queri 2008 meeting 081210 - health services research needed social engineering ... business...
TRANSCRIPT

1
Connecting Researchwith Patient Care
Implementing Research:Lessons Learned from Improving ClinicalPerformance Measures
Peter Woodbridge, MD, MBA 1, 2,Heather Woodward-Hagg 3, Linda
Williams MD 4,Dawn Bravata 4,TeresaDamush 4, Laurie Plue 4, Penny Butler 5
1 Nebraska Western Iowa VA HCS, 2 University ofNebraska College of Public Health, 3 VA HSRD Centeron Implementing Evidence Based Practice, 4 StrokeQUERI, 5 Roudebush VAMC
Introduction
Objective Enrich the dialogue on implementation science
by providing a different perspective
Expose QUERI implementers to an empiricmodel for effecting improvement
Perspective The Goal: Operationalize Research
Implementation science provides guidance But must be adapted for context
Brutally pragmatic about the literature Impact, not understanding, is the measure of value
2
Connecting Researchwith Patient Care
I have built it.Why did they not come?
A Story
You are an ACOS for Ambulatory Care
You have 210 employees (MD, RN, HT)
You are responsible for ensuring that 43,000 uniqueveterans have timely access to 50 monitored clinics Those veterans make 270,000 clinic visits in a year
You are responsible for ensuring that “the clinicsmeet all nationally monitored performancemeasures.” There are Approximately121 clinical performance measures
Approximately 30 access measures
that are tracked for 50 clinics
A young investigator comes to youwith his new stroke screening protocolthat his research shows will benefitpatients
What do you do?
a) Express your regrets saying thatyou would like to help but you donot have capacity due to competingpriorities
b) Say you will put it in the projectqueue and do nothing as the crisisde jeur consumes your time
c) Get right on it and have itimplemented in 30 days
An Alternate Ending:
The young investigator volunteers tofacilitate implementation
What do you think is the likelihood ofadoption?

3
Dougherty, D. and Conway, P.H. (2008, May). "The '3T's' road mapto transform US health care." Journal of the American MedicalAssociation 299(19), pp. 2319-2321
“Health services researchmust evolve from
generating clinical efficacyknowledge to creatingclinical effectiveness
knowledge”
~ Carolyn Clancy, Director, AHRQ atVA HSRD meeting. 2/2008
Our Hypothesis
To shorten the implementationinterval, clinical investigators must“own” their findings and get into themud of quality improvement
Lean Concept:
“Gemba” – where the truth canbe found;” the place wherevalue is added; the shop floor

4
Action Research and LeanHealthcare Change Facilitation
Action Research* Directed at
improving safety,quality, access, etc.(“value”)
Plan, Act, Observe,Reflect (PAOR)
Involvement Vs. “extractive”
Goal: achievechange and“understanding”
Change Facilitation Directed at
improving safety,quality, access, etc.(“value”)
Plan, Do, Study,Act (PDSA)
Gemba Vs. “managing”
Goal: achievechange and“improvement”
* Dick, B. (2002) Action research: action and research [On Lline]. Availableat http://www.scu.edu.au/schools/gcm/ar/arp/aandr.html, accessed 12/7/2008
The Right Stuff:Investigators as Change Facilitators
Existing attributes Passion for topic
(ownership)
Data driven(empiric)
Analytical(deductive)
Hypothesisgeneration(experimentalist)
Project manager
Skills needed Social Engineering Change facilitation
Organizational &group dynamics
Processimprovementmethods (LeanHealthcare)

5
Lean Healthcare
A framework for organizationalimprovement derived from:
Lean (and six sigma)
Complexity science
Business management theory andpractice
Organizational development theory andpractice
Lean Healthcare
Grounded in four useful mental models:
Reppening QI Model
The Value Improvement “Stool”
Rapid Cycle Change PDSA
Stacey Complexity Diagram
With emphasis on practical tools andmethods
Tailored to the “complexity” of the specificinitiative

6
11
Reppenning QI Model
ProcessReliability
Errosion inReliability
Investment inReliability
ActualPerformance
PerformanceGap
DesiredPerformance
Time Spent onImprovement
+
+
-
+
Time SpentWorking
+
Pressure todo work
+
+
Work Harder
Pressure toImprove
Capability+
+
Work Smarter
* Repenning, N. and J. Sterman (2001)., California Management Review, 43, 4: 64-88
DELAY
Value = (Safety + Quality + Access + Service) / Cost
LeanHealthcare
ImprovementModel
Key enabling elements:• Microsystems• √ N• Structure

