pvschools district enrollment packet
TRANSCRIPT

PVSchools District Enrollment Packet Thank you for choosing PVSchools in your school selection process. For more than 100 years, PVSchools has provided state-of-the-art technology coupled with cutting-edge programs to meet the learning needs of all students. PVSchools provides a robust and engaging educational experience, in a technology-rich environment, to ensure students are not only college and career ready, but prepared for life in the 21st century.
To begin your child’s Journey of Excellence, please be sure to fll out the required forms (listed below) and then supply the required documentation (listed below) that is needed to complete the registration process.
Parent/Guardian must supply the following items for all students upon enrollment:
Proof of residency: In order to register your student in the Paradise Valley Unifed School District, the parent or guardian must provide one (1) piece of documentation indicating the place of residency. Complete Arizona Residency Documentation Form.
Immunization Records: Proof of immunizations or signed waiver is required at the time of enrollment.
Ofcial State Issued Birth Certifcate - Must be original, no scanned copies allowed.
Withdrawal Form: Please present withdrawal form from most recently enrolled school.
Legal guardianship or custody papers: Are necessary, if: • An adoption has taken place, it is refected with an
amended birth certifcate, and student lives with adoptive parents as listed on the amended birth certifcate.
• The student lives with one custodial parent as the result of a divorce.
• The student lives with anyone else, i.e. grandparents, aunt, uncle, sibling, friends or other relatives. We must have a photocopy of the court papers granting guardianship within 30 days of enrollment.
Individualized learning plans, evaluations, and other related documents: Students who are presently receiving special services (special education, gifted, ELL, 504) are encouraged to provide copies of these documents upon enrollment.
Checklist ☐ Pupil Registration Form
☐ Arizona Residency Documentation Form
☐ Afdavit of Shared Residence
☐ Primary Home Language Other Than English Survey
☐ Student Health History
☐ Referral for Assessment Form
☐ PVSchools Screening Form
☐ Emergency Card
☐ Outside Media Release & Consent Agreement
☐ McKinney-Vento Eligibility Questionnaire
☐ Official State Issued Birth Certificate

ISS-Admin-741-rev 1/21/20
PARADISE VALLEY UNIFIED SCHOOL DISTRICT PUPIL REGISTRATION FORM
FOR OFFICE USE ONLY School Name: Date Entered in IC w/ Initials:
School Year: Student Start Date:
District Number: 070269 Entry Code:
STUDENT INFORMATION
How did you hear about us?
Legal Last Name Legal First Name Middle Name Sufx Nickname
Birthdate Gender Country of Birth State of Birth Student Cell Phone Grade Entering
M: ☐ F: ☐
Is this student of Hispanic/Latino ethnicity?
Please mark one or more boxes to indicate students race. Native Hawaiian or Other Pacifc Islander: ☐ American Indian or Alaska Native: ☐ (**If checked, please fll in tribe name below)
Black or African American: ☐ White: ☐ Asian: ☐YES: ☐ NO: ☐
**Tribal Name **Date Entered US School
If student identifes as a refugee, please fll out the following:
Refugee Status Date Entered US Date Entered US School
YES: ☐ NO: ☐
What language is preferred for school correspondence?
Last School Attended (Including PVSchools) City/State/Zip Grade Level
Has the student ever been identifed for any of the following programs? (NOTE: If YES, please include IEP)
☐ Special Education ☐ Speech ☐ Gifted ☐ 504 Plan ☐ ESL
I elect to receive only electronic notifcation for student progress and grade reports.
Has your child ever been expelled or long-term suspended?
YES: ☐ NO: ☐ YES: ☐ NO: ☐
Page 1

PARENT/GUARDIAN INFORMATION NOTE: The school will honor the non-custodial parent’s requests for information unless copies of custody papers or court orders restricting the non-custodial parent’s access to such information are on fle at the school. Who has legal custody? ☐ Parents ☐ Mother ☐ Father ☐ Other:
STUDENT’S PRIMARY HOUSEHOLD
Street Address Apt. No. City/State/Zip
Legal Parent/Guardian Information: Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Primary Contact Phone:
Work Phone: Birthdate: Month Day: Year:
Email Address:
Relationship to Student (Father, Mother, Stepfather, Foster Mother, etc.): Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
Is this parent/guardian an active duty member of the Army, Navy, Air Force, Marine Corps, Coast Guard, or National Guard?
YES: ☐ NO: ☐
Is this active duty parent/guardian currently deployed? YES: ☐ NO: ☐
Legal Parent/Guardian Information, or other adult living in same household:
Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Primary Contact Phone:
Work Phone: Birthdate: Month Day: Year:
Email Address:
Relationship to Student (Father, Mother, Stepfather, Foster Mother, etc.): Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
Is this parent/guardian an active duty member of the Army, Navy, Air Force, Marine Corps, Coast Guard, or National Guard?
YES: ☐ NO: ☐
Is this active duty parent/guardian currently deployed? YES: ☐ NO: ☐
Mailing Address (if diferent than above):
ISS-Admin-741-rev 1/21/20
Street Address Apt. No. City/State/Zip
Page 2

PARENT/GUARDIAN INFORMATION NOTE: The school will honor the non-custodial parent’s requests for information unless copies of custody papers or court orders restricting the non-custodial parent’s access to such information are on fle at the school.
SECONDARY HOUSEHOLD (NON-CUSTODIAL)
Street Address Apt. No. City/State/Zip
Legal Parent/Guardian Information: Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Primary Contact Phone:
Work Phone: Birthdate: Month Day: Year:
Email Address:
Relationship to Student (Father, Mother, Stepfather, Foster Mother, etc.): Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
Is this parent/guardian an active duty member of the Army, Navy, Air Force, Marine Corps, Coast Guard, or National Guard?
YES: ☐ NO: ☐
Is this active duty parent/guardian currently deployed? YES: ☐ NO: ☐
Legal Parent/Guardian Information, or other adult living in same household:
Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Primary Contact Phone:
Work Phone: Birthdate: Month Day: Year:
Email Address:
Relationship to Student (Father, Mother, Stepfather, Foster Mother, etc.): Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
Is this parent/guardian an active duty member of the Army, Navy, Air Force, Marine Corps, Coast Guard, or National Guard?
YES: ☐ NO: ☐
Is this active duty parent/guardian currently deployed? YES: ☐ NO: ☐
Mailing Address (if diferent than above):
ISS-Admin-741-rev 1/21/20
Street Address Apt. No. City/State/Zip
Page 3

