quality and its on health and chronic medical€œhas your doctor ever asked you about sleep...
TRANSCRIPT

12
SaturdayGeneralSession
SleepQualityandItsImpactonOverallPatientHealthandChronicMedicalConditions
AlonAvidan,MD,MPHProfessorandViceChair,DepartmentofNeurologyDirector,UCLASleepDisordersCenterDavidGeffenSchoolofMedicineatUCLALosAngeles,CaliforniaEducationalObjectivesBytheendofthiseducationalactivity,participantsshouldbebetterableto:
1. Recognizetheassociationbetweenpoorsleepqualityonpatientqualityoflifeanditsimpactonchronicmedicalconditions.
2. Identifystrategiestoimprovecommunicationwithpatientstoassesssleepquality.
3. Evaluatecurrentpharmacologicoptionstoimprovepatientqualityofsleep.SpeakerDisclosureDr.Avidanhasdisclosedthatheisonthespeaker’sbureauforArborPharmaceuticalsandPernix.SupporterDisclosureThiseducationalactivityissupportedbyaneducationalgrantfromMerck&Company.IthasbeenplannedandproducedbyVemcoMedEdwithTexasAcademyofFamilyPhysiciansstrictlyasanaccreditedcontinuingmedicaleducationactivity.

1
ACTIVITY DESCRIPTION
Target AudienceThis activity is designed to meet the needs of primary care providers, including primary care physicians, doctors of osteopathy, physician assistants, nurse practitioners, and allied healthcare professionals, who are involved in the care of adult patients that would benefit from improved sleep quality.
Learning ObjectivesThis activity is designed to improve the competence and skills of primary care providers to: • Recognize the association between poor sleep quality on patient quality of life and its
impact on chronic medical conditions• Identify strategies to improve communication with patients to assess sleep quality • Evaluate current pharmacologic options to improve patient quality of sleep
FACULTY AND DISCLOSURE
Alon Y. Avidan MD, MPHProfessor and Vice Chair UCLA, Department of NeurologyDirector, UCLA Sleep Disorders CenterDavid Geffen School of Medicine at UCLALos Angeles, CA
Dr. Alon Avidan, MD has relevant financial relationships with the following commercial interests:Speakers Bureau: Pernix, Silenor.
Dr. Avidan does plan to discuss the off-label uses of the following: Discussion will include off-label uses of various CNS-actingmedications for insomnia. Specifically he will cover the use of sedating antidepressants, such as trazodone,amitriptyline, mirtazapine, doxepin; the antipsychotic quetiapine. Antihistamine compounds such as doxylamine, and thoseavailable over-the-counter marketed as sleep aids as single compounds or as a combination therapy with analgesics(ibuprofen or acetaminophen). Dietary supplement sleep aids such as chamomile, passionflower, valerian, hops, kava ,Tart cherry juice and melatonin.
No (other) speakers, authors, planners or content reviewers have any relevant financial relationships to disclose.
Content review confirmed that the content was developed in a fair, balanced manner free from commercial bias. Disclosure of arelationship is not intended to suggest or condone commercial bias in any presentation, but it is made to provide participants with information that might be of potential importance to their evaluation of a presentation.
Difficulties Falling Asleep
(˃ 30 min)
Difficulties Maintaining
Sleep
Early Morning Awakenings
(> 30 minutes before desired wake time)
Next Day Consequences
• Fatigue
• Attention, concentration, or memory impairment
• Social/vocational dysfunction Mood disturbance/irritability
• Proneness for errors/accident at work or while driving
• Tension headaches, and/or GI symptoms in response to sleep loss
• Concerns or worries about sleep
Despite adequate
opportunity for sleep
ICSD III
What is Insomnia?
© Alon Y. Avidan MD, MPH
Clinically significant distress
≥3 nights/week, ≥3 months Not due to substance,
medical condition, inadequate sleep time.
±±
• 62% Family Physician/ Internist
• 8% Psychiatrist
• 4% OB/GYN
• 4% Sleep Specialist
• 22% Other
No one
70%
SecondaryReason for
Consultation
24%
Primary Reason for Consultation
6%
Where do Patients with InsomniaGo for Management?
