quality improvement overview plan - hull and east ... · kpi/measure baseline ... inspection...
TRANSCRIPT

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 1
Introduction
The purpose of this plan is to define, at a high level; the overall continuing quality improvement journey HEY is making and the improvement goals that the trust will work towards over the next 8‐12 months. The plan includes all of the MUST DO and SHOULD DO recommendations in the CQC Quality Reports and detailed plans are being developed for each project/work area. However, the plan is broader than those actions and includes longer‐term pieces of work that the trust is pursuing to improve overall quality and responsiveness across the organisation, for example in relation to Quality Accounts and our Sign Up to Safety Pledges.
The plan outlines the trust’s overall ambition to meets its vision of Great Staff, Great Care, Great Future. It is therefore not the intention that the improvement goals will all be achieved by March 16 but rather significant progress can be demonstrated against all of them. The plan includes a number of key milestones and these will be reported on at the monthly Operational Quality Committee. There are also milestones that partner organisations are responsible for and these too will be monitored. The milestone dates are all the end of the month unless a specific date is recorded. The Plan will be reviewed and refreshed at the end of the financial year.
A separate monthly progress report will be produced to demonstrate progress against milestones and improvement goals. The dates in the plan below will not change unless specifically agreed by the HEY Improvement Board.
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Safety
QIP01 Risk and Incident Management The aim of this project is to ensure there are effective systems and processes in place to ensure incidents and serious incidents are investigated in a timely manner and lessons are learnt and disseminated. Linked to a regulation breach in the HRI and Overall reports. Regulation 12 Safer Care and Treatment (12(2)(b) – doing all that is reasonably practicable to mitigate any such risks). This relates to not reviewing incidents in a timely manner and ensuring learning. Regulation 17(1) and (2) Good Governance incidents are acted upon and audited).
Commissioners and regulators report that the organisation has strong, well embedded systems and processes for risk management There is a clear link between corporate and operational risks with an effective feedback mechanism. Datix is being used effectively across the trust with feedback on risks and incidents being provided to staff
Risks reviewed on the risk register in line with Trust policy
Incidents investigated in line with Trust Policy SIs completed within framework timescales SI extension requests to commissioners made at least 2 weeks prior to completion deadline
NRLS 6 monthly reporting by rate of reporting (target is middle 50% of reporters)
43/56 high risks reviewed in 1 month 126/146 moderate risks reviewed in 3 months 24/27 low/very low risks reviewed in 6 months 29.44 incidents per 1000 bed days (NRLS Sep 2014) 42.7% (2014/15) Baseline to be established 15/16 Bottom 25% of reporters
Sign up to Safety and CQC inspection actions Individual QIP – e.g. learning lessons, governance, falls, pressure ulcers, deteriorating patient Link to cultural transformation programme TDA support to undertake review of governance arrangements
Director of Governance (Liz Thomas)
Head of Risk, Claims & Safety (Mark Green)
Threshold of incident investigations that take longer than 14 days agreed at Operational Quality Committee – Jul 15 Monthly performance reviews with Health Groups established and governance dashboard developed – Aug 15 Interim arrangements implemented to strengthen SI investigation and performance – Sept 15
New Serious Incident policy and procedures in place –Dec 15 RCA training to lead investigators commenced – Dec 15
The existing backlog in overdue SI actions addressed – Jan 16 The backlog in overdue incident investigations within the agreed threshold levels addressed – Jan 16 Audit of incident reporting undertaken (quality of investigations recorded on Datix – feedback to staff) – Mar 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 2
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Improved Trust Staff survey quarterly results on incident reporting (My Trust encourages me to report errors)
Improved National Staff Survey results in relation to incident reporting
73% (Aug 2015) Worst 20% of Trusts – Fairness and effectiveness of incident reporting procedures (3.41) and Percentage witnessing potentially harmful errors, near misses or incidents in the last month (38%)
Safety
QIP02 Learning Lessons The aim of this project is to improve learning from Serious Incidents and Never Events so that the organisation understands the root causes that contributed to those incidents and what improvements have been made as a result. This should be visible through the implementation of sustainable changes and improvements. Linked to a regulation breach in the HRI and Overall reports. Regulation 12 Safer Care and Treatment (12(2)(b) – doing all that is reasonably practicable to mitigate any such risks). This relates to not reviewing incidents in a timely manner and ensuring learning. R Regulation 17(1) and (2) Good Governance incidents are acted upon and audited).
Reduction of serious incidents with same theme (relative to the volume and complexity of activity undertaken) The Trust can evidence where changes in practice have been made as a result of claims, complaints, serious incidents etc Feedback confirms that staff receive information about learning
Reduction in the severity of incidents reported Number of overdue SI actions Number of overdue SI investigations Serious Incidents discussed at Health Group Governance meetings Monthly summary of completed Serious Incidents circulated by Risk team
8 deaths, 18 severe and 169 moderate incidents (NRLS Set 2014)
Number of overdue SI actions – 118 August 2015 12 overdue SI investigations (28.7.15) Not collected Not collected
Sign up to Safety / Quality Account QIP10 Pressure Ulcers QIP09 Falls QIP06 and 07 Deteriorating Patient QIP05 Medicines Management QIP27 and 28 Complaints Transformation
Chief Medical Officer (Kevin Phillips)
Nurse Director Lead (Karen Thirsk) Clinical Quality Director (Oliver Byass)
SI monthly report for the dissemination of learning developed – Aug 15 Lessons learnt working group established – Aug 15 Current Health Group processes for dissemination of completed SI investigations and learning mapped – Sept 15 Claims workshop held at specialty level – Sept 15
Analysis undertaken of actions from completed SI investigations ‐ since 1 April 2015‐ in order to identify key learning, trends and delivery – Nov 15 Process for aggregating learning from different sources developed (i.e. complaints, claims, PALS, PDSA cycle etc), drawing on best practice ‐ Nov 15 Systems for the dissemination of learning agreed – Nov 15 Identification of barriers (Board to ward) for disseminating lessons learnt–Nov 15 Learning Lessons newsletter
Lessons learned Intranet site reviewed and updated – Jan 16 Survey undertaken to determine whether staff are receiving feedback from adverse events – Feb 16 Audits undertaken which demonstrate changes in practice ‐ Mar 16 Learning lessons evidenced through re‐audits against key Serious Incidents – Mar 16 Serious Incidents reviewed and audit requirements determined for inclusion in the 16‐17 Audit Plan – Mar 16
Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 3
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
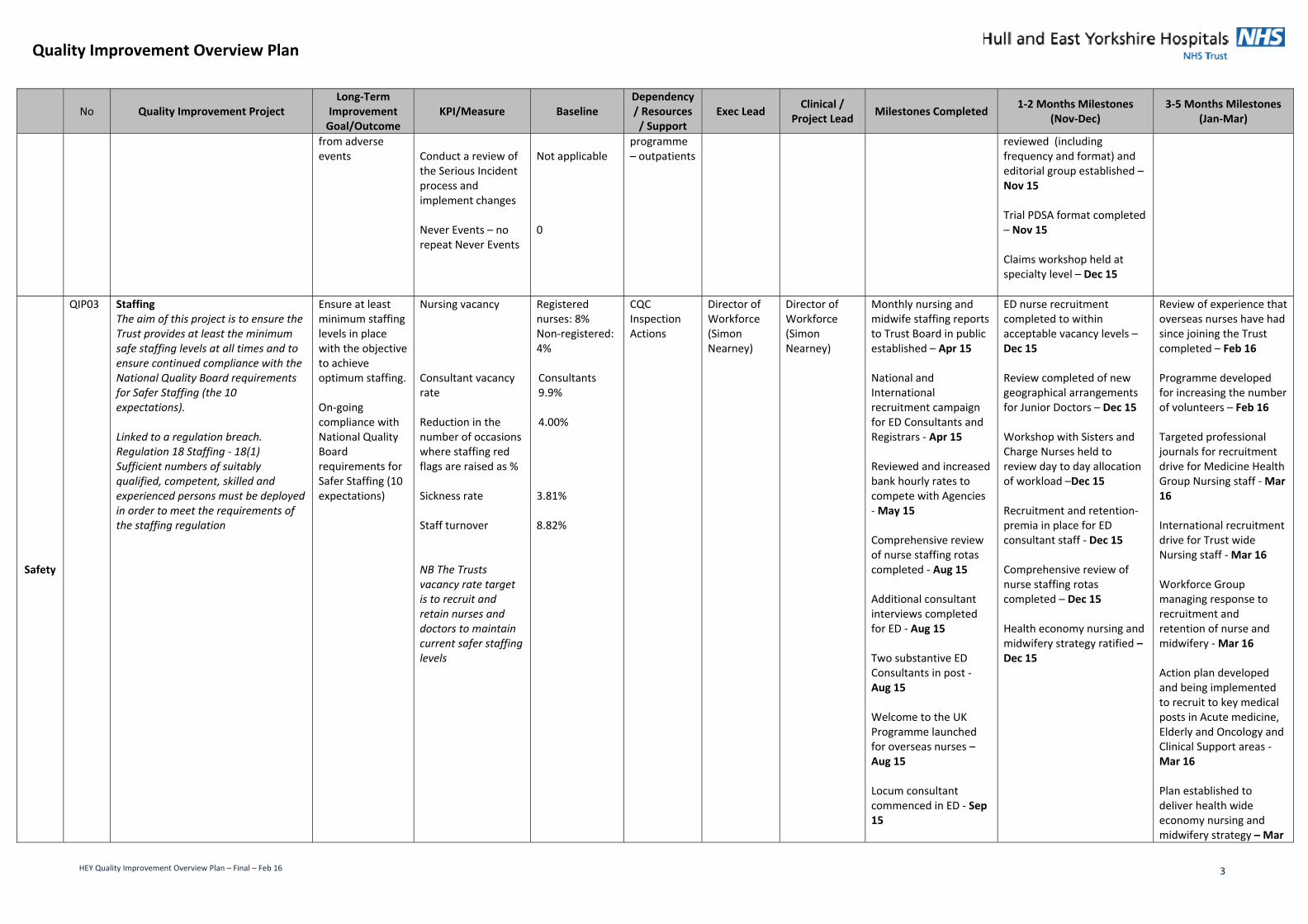
from adverse events
Conduct a review of the Serious Incident process and implement changes Never Events – no repeat Never Events