ISS-Admin-741-rev 1/21/20
EMERGENCY CONTACT INFO. - NON-HOUSEHOLD NOTE: In an emergency, in addition to the parent/legal guardians listed on this application, the individuals noted below may be contacted regarding my student and may be released to the individuals listed below. Please prioritize the non-household individuals below in the order they should be contacted. Parent/legal guardian(s) will be contacted frst.
EMERGENCY CONTACT 1
Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Home Phone:
Work Phone: Gender: ☐ M ☐ F
Relationship to Student:
☐ Stepmother ☐ Stepfather ☐ Grandmother ☐ Grandfather ☐ Aunt ☐ Uncle
☐ Friend ☐ Neighbor ☐ Other:
Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
EMERGENCY CONTACT 2
Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Home Phone:
Work Phone: Gender: ☐ M ☐ F
Relationship to Student:
☐ Stepmother ☐ Stepfather ☐ Grandmother ☐ Grandfather ☐ Aunt ☐ Uncle
☐ Friend ☐ Neighbor ☐ Other:
Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
EMERGENCY CONTACT 3
Legal Last Name: Legal First Name: Middle Init:
Cell Phone Number: Home Phone:
Work Phone: Gender: ☐ M ☐ F
Relationship to Student:
☐ Stepmother ☐ Stepfather ☐ Grandmother ☐ Grandfather ☐ Aunt ☐ Uncle
☐ Friend ☐ Neighbor ☐ Other:
Was the above person ever a student or employed by Paradise Valley Unifed School District?
YES: ☐ NO: ☐
I afrm that the information provided is correct and current:
Parent/Guardian Signature: Date:
Page 4

Arizona Department of Education Arizona Residency Documentation Form
Student School
School District or Charter Holder
Parent/Legal Guardian
As the Parent/Legal Guardian of the Student, I attest* that I am a resident of the State of Arizona and submit in support of this attestation a copy of the following document that displays my name and residential address or physical description of the property where the student resides:
Valid Arizona driver’s license, Arizona identification card or motor vehicle registration ___ Valid Arizona Address Confidentiality Program authorization card
Real estate deed or mortgage documents Property tax bill Residential lease or rental agreement Water, electric, gas, cable, or phone bill Bank or credit card statement W-2 wage statement Payroll stub Certificate of tribal enrollment (506 Form) or other identification issued by a recognized Indian tribe in Arizona Documentation from a state, tribal or federal government agency (Social Security Administration, Veteran’s Administration, Arizona Department of Economic Security)
___ Temporary on-base billeting facility (for military families)
I am currently unable to provide any of the foregoing documents. Therefore, I have provided an original affidavit signed and notarized by an Arizona resident who attests that I have established residence in Arizona with the person signing the affidavit.
Signature of Parent/Legal Guardian Date
*For members of the armed services, the provision of verifiable documentation does not serve as a declaration of official residency for income tax or other legal purposes. Armed service members may utilize a temporary on-base billeting facility as the address for proof of residency.
#2803440

State of Arizona Affidavit of Shared Residence
Student Name:_______________________________________________________________________
Parent/Legal Guardian Name:___________________________________________________________
School Name:________________________________________________________________________
School District or Charter Holder:________________________________________________________
Name of Arizona Resident:______________________________________________________________
I, (resident name)____________________________________ swear or affirm that I am a resident of the State of Arizona and that the persons listed below reside with me at my residence, described as follows:
Persons who reside with me:____________________________________________________________ Location of my residence:________________________________________________________________
I submit in support of this attestation a copy of the following document that displays my name and current residence address or physical description of my property:
Valid Arizona driver’s license, Arizona identification card or motor vehicle registration ___ Valid Arizona Address Confidentiality Program authorization card
Real estate deed or mortgage documents Property tax bill Residential lease or rental agreement Water, electric, gas, cable, or phone bill Bank or credit card statement W-2 wage statement Payroll stub Certificate of tribal enrollment (506 Form) or other identification issued by a recognized Indian tribe in Arizona Documentation from a state, tribal or federal government agency (Social Security Administration, Veteran’s Administration, Arizona Department of Economic Security)
Printed Name of Affiant:
Signature of Affiant:
State of Arizona County of
Acknowledgement
The foregoing was acknowledged before me this By .
day of , 20 ,
My Commission Expires: Notary Public
#2803440

_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
Arizona Department of Education Office of English Language Acquisition Services
Home Language Survey
The responses to this Home Language Survey (HLS) are used by the school to provide the most appropriate instructional programs and services for the student. The answers below will determine if a student will take the Arizona English Language Learner Assessment (AZELLA). Please respond to each of the three questions as accurately as possible. If you need to correct any of your responses, this must be done before the student takes the AZELLA Placement Test.
1. What language do people speak in the home most of the time?
2. What language does the student speak most of the time?
3. What language did the student first speak or understand?
Student Name________________________________ District Student ID_______________
Date of Birth_________________________________ SSID__________________________
Parent/Guardian Signature______________________________ Date___________________
District or Charter____________________________________________________________
School_____________________________________________________________________
Please provide a copy of the Home Language Survey to the EL Coordinator/Main Contact on site. In AzEDS, please enter all three HLS responses.
These HLS questions are in compliance with Arizona Administrative Code (R7-2-306(B)(1),(2)(a-c). (Revised 01-2020)
Office of English Language Acquisition Services 1535 West Jefferson Street • Phoenix, Arizona 85007 • (602) 542-0753 • www.azed.gov/oelas