7
Rapid Cycle Change (RCC) PDSA
Make many small scale, hypothesisdriven, testable changes using PDSA
Those that seem to work, test inincreasingly larger settings
Plan an improvement
Do – Test the improvement
Study the effects byanalyzing data
Act upon this information(adopt, adapt, abandon) Adapted from Kim Voss
14
The Stacey Matrix:Reliability, Variability & Complexity
Anarchy(RandomChaos)
Far fromAgreement
Close toAgreement
Close toCertainty
Far fromCertainty
Com
plexity
(Dynam
icSystem
s;
Deterministic
Chaos)
Rational(Linear)Systems
The Impactof
Variabilityon SystemComplexity V
aria
bility
Rel
iabi
lity
Adapted from Ralph Stacey“Complexity and Creativity in
Organizations”
Technical
So
cia
l

8
Effectiveness of Lean HealthcareImprovement
Aggregate Quality Ranking
103
2
34
27
2922
16
113
114
122
112
84
6456
0
20
40
60
80
100
120
140
07 Q2 07 Q3 07 Q4 08 Q1 08 Q2 08 Q3 08 Q4
Nati
on
al
Ran
kin
g
VAMC #1Implementation
VAMC #2Implementation
VA Quality Aggregate is theoverall average of the individualrankings of 67 evidence-based,clinically significant, preventiveand chronic disease performancemeasures (includes HEDIS andORYX)
Implementation Outside VA(2005-2007)*
* Woodward-Hagg, H., Doebbeling, B , Workman-Germann, J., Flanagan, M., Scachitti, S., Suskovich, D., Corum, C.,(2008) Implementation of Systems Redesign: Approaches to Spread and Sustain Adoption,AHRQ Advances in Patient Safety: New Directions and Alternative Approaches

9
Connecting Researchwith Patient Care
Challenges to Implementing EBP (andResearch)
“To avoid getting stuck inmud, you need to
understand its properties”
~ NOAA file photo
Challenges: “Complexity”
ClinicalGuidelines
Specia
ltyDis
char
ge
Primary CareNew Patient
CommunicatePurpose ofAppointment
Transportaion
Access
Primary Care
Specialty Care
Access Management
Roudebush VA Medical Center1/27/2006
Recall List
Clinic VisitCheckout
Centraliz
ed
Check-in
AppointmentNotification
Research happens incontrolled
environments
Clinical care happensin complex
environments

10
Challenges: Process vs.Professionalism
Systems Engineering Adaptive Systems
Simple
“Follow aRecipe”
PatientCheck-in
LinearDefined
Few Steps
Standardized
Complicated
“Flying anAirplane”
Scheduling aConsult
Non-linearDefinable
Many Steps
RigidAdherence to
Protocols
Complex
“Raising aChild”
Patient Care
Uniqueness
ExperienceHelps
Chaotic
“Emergency”
Emergency
Unpredictable
SpeedImprovisation
Industry vs. Craft Paradox
Adapted from Brenda Zimmerman, 2002
Challenges: Diversity ofOrganizational Perspectives
Macro Senior leadership
Vision and Strategic Direction
Meso Midlevel managers and supervisors
Policies and Procedures
Micro Frontline staff
Processes
- Nelson, et al Quality by Design