Not applicable 0
programme – outpatients
reviewed (including frequency and format) and editorial group established – Nov 15 Trial PDSA format completed – Nov 15 Claims workshop held at specialty level – Dec 15
Safety
QIP03 Staffing The aim of this project is to ensure the Trust provides at least the minimum safe staffing levels at all times and to ensure continued compliance with the National Quality Board requirements for Safer Staffing (the 10 expectations). Linked to a regulation breach. Regulation 18 Staffing ‐ 18(1) Sufficient numbers of suitably qualified, competent, skilled and experienced persons must be deployed in order to meet the requirements of the staffing regulation
Ensure at least minimum staffing levels in place with the objective to achieve optimum staffing. On‐going compliance with National Quality Board requirements for Safer Staffing (10 expectations)
Nursing vacancy Consultant vacancy rate Reduction in the number of occasions where staffing red flags are raised as % Sickness rate Staff turnover NB The Trusts vacancy rate target is to recruit and retain nurses and doctors to maintain current safer staffing levels
Registered nurses: 8% Non‐registered: 4% Consultants 9.9% 4.00% 3.81% 8.82%
CQC Inspection Actions
Director of Workforce (Simon Nearney)
Director of Workforce (Simon Nearney)
Monthly nursing and midwife staffing reports to Trust Board in public established – Apr 15 National and International recruitment campaign for ED Consultants and Registrars ‐ Apr 15 Reviewed and increased bank hourly rates to compete with Agencies ‐ May 15 Comprehensive review of nurse staffing rotas completed ‐ Aug 15 Additional consultant interviews completed for ED ‐ Aug 15 Two substantive ED Consultants in post ‐ Aug 15 Welcome to the UK Programme launched for overseas nurses – Aug 15 Locum consultant commenced in ED ‐ Sep 15
ED nurse recruitment completed to within acceptable vacancy levels – Dec 15 Review completed of new geographical arrangements for Junior Doctors – Dec 15 Workshop with Sisters and Charge Nurses held to review day to day allocation of workload –Dec 15 Recruitment and retention‐premia in place for ED consultant staff ‐ Dec 15 Comprehensive review of nurse staffing rotas completed – Dec 15 Health economy nursing and midwifery strategy ratified – Dec 15
Review of experience that overseas nurses have had since joining the Trust completed – Feb 16 Programme developed for increasing the number of volunteers – Feb 16 Targeted professional journals for recruitment drive for Medicine Health Group Nursing staff ‐ Mar 16 International recruitment drive for Trust wide Nursing staff ‐ Mar 16 Workforce Group managing response to recruitment and retention of nurse and midwifery ‐ Mar 16 Action plan developed and being implemented to recruit to key medical posts in Acute medicine, Elderly and Oncology and Clinical Support areas ‐ Mar 16 Plan established to deliver health wide economy nursing and midwifery strategy – Mar
Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 4
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
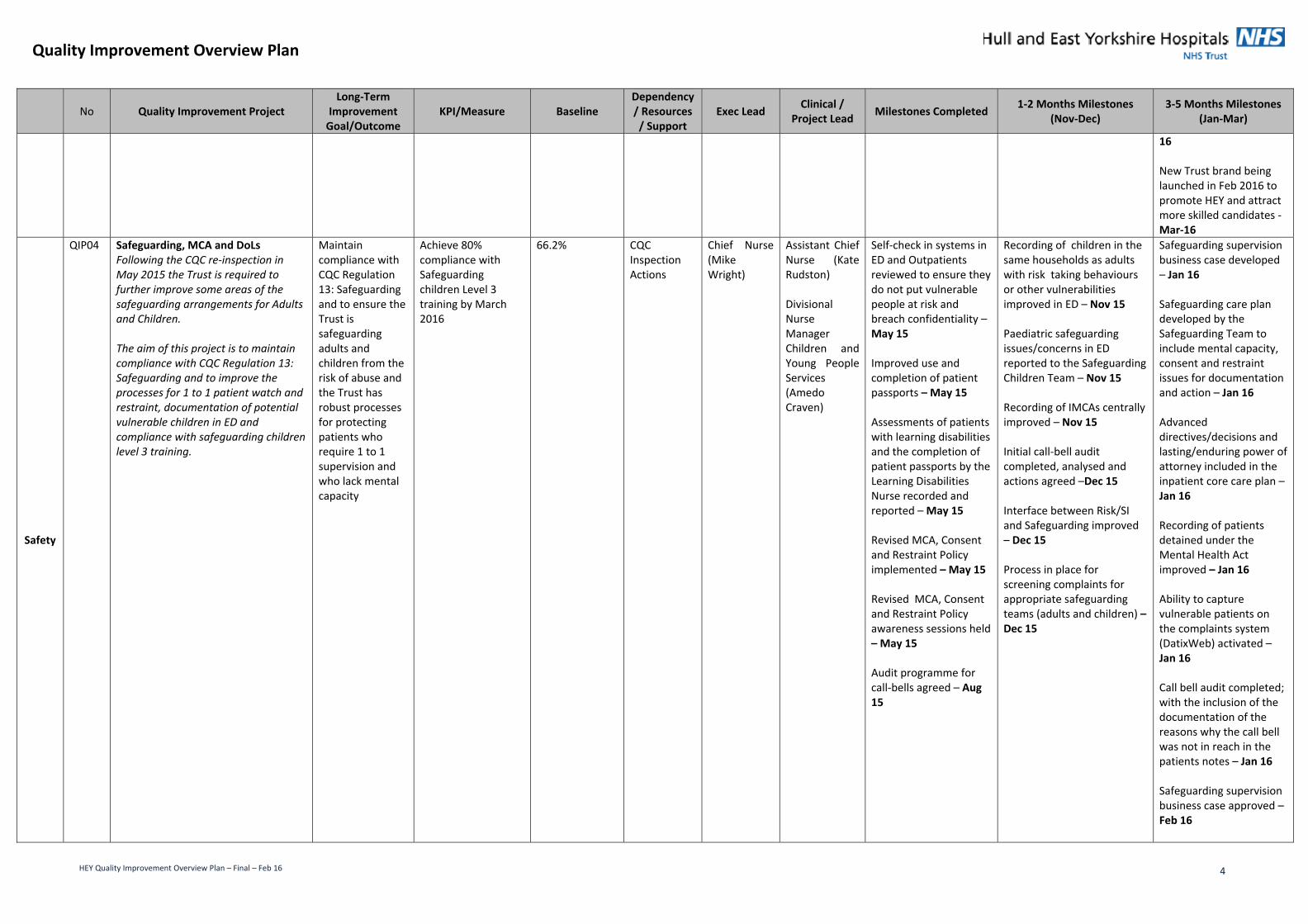
16 New Trust brand being launched in Feb 2016 to promote HEY and attract more skilled candidates ‐ Mar‐16
Safety
QIP04 Safeguarding, MCA and DoLs Following the CQC re‐inspection in May 2015 the Trust is required to further improve some areas of the safeguarding arrangements for Adults and Children. The aim of this project is to maintain compliance with CQC Regulation 13: Safeguarding and to improve the processes for 1 to 1 patient watch and restraint, documentation of potential vulnerable children in ED and compliance with safeguarding children level 3 training.
Maintain compliance with CQC Regulation 13: Safeguarding and to ensure the Trust is safeguarding adults and children from the risk of abuse and the Trust has robust processes for protecting patients who require 1 to 1 supervision and who lack mental capacity
Achieve 80% compliance with Safeguarding children Level 3 training by March 2016
66.2% CQC Inspection Actions
Chief Nurse (Mike Wright)
Assistant Chief Nurse (Kate Rudston) Divisional Nurse Manager Children and Young People Services (Amedo Craven)
Self‐check in systems in ED and Outpatients reviewed to ensure they do not put vulnerable people at risk and breach confidentiality – May 15 Improved use and completion of patient passports – May 15 Assessments of patients with learning disabilities and the completion of patient passports by the Learning Disabilities Nurse recorded and reported – May 15 Revised MCA, Consent and Restraint Policy implemented – May 15 Revised MCA, Consent and Restraint Policy awareness sessions held – May 15 Audit programme for call‐bells agreed – Aug 15
Recording of children in the same households as adults with risk taking behaviours or other vulnerabilities improved in ED – Nov 15 Paediatric safeguarding issues/concerns in ED reported to the Safeguarding Children Team – Nov 15 Recording of IMCAs centrally improved – Nov 15 Initial call‐bell audit completed, analysed and actions agreed –Dec 15 Interface between Risk/SI and Safeguarding improved – Dec 15 Process in place for screening complaints for appropriate safeguarding teams (adults and children) – Dec 15
Safeguarding supervision business case developed – Jan 16 Safeguarding care plan developed by the Safeguarding Team to include mental capacity, consent and restraint issues for documentation and action – Jan 16 Advanced directives/decisions and lasting/enduring power of attorney included in the inpatient core care plan – Jan 16 Recording of patients detained under the Mental Health Act improved – Jan 16 Ability to capture vulnerable patients on the complaints system (DatixWeb) activated – Jan 16 Call bell audit completed; with the inclusion of the documentation of the reasons why the call bell was not in reach in the patients notes – Jan 16 Safeguarding supervision business case approved – Feb 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 5
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Training provided in relation to screening complaints for appropriate safeguarding concerns – Feb 16 Safeguarding care plan implemented – Mar 16 Children ED cards assessed daily to ensure all safeguarding issues/concerns are identified, reported and actioned – Mar 16 Achieved 80% compliance with the Safeguarding Children Level 3 training – Mar 16 All relevant staff receive Safeguarding Level 3 training in ED – Mar 16 All named professionals for safeguarding children accessed Level 3 and 4 training as outlined in the intercollegiate document – Mar 16 Quarterly MCA audit completed – Mar 16 Quarterly MCA audit results analysed and reported to the Safeguarding Committee – Mar 16 Quarterly MCA audits actions implemented – Mar 16 Implementation of enhanced care teams for one to one / specialising in place (for patients with

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 6
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
dementia, falls risk, mental health needs, learning disabilities etc) – Mar 16 Restraint incident reporting improved – Mar 16 Safeguarding supervision post filled – Apr 16
Safety QIP05 Medicines Management This project covers improvement areas identified in the Quality Accounts/Sign up to Safety, CQC inspection from February 2014 and CQC re‐inspection in May 2015. The aims of this project are: To provide a multi‐disciplinary,
person‐centred approach to ensuring our patients receive the right medicines, the right dose at the right time. This will be supported by an accurate record of medications on admission to the hospital by ensuring medicines are reconciled within 24 hours of admission, which will remove the potential for harm and the delivery of a safe and effective medication process for our patients.