Anemia de células falciformes
Paradise Valley Unified School District / Distrito Escolar Unificado Paradise Valley � Phoenix, Arizona STUDENT HEALTH HISTORY / HISTORIAL DE SALUD DEL ALUMNO
To be completed by parent/guardian at the time of registration. / Lo deberá completar un padre o tutor legal al momento de la inscripción.
Student Name / Nombre del alumno: Date of Birth / Fecha de nacimiento: School / Escuela: Age / Edad: Grade / Grado:
Has child previously attended school in the Paradise Valley Unified School District? YES / SÍ NO¿Ha asistido este alumno a la escuela en el Distrito Escolar Paradise Valley?
If yes: Name of School / Nombre de la escuela: Year Attended /Año en que asistió: Si responde afirmativamente:
Has your child been/Is your child presently under treatment of a physician, counselor, and/or psychologist? YES / SÍ NO¿Ha estado o está al presente su hijo bajo tratamiento de un médico, consejero, o psicólogo?
If yes, please provide: Name of Provider / Nombre del especialista: Date Last Seen / Fecha última visita: Si responde afirmativamente, indique:
Reason / Motivo: Has your child ever had a psychological test? YES / SÍ NO Date of Test / Fecha del examen: ¿Alguna vez ha tenido su hijo un examen psicológico?
PRENATAL HISTORY / HISTORIAL PRENATAL MEDICAL HISTORY / HISTORIAL MÉDICO During pregnancy, did the mother: / Durante el embarazo, la madre: Has your child ever had or been diagnosed with: / Alguna vez su hijo ha
YES / SÍ NO tenido, o le han diagnosticado: Have prenatal care? / ¿Tuvo cuidado prenatal? YES / SÍ NO
ADD/ADHD / ADD/ADHD Incur any serious accident or injury? / ¿Sufrió algún Have health problems? / ¿Tuvo problemas de salud?
Allergies / Alergias accidente o lesión grave? Anemia / Anemia
Arthritis/Rheumatic Disease / Artritis/enfermedad BIRTH HISTORY / HISTORIAL DEL NACIMIENTO reumática Birth weight / Al nacer pesó lbs. ozs. Asthma / Asma Length / midió Autism / Autismo
YES / SÍ NO Birth Defect/Developmental Disorder / Defecto del Was birth premature? / ¿Fué prematuro el nacimiento? nacimiento/trastorno del desarrollo Caesarean delivery? / ¿Operación cesárea? Bleeding Disorder / Trastorno de sangrado Any birth injuries/defects? / ¿Alguna lesión/defecto de Connective Tissue Disorder / Trastorno del tejido conectivo nacimiento? Cystic Fibrosis / Fibrosis quística INFANT DEVELOPMENT / DESARROLLO INFANTIL Diabetes / Diabetes Within the first 2 years of life, did your child display normal (average) or Eating/Weight Disorder / Trastorno alimentario/ de peso delayed development in the following events: / Durante los dos primeros años Emotional Disorder / Trastorno emocional de edad su hijo demostró un desarrollo normal (promedio,) o demorado, en las Endocrine Disorder / Trastorno endocrino etapas siguientes? Gastrointestinal Disorder / Trastorno gastrointestinal
DELAYED Genitourinary Disorder / Trastorno genitourinario NORMAL DEMORADO Hearing/Ear Disorder / Trastorno de audición/oído
Sit alone (avg. 7 mos.) / Sentarse solo(a) (prom. 7 meses) • Known hearing loss / Pérdida conocida de audición Crawl (avg. 9 mos.) / Gatear (promedio 9 meses) • Tubes in ears / Tubos en los oídos Stand alone (avg. 10 mos.) / Pararse solo (prom. 10 mes.) • Hearing aids / Audífonos (hearing aids) Walk alone (avg. 12 mos.) / Caminar solo (prom. 12 mes.) • Frequent ear aches/infections / Frecuentes Speak first word (avg. 12 mos.) / Hablar su primera dolores/infecciones de oído palabra (promedio 12 meses) Heart Condition / Afección del corazón Speak first sentence (avg. 24 mos.) / Hablar su primera Hypertension / Hipertensión frase (promedio 24 meses) Malignancy / Tumor maligno Become toilet trained (avg. 24 mos.) / Aprendió a ir solo Neuro Disorder (includes migraines) / Trastorno al baño (promedio 24 meses) neurológico (incluye migrañas) BEHAVIORAL HISTORY / HISTORIAL DEL COMPORTAMIENTO Orthopedic Disorder / Trastorno ortopédico Has your child ever exhibited any of the following: / ¿Alguna vez ha Physical Handicap / Discapacidad física presentado su hijo algo de lo siguiente? Psychiatric Disorder / Trastorno psiquiátrico
NEVER SOMETIMES ALWAYS Scoliosis / Escoliosis NUNCA ALGUNAS VECES SIEMPRE Seizure Disorder / Trastorno convulsivo
Bites nails / Morderse las uñas Serious Injury/Accident / Lesión/accidente grave Difficulty sleeping / Dificultad para Sickle Cell Disease / dormir Skin Disorder / Enfermedades de la piel Fights with others / Pelea con otros Speech Disorder / Trastornos del habla Frequent crying / Llora con frecuencia Substance Use/Abuse / Uso/abuso de substancias/drogas Nightmares / Tiene pesadillas Surgery / Cirugía Poor coordination / Mala coordinación Tuberculosis (active) / Tuberculosis (activa) Poor eating habits / Malos hábitos para Vision/Eye Disorder / Trastornos de la visión/ojo comer • Known vision loss / Pérdida conocida de visión Prefers to play alone / Prefiere jugar solo • Color deficient / Deficiencia en percibir colores Restlessness/hyperactivity / • Glasses/contacts / Anteojos/lentes de contacto Inquietud/hiperactividad Sucks thumb / Se chupa el pulgar (dedo) Tantrums / Tiene rabietas Teeth grinding / Rechina los dientes Wets the bed / Moja la cama
ISE-HS-015-11/17 Parent/Guardian Signature: / Firma Padre/Tutor legal : Date: / Fecha:

