quality of care report 2014/15 - queensland health · the quality of care report is an annual...
TRANSCRIPT

Wide Bay Hospital & Health Service
Improving health, together 1
Clinical
Governance Clinical Information
Consumer Engagement
Clinical Risk
Management
Patient Safety
and Quality
Quality of Care Report
2015/16
Quality of Care Report
2014/15
Continuously improving the quality of patient care
Wide Bay Hospital & Health Service
Improving health, together 2
What is a Quality of Care Report?
The Quality of Care Report is an annual document reporting on the quality of the services delivered by the Wide Bay Hospital and Health Service (WBHHS). Its aim is to increase public awareness, increase health service accountability and drive quality improvement.
Why are we producing a Quality of Care Report?
There is no statutory duty, nor requirement from the State Government in Queensland, to produce a Quality of Care Report. The WBHHS has committed to a voluntary disclosure of its performance in quality domains, demonstrating our commitment to Improving Health, Together. By transparently communicating our quality performance, we allow the commu-nity to reflect on and analyse the care we are providing.
What is in the Quality of Care Report?
This report summarises how the WBHHS is performing against state and health service targets. The report describes:
1. The Patient Safety and Quality outcomes against the strategic objectives
2. Why monitoring the measure is important to improving patient outcomes
3. The WBHHS performance in 2014/2015 against key measures
4. Our goals for 2015/2016 to ensure continued improvements
5. How we are using these measures to make a difference for our community and for our health service.
Introduction

Wide Bay Hospital & Health Service
Improving health, together 3
I am pleased to release the first Quality of Care Report for the Wide Bay Hospital and Health Service (WBHHS). The WBHHS holds safe and quality care provision as a priority. The Quality of Care Report demonstrates our commitment to this, and aligns with our pledge to engage the community by communicating openly and transparently.
The past year has been one of continuous clinical improvement, particularly around our bedside care. This resulted in a very favourable outcome of the ACHS accreditation review in November 2014 against the National Safety and Quality Health Service Stan-dards (NSQHS) and the Equip National Standards.
Successful accreditation results do not occur without a commitment from every staff member to delivering Quality Care Everyday.
This report publicly displays our performance around some of the metrics of care and improvements we have made and are committed to.
Our improvements continued, performance was sustained and everyone associated with the WBHHS should be proud of those achievements.
Adrian PenningtonChief Executive
Wide Bay Hospital & Health Service
Statement on quality from the Chief Executive

Wide Bay Hospital & Health Service
Improving health, together 4
Pledge 1 – Delivering sustainable, patient centred, quality health services
1.1 National Safety and Quality Health Service Standards Compliance1.2 Clinical Incident Rate1.3 Clinical Incident Closure Rate1.4 Medication Error Rate 1.5 Falls Incident Rate1.6 Hospital Acquired Stage 3 & 4 Pressure Injuries1.7 Clinical Audit Compliance 1.8 Mortality Rate1.9 Healthcare – Associated Infections (staphylococcus aureus bacteraemia)1.10 Hand Hygiene Compliance Rate1.11 Immunisation Rate1.12 Mental Health Readmission Rate
Pledge 2 – Engaging with our communities and partners
2.1 Engaging with our communities and partners2.2 Complaints resolved within 35 calendar days2.3 Complaints to Compliments Ratio
Pledge 3 – Developing and empowering our workforce
3.1 Staff turnover3.2 Performance and Development Plan Rates3.3 Mandatory Training Rates
Pledge 4 – Encouraging innovation and excellence
4.1 Case Study – Endoscopy Blitz
Pledge 5 – Delivering value for money
5.1 National Elective Surgery Target (NEST) 5.2 Shorter maximum wait for elective surgery5.3 Emergency Triage Wait Times5.4 National Emergency Department Target (NEAT)5.5 Clinical Incident Management
Contents
Improving health, together

Wide Bay Hospital & Health Service
Improving health, together 5
The development of the Wide Bay Hospital and Health Service Strategic Plan (2014-2017) Improving health, together, clearly articulates the health service’s commitment to ensuring quality and safe care outcomes. The WBHH Board made the following pledges to the community to ensure high-quality services are provided:
1. Delivering sustainable, patient centred, quality health services
2. Engaging with our communities and partners
3. Developing and empowering our workforce
4. Encouraging innovation and excellence
5. Delivering value for money
The performance of the WBHHS is measured against specific indicators, linked to these pledges, and rated against a specific benchmark. The following outlines rating and achievement criteria applied in this report:
Improving health, together
Rating Achievement Criteria
Excellent Better than benchmark
Achieved Benchmark achieved
Very Good 95-99% of Benchmark
Good 80-95% of Benchmark
Poor 60-79% of Benchmark
Very Poor 50-59% of Benchmark
Unacceptable < 50% of Benchmark

Wide Bay Hospital & Health Service
Improving health, together 6
Pledge 1Delivering sustainable, patient centred, quality health services
The Wide Bay Hospital and Health Service aligns service delivery with quality outcomes to safeguard and improve carei. This is based on the principles of continuous quality improve-ment and the commitments made to the community in the Strategic Planii. The WBHHS, in this domain, focuses on the following:
• National Safety and Quality Health Service Standards
• Clinical Incidents
◦ Clinical Incident Rate
◦ Clinical Incident Closure Rate
◦ Medication Error Rate
◦ Fall Incidents
◦ Pressure Injuries
• Clinical Audit Compliance
• Hospital Standardised Mortality Ratio (HSMR)
• Infection Control
◦ Healthcare Associated Infections
◦ Hand Hygiene Compliance Rate
• Immunisation Rate
• Mental Health Readmission Rate