To improve patient safety by reducing the number of missed doses and improving safety on the use of specific high risk medications including anticoagulants, opioids, injectable sedatives and insulin.
To implement Aria electronic prescribing for 80% of chemotherapy prescriptions
To improve the storage, security, recording and administration of medicines on Medical wards
To ensure controlled drugs are stored appropriately and that records of the management of
Provide a multi‐disciplinary, person centred approach to ensuring that patients receive the right medicines, the right dose at the right time.
Achieve 85% of patients reconciliation of medicines on admission to hospital Achieve 75% of patients reconciliation of medicines on admission to hospital within 24 hours Reduce by 20% ‐ Number of patients who have missed a dose of high risk medicines: anticoagulants, opioids, anti‐infective and insulin Achieve 80% of chemotherapy prescriptions prescribed by Aria electronic system.
70% 35% Not collected Not collected
Quality Accounts / Sign up to Safety and CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Chief Pharmacist (David Corral)
Baseline information for medicines reconciliation 2014‐15 collected for Quality Accounts– Aug 15 Performance data for medicines reconciliation collected – Aug 15 Drug Policy revised and approved – Sept 15 Prescribing assessment implemented for FY1 Doctors – Oct 15
Communication campaign launched for: revised Drug Policy,
including safe and secure handling, recording and administration of medicines – Nov 15
appropriate storage and record management of controlled drugs within Emergency Department & Children’s Services – Nov 15
recording and monitoring daily medication fridge temperatures within the Emergency Department – Nov 15
Pharmacy recruitment business plan delivered – Nov 15 New Pharmacists and Medicine Management Technicians trained to use the summary care record for medicine reconciliation – Nov 15 3 monthly CD checks to monitor appropriate storage and accurate record management of controlled drugs within the Emergency Department implemented ‐
Lorenzo IDS pilot completed – Jan 16 Pilot of Pharmacy assisted Drug rounds, including pharmacists – Jan 16 Plan in place to deliver training requirements from the medicine management TNA – Mar 16 Delivered Medication Safety Thermometer CQUIN – Mar 16 Pilot of online ’Script’ for FY1 Doctor training ‐ Mar 16 Safe storage & security of medicines audited– Mar 16 New internal pharmacy inspection process implemented and monitored – Mar 16 Decision on whether to return to 6 monthly controlled drug checks within the Emergency Department – Apr‐16 Decision on whether to

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 7
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
controlled drugs are accurately maintained and audited within A&E and Children Services
Record and monitor daily temperatures of fridges used for storage of medicines within A&E
Linked to a regulation breach. Regulation 12 Safer Care and Treatment – 12(2)(G) – the proper and safe management of medicines.
Nov 15 3 monthly CD checks to monitor appropriate storage and accurate record management of controlled drugs within the Children’s Services audited – Nov 15 Pharmacy support to the Emergency Department increased to support controlled drugs processes and fridge monitoring – Nov 15 Pharmacy support to Acorn ward, Paediatrics, and A&E – Nov 15 Medicine management TNA Completed –Dec 15 Internal CQC medicines management inspections ‐ process updated –Dec 15 Baseline information for 2014/15 collected for the missed doses indicators for Quality Accounts – Dec 15
return to 6 monthly controlled drug checks within Children’s Services – Apr‐16 All wards inspected via 3Gs assessment for medicine management – Apr 16 Medicine Management clinical audit plan delivered – Apr 16
Safety QIP06 Deteriorating Patient (Adult) This was a project in the 2014‐15 Quality Accounts that did not meet all of its targets. DNACPR has also been raised as an issue by the CQC in previous inspection. A number of Serious Incidents during 2014‐15 and 2015‐16 identified the deteriorating patient as an issue. The aim of this project is to ensure early identification of a patient’s deterioration through the use of observations to identify which patients require end of life support and to ensure end of life care plans are documented and include a Do Not
Ensure early identification of a patient’s deterioration.
Achieve 80% of correct completion of the DNACPR orders on the documentation of discussions with the patient and/or their relatives including best interest discussions 95% of completed observations (NEWS) and actioned appropriately
70% 95%
Quality Accounts and Sign up to Safety QIP02 Learning Lessons
Chief Medical Officer (Kevin Phillips)
Clinical Director for Quality (Alex Oboh) Neil Jennison (Resuscitation Manager) Vicky Kirkby (Teacher Practitioner HDU)
AMU project outcome and process measures identified and baselines established – Jul 15 Baseline information for 2014‐15 collected – Aug 15 Performance data for April – Aug 15 collated – Aug 15 Completed Improvement Academy (IA) Achieving Behaviour Change (ABC) Survey by
Pilot of E‐Obs evaluated – Nov 15 Completed IA’s Teamwork and Safety Climate survey with the staff in AMU – Nov 15 Completed SI themes with failure to escalate deteriorating patients analysed and further actions and learning identified – Nov 15 Re‐established AMU working group – Nov 15
Analysed AMU ABC Nurses survey results to identify barriers to behaviour change – Jan 16 E‐Obs piloted and evaluated for wards C14 and C15 – Jan 16 Test interventions identified in the AMU Intervention Strategy ‐ Feb 16 Multidisciplinary Safety Huddles in AMU

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 8
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Attempt Cardio Pulmonary Resuscitation (DNACPR) order form to avoid inappropriate attempts at resuscitation.
Drs working on AMU to identify barriers to the target behaviours: ‘considering and documenting an escalation plan / ceiling of care of patients with NEWS >5’ – Jul 15 Analysed AMU ABC Drs survey results to identify barriers to behaviour change – Aug 15
Funding options for further roll out of the E‐Obs reviewed and next steps agreed – Dec 15 Completed Improvement Academy (IA) Achieving Behaviour Change (ABC) Survey by Nurses working on AMU to identify barriers to the target behaviour: ‘completing observations on time and in full’ – Dec 15 Mapping exercise completed and develop an intervention strategy targeting the barriers identified from the AMU ABC Surveys – Dec 15 Process for identification and escalation of deteriorating patient concerns from a Serious Incident agreed and implemented – Dec 15
Implemented – Feb 16 Continued measurement of observations in a timely manner and in full, documentation of treatment and escalation plans and escalation in AMU – Feb 16 Continued 95% compliance and above with completion of observations (NEWS) and action appropriately – Mar 16 80% of DNACPR orders on the documentation of discussions with the patient and/or their relatives including best interest decisions achieved – Mar 16 Active involvement in the national working groups consultation process to develop an Emergency Care and Treatment plan – Mar 16 Resuscitation Service to review all SIs declared to identify any deteriorating patient concerns and identify learning for dissemination – Mar 16 Monthly spot check of 10 NEWS forms by the Outreach Team – Mar 16 Snapshot audit of 20 patients transferred from EAU/AMU to identify if a treatment and escalation plan was completed

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 9
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
before transfer completed – Mar 16 To ensure all Doctors complete the DNACPR e‐learning package as part of induction or as catch up for those already working in the Trust – Mar 16
Safety QIP07 Deteriorating Patient (Children) The aim of this priority is to ensure early identification of a child’s deterioration through the use of observations and the Paediatric Advance Warning System (PAWS) to identify the requirement of prompt intervention or treatment and to prevent avoidable deterioration.
Ensure early identification of a child’s deterioration
Infant Mortality to achieve a value of 3.8 or below per 1,000 births 95% compliance of PAWS
4.0 Not collected
Quality Accounts and Sign up to Safety
Chief Nurse (Mike Wright)
Divisional Nurse Manager for Children & Young People (Amedo Craven)
Performance data for April – Aug 15 collated – Aug 15 PAW audit approved – Sept 15
Baseline information for 2014‐15 collected – Dec 15 PAW audit completed – Dec 15
Residual actions from audit commenced – Jan 16 Performance data collected – Mar 16 PAW re‐audit completed ‐ Apr 16
Safety QIP08 Infection Control The aim of this project is to ensure compliance with the updated Health & Social Act (2008): code of practice on the prevention and control of infections and related guidance (2015). Linked to a regulation breach. Regulation 12 Safer Care and Treatment – 12(2)(H) assessing the risk of, and preventing, detecting and controlling the spread of infections, including those that are healthcare associated.
Ensure the Organisations compliance with the updated Health & Social Act (2008): code of practice on the prevention and control of infections and related guidance (2015).