Paradise Valley Unified School District - Distrito Escolar Unificado de Paradise Valley REFERRAL FOR ASSESSMENT OF SPECIAL HEALTH CARE SERVICES
REMISIÓN PARA UNA VALORACIÓN DE SERVICIOS ESPECIALES DE ATENCIÓN DE LA SALUD
To be completed by parent/guardian at the time of registration. Un padre de familia o tutor legal deberá completar este formulario durante la inscripción.
NOTE:
NOTA:
If any indicators of significance have been checked, the student will be referred to the school nurse for further evaluation. Si se ha marcado cualquier indicador importante, el estudiante será remitido a la enfermera escolar para una evaluación
adicional.
Student Name: Date of Birth: Nombre del/la estudiante: Fecha de nacimiento: School: Escuela:
Please complete the following by checking off each item that may apply to your child. Por favor complete la información siguiente, marcando cada asunto que corresponda a su hijo/a.
Has no history of significant medical problems. No tiene historial de problemas médicos importantes. Has a birth defect or developmental disability. (Ex: Spina Bifida, Intellectual Disability, Down Syndrome) Tiene una malformación congénita o discapacidad del desarrollo. (Por ejemplo: Espina bífida, Retraso mental, Síndrome de Down) Takes medication(s) which may need monitoring or administration at school. (Ex: topical, injectable, oral, inhaled, or rectal medication) Toma medicamentos que pueden necesitar ser controlados o administrados en la escuela. (Por ejemplo: medicina tópica, inyectable, oral, inhalada o rectal) Has been or presently is under the care of a doctor for a significant medical condition. (Ex: seizure condition, diabetes, uses oxygen, gastrointestinal tube, tracheostomy, acute allergic reaction) Ha estado o está al presente bajo cuidado médico por una afección médica delicada. (Por ejemplo: convulsiones, diabetes, usa oxígeno, tubo gastrointestinal, traqueostomía, reacción alérgica aguda) Has a significant physical impairment. (Ex: uses orthopedic devices or a wheelchair; has impaired vision or hearing) Tiene un impedimento físico importante. (Por ejemplo: usa aparatos ortopédicos o silla de ruedas; tiene deterioro de la visión o audición) Requires special health care procedures to be performed at school. (Ex: intermittent catheterization, suctioning, tube feeding, percussion) Requiere que se la apliquen procedimientos especiales de cuidado de la salud en la escuela. (Por ejemplo: cateterismo intermitente, succión, alimentación por tubos, percusión) Requires special medical equipment or appliances at school. (Ex: oxygen tank, feeding tubes, suctioning machine, slow volume nebulizer [svn] machine) Requiere equipo médico o aparatos especiales en la escuela. (Por ejemplo: tanque de oxígeno, tubos de alimentación, máquina de succión, máquina nebulizadora svn) Has a significant history of medical problem(s) which could affect his/her health status at school. Tiene historial de problema(s) médico(s) importantes que puede(n) afectar el estado de su salud en la escuela. Has a behavioral concern that may impact school performance. Tiene una dificultad de comportamiento que puede afectar su desempeño en la escuela.
List any concerns about your child’s health status. Indique sus inquietudes acerca del estado de salud de su hijo/a.
Parent/Guardian Signature Date Firma de un padre de familia o tutor legal Fecha
ISE-HS-017-11/17
-
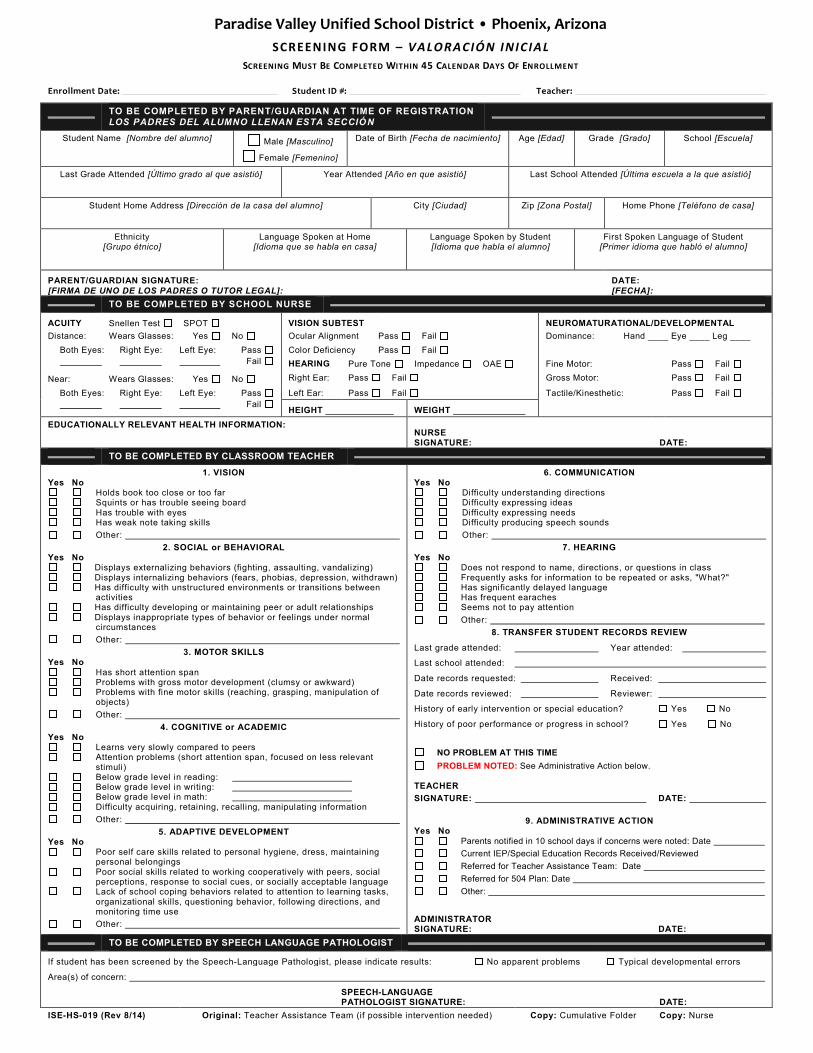
Paradise Valley Unified School District • Phoenix, Arizona SCREENING FORM – VALORACIÓN INICIAL
SCREENING MUST BE COMPLETED WITHIN 45 CALENDAR DAYS OF ENROLLMENT
Enrollment Date: Student ID #: Teacher:
TO BE COMPLETED BY PARENT/GUARDIAN AT TIME OF REGISTRATION LOS PADRES DEL ALUMNO LLENAN ESTA SECCIÓN
Student Name [Nombre del alumno] Date of Birth [Fecha de nacimiento] Age [Edad] Grade [Grado] School [Escuela] Male [Masculino]
Female [Femenino]
Last Grade Attended [Último grado al que asistió] Year Attended [Año en que asistió] Last School Attended [Última escuela a la que asistió]
Student Home Address [Dirección de la casa del alumno] City [Ciudad] Zip [Zona Postal] Home Phone [Teléfono de casa]
Ethnicity Language Spoken at Home Language Spoken by Student First Spoken Language of Student [Grupo étnico] [Idioma que se habla en casa] [Idioma que habla el alumno] [Primer idioma que habló el alumno]
PARENT/GUARDIAN SIGNATURE: DATE: [FIRMA DE UNO DE LOS PADRES O TUTOR LEGAL]: [FECHA]:
TO BE COMPLETED BY SCHOOL NURSE
ACUITY Snellen Test SPOT VISION SUBTEST NEUROMATURATIONAL/DEVELOPMENTAL Distance: Wears Glasses: Yes No Ocular Alignment Pass Fail Dominance: Hand ____ Eye ____ Leg ____
Both Eyes: Right Eye: Left Eye: Pass Color Deficiency Pass Fail Fail HEARING Pure Tone Impedance OAE Fine Motor: Pass Fail
Near: Wears Glasses: Yes No Right Ear: Pass Fail Gross Motor: Pass Fail
Both Eyes: Right Eye: Left Eye: Pass Left Ear: Pass Fail Tactile/Kinesthetic: Pass Fail Fail HEIGHT WEIGHT
EDUCATIONALLY RELEVANT HEALTH INFORMATION: NURSE SIGNATURE: DATE:
TO BE COMPLETED BY CLASSROOM TEACHER 1. VISION 6. COMMUNICATION
Yes No Yes No Holds book too close or too far Difficulty understanding directions Squints or has trouble seeing board Difficulty expressing ideas Has trouble with eyes Difficulty expressing needs Has weak note taking skills Difficulty producing speech sounds Other: Other:
2. SOCIAL or BEHAVIORAL 7. HEARING Yes No Yes No
Displays externalizing behaviors (fighting, assaulting, vandalizing) Does not respond to name, directions, or questions in class Displays internalizing behaviors (fears, phobias, depression, withdrawn) Frequently asks for information to be repeated or asks, "What?" Has difficulty with unstructured environments or transitions between Has significantly delayed language activities Has frequent earaches Has difficulty developing or maintaining peer or adult relationships Seems not to pay attention Displays inappropriate types of behavior or feelings under normal Other: circumstances 8. TRANSFER STUDENT RECORDS REVIEW Other:
Last grade attended: Year attended: 3. MOTOR SKILLS Yes No Last school attended:
Has short attention span Date records requested: Received: Problems with gross motor development (clumsy or awkward)
Problems with fine motor skills (reaching, grasping, manipulation of Date records reviewed: Reviewer: objects)
History of early intervention or special education? Yes NoOther:
History of poor performance or progress in school? Yes No4. COGNITIVE or ACADEMIC Yes No
Learns very slowly compared to peers NO PROBLEM AT THIS TIME Attention problems (short attention span, focused on less relevant stimuli) PROBLEM NOTED: See Administrative Action below. Below grade level in reading: Below grade level in writing: TEACHER Below grade level in math: SIGNATURE: DATE: Difficulty acquiring, retaining, recalling, manipulating information Other: 9. ADMINISTRATIVE ACTION
Yes No Yes No
5. ADAPTIVE DEVELOPMENT Parents notified in 10 school days if concerns were noted: Date
Poor self care skills related to personal hygiene, dress, maintaining Current IEP/Special Education Records Received/Reviewed personal belongings Referred for Teacher Assistance Team: Date Poor social skills related to working cooperatively with peers, social
Referred for 504 Plan: Date perceptions, response to social cues, or socially acceptable language Lack of school coping behaviors related to attention to learning tasks, Other: organizational skills, questioning behavior, following directions, and monitoring time use
ADMINISTRATOR Other: SIGNATURE: DATE: TO BE COMPLETED BY SPEECH LANGUAGE PATHOLOGIST
If student has been screened by the Speech-Language Pathologist, please indicate results: No apparent problems Typical developmental errors
Area(s) of concern:
SPEECH-LANGUAGE PATHOLOGIST SIGNATURE: DATE:
ISE-HS-019 (Rev 8/14) Original: Teacher Assistance Team (if possible intervention needed) Copy: Cumulative Folder Copy: Nurse