Wide Bay Hospital & Health Service
Improving health, together 7
Why it’s important
The National Safety and Quality Health Service Standards (NSQHSS) represent evidence-based, best prac-tice standards that organisations should strive to achieve.
How are we doing?
Source of measure WBHHS Performance 2014/15Service Level Agreement Meet all core actions
Our goal for 2015/2016
The WBHHS commits to being compliant with all the National Safety and Quality Health Service Standards on a day-to-day basis and being accreditation ready at any stage. The following table outlines the WBHHS target for 2015/2016.
Source of Measure QH Target WBHHS Target 2015/16
Service Level Agreement Meet all core standards Meet all core standards and 90% of all non core Standards
How have we used this measure to make a difference?
THE MEASURE National Safety and Quality Health Service Standards Compliance
PLEDGE 1: Delivering sustainable, patient centred, quality health services
… the [WBHHS] clinical governance framework has provided the organisation with a means to … ensure quality and safety is a priority across the organisation. The framework is patient-focused, with a culture of patient-centred care fostered at all levels.
Australian Council on Healthcare Standards WBHHS Accreditation Report
November 2014 Survey
“
Wide Bay Hospital & Health Service
Improving health, together 8
Why it’s important
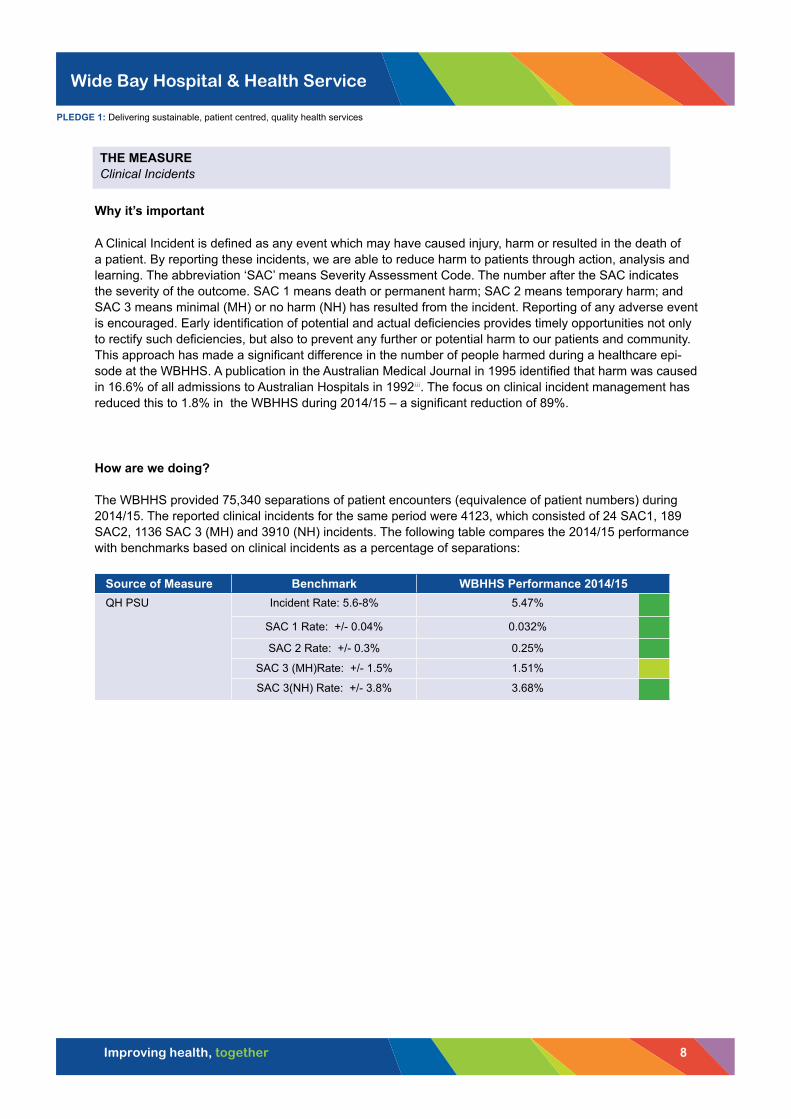
A Clinical Incident is defined as any event which may have caused injury, harm or resulted in the death of a patient. By reporting these incidents, we are able to reduce harm to patients through action, analysis and learning. The abbreviation ‘SAC’ means Severity Assessment Code. The number after the SAC indicates the severity of the outcome. SAC 1 means death or permanent harm; SAC 2 means temporary harm; and SAC 3 means minimal (MH) or no harm (NH) has resulted from the incident. Reporting of any adverse event is encouraged. Early identification of potential and actual deficiencies provides timely opportunities not only to rectify such deficiencies, but also to prevent any further or potential harm to our patients and community. This approach has made a significant difference in the number of people harmed during a healthcare epi-sode at the WBHHS. A publication in the Australian Medical Journal in 1995 identified that harm was caused in 16.6% of all admissions to Australian Hospitals in 1992iii. The focus on clinical incident management has reduced this to 1.8% in the WBHHS during 2014/15 – a significant reduction of 89%.
How are we doing?
The WBHHS provided 75,340 separations of patient encounters (equivalence of patient numbers) during 2014/15. The reported clinical incidents for the same period were 4123, which consisted of 24 SAC1, 189 SAC2, 1136 SAC 3 (MH) and 3910 (NH) incidents. The following table compares the 2014/15 performance with benchmarks based on clinical incidents as a percentage of separations:
Source of Measure Benchmark WBHHS Performance 2014/15QH PSU Incident Rate: 5.6-8% 5.47%
SAC 1 Rate: +/- 0.04% 0.032%
SAC 2 Rate: +/- 0.3% 0.25%
SAC 3 (MH)Rate: +/- 1.5% 1.51%
SAC 3(NH) Rate: +/- 3.8% 3.68%
THE MEASURE Clinical Incidents
PLEDGE 1: Delivering sustainable, patient centred, quality health services

Wide Bay Hospital & Health Service
Improving health, together 9
Our goal for 2015/2016
Source of Measure Benchmark WBHHS Target 2015/16QH PSU Incident Rate: 5.6-8% < 5.5 %
SAC 1 Rate: +/- 0.04% 0.03%
SAC 2 Rate: +/- 0.3% 0.20%
SAC 3 (MH)Rate: +/- 1.5% 1.50%
SAC 3(NH) Rate: +/- 3.8% 3.80%
How have we used this measure to make a difference?
While we constantly strive to ensure the best outcomes for our patients, they are unfortunately sometimes harmed while in our care. Through every tragic event, however, we have an opportunity to learn and improve. An incident in one of our emergency departments allowed our teams to look closely at the systems, processes and environment in which our staff and patients function. Through this process, we were able to uncover a previously unknown issue with one of our types of beds. We have now been able to remove and replace this equipment so an incident like the one we reviewed will never happen again. This is something we have also been able to let teams around the state know about, so they can act to prevent something similar happening in their service.
Patsy Richards,Clinical Governance Facilitator
“
PLEDGE 1: Delivering sustainable, patient centred, quality health services

Wide Bay Hospital & Health Service
Improving health, together 10
Why it’s important
Timely closure of incidents ensures we are responding and acting to make improvements as quickly as pos-sible. The timeframes are balanced to ensure incidents requiring the greatest analysis are given the attention required. The focus and tighter timeframes for the analysis of SAC 3 events (30 days) and for SAC2 events (60 days), introduced by the WBHHS is unique in Queensland. This focus has prevented potential deficien-cies in clinical care becoming actual deficiencies causing harm. The actual impact is difficult to quantify over the short time this has been in place, but the expectation is that the ratio of SAC1 and SAC2 to SAC 3 will reduce over time.
How are we doing?
Source of measure QH Target WBHHS Performance 2014/15
QH PSU
SAC 1: >70% closed in 90 days 78%
SAC 2: no benchmark 75%
SAC 3: no benchmark 58%
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
QH PSU
SAC 1: >70% closed in 90 days SAC 1: 100% closed in 90 days
SAC 2: no benchmark SAC 2: 95% closed in 60 days
SAC 3: no benchmark SAC 3: 90% closed in 30 days
How have we used this measure to make a difference?
THE MEASURE Clinical Incident Closure Rates
PLEDGE 1: Delivering sustainable, patient centred, quality health services
Analysis of incidents in a timely manner provides opportunities to improve the services provided by the WBHHS as soon as possible. While we try to meet the target timeframes, we are committed to ensuring we thoroughly review the incidents first, to truly understand and appropriately address the issues. On many occasions, we have managed to prevent harm to future patients by using this process.
“ Robyn Scanlan
Clinical Governance Programs Manager