85% of wards with a good rating for infection control measured by the 3Gs audits 95% of staff compliant with Hand Hygiene assessments
13% 72%
CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Director of Infection Prevention & Control (Dr Peter Moss) Infection Control Consultant (Dr Rolf Meigh) Lead Nurse Infection Prevention & Control (Greta Johnson)
Annual programme of 3Gs inspections commenced – Apr 15 Agreement of milestones and key areas of focus for Infection Control in the Trust – Aug 15 Lead Nurse Infection Prevention & Control appointed – Aug 15 Neonatal IPC review completed and actions agreed – Aug 15 Review of IPC rates compared to peers completed – Aug 15 Replacement of ‘point of care’ dispensers with individual staff ‘tottles’ in elderly and Gastro care areas– Sept 15 Review existing
External review of theatres for IPC completed by TDA completed and actions agreed – Nov 15 Trust wide roll out and display of Five Moments posters and key message regarding Bare below the Elbows ‐ Nov‐15 Annual compliance audit of identified areas by trust hand hygiene product supplier completed ‐ Nov‐15 Hand hygiene induction training for medical starters at the Trust completed ‐ Nov‐15 Commenced liaison with wards that scored inadequate or requires improvement on 3Gs audits – Nov 15
Trialled an audit tool in Oncology to support the 3Gs audit to be undertaken on a monthly basis ‐ Jan‐16 Competency framework/ assurance of staff knowledge and training on Five Moments hand hygiene reviewed ‐ Jan‐16 Other options and systems for assurance of hand hygiene compliance scoped ‐ Feb‐16 Reviewed system of hand hygiene compliance reports and renewed license until Mar 16 ‐ Feb‐16 IPCT monitored all action plans from inadequate / requiring improvement rated wards and theatres ‐ Mar‐16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 10
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
provision in paediatric areas as best practice (already utilising individual staff ‘tottles’) – Sept 15 Review of existing provision of lockable wall mounted dispensers and lockable versions for notes and drug trollies in elderly care areas and gastro – Sept 15
ED processes reviewed for the cleaning of the environment and patient equipment including cleaning checklists with continued use ‘I am clean’ sticker ‐ Mar‐16 Actions identified from ED cleaning of the environment and patient equipment process review and implemented ‐ Mar‐16 ED IPC 3G Audits completed and disseminated to relevant Health Group for action ‐ Mar‐16 Unannounced quarterly visits to Emergency department completed ‐ Mar‐16 Actions identified from ED quarterly visits and disseminated ‐ Mar‐16 Five Moments hand hygiene learning event which includes IPCT link practitioners and leading experts on hand hygiene compliance supported by Trust hand hygiene product supplier ‐ Mar‐16 IPCT monitored all action plans from inadequate / requiring improvement rated wards and theatres ‐ Mar‐16 CHH and HRI Theatre processes reviewed for
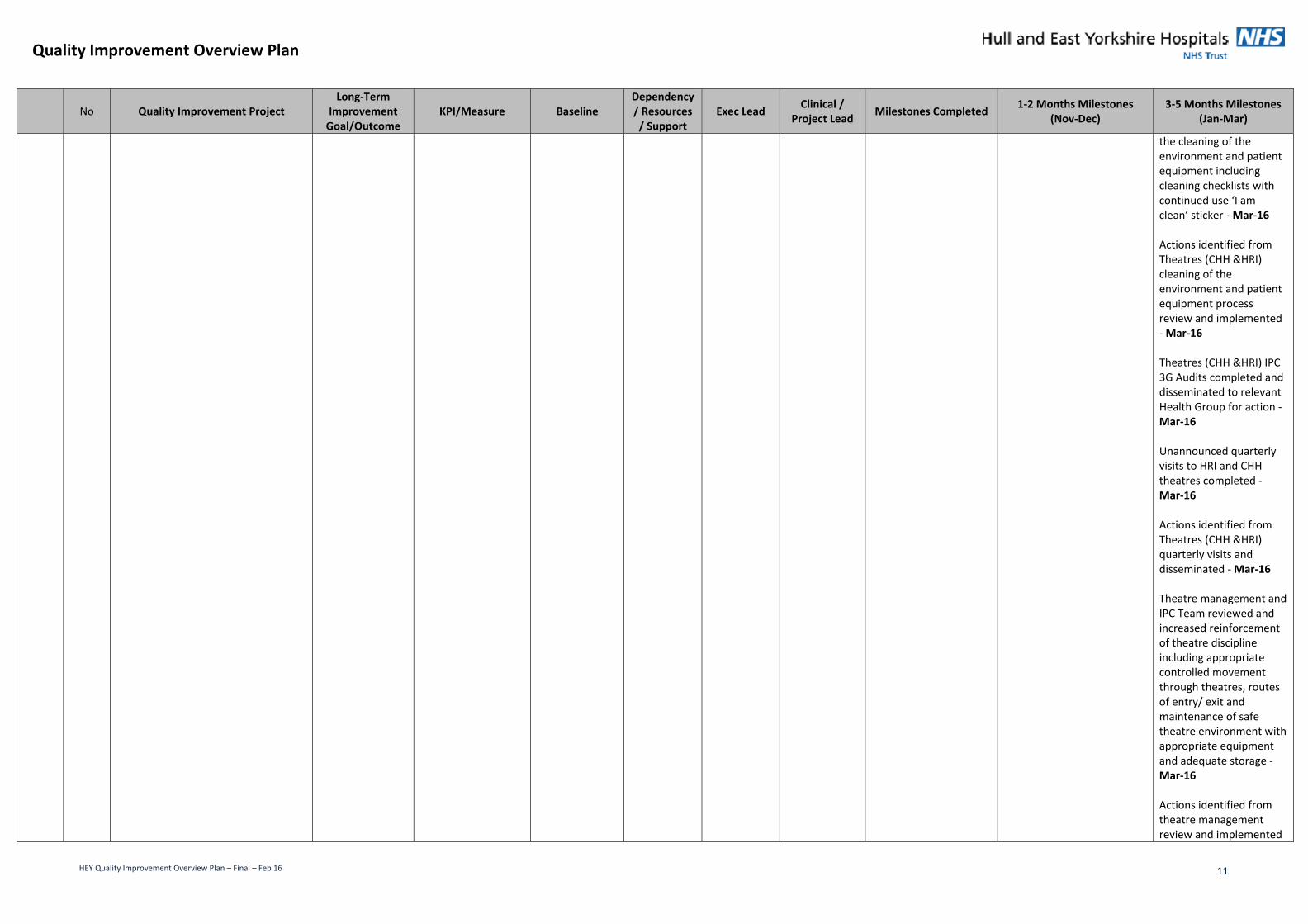
Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 11
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
the cleaning of the environment and patient equipment including cleaning checklists with continued use ‘I am clean’ sticker ‐ Mar‐16 Actions identified from Theatres (CHH &HRI) cleaning of the environment and patient equipment process review and implemented ‐ Mar‐16 Theatres (CHH &HRI) IPC 3G Audits completed and disseminated to relevant Health Group for action ‐ Mar‐16 Unannounced quarterly visits to HRI and CHH theatres completed ‐ Mar‐16 Actions identified from Theatres (CHH &HRI) quarterly visits and disseminated ‐ Mar‐16 Theatre management and IPC Team reviewed and increased reinforcement of theatre discipline including appropriate controlled movement through theatres, routes of entry/ exit and maintenance of safe theatre environment with appropriate equipment and adequate storage ‐ Mar‐16 Actions identified from theatre management review and implemented

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 12
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
‐ Mar‐16 Safety QIP09
Falls The aim of this project is to reduce the number of falls and the level of harm caused from falls by undertaking falls improvement work to understand the root causes of falls and to implement prevention measures to raise awareness of falls and improve the assessment of risk.
Eliminate all avoidable falls
Falls with harm below England average 25% reduction in the number of avoidable patient falls per 1000 bed days 40% reduction in the number of avoidable falls rated moderate or above Reduce the number of SIs resulting in fractured neck of femur or other injury
Below England average 6.94 per 1,000 bed days in 14/15. Number of falls moderate or above in 14/15 = 78 SI = 31 2014/15
Sign up to Safety and Quality Accounts
Chief Nurse (Mike Wright)
Chair of Falls Committee (Rosie Hoyle)
Re‐launched staying safe in hospital leaflet – Apr 15 Revised documentation and assessment tool introduced – July 15 Falls safety huddles started every day on Ward 70 as pilot site – Aug 15 Improvement Academy teamwork / safety culture survey completed on w80 and analysis and feedback given – Sept 15 Review of Improvement Academy project on Ward 70 completed – Sept 15
Fall project on Ward 80 commenced –Nov 15 Fall project on Ward H12 commenced – Nov 15 Focus group undertaken on Ward 70 on barriers and evidence based interventions – Nov 15 Residual actions on Ward 70 implemented – Nov 15 Review of benefits of 1‐2‐1 care and alternative interventions for high risk fallers completed – Nov 15 Sensory alarms implemented within wards with the highest falls risk – Nov 15 Trust wide Falls Implementation Plan commenced – Nov 15 Safety Huddle coaches (first tranche)identified – Nov 15 Falls project group established – Nov 15 Falls safety huddles completed every day on Ward 70 – Nov 15 Audit of Safety Huddles on Ward 70 completed – Dec 15 New e‐learning package developed – Dec 15
Visual alert systems piloted (yellow wrist bands) – Feb 16 Recommendations following review of Ward 80 completed – Mar 16 Trust wide Falls Implementation Plan completed – May 16
Safety QIP10 Pressure Ulcers The aim of this project is to reduce the number of patients who acquire avoidable hospital acquired grade 3, 4 or unstageable pressure ulcers. To
Zero incidence of avoidable Hospital Acquired pressure ulcers
Number of avoidable pressure ulcers Number of avoidable Hospital acquired
339 1
Sign up to Safety and Quality Accounts
Chief Nurse (Mike Wright)
Tissue Viability Matron (Angie Oswald and Karen Harrison)
Baseline information for 2014‐15 collected – Aug 15 Performance data for
Audit completed of skin care bundle – Dec 15 Secondment role (6 months) for Band 5 established into
Recommendations from audits and SIs implemented – Jan 16 Tested lessons learnt

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 13
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
ensure the appropriate risk assessments are undertaken to identify patients who are at risk of developing pressure ulcers and the implementation of the Skin Care Bundle.
Grade 3 Pressure Ulcers Number of avoidable Hospital acquired unstageable Pressure Ulcers Improve compliance with Skin Care Bundle
34 Not collected
April – Aug 15 collated – Aug 15 Formal communication issued to the Trust from Chief Nurse on expectations for Skin Care – Sept 15 Video Conference held on actions / issues to be addressed – Sept 15 Tissue Viability Link Nurse meeting held on actions / issues to be addressed – Sept 15
the Tissue viability Service –Dec 15 Re‐launch of skin care bundle campaign – Dec 15 Review completed on “Stop the Pressure” at East Midlands – Dec 15 Serious Incident review of pressure ulcers completed – Dec 15 Weekly performance returns established – Dec 15 Future reporting arrangements agreed – Dec 15
theory by re‐visiting areas with previous pressure ulcer serious incident to gain assurance ‐ Jan 16 Bespoke bedside assessment tool developed – Mar 16
Safety QIP11 Maternity The Trust is not in line with the National birth to Midwife ratio of 1:28 and the RCOG 'Setting standards to improve women's health' Good Practice No10 January 2010 of 168 Consultant Hours presence on the labour ward and is required to continue to work to achieve these staffing establishments. The Trust is currently rated as red on national score card as 1:32 ratio and the CQC have identified both of these areas as ‘should do’ areas for improvement following the May 2015 re‐inspection. The aim of this project is to monitor Midwifery and Consultant staffing establishments and to undertake a review against the Kirkup Morecombe Bay report to ensure the Maternity Services provided are safe and lessons are learned from external reviews.