Parents of new students: Please fill out form in its entirety. A los padres de los alumnos nuevos: Favor de llenar completamente este formulario. Parents of returning students: Make corrections to pre-printed information in shaded area below each proper section, complete reverse side, date and sign card, and return to the classroom teacher. NOTE: Registration and enrollment requirements are NOT satisfied until this emergency card is completed, signed by the parent/guardian and on file in the health office. Grades will NOT BE RECORDED for students with incomplete registration status. A los padres de alumnos que regresan nuevamente con nosotros: Si tienen cambios, favor de hacer las correcciones en el espacio sombreado indicado abajo de la información impresa que desean cambiar, completen el reverso de la hoja con su firma y fecha en que firmaron y devuelvan al maestro. NOTA IMPORTANTE: NO quedará completa la inscripción ni los requisitos de inscripción hasta que dicho formulario esté llenado debidamente con firma del padre de familia o tutor legal y se encuentre en el expediente del alumno en la enfermería de la escuela. Las calificaciones del alumno NO QUEDARÁN registradas mientras que la inscripción permanezca en estatus incompleto.
Student Last Name Apellido del alumno Student First Name Nombre del alumno Student Middle Name Segundo nombre del alumno
Date of Birth Fecha de nacimiento
Gender Sexo
Student # # ident. del alumno
School # # de la escuela
Grade Grado
Teacher Name Nombre maestro(a)
Student Home Address Dirección del alumno City Ciudad Zip Code Zona postal Primary Phone Teléfono principal Student Cell Phone Teléfono celular del alumno
Parent/Guardian Last Name Apellido de uno de los padres o tutor legal
Parent/Guardian First Name Nombre de este padre o tutor legal
Parent/Guardian Last Name Apellido de uno de los padres o tutor legal
Parent/Guardian First Name Nombre de este padre o tutor legal
Parent/Guardian Relationship Relación con el alumno de este padre o tutor legal
☐ Father ☐ Mother ☐ Stepparent ☐ Guardian ☐ Fosters ☐ Other
☐ Padre ☐ Madre ☐ Padrastro/a ☐ Tutor legal ☐ Padres de crianza ☐ Otro
Parent/Guardian Relationship Relación con el alumno de este padre o tutor legal
☐ Father ☐ Mother ☐ Stepparent ☐ Guardian ☐ Fosters ☐ Other
☐ Padre ☐ Madre ☐ Padrastro/a ☐ Tutor legal ☐ Padres de crianza ☐ Otro
Parent/Guardian Address Dirección del padre/tutor legal City Ciudad State Estado Zip Code Zona postal Parent/Guardian Address Dirección del padre/tutor legal City Ciudad State Estado Zip Code Zona postal
☐ Same as above La misma de arriba ☐ Same as above La misma de arriba
Home Phone Teléfono de la casa
Cell Phone Teléfono celular
Work Phone Teléfono del trabajo
E-Mail Address Dirección de correo electrónico
Home Phone Teléfono de la casa
Cell Phone Teléfono celular
Work Phone Teléfono del trabajo
E-Mail Address Dirección de correo electrónico
Parent Marital Status Estado civil de los padres ☐ Single Solteros ☐ Married Casados ☐ Divorced Divorciados ☐ Separated Separados ☐ Widowed Viuda/o ☐ Other Otro
Student Lives With: El alumno vive con: ☐ Both Parents Ambos padres ☐ Father Padre ☐ Mother Madre ☐ Guardian Tutor legal ☐ Foster Padres de crianza ☐ Other Otro
Custody Papers/Court Order Documentos de custodia/Orden judicial ☐ Joint Conjunta ☐ Father Padre ☐ Mother Madre ☐ Guardian Tutor legal ☐ State Estado ☐ Temporary Temporal ☐ Other Otro
Emergency Contact/Release Designee (Other than Parent/Guardian) Personas de contacto en caso de emergencia/Autorizadas para recoger al alumno (además de los padres o tutores legales)
Last Name Apellido First Name Nombre Relationship Relación Gender Sexo Home Phone Teléfono de la casa Cell Phone Teléfono celular Work Phone Teléfono del trabajo
Last Name Apellido First Name Nombre Relationship Relación Gender Sexo Home Phone Teléfono de la casa Cell Phone Teléfono celular Work Phone Teléfono del trabajo
Last Name Apellido First Name Nombre Relationship Relación Gender Sexo Home Phone Teléfono de la casa Cell Phone Teléfono celular Work Phone Teléfono del trabajo
First and Last Name of Primary Healthcare Provider for Child Nombre y apellido del proveedor de servicios médicos del alumno
Health Insurance Plan Plan de seguro médico
Healthcare Provider Phone Número de teléfono del proveedor de servicios médicos
Preference of Local Hospital Preferencia de hospital local
Please provide the following information for brothers/sisters of this student. Proporcione a continuación la información correspondiente a los hermanos/hermanas de este alumno.
Last Name Apellido First Name Nombre Birth Date Fecha de nacimiento Grade Grado School Attending Escuela a la que asiste
1.
2.
3.
PVSCHOOLS STUDENT EMERGENCY CARD • TARJETA DE EMERGENCIA DEL ALUMNO Complete and Sign Reverse Side » Llene y frme el reverso »ISE-HS-013 (Rev 11/01/17)