Wide Bay Hospital & Health Service
Improving health, together 11
Why it’s important
Use of medicines is one of the most common therapeutic interventions in Australian hospitals. It is also one of the most complex, with as many as 30 steps involved in the delivery of each dose of medicine. The potential for errors is high because of this complexity, but preventable. Medication errors such as mistakes in prescribing, dispensing and administering medications may cause harm to hundreds of thousands of people a year across the world. Medication incidents have been estimated to cost the Australian healthcare system more than $660 million per year and represent 27% of all clinical incidents occurring in Australian hospitalsiv.
How are we doing?
Medication errors are expressed as a percentage of bed days of care provided. The WBHHS provided 150,154 days of care in 2014/15 and 1096 errors were reported. This is well below the benchmark, as demonstrated in the following table:
Source of measure Benchmark WBHHS Performance 2014/15
QH PSU < 2% 0.52%
Our goal for 2015/2016
Source of measure Benchmark WBHHS Target 2015/16
QH PSU < 2% < 0.52%
How have we used this measure to make a difference?
THE MEASURE Medication Error Rate
PLEDGE 1: Delivering sustainable, patient centred, quality health services
The WBHHS is striving to ensure safe medication management processes are in place so we can provide the best patient outcomes. In the past 12 months, the WBHHS has initiated significant changes in the way we monitor and review medication management. These include the establishment of a Medication Safety Committee to ensure representation from all sectors of the WBHHS are reviewing incidents and processes, and acting to implement quality improvements; the development of a Medication Management Framework to ensure all clinicians are safely engaged in the medication continuum; the development of a High-Risk Medications Register with safety strategies applied to those medications we know pose the highest risks to our patients; and a recent move to have senior pharmacists and clinical governance facilitators working directly with frontline clinicians to provide a proactive response to preventing potential harm from medications. All of these initiatives help support the WBHHS’s commitment to providing safe care for patients.
Aaron Basing Advanced Pharmacist, WBHHS, Chair of the WBHHS Medication Safety Committee
“

Wide Bay Hospital & Health Service
Improving health, together 12
Why it’s important
Hospital patients are often in a weakened or confused state and are more susceptible to falling. Falls are a leading cause of hospital-acquired injury, and frequently prolong or complicate hospital stays. Falls occurring in hospital can result in patient harm and are regarded as adverse events, some of which may be preventable and can be used as one indicator of safety for hospitals. Falls among hospital inpatients are common, generally ranging from 2.3 to seven falls per 1000 patient daysv. Approximately 30% of inpatient falls result in injury, with 4% to 6% resulting in serious injuryvi. Prevention of falls in the hospital setting is therefore an important patient safety and public health issue. How are we doing?
Source of measure QH Target WBHHS Performance 2014/15
QH PSU < 2.6% 0.4%
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
QH PSU < 2.6% < 0.4%
How have we used this measure to make a difference?
THE MEASURE Fall Incident Rate
PLEDGE 1: Delivering sustainable, patient centred, quality health services
The WBHHS is committed to preventing falls within our service. We are pleased with the reported rate of falls being well below the target benchmark, but that doesn’t mean we stop trying to continually improve. We have processes in place to ensure a falls risk screening is undertaken on all patients admitted to our service. Where risk is identified, prevention strategies are implemented in consultation with the patient and family. To standardise the care we provide and to ensure falls prevention is undertaken in alignment with best practice guidelines, the WBHHS has implemented statewide forms for screening and clinical pathways for the management of a patient should a fall still occur.
Katrina OllisNursing Director Surgical Services North
Chair of the WBHHS Pressure Injury and Falls Prevention Committee
“

Wide Bay Hospital & Health Service
Improving health, together 13
Why it’s important
Pressure injures are internationally recognised as a quality indicator of care provided. These localised injuries to the skin and/or underlying tissue are caused by unrelieved pressure, friction and shear factors. Research suggests 95% of pressure injuries are preventable, particularly hospital-acquired pressure injuries, which result in a considerable cost to the patient, their family, the organisation and health systemvii. In Australia the cost of hospital-acquired pressure injuries was estimated at $12.2 million annuallyviii. By monitoring the rates of this level of pressure injuries we can evaluate our screening, assessment and prevention strategies and make improvements if we find a problem.
How are we doing?
Source of measure QH Target WBHHS Performance 2014/15
QH PSU < 0.01% 0.04%
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
QH PSU < 0.01% < 0.01%
How have we used this measure to make a difference?
THE MEASURE Hospital acquired Stage 3 & 4 pressure injuries
PLEDGE 1: Delivering sustainable, patient centred, quality health services
To ensure we are continually providing the best care possible to our patients, the WBHHS utilises nationally and internationally recognised best practice guidelines and screening tools. We are also fortunate enough to have specialist wound care nurses to support our frontline staff in the identification and management of pressure injuries. Despite this, we have still not achieved the outcomes for our patients that we really wanted to achieve. To improve, we are currently undertaking an intensive review of our systems and processes in relation to pressure injury prevention. The results of these reviews are uncovering some great areas where we can make significant changes. Involving frontline team members in the quality improvement processes for pressure injury prevention will ensure that patients in the WBHHS will receive the best outcomes.
Fiona SewellExecutive Director of Nursing and Midwifery Services, WBHHS
Chair of the WBHHS Provision of Care and Service Delivery Committee
“

Wide Bay Hospital & Health Service
Improving health, together 14
Why it’s important
Clinical audit has been defined as “a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and the implementation of change”ix. While clinical audit makes great sense, there can be problems in persuading hospitals and clinicians to undertake and apply clinical audit in their work. Nonetheless, clinical audit is one of the key components of clinical governance measures that are required by the WBHHS. It is a cyclical process of reviewing clinical performance, refining practice as a result and measuring the outcomes against agreed standards and is an essential component of evidence-based clinical practice. Compliance with the WBHHS Clinical audit schedule are measured to ensure:
1. That clinical audit occurs2. More importantly, that quality improvement initiative can be identified pro-actively.
How are we doing?
Compliance with Clinical Audit at the WBHHS, as illustrated in the table below, is not at the level expected. Significant effort is directed to improving compliance with good trends noted currently.
Source of measure Target WBHHS Performance 2014/15
CGov No Benchmark: WBHHS > 80% 52%
Our goal for 2015/2016
Source of measure Target WBHHS Target 2015/16
CGov No Benchmark: WBHHS > 80% > 80%
How have we used this measure to make a difference?
THE MEASURE Clinical Audit Compliance
PLEDGE 1: Delivering sustainable, patient centred, quality health services
Clinical audits are undertaken regularly by most departments and are used in decision processes regarding improvement of quality of care. Some examples of recent audits which have contributed to improvement are theatre turnover time, readmissions within 30 days, VTE assessment form completion, pre-op/peri-admission clerking of patients, subtrochanteric fracture re-operation rates, CTPA rates in ED, patient satisfaction and rate of infection/complication using Port A Cath/PICC in chemotherapy. Clinical staff appreciate the value of the audit processes when applied to areas of direct relevance to their care and the scope of these activities is gradually increasing.
Dr Greg Coffey MBBS, FRACGP, GDipPH, MHM, FRACMA, MFMLM
District Director of Medical Services
“