Suitable Midwifery and Consultant staffing levels Provide assurance that the Maternity Service is safe and any lessons to learn are implemented from external reviews
Continue to work towards achieving the National Birth to Midwife ratio of 1:28 Continue to work towards achieving the RCOG 'Setting standards to improve women's health' Good Practice No10 January 2010 of 168 Consultant Hours presence on the labour ward Undertake a self‐assessment against the Morecombe Bay report and provide assurance that the Maternity Service provided at HEYHT is safe
1:32 101 Not collected, review to be undertaken during 15/16
CQC Inspection Actions
Chief Nurse (Mike Wright)
FWH Nurse Director (Karen Thirsk) FWH Medical Director (Colin Vize)
First maternal death external review completed – Jan 15 Medical Cover Labour Ward audit approved – May 15 Medical Cover Labour Ward audit completed – May 15 Medical staff reminded to sign in at the beginning of every shift – May 15 3WTE Consultant Obstetricians recruited – Jun 15 Increased consultant hours on Labour Ward achieved – Jun 15 Self‐assessment against the 44 Morecombe Bay recommendations
Re‐audit of Medical Cover on Labour Ward completed – Nov 15 Six monthly review of midwifery staffing establishment completed – Nov 15 Maternal death action plan implemented ‐ Dec 15 Quarterly review of actions implemented from the Maternity Summit completed – Dec 15
Learning lessons from incidents, complaints and PALS, Serious Incidents ,external reviews of the service demonstrated and evidenced – Mar 16 Quarterly review of actions implemented from the Maternity Summit completed – Mar 16 Annual review of midwifery and consultant staffing establishment completed – May 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 14
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
detailed in the Kirkup report and the RCOG and RCM responses completed – Jul 15 Self‐assessment against the 44 Morecombe Bay recommendations presented for assurance that the service is safe – Jul 15 Second maternal death external review completed – Sept 15 Maternity safety summit held and next steps agreed – Oct 15 5 task and finish groups established following maternity safety summit – Oct 15
Safety QIP12 Children and Young People with Mental Health needs and CAMHS Following the February 2014 and the May 2015 CQC inspections the Trust is required to improve its mental health support for Children and Young People within the Children’s Emergency Department and on the 13th floor. The aim of this project is to improve access to the local Child and Adolescent Mental Health Services (CAMHS) for Children and Young People within the Children’s Emergency Department and to improve the facilities on the 13th floor and support provided to the vulnerable Children and Young People admitted. Linked to a regulation breach. Regulation 12 Safer Care and Treatment – 12(2)(A) – assessing the risks to health and safety of service
Accessible, responsive and safe service for Children and Young People with mental health needs
Achieve 100% completion of all milestones within the agreed timescales Compliance with the quarterly Health and Safety Audits ‐ Anti Ligature Risk Assessment Implementation of the Individual Risk Assessments for Children and Young People at risk of self‐harm
Not collected Not collected Not collected
CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Divisional Nurse Manager Children and Young People Services (Amedo Craven) Matron ED (Helen Hudson)
Pilot of the mental health teams available in the Emergency Department on weekend to ensure rapid access completed – Jun 15 Compliance with HBN 23: Hospital Accommodation for Children and Young People in relation to ligature risk confirmed to the CQC – Aug 15 Joint self‐assessment by HEYHT and CAMHS on the facilities on the 13th floor including the ‘Green Room’ for ligature points completed – Aug 15
Individual self‐harm risk assessment to be undertaken on all children and young people with mental health illness to determine their risk of self‐harm and care plans developed – Nov 15 CAMHS risk added to the risk register – Nov 15 Out of hours process for accessing mental health support for ED developed by CAMHS – Dec 15 Business case to increase the mental health provision in the Emergency Department developed –Dec 15 Individual self‐harm risk assessments implemented –
Options appraisal for the facilities for children and young people with mental health needs completed and risks appropriately managed – Jan 16 Anti‐ligature risk assessment tool implemented – Jan 16 Audit of the individual self‐harm risk assessments completed – Feb 16 Baseline of compliance against the individual self‐harm risk assessments established – Feb 16 Mental health training

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 15
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
users of receiving the care or treatment.
Anti‐ligature risk assessment tool developed using CAMHS template – Oct 15
Dec 15
provided by CAMHS arranged – Mar 16 Residual actions from the joint self‐assessment implemented – Mar 16 Staff trained to offer advice and support to vulnerable children and young people who may pose a threat to themselves who are admitted – Mar 16 Baseline health and safety audit against the anti‐ligature risk assessment tool completed – Mar 16
Safety QIP13 Environment (Theatres and General Clinical Areas) The aim of this project is to remedy the immediate issues identified during the CQC inspection in May 2015 and to ensure the Theatres that are fit for purpose to meet all legislative requirements. Linked to a regulation breach. Regulation 12 Safer Care and Treatment – 12(2)(H) – assessing the risk of, and preventing, detecting and controlling the spread of infections, including those that are healthcare associated.
Theatres that are fit for purpose to meet all legislative requirements
Achieve 100% delivery of all milestones within the agreed timescales
Not collected
CQC Inspection Actions QIP08 Infection Control
Director of Facilities (Duncan Taylor)
Project Manager Capital Development (Mark Porteous)
HRI main theatres circulation areas loose plaster removed, walls repaired, bare wood sealed – May 15 Condition survey of all circulation areas completed – Aug 15 Infection control wash hand basins installed in department entrance – Aug 15 Two sets of new doors installed in corridor for trial – Aug 15 Works designed / tendered for corridor protection works and new doors – Aug 15 Mock up designs produced for new Impact resistant walling system – Aug 15
Protection works to disposal hold completed –Nov 15 Full detailed survey of all 39 operating theatres undertaken by Estates Team – Nov 15 Detailed progress of maintenance works / environmental upgrade to be issued / approved by Surgery Health Group and Infection Control Team – Nov 15 Works to create new recovery in Women & Children’s Hospital commenced by PFI contractors – Nov 15 New entrance design proposals approved – Nov 15 Theatre 5 in Women & Children’s Hospital in use – Dec 15
New HRI theatre reception completed – Feb 16 HRI theatre recovery, improvements to storage, lights, decoration and art work complete – Feb 16 11 theatres (five at HRI and six at CHH) redecorated and full maintenance undertaken including ventilation cleaning and validating – Mar 16 All damaged flooring in corridors heading up to theatres to be repaired – Mar 16 Detailed process for remaining theatres at HR/CHH progressed for April 2016 to March 2017 – Mar 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 16
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Main Theatres Clean corridors / ceilings ,walls and doors works complete– Dec 15 Theatre 4 environment upgrade and maintenance , ventilation clean / validate complete – Dec 15 Main Theatres Dirty Corridor in main theatres upgraded with new doors – Dec 15
Safety QIP14 VTE The aim of this project is to continue to achieve the 95% of patients assessed for VTE within 24 hours of admission.
Continue to achieve the 95% of patients assessed for VTE within 24 hours of admission
95% compliance with the VTE Risk Assessment 0 VTE Serious Incidents
95.39% 4 VTE SIs in 14/15
Quality Accounts and Sign up to Safety
Chief Medical Officer (Kevin Phillips)
Deputy Medical Director, Surgery (Dr Ahmed Saleh)
Revised Orthopaedic procedures implemented ‐ June 15 VTE risk assessments implemented in the Ambulatory Care Unit and the Medical Assessment Unit – July 15 Baseline information for 2014/15 collected for the indicators – July 15 Performance data collected for April to August – Aug 15
Senior Doctor completion of VTE e‐learning increased –Dec 15 VTE quality accounts audit completed – Dec 15 The option of a traffic light system for VTE risk assessments on Cayder Board explored – Dec 15
Quarterly Safety Thermometer audits completed – Mar 16 Completed RCAs following the quarterly Safety Thermometer Audits and lessons learned identified – Mar 16 No VTE SIs reported – Mar 16 Achieved 95% compliance with the completion of the VTE risk assessments – Mar 16 Electronic VTE risk assessment introduced – Mar 16 Electronic listing of patients VTE status implemented on all wards – Mar 16 VTE e‐module to be mandatory on 247 for Senior Doctors – Mar 16 VTE ‘short form’ on Lorenzo removed and

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 17
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
staff continue to complete the VTE full risk assessment – Mar 16 Shift handover documentation reviewed to include the completion of the VTE risk assessment – Mar 16 ‘Stop’ option in Lorenzo explored to identify if a ‘stop’ process can be set up on Lorenzo which does not allow staff to continue further into the patients record until the VTE risk assessment has been completed – Mar 16
Safety QIP15 Sepsis The aim of this project is to raise awareness of the Sepsis Six, implement the Sepsis care bundle and reduce death from Sepsis. In addition approximately 50% of patients coded with sepsis attending ED do not have it. The project intends to improve coding of this condition.
The Sepsis Six care bundle implemented and patients appropriately assessed for Sepsis when attending ED and improved coding of diagnosis and death of Sepsis
90% of patients assessed for Sepsis in the ED Increase the number of patients correctly coded with sepsis Reduce the number of patients dying from avoidable septic shock
0 Not collected Not collected
Quality Accounts and CQC Mortality Outlier Alerts
Chief Medical Officer (Kevin Phillips)
Director of Infection Prevention & Control (Dr Peter Moss)
Appointment of Sepsis Nurse to 1 year secondment – Sept 15 Training delivered to the two acute surgical admission wards at HRI (6th Floor) – Sept 15 Training delivered to Paediatrics Staff – Sept 15 Training delivered to ED and AAU staff – Sept 15 Baseline audit on the implementation of the Sepsis care bundle completed – Sept 15 Further audit arrangements agreed following completion of the baseline – Sept 15 Target % determined for the increase in patients coded with
Coding exercise following Dr Foster alert completed – Nov 15 Training completed in HDU on Sepsis Bundle – Nov 15 Audit of Sepsis Bundle completed – Dec 15 Audit of Sepsis Sticker completed – Dec 15
90% of patients assessed for sepsis in the ED – Jan 16 Process for multi‐disciplinary meetings established – Jan 16 Additional audit questions included on place of residence trialled – Jan 16 Monthly multi‐disciplinary meetings commenced – Feb 16 Sepsis stickers to be in place in all areas of the Trust – Feb 16 Route cause analysis commenced on patients that die from severe sepsis / septic shock – Feb 16 Sepsis link nurse on every ward – Apr 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 18
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
sepsis – Sept 15 Sepsis assessment sticker implemented in ED – Sept 15
Sepsis intranet site developed – Apr 16
Safety QIP16 Equipment (Resuscitation) The aim of this project is to ensure that all resuscitation equipment trolleys are completed in accordance with the Trusts policy Linked to a regulation breach. Regulation 12 Safe care and treatment – 12(2)(E) ensuring that equipment is used by the service provider for providing care or treatment to a service user is safe for such use and is used in a safe way.
To ensure that all resuscitation equipment is checked, safe and fit for purpose.