Ancoli-Israel S, Roth T. Sleep. 1999;22:S347-S353. The Gallup Organization for the National Sleep Foundation, 1995. National Sleep Foundation. “Sleep in America” Poll. March 2005. Available at: https://sleepfoundation.org/sleep-polls-data/sleep-in-america-poll/2005-adult-sleep-habits-and-styles.
29%
70%
0%
20%
40%
60%
80%
Yes No
“Has your doctor ever asked you about sleep issues?”
Psychiatric 40%
Primary / psychophysiologic
20%
Periodic limb movement
10%
Circadian rhythm (DSPS /
shift ) 10%
Breathing related 5%
Substances 5%
Other 10%
Presentations of Insomnia by Underlying Causes
Ohayon MM. Sleep Med Rev. 2002;6:97-111.

2
Impact of Insomnia
InsomniaMedical Illnesses
Reduced Quality of
Life
Higher Absenteeism
Increased Accident
Risk Higher Healthcare
Costs
Cognitive Impairment
Psychiatric Disorders
Benca RM. J Clin Psychiatry. 2001;62(suppl 10):33-38.
Contribution of Medical Conditions to Insomnia
CARDIACIschemia
Congestive heart failure
NEUROLOGICStrokeDegenerative conditionsDementiaPeripheral nerve damage Myoclonic jerksRestless leg syndromeHypnic jerkCentral sleep apneaChronic pain
PULMONARYCOPDAsthmaCentral alveolar hypoventilation Obstructive sleep apnea
GASTROINTESTINALGastroesophageal reflux
disease
ENDOCRINEHyperthyroidism
MenopauseMenstrual cycle
PregnancyHypogonadism
SUBSTANCESStimulantsOpioidsCaffeineAlcoholOr withdrawal from any of these
Medications - decongestants, corticosteroids, and bronchodilators
Bidirectionality of Insomnia & Psychiatric Conditions
Alterations in REM sleep As many as 40% of people
with depression have insomnia
DEPRESSION PTSD
Vivid and terrifying nightmares
ANXIETY
Generalized anxiety disorder, panic disorder, and anxiety disorders not otherwise specified
Predispose to insomnia
OTHER
Thought disorders and misperception of sleep state
PSYCH MEDS
Antidepressants may interfere with normal REM sleep patterns
Benzodiazepines or other hypnotic agents rebound insomnia
INSOMNIA
When did the insomnia begin?
When did the insomnia begin?
Was thereA specific Trigger?
Was thereA specific Trigger?
Frequency?Days/week?Frequency?Days/week?
Is it problems with:InitiationMaintenanceEarly AM awakening?
What have you tried so far?
What have you tried so far?
Why are you seeking help now?
Why are you seeking help now?
What is your expectation for management?
What is your expectation for management?
How has insomnia affected you?
How has insomnia affected you?
Insomnia Evaluation | History
Difficulties Maintaining
Sleep
Difficulties Maintaining
Sleep
Early morning
awakening
Insomnia According to Timing at Night
ASPSDepression
Drugs
RLSAnxietyDrugs
Primary Sleep Disorder:
OSA, NocturiaPoor sleep
environment
RLS, restless leg syndrome; OSA, obstructive sleep apnea; ASPS, advanced sleep phase syndrome
Difficulties Initiating
Sleep
Polysomnogram: Indications in the Evaluation of Insomnia

3
AASMN Sleep Diary. Available at: http://yoursleep.aasmnet.org/pdf/sleepdiary.pdf.