11
21
Case Study: HypertensionPolicy v. Process
Performance Measure:
Hypertension) BP =<140/90
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct
-05
Nov
-05
Dec
-05
Jan-
06
Feb
-06
Mar
-06
Apr
-05
May
-06
Jun-
06
Jul-0
6
Aug
-06
Oct
-06
Nov
-06
Dec
-06
Jan-
07
Feb
-07
Mar
-07
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Monthly RateFYTD 06 Running CumFY'07 Target (75%)FYTD 07 Running Cum
Action:
-Clinical pharmacists w ill be utilized for medication management follow ing established protocols
-Essential to get data base w hich w ould prov ide the prov iders w ith monthly data of patients w ith elevated BP; w hat % are controlled:
w hat % are on diuretic; Dr. Walsh to ask new data group if this is av ailable data
-Determine if clinical reminder has protocol use of diuretic Dr. Pratt/Dr. Suelzer to meet w ith all primary care prov iders in May
-A Rapid Process Improv ement w ill be done May 21st for rapid cycle changes
2006 Performance “Policy” RP
IW
Interventions:
Provider & clinic specific data
PharmD manage new HTN
Return to RN Q 3 weeks
Intervention:
Monthly review of data
“Work harder”
Interventions:
Standardized work
Checkout reminder
22
Case Study: MedicationManagement
After a hiatus of one year, a medical centerresumes weekly tracers
Review of the tracer data reveals asignificant problem with medicationmanagement (unsecured medications,missing meds, outdated medications, etc.)
The medical center uses de-centralizedmedication servers in patient’s rooms
What should leadership do?
A) Instruct the pharmacy to lock upall medications in Pyxis machines
B) Educate the nursing staff as tomedical center policy andprocedures regarding medicationmanagement
C) Charter a LSS PI team to addressprocess issues (work smarter)
D) Charge a containment team to finda quick (work harder) fix
Containment Team Outcome:
10 fold decrease in medicationmanagement errors in 2 weeks
Containment Team Discoveries:
Unreliable processes and systems work arounds
Charter an RPIW to look atmedication management on oneward (microsystem)
Other wards to adapt / adopt

12
The Incubators of Improvement:Clinical Microsystems
Microsystems are the building blocks of hospitals
It is where: Care is made
Quality, safety, reliability, efficiency and innovation is made
Staff morale and patient satisfaction is made
Hospital quality = sum of the quality of its microsystems
Therefore, the job of every person in each microsystemto: Care for their patients
And, to improve care
“A small group of people that work together toprovide care to discrete subgroup of patients”
- Nelson, et al Quality by Design
The Key to Improvement
Create an organizational culture of“experimentalists” that strive continuously, intheir microsystems, to reduce processambiguity and workarounds so as to improvesafety, effectiveness, patient-centeredness,timeliness, efficiency and equity
“What sets companies like Toyota apart is nottheir portfolio of existing solutions but their abilityto generate new ones repeatedly”
– S. Spears
The Common Ground forResearch and Patient Care

13
Connecting Researchwith Patient Care
Overcoming the Challenges
Goa
l-drive
n
Pro
cess
es
Care
Managem
ent
Guidelines
Nurses
Adm
inis
trat
ors
Discover Common Purpose
Patient Safety
Quality*
Evidence
*But what doesquality mean?

14
Discover Common Purpose
Reduce hassles and waste
What is waste?
How can we tackle it?
“Physicians need time to listen, examine, think,explain, interpret, and comfort (value adding).Activities that take time away are waste. Healthcareorganizations need to improve flow and identify andeliminate time stealers.” ~ p. 5
Reinertsen JL, Gosfield AG, Rupp W, Whittington JW. IHI InnovationSeries white paper. Cambridge, MA: Institute for HealthcareImprovement; 2007
Lean Basics
A generic process managementphilosophy directed at smoothing flowand eliminating waste
Although rooted in manufacturing(Toyota), extensively adapted to serviceindustries including healthcare

15
Lean Concepts
Value
Value is determined by the “customer” (patients;ordering provider; the person we serve)
Waste
Anything that does not add value from thecustomer’s perspective
Value stream
The actions (and waste) taken to create value
What is Waste?
Mura – unevenness indemand
Muri – overburdeningpeople or equipment
Muda – process stepsthat do not add value
NonNon--value adding, resourcevalue adding, resourceconsuming activitiesconsuming activities

16
Overburdening and Errors
Nurse overloading leads to 24% of allsentinel events
For each patient over optimumpatient-to nurse staffing ratio, the 30day mortality rate increases by 7%
Aiken L.H., et al.: Hospital nurse staffing and patientmortality, nurse burnout, and job dissatisfaction. JAMA288:1987–1993, Oct. 23, 2002.
Eugene Litvak, PhD, IHI MHO Course
Artificial Overburdening
NWI FY 06
Number of Discharges and Admissions by Time of Day
-
100
200
300
400
500
600
700
00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Time of Day
When does thepharmacy delivermedications?
Admissions
Discharges
Changing to 7 PM not onlysmoothes work but eliminatesrework for pharmacy
Under current state, pharmacypulling meds before residentsfinish rounds

