purpose to decrease the number of ventilator-associated pneumonias (vap) at the smbd-jgh
TRANSCRIPT

PurposePurpose
To decrease the number of To decrease the number of Ventilator-Associated Ventilator-Associated Pneumonias (VAP) at the Pneumonias (VAP) at the SMBD-JGHSMBD-JGH

PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs
7.7. Education/supportEducation/support


PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs
7.7. Education/supportEducation/support


PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its Evidence supporting its claimsclaims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs
7.7. Education/support Education/support

Absolute Absolute Attributable Attributable MortalityMortality5.8% (-2.4, 14.0)5.8% (-2.4, 14.0)
Relative Risk Relative Risk IncreaseIncrease32.3% (-20.6, 85.1)32.3% (-20.6, 85.1)
Attributable LOSAttributable LOS4.3 days (1.5, 7.0)4.3 days (1.5, 7.0)
Effect varies across Effect varies across subgroupssubgroups
23,7
1917,9
14
%Mortality ICU LOS(days)
Cases Controls
The Attributable The Attributable Morbidity and Mortality Morbidity and Mortality of VAPof VAP
Heyland Am J Resp Crit Care Med 1999;159:1249

Pneumonia in the ICUPneumonia in the ICU . . Rello J, Crit Care Med 2003 31:2544-51

Evidence: Valles 1995Evidence: Valles 1995
Setting: Setting: Medical-surgical ICU. Medical-surgical ICU. Patients: Patients: 190 admitted to ICU during a 33-month period and whose 190 admitted to ICU during a 33-month period and whose
condition suggested the need for prolonged intubation (>3 days). condition suggested the need for prolonged intubation (>3 days). Intervention: Intervention: 76 patients randomly allocated to receive CASS, 77 control 76 patients randomly allocated to receive CASS, 77 control
patients allocated to usual care. patients allocated to usual care. Results: Results: CASS vs Controls CASS vs Controls
– 19.9 vs 39.6 episodes/1000 ventilator days (relative risk, 1.98; 95% CI, 1.03-19.9 vs 39.6 episodes/1000 ventilator days (relative risk, 1.98; 95% CI, 1.03-3.82)3.82)
– VAP occurred later in CASS pts 12.0 +/-7.1 days vs 5.9 +/-2.1 days (P = 0.003). VAP occurred later in CASS pts 12.0 +/-7.1 days vs 5.9 +/-2.1 days (P = 0.003). – The same microorganisms isolated from protected specimen brush or The same microorganisms isolated from protected specimen brush or
bronchoalveolar lavage cultures in patients with VAP were previously isolated bronchoalveolar lavage cultures in patients with VAP were previously isolated from cultures of subglottic secretions in 85% of cases.from cultures of subglottic secretions in 85% of cases.
Conclusions: Conclusions: The incidence of nosocomial pneumonia in mechanically The incidence of nosocomial pneumonia in mechanically ventilated patients can be significantly reduced by using a simple method ventilated patients can be significantly reduced by using a simple method
that decreases the chronic microaspirations through the cuff of ETTs.that decreases the chronic microaspirations through the cuff of ETTs.



5 studies , 896 patients.
Subglottic secretion drainage reduced the incidence of VAP by nearly half (risk ratio [RR] 0.51; 95% CI 0.37 to 0.71), primarily by reducing early-onset pneumonia (pneumonia occurring within 5 to 7 days after intubation).
CASS shortened – duration of mechanical ventilation by 2 days (95% CI:
1.7-2.3 days) – ICU length of stay by 3 days (95% CI: 2.1 to 3.9 days)– delayed the onset of pneumonia by 6.8 days (95% CI: 5.5
to 8.1 days).

Conclusion: Subglottic secretion drainage appears effective in preventing early-onset VAP among patients expected to require 72 hours of mechanical ventilation.