A 17y/o girl presents with her mother for evaluation of nighttime insomnia and difficulties with daytime functioning. She goes to bed at 2 AM and struggles to make it to her 7AM classes. She sleep in until 2-4PM on the weekends. She is an honors student, does homework on the computer until 1AM, but is now struggling academically. The best treatment is
Patient Case 1
1. Zolpidem at bedtime2. Melatonin at bedtime3. Bright light in the AM, avoidance of light at night4. Insight oriented psychotherapy
Delayed Sleep Phase Disorder Treatment – Intervention
• Light exposure in the morning upon waking
• Incremental advancement of sleep schedule by 15 minutes every day
• Avoid light exposure in evening
• Timed low dose melatonin (low dose is 0.5mg) 9 to 11 hours before middle of sleep episode
• Exposure to light from media – Delays circadian rhythm
• Media activities are stimulating
Treatment – Prevention
• Later school day starting times
• Schools limit late-evening activities
• Schools to educate students about sleep and circadian rhythms
• Parents to set appropriate bedtime
• Avoid light exposure and stimulating activities

4
Nadolski N. Plast Surg Nurs. 2005;25:167-173. Roth T, Culpepper L. Clin Symp. 2008;58:3-32.
• Restore and improve sleep quality and duration
• Prevent progression from acute to chronic insomnia
• Reduce impact on comorbid condition
Kupfer DJ, Reynolds CF III. N Engl J Med. 1997;336:341-346.Consensus Conference. JAMA. 1984;251:2410-2414.
Stepwise Approach for Managing Insomnia
Discuss Sleep
Diagnosis
Education, Including
Good Sleep Practices
Nonpharmacologicand/or
Pharma-cologicTherapy
Goals of Treatment• Relieve an upsetting symptom• Improve next-day consequences• Improve outcome of co-morbidity
• Psychiatric• Medical
Refer toSleep
Specialist(If Treatment
Failure)
Non-pharmacologic Approaches Patient Education Sleep Hygiene Aerobic exercise Cognitive behavior therapy–insomnia
(CBT-I) and other types of therapy
Pharmacologic Approaches• FDA-approved medications• Off-label prescription medications• Over-the-counter medications• Dietary supplements (unregulated)
Current Approaches for Treatment
1. Spielman AJ et al. Psychiatr Clin North Am. 1987;10:541-553. 2. Walsh JK et al. NIH Publication No. 98-4088. 3. Morin CM. Principles and Practice of Sleep Medicine, 4th ed. 2005:726-737. 4. Ringdahl EN et al. J Am Board Fam Pract. 2004;17:212-219.
This technique… Targets these symptoms
Stimulus control
Relaxation Techniques
Cognitive
Sleep hygiene education
Associating bed with wakefulness
Excessive time spent in bed; fragmented sleepExcessive time spent in bed; fragmented sleep
High physiologic, cognitive, or emotional arousal
Misconceptions about sleep and insomnia
Behaviors that undermine good quality sleep
Sleep restriction ☞
☞
☞
☞
☞
Cognitive & Behavioral Therapy
Do’s:• Enhance sleep environment: dark, quiet, cool temperature• Increase exposure to bright light during the day• Practice relaxing routine• Reduce time in bed; regular sleep/wake cycle• Incorporate regular exercise in the morning and/or afternoon
Don’ts: • “Watch the clock”• Use stimulants
(e.g., caffeine, nicotine, particularly near bedtime)• Consume a heavy meal or drink alcohol within 3 hours of bed• Use bright lights during the night, avoid TV/computers, e-gadgets.
Sleep Hygiene 101
NHLBI Working Group on Insomnia. 1998. NIH Publication. 98‐4088.Kupfer DJ, Reynolds CF. N Engl J Med. 1997;336:341‐346.Lippmann S, et al. South Med J. 2001;94:866‐873.
• CBT-I is the treatment of choice for:‒ Most patients with insomnia
‒ Better short-term efficacy compared to hypnotics‒ Better durability of effectiveness following cessation of hypnotics Rx
Downside: Some patients may lack:‒ Access to CBT-I‒ Response to CBT-I‒ Capacity of utilizing CBT-I
• Short-term course of hypnotic medication + CBT-I: may enhance outcome
Cognitive & Behavioral Therapy

5
Sleep Hygiene CBTi
Avoid stimulants for several hours before bedtime.• Avoid alcohol around bedtime.• Exercise regularly but not too late.• Allow 1-hour period to unwind before bedtime.• Keep bedroom environment quiet, dark and cool.• Maintain a regular sleep schedule.
