pre-certification is required for the initial three months of therapy.
B. To pre-certify, please complete HMSA’s Drug Review Request and mail or fax the form as indicated. The following documentation from the medical record must be submitted:
1. Clinical notes that include the history of previous treatments;
2. Current oncology notes;
3. Pathology reports;
4. Imaging studies.
C. Pre-certification is required for continuation of sunitinab for each additional three months. The
following documentation from the medical record must be submitted:
1. Current oncology notes documenting the patient's response to treatment and that indicate no progression of disease; and
2. Current imaging studies that show no progression of disease when compared with
previous imaging studies

QUEST Provider Handbook Benefit Policies Rev. 05/08
V. Important Reminder The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
VI. Scientific Background
Gastrointestinal Stromal Tumor In a randomized controlled trial (n=312), for patients who failed on imatinib treatment (n=207), sunitinib showed significant improvement in: delaying the time-to-tumor progression (27.3 weeks) vs. placebo plus best supportive care (6.4 weeks, p<0.0001), increasing progression-free survival (24.1 weeks) vs. placebo (6.0 weeks, p<0.0001) and objective response rate (6.8%) vs. placebo-treated patients (0%, p<0.006). Because the study was terminated early, and because treatment crossover was allowed after the endpoint was reached, median survival could not be calculated.
Advanced Renal Cell Carcinoma The National Comprehensive Cancer Network (NCCN) has issued guidelines for the treatment of kidney cancer (v.2.2007) that specify sunitinib as a potential first or second-line therapy for patients with stage IV or relapsing stage I-III kidney cancer.
In a randomized controlled trial used to qualify for FDA approval, sunitinib was compared to interferon alfa in 750 patients with previously untreated, metastatic renal cell carcinoma. The median duration of treatment for sunitinib (n=375) was six months and four months for the interferon alfa group (n=375). The median progression-free survival was 11 months in patients receiving sunitinib and five months for patients receiving interferon alfa. Median overall survival had not been reached.
VII. References
1. FDA Center for drug evaluation and research. Label information for Sutent. Accessed October 10, 2007. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.
2. Fiedler W, et al. “A phase 1 study of SU11248 in the treatment of patients with refractory or
resistant acute myeloid leukemia (AML) or not amenable to conventional therapy for the disease.” Blood. 2005; 105:986-93.

S Sunitinib (Sutent) (continued)
QUEST Provider Handbook Benefit Policies Rev. 05/08
3. Motzer RJ, Dror Michaelson M, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006; 24(1):16-24.
4. Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in Patients with Metastatic Renal Cell
Carcinoma. JAMA. 2006; 295:2516-2524.
5. National Comprehensive Cancer Network, Clinical Practice Guidelines in Oncology. Kidney Cancer. V.2.2007. Available at: http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. Accessed 10/15/07.
6. Sutent prescribing information, Pfizer Labs, New York, NY. 2/2007.
7. The Regence Group. Medication Policy Manual. Sutent, sunitinib. Policy No. dru128. Revised
March 15, 2007.
8. Demetri GD, van Oosterom AT, Garrett CR, Blackstein ME, Shah MH, Verweij J, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomized controlled trial. Lancet. 2006 Oct. 14; 368(9544):1329-38.
9. Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukokowski RM, Rixie O, et al.
Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007 Jan 11; 356(2):115-24.