17
Bar Code Medication AdministrationBypassing: A Case Study
The Evidence: IOM – Medication errors 7,000 deaths annually
FDA – Barcodes 500,000 in adverse medicationevents over 20 years
VA – 3.7% of IP medication administrations are “FiveRights” violations (VA data)
Only 1.2-7.7% of adverse events and medication errorsare reported (Vicente, 2003)
BCMA reduces medication errors by: 86% ( Johnson, et al, 2002)
71% (Puckett, 1995)
BCMA introduced in VA to reduce medication errorsin 1999
Current State Analysis: Bypassing is endemic
• At one VA:
• 94 incidents since 10/2002
• 10/13 aggregate RCA related to BCMA
• VA Study*:
• BCMA bypassed 47% of time on acute patient wards
• BCMA bypassed 92% of time on long-term care wards
* Rogers, Patterson, Render, Woods, Cook, Ebright, VAGetting at Patient Safety (GAPS) Center
Prior Interventions at one VA:
• Wristband printers replaced
• Increased number of laptops
• CAC-BCMA Coordinator created and filled
• Missed Medication and PRN Reports (autoprint)
• LR/NS Bolus stocked on floors
• No more D5W on floors
• Removed barcodes from patient labels
• I-Carts
Problem Persists; Lean Healthcare RPIWChartered
BCMA Bypass Analysis
Nurses spend about 10% of their timein direct patient contact.
For the most part, the remainder isspent on what I call “hunting andgathering” (Heinrich, 2005)

18
35
14 minutes in the life of a Pharmacy Tech
Med/Isolation Carts – CurrentState

19
BCMA Cart – Post 5S Mock-up
Place forWater Jug
Place for IVBags
LaminatedInstructions
CommonSupplies
BCMA Cart – Post 5S
IV Drawer

20
RPIW Baseline / Outcomes Data
318Total time to pass meds to onepatient
310Totals log-ins per patient medpass
1.03.3Number of attempts before medpass complete for one patient
33181Distance traveled to pass meds toone patient
Post-RPIW
Baseline
Time saved for other patient care activities = 15 min x 100ADC x 3 shifts x 365 = 27,375 hours per year (~16 FTE)
Connecting Researchwith Patient Care
Lean Healthcare:Leadership, Ownership & Structure

21
Value = (Safety + Quality + Access + Service) / Cost
LeanHealthcare
ImprovementModel
Key enabling elements:• Microsystems• √ N• Structure
42
Why Leadership?
“To introduce any new article offood among seamen, let it beever so much for their good,requires both the example andthe authority of theCommander”
-James Cook, 1780
Berwick, JAMA (2003) 289:1969

22
43
Why Leadership?
JCAHO 2006 Root Cause Analysis of Sentinel Events
11%
13%
18%
18%
31%
32%
33%
34%
42%
49%
51%
65%
0% 20% 40% 60% 80% 100%
Continuum of care
Staffing
Care planning
Organizational culture
Availability of information
Orientation / training
Competency
Envrionment
Procedural compliance
Leadership
Patient assessment
Communication
In almost 1/2 of sentinelevents, a breakdown inleadership contributed tothe failure
Leadership and Ownership:The NWI Way Leadership Initiative
We are all leaders North Platte Canteen*
We are all owners Take ownership for what
you do
We all create value The lens by which all our
activities are examined
NWI Way
* Greene, B “Once Upon a Town” Perennial, 2003

23
45
Lean Healthcare Ownership Roles
Sponsor Senior leader
Macro-perspective
Management GuidanceTeam (MGT) Mid-level managers
Meso-perspective
“Policy”
Owner “Eye on the ball”
Micro-perspective
Improvement Team Understand process
“In the mud”
LH Change Facilitator “In the boat” with the
team
Help teams see theproblem
Provides just-in-timetraining and assistance
Measurement Specialist Team member
Administrative Support Team member
Consultants & Stakeholders Perspective
PerformanceMeasure Datanot meeting
target
CharterManagement
Team
Obtain ProcessLevel Data
DefineProject Scope
CharterPAT
Weekly meetingsto develop/test/implement
5 RCCs/month
Scope/Complexityof process?
CharterRPIW
Process/System
Redesign
PeriodicFeedbackTo EMT/
PerformanceMeasure
Board
PeriodicFeedbackTo EMT/
PerformanceMeasure
Board
PerformanceMeasureReviewBoard
Lean Improvement Cycle

