public health surveillance - c.ymcdn.comc.ymcdn.com/sites/ reports based on a standard case...
TRANSCRIPT
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 1
Slide 1: Introduction
Hello, and welcome to module 7, public health
surveillance. My name is Krissy Simeonsson and
I’m an assistant professor in the Department of
Pediatrics and Public Health at the Brody School
of Medicine.
Slide 2: Acknowledgements
This education module is made possible through
the Centers for Disease Control and Prevention,
and the Association for Prevention Teaching and
Research cooperative agreement. APTR wishes
to acknowledge the following individuals that
developed this module.
Slide 3: Presentation Objectives
Through the course of this presentation we will
start with defining surveillance, then we’ll
discuss some of the uses of surveillance, we’ll
spend some time reviewing notifiable disease
surveillance, and then finally describe some of
surveillance’s limitations.
Developed through the APTR Initiative to Enhance Prevention and Population
Health Education in collaboration with the Brody School of Medicine at East
Carolina University with funding from the Centers for Disease Control and
Prevention
Public Health Surveillance
Developed through the APTR Initiative to Enhance Prevention and Population
Health Education in collaboration with the Brody School of Medicine at East
Carolina University with funding from the Centers for Disease Control and
Prevention
Public Health Surveillance
APTR wishes to acknowledge the following individuals that developed this module:
Kristina Simeonsson, MD, MSPHDepartment of Public Health
Brody School of Medicine at East Carolina University
Julie Daugherty, MPHDepartment of Public Health
Brody School of Medicine at East Carolina University
This education module is made possible through the Centers for Disease Control and Prevention (CDC) and the
Association for Prevention Teaching and Research (APTR) Cooperative Agreement, No. 5U50CD300860. The module
represents the opinions of the author(s) and does not necessarily represent the views of the Centers for Disease
Control and Prevention or the Association for Prevention Teaching and Research.
APTR wishes to acknowledge the following individuals that developed this module:
Kristina Simeonsson, MD, MSPHDepartment of Public Health
Brody School of Medicine at East Carolina University
Julie Daugherty, MPHDepartment of Public Health
Brody School of Medicine at East Carolina University
This education module is made possible through the Centers for Disease Control and Prevention (CDC) and the
Association for Prevention Teaching and Research (APTR) Cooperative Agreement, No. 5U50CD300860. The module
represents the opinions of the author(s) and does not necessarily represent the views of the Centers for Disease
Control and Prevention or the Association for Prevention Teaching and Research.
1. Define surveillance2. Discuss the uses of surveillance3. Review notifiable disease surveillance4. Describe surveillance limitations
1. Define surveillance2. Discuss the uses of surveillance3. Review notifiable disease surveillance4. Describe surveillance limitations
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 2
Slide 4: Surveillance – Information for Action
Surveillance is basically information for action.
This slide displays the 3 public health core
functions, assessment, policy development, and
assurance, which you can see on the outside of
the circle. The multi-colored pieces in the center
represent the 10 Essential Public Health Services.
Surveillance activity occurs as part of the
assessment pieces; monitoring health, and diagnosing and investigating disease, or
health problems. Good surveillance provides data needed to give an accurate
assessment of the status of health in a given population. Good surveillance can also
provide an early warning of disease problems, so immediate control measures can be put
into place. It can also give us information to design and plan public health programs, and
also information to plan and conduct research.
Slide 5: Surveillance
We mentioned previously that surveillance is
information for action, but on this slide a more
formal definition of surveillance is displayed.
Surveillance as defined by the Centers for
Disease Control and Prevention is the ongoing
systematic collection, analysis, and
interpretation of health data, essential to
planning, implementation, and evaluation of public health practice, closely integrated
with the timely dissemination to those who need to know.
Source: http://www.health.gov/phfunctions/public.htmSource: http://www.health.gov/phfunctions/public.htm
The ongoing systematic collection, analysis, and interpretation of health data, essential to the planning, implementation, and evaluation of public health practice, closely integrated with the timely dissemination to those who need to know.
www.cdc.gov
The ongoing systematic collection, analysis, and interpretation of health data, essential to the planning, implementation, and evaluation of public health practice, closely integrated with the timely dissemination to those who need to know.
www.cdc.gov
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 3
Slide 6: Sources of Surveillance Data
Where does surveillance data come from? There
are many sources of surveillance data available.
This slide is only a partial listing of some of the
sources. We are going to review notifiable
disease surveillance later in the presentation.
But some other sources of data that you may be
familiar with include vital records, such as birth
certificates, and death certificates. Environmental monitoring systems, animal health
data, information provided from individuals, information from laboratories, medical
records at outpatient healthcare facilities, as well as hospitals. Over the counter
medication sales can be a source of data. Registries are sources of data, and finally
surveys. Some examples of surveys are population-based surveys such as the National
Health Interview Survey, and the National Health & Nutrition Examination Survey, or
NHANES. And then there are also provider-based surveys. Some examples of these are
the National Ambulatory Medical Care Survey, and also the National Hospital Discharge
Survey, which looks at ICD-9 codes.
Slide 7: Types of Surveillance
Let’s turn now to talk about different types of
surveillance, and there are three types I would
like to discuss in this presentation. Passive
surveillance, active surveillance, and also
syndromic surveillance.