PVSCHOOLS STUDENT EMERGENCY CARD • TARJETA DE EMERGENCIA DEL ALUMNO
Student Name Nombre del alumno: Grade Grado:
EMERGENCY CARDS ARE NOT RETAINED FROM ONE SCHOOL YEAR TO THE NEXT. The following information must be completed EVERY SCHOOL YEAR to update your student’s health records.LAS TARJETAS DE EMERGENCIA NO SE GUARDAN DE UN AÑO LECTIVO A OTRO. La siguiente información debe completarse CADA AÑO LECTIVO para actualizar los archivos de salud de su alumno.
Please check ONGOING if your child has any of the following health condition(s). If the condition is NEWLY DIAGNOSED this school year and/or not previously reported to the school nurse, please check NEW. Marque ONGOING Continua si su hijo tiene cualquiera de las enfermedades o afecciones que se indican a continuación. Si se trata de una enfermedad o afección nueva que le diagnosticaron este año, o de la que no se ha informado antes a la enfermera escolar, marque NEW Nueva.
HEALTH CONDITION NEW ONGOING HEALTH CONDITION NEW ONGOING HEALTH CONDITION NEW ONGOING Enfermedad o Afección Nueva Continua Enfermedad o Afección Nueva Continua Enfermedad o Afección Nueva Continua
Other health condition / information pertinent to the care of your student
Otra afección de salud o información relacionada con el cuidado de su hijo
Medication Medicamento
Dosage Dosis
Frequency Frecuencia
1.
2.
3.
4.
5.
6.
Daily Medication Regimen Plan Diario de Medicamentos
Hearing/Ear Disorder Afección de la audición/el oído • Hearing aids/ Cochlear Implant
aparatos para audición/Implante coclear
Heart Condition Afección cardíaca
Neuro Disorder (includes migraines) Afección neurológica (incluye migrañas)
Orthopedic Disorder Afección ortopédica
Seizure Disorder Enfermedad convulsiva
Vision/Eye Disorder Afección de la visión/los ojos • Glasses/contacts
Anteojos/lentes de contacto
ADD/ADHD Defcit de atención/con hiperactividad
Allergies Alergias • To Food a alimentos
List: Enumere:
• To Insect stings/bites a picaduras de insectos
• To Latex al material látex • To Medication(s) a medicamentos
List: Enumere:
· To Animals a animales • Seasonal por la estación • Life Threatening peligro de muerte
List: Enumere:
Arthritis/Rheumatic Disease Artritis/enfermedad reumática
Asthma Asma
Autism Autismo
Birth Defect/Developmental Disorder Defectos de na-cimiento/problemas de desarrollo
Bleeding Disorder Trastorna de sangrado Specify: Especifque:
☐ ☐
☐ ☐ ☐ ☐ ☐
☐ ☐ ☐
☐
☐
☐
☐ ☐
☐ ☐ ☐ ☐ ☐
☐ ☐ ☐
☐
☐
☐
☐
☐
☐
☐
Cancer Cáncer
Cystic Fibrosis Fibrosis quística
Diabetes – Type 1 Diabetes – Tipo 1
Diabetes – Type 2 Diabetes – Tipo 2
Emotional/Psychiatric Disorder Afección emocional/psiquiátrica • Depression Depresión • Bipolar Bipolar • Anxiety Ansiedad • Eating Disorder
Trastorno alimentario • Other Otro
Specify: Especifque:
Endocrine Disorder Enfermedad del sistema endocrino Specify: Especifque:
Gastrointestinal Disorder Enfermedad gastrointestinal Specify: Especifque:
Genitourinary Disorder Enfermedad genitourinaria Specify: Especifque:
☐ ☐
☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐
☐
☐
☐ ☐
☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐
☐
☐
☐ ☐
☐ ☐ ☐
☐ ☐
☐
☐
☐
☐ ☐
☐
☐ ☐ ☐ ☐ ☐
PARENT/GUARDIAN SIGNATURE ON THIS CARD ACKNOWLEDGES THE FOLLOWING La firma de uno de los padres/tutor legal en esta tarjeta indica lo siguiente: 1. It is the responsibility of the parent/guardian to update information on this emergency card with appropriate documentation as changes occur.
Es responsabilidad de uno de los padres/tutor legal mantener al día la tarjeta de emergencia, con la documentación apropiada, cuando haya algún cambio. 2. Person(s) listed as emergency contact(s) are permitted to pick up student from school.
Las personas indicadas como contacto en una emergencia, pueden recoger de la escuela a este alumno. 3. By signing the Emergency/Information Card and providing your phone number, you are authorizing the school and/or Paradise Valley Unified School District to deliver or cause to be delivered information and notifications regarding your child, the school, and the District via autodialed calls or prerecorded calls. You may request to be removed from future notifications at any time by calling or emailing the school/District or using the opt-out feature
when you receive a call. Al firmar la Tarjeta de Información para contactar a los padres en casos de Emergencia y proporcionando su número telefónico, ustedes autorizan que la escuela y el Distrito Escolar Unificado Paradise Valley envíe o cause el
envío de información y notificaciones con respecto a su hijo/a, a la escuela y al distrito escolar por media de llamadas automatizadas o mensajes pregrabadas. Ustedes pueden solicitar en cualquier momento dejar de recibir futuras notificaciones llamando o enviando un correo electrónico a la escuela o el distrito escolar u oprimiendo la opción indicada cuando reciban una llamada automatizada.
4. In the event of an accident or illness when authorization for medical treatment cannot be obtained from parent or personal physician, the undersigned gives permission and assumes full responsibility for the school nurse and/or the school administrator to call for emergency medical assistance, including ambulance service.
En caso de un accidente o enfermedad y cuando no se pueda obtener autorización de los padres o del médico personal para tratamiento, la persona abajo firmante autoriza y asume la responsabilidad para que la enfermera y/o un miembro del personal administrativo de la escuela obtengan ayuda médica de emergencia, incluyendo servicio de ambulancia.
5. To assure the safety and well-being of my child, the school nurse has permission to share pertinent health concerns with appropriate school personnel. A fin de garantizar la seguridad y bienestar de mi hijo(a), la enfermera tiene permiso para informar al personal apropiado de la escuela cualquier inquietud sobre su salud.
6. Registration and enrollment for the current school year is incomplete until this emergency card and the Release Consent and Acknowledgment form have been completed and signed by the parent/guardian and returned to the school.
La inscripción y matrícula para el año lectivo actual estarán incompletas, hasta que uno de los padres de familia o tutor legal llene y firme, al igual que el alumno, esta tarjeta de emergencia y el Acuerdo de Autorización de los padres, y los devuelvan a la escuela.
PARENT/GUARDIAN SIGNATURE (IN INK) Date Firma de uno de los padres/tutor legal (en tinta) Fecha
ISE-HS-013 (Rev 11/01/17)