Achieve 95% compliance of daily checks completed Achieve 95% compliance with the monthly checks completed
58% 94%
CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Resuscitation Manger (Neil Jennison)
Baseline audit of resuscitation equipment checks completed by the Resuscitation Department – Jul 15
Audit of resuscitation equipment checks completed by the Audit Team for April to October 15 – Nov 15 Actions and next steps from the audit completed by the Clinical Audit Team identified and disseminated within wards, Divisional Managers and Resuscitation Committee – Nov 15 Actions completed in all wards – Dec 15
Continued audit of the resuscitation equipment checks completed by the Audit Team – Jan 16 Re‐audit of resuscitation equipment checks by the Resuscitation Department – Feb 16 Actions and next steps from the audit completed by the Resuscitation Department identified and disseminated within wards, Divisional Managers and Resuscitation Committee – Mar 16 Actions completed in all wards – Apr 16
Safety QIP17 Hysteroscopy Consent This was identified as a ‘must do’ area of improvement following the May 15 CQC re‐inspection. The aim of this project is to implement patient consent for women undergoing a hysteroscopy and adherence to the WHO checklist within outpatients. Linked to a regulation breach. Regulation 11 Need for Consent ‐ 11 (1) – care and treatment of service users must only be provided with the consent of the relevant person.
Appropriate consent obtained prior to procedure
100% compliance with the Trust Consent procedures (Hysteroscopy Consent form) 100% compliance with completion of the WHO compliance for Hysteroscopy procedures)
100% 98.24% (baseline audit completed between 27 May and 9 June 2015)
CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
FWH Health Group Medical Director (Mr Colin Vize)
A patient consent form for a Hysteroscopy developed and distributed – May 15 Official printed Hysteroscopy consent forms ordered – May 15 Printed Hysteroscopy consent forms available in relevant areas – May 15 Monitoring arrangements agreed – May 15 Communication campaign of the new Hysteroscopy consent
Re‐audit of written consent and WHO checklist completed – Dec 15 Re‐audit of written consent and WHO checklist results analysed and further actions identified ‐ Dec 15 Audit results and performance presented to the Family and Women’s Health Group Governance Committee – Dec 15 100% compliance with the Hysteroscopy consent form achieved – Dec 15 100% compliance with the WHO checklist achieved –
Actions from re‐audit implemented including communication of the formal consent procedure – Jan 16 Review and update the Hysteroscopy consent patient information leaflet – Feb 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 19
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
form and the completion of the WHO checklist completed – June 15 Audit of written consent and WHO checklist completed in Hysteroscopy– June 15 Hysteroscopy consent and WHO checklist targets and baselines identified – June 15 Hysteroscopy consent implemented – June 15 WHO checklist for Hysteroscopy procedures implemented – June 15 Audit results and performance presented to the Family and Women’s Health Group Governance Committee – July‐15
Dec 15
Safety QIP18 Histopathology The aim of this project is to improve the staffing numbers of suitably skilled and qualified staff in line with best practice (5 out of 13 consultant posts vacant) and to ensure improve performance against the reporting of cell pathology test results. Linked to a regulation breach. Regulation 18 Staffing – 18(1) sufficient numbers of suitably qualified, skilled and experienced persons must be deployed in order to meet these requirements) and Regulation 17 Good Governance 17(2)(A) – assess, monitor and improve the quality and safety of the services provided in the carrying on of
Service staffed with suitably qualified skill mix. Performance meets acceptable standards for reporting of cell pathology test results
Reduce the number of consultant Histopathologist vacancies Reduce the backlog number of unreported test results in cell pathology
3.70 WTE Consultant Histopathologist To be determined
CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Operations Director Clinical Support (Jonathan Wood)
Recruitment interviews for 2 Consultant Histopathologist undertaken – Aug 15 1 Consultant Histopathologist commenced in post – Sept 15
Identified laboratory staff trained to be advanced practitioners in histological dissection – Nov 15
2nd Consultant Histopathologist commenced in post on a part time basis – Jan 16 Clinical Network established with Sheffield supported by Digital Pathology to involve support from Sheffield in two tumour sites – Mar 16 New and extended roles for scientific staff developed – Apr 16 2nd Consultant Histopathologist

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 20
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
the regulated activity). This relates to ensuring there is a sustainable action plan to improve reporting performance of histopathology service.
increased to full time basis – May 16
Effectiveness
QIP19 Governance The aim of this project is to ensure there are systems established and operated effectively to ensure the Trust is able to assess, monitor and ensure compliance with all aspects of quality and safety. Linked to a regulation breach. Regulation 17 Good Governance 17(1) and 17(2) ensure there are timely and effective governance processes in place to identify and actively manage risks throughout the organisation)
Appropriate governance arrangements are in place which provide assurance on all aspects of quality and safety as well as early warning of potential problems / issues
Reduction in the risks identified in the quarterly CQC intelligence monitoring No overdue CQC mortality alerts No overdue CAS Alerts
4 elevated risks, 11 risks (May 2015) 1 ‐ Currently non‐compliance with Sepsis from July 2015 0
Sign up to Safety CQC inspection actions QIP 01 (risk Management) QIP 02 (Lessons Learned) TDA support to review Health Group governance arrangements
Director of Governance (Liz Thomas)
Director of Governance (Liz Thomas)
The TOR of external review of governance arrangements agreed – Sept 15 The external review commenced and milestones agreed – Sept 15 Quality Improvement Plan and milestones agreed – Sept 15
External review of governance completed including recommendations ‐ Nov 15 Quality Improvement Plan reporting structures agreed – Nov 15 Recommendations from external review accepted and milestones agreed – Dec 15
New governance and accountability structures in place – Mar 16
Effectiveness
QIP20 Duty of Candour The aim of this project is to ensure the Duty of Candour process is embedded across the organisation and all incidents reported as moderate or above including missed and delayed diagnosis comply with the duty of candour requirements. Linked to a regulation breach. Regulation 17 Good Governance 17(2)(A) assess, monitor and improve the quality and safety of the services provided in the carrying out of the regulated activity including the quality of the experience of service users in receiving those services.
Full compliance with the CQC Regulation 20 – Duty of Candour
100% of moderate incidents and above where an apology is given within the Trust internal standard of 10 days 100% of moderate incidents or above where patients have requested feedback are informed of the outcome of the investigation within the Trust internal standard of 10 days. All Serious Incident investigation reports are to be shared with the relevant person when requested
78% of cases for an apology being provided (May 2015)
43% for patients being informed of the outcome of investigation (May 2015)
Not collected
CQC Inspection Actions
Director of Governance (Liz Thomas)
Head of Risk, Claims & Safety (Mark Green)
Health group governance score card developed which includes performance against Duty of Candour – Aug 15 Audit process developed – Sept 15 Audit process implemented – Oct 15
Results of Q1 audit analysed to inform further actions required – Nov 15 Policy review completed (DofC, Being Open, SI) – Nov 15 Workshop held across the Trust – Dec 15
Knowledge of duty of candour tested and gaps identified– Mar 16 Future arrangements for training determined – Mar 16 Quarterly Audits completed and reported at Operational Quality Committee – Mar 16
Effectiveness
QIP21 Training, Appraisal And Supervision The aim of the project is to ensure
To ensure that all Trust staff has
Achieve 85% compliance with
84% CQC Inspection
Director of Workforce
Head of Education
Teacher trainer has delivered an internal
Learning Management System is available via any
Monthly reporting dashboard related to

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 21
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
that all Trust staff has access to and are provided with statutory, mandatory and developmental training and learning that all staff receive regular and constructive appraisal and supervision.
access to and are provided with statutory, mandatory and developmental training and learning that all staff receive regular and constructive appraisal and supervision.
Statutory and Mandatory training overall with the core subjects
Actions (Simon Nearney)
(Dave Withers) development programme to the overseas nurses in Elderly Care ‐ Aug 15 All programmes of development have (where appropriate) (including all statutory and mandatory topics) e‐learning/blended learning option to ensure true flexibility of access ‐ Aug 15 Learning Management System displays real time data which is available at login to ensure staff can view their training record ‐ Aug 15 Further simplified appraisal framework and linked to updated Trust values and agreed behaviours ‐ Aug 15
internet connection and appropriate for all devices i.e. tablet etc. ‐ Nov 15
training compliance, activity sent to all managers and relevant committees ‐ Mar 16 Learning Management System hosts information / guidance / promotional materials for all professional development programmes including our external partners i.e. University of Hull ‐ Mar 16 Statutory / mandatory training is monitored and reviewed in Health Group monthly performance meetings with Executive to ensure 85% compliance is achieved ‐ Mar 16
Effectiveness
QIP22 Nutrition During both the CQC inspection in February 2014 and May 2015 the CQC raised concerns that patients were not adequately hydrated or provided nutrition. The aim of this project is to ensure patients have appropriate personal nutritional needs assessment completed and receive an appropriate care plan or referral to a dietician where required. Linked to a regulation breach. Regulation 14 Meeting Nutritional and Hydration needs 14(1), 14(4)(A) and 14(4)(D) – nutritional and hydration of service users must be met; must be suitable and nutritious food and
Patients have appropriate personal nutritional needs assessment and receive an appropriate care plan or referral to a dietician where required. All patients monitored for risk of malnutrition and dehydration and any related deterioration.