T Transcutaneous Electrical Nerve Stimulation (TENS)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Transcutaneous electrical nerve stimulation (TENS) is an electronic device that is used to relieve chronic, intractable pain, post-surgical pain, and pain associated with active or post-trauma injury unresponsive to other standard pain therapies. It consists of an electrical pulse generator connected by wire to two or more electrodes, which are applied to the surface of the patient’s skin at the site of the pain.
II. Criteria/Guidelines
A. A transcutaneous electrical nerve stimulator (TENS) will be covered (subject to Limitations/ Exclusions and Administrative Guidelines) when ordered by a physician and used on a trial basis for the following conditions:
1. Acute pain resulting from surgery and used as an adjunct or as an alternative to drugs, or
2. Chronic, intractable pain, when the following criteria are met:
a. The pain must have been present for at least three months, and
b. Standard treatment modalities have been tried and failed and/or are
contraindicated.
B. A TENS will be covered (subject to Limitations/Exclusions and Administrative Guidelines) for purchase after the trial period when all of the following are met:
1. The physician had determined that the patient is likely to derive significant therapeutic
benefit from continuous use of the unit over a long period of time.
2. The physician has documented in the patient’s medical record that a reevaluation of the patient was performed at the end of the trial period. The reevaluation must indicate how often the patient used the TENS unit, the typical duration of use each time and that the patient has responded to use with a decrease in pain medication and in restoration of function.
C. A conductive garment will be covered when any one of the following indications are met:
1. There are multiple sites or the area is too large to be stimulated and the stimulation
would have to be delivered so frequently that it is not feasible to use conventional electrodes, adhesive tapes and lead wires.
2. The areas or sites to be stimulated are inaccessible with the use of conventional
electrodes, adhesive tapes and lead wires.
3. The patient requires electrical stimulation beneath a cast to treat chronic intractable pain.
4. The patient has a documented medical condition, such as skin problems, that preclude the application of conventional electrodes, adhesive tapes and lead wires.

QUEST Provider Handbook Benefit Policies Rev. 05/08
III. Limitations/Exclusions A. TENS for acute post-operative pain is subject to the following limitations:
1. Treatment is generally limited to 30 days from the date of surgery. Coverage for TENS
longer than 30 days will be determined by individual consideration based upon documentation supporting medical necessity provided by the ordering physician.
2. Payment will be made only as a rental of the TENS.
B. The use of TENS for the treatment of chronic, intractable pain is subject to the following
limitations:
1. A TENS unit will be allowed on a trial basis for a minimum of 30 days but not to exceed two months. The trial period will be paid as a rental which may count toward the eventual purchase cost.
C. TENS will not be covered for conditions not accepted as responding to TENS therapy
including, but not limited to, the treatment of headache, visceral abdominal pain, pelvic pain and temporomandibular joint pain.
D. TENS is contraindicated for use in pregnant women and patients with pacemakers.
E. Pulsed electrical stimulation device, including transcutaneous electrical joint stimulation
device, HCPCS code E0762 (e.g., Bionicare) is not covered. This device is not known to be effective in improving health outcomes.
IV. Administrative Guidelines
A. Pre-certification is required. To pre-certify, please complete HMSA’s Pre-certification Request and mail or fax the form as indicated.
B. Pre-certification requests must include all of the following documentation from the medical
record:
1. Location, duration and etiology of the pain.
2. Other treatment modalities that were used, including the names and dosages of medication, the length of time that each type of treatment was used, and the results.
C. The order for TENS unit and a completed Certificate of Medical Necessity (CMN) (A CMN is
needed for purchase) must be signed and dated by the ordering physician and must be kept on file by the supplier.
D. During the rental of a TENS unit, supplies are included in the rental allowance. If a TENS unit
is purchased, the allowance includes lead wires and one month’s supply of electrodes, conductive paste or gel (if needed) and batteries. Separate allowance will be made for replacement supplies when they are medically appropriate.

T Transcutaneous Electrical Nerve Stimulation (TENS) (continued)
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
CPT Code Description 64550 Application of surface (transcutaneous) neurostimulator
HCPCS Code Description E0720 TENS, two lead, localized stimulation E0730 Transcutaneous electrical nerve stimulation device (TENS), four or more
leads, for multiple nerve stimulation E0731 Form-fitting conductive garment for delivery of TENS or NMES (with
conductive fibers separated from the patient’s skin by layers of fabric) A4557 Lead wires, (e.g., apnea monitor), per pair A4595 Electrical stimulator supplies, 2 lead, per month (e.g., TENS, NMES)*
*Codes A4556 (Electrodes, [e.g., apnea monitor], per pair), A4558 (Conductive paste or gel), and A4630 (Replacement batteries, for medically appropriate TENS owned by patient) are not valid for claim submission. A4595 should be used instead.
V. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes § 432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
VI. References
1. Blue Cross Blue Shield Association. Transcutaneous Electrical Nerve Stimulator (TENS). Medical Policy Reference Manual. Policy 1.01.09. Updated 2/15/07.
2. Carroll D, Moore RA, McQuay HJ, et al. Transcutaneous electrical nerve stimulation (TENS)
for chronic pain (Cochrane Review). The Cochrane Library, Issue 3, 2002.
3. LCD for Transcutaneous Electrical Nerve Stimulators (TENS) (L11495) Electronic Data Systems Corp (DME PSC) and Noridian Administrative Services (DME MAC). Revision effective 1/1/07.
4. CMS Manual System, Pub. 100-03, Medicare Coverage Determinations Manual, Chapter 1,
Section 10.2, 160.7.1, 160.13, 280.13.