Wide Bay Hospital & Health Service
Improving health, together 15
Why it’s important
The hospital standardised mortality ratio (HSMR) has emerged as a potentially universal system-level indicator for comparing mortality between hospitals both within and across different countries. This indicator is a comparison between the expected in-hospital deaths and the actual number of deaths based on the patient population’s characteristics. It is presently reported in the United Kingdom, Sweden, Netherlands, Canada, United States and Australiax. The Australian Health Ministers endorsed this as a core set of national indicators of safety and quality xi. Measuring death rates has the advantage that death is a definite unique event unlike morbidity, which often represents a spectrum of severity and can be difficult to record accurately. Death rates can, when adjusted for the factors that affect death rates, act as markers of a hard outcome of healthcare. In England, the hospital standardised mortality ratio (HSMR), an overall measure of in-hospital mortality, has been used since 1999xii. How are we doing?
The table below illustrates that the HSMR at WBBHS is less than 50% of what is predicted by Queensland Health. This is a very significant indication of the quality of care provided especially in light of the health risks of the WBHHS population.
Source of measure Deaths Target Mortality Ratio WBHHS Performance 2014/15
QH Expected Deaths 538 1 0.49
WBHHS Deaths 261 0.49
Our goal for 2015/2016
Source of measure Target Mortality Rate WBHHS Target 2015/16
PSU 1 <1
How have we used this measure to make a difference?
The HSMR, like all statistical indicators, is not perfect but the WBHHS closely monitors it on an ongoing basis as a measure of safe, high-quality care and a warning sign that things are going wrong.
THE MEASURE Hospital Standardised Mortality Ratio (HSMR)
PLEDGE 1: Delivering sustainable, patient centred, quality health services
There is sometimes debate about the validity of comparing hospitals using this indicator, as tertiary and quaternary services will always have a more complex case-load, but valid comparisons between similar group hospitals cannot be disputed, and changes over time are also accepted as reliable indications of quality of care. The HHS will therefore be watching for any trends over time, and comparing with other regional centres.
Dr Greg Coffey MBBS, FRACGP, GDipPH, MHM, FRACMA, MFMLM
District Director of Medical Services
“
Wide Bay Hospital & Health Service
Improving health, together 16
Why it’s important
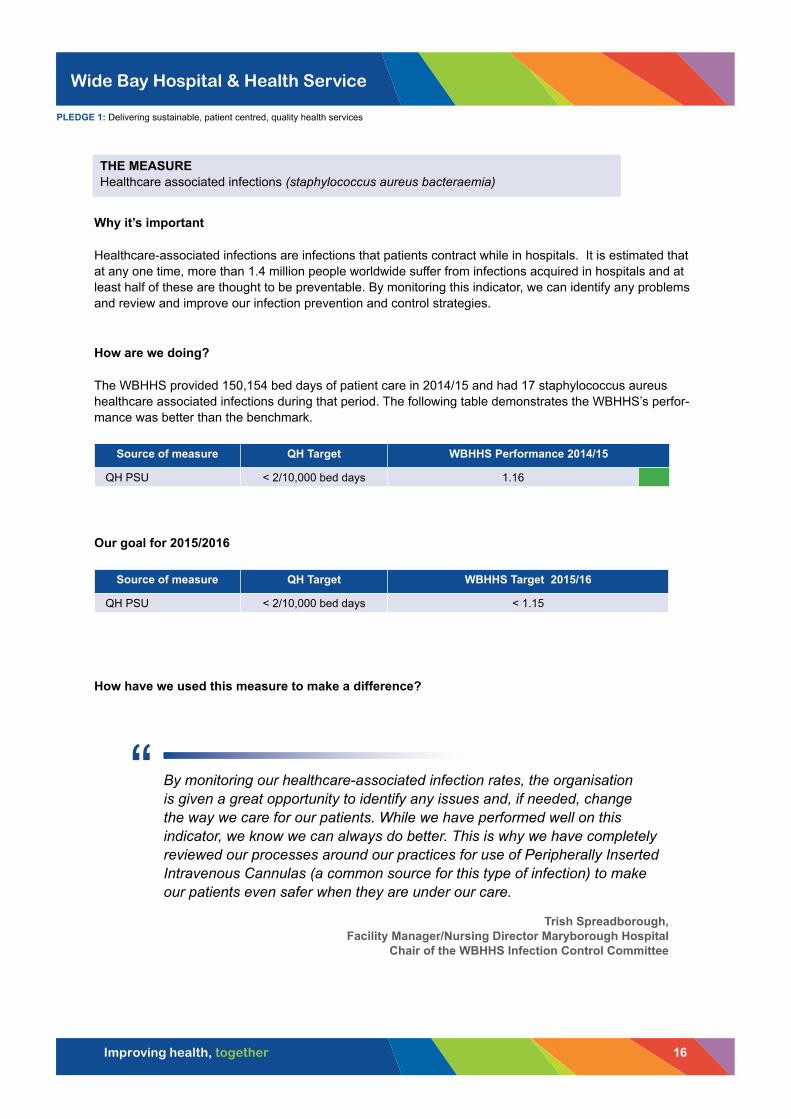
Healthcare-associated infections are infections that patients contract while in hospitals. It is estimated that at any one time, more than 1.4 million people worldwide suffer from infections acquired in hospitals and at least half of these are thought to be preventable. By monitoring this indicator, we can identify any problems and review and improve our infection prevention and control strategies.
How are we doing?
The WBHHS provided 150,154 bed days of patient care in 2014/15 and had 17 staphylococcus aureus healthcare associated infections during that period. The following table demonstrates the WBHHS’s perfor-mance was better than the benchmark.
Source of measure QH Target WBHHS Performance 2014/15
QH PSU < 2/10,000 bed days 1.16
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
QH PSU < 2/10,000 bed days < 1.15
How have we used this measure to make a difference?
THE MEASURE Healthcare associated infections (staphylococcus aureus bacteraemia)
PLEDGE 1: Delivering sustainable, patient centred, quality health services
By monitoring our healthcare-associated infection rates, the organisation is given a great opportunity to identify any issues and, if needed, change the way we care for our patients. While we have performed well on this indicator, we know we can always do better. This is why we have completely reviewed our processes around our practices for use of Peripherally Inserted Intravenous Cannulas (a common source for this type of infection) to make our patients even safer when they are under our care.
Trish Spreadborough, Facility Manager/Nursing Director Maryborough Hospital
Chair of the WBHHS Infection Control Committee
“

Wide Bay Hospital & Health Service
Improving health, together 17
Why it’s important
Hand hygiene, either by handwashing or hand disinfection, remains the single most important measure to prevent hospital-acquired infectionsxiii. Poor hand hygiene practice (handwashing, hand disinfection) among healthcare workers is strongly associated with healthcare-acquired infection transmission and is a major factor in the spread of antibiotic-resistant pathogens within hospitalsxiv. The WBHHS has made hand-hygiene education compulsory for all staff and compliance is measured on a monthly basis.
How are we doing?
Hand hygiene is a mandatory training requirement for all WBHHS staff and compliance with this expectation was not met during 2014/15 as outlined in the table below. While theoretical training rates have not reached the compliance target, our low infection rate indicates hand-hygiene practice is of a high standard.
Source of measure WBHHS Target WBHHS Performance 2014/15
ETRS CGov data base 100% compliance 75.89%
Our goal for 2015/2016
Source of measure WBHHS Target WBHHS Target 2015/16
QH PSU 100% compliance 100%
How have we used this measure to make a difference?
THE MEASURE Hand Hygiene Training Compliance Rate
PLEDGE 1: Delivering sustainable, patient centred, quality health services
To assist in preventing transmission of infections from healthcare providers to our patients, the WBHHS is committed to the National Hand Hygiene initiatives. Regular monitoring of educational competency as well as auditing our clinicians’ compliance with the initiatives occurs in all relevant areas of our health service. An initiative entitled ‘Bare Below the Elbows’ has been implemented in high-risk areas in our health service to facilitate good hand hygiene practices and minimise the inadvertent transmission of infections.
Raelene FisherClinical Nurse Consultant, Infection Control
“