Achieve >89% completion rate of food charts, hydration assessment , monitoring of patients weight, patients nutritionally screened, patients appropriately referred to a dietician
Compliance with PLACE assessments
Baseline to be established
CHH 93.90% HRI 93.80%
Quality Account / Sign up to Safety and CQC Inspection Actions
Chief Nurse (Mike Wright)
Chair of Nutrition Steering Group (Steve Jessop) Head of Dietetics (Tina McDougall) Head of Facilities (Jill Venables)
Proposed changes to Food Chart Completion process agreed ‐ Nov 15 Audit process established – Nov 15 Audit piloted on elderly care wards – Dec 15 Training and rollout of amended food record chart commenced ‐ Dec 15 Hydration Assessment Process agreed ‐ Dec 15
Audit process rolled‐out Trust wide – Jan 16 Trial commenced of new hydration record chart process ‐ Jan 16 Red top jug system is applied consistently on all medical wards ‐ Feb 16 New oral hygiene assessment sheet trialled ‐ Feb 16 Baseline for targets established – Mar 16
Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 22
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
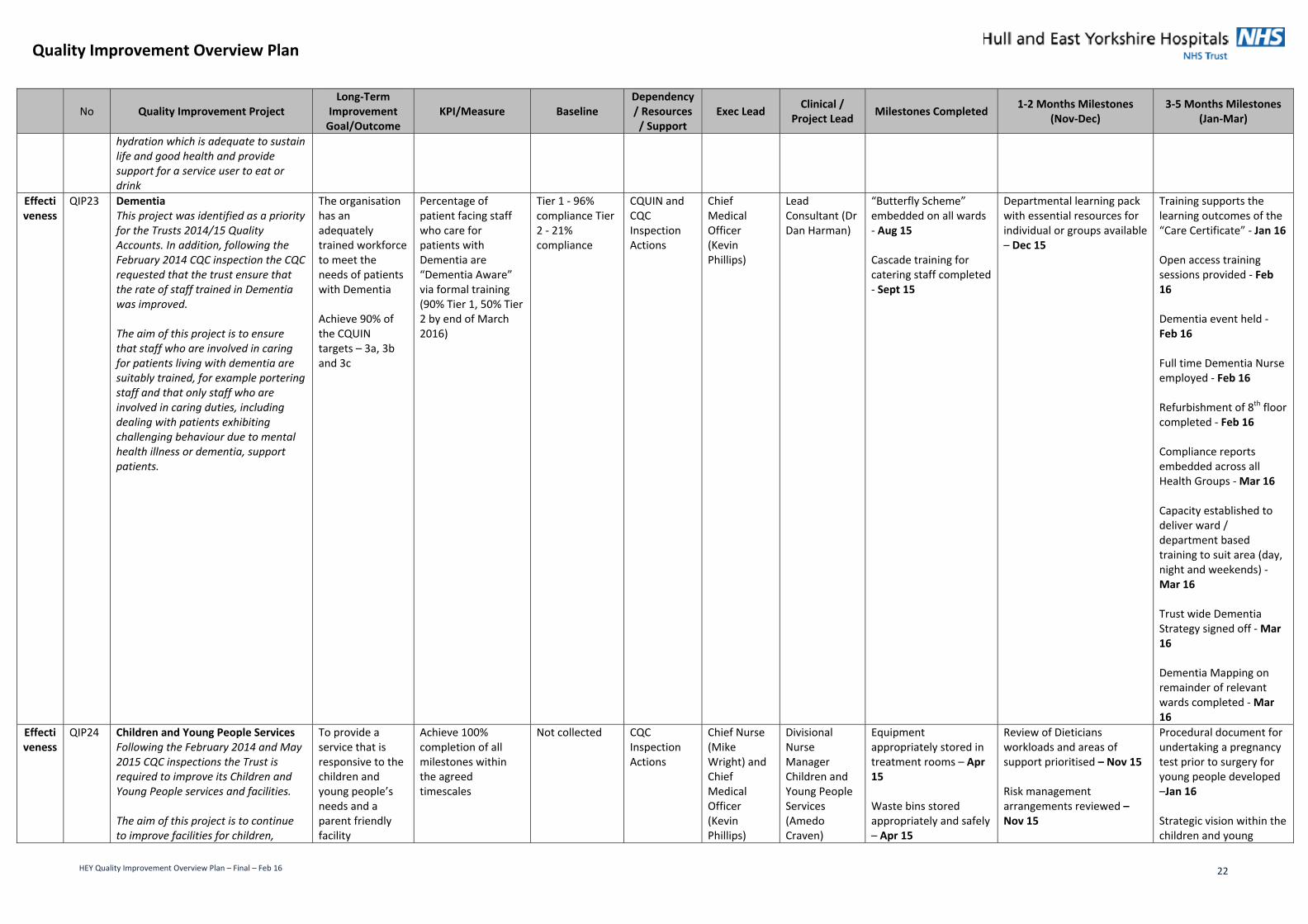
hydration which is adequate to sustain life and good health and provide support for a service user to eat or drink
Effectiveness
QIP23 Dementia This project was identified as a priority for the Trusts 2014/15 Quality Accounts. In addition, following the February 2014 CQC inspection the CQC requested that the trust ensure that the rate of staff trained in Dementia was improved. The aim of this project is to ensure that staff who are involved in caring for patients living with dementia are suitably trained, for example portering staff and that only staff who are involved in caring duties, including dealing with patients exhibiting challenging behaviour due to mental health illness or dementia, support patients.
The organisation has an adequately trained workforce to meet the needs of patients with Dementia Achieve 90% of the CQUIN targets – 3a, 3b and 3c
Percentage of patient facing staff who care for patients with Dementia are “Dementia Aware” via formal training (90% Tier 1, 50% Tier 2 by end of March 2016)
Tier 1 ‐ 96% compliance Tier 2 ‐ 21% compliance
CQUIN and CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
Lead Consultant (Dr Dan Harman)
“Butterfly Scheme” embedded on all wards ‐ Aug 15 Cascade training for catering staff completed ‐ Sept 15
Departmental learning pack with essential resources for individual or groups available – Dec 15
Training supports the learning outcomes of the “Care Certificate” ‐ Jan 16 Open access training sessions provided ‐ Feb 16 Dementia event held ‐ Feb 16 Full time Dementia Nurse employed ‐ Feb 16 Refurbishment of 8th floor completed ‐ Feb 16 Compliance reports embedded across all Health Groups ‐ Mar 16 Capacity established to deliver ward / department based training to suit area (day, night and weekends) ‐ Mar 16 Trust wide Dementia Strategy signed off ‐ Mar 16 Dementia Mapping on remainder of relevant wards completed ‐ Mar 16
Effectiveness
QIP24 Children and Young People Services Following the February 2014 and May 2015 CQC inspections the Trust is required to improve its Children and Young People services and facilities. The aim of this project is to continue to improve facilities for children,
To provide a service that is responsive to the children and young people’s needs and a parent friendly facility
Achieve 100% completion of all milestones within the agreed timescales
Not collected CQC Inspection Actions
Chief Nurse (Mike Wright) and Chief Medical Officer (Kevin Phillips)
Divisional Nurse Manager Children and Young People Services (Amedo Craven)
Equipment appropriately stored in treatment rooms – Apr 15 Waste bins stored appropriately and safely – Apr 15
Review of Dieticians workloads and areas of support prioritised – Nov 15 Risk management arrangements reviewed –Nov 15
Procedural document for undertaking a pregnancy test prior to surgery for young people developed –Jan 16 Strategic vision within the children and young

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 23
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
young people and their parents on the 13th floor and to ensure the service is responsive to the needs of its service users. Linked to a regulation breach. Regulation 12 Safer Care and Treatment 12(2)(I) – where responsibility for the care and treatment of service users is shared with, or transferred to, other persons, working with such other persons, service users and other appropriate persons to ensure that timely care planning takes place to ensure the health, safety and welfare of service users) and 12(2)(D) – ensuring the premises used by the service provider are safe to use for their intended purpose and are used in a safe way)
Matron Children and Young People Services (Lesley Harrison)
Process for ensuring children are assessed and treated in an appropriate environment within ED during out of hours implemented – Apr 15 All Emergency Department Nursing staff on a rota to work in Children’s Emergency Department – Apr 15 Sensory play equipment for children with special needs available in Children’s Outpatient Departments – Apr 15 Self‐assessment of all windows to ensure compliance with the appropriate standards completed and assurance provided – May 15 Compliance with HTM 55 and HBN 00‐10 confirmed to the CQC – May 15 Additional Locums recruited in the Dietetic Department for support to the Children and Young People service – May 15 Re‐inspected all windows and compliance confirmed against the latest guidance in terms of robustness and restricting the opening –
Procedural document ensuring there is effective transition for young people to adult services developed – Dec 15 Procedural document ensuring there is effective transition for young people to adult services approved –Dec 15 Monthly leadership meetings revised and include services outside of children and young people – Dec 15 The parents ‘sitting room’ facilities improved – Dec 15
people service promoted – Jan 16 Procedural document for undertaking a pregnancy test prior to surgery for young people approved –Jan 16 Communication campaign promoting the procedural document ensuring there is effective transition for young people to adult services launched – Feb 16 Communication campaign informing staff of the procedural document for undertaking a pregnancy test prior to surgery for young people launched – Feb 16 The number of Consultant Paediatric Surgeons in post increased – Mar 16 Sustainability and effectiveness of the Paediatric Consultant rota reviewed – Mar 16 Continued working with Infrastructure and Development to plan for relocation of the children’s wards from the 13th floor. This will include improved environment for both children and their families – Mar 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 24
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Sept 15 3 Advanced Nurse Practitioners in Paediatrics recruited – Sept 15 Converted a cubicle to ‘en‐suite’ to continue to improve parental facilities – Oct 15
Effective ness
QIP25 Major Trauma and Incident within the Emergency Department The aim of this project is to improve the communication and availability of its Major Incident Plan and provide adequate training to ensure staff is able to respond appropriately. Equipment must also be checked frequently and fit for purpose. Linked to a regulation breach. Regulation 12 Safer Care and Treatment – 12(1) care and treatment must be provided in a safe way for service users). This relates to ensuring that there are appropriate arrangements in place to respond to major trauma and incidents in ED.
Emergency Department team are suitably trained and have the tools and equipment necessary to deal with a major incident.