• Sleep Restriction• Stimulus Control• Relaxation Training• Cognitive Therapy• Sleep Hygiene Education
Standard Guideline Individualized Multi-Component Intervention
Helps Normal Sleepers Maintain Sleep Health Treatment for Insomnia Disorder
Preventative Curative
The Dental Hygienist The dentist
Minimal Impact on Insomnia Disorder Very Effective Insomnia Disorder Treatment
Inactive Condition in Insomnia Research Active Condition in Insomnia Research
CBTi vs. Sleep Hygiene
Alcohol1,2,3
Herbals3,4
Dietary supplements1,4
Homeopathic preparations4
Melatonin1,3,4
OTC sleep aids2
Sedating antidepressants1
Sedative-hypnotics1,5
Melatonin-receptor agonistHypocretin-receptor antagonist
What Do People Take to Try to Improve Their Sleep?
1. Neubauer DN. Clinical Cornerstone. 2003;5:16-27. 2. Ancoli-Israel S, Roth T. Sleep. 1999;22(suppl 2):S347-S353. 3. Wagner J, et al. Neuropsychiatry. 1998;32:680-691. 4. Larzelere MM, Wiseman P. Prim Care Clin Office Pract. 2002;29:339-360. 5. Mitler MM. Sleep. 2000;23(suppl 1):S39-S47.
Drug ClassesDrug Classes
Histamine-Receptor
Antagonist
Histamine-Receptor
Antagonist
Melatonin-Receptor Agonist
Melatonin-Receptor Agonist
ZolpidemEszopiclone
ZaleplonTriazolam
ZolpidemEszopiclone
ZaleplonTriazolam
DoxepinDoxepinSuvorexant Ramelteon
BZA-Receptor Agonists
Hypocretin-Receptor
Antagonist
Hypnotics: Mechanism of Action & LabelingClass1 Drugs1,2 Acts on:1 Controlled Substance
Schedule2
Non-benzodiazepines Zolpidem, eszopiclone, zaleplon GABA IV
BenzodiazepinesTemazepam, estazolam, flurazepam, quazepam, triazolam
GABA IV
Melatonin-receptor agonist
Ramelteon Melatonin Not scheduled
Orexin-receptor antagonist4 Suvorexant Orexin IV
Antihistamines Diphenhydramine5 Histamine Not scheduled
Antidepressants Tradozone, amitriptyline Serotonin/histamine Not scheduled
BarbituratesPhenobarbital, mephobarbital, amobarbital, secobarbital
Non-selective CNS depressants II, III, IV
Antipsychotics Quetiapine, risperidone, aripiprazole Dopamine, serotonin Not scheduled
Selective H1
receptor antagonist3 Doxepin Histamine H1 Not scheduled
1. Roth T, Culpepper L. Clinical Symposia. 2008;58:1-32; 2. Controlled Substances Act. http://www.deadiversion.usdoj.gov/21cfr/21usc/812.htm. Accessed June 12, 2017; 3. SILENOR® (doxepin) [package insert]. Morristown, NJ: Pernix Therapeutics; 2014; 4. Belsomra® (suvorexant) [package insert]. Whitehouse Station, NJ; Merck and Co. 2016; 5. Richardson GS, et al. J Clin Psychopharmacol. 2002;22:511-515.
A 57 y/o male executive presents with middle of the night insomnia, beginning at 1AM. 2-3 times a week. He needs to be awake at 7AM. He would like to start a medication to help him with sleep maintenance difficulties. Which would be the most appropriate choice for him?
Patient Case 2
1. Ramelteon, 8mg po QHS2. Melatonin, 3mg po QHS3. Zolpidem, 5mg po QHS4. Sublinguial Zolpidem, 3.5mg Sublingual PRN, middle of the night
insomnia.