Wide Bay Hospital & Health Service
Improving health, together 18
Why it’s important
Immunisations are simple, effective and safe ways to protect individuals against serious disease. Immunisation programs help protect the community against the spread of potentially serious illness and disease, but success depends on maintaining high immunisation rates over time.
How are we doing?
Source of measure Benchmark WBHHS Performance 2014/15
WBHHS Public Health Unit 90% >90%
Our goal for 2015/2016
For 2015/2016, the WBHHS aims to meet the Queensland Immunisation Strategy (2014-2017) target for 95% of children to be fully immunised.
Source of measure Benchmark WBHHS Target 2015/16
WBHHS Public Health Unit 90% > 95%
How have we used this measure to make a difference?
THE MEASURE Immunisation Rate
PLEDGE 1: Delivering sustainable, patient centred, quality health services
To improve childhood immunisation rates, the Wide Bay Public Health Unit conducts a regular audit of children who are overdue for their immunisations. Timeliness of vaccination is important to ensure the best protection, and the Australian Childhood Immunisation Register is regularly checked by the WBHHS Public Health Team for completeness. Medical practices are contacted to cross-check and update immunisation records and reminders are sent to parents/carers who require additional vaccines. This strategy will be ongoing as it ensures a high rate of compliance within the WBHHS.
Dr Margaret YoungPublic Health Physician
Director of the WBHHS Public Health Unit
“

Wide Bay Hospital & Health Service
Improving health, together 19
Why it’s important
Mental health care is focused on a recovery-based model which provides treatment in a least restrictive environment. This measure allows Mental Health to monitor a person’s discharge and their engagement in the community for follow-up to reduce the need for readmission, including the monitoring and management of symptoms to decrease relapse and the need for inpatient admission.
How are we doing?
Source of measure QH Target WBHHS Performance 2014/15
Service Level Agreement < 12% 10.10%
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
Service Level Agreement < 12% < 10%
How have we used this measure to make a difference?
THE MEASURE 28-day Mental Health Readmission Rate
PLEDGE 1: Delivering sustainable, patient centred, quality health services
Through monitoring the 28-day readmission rates for our clients, we are able to ascertain whether the community support strategies we implement are applicable to our clients’ needs. This measure gives us an opportunity to review our practices and implement continuous quality improvement throughout our service. The Mental Health Alcohol and Other Drugs Service in the WBHHS has better than targeted outcomes. A broad range of initiatives have been implemented to ensure our clients receive consumer-focused care in the least restrictive environment. These include ensuring, at a minimum, a seven-day post-discharge follow-up in the community to review any concerns and implement any improvements to our clients’ discharge plan as required. This ensures our consumers are linked to community support services suitable to their needs.
Robyn BradleyExecutive Director of Mental Health Services, WBHHS
“

Wide Bay Hospital & Health Service
Improving health, together 20
The WBHHS values engaging with our community. An extensive consultation program was undertaken by the WBHH Board to develop a comprehensive strategic plan for 2014-2017. This enabled the organisation to identify areas for improvements in meeting the community’s needs. The WBHHS, in this domain, focused on the following quality indicators:
• Complaints management
◦ Acknowledgment within five days
◦ Resolution within 35 days
• Ratio of complaints to compliments
Complaints and compliments give us a gauge of how well we are meeting our community’s healthcare needs. Further to this, complaints give us a valuable source of information on how we can build and strengthen our services. The WBHHS welcomes feedback in all its forms.
Pledge 2Engaging with our communities and partners
Wide Bay Hospital & Health Service
Improving health, together 21
Why it’s important
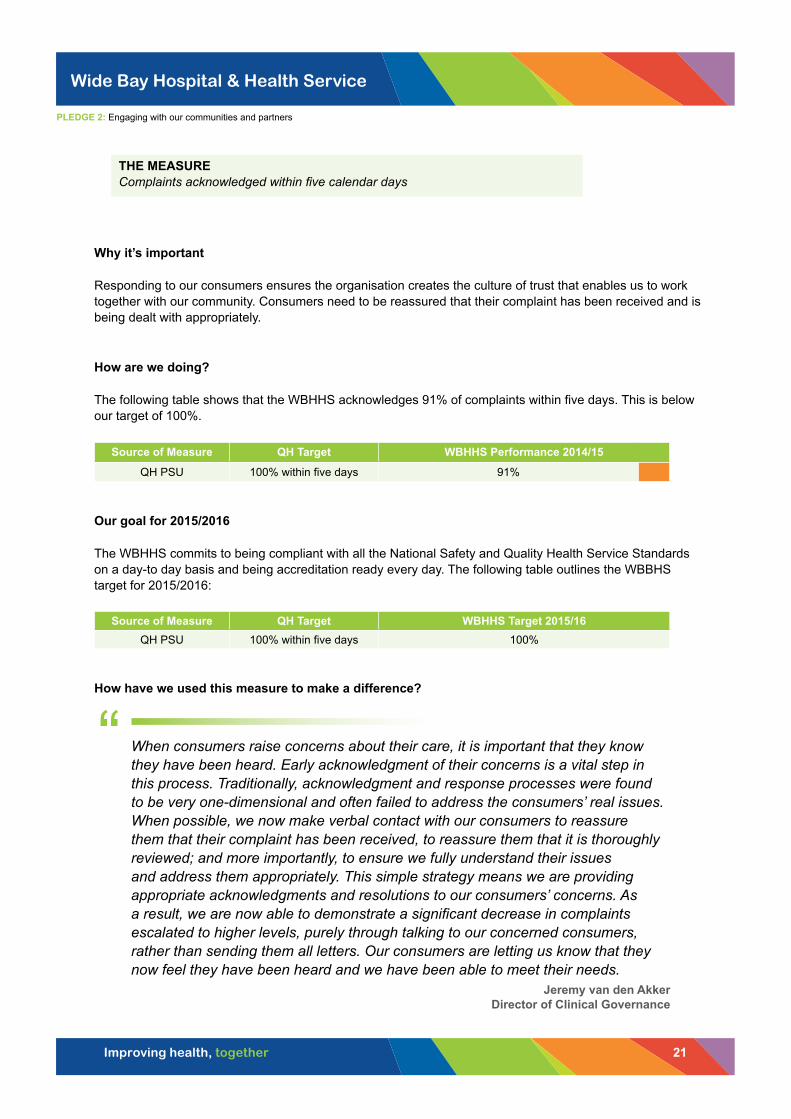
Responding to our consumers ensures the organisation creates the culture of trust that enables us to work together with our community. Consumers need to be reassured that their complaint has been received and is being dealt with appropriately. How are we doing?
The following table shows that the WBHHS acknowledges 91% of complaints within five days. This is below our target of 100%.
Source of Measure QH Target WBHHS Performance 2014/15
QH PSU 100% within five days 91%
Our goal for 2015/2016
The WBHHS commits to being compliant with all the National Safety and Quality Health Service Standards on a day-to day basis and being accreditation ready every day. The following table outlines the WBBHS target for 2015/2016:
Source of Measure QH Target WBHHS Target 2015/16QH PSU 100% within five days 100%
How have we used this measure to make a difference?
THE MEASURE Complaints acknowledged within five calendar days
When consumers raise concerns about their care, it is important that they know they have been heard. Early acknowledgment of their concerns is a vital step in this process. Traditionally, acknowledgment and response processes were found to be very one-dimensional and often failed to address the consumers’ real issues. When possible, we now make verbal contact with our consumers to reassure them that their complaint has been received, to reassure them that it is thoroughly reviewed; and more importantly, to ensure we fully understand their issues and address them appropriately. This simple strategy means we are providing appropriate acknowledgments and resolutions to our consumers’ concerns. As a result, we are now able to demonstrate a significant decrease in complaints escalated to higher levels, purely through talking to our concerned consumers, rather than sending them all letters. Our consumers are letting us know that they now feel they have been heard and we have been able to meet their needs.
Jeremy van den AkkerDirector of Clinical Governance
“
PLEDGE 2: Engaging with our communities and partners