________________________________________________________
________________________________________________________
STUDENT NAME STUDENT ID GRADE
SCHOOL TEACHER PERIOD
RELEASE, CONSENT, AND ACKNOWLEDGEMENT FORM FOR PARENTS AND GUARDIANS IN PV SCHOOLS
In order to provide information about PVSchools programs and operations to our parents and the general public, it’s necessary to include information, photos and/or video of our students’ enrollment and participation in our schools. This document allows an opportunity to opt out or include your student in our communications to keep everyone in our community better informed on the opportunities and achievements of our District. Additionally, this document affirms acknowledgement of the PVSchools Parent Student Handbook. If this form is not returned, school enrollment will not be considered complete.
I hereby grant permission to the Paradise Valley Unified School District (the “District”) and its employees to record and use the student’s image or performance on video, photograph or any other medium (the ”Recordings”) for the purpose of promotion or any other appropriate use as determined by the District and that the District deems necessary. I also give the District permission to use, modify, and distribute the Recordings, in whole or in part, in any media, including but not limited to print, broadcast or the Internet.
I hereby release the District and its legal representatives for any and all claims related to my child’s Recordings for editorial, publicity, or other purposes. I waive the right to inspect or approve any finished product, including written or electronic, wherein my child’s Recordings appear. I waive any and all right to royalties or other compensation from the District associated with District use of the materials listed above.
I hereby certify that I am a legal adult and a parent or legally appointed guardian of the student, and have the right to make decisions for the minor in the above regard. I state further that I have read the above authorization, release, and agreement and that I am fully familiar with the contents of it. This release shall be binding upon the student and me, and our legal representatives.
Once signed and dated this Release and Consent Agreement shall remain in effect until rescinded. This release may be rescinded by the legal parent or guardian of the student at any time by submitting a formal written request directly to your school principal. Any recording of the student made prior to the withdrawal of the release will remain the property of the District subject to the provisions and terms listed in the Release, Consent, and Acknowledgement Form.
If you give consent for student to be photographed or recorded for district purposes, sign and date this form on reverse side.
_____ I DO NOT grant permission for my student to be photographed or recorded for district purposes.
PV SCHOOLS OUTSIDE MEDIA RELEASE AND CONSENT AGREEMENT
If you give consent for student’s video/photo to be used in school related activities by representatives of the media (which could include television), sign and date on reverse side. This does not include athletic events, which are considered public events.
_____ I DO NOT grant permission for my student to be photographed or recorded by representatives of the media. (OVER)