QUEST Provider Handbook Benefit Policies Rev. 05/08
5. Yurtkuran M, Kocagil T. TENS, electroacupuncture and ice massage: Comparison of treatment for osteoarthritis of the knee. Am J Acupunct 1999; 27(3-4):133-140.

V Vacuum Assisted Breast Biopsy
CPT only © 2007, American Medical Association. All rights reserved. (Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
I. Description Vacuum assisted core biopsy is a technique in which a cannula equipped with a suction device is inserted into the breast through a small skin incision. Multiple cores can be taken using one incision. The Mammotome and ABBI are different types of vacuum assisted breast biopsy (VABB) systems. A metallic clip may be placed at the site of the biopsy to facilitate its identification if further surgical excision or radiologic follow-up is necessary. Initially used for biopsying clusters of micro-calcifications, the use of VABB has expanded to include biopsy of a wider range of palpable and non-palpable breast lesions.
A variety of imaging techniques may accompany the biopsy. Stereotactic guidance is particularly useful for guiding the biopsy of micro-calcifications. Ultrasound guidance may be preferable for masses that have been previously detected by ultrasound. Advantages of ultrasound guidance include the absence of radiation. Computed tomography (CT) and magnetic resonance imaging (MRI) are also used for guidance.
When the results of fine needle aspiration or conventional needle core biopsy are suspicious or positive for malignancy, an open excisional biopsy or lumpectomy is typically performed to confirm the findings and ensure that the entire lesion has been removed.
II. Criteria/Guidelines
A. Vacuum assisted breast biopsy is the preferred method of sampling suspicious micro-calcifications and is medically necessary for this indication.
B. Patients with other types of non-palpable breast lesions may be eligible for coverage of
vacuum assisted breast biopsy as an alternative to standard core biopsy or fine needle aspiration. Documentation for the medical necessity of VABB (compared to standard core biopsy or fine needle aspiration) must be included in the medical record and available if requested.
III. Limitations/Exclusions
A. Vacuum assisted breast biopsy is not eligible for coverage for patients with palpable breast lesions.
B. Vacuum assisted breast biopsy is not eligible for coverage for patients as an alternative to open
excisional biopsy or lumpectomy.
C. Combinations of fine needle biopsy or conventional core biopsy and vacuum assisted breast biopsy will not be eligible for coverage.
IV. Administrative Guidelines
CPT Code Description 19103 Biopsy of breast, percutaneous, automated, vacuum assisted or rotating
biopsy device, using imaging guidance 19295 Image guided placement, metallic localization clip, percutaneous, during
breast biopsy (list separately in addition to code for primary procedure) 76098 Radiological exam, surgical specimen

CPT only © 2007, American Medical Association. All rights reserved. QUEST Provider Handbook Benefit Policies Rev. 05/08
CPT Codes Description 76942 Ultrasonic guidance for needle placement (e.g., biopsy, aspiration,
injection, localization device), imaging supervision and interpretation 77031 Stereotactic localization guidance for breast biopsy or needle placement
(e.g., for wire localization or for injection), each lesion, radiological supervision and interpretation
77032 Mammographic guidance for needle placement, breast (e.g., for wire localization or for injection), each lesion, radiological supervision and interpretation
99070 Surgical supplies
ICD-9-CM Code Description 174.0 – 174.9 Malignant neoplasm, female breast 175.0 – 175.9 Malignant neoplasm, male breast 217 Benign neoplasm, breast 233.0 Carcinoma in situ, breast 238.3 Neoplasm of uncertain behavior, breast 239.3 Neoplasms of unspecified nature, breast 611.72 Lump or mass in breast 793.81 Nonspecific abnormal findings on radiological and other examination,
breast, mammographic microcalcification
ICD-9-CM Procedure Code
Description
85.11 Closed (percutaneous) (needle) biopsy of breast 87.37 Soft tissue x-ray of thorax, other mammography
V. Scientific Background
Vacuum assisted breast biopsy (VABB) has found acceptance by physicians. The Mammotome device has particularly found favor because of its efficacy in sampling micro-calcifications. VABB samples are larger and this is thought to reduce false negative results.
Studies comparing fine needle aspiration, conventional core biopsy, and vacuum assisted core biopsy have not been done. Meyer et al., (1997) investigated vacuum assisted and traditional core biopsy and results suggested that vacuum assisted breast biopsy is more effective in sampling micro-calcifications. Nesbit and colleagues (2000) also found VABB was associated with improved sampling of micro-calcifications.
Diagnostic accuracy was examined by Jackman and associates (1997). They concluded that the increased amount of tissue obtained and examined using VABB, increased diagnostic accuracy when compared to conventional core biopsy. Underestimates of carcinoma were significant with both of these non surgical biopsy procedures, therefore, surgical biopsy must still be performed when non surgical biopsies had suspicious findings.
Simon et al., (2000) looked at the safety of VABB based on bleeding time and found bleeding time was less than 10 minutes. Burbank (1997) found about a one percent complication rate when 340 vacuum assisted breast biopsies were investigated. Liberman and colleagues (1997), and Lamm