Wide Bay Hospital & Health Service
Improving health, together 22
Why it’s important
Complaints are an important source of information which we use to improve quality and safety. Timely investigation and appropriate resolution demonstrates a willingness to listen, act and work with consumers to continuously improve our services.
How are we doing? The following table demonstrates that the WBHHS completed 77% of complaint investigations within 35 days. This is slightly below the 80% target.
Source of measure QH Target WBHHS Performance 2014/15
QH PSU 80% within 35 days 77%
Our goal for 2015/2016
Source of measure QH Target WBHHS Target 2015/16
WBHHS Public Health Unit 80% within 35 days >80%
How have we used this measure to make a difference?
THE MEASURE Complaints resolved within 35 calendar days
PLEDGE 2: Engaging with our communities and partners
The WBHHS receives more compliments about its service than complaints. However, every complaint or comment received is an opportunity for the health service to make an improvement. This is how the WBHHS approaches the receipt of complaints. The service is striving to ensure all complaints received are responded to in a timely manner to the satisfaction of the complainant.
Martin ChambersConsumer representative
WBHHS Safety and Quality Committee
“

Wide Bay Hospital & Health Service
Improving health, together 23
Why it’s important
Knowing and understanding what we are doing well and whether we meet community needs is important. This assists with sharing the good lessons across our services.
How are we doing?
The table below shows that the WBHHS receives nearly two compliments for every complaint.
Source of measure Benchmark WBHHS Performance 2014/2015
QH PSU No benchmark 1 complaint: 1.9 compliments
Our goal for 2015/2016
Source of measure Benchmark WBHHS Target 2015/2016
WBHHS Public Health Unit No benchmark 1 complaint: 2 compliments
How have we used this measure to make a difference?
THE MEASURE Ratio of complaints to compliments
PLEDGE 2: Engaging with our communities and partners
The respect, care, compassion and dignity which all staff provided to my mum and family… was exemplary. No matter what was required, all staff went above and beyond with all duties. I can honestly say that I have never had the privilege of meeting a more dedicated group of healthcare professionals … My wife and I have seen our fair share of hospitals both in Australia and abroad … Given that Childers Hospital is a small rural facility, the staff and management should be extremely proud of the world-class service they provide to patients and their families.
Simon FauchonFeedback given on the care provided at Childers Hospital
“

Wide Bay Hospital & Health Service
Improving health, together 24
Pledge 3Developing and empowering our workforce
In order to deliver safe, high-quality care to our patients and community, the WBHHS needs to ensure it has the right people for the job and a stable workforce that is well trained, with performance adequately monitoredxv. The WBHHS, in this domain, focused on the following:
• Staff Turnover Rates
• Performance and Development Plan Rates
• Mandatory Training Rates
Through developing and empowering our workforce, and ensuring they are delivering the best outcomes for our patients, we can be assured we are delivering “Quality Care Everyday”.

Wide Bay Hospital & Health Service
Improving health, together 25
Why it’s important
Staff turnover rates can indicate how well the organisation is meeting the needs of its staff and highlight circumstances that may need addressing to ensure a stable workforce. Where a positive staff experience and organisational support are available, people are more likely to stay. Staff turnover rates are also a vital planning tool that enable strategies to be put in place to address identified problems, and implement strategies to remedy any instability in the workforce.
Stable staff turnover rates result in positive benefits for our patients, community and organisation, including:
• Experienced, confident healthcare providers that facilitate:
◦ Better patient results and experience due to consistent care
◦ Stable and consistent in-service delivery and standards of care
◦ Decreased costs. With less expenditure on recruitment and commencement expenses, resources are available for focus on clinical service provision.
How are we doing?
Source of Measure Target WBHHS Performance 2014/15WBHHS HR 1.08% 1.17%
Our goal for 2015/2016
Source of Measure Target WBHHS Target 2015/16WBHHS HR 1.08% <1.08%
How have we used this measure to make a difference?
THE MEASURE Staff Turnover Rate
Critical to minimising workforce turnover rates is creating an environment that meets our staff needs. The work undertaken in workforce planning and creating a stable workforce has brought our rate down to close to the target benchmark. As an organisation, we will continue to work hard at recruiting and retaining the right people for our patients. We know quality of care improves with a stable workforce; this is our priority.
Peter HeinzExecutive Director of Human Resource Services, WBHHS
Chair of the WBHHS Workforce Planning and Management Committee
“
PLEDGE 3: Developing and empowering our workforce

Wide Bay Hospital & Health Service
Improving health, together 26
Why it’s important
Developing skills and understanding of staff is key to the success of our organisation and the quality of services we provide. It is important that staff are regularly reviewed to ensure their performance, skills, talents and training align with the strategic goal of Improving health, together.
How are we doing?
Source of measure WBHHS Target WBHHS Performance 2014/15
ETRS CGov database 100% 50.93%
Our goal for 2015/2016
Source of measure WBHHS Target WBHHS Target 2015/16
ETRS CGov database 100% 100%
How have we used this measure to make a difference?
THE MEASURE Performance and development plan rates
PLEDGE 3: Developing and empowering our workforce
The success of an organisation in providing quality care depends on ensuring regular review of our staff performance. This creates an opportunity to build and grow our workforce in a way that meets the needs of our patients and the community. Using the Performance and Development process we are able to inform our educational frameworks and improve our staff retention rates through greater staff commitment.
Glenda BowaterManager Human Resource Services, WBHHS
“

Wide Bay Hospital & Health Service
Improving health, together 27
Why it’s important
An adequately trained workforce helps ensure staff can work in a safe environment and we can provide the highest-quality care to our consumers. Our mandatory training rate covers all areas of the health service, both clinical and non-clinical.
How are we doing?
Source of measure WBHHS Target WBHHS Performance 2014/15
ETRS CGov data base 100% 76.04%
Our goal for 2015/2016
Source of measure WBHHS Target WBHHS Target2015/16
ETRS CGov database 100% 100%
How have we used this measure to make a difference?
THE MEASURE Mandatory Training Rate
PLEDGE 3: Developing and empowering our workforce
Mandatory training is a priority within the WBHHS Education and Training strategic plan. It is a shared commitment between staff and line managers, ensuring safe and high-quality care is provided to our patients. To increase our performance in this measure, we have focused on improving accessibility for staff through moving training delivery to an online learning platform and redesigning the mandatory training elements to meet WBHHS workforce needs. These strategies have seen excellent improvements in staff engagement with the mandatory component of their professional development.
Darian WardDirector of Education, Training and Research, WBHHS
“

Wide Bay Hospital & Health Service
Improving health, together 28
Pledge 4Encouraging innovation and excellence
The WBHHS is committed to building an organisational culture of innovation and excellence. By empowering our staff to drive improvements, we are able to build an environment where the future of healthcare delivery can be transformed. The three principles guiding transformational care, innovation and excellence should be:
1. Value for the patient
2. Care delivery organised around patient needs and care cycles
3. All results are risk adjusted and measuredxvi
Using these principles to drive innovation and excellence contributes to a new evidence base for best patient outcomes. In this domain, the work undertaken to decrease Endoscopy waiting times for WBHHS patients is highlighted as an example of innovation and excellence.
Photo: Michael Marston