24
47
Using Lean Healthcare to AddressComplexity
Anarchy(RandomChaos)
Far fromAgreement
Close toAgreement
Close toCertainty
Far fromCertainty
Complexity
(Dynam
icSystem
s;
Determ
inisticChaos)
Rational(Linear)Systems
Adapted from Ralph Stacey“Complexity and Creativity in
Organizations”
Anarchy(RandomChaos)
Far fromAgreement
Close toAgreement
Close toCertainty
Far fromCertainty
Com
plexity
(Dynamic
Systems;
Deterministic
Chaos)
Rational(Linear)Systems
NegotiatedSystems
EvolvingSystems
(RCC PDSA)
So
cia
l
48
Matching Intensity of Effort toInitiative Complexity
5 RCC PDSA Within a clinical
microsystem
Microsystem is capable
Fast Start Project Defined charter
Little analysis required
Motivated team
Rapid ProcessImprovementWorkshop (RPIW) Defined charter
Many RCC PDSA
A lot of progress likelyin one week
100 Day Project Analysis required
Ambiguous charter
Follows DMAIC

25
49
5 RCC PDSA
5 RCC PDSA per month Responsibility of Owner,
MGT, and Sponsor
Indentify 5 improvementideas to test each month
Use small tests of change
Test each idea forquantifiable impact
No charter “Improvement” is charter
Success depends on Motivated team
Capable team
Use when there is good“agreement” but weakevidence as to best practice
50
Fast Start Project
One day “mini-blitz”followed by weeklymeetings First day:
Process map
Isolate problems
Identify RCC PDSA
Up to 6 weeks Analyze results RCC
PDSA
Additional RCC PDSA
Has charter
Progress tracked atmonthly milestonemeetings
Best used for “simple”problems that may requirea structured environmentfor “negotiation”

26
51
Rapid Process ImprovementWorkshop (RPIW)
Weeklong (40 hour)event + 90 day weeklyfollow-up Combine education and
improvement
Highly structured
Day 1-2 analysis VOC & PD
Process map
Isolate problems
Day 3-5 RCC PDSA 20-30 small tests of
change in one week
Best used for“complicated” but welldefined problems
52
100 Day Project
Advanced Lean Based on DEDISS cycle
Define Evaluate Design Implement Spread Sustain
3 hour meetings weeklyfor 8 weeks followed by1 hour meetings for 6weeks
Just in time training ofteam
Formal “go / no-go”milestones
Often requires valuestream mapping
Use for “complex”problems May spin off other
project teams

27
53
Systems Engineering
Systems EngineeringProject Uses engineering tools
to analyze problemsand simulate solutions
Formal project planwith defined milestones
Formal “go / no-go”milestones
Solutions often rest onimproving humanperformance (humanfactors and cognitiveengineering)
Use for “chaotic”problems Separate deterministic
from random chaos
Coaching and Lean HealthcareChange Facilitation
Give a man a fish and he will eat fora day. Teach a man to fish and hewill eat for a lifetime. ~Confucius
But to teach, you must get inthe boat!!

28
Connecting Researchwith Patient Care
Lean Healthcare:Creating Improvement Capability
Value = (Safety + Quality + Access + Service) / Cost
LeanHealthcare
ImprovementModel
Key enabling elements:• Microsystems• √ N• Structure

29
Lean Improvement
Define theProblem
EvaluateCurrent State
IdentifyOperational
Barriers
ImproveSystems
SustainabilityStrategy
Project Charter
Process Map
Check Sheet
Process ObservationWorksheet
Spaghetti Diagram
Waste Worksheet
Lean Tools
Process ControlPlan
Adapted with permission: LSSHC
Lean Improvement
Define theProblem
EvaluateCurrent State
IdentifyOperational
Barriers
ImproveSystems
SustainabilityStrategy
Project Charter
Process Map
Check Sheet
Process ObservationWorksheet
Spaghetti Diagram
Waste Worksheet
Lean Tools
Process ControlPlan
Adapted with permission: LSSHC

30
PatientArrives
At Radiology
Patientescorted tooutpatientradiology
ClerkAssigns
Patient toRegistrar
PatientPre-
registered?
Clerk RequestsID and Medical
Card
Not EnoughEscorts
PatientArrives
at RegistrationDesk
RegistrarEnterspatient
informationinto system
Not EnoughRegistrars
Patient WaitTimes
Yes
No
“Kapowie”
Courtesy LSSHC
Outpatient RegistrationCurrent State Process Map
Process Flow Diagram
Square = steps, one per sticky
Square at angle = branch
Stars = ambiguities, workarounds
Flowers = ideas for solvingAt High Level