Number of staff trained in Major Incident
All new starters CQC Inspection Actions
Chief Medical Director (Kevin Phillips)
Assistant Director of Planning (Alan Harper) Strategy and Planning (Chris O’Neill)
Formal expression of interest submitted to Department of Health funded exercise to update Major Incident Plan – Jul 15 Business continuity course funded by Hull CCG completed by selected Business Continuity leads – Jul 15 Chemical, Biological, Radiological and Nuclear (CBRN) Plan revised – Aug 15 Strategic Leadership in Crisis training delivered to targeted directors and “2nd on call” managers – Sept 15 Call out cascade tests completed – Sept 15 All 24 hour powered respirator protective suits recertified in accordance with Department of Health requirements – Sept 15 All staff within the Emergency Department
Communication plan (including training) developed – Nov 15
Equipment replaced in Major Incident Store –Dec 15
Audit arrangements in place for equipment check in Major Incident Store – Dec 15 Review of Major Incident Policy completed –Dec 15
Call out cascade test completed – Mar 16 Ongoing audit of compliance initiated – Mar 16
Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 25
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
aware of where to access the major incident plan – Oct 15 All equipment in the Major Incident Store checked – Oct 15
Effectiveness
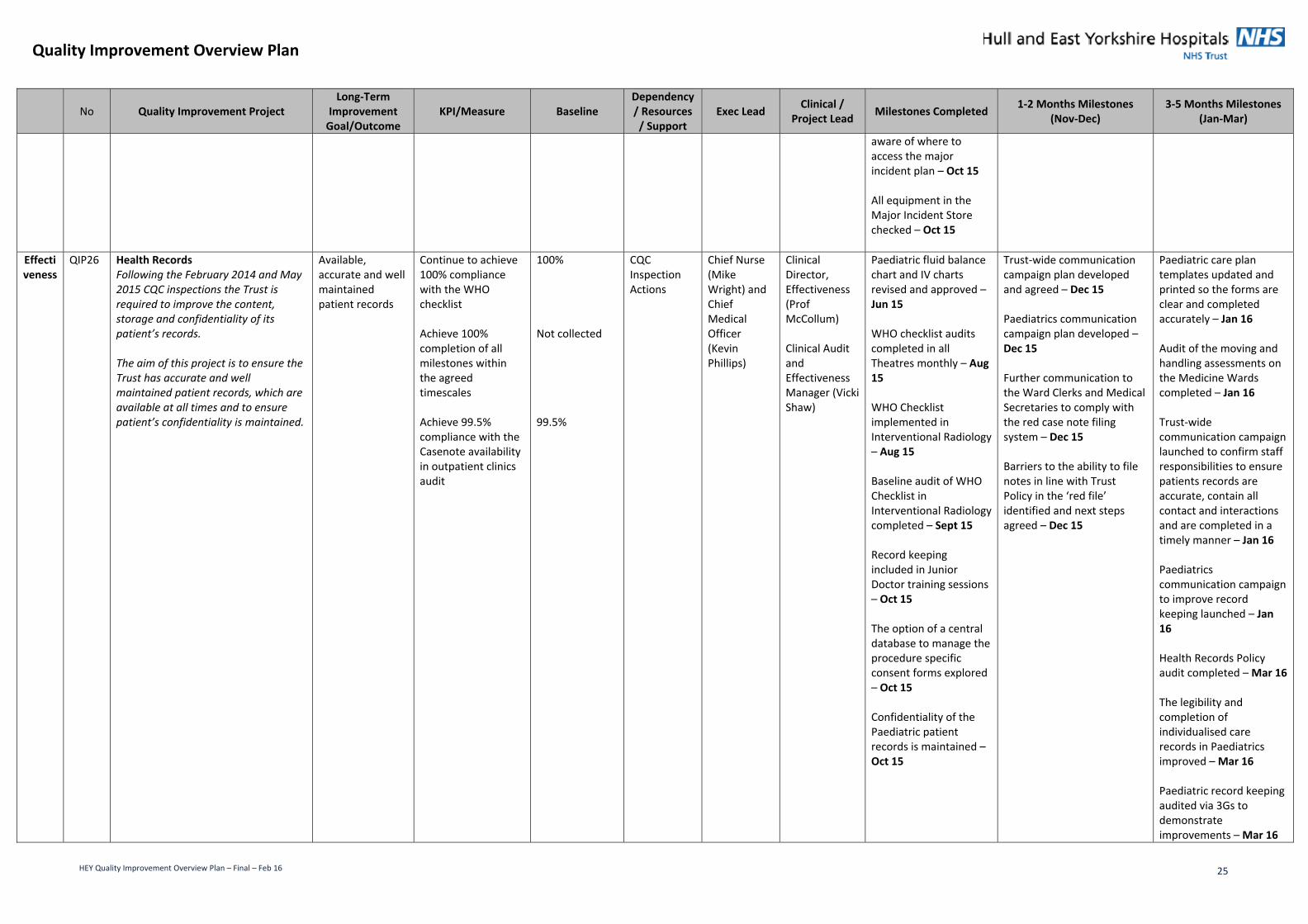
QIP26 Health Records Following the February 2014 and May 2015 CQC inspections the Trust is required to improve the content, storage and confidentiality of its patient’s records. The aim of this project is to ensure the Trust has accurate and well maintained patient records, which are available at all times and to ensure patient’s confidentiality is maintained.
Available, accurate and well maintained patient records
Continue to achieve 100% compliance with the WHO checklist Achieve 100% completion of all milestones within the agreed timescales Achieve 99.5% compliance with the Casenote availability in outpatient clinics audit
100% Not collected 99.5%
CQC Inspection Actions
Chief Nurse (Mike Wright) and Chief Medical Officer (Kevin Phillips)
Clinical Director, Effectiveness (Prof McCollum) Clinical Audit and Effectiveness Manager (Vicki Shaw)
Paediatric fluid balance chart and IV charts revised and approved – Jun 15 WHO checklist audits completed in all Theatres monthly – Aug 15 WHO Checklist implemented in Interventional Radiology – Aug 15 Baseline audit of WHO Checklist in Interventional Radiology completed – Sept 15 Record keeping included in Junior Doctor training sessions – Oct 15 The option of a central database to manage the procedure specific consent forms explored – Oct 15 Confidentiality of the Paediatric patient records is maintained – Oct 15
Trust‐wide communication campaign plan developed and agreed – Dec 15 Paediatrics communication campaign plan developed – Dec 15 Further communication to the Ward Clerks and Medical Secretaries to comply with the red case note filing system – Dec 15 Barriers to the ability to file notes in line with Trust Policy in the ‘red file’ identified and next steps agreed – Dec 15
Paediatric care plan templates updated and printed so the forms are clear and completed accurately – Jan 16 Audit of the moving and handling assessments on the Medicine Wards completed – Jan 16 Trust‐wide communication campaign launched to confirm staff responsibilities to ensure patients records are accurate, contain all contact and interactions and are completed in a timely manner – Jan 16 Paediatrics communication campaign to improve record keeping launched – Jan 16 Health Records Policy audit completed – Mar 16 The legibility and completion of individualised care records in Paediatrics improved – Mar 16 Paediatric record keeping audited via 3Gs to demonstrate improvements – Mar 16

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 26
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
Completion of moving and handling assessments improved on the Medicine Wards – Mar 16 List of abbreviations to help with the documentation developed and agreed – Mar 16 Multi‐disciplinary documentation of care records increased by Physio and OT – Mar 16 Monthly audits of the case note availability in outpatient clinics completed – Mar 16 Results analysed from the Health Records Policy audit and next steps and learning identified – Apr 16
Experience
QIP27 Patient Communication Following the May 2015 CQC inspection it was reported that the Trust Board did not receive patient stories and there was no clear process for ensuring board level understanding of complaints. The aim of this project is to improve escalation and information to the Trust Board relating PALS and Complaints to ensure all Trust Board members have an understanding of the patient stories and experiences across the Trust.
Board level understanding of patient stories (positive and negative) and experiences.
Trust board to receive a patient story at each meeting) 9 complaint reports presented to the Trust Board 100% of complaints letters provided to the Chairman
Not collected Not collected Not collected
CQC Inspection Actions
Chief Nurse (Mike Wright)
Assistant Chief Nurse – Patient Experience (Sarah Bates)
Process for ensuring board level understanding of complaints agreed – Aug 15 Chief Nurse includes a complaint briefing report and lessons learnt in the quality papers (monthly) – Aug 15
Trust board to receive a patient story at each meeting – Mar 16 Chairman receives a copy of every complaint sent to the Trust – Mar 16 End of year review of suitability of process completed – Mar 16
Experience
QIP28 Patient Experience and Complaints The aim of this project is to seek and act on feedback from our patients their relatives and carers. This will enable us to learn what is working well and what requires further
Seek and act on feedback from patients, their relatives and cares.
95% patients recommending the Trust through Friends and Family Test
94%
Quality Account Priority / Sign up to Safety and CQC
Chief Nurse (Mike Wright)
Assistant Chief Nurse – Patient Experience (Sarah Bates)
Baseline of satisfaction with the complaints process ‐ Sept 15
Quarterly post complaints survey
Quarterly post complaints survey completed – Dec 15 Quarterly results analysed and themes identified – Dec 15
Quarterly post complaints survey completed – Mar 16 Quarterly results analysed and themes

Quality Improvement Overview Plan
HEY Quality Improvement Overview Plan – Final – Feb 16 27
No Quality Improvement Project Long‐Term
Improvement Goal/Outcome
KPI/Measure Baseline Dependency / Resources / Support
Exec Lead Clinical / Project Lead Milestones Completed 1‐2 Months Milestones
(Nov‐Dec) 3‐5 Months Milestones
(Jan‐Mar)
improvement and to use the feedback to inform those required changes. This will ensure the services are responsive to our service users. Linked to a regulation breach. Regulation 16 Receiving and acting on complaints ‐ 16(1) any complaint received must be investigated and necessary and proportionate action must be taken in response to any failure identified by the complainant or investigation.
90% of formal complaints to be closed within 40 days and actions recorded where appropriate To increase the number of volunteer recruits in the Trust to 350, to benefit patients in clinical areas
Not collected 250 recruited during 2014/15
Inspection Actions
completed – Sept 15 Quarterly results analysed and themes identified – Sept 15 Quarterly action plan developed and implemented – Sept 15 Patient experience hub opened and staffed – Oct 15
Quarterly action plan developed and implemented – Dec 15 Volunteers located in ED giving out FFT forms – Dec 15 Volunteers located in ED running the refreshment rounds – Dec 15 New complaints policy approved by Patient Experience Forum – Dec 15 Patient Experience Strategy format agreed – Dec 15 Accurate way of recording the 40 day target on DATIX identified – Dec 15 Facility to meet the 40 day target implemented – Dec 15
identified – Mar 16 Quarterly action plan developed and implemented – Mar 16 New complaints policy launched ‐ Jan 16 Complaints policy audited quarterly – Mar 16 350 volunteers recruited – Mar 16 ‘You said we did’ boards used to improve services – Mar 16 40 day target results published monthly – Mar 16
Experience
QIP29 Missed & delayed diagnosis The aim of this project is to reduce the number of missed and delayed diagnosis Serious Incidents and to improve patient safety. Linked to a regulation breach. Regulation 17 Good Governance ‐17(2)(B) assess, monitor and mitigate the risks relating to the health, safety and welfare of service users and others who may be at risk which arise from the carrying on of the regulated activity). This relates to ensuring the use of best practice guidance, such as the five steps to safer surgery checklist.
To reduce the number of missed and delayed diagnosis Serious Incidents and to reduce the number of patients waiting over 6 weeks for a diagnostic test.
Reduce the number of missed and delayed diagnosis Serious Incidents Reduce to <=1% of patients waiting over 6 weeks for diagnostic test
10 (April 2014 – March 2015) 0.71%
Sign up to Safety / Quality Account Priority and CQC Inspection Actions
Chief Medical Officer (Kevin Phillips)
(Clinical Quality Director) Dr Oliver Byass
Serious Incidents with a missed and delayed diagnosis element identified – Oct 15
Review of Serious Incident themes completed – Nov 15 Recurrent themes from Serious Incidents identified – Nov 15 Future actions and milestones agreed – Nov 15 Themes from the 10 reported in 2014/15 to be reviewed by the Risk Team ‐ Dec 15
HEY results go live ‐ Jan 16 GP results go live ‐ March 16 Retrospective results ‐ March 16