Agent Initiates Sleep
Maintains Sleep
Sleep with limited
opportunity
Required Inactivity
(hr)
Dose (mg)
Eszopiclone √ 8+ 1,2,3
Zaleplon √ √ 4 5,10
Zolpidem √ 7-8 5,10
Extended-release √ 7-8 6.25, 12.5
Sublingual √ (4 hrs) 4 1.75, 3.5
Oral spray √ 4 5, 10
Sublingual √ 4 5, 10
Doxepin (Ultra-low dose) 7-8 3, 6
Ramelteon √ - 8
Suvorexant √ 7 5, 10, 15, 20
6
Address underlying pathophysiology
Rapid sleep induction
Minimal adverse effect on
sleep physiology
Optimal duration of action
No formation of active metabolites
No memory deficits
No respiratorydepression
No interaction with
ethanol
No physicaldependence
No reboundinsomnia
No residualeffects
Ideal Hypnotic
Ideal Hypnotic
Rapid absorption
No tolerance
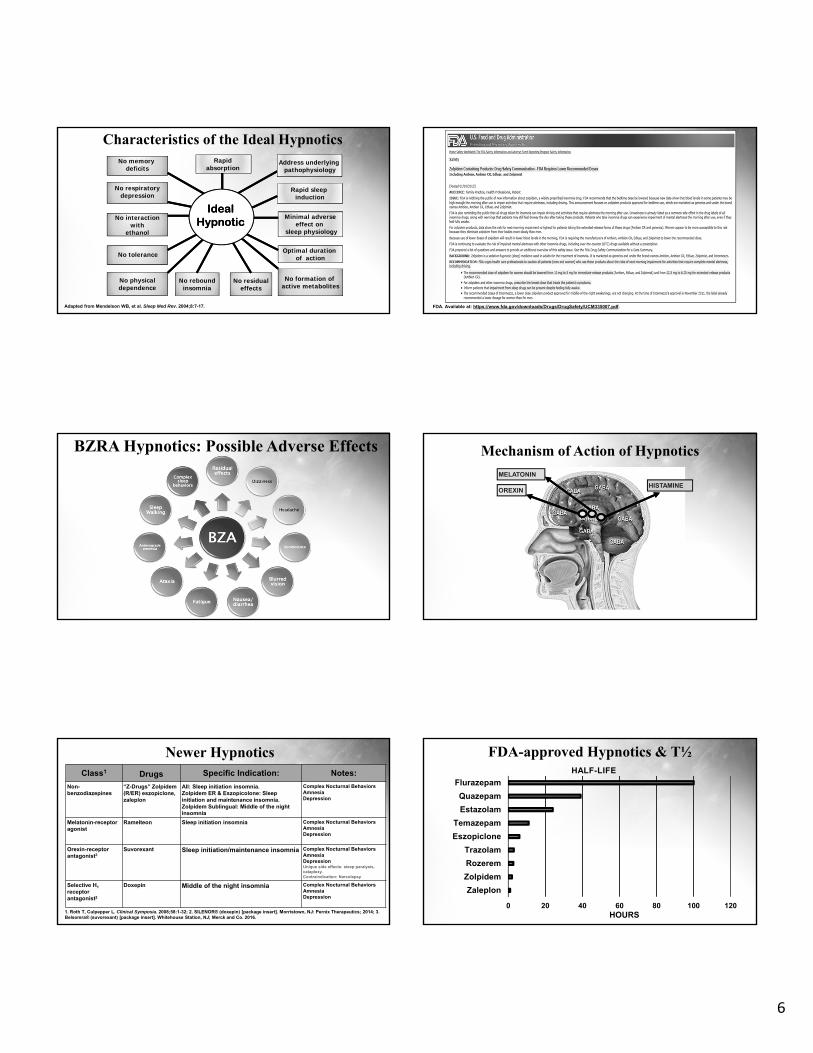
Characteristics of the Ideal Hypnotics
Adapted from Mendelson WB, et al. Sleep Med Rev. 2004;8:7-17. FDA. Available at: https://www.fda.gov/downloads/Drugs/DrugSafety/UCM335007.pdf.
BZRA Hypnotics: Possible Adverse Effects Mechanism of Action of Hypnotics
OREXIN
MELATONIN
HISTAMINE
Newer HypnoticsClass1 Drugs Specific Indication: Notes:
Non-benzodiazepines
“Z-Drugs” Zolpidem(R/ER) eszopiclone, zaleplon
All: Sleep initiation insomnia.Zolpidem ER & Eszopicolone: Sleep initiation and maintenance insomnia. Zolpidem Sublingual: Middle of the night insomnia
Complex Nocturnal BehaviorsAmnesiaDepression
Melatonin-receptor agonist
Ramelteon Sleep initiation insomnia Complex Nocturnal BehaviorsAmnesiaDepression
Orexin-receptor antagonist3
Suvorexant Sleep initiation/maintenance insomnia Complex Nocturnal BehaviorsAmnesiaDepressionUnique side effects: sleep paralysis, cataplexy.Contraindication: Narcolepsy
Selective H1
receptorantagonist2
Doxepin Middle of the night insomnia Complex Nocturnal BehaviorsAmnesiaDepression
1. Roth T, Culpepper L. Clinical Symposia. 2008;58:1-32; 2. SILENOR® (doxepin) [package insert]. Morristown, NJ: Pernix Therapeutics; 2014; 3. Belsomra® (suvorexant) [package insert]. Whitehouse Station, NJ; Merck and Co. 2016.
FDA-approved Hypnotics & T½
0 20 40 60 80 100 120
Zaleplon
Zolpidem
Rozerem
Trazolam
Eszopiclone
Temazepam
Estazolam
Quazepam
Flurazepam
HOURS
HALF-LIFE

7
Stahl SM. Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications, 3rd Edition. Cambridge University Press, 2008. p.835.
Moderately Long Half-Life Hypnotics Do Not Wear Off Until After Time to Awaken (Hangover)
Ultrashort Half-Life Hypnotics Wear Off Before Time to Awaken (Loss of Sleep Maintenance)
Stahl SM. Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications, 3rd Edition. Cambridge University Press, 2008. p.840.
Half-Life ≈ 6 hours Optimized Duration of Action
Stahl SM. Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications, 3rd Edition. Cambridge University Press, 2008. p.841.
Guideline Consensus Recommendations
Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2): 307–349.
USE: As a treatment for sleep onset and/or sleep maintenance insomnia1. Suvorexant2. Eszopiclone3. Zaleplon4. Zolpidem 5. Triazolam6. Temazepam7. Ramelteon8. Doxepin
DO NOT USE as a treatment for sleep onset or sleep maintenance insomnia:1. Trazodone2. Tiagabine 3. Diphenhydramine4. Melatonin5. Tryptophan6. Valerian
Data Compares: Versus no treatment, in adults. Level of Evidence: WEAK
Sateia MJ, et al. J Clin Sleep Med. 2017;13:307-49.
2017 AASM Treatment Recommendations

8
Qaseem, A., et al. (2016). "Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians." Annals of Internal Medicine 165(2): 125-133 (Appendix 2).
CBTI vs. Medication for Insomnia
Adapted from Morin CM et al. JAMA 1999; 281.
The Sleepless Patient: Summary
• Assessment requires careful inventory of potential confounders• CBT-I is an important option• Numerous medications are available, BUT:
‒ Risk analysis: Evaluate cost-benefit‒ Rx has variable benefit profiles‒ Insomnia therapy needs to be individualized to meet patient’s
expectations and needs• Insomnia is highly prevalent and can impact the general well-being
of patients• Evaluation of sleep should be a routine part of acute care and well
visits

MedicationIndexSleepQualityandItsImpactonOverallPatientHealthandChronicMedicalConditions
GenericName TradeNameAmitriptyline NoneAmobarbital NoneAripiprazole Abilify,AristadaDiphenhydramine BenadrylDoxepin Silenor,ZonalonEstazolam NoneEszopiclone LunestaFlurazepam NoneMephobarbital NonePhenobarbital NoneQuazeopam DoralQuetiapine SeroquelRamelteon RozeremRisperidone RisperdalSecobarbital SeconalSodiumSuvorexant BelsomraTemazepam RestorilTiagabine GabitrilTrazodone NoneTriazolam HaliconZaleplon SonataZolpidem Ambien,Edluar,Intermezzo,Zolpimist
Thefollowingmedicationswerediscussedinthispresentation.Thetablebelowliststhegenericandtradename(s)ofthesemedications.

Notes