V Vacuum Assisted Breast Biopsy (continued)
(Continued on Next Page) QUEST Provider Handbook Benefit Policies Rev. 05/08
and Jackman (2000) looked at the future use of mammograms in patients having had VABB. There was minimal scarring as a result of VABB and they concluded that mammographic findings were not compromised.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA reconsider the application of the Medical Policy to the case at issue.
VII. References
1. Adrales G, Turk P, Wallace T, et al. Is surgical excision necessary for atypical ductal hyperplasia of the breast diagnosed by Mammotome? Am J Surg 2000: 180(4):313-5.
2. BlueCross Blue Shield Association Medical Policy Reference manual Policy 6.01.09 Vacuum
assisted breast biopsy. (1:2003).
3. Burbank F. Stereotactic breast biopsy: comparison of 14- and 11-gauge Mammotome probe performance and complication rates. Am Surg 1997; 63(11):988-95.
4. Darling ML, Smith DN, Lester SC, et al. Atypical ductal hyperplasia and ductal carcinoma in
situ as revealed by large-core needle breast biopsy: results of surgical excision. AJR Am J Roentgenol 2000; 175(5):1341-6.
5. Jackman RJ, Burbank F, Parker SH, et al. Atypical ductal hyperplasia diagnosed at stereotactic
breast biopsy; improved reliability with 14-guage, directional, vacuum-assisted biopsy. Radiology 1977; 204(2): 485-8.
6. Kettritz U, Rotter K, Schreer I, Murauer M, Schulz-Wendtland R, Peter D. Heywang-
Krobrunner SH. Stereotactic vacuum assisted breast biopsy in 2874 patients: A multicenter study. Cancer 2004 Jan 15; (2)245-51.
7. Lamm RL, Jackman RJ. Mammographic abnormalities caused by percutaneous stereotactic
biopsy of histologically benign lesions evident on follow-up mammograms. AJR Am J Roentgenol 2000; 174(3):753-6.

QUEST Provider Handbook Benefit Policies Rev. 05/08
8. Lehman DC, Deperi ER, Peacock S, McDonough MD, Demartini WB, Shook J. Clinical experience with MRI-guided vacuum assisted breast biopsy. Am J Roentgenol 2005 June; 184(6):1787-7.
9. Liberman L, Hann LE, Dershaw DD, et al. Mammographic findings after stereotactic 14-guage
vacuum biopsy. Radiology 1997; 203(2): 343-7.
10. Meyer JE, Smith DN, DiPiro PJ, et al. Stereotactic breast biopsy of clustered microcalcifications with a directional, vacuum-assisted device. Radiology 1997; 204(2):575-6.
11. Nisbet AP, Borthwick-Clark A, Scott N. 11-guage vacuum-assisted directional biopsy of breast
calcifications, using upright stereotactic guidance. Eur J Radiol 2000; 36(3):144-6.
12. Simon JR, Kalbhen CL, Cooper RA, et al. Accuracy and complication rates of US-guided vacuum-assisted core breast biopsy; initial results Radiology 2000; 215(3):694-7.