31
Voice of the Customers
Select Key Process Customers:
Customers that are important to theproject success
Customers that are not adequatelyrepresented within the teammembership.
By permission: LSSHC
“Customers” are anyoneimpacted by the process
Voice of the CustomerInterviews
What do you like about our services(Strengths)?
What do you think needs improvement(Weaknesses)?
What Opportunities do you feel we couldtake advantage of?
What could potentially Threaten oursuccess?
Let the Customer Talk - Listen Carefully -Record Responses
By permission: LSSHC

32
Identify the “Positive Deviants”
Positive deviants are the successful outliers They are the individuals that get it right when
others fail
Learn from the positive deviants Analyze their success Use their practices to identify process
improvements
Make positive deviant activities visible toothers in the group Healthcare workers are “learners” They learn best from peers
Observe the ProcessGather Process Data

33
Process Observation WorksheetExample
Process Observation Worksheet
Process: Patient check-in
Step # Description Distance
Clock
Time
Task
Time
Wait
Time Observations
0:00
1 Patient arrives 0:10 0:10
2 Clerk requests ID 0:13 0:03
3 Patient registered (Y/N) N
3A Patient sent to HBU 575 0:15 0:02
3B HBU registers patient 0:47 0:32 0:20
4 Appointment (Y/N) 575 N
4A Make walk-in appointment 0:50 0:03
5 Check patient in 0:52 0:02
6 Patient sent to waiting room 100 0:56 0:04
Enter time that stepwas completed.
Distance traveledIn steps
Task time calculatedlater…
Check-sheet Example
Project Name: MRSA
Output Metric: Handwashing
Date / Time Unit Room #
Followed
handwashing
protocol
Reason for Non-
compliance Comment
5/18/2007 5E 124 Yes
5/18/2007 5E 126 No
Non-cleanser in
dispenser
5/18/2007 5S 148 No
Nurse carrying
items; no place to
put down

34
Spaghetti DiagramClinic 5 Room Turnover Project
Exa
mR
oo
m
Exa
mR
oo
m
Exa
mR
oo
m
Exa
mR
oo
m
“6+ Miles per Day”
Lean Improvement
Define theProblem
EvaluateCurrent State
IdentifyOperational
Barriers
ImproveSystems
SustainabilityStrategy
Project Charter
Process Map
Check Sheet
Process ObservationWorksheet
Spaghetti Diagram
Waste Worksheet
Lean Tools
Process ControlPlan
Adapted with permission: LSSHC

35
Lean & RCC PDSA
Many SmallTests of Change
Start Smalland Evolve to
Full Scale
Basic Lean Tools
Apply Lean Tools to reduce oreliminate waste
5S
Visual Controls
Visual Workplace rules
Workstation Design
Setup Reduction

36
5S Workplace Organization
Five “S”
Sort
Simplify (Set inorder)
Standardize
Sweep (Shine)
Sustain (SelfControl)
NOT
Scrounge
Steal
Stash
Scramble
Search
From Virginia Mason

37
From Virginia Mason
Pittsburg VA –Equipment Room
BEFORE
BenefitsBenefits
Clean equipment =pathogen vector
Saves frustration, searching
Freed up $20K-worth ofunused equipment for useelsewhere
IV Pumps(4)
Always Plugged In
AFTER
Whiteboardindicateslocation

38
Connecting Researchwith Patient Care
Lean Healthcare:Sustainability and Spread
Value = (Safety + Quality + Access + Service) / Cost
LH ValueImprovement
Model
Key enabling elements:• Microsystems• √ N• Structure

39
Connecting Researchwith Patient Care
Sustainability
“The first rule of sustainability isto align with natural forces, or at
least not try to defy them.”~Paul Hawken
Lean Improvement
Define theProblem
EvaluateCurrent State
IdentifyOperational
Barriers
ImproveSystems
SustainabilityStrategy
Project Charter
Process Map
Check Sheet
Process ObservationWorksheet
Spaghetti Diagram
Waste Worksheet
Lean Tools
Process ControlPlan
Adapted with permission: LSSHC

40
79
VAP Bundle Implementation
What does this processlook like at week 15?
80
Whathappened?
Sustainability
Woodward-Hagg, H., El-Harit, J., Vanni, C., Scott, P., (2007). Application of Lean Six Sigma Techniques to Reduce Workload Impact DuringImplementation of Patient Care Bundles within Critical Care – A Case Study. Proceedings of the 2007 American Society for Engineering EducationIndiana/Illinois Section Conference, Indianapolis, IN, March 2007.
Whathappened?