Notifiable diseases Vital records Environmental monitoring systems Animal health data Individuals Laboratories Medical records Over the counter medication sales Registries Surveys
population-based provider-based
Notifiable diseases Vital records Environmental monitoring systems Animal health data Individuals Laboratories Medical records Over the counter medication sales Registries Surveys
population-based provider-based
Passive
Active
Syndromic
Passive
Active
Syndromic
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 4
Slide 8: Passive Surveillance
Passive surveillance is the most common form of
surveillance and occurs when laboratories,
physicians, or other healthcare providers
regularly report cases or disease to the local
health department. These reports are based on
standard case definitions for a particular disease
or condition. Passive surveillance means that the
healthcare provider or laboratory initiates the forwarding of the data to the health
department.
Slide 9: Active Surveillance
A second form of surveillance is active
surveillance. This occurs when the collection of
data from the lab, physician, or other healthcare
provider is initiated by the health department.
Active surveillance is often used during outbreak
investigations or research studies. Active
surveillance has an advantage over passive
surveillance because it achieves more complete and accurate reporting. However, the
draw-back is that it’s more resource intensive for the public health agency that is
conducting the active surveillance. It costs more, it takes more personnel, and more
time to do active surveillance.
Slide 10: Syndromic Surveillance
A third type of surveillance is syndromic
surveillance. It is defined as the ongoing,
systematic collection, analysis, interpretation,
and application of real-time indicators for
disease that allow for detection before public
health authorities would otherwise identify
them. Syndromic surveillance data are collected
in real time, meaning that the data are automated so that they can be received daily, or
even more frequently. The type of data collected is not actual disease, instead we are
interested in specific indicators of disease. The definition of syndromic surveillance,
you’ve probably noticed is similar in ways to the definition of surveillance in general. It’s
on-going and systematic collection, there’s analysis and interpretation of data, however,
the time component and type of data collected are different from passive, or even
active, surveillance. Some common surveillance syndromes are: gastrointestinal illness,
Laboratories, physicians, or others regularly report cases of disease / death to the local or state health department
Case reports based on a standard case definition of that particular disease
Deaths reported on standard certificate
Laboratories, physicians, or others regularly report cases of disease / death to the local or state health department
Case reports based on a standard case definition of that particular disease
Deaths reported on standard certificate
Local or state health departments initiate the collection of information from laboratories, physicians, health care providers or the general population.
Achieves more complete and accurate reporting
More resource intensive for the public health agency
▪ money
▪ personnel
▪ time
Local or state health departments initiate the collection of information from laboratories, physicians, health care providers or the general population.
Achieves more complete and accurate reporting
More resource intensive for the public health agency
▪ money
▪ personnel
▪ time
The ongoing, systematic collection, analysis, interpretation, and application of real-time indicators for disease that allow for detection before public health authorities would otherwise identify them.
Common surveillance syndromes
Gastrointestinal
Influenza-like illness
Rash and Fever
The ongoing, systematic collection, analysis, interpretation, and application of real-time indicators for disease that allow for detection before public health authorities would otherwise identify them.
Common surveillance syndromes
Gastrointestinal
Influenza-like illness
Rash and Fever
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 5
influenza-like illness, or rash and fever syndrome.
Slide 11: Ideal Surveillance System
What are the key features of an ideal
surveillance system? We want the system to be
simple, which means it’s easy to participate in
and the daily operation of it is not too
cumbersome. It also needs to be timely, data
that’s not available when we need it, is not
helpful for planning or response. It needs to be
representative, which means that a surveillance system needs to collect data that’s
representative of the population that we’re following. It needs to be flexible, which
means at certain times, such as outbreak situations, you need to be able to ramp it up,
but then in times when there are not a lot of cases you need to be able to scale back. It
needs to be sensitive and have strong predictive value, which we’ll talk about in the next
few slides. It certainly needs to be acceptable. Both the public and healthcare providers
need to feel like what they’re doing makes sense, and that it’s not too intrusive. And
finally, an ideal surveillance system needs to be cost effective.
Slide 12: Ideal Surveillance System
So in the next few slides we’re going to spend a
little bit more time talking about these two
characteristics (Sensitive and Strong Predictive
Value) of an ideal surveillance system.
Simple Timely Representative Flexible Sensitive Strong predictive value Acceptable
public
health care providers Cost-effective
Simple Timely Representative Flexible Sensitive Strong predictive value Acceptable
public
health care providers Cost-effective
Simple Timely Representative Flexible Sensitive Strong predictive value Acceptable
public
health care providers Cost effective
Simple Timely Representative Flexible Sensitive Strong predictive value Acceptable
public
health care providers Cost effective
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 6
Slide 13: Ideal Surveillance System – Sensitivity
and Predictive Value
For an ideal surveillance system to be sensitive,
we want it to not miss many cases. We want to
have few, if any, missed cases of the disease
we’re trying to track. We increase the sensitivity
of a surveillance system by having very broad
case definitions, which means that we capture
cases that may not actually be cases by only have a few characteristics that we’re looking
for, for each disease. Clearly, the problem with that is there will be cases counted that
might not actually be true cases of disease. But if you really are trying to catch every
case out there, and not miss any then we have to have a sensitive surveillance system.
The flip side of that is positive predictive value of a surveillance system. All case reports
that we are receiving for a disease or illness meet the case definition; we can feel fairly
certain that any cases we’re capturing in our system truly represent cases. We can
increase the predictive value of a surveillance system by adopting a more restrictive case
definition: individuals have to match more characteristics of a disease to be counted as a
case. There is a balance, or a trade-off, between sensitivity and predictive value of a
surveillance system.
Slide 12: Uses of Public Health Surveillance
Next we’re going to talk a little bit about the uses
of public health surveillance. Public health
surveillance can be used to estimate the
magnitude of a health problem; it can help us
determine the geographic distribution of an
illness. It helps to portray the natural history of a
disease, is it on the rise, is it on the decline? It
helps us detect epidemics, or define problems in the community. It can help us generate
hypotheses, and stimulate research. It helps us evaluate our control measures. We can
monitor changes in infectious agents, for examples whether certain bacteria are
becoming more resistant to some of the antibiotics that are in use. Surveillance helps us
detect changes in health practices; are more people getting screened in a community, or
are less people, and what are the barriers? Finally, surveillance can help us facilitate
planning.
Sensitivity
Few if any missed cases
Increase by having broad case definitions
Positive predictive value
Almost all case reports received for illnesses meet the surveillance case definition
Increase by adopting a more restrictive case definition
Hopkins, R. 2005
Sensitivity
Few if any missed cases
Increase by having broad case definitions
Positive predictive value
Almost all case reports received for illnesses meet the surveillance case definition
Increase by adopting a more restrictive case definition
Hopkins, R. 2005
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
http://www.cdc.gov/osels/ph_surveillance/nndss/phs/overview.htm
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
http://www.cdc.gov/osels/ph_surveillance/nndss/phs/overview.htm
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 7
Slide 13: Uses of Public Health Surveillance
Let’s follow with a few examples. The first
example is going to illustrate how surveillance
helps us estimate the magnitude of a problem,
and also at the same time determine the
geographic distribution of illness.
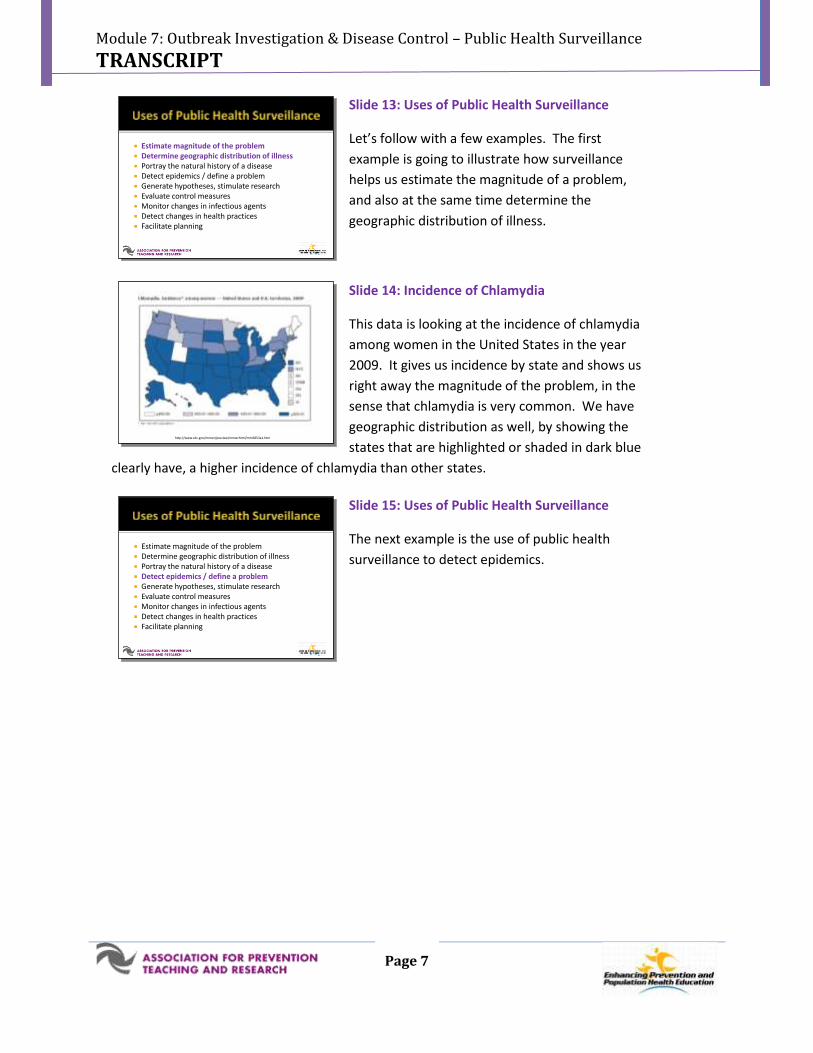
Slide 14: Incidence of Chlamydia
This data is looking at the incidence of chlamydia
among women in the United States in the year
2009. It gives us incidence by state and shows us
right away the magnitude of the problem, in the
sense that chlamydia is very common. We have
geographic distribution as well, by showing the
states that are highlighted or shaded in dark blue
clearly have, a higher incidence of chlamydia than other states.
Slide 15: Uses of Public Health Surveillance
The next example is the use of public health
surveillance to detect epidemics.
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5853a1.htmhttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5853a1.htm
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 8
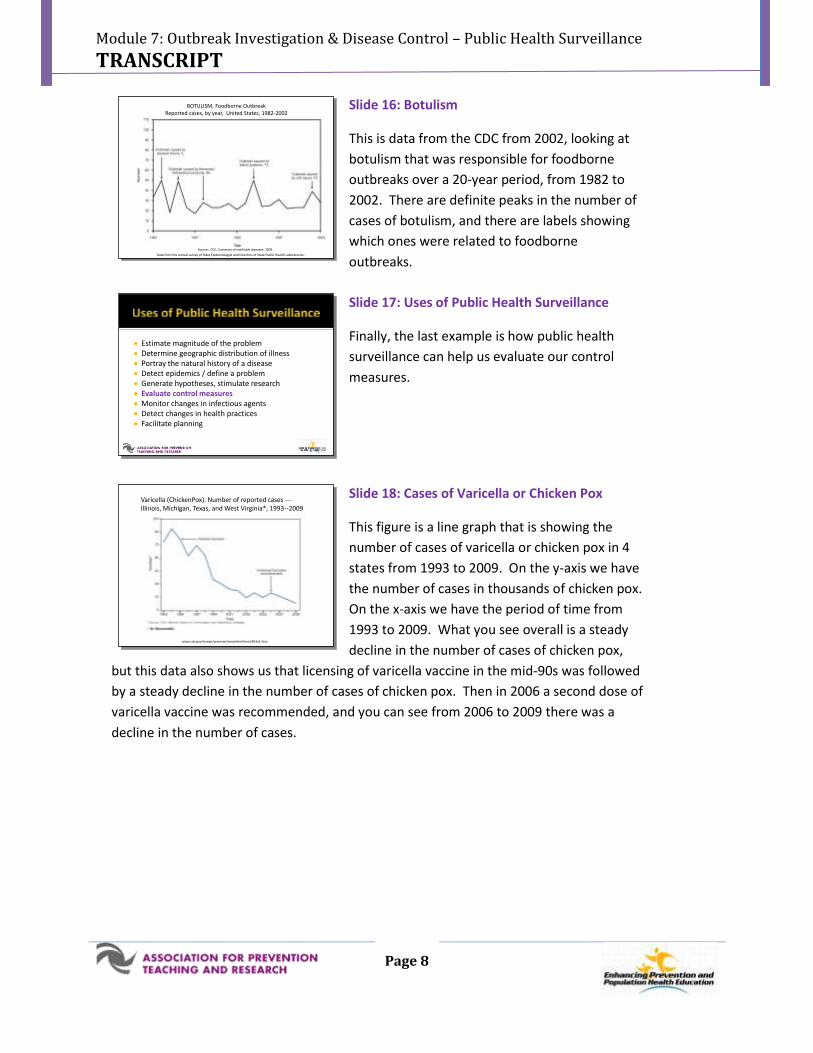
Slide 16: Botulism
This is data from the CDC from 2002, looking at
botulism that was responsible for foodborne
outbreaks over a 20-year period, from 1982 to
2002. There are definite peaks in the number of
cases of botulism, and there are labels showing
which ones were related to foodborne
outbreaks.
Slide 17: Uses of Public Health Surveillance
Finally, the last example is how public health
surveillance can help us evaluate our control
measures.
Slide 18: Cases of Varicella or Chicken Pox
This figure is a line graph that is showing the
number of cases of varicella or chicken pox in 4
states from 1993 to 2009. On the y-axis we have
the number of cases in thousands of chicken pox.
On the x-axis we have the period of time from
1993 to 2009. What you see overall is a steady
decline in the number of cases of chicken pox,
but this data also shows us that licensing of varicella vaccine in the mid-90s was followed
by a steady decline in the number of cases of chicken pox. Then in 2006 a second dose of
varicella vaccine was recommended, and you can see from 2006 to 2009 there was a
decline in the number of cases.
BOTULISM, Foodborne OutbreakReported cases, by year, United States, 1982-2002
Source: CDC. Summary of notifiable diseases. 2002.
Data from the annual survey of State Epidemiologist and Directors of State Public Health Laboratories..
BOTULISM, Foodborne OutbreakReported cases, by year, United States, 1982-2002
Source: CDC. Summary of notifiable diseases. 2002.
Data from the annual survey of State Epidemiologist and Directors of State Public Health Laboratories..
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
Estimate magnitude of the problem Determine geographic distribution of illness Portray the natural history of a disease Detect epidemics / define a problem Generate hypotheses, stimulate research Evaluate control measures Monitor changes in infectious agents Detect changes in health practices Facilitate planning
Varicella (ChickenPox). Number of reported cases ---Illinois, Michigan, Texas, and West Virginia*, 1993--2009
www.cdc.gov/mmwr/preview/mmwrhtml/mm5853a1.htm
Varicella (ChickenPox). Number of reported cases ---Illinois, Michigan, Texas, and West Virginia*, 1993--2009
www.cdc.gov/mmwr/preview/mmwrhtml/mm5853a1.htm
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 9
Slide 19: Notifiable Disease Surveillance
We are going to turn now to notifiable disease
reporting. It has been said that no health
department can effectively prevent or control
disease without knowledge of when, where, and
under what conditions cases are occurring.
Public health agencies monitor diseases and
conditions of importance by designating them as
notifiable. The foundation of notifiable disease surveillance is the state and local
application of the National Notifiable Disease Surveillance System. A list of nationally
notifiable diseases is available at the Centers for Disease Control and Prevention website.
You will find that most of the diseases are infectious in nature, but there are some that
are non-infectious, and I’ve listed some of the examples here. Cancer, elevated blood
lead levels, and pesticide-related illness are just some examples of conditions that are
reportable, but are non-infectious.
Slide 20: National Notifiable Disease
Surveillance System (NNDSS)
The National Notifiable Disease Surveillance
System is a system for passing reports from local
and state public health agencies through to the
CDC. There is a role for the Council and State
and Territorial Epidemiologists (CSTE) who work
closely with the CDC in revising the list of
nationally notifiable disease every year. The CDC keeps a list of disease and laboratory
findings of public health interest, and also with support from the CSTE, maintains case
definitions for their surveillance. The CDC also works to disseminate surveillance data
back to healthcare providers. They do this through the Morbidity and Mortality Weekly
Report (MMWR). They also publish an Annual summary of Notifiable Diseases.
Foundation is state and local application of the reportable disease surveillance system known as National Notifiable Disease Surveillance System (NNDSS)
Infectious reportable diseases
Noninfectious reportable diseases
▪ Cancer
▪ Elevated blood lead levels
▪ Pesticide-related illness
Foundation is state and local application of the reportable disease surveillance system known as National Notifiable Disease Surveillance System (NNDSS)
Infectious reportable diseases
Noninfectious reportable diseases
▪ Cancer
▪ Elevated blood lead levels
▪ Pesticide-related illness
System for passing reports from the local to state health departments, and then on to CDC
Role of the Council of State and Territorial Epidemiologists (CSTE)
List of disease and laboratory findings of public health interest
Case definitions for their surveillance
Dissemination of surveillance data
Morbidity and Mortality Weekly Report (MMWR)
MMWR Annual Summary of Notifiable Diseases
System for passing reports from the local to state health departments, and then on to CDC
Role of the Council of State and Territorial Epidemiologists (CSTE)
List of disease and laboratory findings of public health interest
Case definitions for their surveillance
Dissemination of surveillance data
Morbidity and Mortality Weekly Report (MMWR)
MMWR Annual Summary of Notifiable Diseases
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 10
Slide 21: Case Definitions
This is an example of a case definition that you
can find at the CDC website. This is the 2011
case definition for hepatitis A, which is a
nationally notifiable disease. The case definition
includes a clinical component, a laboratory
component, and an epidemiologic component,
(often used during outbreak investigations).
Slide 22: MMWR Annual Summary of Notifiable
Diseases
The CDC disseminates surveillance data back to
providers. More detailed information is
published in the MMWR Annual Summary of
Notifiable Diseases. In this publication, data for
all reportable or notifiable diseases are
published, along with a brief summary of the
year’s activity and information on recent case definitions. At the end of the report are
summary tables and maps. This is an example of a map showing the rate of newly
reported AIDS cases per 100,000 people in the United States in 2002. The information
from the CDC is invaluable source for learning about and understanding the broad scope
of disease surveillance around the country. It also allows healthcare professionals and
public health officials to see what’s going on in their own state, as well as other states
around them. Finally, the publication of these reports shows the collaborative nature of
surveillance. Without the work of healthcare providers and local health departments
these data would not be available.
Uniform criteria for reporting cases
Clinical, Laboratory, Epidemiologic
http://www.cdc.gov/osels/ph_surveillance/nndss/casedef/hepatitisacurrent.htm
Uniform criteria for reporting cases
Clinical, Laboratory, Epidemiologic
http://www.cdc.gov/osels/ph_surveillance/nndss/casedef/hepatitisacurrent.htm
MMWR Annual Summary of Notifiable Diseases
http://www.cdc.gov/mmwr/PDF/wk/mm5754.pdf
MMWR Annual Summary of Notifiable Diseases
http://www.cdc.gov/mmwr/PDF/wk/mm5754.pdf
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 11
Slide 23: State Participation in NNDSS
State participation in the National Notifiable
Disease Surveillance System is voluntary. There is
not a legal requirement that states have to
participate in this system; however, all states
choose to participate. Reporting of notifiable
disease is mandated at the state level and the list
of diseases varies by state. Reportable
conditions are determined by laws and regulations of each state and jurisdiction. Some
conditions deemed nationally notifiable might not be reportable in certain states or
jurisdictions. It’s important as a healthcare provider to know what the list of diseases
that are notifiable, are in the states that you’re practicing in.
Slide 24: Example of Physician Report –
Hepatitis B
The next few slides are going to highlight
examples of healthcare providers who did their
part in surveillance and reported a notifiable
disease to their local health department. The
first is an example of a physician who reported a
case of hepatitis B to the local health
department. This case of acute hepatitis B was in a resident of a long-term care facility,
who was admitted to the hospital with hepatitis B. After the physician made the report
for this one case, the health department nurse remembered that there were several
other cases of acute hepatitis B that had occurred recently at the same long-term care
facility. An investigation was begun, and an unsuspected outbreak was discovered at the
long-term care facility.
Slide 25: Example of Physician Report –
Hepatitis B
These cases ended up being part of a larger study
that looked at the transmission of hepatitis B
virus among people undergoing blood glucose
monitoring in long-term care facilities
Reporting by states to the CDC is voluntary Reporting mandated at state level
state legislation or regulation
Variation in the lists of reportable diseases exists between states
Reporting by states to the CDC is voluntary Reporting mandated at state level
state legislation or regulation
Variation in the lists of reportable diseases exists between states
Resident of long-term care facility hospitalized with acute hepatitis B
Physician reports case to local health department (LHD)
▪ LHD nurse remembers several other cases of acute hepatitis B at same facility in past year
▪ Unsuspected outbreak of acute hepatitis B was discovered in the facility
Resident of long-term care facility hospitalized with acute hepatitis B
Physician reports case to local health department (LHD)
▪ LHD nurse remembers several other cases of acute hepatitis B at same facility in past year
▪ Unsuspected outbreak of acute hepatitis B was discovered in the facility
MMWR, March 11, 2005 / 54(09);220-223MMWR, March 11, 2005 / 54(09);220-223
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 12
Slide 26: Example of Physician Report –
Listeriosis
Another example is a health care provider who
reported a case of listeriosis to their local health
department. This was a pediatrician who
attended a delivery of a stillborn infant. The
physician reported this case to the local health
department and because of this case report and
further investigation, the health department discovered an outbreak of listeriosis,
identified among Hispanic females with 12 cases identified over four months. There
were five stillbirths associated with this outbreak, three premature births and two
newborns who were infected with listeriosis. A case control study was performed to
discover what the source of the exposure was for all of these cases.
Slide 27: Example of Physician Report –
Listeriosis
Investigators found that the source of the
outbreak of Listeriosis was associated with
homemade Mexican style cheese or queso
fresco.
Slide 28: Example of Physician Report –
Listeriosis
This is one of the samples that was tested during
this outbreak investigation. Again this outbreak
was initially identified because a healthcare
provider had reported the disease to the local
health department.
Stillborn infant delivered at hospital diagnosed with listeriosis
Physician reports case to LHD
▪ Outbreak of listeriosis was identified among Hispanic females with 12 cases identified over 4 month period
5 stillbirths
3 premature births
2 infected newborns
▪ Case-control study identified common source of exposure
Stillborn infant delivered at hospital diagnosed with listeriosis
Physician reports case to LHD
▪ Outbreak of listeriosis was identified among Hispanic females with 12 cases identified over 4 month period
5 stillbirths
3 premature births
2 infected newborns
▪ Case-control study identified common source of exposure
MMWR, July 06, 2001 / 50(26);560-2MMWR, July 06, 2001 / 50(26);560-2
Used with permission from Robert E. WhitwamUsed with permission from Robert E. Whitwam
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 13
Slide 29: Limitations of Surveillance
With all systems and programs there are
limitations. Some of the limitations of
surveillance systems are listed here. We’re
always dealing with incomplete data. There's
overwhelming volumes of data sometimes
coming in from a variety of sources which makes
the organization and management of all that
data complicated. With the continuing advancement of information technology, there's
uneven application of surveillance. Some jurisdictions still have paper-based reporting,
where case reports are completed on paper and mailed in or faxed. There is a transition
over to electronic reporting or internet-based reporting. So we're in a period of
transition with an uneven application of the information technology; two systems trying
to merge together. Timeliness is an issue, how fast can we get the data that we need?
Completeness of the data that's being reported is another issue. Sometimes cases aren’t
reported at all and sometimes the cases that are reported have data that's missing.
Trying to improve all of these areas are challenges that public health agencies face on a
daily basis.
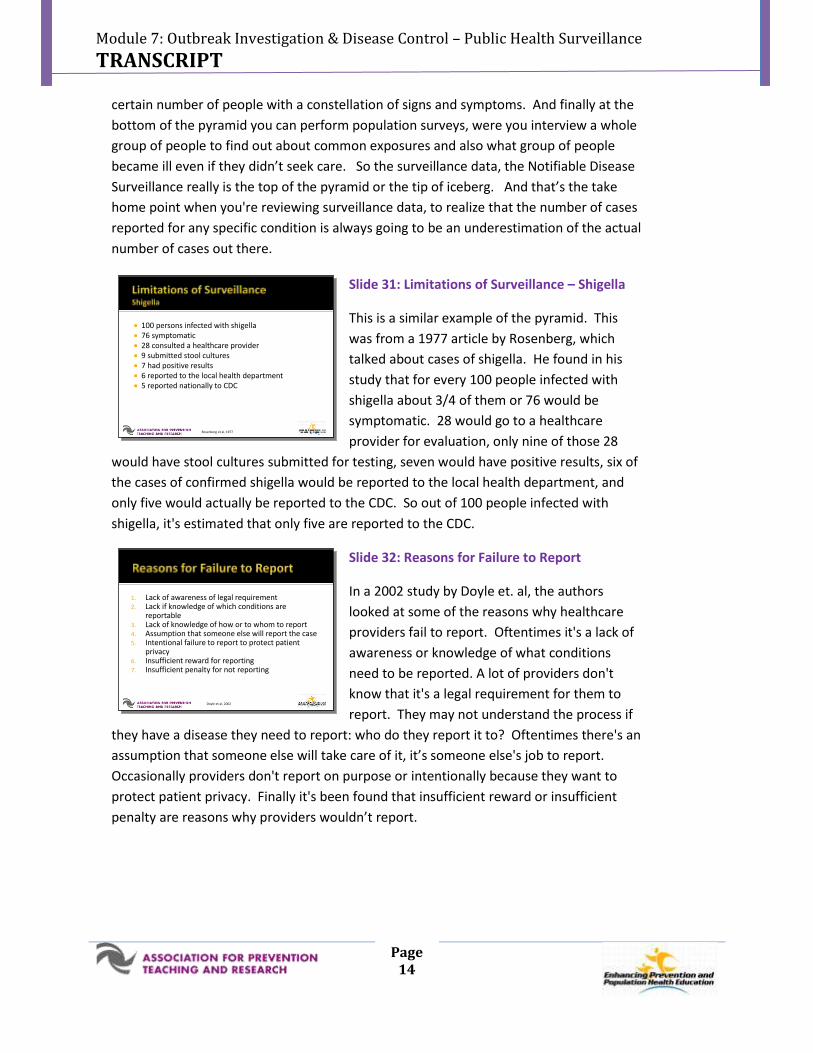
Slide 30: Burden of Illness Pyramid
The burden of illness pyramid depicted here is a
model for understanding foodborne disease
reporting. This illustrates steps that must occur
for an episode of illness in the population to be
registered in a surveillance database. Starting
from the bottom of the pyramid, the areas in
yellow, shows that some members of the general
population can be exposed to an organism, but not all of them will become ill. The next
line of the pyramid represents people who do become ill. In the pink portion of the
pyramid, a percentage of people who become ill will seek care, and of those that do seek
care, in a proportion of them a specimen will be obtained. Then in the purple portion of
the pyramid some of those lab tests will be submitted for the organism of interest and
the laboratory will confirm a case. Only a small proportion of those will be reported to
the health department, which represents that very small section at the top of the
pyramid in green. You can get data on foodborne illnesses in other ways; surveillance is
really just the tip of the iceberg in terms of diseases that are reported to the health
department. There are surveys that are done at the laboratory level to look at what lab
tests are positive. Active surveillance can involve a physician survey targeting that pink
portion of the pyramid, where you can actually ask healthcare providers if they've seen a
Incomplete data Overwhelming volumes of data from a variety of
sources make management complex Uneven application of information technology
Paper versus electronic reporting Timeliness
Reporting time requirement
Reporting burden Completeness
Unreported cases
Incomplete reports
Incomplete data Overwhelming volumes of data from a variety of
sources make management complex Uneven application of information technology
Paper versus electronic reporting Timeliness
Reporting time requirement
Reporting burden Completeness
Unreported cases
Incomplete reports
CDC’s Burden of Illness Pyramid: Underascertainment of Foodborne Illness in Notifiable Diseases Surveillance
Source: Adapted from Centers for Disease Control and Prevention, “FoodNet Surveillance - Burden of Illness Pyramid.” http://www.cdc.gov/foodnet/surveillance_pages/burden_pyramid.htm. Accessed October 3, 2011.
CDC’s Burden of Illness Pyramid: Underascertainment of Foodborne Illness in Notifiable Diseases Surveillance
Source: Adapted from Centers for Disease Control and Prevention, “FoodNet Surveillance - Burden of Illness Pyramid.” http://www.cdc.gov/foodnet/surveillance_pages/burden_pyramid.htm. Accessed October 3, 2011.
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 14
certain number of people with a constellation of signs and symptoms. And finally at the
bottom of the pyramid you can perform population surveys, were you interview a whole
group of people to find out about common exposures and also what group of people
became ill even if they didn’t seek care. So the surveillance data, the Notifiable Disease
Surveillance really is the top of the pyramid or the tip of iceberg. And that’s the take
home point when you're reviewing surveillance data, to realize that the number of cases
reported for any specific condition is always going to be an underestimation of the actual
number of cases out there.
Slide 31: Limitations of Surveillance – Shigella
This is a similar example of the pyramid. This
was from a 1977 article by Rosenberg, which
talked about cases of shigella. He found in his
study that for every 100 people infected with
shigella about 3/4 of them or 76 would be
symptomatic. 28 would go to a healthcare
provider for evaluation, only nine of those 28
would have stool cultures submitted for testing, seven would have positive results, six of
the cases of confirmed shigella would be reported to the local health department, and
only five would actually be reported to the CDC. So out of 100 people infected with
shigella, it's estimated that only five are reported to the CDC.
Slide 32: Reasons for Failure to Report
In a 2002 study by Doyle et. al, the authors
looked at some of the reasons why healthcare
providers fail to report. Oftentimes it's a lack of
awareness or knowledge of what conditions
need to be reported. A lot of providers don't
know that it's a legal requirement for them to
report. They may not understand the process if
they have a disease they need to report: who do they report it to? Oftentimes there's an
assumption that someone else will take care of it, it’s someone else's job to report.
Occasionally providers don't report on purpose or intentionally because they want to
protect patient privacy. Finally it's been found that insufficient reward or insufficient
penalty are reasons why providers wouldn’t report.
100 persons infected with shigella 76 symptomatic 28 consulted a healthcare provider 9 submitted stool cultures 7 had positive results 6 reported to the local health department 5 reported nationally to CDC
Rosenberg et al, 1977
100 persons infected with shigella 76 symptomatic 28 consulted a healthcare provider 9 submitted stool cultures 7 had positive results 6 reported to the local health department 5 reported nationally to CDC
Rosenberg et al, 1977
1. Lack of awareness of legal requirement2. Lack if knowledge of which conditions are
reportable3. Lack of knowledge of how or to whom to report4. Assumption that someone else will report the case5. Intentional failure to report to protect patient
privacy6. Insufficient reward for reporting7. Insufficient penalty for not reporting
Doyle et al, 2002
1. Lack of awareness of legal requirement2. Lack if knowledge of which conditions are
reportable3. Lack of knowledge of how or to whom to report4. Assumption that someone else will report the case5. Intentional failure to report to protect patient
privacy6. Insufficient reward for reporting7. Insufficient penalty for not reporting
Doyle et al, 2002
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 15
Slide 33: Limitations of Syndromic Surveillance
I wanted to mention limitations of syndromic
surveillance as well. We’ve mentiond that
syndromic surveillance certainly has advantages
over passive surveillance because it's real time
data, it’s automated, it's coming in quickly. But
syndromic surveillance systems are costly and
they require resources to bring together all of
the different syndromic data from hospitals, ambulance transport, poison control
centers, and even school absenteeism as part of the syndromic surveillance system.
They require significant staff expertise and dedicated time. We talked early on about an
ideal surveillance system would be simple, but certainly syndromic surveillance requires
staff expertise. Finally formal evaluations of existing syndromic surveillance systems are
incomplete, so the data still out on how well these work in terms of how cost effective
they are. It’s important to keep in mind that syndromic surveillance systems are not
meant to replace regular surveillance systems but rather to enhance the data that we are
already getting from a passive surveillance system.
Slide 34: Limitations of Syndromic Surveillance
Other limitations of syndromic surveillance are
false alarms and failure to detect outbreaks.
False alarms can occur because of non-specific
case definitions. Syndromic surveillance systems
are run off software that recognizes keywords as
part of the syndrome’s case definition (e.g. fever
and rash). This results in many more cases being
picked up that aren’t representative; these are considered false alarms. There can also
be inadequate sensitivity meaning syndromic surveillance is not detecting all outbreaks
or bioterrorism events. This can occur if the outbreak is too small to raise a red flag that
the number of cases has gone beyond a set threshold. Also, if this syndromic
surveillance data are coming from a number of different healthcare facilities across a
state or region, an outbreak can be missed. If a group of people is exposed in one
location but disperses after the event, the cluster may not be evident via syndromic
surveillance.
Costly
Staff expertise required
Formal evaluations of syndromic surveillance systems are incomplete
Costly
Staff expertise required
Formal evaluations of syndromic surveillance systems are incomplete
Inadequate specificity = false alarms Software recognizes key words
Uses resources in investigation
Inadequate sensitivity = failure to detect outbreaks or bioterrorism events Outbreak is too small
Population disperses after exposure, cluster not evident
Inadequate specificity = false alarms Software recognizes key words
Uses resources in investigation
Inadequate sensitivity = failure to detect outbreaks or bioterrorism events Outbreak is too small
Population disperses after exposure, cluster not evident
Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 16
Slide 35: Summary
In summary, surveillance data has many practical
uses and is the crux of the public health core
function assessment. Notifiable disease
surveillance is fundamental to prevention and
control efforts in public health. Regardless of
where you practice the list of notifiable diseases
is going to vary by state. Finally we've talked
about limitations in surveillance, but significant improvements are being made in
advancing surveillance and reporting, so stay tuned and make sure you understand your
role in this vital public health function.
Center for Public Health Continuing EducationUniversity at Albany School of Public Health
Department of Community & Family MedicineDuke University School of Medicine
Mike Barry, CAELorrie Basnight, MDNancy Bennett, MD, MSRuth Gaare Bernheim, JD, MPHAmber Berrian, MPHJames Cawley, MPH, PA-CJack Dillenberg, DDS, MPHKristine Gebbie, RN, DrPHAsim Jani, MD, MPH, FACP
Denise Koo, MD, MPHSuzanne Lazorick, MD, MPHRika Maeshiro, MD, MPHDan Mareck, MDSteve McCurdy, MD, MPHSusan M. Meyer, PhDSallie Rixey, MD, MEdNawraz Shawir, MBBS
Surveillance data has many practical uses Notifiable disease surveillance is fundamental to
prevention and control efforts List of notifiable diseases varies by state Significant improvements are being made in
advancing surveillance and reporting
Surveillance data has many practical uses Notifiable disease surveillance is fundamental to
prevention and control efforts List of notifiable diseases varies by state Significant improvements are being made in
advancing surveillance and reporting

Module 7: Outbreak Investigation & Disease Control – Public Health Surveillance
TRANSCRIPT
Page 17
Sharon Hull, MD, MPHPresident
Allison L. LewisExecutive Director
O. Kent Nordvig, MEd
Project Representative