Wide Bay Hospital & Health Service
Improving health, together 29
Why it’s important Cancer is the leading cause of burden of disease, accounting for 19% of total burden in Australia. The incidence of cancer is significantly higher in the Wide Bay, most notably for bowel and prostate cancers – the two most commonly diagnosed across the country. Endoscopy is the most important and effective diagnostic procedure for identifying bowel cancer, which has now overtaken heart disease as the leading cause of death in Australia. Early diagnosis of cancer enables early treatment and more likely chance of cure. In July 2013, the average wait time for Category 4 patients was 12 months and Category 6 up to three years. All patients identified with bowel cancer on diagnostic procedure were reported on the PRIME CI system. Following trending analysis the clinicians were concerned that lives were being impacted due to late diagnosis. The WBHHS Cancer Care Strategic Plan was released in 2015, outlining specific pathways with pre-defined timelines for the treatment of cancer from first suspicion to final outcome, in response to those concerns.
How are we doing?
Source of Measure QH Target WBHHS Performance 2014/15 ESISS 100% Cat 4 – 30 days 78%
100% Cat 5 – 90 days 95%
100% Cat 6 – 365 days 100%
Our goal for 2015/2016
Source of Measure QH Target WBHHS Target 2015/16 ESISS 100% Cat 4 – 30 days 100% Cat 4 - 28 days
100% Cat 5 – 90 days 80% Cat 5 - 28 days
100% Cat 6 – 365 days 75% Cat 6 - 28 days
THE MEASURE Endoscopy wait times
PLEDGE 4: Encouraging innovation and excellence

Wide Bay Hospital & Health Service
Improving health, together 30
How have we used this measure to make a difference?
WBHHS is committed to sustainably eliminating long waits for endoscopy. Development of a four-week pathway from GP to diagnosis was clinician led to ensure no patient dies while waiting. This pathway was the first of its kind in Australian public health system, which resulted in a Director-General Commendation Innovation Award in 2014. Two models were trialled in Bundaberg and Fraser Coast. One had exceptional clinician engagement and patient focus, which resulted in collection of accurate data. This revealed that 1.6% of diagnostic procedures resulted in a cancer diagnosis with Category 1 elective surgery wait time applied.
One in two Australian men and one in three Australian women will be diagnosed with cancer in their lifetime. We know a cancer diagnosis can be overwhelming for patients and their family. That’s why our service is dedicated to the highest quality, innovative and efficient cancer services every step of the way from diagnosis to treatment.
Ray Johnson Operations Director, WBHHS Cancer Care Service
“

Wide Bay Hospital & Health Service
Improving health, together 31
Quality, value and cost have been linked for decades. Providing quality, timely clinical care provides value for money. The WBHHS, in this domain, focuses on the following.
Waiting times:
• For Elective Surgery -– National Elective Surgery Target (NEST)
◦ From referral to surgery – A 90-day target based on the WBHHS Strategic Plan commitment
◦ In the Emergency Department based on Triage code
◦ For admission or discharge from the Emergency Department – National Emergency Department Target (NEAT)
• Reduction in Clinical Incidents
The delivery of care based on a current and emerging evidence base minimises unnecessary long stays, unnecessary harm and unnecessary complications for our patients. This in turn ensures we delivery patient-centred value for money while increasing our quality of carexvii.
Pledge 5Delivering value for money

Wide Bay Hospital & Health Service
Improving health, together 32
Why it’s important Surgeries can be performed under elective or emergency conditions, depending on the patient’s needs. Elective surgery or elective procedure is surgery that is scheduled in advance because it does not involve a medical emergency, and semi-elective surgery is a surgery that must be done to preserve the patient’s life, but does not need to be performed immediately. Much elective surgery is therefore important to maintaining health and wellbeing. The length of time a patient has waited from the time their elective surgery is booked to when they are admitted for their elective surgery is known as waiting timexviii. Waiting times assist in measuring the rate of turnover on hospital waiting lists and are considered a more reliable indicator of a hospital’s performance than the size of the waiting list xix. NEST is designed to improve services so that patients can receive elective surgery within the clinically recommended time.
How are we doing?
Source of Measure QH Target WBHHS Performance 2015/16
Service Level Agreement Cat 1 : 100% within 30 days 95%
Cat 2 : 94% within 90 days 83%
Cat 3 : 97% within 365 days 92%
Our goal for 2015/2016
Source of Measure QH Target WBHHS Target 2015/16
Service Level Agreement Cat 1 : 100% within 30 days 100%
Cat 2 : 94% within 90 days 94%
Cat 3 : 97% within 365 days 97%
How have we used this measure to make a difference?
THE MEASURE National Elective Surgery Target (NEST)
Pledge 5: Delivering value for money
When our patients need surgery we do what we can to ensure they receive it as soon as they require it. We understand the difficulties and uncertainty our patients face when waiting for their procedure. This is why we are committed to not only meeting the National Elective Surgery Targets but working towards exceeding them.
“ James Thomas
General Manager of Surgical Services

Wide Bay Hospital & Health Service
Improving health, together 33
Why it’s important Beyond the NEST, the WBHHS has committed to decreasing the wait times for those who experience the longest wait – our Category 3 elective surgery patients – across five specialties. As with the driver for the NEST, we know that undue long waits have detrimental effects on our patients. By providing procedures as soon as possible, we are able to prevent patient harm.
How are we doing?
Source of Measure QH Target WBHHS Performance 2014/15
Service Level Agreement ENT surgery: 365 days 141 days
General surgery: 365 days 328 days
Gynaecology: 365 days 332 days
Orthopaedic surgery: 365 days 353 days
Urology: 365 days 264 days
Our goal for 2015/2016
Source of Measure QH Target WBHHS Target 2015/16
Service Level Agreement
ENT surgery: 365 days < 183 days
General surgery: 365 days < 183 days
Gynaecology: 365 days < 183 days
Orthopaedic surgery: 365 days < 183 days
Urology: 365 days < 183 days
How have we used this measure to make a difference?
THE MEASURE Shorter maximum wait for elective surgery (from referral to surgery)
Pledge 5: Delivering value for money
Orthopaedic patients in the WBHHS are receiving their surgeries more quickly than the statewide target. Our aim is to continually improve on these outcomes so our patients can receive the care they require as soon as possible.
Dr Eugene Gehr Director of Orthopaedics, Hervey Bay
“

Wide Bay Hospital & Health Service
Improving health, together 34
Why it’s important Triage is an internationally recognised system to ensure patients needing priority medical care receive it in a timeframe that will minimise poor outcomes xx. The higher the acuity of the patient (eg Category 1), the more quickly a patient needs to be seen to prevent death, deterioration or permanent harm.
How are we doing?
Source of Measure ACEM Benchmark WBHHS Performance 2014/15
Service Level Agreement
Cat 1 : 100% within 2 minutes 100%
Cat 2 : 80% within 10 minutes 85%
Cat 3 : 75% within 30 minutes 81%
Cat 4 : 70% within 60 minutes 76%
Cat 5 : 70% within 120 minutes 90%
Our goal for 2015/2016
Source of Measure ACEM Benchmark WBHHS Target 2015/16
Service Level Agreement
Cat 1 : 100% within 2 minutes 100%
Cat 2 : 80% within 10 minutes 88%
Cat 3 : 75% within 30 minutes 80%
Cat 4 : 70% within 60 minutes >70%
Cat 5 : 70% within 120 minutes >70%
How have we used this measure to make a difference?
THE MEASURE Waiting time by triage code
Pledge 5: Delivering value for money
Across all the triage categories, the WBHHS has ensured patients are seen within the clinically recommended timeframes. Through a concerted effort by our clinical teams, who have streamlined our patient flows through our triage and emergency departments, patients are now being seen more quickly and receiving the care they need, to achieve optimal outcomes.
Rick van Groningen General Manager, Critical Care Division, WBHHS
“

Wide Bay Hospital & Health Service
Improving health, together 35
Why it’s important A UK study comparing performance of hospitals close to the border between England (where waiting time targets existed) and Wales (where such targets did not), showed that patients attending English hospitals faced shorter ED waiting times and had lower mortality rates than those attending Welsh hospitals xxi. NEAT is measured as the percentage of patients who leave the emergency department (ED) within four hours arrival. The time is calculated from when patients arrive at the emergency department to the time they have left.
How are we doing?
Source of Measure QH Target WBHHS Performance 2014/15Service Level Agreement 83% 77%
Our goal for 2015/2016
Source of Measure QH Target WBHHS Target 2015/16Service Level Agreement 83% > 85%
How have we used this measure to make a difference?
THE MEASURE National Emergency Department Target (NEAT)
Pledge 5: Delivering value for money
The WBHHS is committed to ensuring patients receive the care they need in clinically appropriate times. The NEAT measure is aimed at delivering on this commitment. While the benchmark was not quite reached, the majority of our patients have been seen and treated within the set four-hour target. Our teams are redesigning processes in patient flow to ensure we meet this target for all patients, with the knowledge that they will receive the best possible care.
Cameron DuffyNursing Director of Medical and Rehabilitation Services, Bundaberg Hospital
Chair of the WBHHS Recognition and Management of the Deteriorating Patient
“

Wide Bay Hospital & Health Service
Improving health, together 36
Why it’s important Clinical incidents that may have caused harm or resulted in the death of a patient, have a financial and personal cost. Health services, by reducing these types of clinical incidents, free up resources that can be either redirected or reinvested in other areas of healthcare. A New Zealand study published in 2001 estimated that clinical incidents, associated with harm, led to an average of 6.7 days of healthcare per eventxxii. The WBHHS Clinical Incident program is aimed at increasing the reporting of clinical incidents that have a potential for harm, so that the number of clinical incidents that cause harm can be kept to a minimum. Clinical incident management has made a significant difference as stated in Pledge 1 - Clinical Incident Rate. The focus on this over the past two decades has reduced the number of people harmed during health care. The reduction, if one assumes that WBHHS was equal to the average in 1992xxiii, is a staggering 89%. The potential wasted bed days saved through clinical incident management, in 2014/2015, if the rate of harm (16.6%) were the same as in 1992 is 75,060xxiii. The WBHHS would have needed an extra 205 beds in 2014/2015, if the rate of harm was still at the 1992 rate of 16.6%. How are we doing?
Source of Measure Benchmark WBHHS Performance 2014/15
QH PSU
Incidents associated with harm: < 1.8% 1.79%
SAC 1 Rate: +/- 0.04% 0.032%
SAC 2 Rate: +/- 0.21% 0.25%
SAC 3 (MH)Rate: +/- 1.5% 1.51%
Our goal for 2015/2016
Source of Measure Benchmark WBHHS Target 2015/16
QH PSU
Incidents associated with harm: < 1.8% 1.73%
SAC 1 Rate: +/- 0.04% 0.03%
SAC 2 Rate: +/- 0.21% 0.20%
SAC 3 (MH)Rate: +/- 1.5% 1.50%
THE MEASURE Clinical Incident Management
Pledge 5: Delivering value for money

Wide Bay Hospital & Health Service
Improving health, together 37
How have we used this measure to make a difference?
Incidents that occur during the delivery of healthcare can have serious and permanent consequences for our patients. Effective evidence-based care within a strong clinical governance framework creates the opportunity to deliver the highest quality of care. This will have the effect of minimising the occurrence of clinical incidents and ensuring patients remain safe in our services. The five pledges in the WBHHS strategy have set a framework for the delivery of safe and high-quality care by engaging with our community and building and empowering a strong clinical workforce through innovation and excellence. This will ensure the WBHHS delivers value for money for our community and a service that our community can be proud of and feel safe in.
Dr Pieter PikeExecutive Director of Clinical Governance
“

Wide Bay Hospital & Health Service
Improving health, together 38
References
i Australian Commission on Safety and Quality in Healthcare, 2012, Standard 1, ‘Governance for Safety and Quality in Health Service Organisations’
ii WBHHS Strategic Plan 2014-2017iii Wilson RM, Runciman WB et al (1995) Quality in Australian Health Care Study (1995) Medical Journal of Aus-
tralia 1995;163:458-71.iv Roughead, E., & Semple, S. Medication safety in acute care in Australia: where are we now? Part 1: a review
of the extent and causes of medication problems 2002-2008. Australia and New Zealand Health Policy. 2009: 6(1):18.
v Halfon P, Eggli Y, Van Melle G, Vagnair A. Risk of falls for hospitalized patients: a predictive model based on routinely available data. J Clin Epidemiol. 2001;54:1258–66. [PubMed]
vi Ash KL, MacLeod P, Clark LA. Case control study of falls in the hospital setting. J Gerontol Nurs. 1998;24:7–15. [PubMed].
vii Nursing Executive Centre, Safeguarding against Nursing Never Events: Best practices for preventing pressure ulcers and patient falls, The Advisory Board Company. (2009).
viii Wounds West Wound Prevalence Survey, 2011, State wide Overview Report, Perth, Western Australia.ix Ghosh R., ed; Clinical Audit for Doctors. Nottingham: Developmedica, 2009x Jarman B, Pieter D, van der Veen AA, et al. The hospital standardised mortality ratio: a powerful tool for Dutch
hospitals to assess their quality of care? Qual Saf Health Care 2010; 19: 9-13. <PubMed>xi Australian Commission on Safety and Quality in Health Care. Update. Issue 10, Mar 2010. Sydney:
ACSQHC, 2010. http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/C6E96E608654099 CCA257753001ECA1A/$File/Issue-10.pdf (accessed May 2011).
xii Jarman B, Gault S, Alves B, et al. Explaining differences in English hospital death rates using routinely collect-ed data. BMJ 1999;318:1515–20.
xiii Larson EL, and the Association for Professionals in Infection Control and Epidemiology 1992-1994 and 1994 APIC Guidelines Committee. APIC guideline for hand washing and hand antisepsis in healthcare settings. AMJ Infect Control 1995;23:251-69.
xiv Pittet D, Allegranzi B, Sax H, Dharan S, Pessca-Silva, Donaldson L, Boyce J. Evidence-based model for hand transmission during patient care and the role of improved practices. The Lancet Infectious Diseases 2006 Oct 6:641-652.
xv Australian Council on Healthcare Standards, 2012, Standard 13 ‘Workforce Planning and Management’xvi Porter, ME and Teisberg, EO. 2007 ‘How physicians can change the future of health care’, Journal of the Amer-
ican Medical Association, vol 297, no 10, pp 1103-1111xvii Grol, R and Grimshaw, J. 2003, ‘From best evidence to best practice: effective implementation of change in
patients care’, The Lancet, vol 362, no 9391, pp 1225-1230xviii Australian Institute of Health and Welfare, Australian hospital statistics 2005 06, AIHW, Canberra, p.47-48.
URL:http://www.aihw.gov.au/publications/index.cfm/title/10455#full_publication, accessed 13 February 2008. xix Australian Institute of Health and Welfare, Australia s health 2006, AIHW, Canberra, 2006, p. 374. xx Australian Government, 2009, Emergency Triage Education Kitxxi Hauck K, Street A. Do targets matter? A comparison of English and Welsh national health priorities. Health
Econ 2007; 16: 279-290.xxii Clinical leadership and clinical governance: a review of developments in New Zealand and Internationally
(2001) published by Clinical Leaders Associated of New Zealand Inc)xxiii Wilson RM, Runciman WB et al (1995) Quality in Australian Health Care Study (1995) Medical Journal of Aus-
tralia 1995;163:458-71