41
81
Multiple factorsimpacting sustainability
ProcessReliability
Errosion inReliability
Investment inReliability
ActualPerformance
PerformanceGap
DesiredPerformance
Time Spent onImprovement
+
+
-
+
Time SpentWorking
+
Pressure todo work
+
+
Work Harder
Pressure toImprove
Capability+
+
Work Smarter
ImproveReliability
ImproveClinician Effectiveness
of “Work Smarter” Loop
TimelyIdentification of
PerformanceGaps
ReduceReliabilityErosion
delay
ImproveStaff Engagement
In the Initiative
AlignIncentive Systems
Courtesy: HeatherWoodward-Hagg
Connecting Researchwith Patient Care
Spread

42
Berwick’s rules for Change inHealthcare
Find Sound Innovations
Find and support Innovators
Invest in Early Adopters
Make early adopter activityobservable
Trust and enable reinvention
Create ‘slack’ for change
Berwick, JAMA (2003) 289:1969
Factors that Determine Spread(and Sustainability)
Innovation attributes
Relative advantage
Compatibility
Complexity / Simplicity
Trialability
Observability
Communication
The “Early Adopter” Opinion Leader
Berwick, JAMA (2003) 289:1969

43
Staff Engagement /Communication:
Don’t make changes:
Without soliciting staff feedback
Without soliciting MGT and sponsorfeedback
Be transparent:
Demonstrate mock-ups widely
Share data
The team serves those not in the room!!
Connecting Researchwith Patient Care
Lean Healthcare:Measurement

44
Value = (Safety + Quality + Access + Service) / Cost
LH ValueImprovement
Model
Key enabling elements:• Microsystems• √ N• Structure
Information Triangle
Decisions
Data
Information
Knowledge
Data: symbols, facts, numbers
Data that has been processed giving itmeaning by way of relational connection
Justified, true, andbelieved Information
Purdy & Giaeidi, VEHU 303 (2007)
45
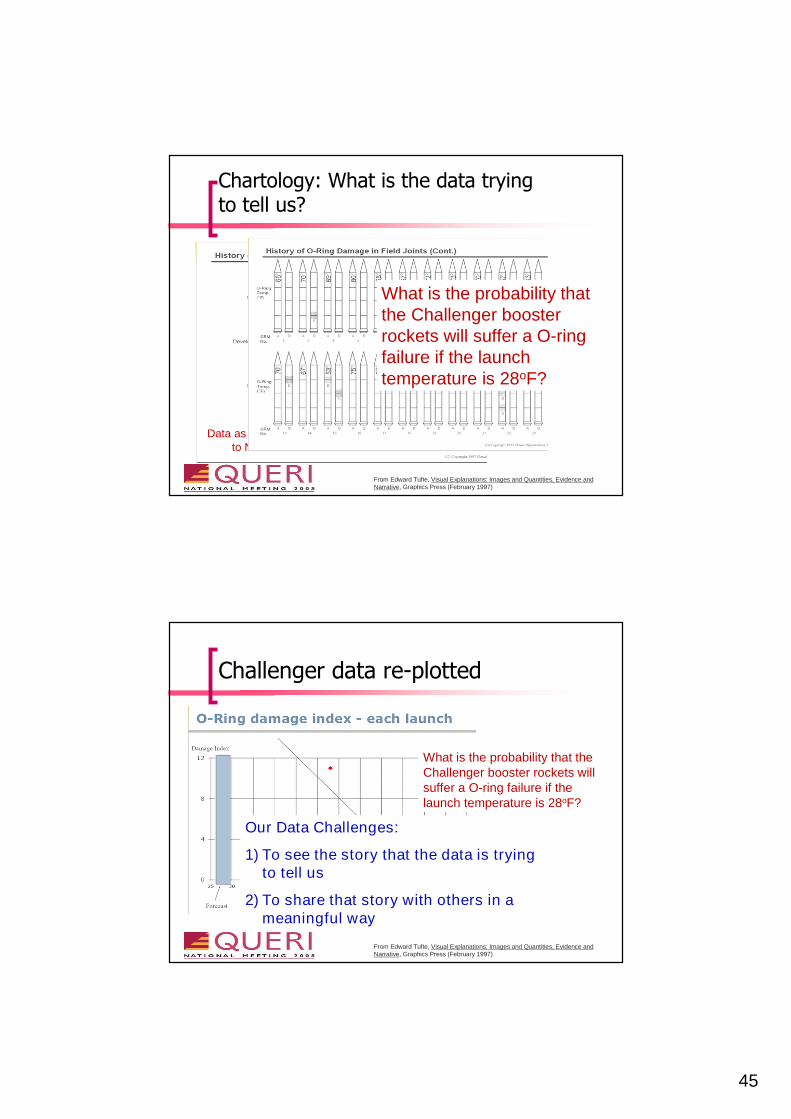
Chartology: What is the data tryingto tell us?
Data as presentedto NASA
From Edward Tufte, Visual Explanations: Images and Quantities, Evidence andNarrative, Graphics Press (February 1997)
What is the probability thatthe Challenger boosterrockets will suffer a O-ringfailure if the launchtemperature is 28oF?
Challenger data re-plotted
What is the probability that theChallenger booster rockets willsuffer a O-ring failure if thelaunch temperature is 28oF?
From Edward Tufte, Visual Explanations: Images and Quantities, Evidence andNarrative, Graphics Press (February 1997)
Our Data Challenges:
1) To see the story that the data is tryingto tell us
2) To share that story with others in ameaningful way