______________________________________ _____________________________________________
______________________________________ _____________________________________________
DIRECTORY INFORMATION I hereby give consent for the release of student directory information as it applies to school related activities and programs such as: athletics, musical programs, honors and awards, drama productions, commencement, parent/teacher organizations, etc. This does not apply to confidential student records. Directory information includes student's name, address, telephone, email, date and place of birth, major field of study, dates of attendance, participation in officially recognized activities and sports, weight and height of members of athletic teams, and awards received.
Consent for the release of directory will remain in effect for the current school year or until permission is revoked by the parents, requested in writing, to the school principal. Further details regarding the release of directory information may be secured by contacting the school office, the PV Schools Parent Student Handbook, and the PV Schools website.
Directory Information If you give consent to the release of directory information, sign and date this form below.
_____ I DO NOT grant permission for the release of directory information. I understand information will not be released to school organizations and school approved vendors.
Yearbook If you give consent to including your child’s photo in the yearbook, sign and date this form below.
_____ I DO NOT grant permission for the school to include a picture of my child in the yearbook. I understand my child will NOT be included in the school yearbook.
Military Recruitment (High School Only) If you give consent to release your child’s information to military recruiters sign and date this form below (High School Only).
_____ I DO NOT grant permission for the school to release information regarding my high school student to military recruiters.
Higher Education (High School Only) If you give consent to release your child’s information to institutes of higher education sign and date this form below (High School Only).
_____ I DO NOT grant permission for the school to release information regarding my high school student to institutions of higher education.
Parent Student Handbook Acknowledgement
By signing below, I am acknowledging that I am aware that the PVSchools Parent Student Handbook is available to both parents and students on the district website (www.pvschools.net) and individual school websites. The handbook includes district and school policies and procedures and includes the district’s code of conduct and attendance procedures. Hard copies of the handbook are available upon request at any school site. Student signature is also required on this form to confirm awareness and agreement to abide by the rules and expectations contained in the district handbook. Parents should review content with student, especially with a younger child. As parent or legal guardian, I acknowledge and verify the information required on this form.
Print Parent Name Parent Signature Date
Print Student Name Student Signature Date

______________________________________________________________________________________________
Paradise Valley Unified School District Residency Questionnaire
School name:_______________________________________________________________________
Student Name(s): ___________________________________________________________________ Last First Middle Initial
Date Of Birth: __________________________ _________________ _______________________________ Month/Day/Year Grade Student I.D.
This questionnaire is intended to address the McKinney-Vento Act (42 U.S.C. 11431 et seq.). The answers to this residency information help to determine the services the student may be eligible to receive. Eligibility must be reviewed and reevaluated every school year.
1. Is your current address a temporary living arrangement? Yes ______ No ______ 2. If temporary, is this living arrangement due to loss of housing or economic hardship? Yes ______ No ______
If you answered YES to questions 1 and 2, please complete the remainder of this form. If you answered NO to either question, you do not need to complete the remainder of this form.
Where is the student presently living? (Check One) _____ In a hotel/motel _____ In a homeless shelter _____ With more than one family in a house or apartment _____ In a place not ordinarily used for sleeping (car, park, etc.)
Name of Parent(s)/Legal Guardian(s): _______________________________________________________________
Address: __________________________________________________________________ Zip _________________
Phone: ____________________________________ How long have you lived at current address: _______________
By signing, I attest that this information is true and accurate.
Parent/Legal Guardian ____________________________________________ Date __________________________
For Office Staff: Do not make copies of this form. If numbers 1 or 2 are checked, please send the completed form to Kathy Nell at Title 1-DAC. [email protected] Per McKinney-Vento guidelines, a copy should not be placed in the
student’s cumulative file. Please shred any forms that do not have check marks in 1 or 2.