pueblo v-1-2 office-print 24jun -...
TRANSCRIPT
....continued from page 2 Acid Reflux and IBS
Diet and lifestyle changes that reduce stress should benefit both IBS and GERD. An elimination diet that starts with very bland and simple foods, and then introduces new food groups in stages, may help identify foods that trigger symptoms. Each condition may also be treated separately with medications. Antacid and acid-blocking medications are often used for GERD; antispasmodic medications and anti-anxiety medications may be used for IBS.”
Chicken ParmigianaThis recipe is much lower in fat and better than the restaurant version.
Makes 4 servings
• ½ cup egg substitute
• ¾ cup Italia-style or plain bread crumbs
• 1/8 tsp. freshly ground pepper
• 4 boneless, skinless chicken breasts, pounded well with a meat mallet to even the thickness
• Olive or canola cooking spray
• 2 tsp. olive or canola oil
• 1/3 cup beer, sherry, or white wine (optional)
• 1 ½ cups bottled marinara sauce
• ¾ cup grated part-skim mozza rella cheese (or 3 oz. thinly sliced)
• 2 to 3 tbs. grated parmesan cheese
Preparation
1. Put the eggs substitute in a pie plate. On waxed paper, blend the bread crumbs with the pepper. Dip the chicken breasts first in the egg then in the bread crumbs, the repeat to coat well. Set each piece of chicken aside on a plate.
2. Coat a large heavy nonstick skillet generously with cooking spray. Add the oil and heat over medium-high heat until hot. Add the chicken and brown on the bottom, approximately five minutes. Spray the tops of the chicken with cooking spray, flip over, and brown on the second side, approximately five minutes. Add the beer if the pan seems dry.
3. When the chicken is brown on both sides, spoon the sauce over each breast, top with the mozzarella, and sprinkle with the Parmesan. Reduce the heat to low cover and continue cooking for approximately three to five minutes or until the cheese is melted.
Per serving: 394 calories, 41 g protein, 25 g carbohydrate, 14 g fat (4.7 g saturated fat), 87 mg cholesterol, 1 g fiber, 600-1,000 mg sodium. Calories from fat: 33%.
Our Offices
Florida DigestiveSpecialists – St. Pete5767 49th St NSt. Petersburg, FL 33709Tel: (727) 443-4299Fax: (727) 443-0255
Florida DigestiveSpecialists – Clearwater1417 S. Belcher Road, Suite AClearwater, FL 33764Tel: (727) 443-4299Fax: (727) 443-0255
Surgery Center5771 49th St NSt. Petersburg, FL 33709
REQUEST AN APPOINTMENT
hg
Review Us On...
Acid Reflux and IBS
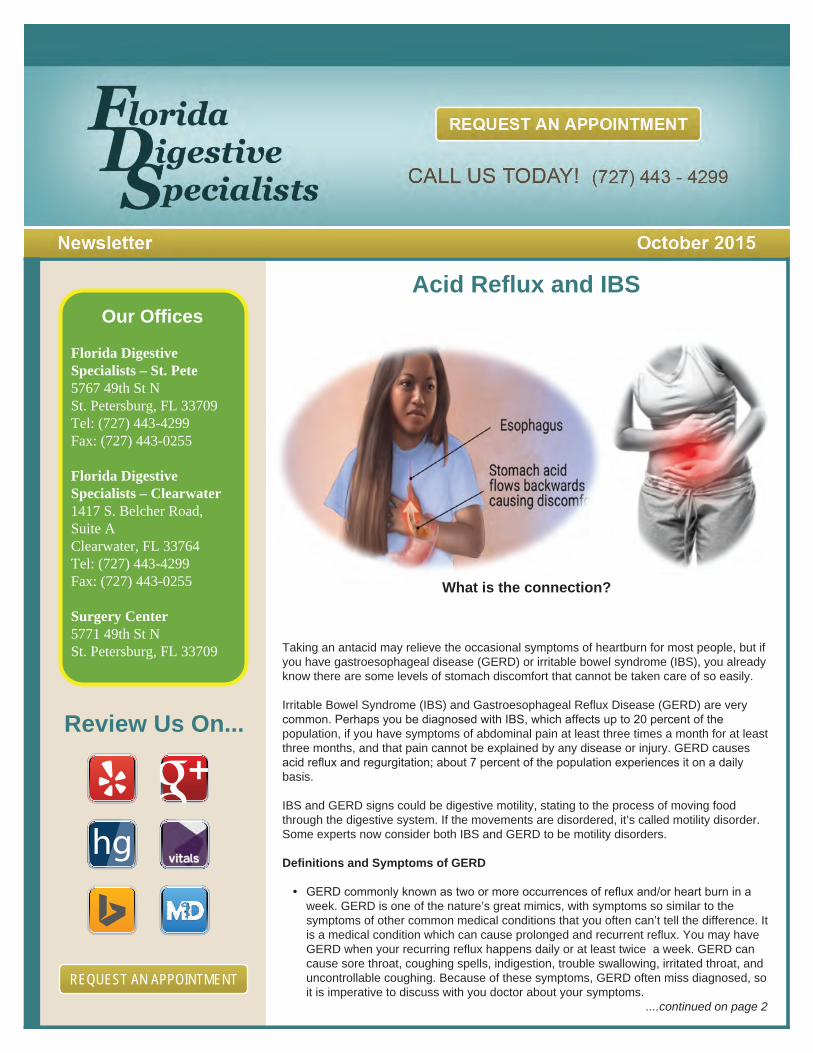
Taking an antacid may relieve the occasional symptoms of heartburn for most people, but if you have gastroesophageal disease (GERD) or irritable bowel syndrome (IBS), you already know there are some levels of stomach discomfort that cannot be taken care of so easily.
Irritable Bowel Syndrome (IBS) and Gastroesophageal Reflux Disease (GERD) are very common. Perhaps you be diagnosed with IBS, which affects up to 20 percent of the population, if you have symptoms of abdominal pain at least three times a month for at least three months, and that pain cannot be explained by any disease or injury. GERD causes acid reflux and regurgitation; about 7 percent of the population experiences it on a daily basis.
IBS and GERD signs could be digestive motility, stating to the process of moving food through the digestive system. If the movements are disordered, it’s called motility disorder. Some experts now consider both IBS and GERD to be motility disorders.
Definitions and Symptoms of GERD
• GERD commonly known as two or more occurrences of reflux and/or heart burn in a week. GERD is one of the nature’s great mimics, with symptoms so similar to the symptoms of other common medical conditions that you often can’t tell the difference. It is a medical condition which can cause prolonged and recurrent reflux. You may have GERD when your recurring reflux happens daily or at least twice a week. GERD can cause sore throat, coughing spells, indigestion, trouble swallowing, irritated throat, and uncontrollable coughing. Because of these symptoms, GERD often miss diagnosed, so it is imperative to discuss with you doctor about your symptoms. ....continued on page 2
....continued from page 1 Acid Reflux and IBS • Examining the Esophagus
- The esophagus is GERD’s main staging area, site of its most classic symptom:
heartburn – a sharp, burning sensation right in the center of your upper abdomen cause by acid reflux hitting the delicate esophageal tissues.
- Heartburn due to reflux is so common that you may assume that anyone with reflux has it. On the contrary, as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) points out:
Everyone with GERD has reflux. Not everyone with reflux has heartburn. But anyone who has heartburn more than twice a week should be evaluated for GERD.
Definitions and Symptoms of IBS The two symptoms of Irritable Bowel Syndrome (IBS) that characterize and truly define this disorder are abdominal pain and disordered bowel function ( either constipation or diarrhea). The presence of abdominal pain is the hallmark of IBS; if the person does not have abdominal pain then he or she cannot be formally diagnosed as having IBS.
IBS is classified as a functional gastrointestinal (GI)disorder. By “functional” we mean that the disorder is in the way of the organ works, not because of a physical problem with the organ that can be identified by an x-ray, like a gastric ulcer. This means that, while patients have symptoms that indicate a problem in the gastrointestinal tract, no problem can be documented when testing is done. Such testing might include laboratory test, x-ray studies, and endoscopic procedure, such as a colonoscopy. Making an accurate and timely diagnosis of IBS is critical for the proper treatment of this condition. First, an accurate diagnosis identifies and provides a name of the multiple symptoms that have been troubling the patient, sometimes for years. Second, the patient learns that there are many other people who have similar symptoms; people with IBS often suffer in silence not realizing that others share similar problems. Third, a definitive diagno-sis provides the opportunity for the patient to become informed about this medical condition.
Why Me? Why Now?
Irritable bowel syndrome is one of the most common disorders treated by the medical practitioners today.
During a typical week, the average family doctor or internist will see more patients with irritable bowel syndrome that patients with asthma, diabetes, hypertension, or cardiovascu-lar disease. Despite being so common, this condition remains widely misunderstood.
Ignorance and misunderstanding regarding IBS are pervasive. It is not only the general public who remain misinformed, but also employers, insurers, and even many physicians. The confusion that surrounds IBS occurs on multiple levels. For example, many people believe that IBS uncommon and that the attention paid to it occurs only because of the actions of a small but vocal group of people with IBS. On the contrary multiple large, population-based research studies have demonstrated that up to 20% of adult Americans suffer from IBS.
Contributing factors in the Development of IBS
This diagram illustrates likely influences in a sequence. Research studies have shown that some people have a genetic predisposition to develop IBS. This predisposition is not a guarantee that IBS will develop, but it does increase the likelihood that IBS will occur. One theory is that, for IBS to develop, a second or third inciting factor needs to be present as well. For example, a common infection of the GI tract early in life ( such as a “stomach flu”) followed by a period of stress might produce the right setting for IBS to develop.
....continued on page 3
What is the connection?
....continued from page 2 Acid Reflux and IBS
Diet and lifestyle changes that reduce stress should benefit both IBS and GERD. An elimination diet that starts with very bland and simple foods, and then introduces new food groups in stages, may help identify foods that trigger symptoms. Each condition may also be treated separately with medications. Antacid and acid-blocking medications are often used for GERD; antispasmodic medications and anti-anxiety medications may be used for IBS.”
Chicken ParmigianaThis recipe is much lower in fat and better than the restaurant version.
Makes 4 servings
• ½ cup egg substitute
• ¾ cup Italia-style or plain bread crumbs
• 1/8 tsp. freshly ground pepper
• 4 boneless, skinless chicken breasts, pounded well with a meat mallet to even the thickness
• Olive or canola cooking spray
• 2 tsp. olive or canola oil
• 1/3 cup beer, sherry, or white wine (optional)
• 1 ½ cups bottled marinara sauce
• ¾ cup grated part-skim mozza rella cheese (or 3 oz. thinly sliced)
• 2 to 3 tbs. grated parmesan cheese
Preparation
1. Put the eggs substitute in a pie plate. On waxed paper, blend the bread crumbs with the pepper. Dip the chicken breasts first in the egg then in the bread crumbs, the repeat to coat well. Set each piece of chicken aside on a plate.
2. Coat a large heavy nonstick skillet generously with cooking spray. Add the oil and heat over medium-high heat until hot. Add the chicken and brown on the bottom, approximately five minutes. Spray the tops of the chicken with cooking spray, flip over, and brown on the second side, approximately five minutes. Add the beer if the pan seems dry.
3. When the chicken is brown on both sides, spoon the sauce over each breast, top with the mozzarella, and sprinkle with the Parmesan. Reduce the heat to low cover and continue cooking for approximately three to five minutes or until the cheese is melted.
Per serving: 394 calories, 41 g protein, 25 g carbohydrate, 14 g fat (4.7 g saturated fat), 87 mg cholesterol, 1 g fiber, 600-1,000 mg sodium. Calories from fat: 33%.
REQUEST AN APPOINTMENT
10 Ways to Improve and
maintain your Weight
1. Begin with breakfast2. Don’t miss meals3. Eat slowly4. Snack on nuts5. Opt for Apples6. Stay hydrated7. Find reason to move8. Take the stairs when possible9. Sleep in10. Add fiber to your diet
Diet and Lifestyle Tips
- Exercise (Exercise helps most patients improve their sense of well being)
- Sleep (Sleep at least 7 to 8 hours per night)
- Soluble fiber (such as oats, beans, barley, bananas, and so on)
- Water (water intake is essential for constipated patients)
Acid Reflux and IBS
Taking an antacid may relieve the occasional symptoms of heartburn for most people, but if you have gastroesophageal disease (GERD) or irritable bowel syndrome (IBS), you already know there are some levels of stomach discomfort that cannot be taken care of so easily.
Irritable Bowel Syndrome (IBS) and Gastroesophageal Reflux Disease (GERD) are very common. Perhaps you be diagnosed with IBS, which affects up to 20 percent of the population, if you have symptoms of abdominal pain at least three times a month for at least three months, and that pain cannot be explained by any disease or injury. GERD causes acid reflux and regurgitation; about 7 percent of the population experiences it on a daily basis.
IBS and GERD signs could be digestive motility, stating to the process of moving food through the digestive system. If the movements are disordered, it’s called motility disorder. Some experts now consider both IBS and GERD to be motility disorders.
Definitions and Symptoms of GERD
• GERD commonly known as two or more occurrences of reflux and/or heart burn in a week. GERD is one of the nature’s great mimics, with symptoms so similar to the symptoms of other common medical conditions that you often can’t tell the difference. It is a medical condition which can cause prolonged and recurrent reflux. You may have GERD when your recurring reflux happens daily or at least twice a week. GERD can cause sore throat, coughing spells, indigestion, trouble swallowing, irritated throat, and uncontrollable coughing. Because of these symptoms, GERD often miss diagnosed, so it is imperative to discuss with you doctor about your symptoms. ....continued on page 2
....continued from page 1 Acid Reflux and IBS • Examining the Esophagus
- The esophagus is GERD’s main staging area, site of its most classic symptom:
heartburn – a sharp, burning sensation right in the center of your upper abdomen cause by acid reflux hitting the delicate esophageal tissues.
- Heartburn due to reflux is so common that you may assume that anyone with reflux has it. On the contrary, as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) points out:
Everyone with GERD has reflux. Not everyone with reflux has heartburn. But anyone who has heartburn more than twice a week should be evaluated for GERD.
Definitions and Symptoms of IBS The two symptoms of Irritable Bowel Syndrome (IBS) that characterize and truly define this disorder are abdominal pain and disordered bowel function ( either constipation or diarrhea). The presence of abdominal pain is the hallmark of IBS; if the person does not have abdominal pain then he or she cannot be formally diagnosed as having IBS.
IBS is classified as a functional gastrointestinal (GI)disorder. By “functional” we mean that the disorder is in the way of the organ works, not because of a physical problem with the organ that can be identified by an x-ray, like a gastric ulcer. This means that, while patients have symptoms that indicate a problem in the gastrointestinal tract, no problem can be documented when testing is done. Such testing might include laboratory test, x-ray studies, and endoscopic procedure, such as a colonoscopy. Making an accurate and timely diagnosis of IBS is critical for the proper treatment of this condition. First, an accurate diagnosis identifies and provides a name of the multiple symptoms that have been troubling the patient, sometimes for years. Second, the patient learns that there are many other people who have similar symptoms; people with IBS often suffer in silence not realizing that others share similar problems. Third, a definitive diagno-sis provides the opportunity for the patient to become informed about this medical condition.
Why Me? Why Now?
Irritable bowel syndrome is one of the most common disorders treated by the medical practitioners today.
During a typical week, the average family doctor or internist will see more patients with irritable bowel syndrome that patients with asthma, diabetes, hypertension, or cardiovascu-lar disease. Despite being so common, this condition remains widely misunderstood.
Ignorance and misunderstanding regarding IBS are pervasive. It is not only the general public who remain misinformed, but also employers, insurers, and even many physicians. The confusion that surrounds IBS occurs on multiple levels. For example, many people believe that IBS uncommon and that the attention paid to it occurs only because of the actions of a small but vocal group of people with IBS. On the contrary multiple large, population-based research studies have demonstrated that up to 20% of adult Americans suffer from IBS.
Contributing factors in the Development of IBS
This diagram illustrates likely influences in a sequence. Research studies have shown that some people have a genetic predisposition to develop IBS. This predisposition is not a guarantee that IBS will develop, but it does increase the likelihood that IBS will occur. One theory is that, for IBS to develop, a second or third inciting factor needs to be present as well. For example, a common infection of the GI tract early in life ( such as a “stomach flu”) followed by a period of stress might produce the right setting for IBS to develop.
....continued on page 3

....continued from page 2 Acid Reflux and IBS
Diet and lifestyle changes that reduce stress should benefit both IBS and GERD. An elimination diet that starts with very bland and simple foods, and then introduces new food groups in stages, may help identify foods that trigger symptoms. Each condition may also be treated separately with medications. Antacid and acid-blocking medications are often used for GERD; antispasmodic medications and anti-anxiety medications may be used for IBS.”
Chicken ParmigianaThis recipe is much lower in fat and better than the restaurant version.
Makes 4 servings
• ½ cup egg substitute
• ¾ cup Italia-style or plain bread crumbs
• 1/8 tsp. freshly ground pepper
• 4 boneless, skinless chicken breasts, pounded well with a meat mallet to even the thickness
• Olive or canola cooking spray
• 2 tsp. olive or canola oil
• 1/3 cup beer, sherry, or white wine (optional)
• 1 ½ cups bottled marinara sauce
• ¾ cup grated part-skim mozza rella cheese (or 3 oz. thinly sliced)
• 2 to 3 tbs. grated parmesan cheese
Preparation
1. Put the eggs substitute in a pie plate. On waxed paper, blend the bread crumbs with the pepper. Dip the chicken breasts first in the egg then in the bread crumbs, the repeat to coat well. Set each piece of chicken aside on a plate.
2. Coat a large heavy nonstick skillet generously with cooking spray. Add the oil and heat over medium-high heat until hot. Add the chicken and brown on the bottom, approximately five minutes. Spray the tops of the chicken with cooking spray, flip over, and brown on the second side, approximately five minutes. Add the beer if the pan seems dry.
3. When the chicken is brown on both sides, spoon the sauce over each breast, top with the mozzarella, and sprinkle with the Parmesan. Reduce the heat to low cover and continue cooking for approximately three to five minutes or until the cheese is melted.
Per serving: 394 calories, 41 g protein, 25 g carbohydrate, 14 g fat (4.7 g saturated fat), 87 mg cholesterol, 1 g fiber, 600-1,000 mg sodium. Calories from fat: 33%.
REQUEST AN APPOINTMENT
Referrals AreEverything
A very special thank you to all of our patients who have kindly referred family and friends to our practice. It means a lot to us that you would trust us with the care of your loved ones. We take pride in the service we provide and will strive to deliver the same thoughtful planning with each and every new patient. THANK YOU FOR YOUR TRUST!!!
Florida DigestiveSpecialists would like to celebrate Halloween with our valued patients. Our staff will/can dress up with their favoritecharacter costume on Thursday October 29th inobservance of Halloween.
Acid Reflux and IBS
Taking an antacid may relieve the occasional symptoms of heartburn for most people, but if you have gastroesophageal disease (GERD) or irritable bowel syndrome (IBS), you already know there are some levels of stomach discomfort that cannot be taken care of so easily.
Irritable Bowel Syndrome (IBS) and Gastroesophageal Reflux Disease (GERD) are very common. Perhaps you be diagnosed with IBS, which affects up to 20 percent of the population, if you have symptoms of abdominal pain at least three times a month for at least three months, and that pain cannot be explained by any disease or injury. GERD causes acid reflux and regurgitation; about 7 percent of the population experiences it on a daily basis.
IBS and GERD signs could be digestive motility, stating to the process of moving food through the digestive system. If the movements are disordered, it’s called motility disorder. Some experts now consider both IBS and GERD to be motility disorders.
Definitions and Symptoms of GERD
• GERD commonly known as two or more occurrences of reflux and/or heart burn in a week. GERD is one of the nature’s great mimics, with symptoms so similar to the symptoms of other common medical conditions that you often can’t tell the difference. It is a medical condition which can cause prolonged and recurrent reflux. You may have GERD when your recurring reflux happens daily or at least twice a week. GERD can cause sore throat, coughing spells, indigestion, trouble swallowing, irritated throat, and uncontrollable coughing. Because of these symptoms, GERD often miss diagnosed, so it is imperative to discuss with you doctor about your symptoms. ....continued on page 2
....continued from page 1 Acid Reflux and IBS • Examining the Esophagus
- The esophagus is GERD’s main staging area, site of its most classic symptom:
heartburn – a sharp, burning sensation right in the center of your upper abdomen cause by acid reflux hitting the delicate esophageal tissues.
- Heartburn due to reflux is so common that you may assume that anyone with reflux has it. On the contrary, as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) points out:
Everyone with GERD has reflux. Not everyone with reflux has heartburn. But anyone who has heartburn more than twice a week should be evaluated for GERD.
Definitions and Symptoms of IBS The two symptoms of Irritable Bowel Syndrome (IBS) that characterize and truly define this disorder are abdominal pain and disordered bowel function ( either constipation or diarrhea). The presence of abdominal pain is the hallmark of IBS; if the person does not have abdominal pain then he or she cannot be formally diagnosed as having IBS.
IBS is classified as a functional gastrointestinal (GI)disorder. By “functional” we mean that the disorder is in the way of the organ works, not because of a physical problem with the organ that can be identified by an x-ray, like a gastric ulcer. This means that, while patients have symptoms that indicate a problem in the gastrointestinal tract, no problem can be documented when testing is done. Such testing might include laboratory test, x-ray studies, and endoscopic procedure, such as a colonoscopy. Making an accurate and timely diagnosis of IBS is critical for the proper treatment of this condition. First, an accurate diagnosis identifies and provides a name of the multiple symptoms that have been troubling the patient, sometimes for years. Second, the patient learns that there are many other people who have similar symptoms; people with IBS often suffer in silence not realizing that others share similar problems. Third, a definitive diagno-sis provides the opportunity for the patient to become informed about this medical condition.
Why Me? Why Now?
Irritable bowel syndrome is one of the most common disorders treated by the medical practitioners today.
During a typical week, the average family doctor or internist will see more patients with irritable bowel syndrome that patients with asthma, diabetes, hypertension, or cardiovascu-lar disease. Despite being so common, this condition remains widely misunderstood.
Ignorance and misunderstanding regarding IBS are pervasive. It is not only the general public who remain misinformed, but also employers, insurers, and even many physicians. The confusion that surrounds IBS occurs on multiple levels. For example, many people believe that IBS uncommon and that the attention paid to it occurs only because of the actions of a small but vocal group of people with IBS. On the contrary multiple large, population-based research studies have demonstrated that up to 20% of adult Americans suffer from IBS.
Contributing factors in the Development of IBS
This diagram illustrates likely influences in a sequence. Research studies have shown that some people have a genetic predisposition to develop IBS. This predisposition is not a guarantee that IBS will develop, but it does increase the likelihood that IBS will occur. One theory is that, for IBS to develop, a second or third inciting factor needs to be present as well. For example, a common infection of the GI tract early in life ( such as a “stomach flu”) followed by a period of stress might produce the right setting for IBS to develop.
....continued on page 3
GeneticPredisposition
Development ofIBS
Manifestation ofIBS symptoms
Stress
History ofabuse
EnvironmentalInfluences
Infection /Inflammation
Stress
Poor CopingSkills
Other factors
Other factors
Parentalmodeling
Anxiety
Somatization
Depression

....continued from page 2 Acid Reflux and IBS
Diet and lifestyle changes that reduce stress should benefit both IBS and GERD. An elimination diet that starts with very bland and simple foods, and then introduces new food groups in stages, may help identify foods that trigger symptoms. Each condition may also be treated separately with medications. Antacid and acid-blocking medications are often used for GERD; antispasmodic medications and anti-anxiety medications may be used for IBS.”
Chicken ParmigianaThis recipe is much lower in fat and better than the restaurant version.
Makes 4 servings
• ½ cup egg substitute
• ¾ cup Italia-style or plain bread crumbs
• 1/8 tsp. freshly ground pepper
• 4 boneless, skinless chicken breasts, pounded well with a meat mallet to even the thickness
• Olive or canola cooking spray
• 2 tsp. olive or canola oil
• 1/3 cup beer, sherry, or white wine (optional)
• 1 ½ cups bottled marinara sauce
• ¾ cup grated part-skim mozza rella cheese (or 3 oz. thinly sliced)
• 2 to 3 tbs. grated parmesan cheese
Preparation
1. Put the eggs substitute in a pie plate. On waxed paper, blend the bread crumbs with the pepper. Dip the chicken breasts first in the egg then in the bread crumbs, the repeat to coat well. Set each piece of chicken aside on a plate.
2. Coat a large heavy nonstick skillet generously with cooking spray. Add the oil and heat over medium-high heat until hot. Add the chicken and brown on the bottom, approximately five minutes. Spray the tops of the chicken with cooking spray, flip over, and brown on the second side, approximately five minutes. Add the beer if the pan seems dry.
3. When the chicken is brown on both sides, spoon the sauce over each breast, top with the mozzarella, and sprinkle with the Parmesan. Reduce the heat to low cover and continue cooking for approximately three to five minutes or until the cheese is melted.
Per serving: 394 calories, 41 g protein, 25 g carbohydrate, 14 g fat (4.7 g saturated fat), 87 mg cholesterol, 1 g fiber, 600-1,000 mg sodium. Calories from fat: 33%.
To Sign Up for Our NewsletterVisit Our Web Site at: www.FLDigestiveSpecialists.com
Acid Reflux and IBS
Taking an antacid may relieve the occasional symptoms of heartburn for most people, but if you have gastroesophageal disease (GERD) or irritable bowel syndrome (IBS), you already know there are some levels of stomach discomfort that cannot be taken care of so easily.
Irritable Bowel Syndrome (IBS) and Gastroesophageal Reflux Disease (GERD) are very common. Perhaps you be diagnosed with IBS, which affects up to 20 percent of the population, if you have symptoms of abdominal pain at least three times a month for at least three months, and that pain cannot be explained by any disease or injury. GERD causes acid reflux and regurgitation; about 7 percent of the population experiences it on a daily basis.
IBS and GERD signs could be digestive motility, stating to the process of moving food through the digestive system. If the movements are disordered, it’s called motility disorder. Some experts now consider both IBS and GERD to be motility disorders.
Definitions and Symptoms of GERD
• GERD commonly known as two or more occurrences of reflux and/or heart burn in a week. GERD is one of the nature’s great mimics, with symptoms so similar to the symptoms of other common medical conditions that you often can’t tell the difference. It is a medical condition which can cause prolonged and recurrent reflux. You may have GERD when your recurring reflux happens daily or at least twice a week. GERD can cause sore throat, coughing spells, indigestion, trouble swallowing, irritated throat, and uncontrollable coughing. Because of these symptoms, GERD often miss diagnosed, so it is imperative to discuss with you doctor about your symptoms. ....continued on page 2
....continued from page 1 Acid Reflux and IBS • Examining the Esophagus
- The esophagus is GERD’s main staging area, site of its most classic symptom:
heartburn – a sharp, burning sensation right in the center of your upper abdomen cause by acid reflux hitting the delicate esophageal tissues.
- Heartburn due to reflux is so common that you may assume that anyone with reflux has it. On the contrary, as the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) points out:
Everyone with GERD has reflux. Not everyone with reflux has heartburn. But anyone who has heartburn more than twice a week should be evaluated for GERD.
Definitions and Symptoms of IBS The two symptoms of Irritable Bowel Syndrome (IBS) that characterize and truly define this disorder are abdominal pain and disordered bowel function ( either constipation or diarrhea). The presence of abdominal pain is the hallmark of IBS; if the person does not have abdominal pain then he or she cannot be formally diagnosed as having IBS.
IBS is classified as a functional gastrointestinal (GI)disorder. By “functional” we mean that the disorder is in the way of the organ works, not because of a physical problem with the organ that can be identified by an x-ray, like a gastric ulcer. This means that, while patients have symptoms that indicate a problem in the gastrointestinal tract, no problem can be documented when testing is done. Such testing might include laboratory test, x-ray studies, and endoscopic procedure, such as a colonoscopy. Making an accurate and timely diagnosis of IBS is critical for the proper treatment of this condition. First, an accurate diagnosis identifies and provides a name of the multiple symptoms that have been troubling the patient, sometimes for years. Second, the patient learns that there are many other people who have similar symptoms; people with IBS often suffer in silence not realizing that others share similar problems. Third, a definitive diagno-sis provides the opportunity for the patient to become informed about this medical condition.
Why Me? Why Now?
Irritable bowel syndrome is one of the most common disorders treated by the medical practitioners today.
During a typical week, the average family doctor or internist will see more patients with irritable bowel syndrome that patients with asthma, diabetes, hypertension, or cardiovascu-lar disease. Despite being so common, this condition remains widely misunderstood.
Ignorance and misunderstanding regarding IBS are pervasive. It is not only the general public who remain misinformed, but also employers, insurers, and even many physicians. The confusion that surrounds IBS occurs on multiple levels. For example, many people believe that IBS uncommon and that the attention paid to it occurs only because of the actions of a small but vocal group of people with IBS. On the contrary multiple large, population-based research studies have demonstrated that up to 20% of adult Americans suffer from IBS.
Contributing factors in the Development of IBS
This diagram illustrates likely influences in a sequence. Research studies have shown that some people have a genetic predisposition to develop IBS. This predisposition is not a guarantee that IBS will develop, but it does increase the likelihood that IBS will occur. One theory is that, for IBS to develop, a second or third inciting factor needs to be present as well. For example, a common infection of the GI tract early in life ( such as a “stomach flu”) followed by a period of stress might produce the right setting for IBS to develop.
....continued on page 3