www.ahrq.govwww.ahrq.gov



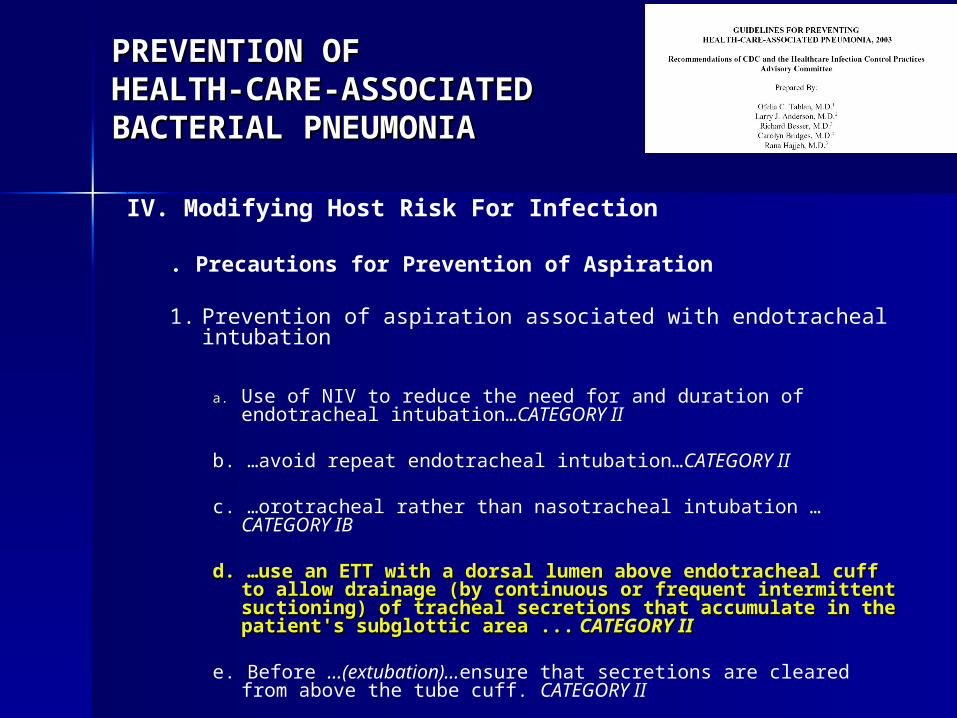
PREVENTION OFPREVENTION OFHEALTH-CARE-ASSOCIATED HEALTH-CARE-ASSOCIATED BACTERIAL PNEUMONIABACTERIAL PNEUMONIA
IV. Modifying Host Risk For Infection
. Precautions for Prevention of Aspiration
1. Prevention of aspiration associated with endotracheal intubation
a. Use of NIV to reduce the need for and duration of endotracheal intubation…CATEGORY II
b. …avoid repeat endotracheal intubation…CATEGORY II
c. …orotracheal rather than nasotracheal intubation …CATEGORY IB
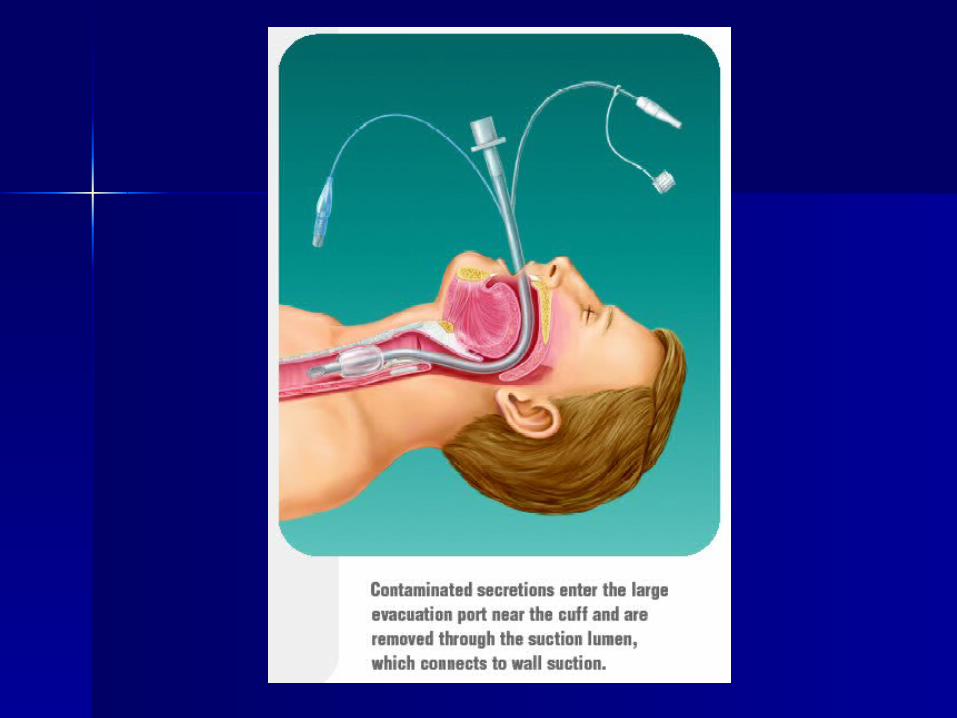
d. …use an ETT with a dorsal lumen above endotracheal cuff d. …use an ETT with a dorsal lumen above endotracheal cuff to allow drainage (by continuous or frequent intermittent to allow drainage (by continuous or frequent intermittent suctioning) of tracheal secretions that accumulate in the suctioning) of tracheal secretions that accumulate in the patient's subglottic area ...patient's subglottic area ... CATEGORY II CATEGORY II
e. Before …(extubation)…ensure that secretions are cleared from above the tube cuff. CATEGORY II

Am J Respir Crit Care Med Am J Respir Crit Care Med
Vol 171. pp 388–416, 2005Vol 171. pp 388–416, 2005

Major Points and Recommendations for Modifiable Risk FactorsIntubation and mechanical ventilation.
1. Intubation and reintubation should be avoided, if possible, as it increases the risk of VAP (Level I)
2. Noninvasive ventilation should be used whenever possible in selected patients with respiratory failure (Level I)
3. Orotracheal intubation and orogastric tubes are preferred over nasotracheal intubation and nasogastric tubes to prevent nosocomial sinusitis and to reduce the risk of VAP, although direct causality has not been proved (Level II)
4. Continuous aspiration of subglottic secretions can reduce the risk of Continuous aspiration of subglottic secretions can reduce the risk of early-onset VAP, and should be used (Level I) early-onset VAP, and should be used (Level I)
5. The ETT cuff pressure should be maintained at > 20 cm H2O to prevent leakage of bacterial pathogens around the cuff into the lower respiratory tract (Level II)
6. Contaminated condensate should be carefully emptied from ventilator circuits and condensate should be prevented from entering either the endotracheal tube or inline medication nebulizers (Level II)
7. Passive humidifiers or HMEs decrease ventilator circuit colonization, but have not consistently reduced the incidence of VAP, and thus they cannot beregarded as a pneumonia prevention tool (Level I)
8. Reduced duration of intubation and mechanical ventilation may prevent VAP and can be achieved by protocols to improve the use of sedation and to accelerate weaning(Level II)
9. Maintaining adequate staffing levels in the ICU can reduce length of stay, improve infection control practices, and reduce duration of mechanical ventilation (Level II)

Purpose: To develop an evidence-based guideline for VAP prevention
Subglottic Secretion DrainageOn the basis of evidence from five level 2 trials, we conclude that subglottic secretion drainage is associatedwith decreased incidence of VAP, especially early onsetVAP.Status: We recommend that clinicians consider the Status: We recommend that clinicians consider the use ofuse ofsubglottic secretion drainage.subglottic secretion drainage.
Ann Intern Med. 2004;141:305-313

Pneumonia Prevention in the ICUPneumonia Prevention in the ICU
Rello J, Crit Care Med 2003 31:2544-51Rello J, Crit Care Med 2003 31:2544-51

PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs
7.7. Education/supportEducation/support

OPPORTUNITIESOPPORTUNITIES
Decrease the rate of ventilator-Decrease the rate of ventilator-associated pneumonia (VAP) associated pneumonia (VAP)
Improve ICU access by reducing Improve ICU access by reducing hospital-related LOS from VAPhospital-related LOS from VAP
Potential to decrease mortality and Potential to decrease mortality and costs associated with development of costs associated with development of VAP, especially if earlier extubation. VAP, especially if earlier extubation.

OPPORTUNITIESOPPORTUNITIES
CALCULATIONCALCULATION$ COST $$ COST $
~~600 intubations/yr in ICU + ED + Wards (code blue etc)600 intubations/yr in ICU + ED + Wards (code blue etc)~600 intubations/yr in OR who would qualify for ventilation ~600 intubations/yr in OR who would qualify for ventilation
> 48 hrs> 48 hrs= 1200 intubations/yr = 1200 intubations/yr who would qualify for ventilation > 48 who would qualify for ventilation > 48
hourshours
Conventional JGH ETT: $1.88/ETTConventional JGH ETT: $1.88/ETTEVAC : $7.25/ETTEVAC : $7.25/ETT
Differential increment in costDifferential increment in cost = $5.375/ETT= $5.375/ETT= 1200 X $5.375 = = 1200 X $5.375 = $6450 /yr$6450 /yr

OPPORTUNITIESOPPORTUNITIESCALCULATIONCALCULATION
BENEFIT = ICU BENEFIT = ICU ACCESSIBILITYACCESSIBILITY
A 30% decrease in VAP at the JGH ICU would = A 30% decrease in VAP at the JGH ICU would = 14 pneumonias prevented14 pneumonias prevented
If the attributable ICU LOS/VAP = 4.3 days,If the attributable ICU LOS/VAP = 4.3 days,4.3d X 14 prevented VAP = 4.3d X 14 prevented VAP = 60 ICU days60 ICU days preventedprevented, , or or accessibleaccessible for other for other patientspatients
Cost Cost = $6450/60days = $108/ICU day made accessible= $6450/60days = $108/ICU day made accessibleEquivalent to costs of treating the prevented VAPs !Equivalent to costs of treating the prevented VAPs !

Indications for EVAC in the Indications for EVAC in the OROR
Oxygen therapy prior to surgeryOxygen therapy prior to surgery– Chronically (at home)Chronically (at home)– AcutelyAcutely
Emergency cardiothoracic or upper abdominal surgeryEmergency cardiothoracic or upper abdominal surgery(< 24 hours of admission/incident)(< 24 hours of admission/incident)
Depressed level of consciousness pre-op (non-med-related)Depressed level of consciousness pre-op (non-med-related)
Cardiovascular surgeryCardiovascular surgery– circulatory arrest contemplatedcirculatory arrest contemplated– CV surgery combined with non-cardiac surgeryCV surgery combined with non-cardiac surgery– Intraoperative insertion of Intra Aortic Blood Pump (IABP) Intraoperative insertion of Intra Aortic Blood Pump (IABP) – Crash intubation in the Cardiac Catheterization LabCrash intubation in the Cardiac Catheterization Lab– major aortic reconstructionmajor aortic reconstruction– + acute preoperative renal failure+ acute preoperative renal failure
At the discretion of anesthetist when a rocky post-op course is At the discretion of anesthetist when a rocky post-op course is foreseenforeseen

PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems6.6. Product SpecsProduct Specs
7.7. Education/support Education/support
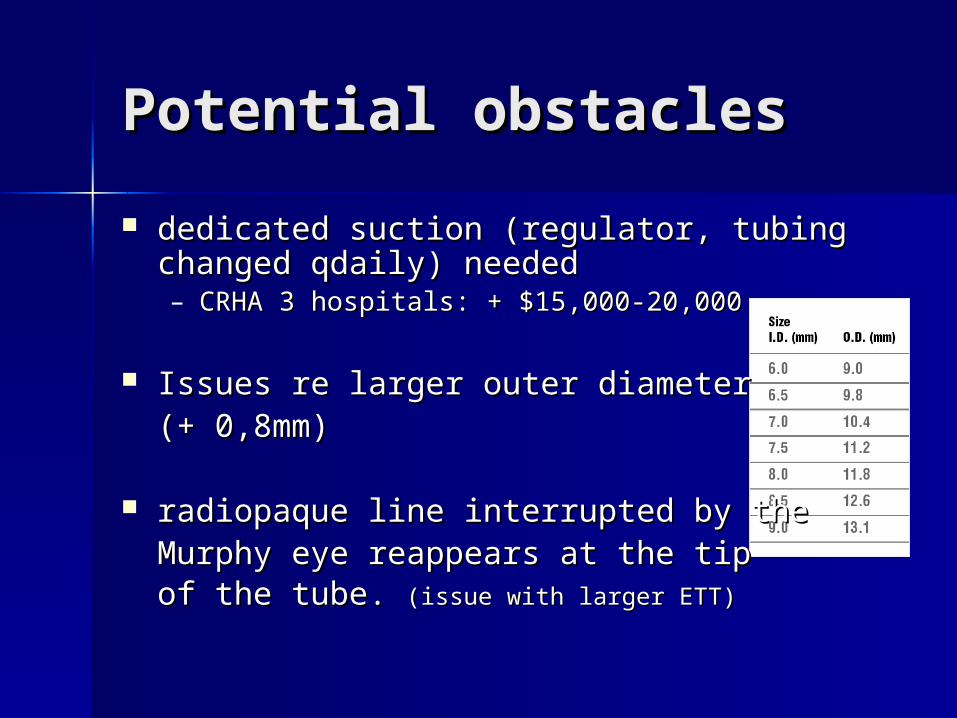
Potential obstaclesPotential obstacles
dedicated suction (regulator, tubing changed dedicated suction (regulator, tubing changed qdaily) neededqdaily) needed– CRHA 3 hospitals: + $15,000-20,000 CRHA 3 hospitals: + $15,000-20,000
Issues re larger outer diameter Issues re larger outer diameter (+ 0,8mm)(+ 0,8mm)
radiopaque line interrupted by the radiopaque line interrupted by the Murphy eye reappears at the tip Murphy eye reappears at the tip of the tube. of the tube. (issue with larger ETT)(issue with larger ETT)

PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs7.7. Education/supportEducation/support

Product SpecsProduct Specs
MaintainMaintain– Suction @ < 20-30 torrSuction @ < 20-30 torr
MonitorMonitor– EVAC lumen patency (air EVAC lumen patency (air
flush)flush)– ETT cuff pressureETT cuff pressure

PLANPLAN
1.1. What it looks likeWhat it looks like
2.2. How it worksHow it works
3.3. Evidence supporting its claimsEvidence supporting its claims
4.4. Opportunities for the JGHOpportunities for the JGH
5.5. Potential problemsPotential problems
6.6. Product SpecsProduct Specs
7.7. Education/supportEducation/support

Education, SupportEducation, Support
Canadian CollaborativeCanadian Collaborative– Experience, protocols etc.Experience, protocols etc.
ManufacturerManufacturer– VideoVideo ((Silent Aspiration AW04398)Silent Aspiration AW04398)
– ChecklistChecklist– In-servicingIn-servicing– ProtocolsProtocols available from 4 other available from 4 other
centerscenters

