pukwana ya kganya - mykganya.com · groblersdal po box 1438 groblersdal, 0470 tel: 013 262 3013 fax...
TRANSCRIPT

Pukwanaya Kganya
Claim Form
The Member is our most important asset. As a group, they loyally support Kganya by paying contributions regularly in the knowledge that one day a claim will be submitted. That day has now arrived and you as claimant deserve to be assisted in the most efficient and sympathetic way.
It is our duty as Kganya to make sure that the claims process is as smooth and simple as possible. This Pukwana ya Kganya Personal Accident Claim Form has been created with this in mind.
Please accept our sympathy for your accident. If you follow the process closely we will be able to guide you through this stressful time.
PERSONAL ACCIDEN
T
Z ION C HRISTIAN C HURCH
February 2018
South Africa

TO COMPLETE THE CLAIM FORM1. All the information required on the form must be provided accurately.2. The claim form must be accompanied by originals or certified copies of: • The Member’s contribution booklet (original only) as well as previous contribution booklets held, • A Personal Accident Medical Report, • The Member’s Identity Document, • Verification of the bank account number and branch code for the Member / beneficiary in the event that EFT claims payment option is selected.3. Kganya Benefits Fund Trust reserves the right in all cases to call for additional information where necessary to settle a claim.4. The Church Committee member completing the form must remember: • The Member must be in good standing, that is have paid a contribution in the calendar month preceding the month in which the accident occurred or in the calendar month in which the accident occurred provided the contribution was paid prior to date of the accident. • The beneficiary is the Member. • At least 3 members of the Church Committee must sign the form. • The Church Committee should always contact Kganya Insurance Administrators (Pty) Ltd (RF) office for assistance.
The form must be taken in person together with all the required documentation to one of the following Kganya Service Centres listed below. Alternatively one of the Sanlam Client Care Offices listed in the Member’s Membership Book may be used.
PERSONAL ACCIDENT CLAIM NOTIFICATION FORMIMPORTANT
AN OFFICIAL CLAIM FORM MUST BE COMPLETEDFOR EACH CLAIM AND SIGNED BY AT LEAST 3 COMMITTEE MEMBERS
PRETORIA1249 Francis Baard StreetHatfield0083PO Box 11929Hatfield, 0028Tel: 010 350 0500Fax: 087 233 0003
JOHANNESBURG1st Floor357 Rivonia BoulevardRivoniaPO Box 2876Rivonia, 2128Tel: 011 234 3448Fax: 011 234 3408
NELSPRUITOffice No 22Canary Walk Mall8 Bester Str. NorthPO Box 16386Nelspruit, 1200Tel: 013 753 2195Fax: 013 752 8205
VRYBURGOffice No 3,Wie-cla CentreCnr Market & Molopo Str.Vryburg, 8600Tel: 053 927 3229Fax: 053 927 3524
MTHATHANo. 8, LCM Ludidi Building, 63 Madiera Street, Mthatha, 5099Tel: 047 531 0039Fax: 047 531 0039
THOHOYANDOUOffice No 2, Ndou MallCnr Tshanduko & Thulamela Str.Thohoyandou, 0950Tel: 015 962 5456Fax: 015 962 6076
TZANEEN19 Danie Joubert St.Tzaneen 0850PO Box 3494Tzaneen, 0850Tel: 015 307 6887Fax: 015 307 3499
POLOKWANE26 General Joubert StreetPolokwane 0699Private Bag X9542Polokwane, 0700Tel: 015 291 5182Fax: 015 291 3005
RUSTENBURGOffice No 1 Five EFS BuildingCnr Berg & Oliver Tambo StreetsRustenburg, 0299Tel: 014 592 0505Fax: 014 592 0226
WELKOM1st Floor, ABK CentreHeeren StreetWelkomPO Box 795Welkom, 9460Tel: 057 357 1056Fax: 057 357 1057
BURGERSFORTOffice No 1, 1st Floor,Maphutha Ditshaba BuildingCnr Eddie & Church Streets,BurgersfortPO Box 3079 Burgersfort, 1150Tel: 013 231 7650Fax: 013 231 8640
MOKOPANEOffice No 22 Canary Walk Mall 8 Bester Street NorthNelspruit,1200Tel: 015 491 7651Fax: 015 491 7079
BUSHBUCKRIDGEBushbuckridge ShoppingCentre, Office No. 6ACnr Main Bushbuck &Graskop RoadsPO Box 2223Bushbuckridge, 1280Tel: 013 799 0005Fax: 013 799 0006
LOUIS TRICHARDTOffice No 10, Game CentreCNR President & Songozwi Streets, Makhado, 0920P O Box 745, Makhado 0920Tel: 015 516 7368
GIYANIShop No. 28Masingita PlazaCnr Malamulele &Main RoadsPO Box 4275Giyani, 0826Tel: 015 812 0673Fax: 015 812 0674
GROBLERSDAL7 Kruger Street, ext 2GroblersdalPO Box 1438Groblersdal, 0470Tel: 013 262 3013Fax: 013 262 5054
KLERKSDORPRoom 311ADanfor Medical CentreJersich Street No. 1OR Tambo StreetPO Box 14362Flamwood Walk, 2535KlerksdorpTel: 018 462 6009Fax: 018 462 6108

KGANYA INSURANCE ADMINISTRATORS (PTY) LTD (RF)Authorised Financial Services Provider
PERSONAL ACCIDENT CLAIM NOTIFICATION FORMIMPORTANT: In all cases the final decision as to whether or not to admit a claim rests with the Kganya Benefits Fund Trust.
Kganya Claim Number:
A: PARTICULARS OF MEMBER:
SECTION 1: TO BE COMPLETED BY MEMBER
Member’s First Names:
Member’s Surname:
Member’s ID Number:
Member’s Book Number: Contact Number:
Church Code No: Church Name:
Type of vehicle in which injured person was traveling (If applicable):
Vehicle Registration Number:
What is the nature of the injury?:
How did the accident happen?:
Name and address of hospital/clinic where injured person was treated:
Was the accident reported to the South African Police?: Yes No
Date of accident: Time of accident:D D M M Y Y :
If yes, which station:
SAPS Case Number:
Place of accident:
C: CLAIM DOCUMENTS REQUIRED TO FINALISE YOUR CLAIM:Required Included
COMPLETED PERSONAL ACCIDENT CLAIM FORM To be obtained from Church Committee and completed with their assistance. Requires the signature of at least 3 Church Committee members.
ID BOOK OF MEMBER OR CERTIFIED COPY Required in all cases. For ID cards, copy should include front and back of card.
PUKWANA YA KGANYA MEMBERSHIP BOOK Original membership book required. In certain cases previous membership books held may be required.
ID BOOK OF DEPENDENT OR CERTIFIED COPY Required where Dependent incurs a permanent disability. A birth certificate will be also be accepted. For ID cards, copy should include front and back of card.
BANK STATEMENTS OR PROOF OF BANK ACCOUNT Required where EFT payment option is selected by the Member.
COMPLETED PERSONAL ACCIDENT MEDICAL REPORT To be obtained from Church Committee and completed by a medical specialist. The form must be fully completed. Any costs or fees payable to any medical professional are for the claimant’s account.
B: PARTICULARS OF INJURED PERSON:
Injured Person’s First Names:
Injured Person’s Surname:
Injured Person’s ID Number:
Injured Person is: Member Dependant
Date: Signature:D D M M Y Y
If the injured person is a Dependant, is he/she registered in the Membership Book?: Yes No
Injured Person’s Date of Birth: D D M M Y Y Male FemaleGender of Injured Person:
Address of Injured Person:
I hereby declare that I am the Member and that the answers given to the questions are true and correct in every respect and made without reservation. I authorise any hospital, physician or other person who has attended to myself or my Dependent to furnish Kganya Insurance Administrators (Pty) Ltd (RF) or its representatives any and all information with respect to any sickness or injury, medical history, consultation, prescription or treatment and copies of all hospital or medical records. I confirm not having withheld any information which could be material to the assessment of this claim.
FEBRUARY 2018
The Kganya Benefits Fund Trust reserves the right to request any additional information required.

SECTION 3: TO BE COMPLETED BY SERVICE CENTRE MANAGER (SCM) / CLIENT CARE REPRESENTATIVE (CCR)
I confirm that: (1) other than as set out above, all claim documentation has been received and is correctly completed (2) the receipts specified above are inserted in the Membership book of the Member specified in Section 1A
D D M M Y YDate:Signed by Member:
D D M M Y YDate:Signed by SCM / CCR:
A: DETERMINATION OF GOOD STANDING:
Claim is APPROVED for payment (complete Section 3C)
Claim is PENDING
Claim is REPUDIATED (complete Section 3B)
D D M M Y YDate:Signed by SCM / CCR:
D D M M Y YDate:Signed by the Member:
I have informed the Member that the claim has been repudiated by the Kganya Benefits Fund Trust in terms of the Personal Accident Regulations on the basis set out in the Claim Repudiation Notice, a copy of which has been handed to the Member.
B: TO BE COMPLETED WHERE THE CLAIM IS REPUDIATED:
Claimant has requested the following payment option: EFT Cheque Benefit Card
Missing and/or incomplete Claim documentation
Bank Account Number / Benefit Card Number / Cheque Number :
Is all the claim documentation including Personal Accident Claim Notification Form held and correctly completed? Yes No
Were any of the Receipts shown above purchased on or after the date of Accident? Yes No
Where the Member was injured, I am able to provide visual confirmation of the injuries listed on the Personal Accident Medical Report? Yes No
C: DECLARATION BY MEMBER:
I, being the undersigned Member in respect of the claim referred to above confirm that all of the information provided by myself, including any amendments made above by the Service Centre Manager / Client Care Representative, are to the best of my knowledge correct. I confirm that I have:
Received Cheque/Card Number: For: in settlement of the claim.R
Requested EFT payment: For: in settlement of the claim.R
D D M M Y YDate:Signed by the Member:
SECTION 2: TO BE COMPLETED BY CHURCH COMMITTEE
Name: D D M M Y YSignature:
Name: D D M M Y YSignature:
Name: D D M M Y YSignature:
It is certified by the following Church Committee members that the information in Section 1 and Section 2 is to the best of our knowledge believed to be true and correct. At the date of accident the person shown in Section 1A was a Member in good standing of ZCC and has been approved by the Committee as the beneficiary. In addition, the person shown in Section 1B is known to the Committee.
Committee Position:
Z.C.C Branch File Number:
Was the injured a registered Moria Worker at the time of injury (not a volunteer)? Yes No
Was the injured a Committee member? Yes No
Was the injured a registered Youth Committee member at time of injury? Yes No
If the answer to any of the above is yes, date of appointment: D D M M Y Y
Service Centre / Client Care Office:
SCM / CCR Contact No.:
SCM / CCR Email:
D D M M Y YDate:
Show Receipts from Membership Book ending with the last sticker purchased prior
to date of accident
Type: Number: Date sold by Church:
3
1
2
Pukwanaya KganyaMedical Report
The Member is our most important asset. As a group, they loyally support Kganya by paying contributions regularly in the knowledge that one day a claim will be submitted. That day has now arrived and you as claimant deserve to be assisted in the most efficient and sympathetic way.
It is our duty as Kganya to make sure that the claims process is as smooth and simple as possible. This Pukwana ya Kganya Personal Accident Medical Report has been created with this in mind.
Please accept our sympathy for your injury. If you follow the process closely we will be able to guide you through this stressful time.
PERSONAL ACCIDEN
T
Z ION C HRISTIAN C HURCH
February 2018
South Africa

I, the undersigned, a registered Medical Specialist, whose name appears below, certify the following facts in respect of the under mentioned Patient. I am aware that the patient is liable for any costs and fees incurred in obtaining this medical report.
A: PATIENT DETAILS:
B: PARTICULARS OF INJURY:
Member’s First Names:
Member’s Surname:
Member’s ID Number:
Describe the injuries sustained?:
Date of incident:
Is the new injury the result of an accident? YES NO
Is the injury permanent and likely to affect the patient for the rest of his / her life? YES NO
Has the injury resulted in total loss or loss of use in the affected area? YES NO
In the case of loss of vision, is the loss permanent, total and irreversable? YES NO
Are any of the following applicable?
• Is the injury temporary and can the patient recover with treatment? YES NO
• Are there any pre-existing injuries or medical conditions that resulted in the new injury? YES NO
If yes, please state details:
• How long has the patient had the pre-existing injury? DAY(S) MONTH(S) YEAR(S)
• Is there any evidence of wilful exposure to danger? YES NO
• Is there any evidence of an attempt to commit suicide? YES NO
• Is the injury self-inflicted? YES NO
Which of the following categories best describes the nature of the new injury incurred?
Permanent and total quadriplegia.
Permanent and total paraplegia or the loss of two or more limbs at or above the wrist or ankle.
Permanent and total loss of speech.
Permanent and total loss of hearing in both ears.
Permanent and total loss of hearing in one ear.
Partial loss of hearing in one ear (a loss of at least 50%).
Permanent and total loss of sight in both eyes.
Permanent and total loss of sight in one eye.
Partial loss of sight in one eye (a loss of at least 50%).
Signature
Tick
Signature
Signature
Signature
Signature
Signature
Signature
Signature
Signature
PLEASE NOTE THAT THE INFORMATION FOR SECTIONS A, B AND C IS MATERIAL AND ALL QUESTIONS SHOULD BE ANSWERED ACCURATELY AND COMPREHENSIVELY
D D M M Y Y
FEBRUARY 2018
MEDICAL REPORT PERSONAL ACCIDENTTO BE COMPLETED BY A MEDICAL SPECIALIST
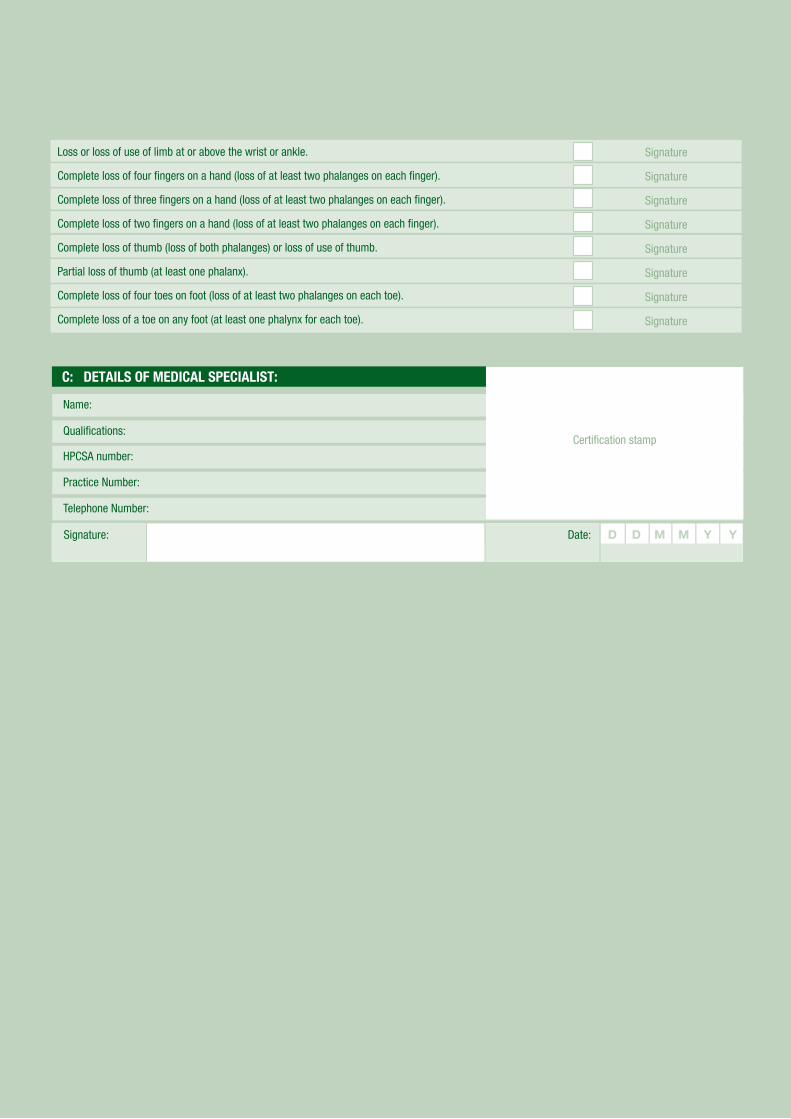
C: DETAILS OF MEDICAL SPECIALIST:
Name:
Qualifications:
HPCSA number:
Practice Number:
Telephone Number:
D D M M Y YDate:Signature:
Certification stamp
Signature
Signature
Signature
Signature
Signature
Signature
Signature
Signature
Loss or loss of use of limb at or above the wrist or ankle.
Complete loss of four fingers on a hand (loss of at least two phalanges on each finger).
Complete loss of three fingers on a hand (loss of at least two phalanges on each finger).
Complete loss of two fingers on a hand (loss of at least two phalanges on each finger).
Complete loss of thumb (loss of both phalanges) or loss of use of thumb.
Partial loss of thumb (at least one phalanx).
Complete loss of four toes on foot (loss of at least two phalanges on each toe).
Complete loss of a toe on any foot (at least one phalynx for each toe).