46
91
Case Study: Colon CancerScreening
A LSS Fast Start project is chartered toaddress the medical center’s failingColon Cancer Screening performancemeasures
The medical center does not doscreening colonoscopies!!!
92
Problemwith Returns
Problemwith
Screening
Additional Analysis:
If not returned in 2weeks, not returned
Additional Analysis:
Weak process – relianceon providers to writeorders; poor reminders;variance
What does the data tell us?
Metperformancemeasure
Somebody isDoing Screening
Colonoscopy
Additional Analysis:
Co-managed carepatients

47
Connecting Researchwith Patient Care
SR, ACA, ACA2, LSS, IE, LH:What’s in a name?
“Potato, potahto, Tomato, tomahto,
Let's call the whole thing off”
~ Louis Armstrong
It’s a Toolbox!

48
Connecting Researchwith Patient Care
Parting Words
“Courage and perseverance havea magical talisman, before whichdifficulties disappear andobstacles vanish into air. "~ John Quincy Adams
An Emergent Model forImprovement
Is there a welldefined policy?
Is there anawareness gap?
Is this a design /development project?
Policy DevelopmentProject(MGT)
Employee EducationProject(LRM)
Lean Design Team(MGT)
Is thereorganizationalcommitment*?
Formal(DEDISS) Project
Not a project!!
Yes
No
Yes
Yes
No
No
No
Yes
* Organizational Commitment:A willingness to free up 8-10front line staff for 50 hours eachto fix the process
Is this a crisis?Containment Team
(MGT)Yes
No

49
Improvement Life Cycle
Define
Evaluate
Design
Implement
Spread
Sustain
Quantify the problemSet goal: Specific, Measurable,Achievable, Relevant, Time-bound(SMART)
Current State Analysis: Processmaps, constraint identification,barriers, etc.
Brainstorm solutionsPlan RCC PDSA small tests ofchange (how to measure impact)
Conduct small tests of changeWhat was impact?Adopt, Adapt, Abandon
Go from small tests of change toexpanded tests and full scaleimplementation (training, policies,etc.)
Plan for “erosion”Identify “critical to quality” stepsSet action limit measuresDefine contingency plan
The Lean Six SigmaDMAIC cycle adapted
for healthcare
An Improvement Challenge to theResearch Community
CoachingExtracting
DataDocumenting
Problems
EngagingGeneratingInformation
AnticipatingFailures
TransformingCreating
KnowledgePredicting
Vulnerabilities
EffecterActivities
AnalyticalActivities
AfferentActivities
C
ap
ab
ilit
yE
vo
luti
on

50
Questions?
Contact information: